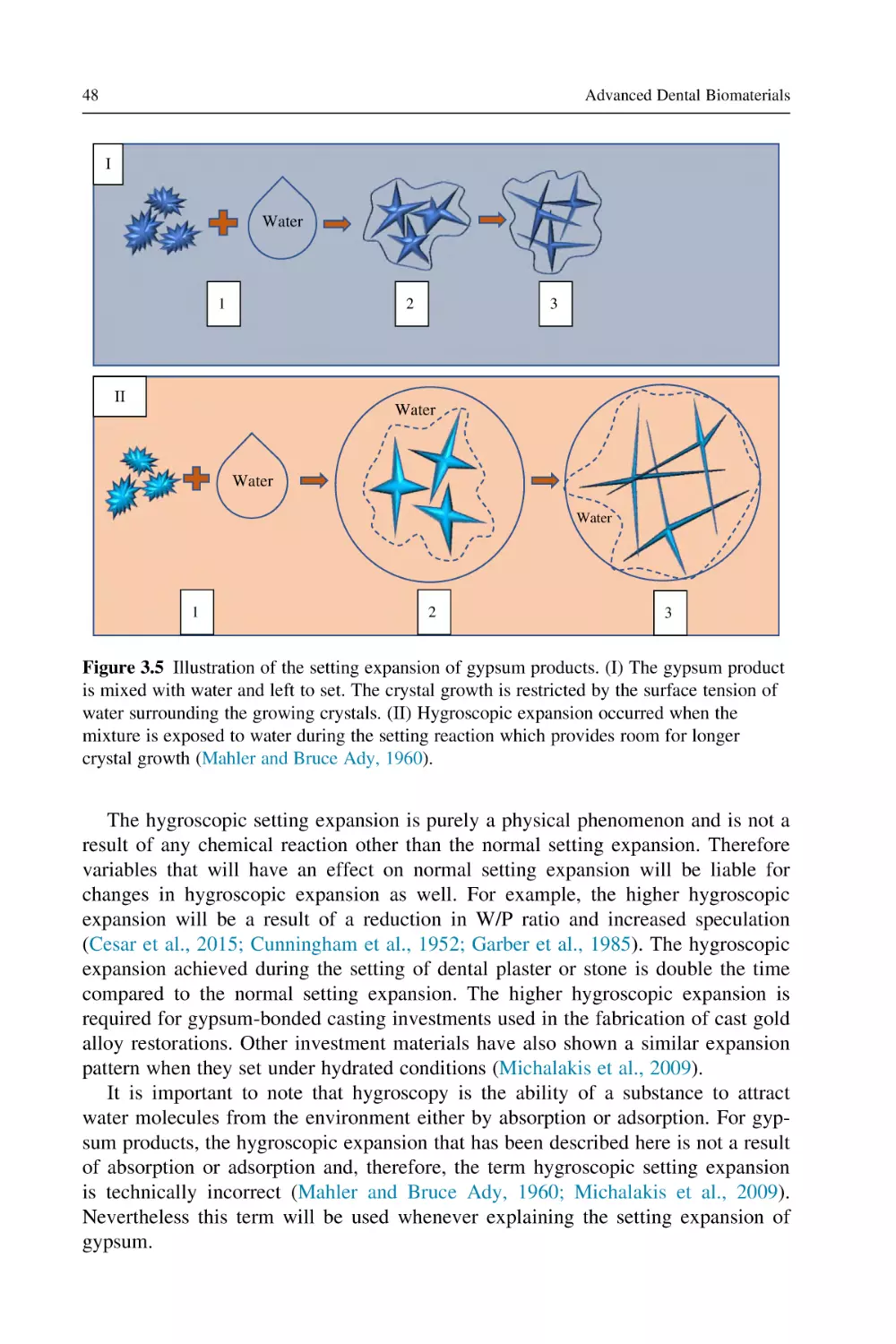
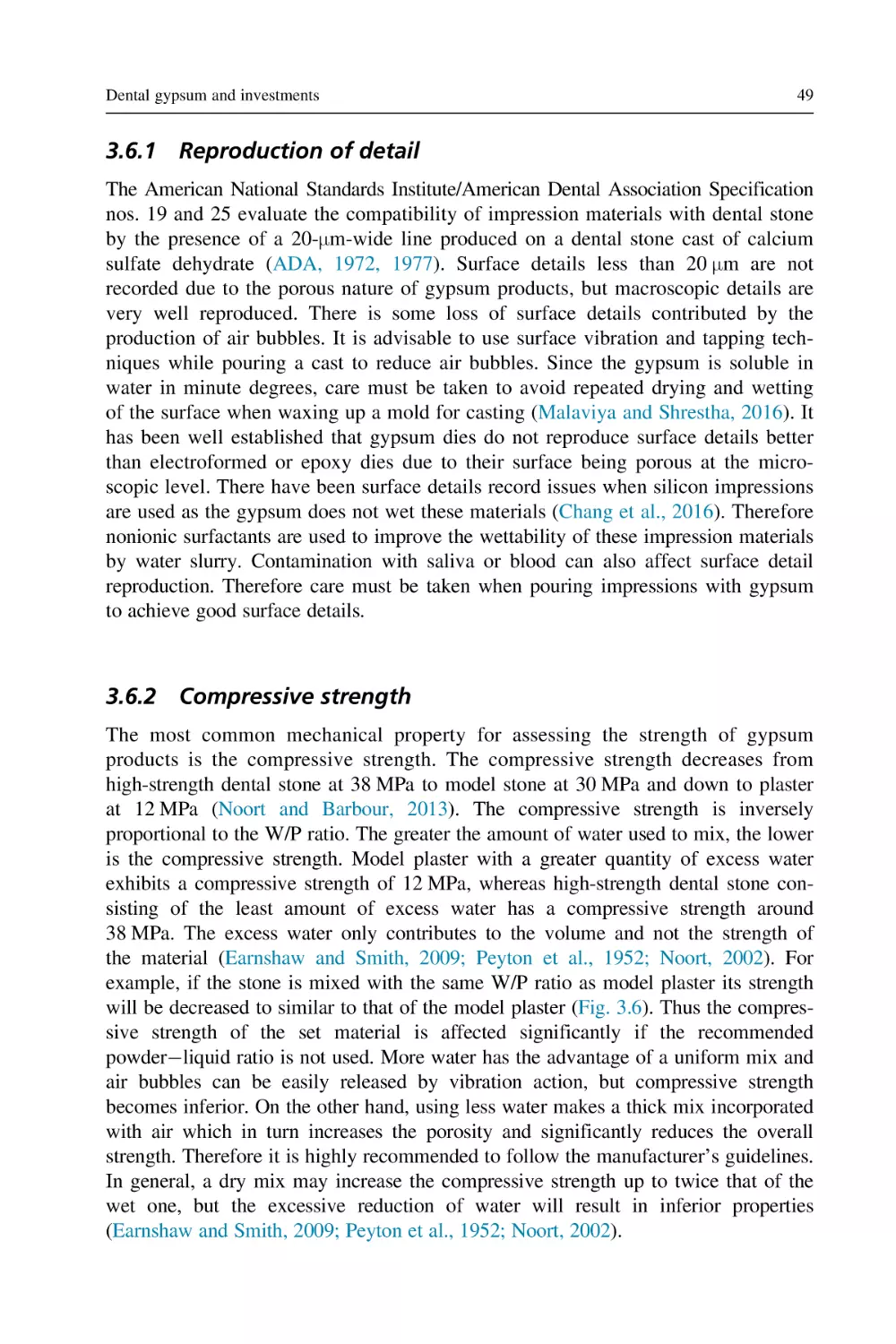
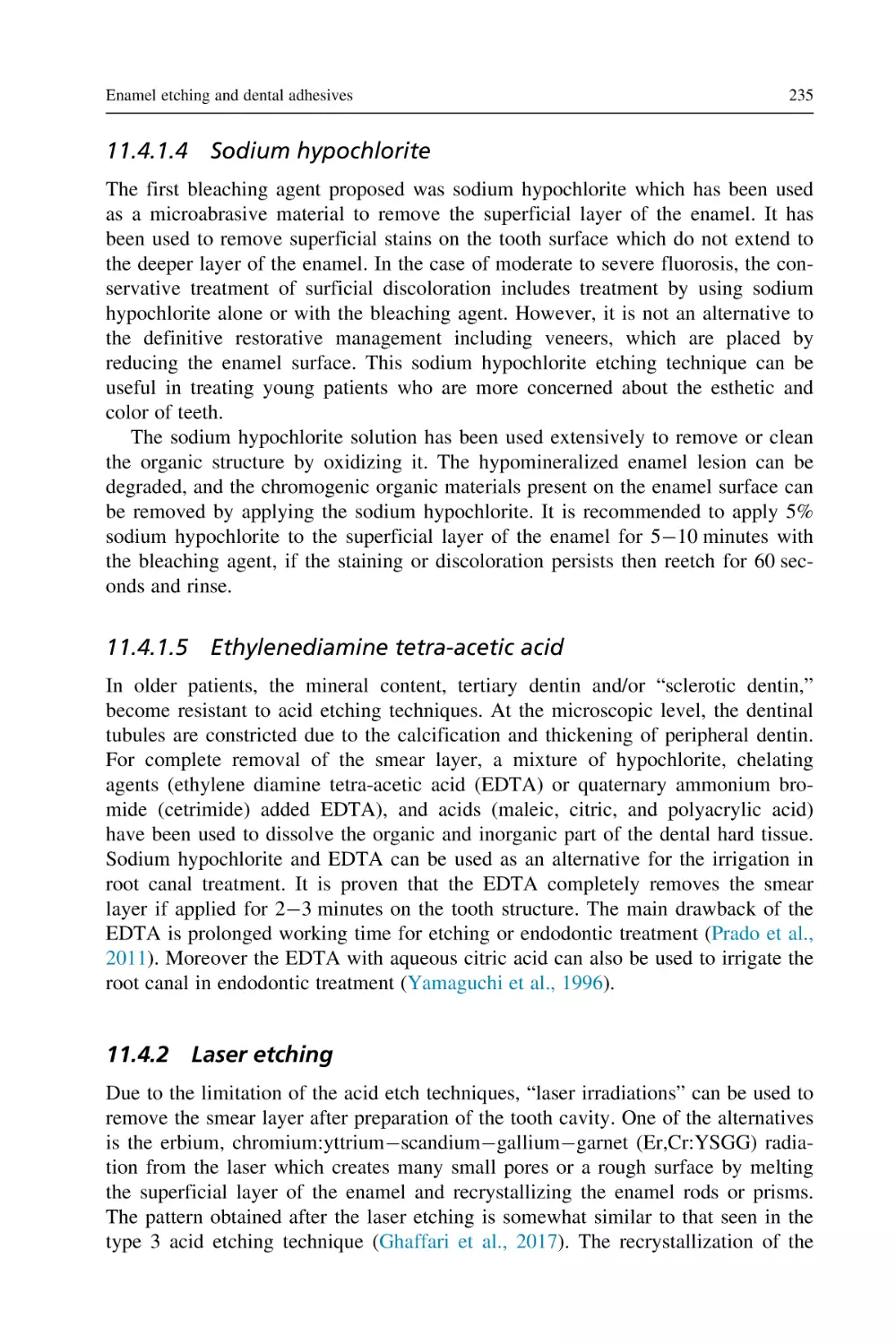
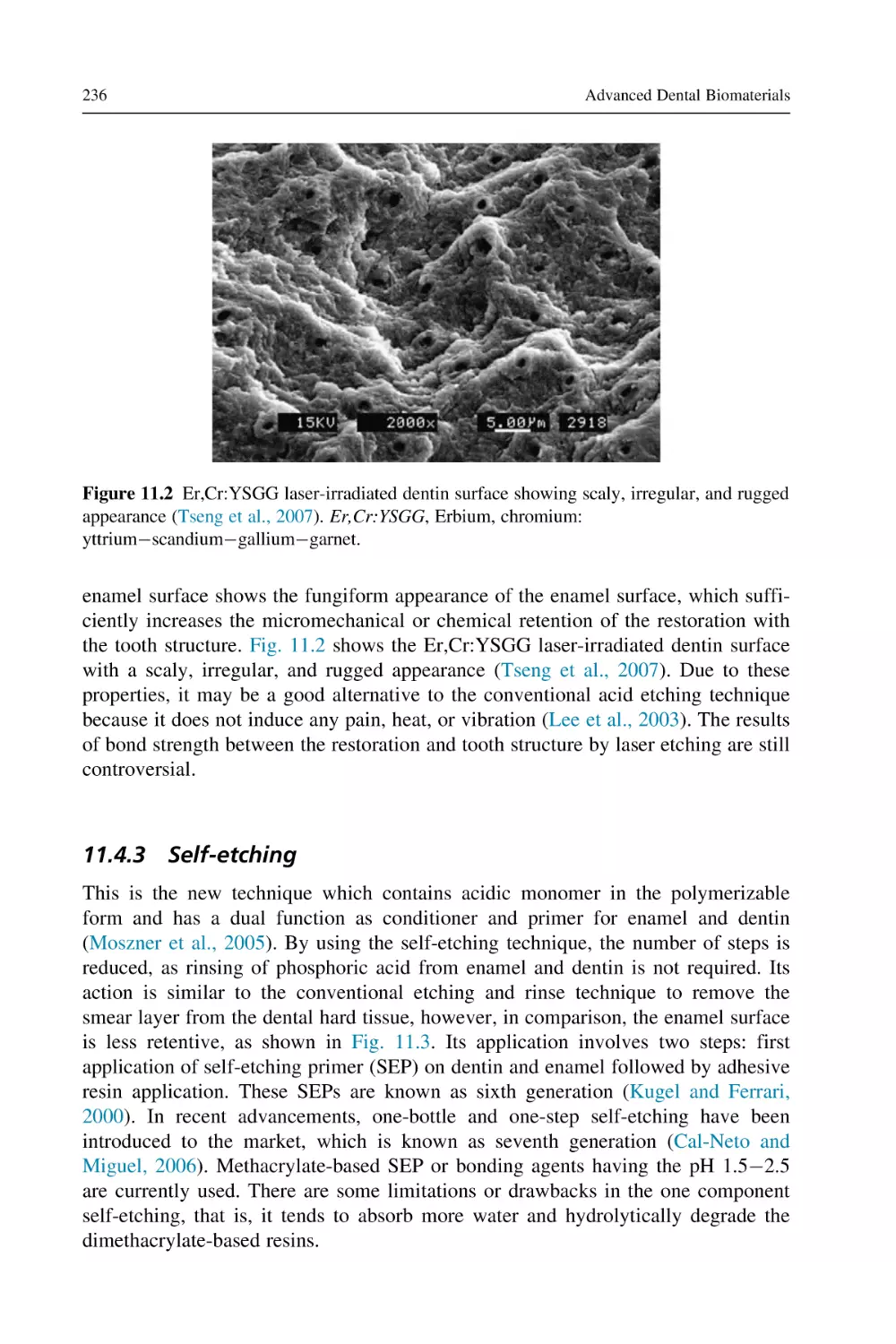
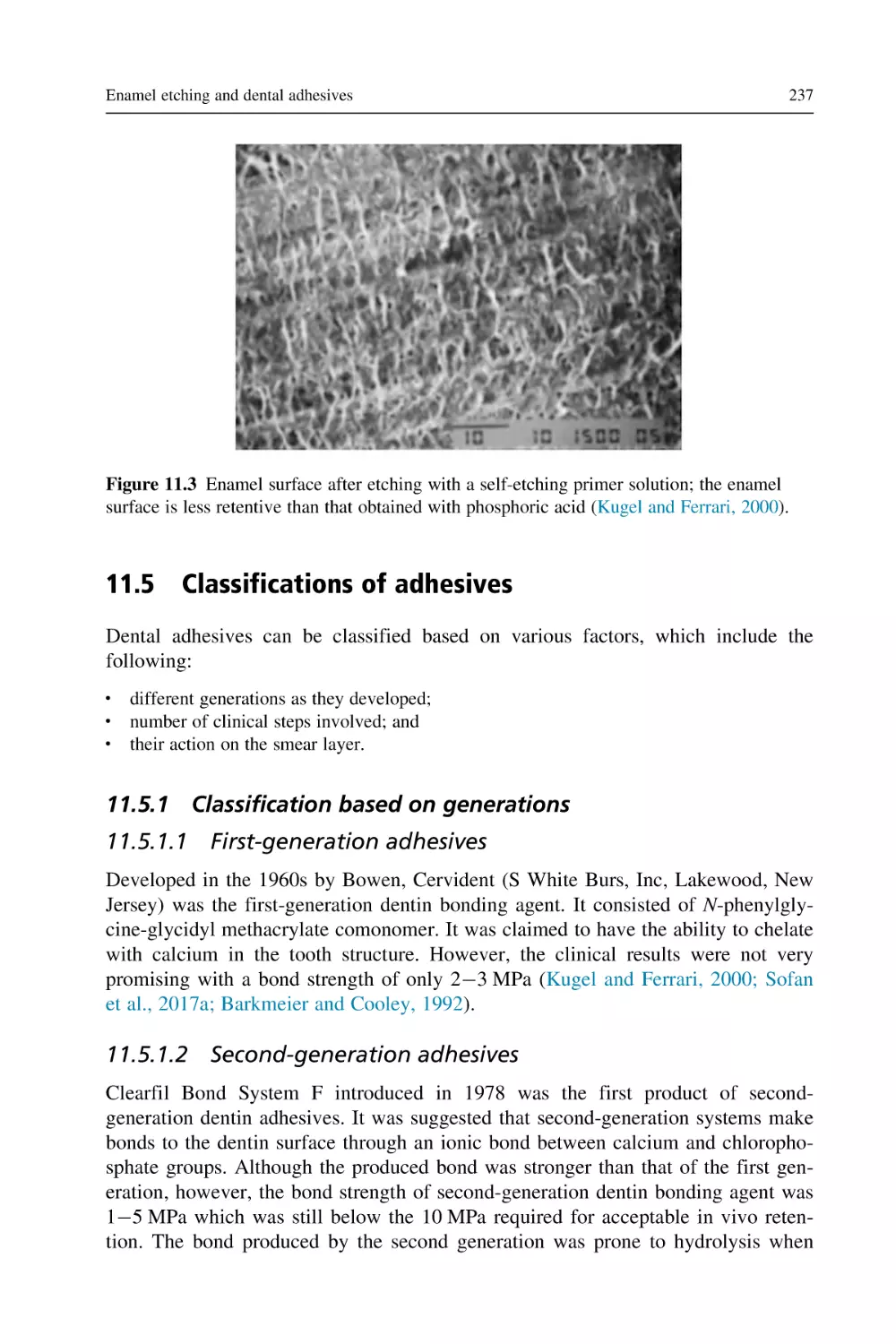
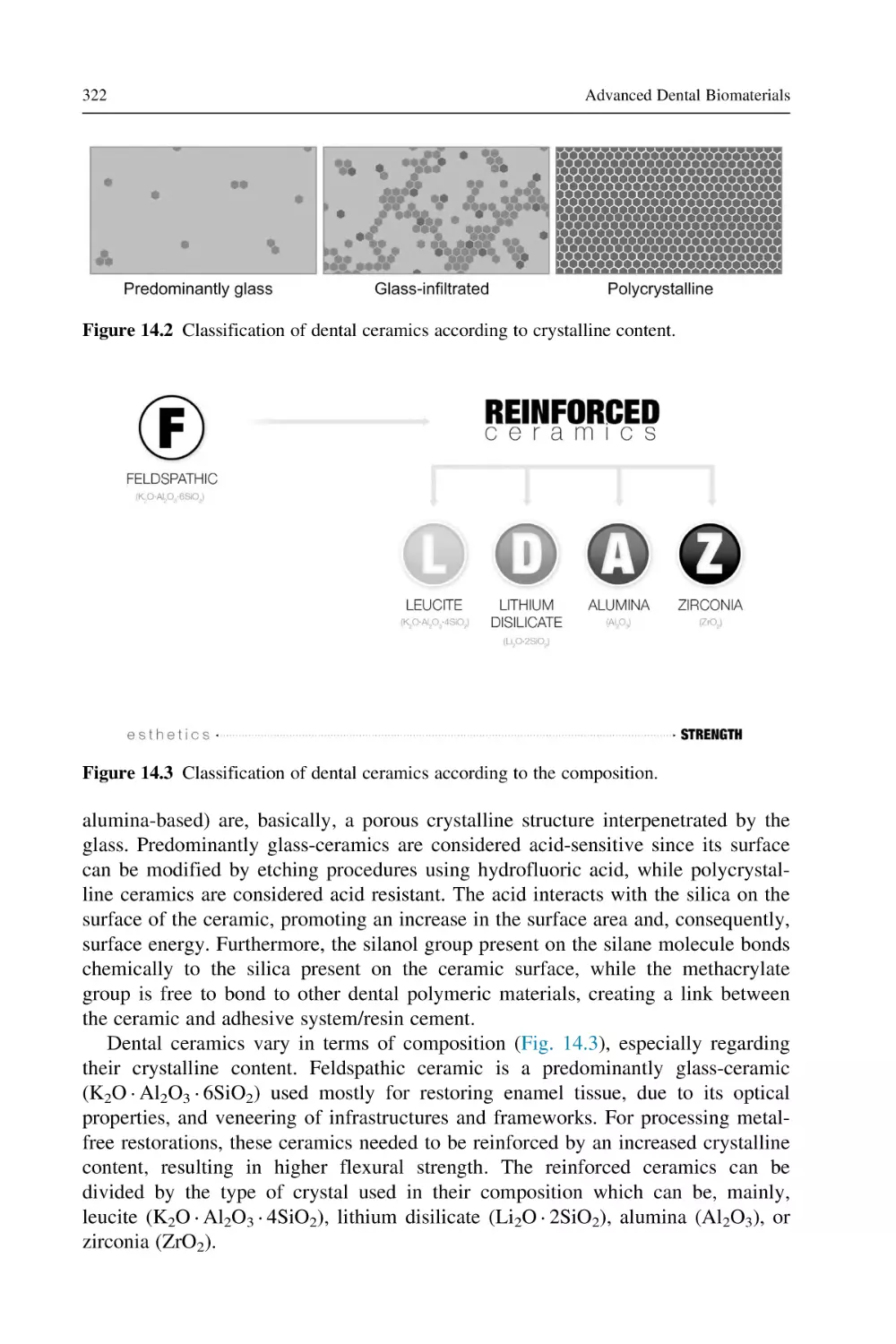
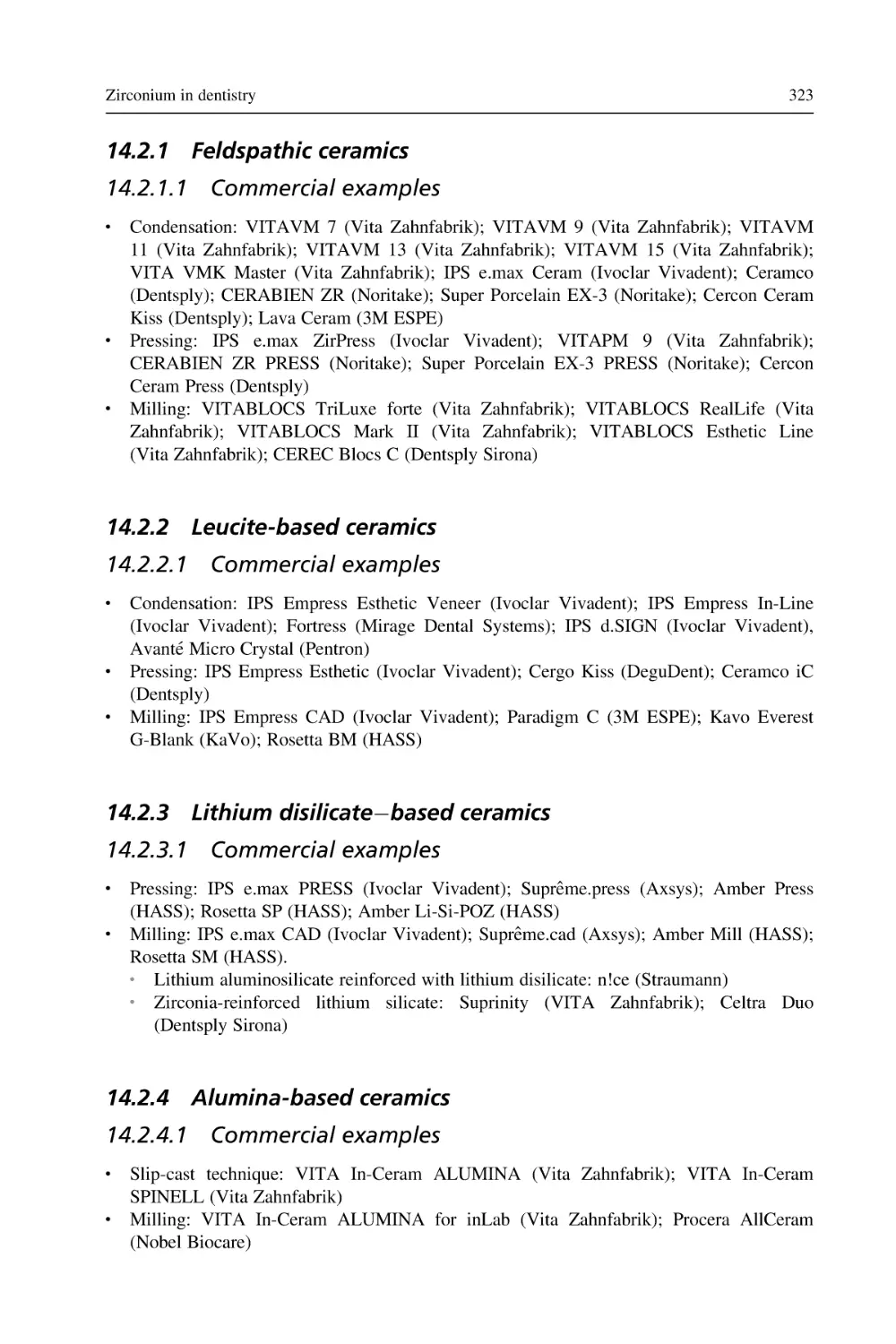
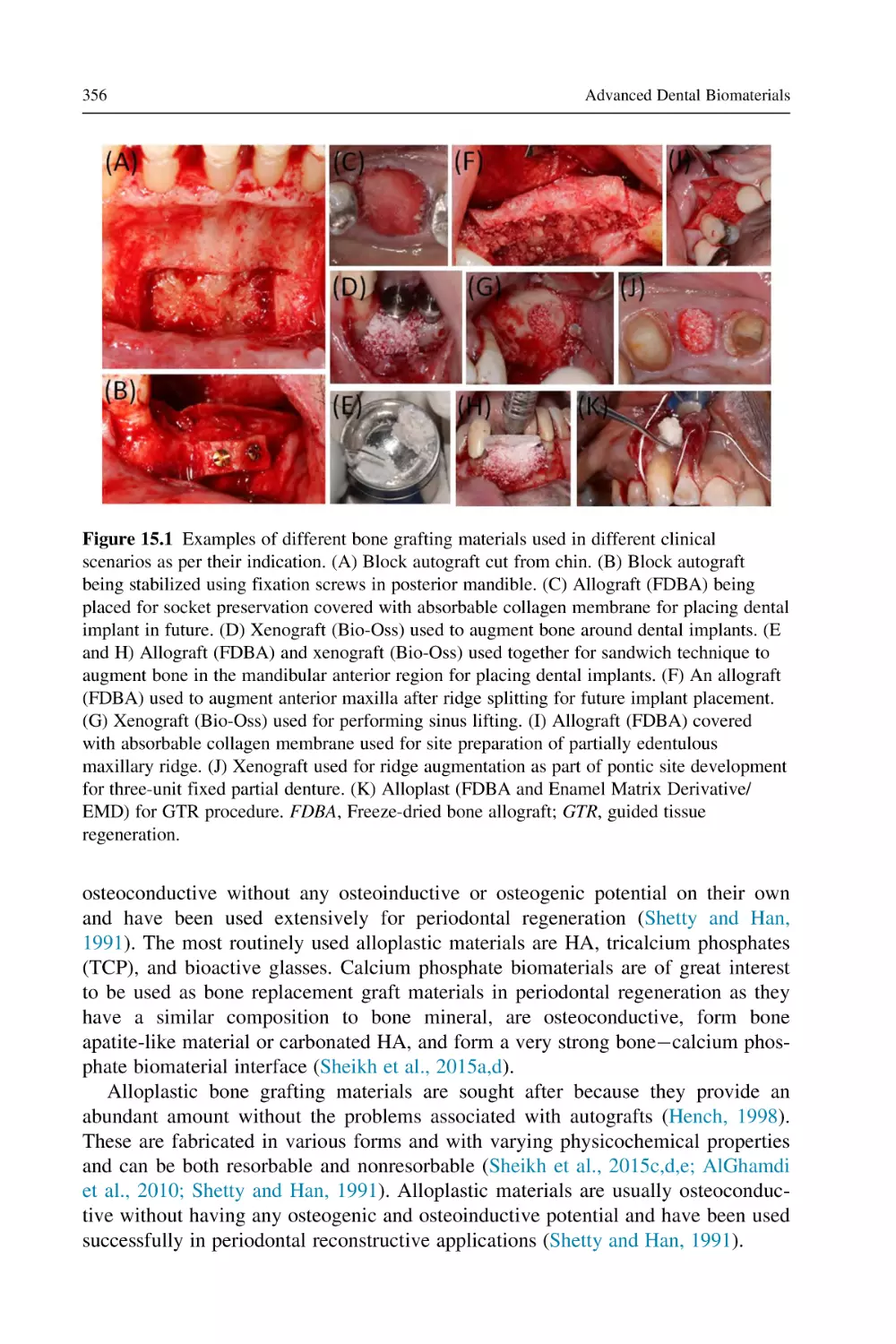
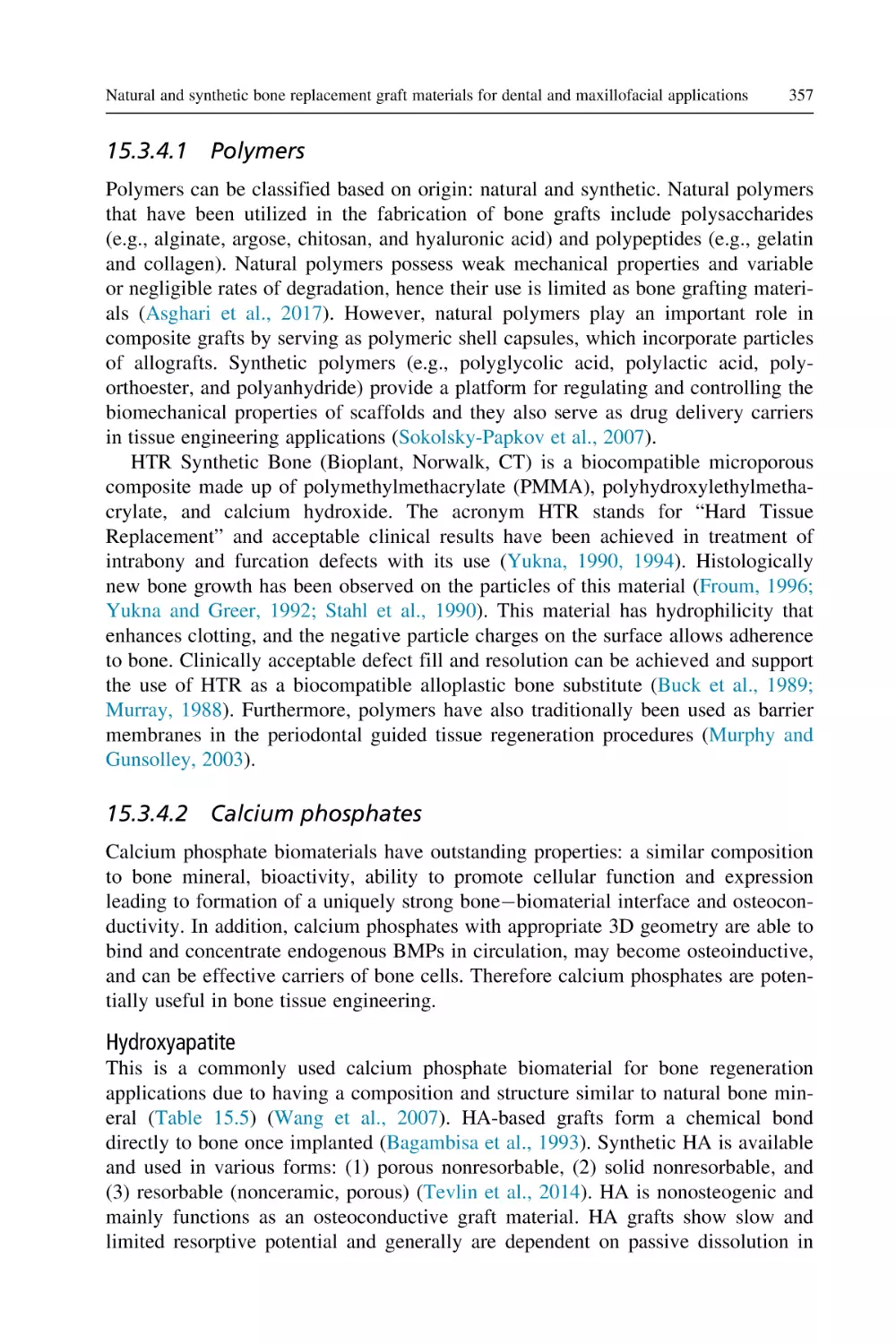
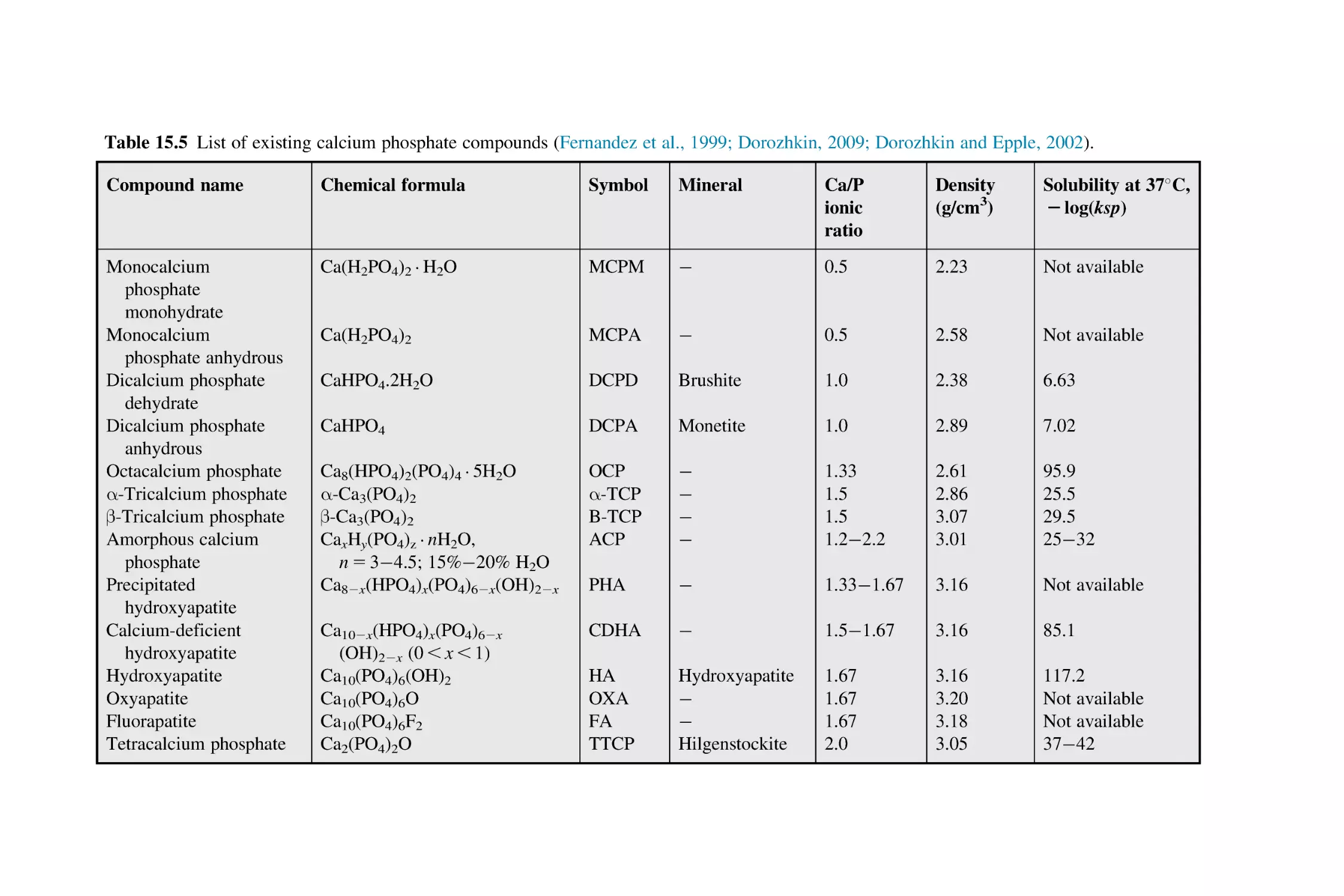
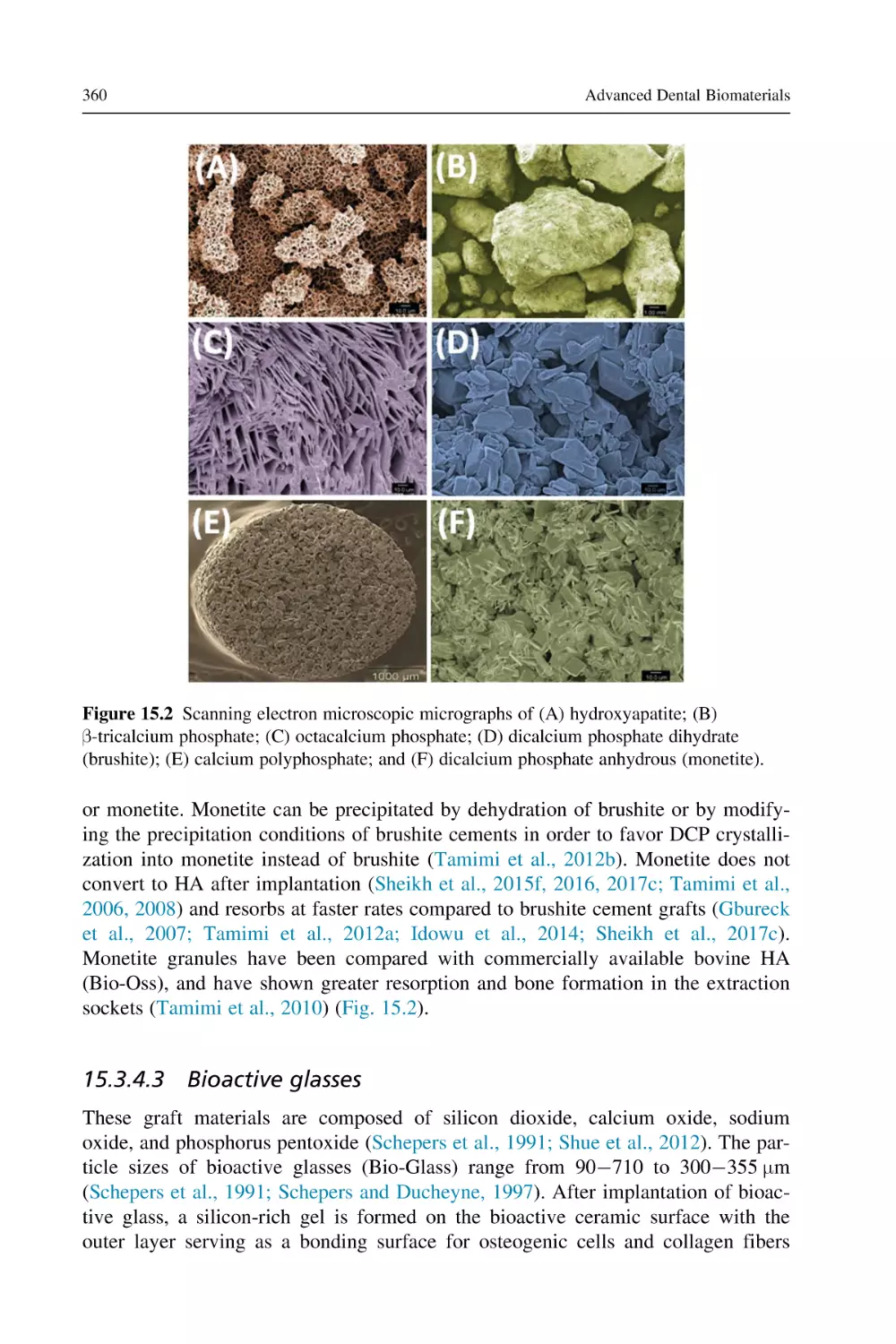
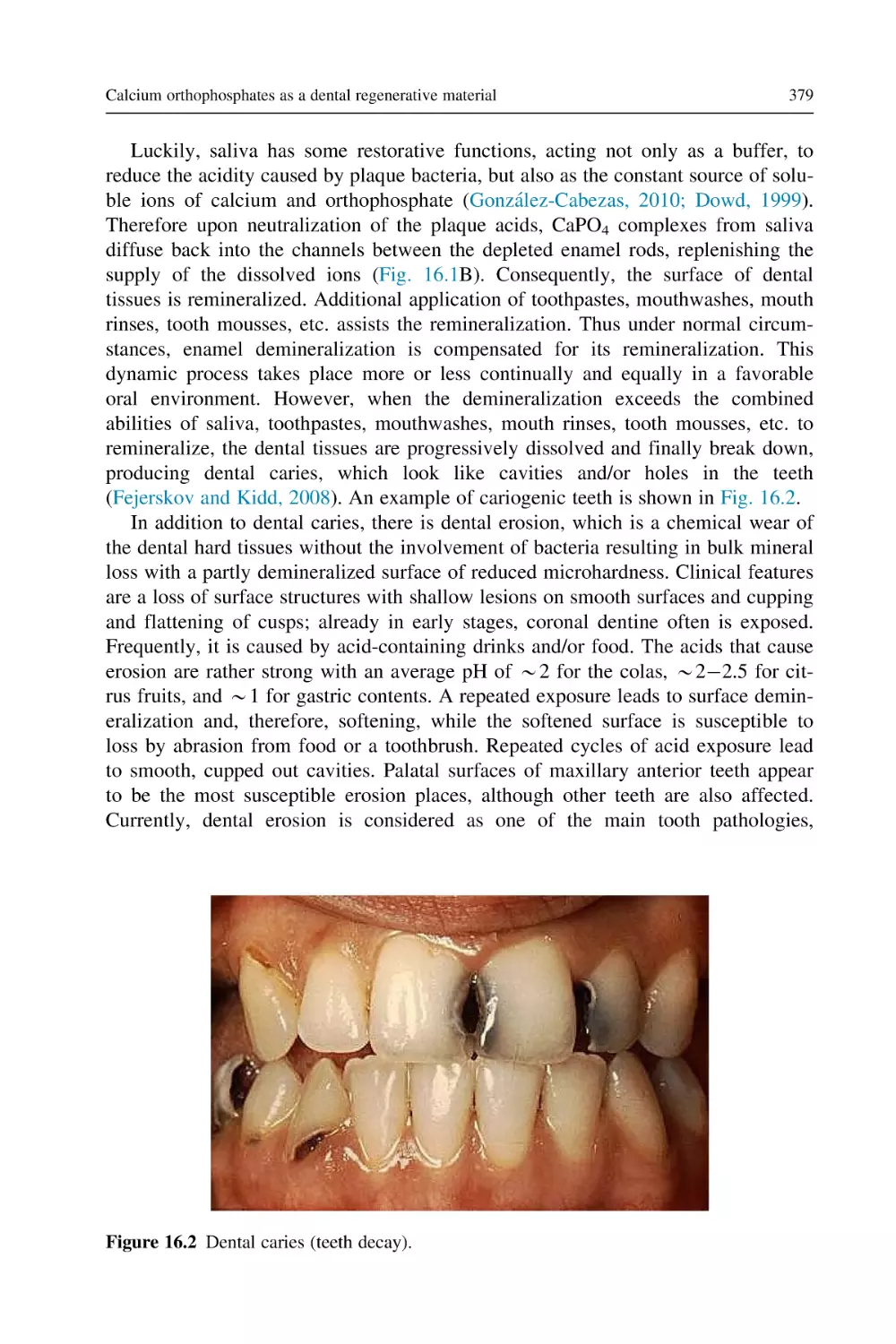
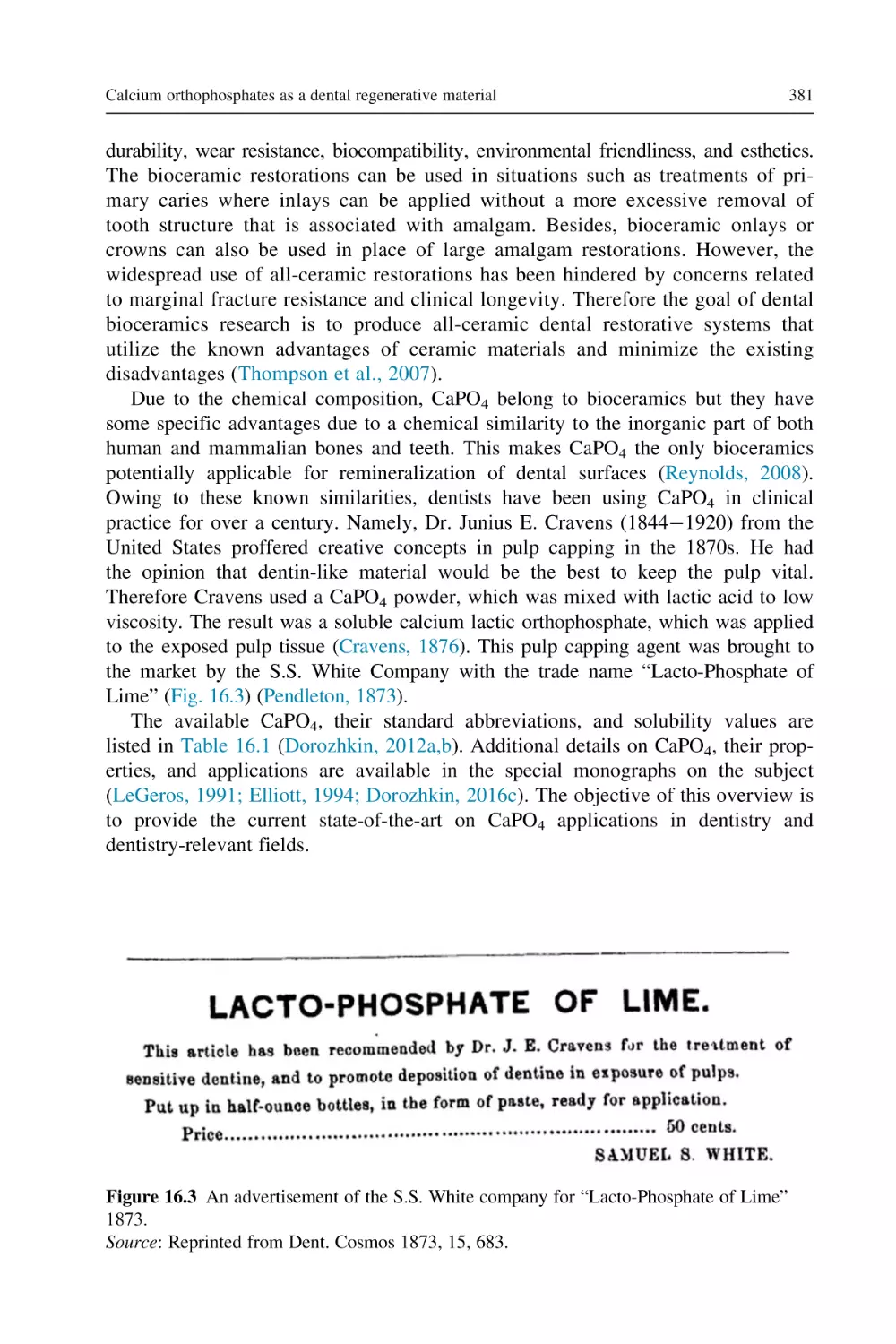
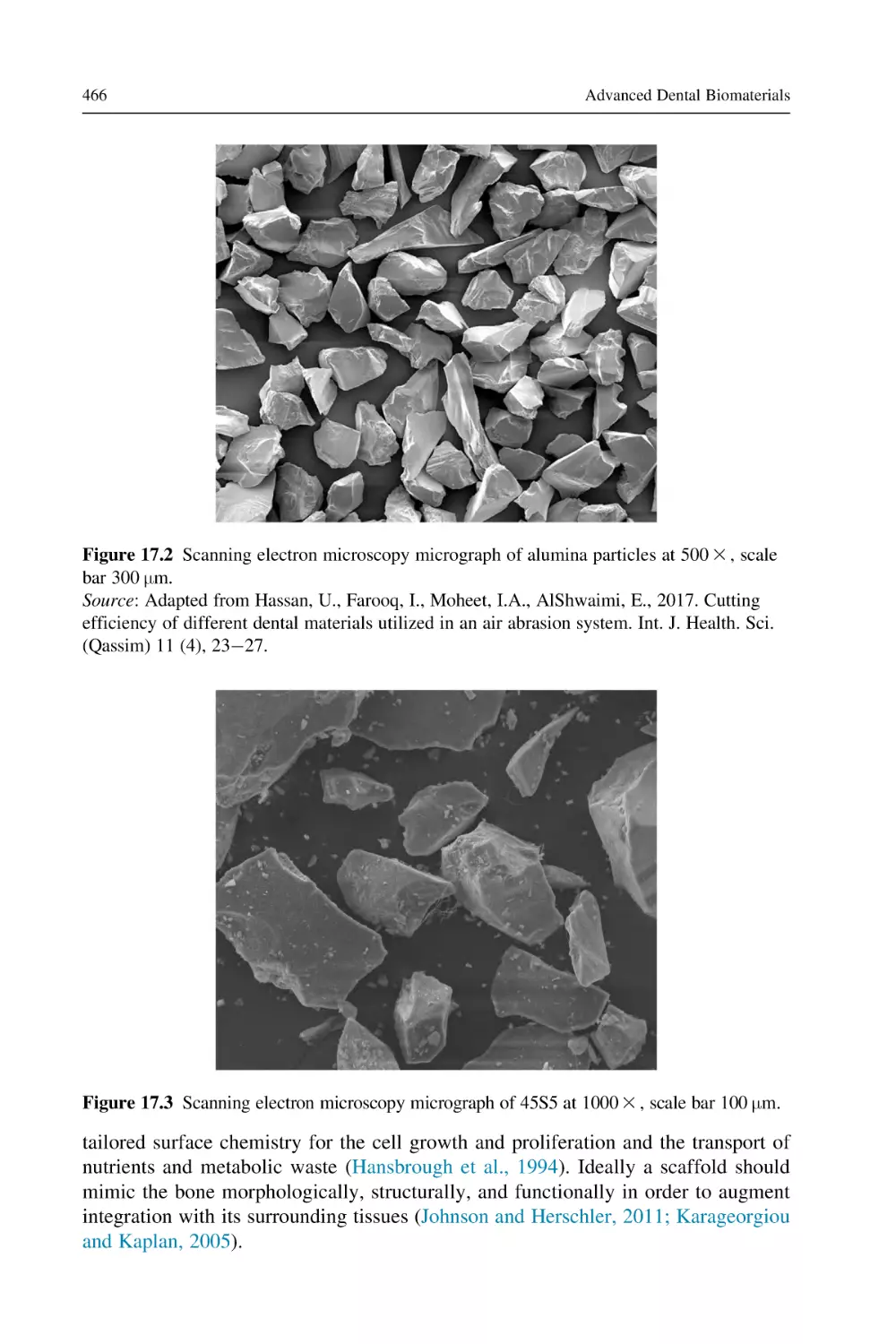
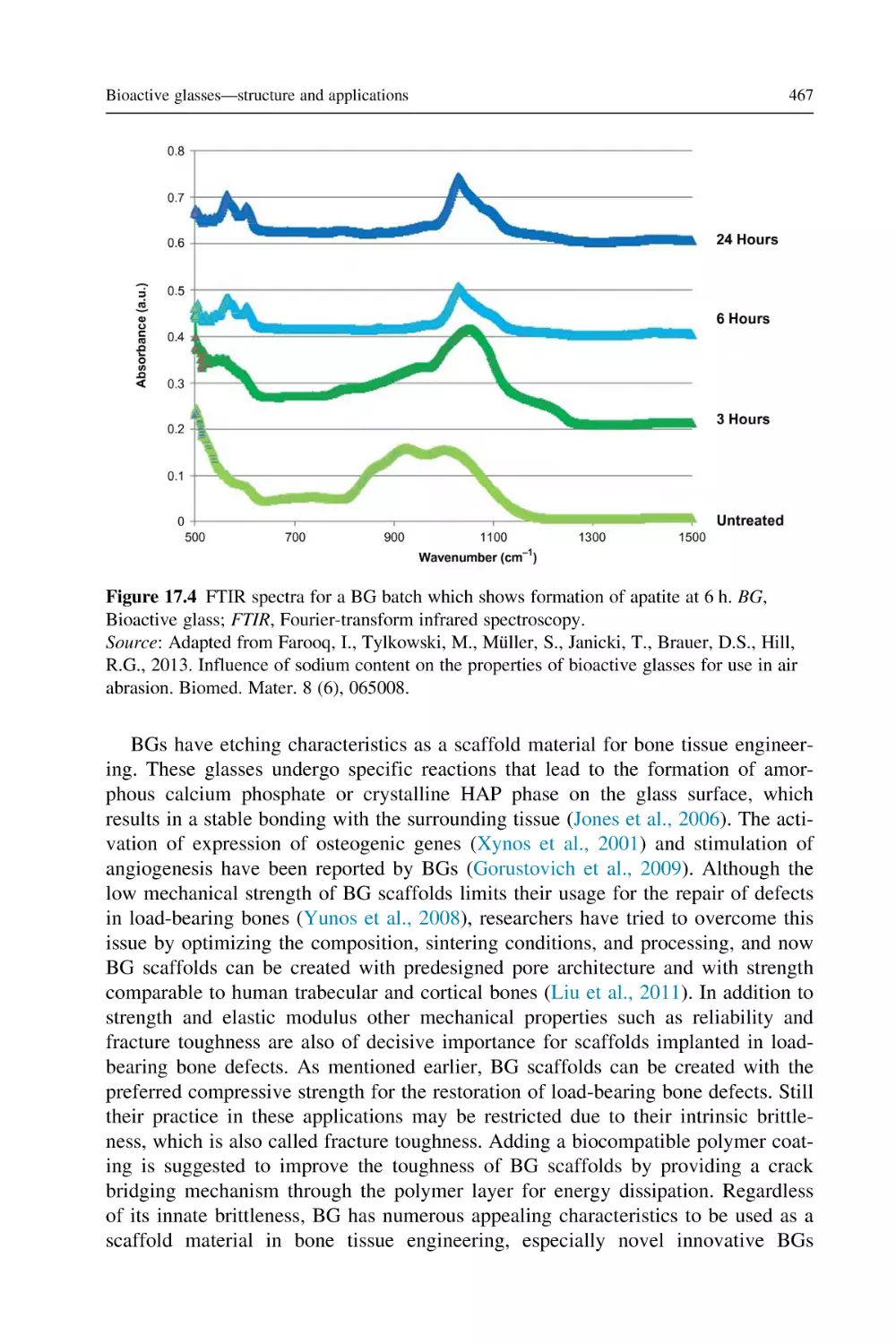
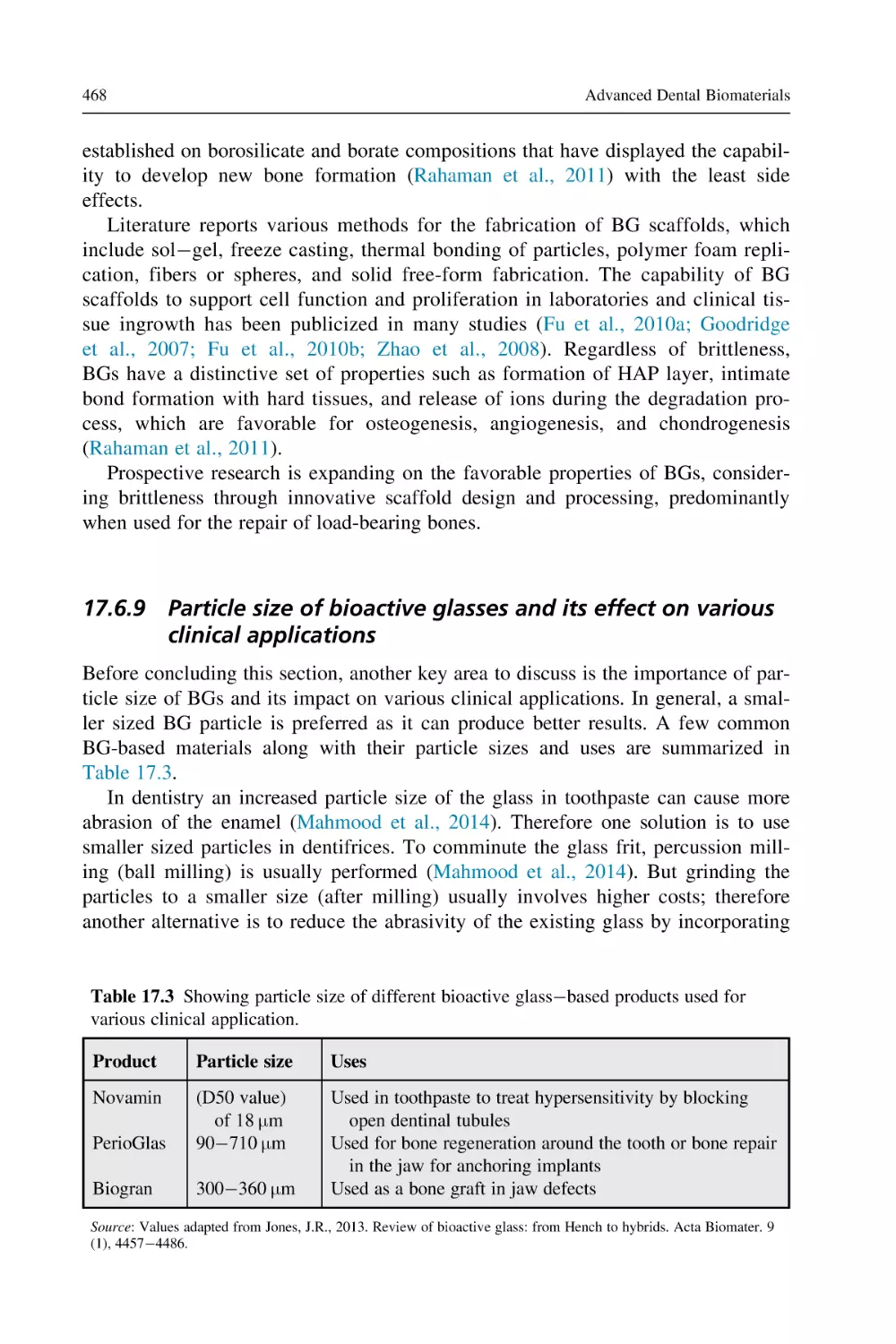
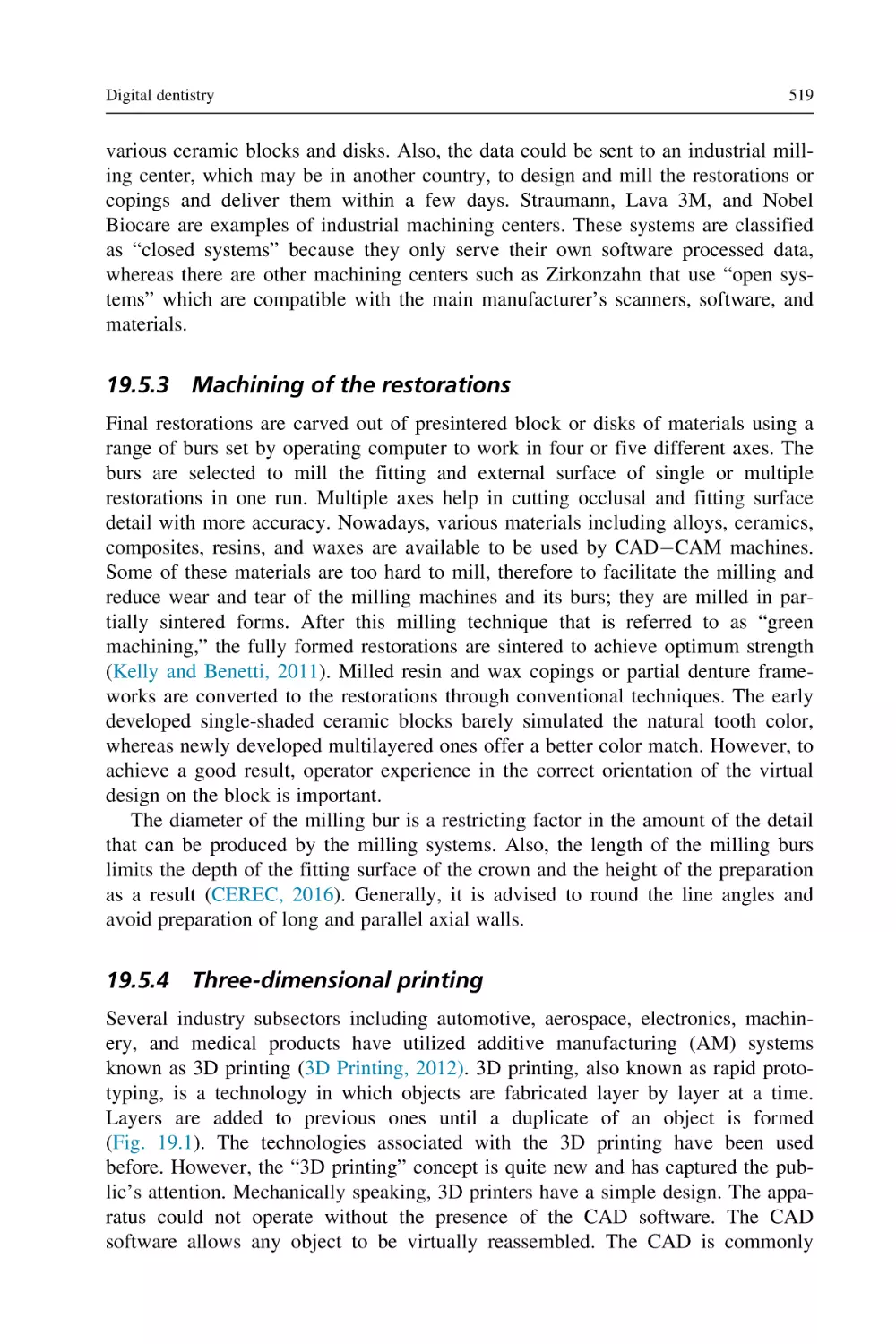
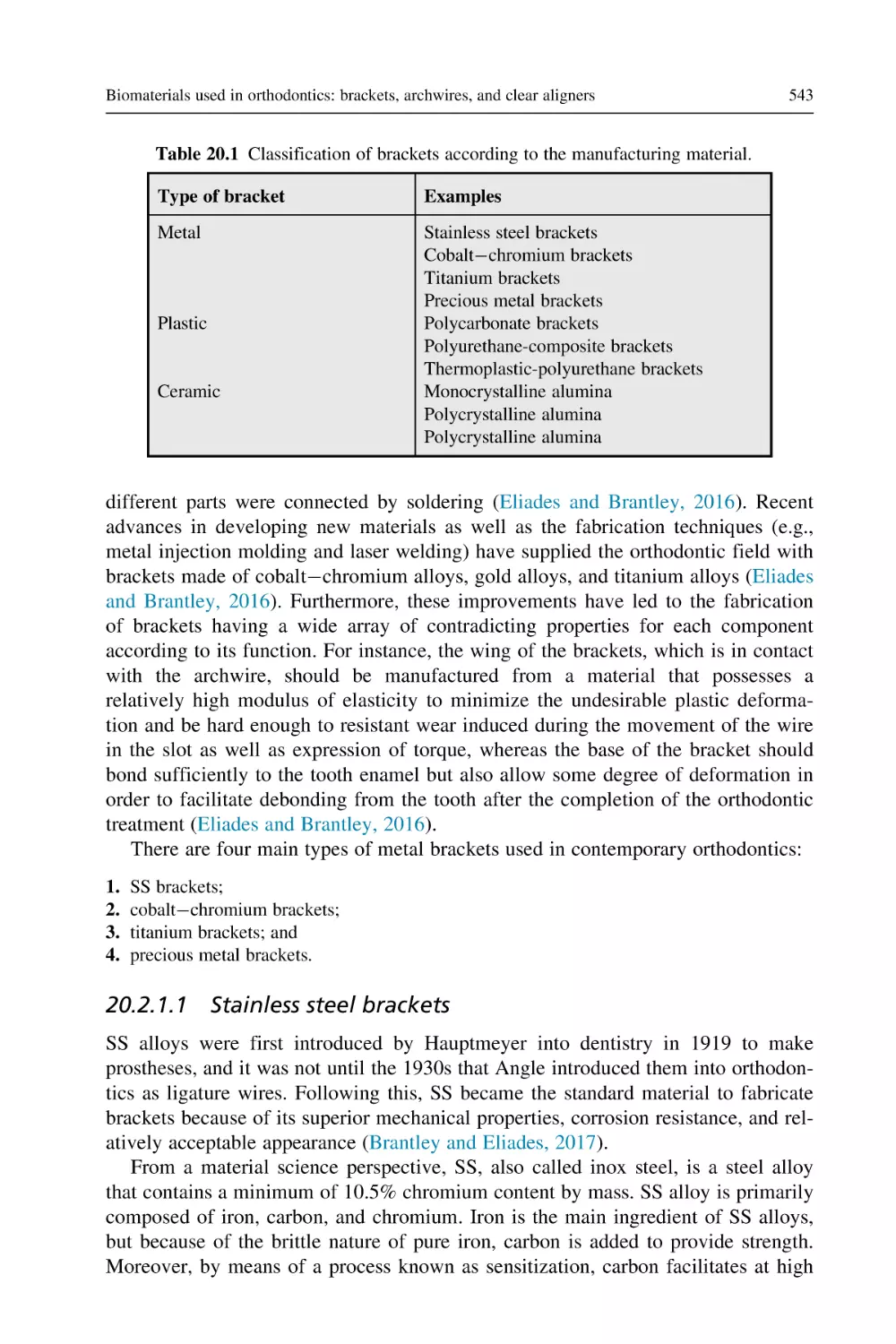
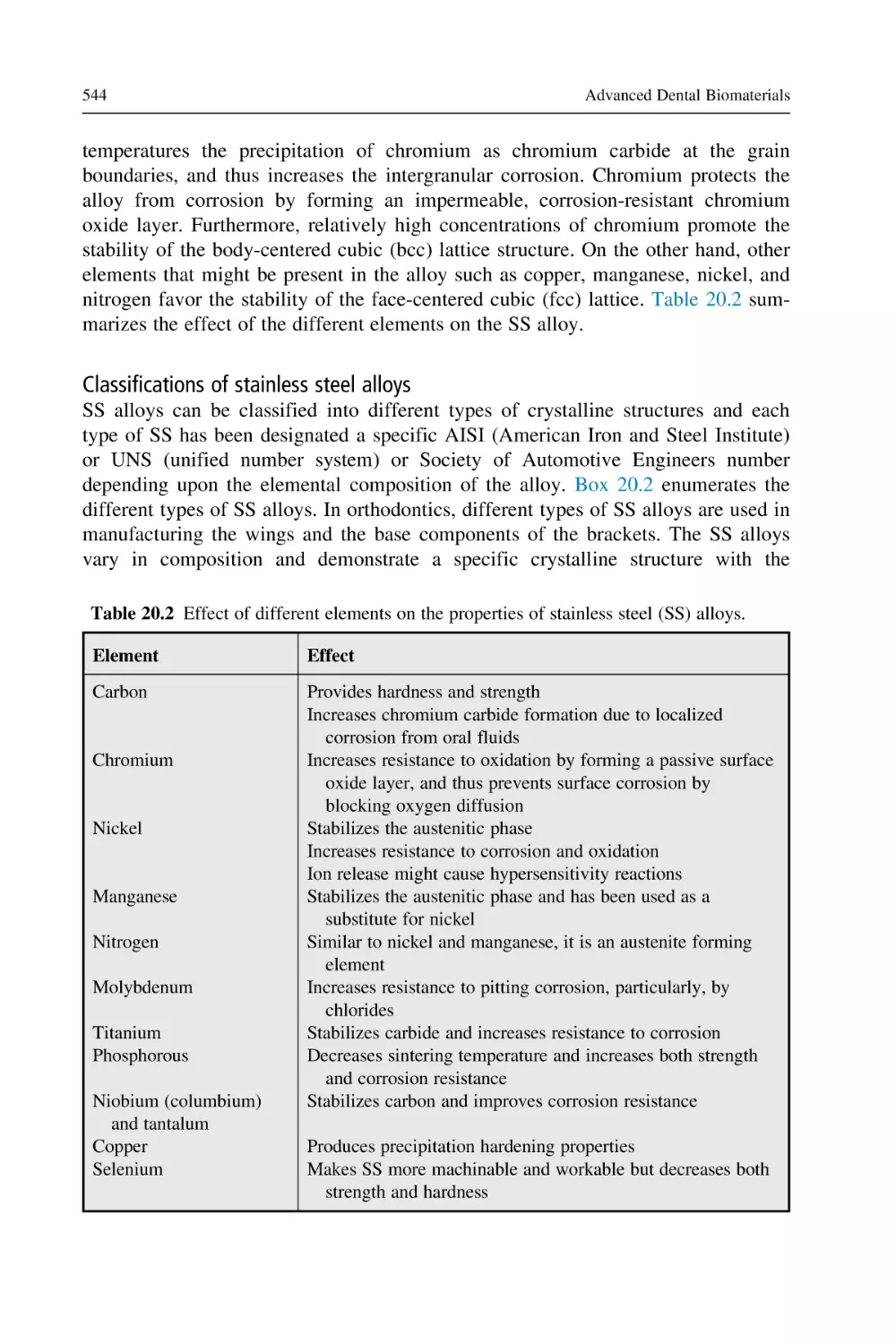
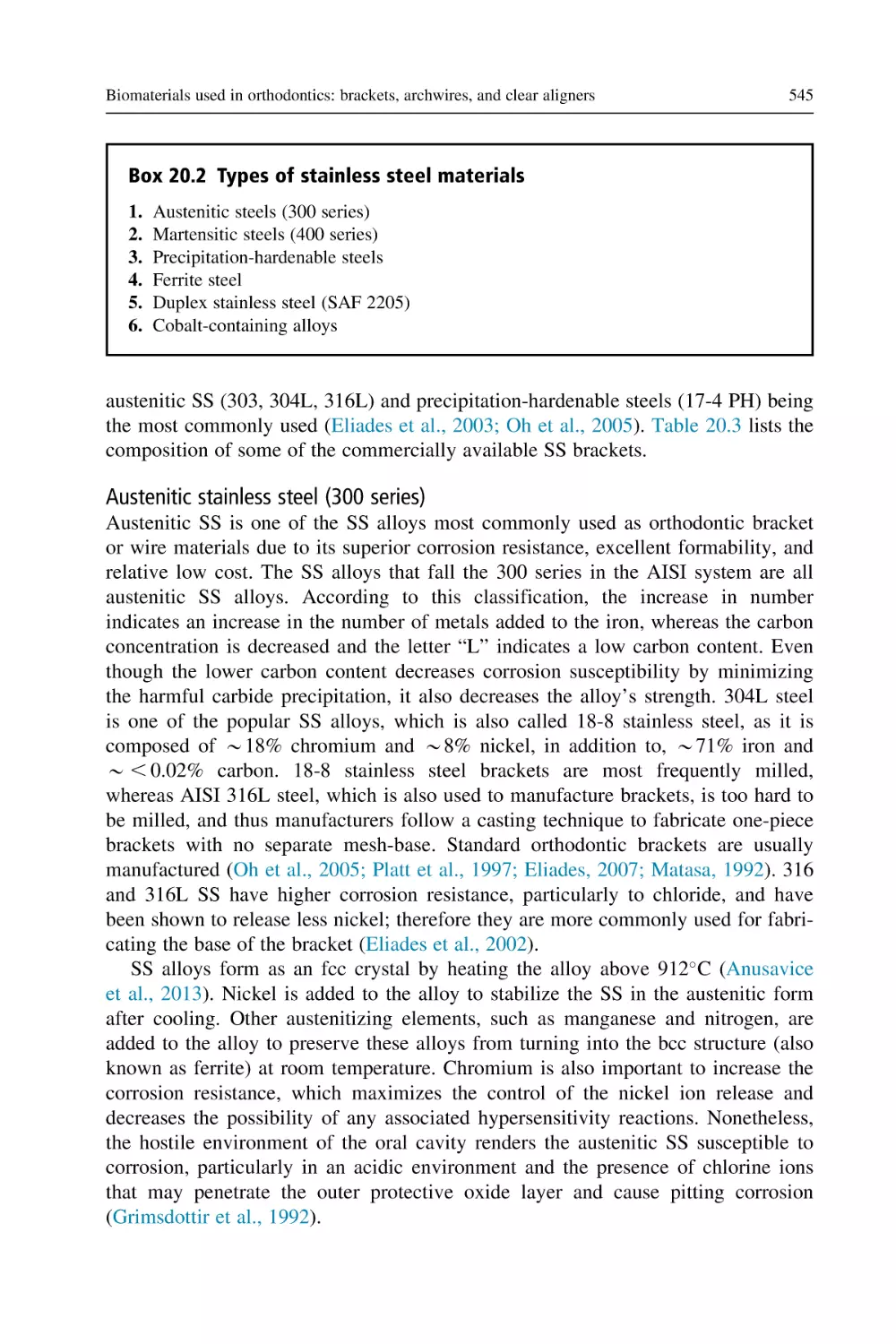
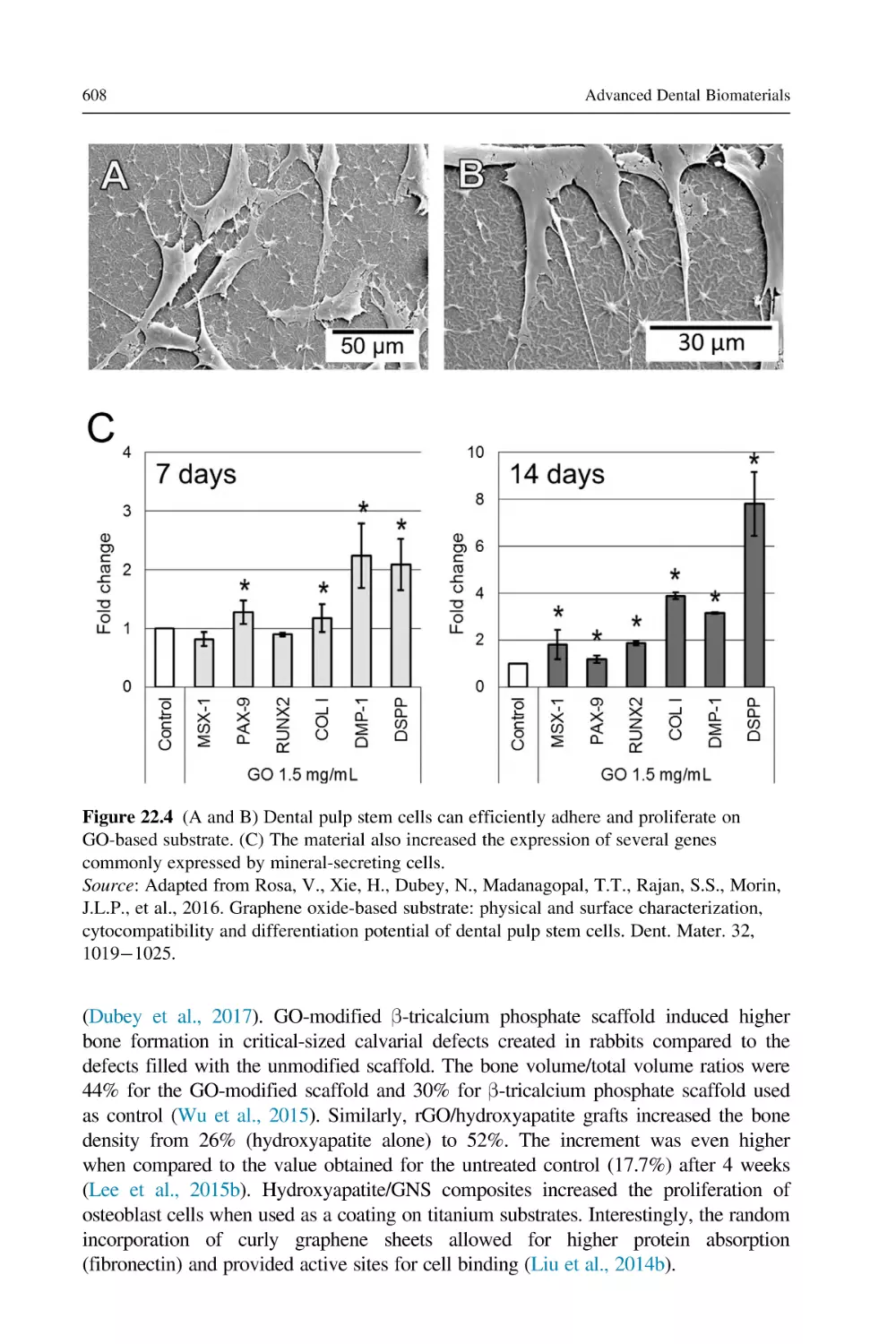
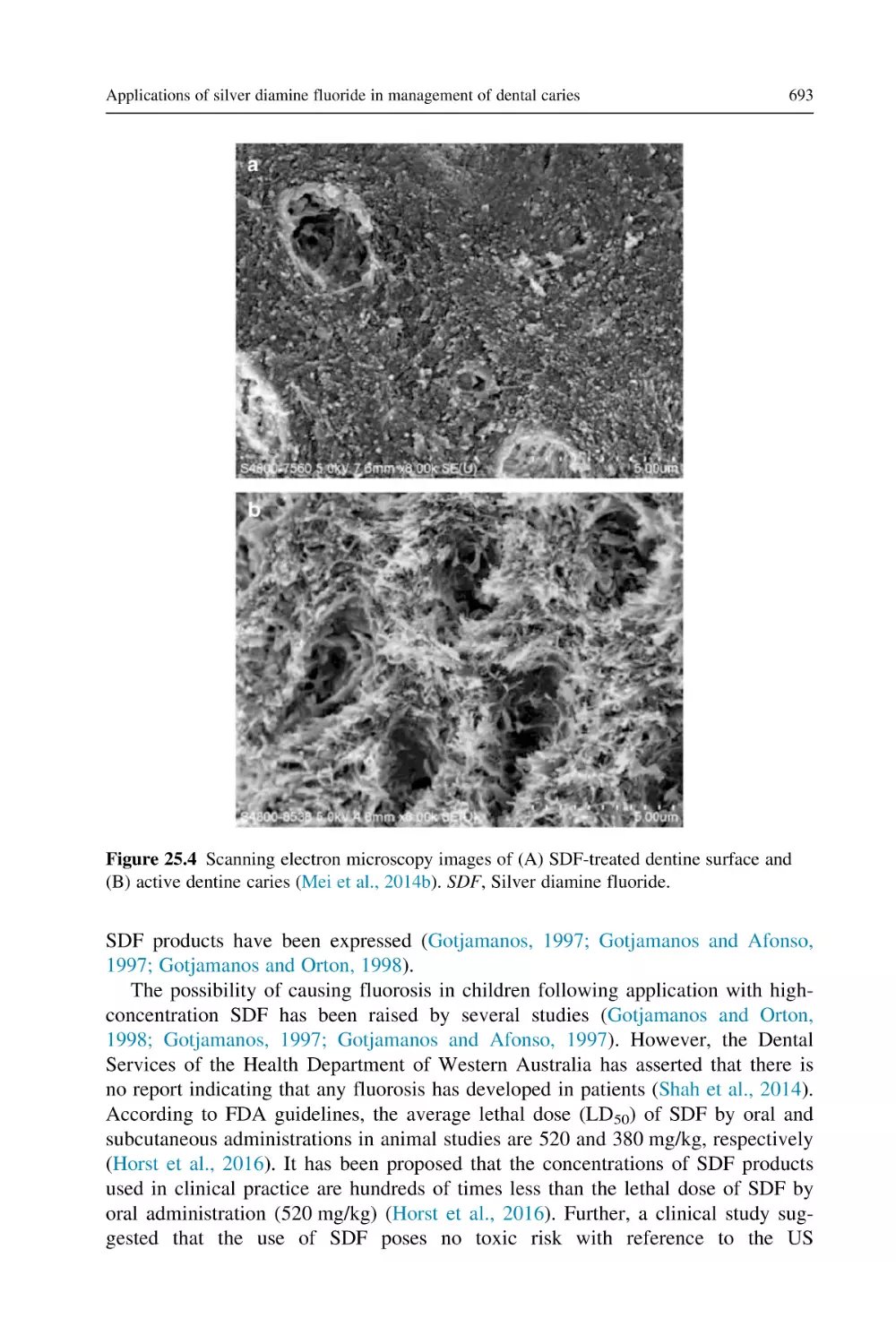
/













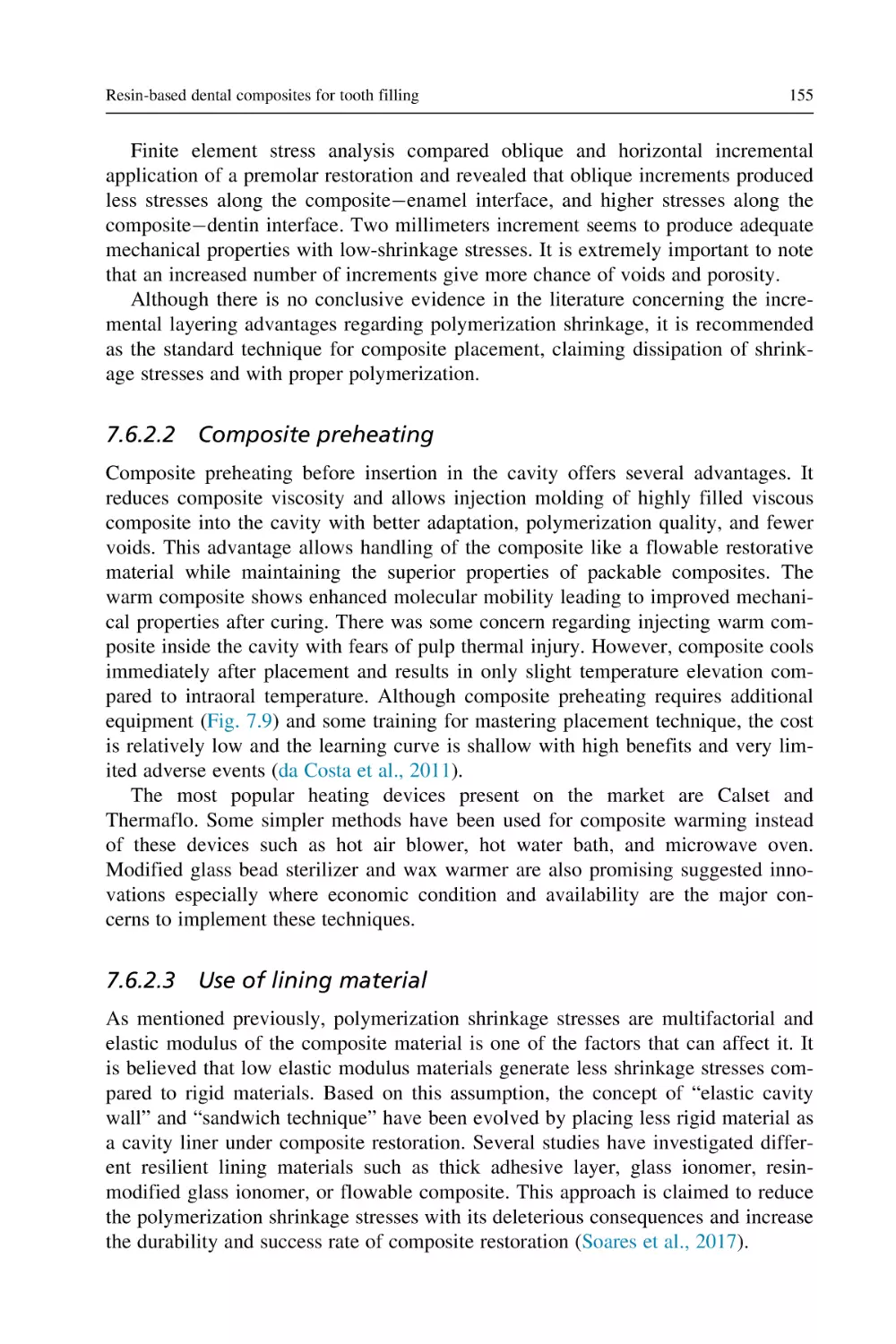













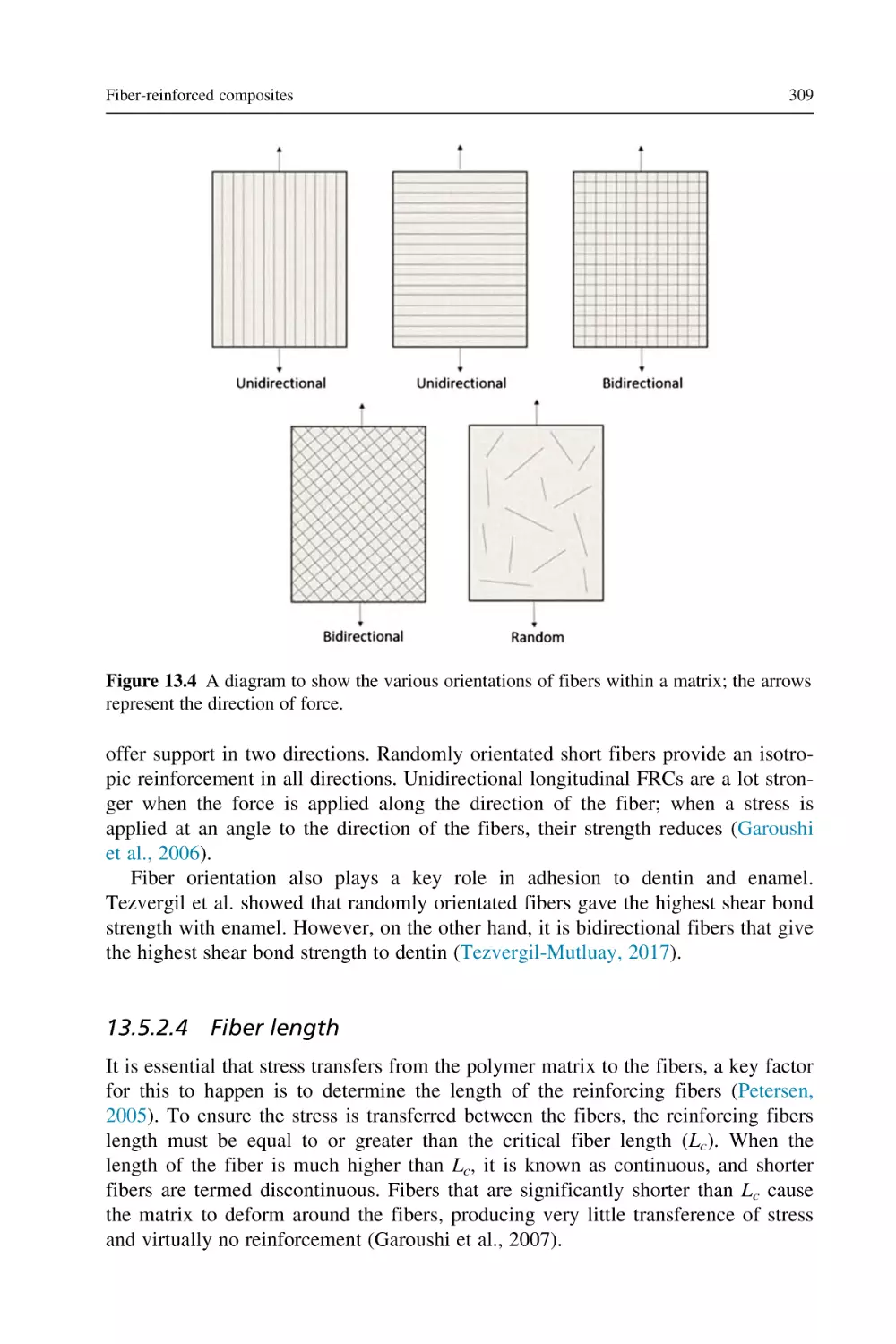



























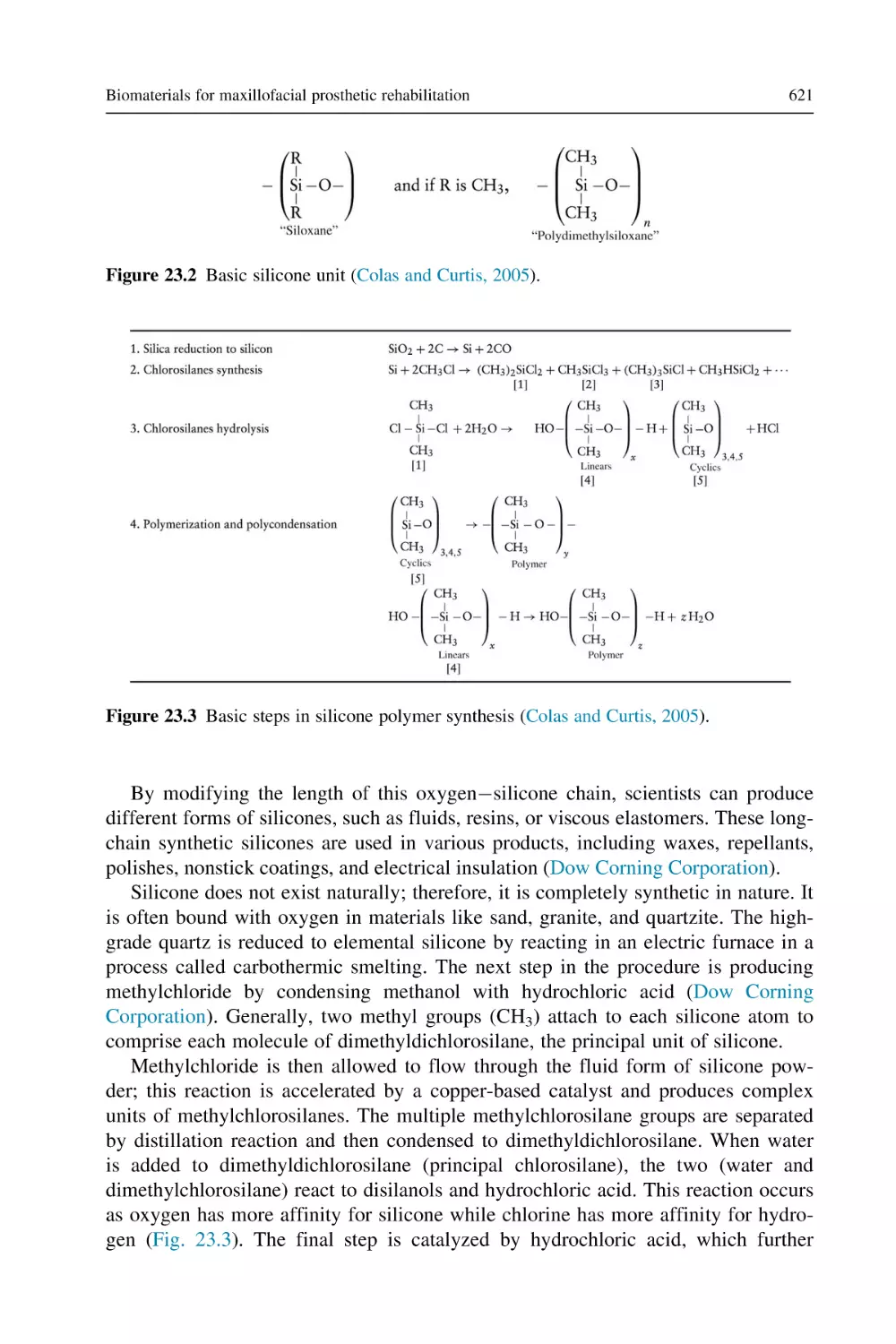
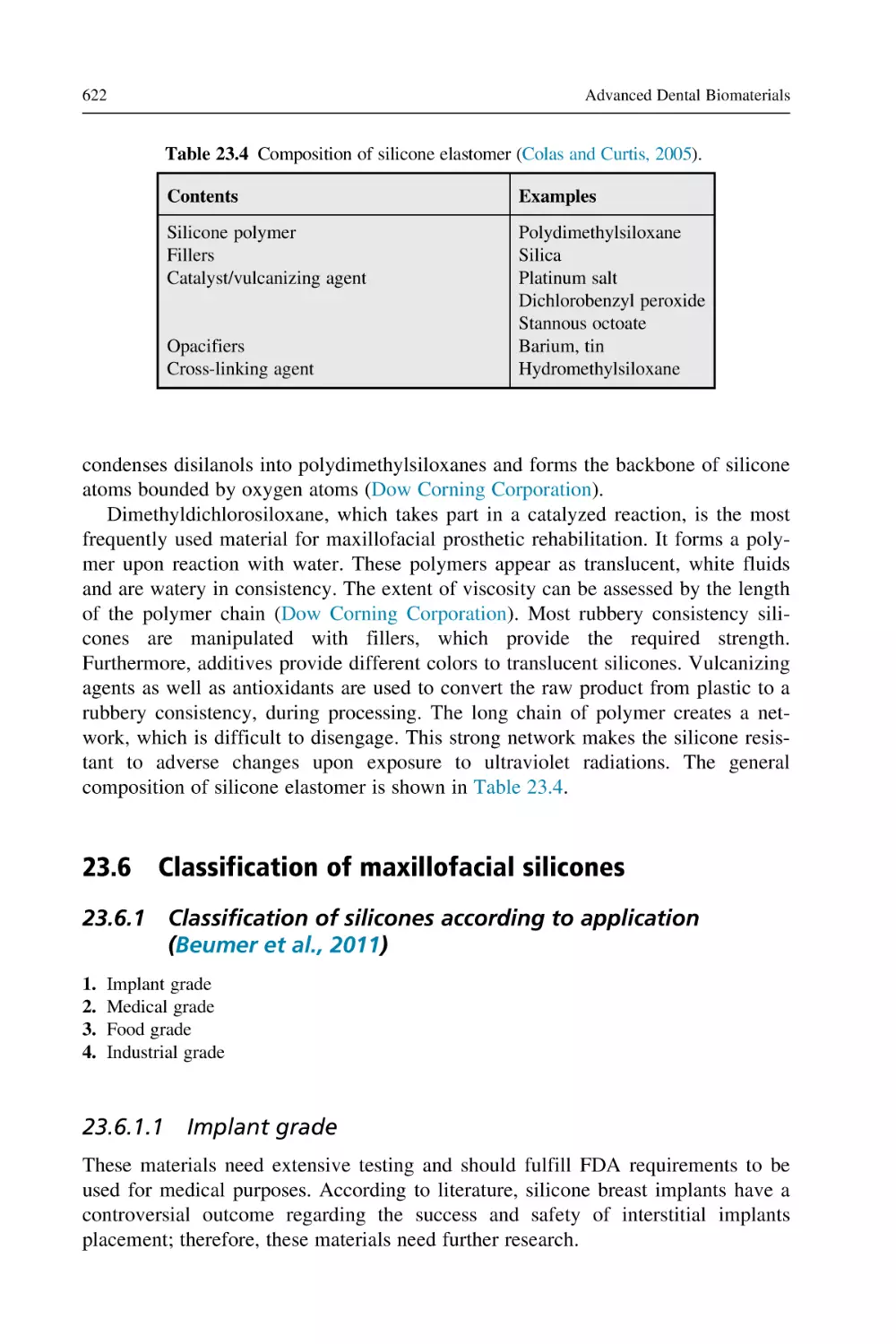









Текст
Advanced Dental Biomaterials
WOODHEAD PUBLISHING SERIES IN BIOMATERIALS
Advanced Dental
Biomaterials
Edited by
Zohaib Khurshid
Shariq Najeeb
Muhammad Sohail Zafar
Farshid Sefat
Woodhead Publishing is an imprint of Elsevier
The Officers’ Mess Business Centre, Royston Road, Duxford, CB22 4QH, United Kingdom
50 Hampshire Street, 5th Floor, Cambridge, MA 02139, United States
The Boulevard, Langford Lane, Kidlington, OX5 1GB, United Kingdom
Copyright © 2019 Elsevier Ltd. All rights reserved.
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or
mechanical, including photocopying, recording, or any information storage and retrieval system, without
permission in writing from the publisher. Details on how to seek permission, further information about the
Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance
Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher
(other than as may be noted herein).
Notices
Knowledge and best practice in this field are constantly changing. As new research and experience broaden our
understanding, changes in research methods, professional practices, or medical treatment may become
necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using
any information, methods, compounds, or experiments described herein. In using such information or
methods they should be mindful of their own safety and the safety of others, including parties for whom they
have a professional responsibility.
To the fullest extent of the law, neither the Publisher nor the authors, contributors, or editors, assume any
liability for any injury and/or damage to persons or property as a matter of products liability, negligence or
otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the
material herein.
British Library Cataloguing-in-Publication Data
A catalogue record for this book is available from the British Library
Library of Congress Cataloging-in-Publication Data
A catalog record for this book is available from the Library of Congress
ISBN: 978-0-08-102476-8 (print)
ISBN: 978-0-08-102477-5 (online)
For information on all Woodhead Publishing publications
visit our website at https://www.elsevier.com/books-and-journals
Publisher: Matthew Deans
Acquisition Editor: Sabrina Webber
Editorial Project Manager: Joshua Mearns
Production Project Manager: Debasish Ghosh
Cover Designer: Greg Harris.
Typeset by MPS Limited, Chennai, India
List of contributors
Mohamed-Nur Abdallah Faculty
Toronto, ON, Canada
of
Dentistry,
University
of
Toronto,
Azeem Ajaz Department of Prosthodontics and Dental Implantology, College of
Dentistry, King Faisal University, Al-Ahsa, Kingdom of Saudi Arabia
Mai Saleh Ali Faculty of Dentistry, University of Toronto, Toronto, ON,
Canada; Private Practice, Amman, Jordan
Saqib Ali Department of Biomedical Dental Sciences, College of Dentistry, Imam
Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Sanam Almassi Almassi Specialist Clinic, Tehran, Iran
Ahmad A. Alnazzawi Department of Substitutive Dental Sciences, College of
Dentistry, Taibah University, Medina, Saudi Arabia
Mothanna Alrahabi Department of Restorative Dentistry, College of Dentistry,
Taibah University, Medina, Saudi Arabia
Abdullah Alwadaani Department of Prosthodontics and Dental Implantology,
College of Dentistry, King Faisal University, Al-Ahsa, Saudi Arabia
Marina Amaral Department of Dentistry, University of Taubaté, Taubaté, Brazil
Faiza Amin Department of Science of Dental Materials, Dow Dental College,
Dow University of Health Sciences, Karachi, Pakistan
Paul Anderson Centre for Oral Bioengineering, Institute of Dentistry, Queen Mary
University of London, London, United Kingdom
Sukumaran Anil Department of Dentistry, Hamad Medical Corporation, Doha,
Qatar
Anderson Catelan Faculty of Health Sciences, University of Western São Paulo,
Presidente Prudente, Brazil
xxii
List of contributors
Elna Paul Chalisserry Interdisciplinary Program of Marine-Biomedical, Electrical
and Mechanical Engineering, Center for Marine-Integrated Biomedical Technology
(BK21 Plus), Pukyong National University, Busan, South Korea
Amritpaul Singh Dhillon Dental Institute, King’s College London, London,
United Kingdom
Sergey V. Dorozhkin Moscow, Russia
Tomas Duminis Centre for Oral Bioengineering, Institute of Dentistry, Barts and
the London School of Medicine and Dentistry, London, United Kingdom
Daghigh Ahmadi Ehsaneh Centre for Nanohealth, College of Engineering,
Swansea University, Swansea, United Kingdom
Ahmed El-Banna Dental Biomaterials Department, Faculty of Dentistry, AinShams University, Cairo, Egypt
Muhammad A. Fareed Adult Restorative Dentistry, Dental Biomaterials and
Prosthodontics Oman Dental College, Muscat, Sultanate of Oman
Azita Farhadi Shamsabadi Centre for English Language Education, Nottingham
University, Nottingham, United Kingdom
Imran Farooq Department of Biomedical Dental Sciences, College of Dentistry,
Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Amr S. Fawzy UWA Dental School, University of Western Australia, Nedlands,
WA, Australia
Pegah Firouzmanesh Babol University of Medical Sciences, Babol, Iran
Hani Ghabbani Department of Restorative Dentistry, College of Dentistry, Taibah
University, Medina, Saudi Arabia
Shadi Ghalami Department of Anatomy and Pathology, University of Siena,
Siena, Italy
Michael Glogauer Faculty of Dentistry, University of Toronto, Toronto, ON,
Canada; Institute of Biomaterials and Biomedical Engineering, University of
Toronto, Toronto, ON, Canada
List of contributors
xxiii
Marc Grynpas Lunenfeld-Tanenbaum Research Institute, Mount Sinai Hospital,
Toronto, ON, Canada; Department of Laboratory Medicine and Pathobiology,
University of Toronto, Toronto, ON, Canada; Princess Margaret Cancer Centre,
Department of Dental Oncology and Maxillofacial Prosthetics, Toronto, ON, Canada
Nader Hamdan Department of Dental Clinical Sciences, Faculty of Dentistry,
Dalhousie University, Halifax, NS, Canada
Zoe Hancox Biomedical and Electrical Engineering Department, School of
Engineering, University of Bradford, Bradford, United Kingdom
Nasira Haque Department of Biomedical and Electronics Engineering, School of
Engineering, University of Bradford, Bradford, United Kingdom
Robert G. Hill Dental Physical Sciences, Institute of Dentistry, Barts and The
London School of Medicine and Dentistry, Queen Mary University of London,
London, United Kingdom
Wei-Te Huang Centre for Oral Bioengineering, Institute of Dentistry, Queen Mary
University of London, London, United Kingdom
Shehriar Husain Department of Dental Materials Science, Jinnah Sindh Medical
University, Karachi, Pakistan
Seyed Hassan Jafari School of Chemical Engineering, College of Engineering,
University of Tehran, Tehran, Iran
Bassel Kano Division of Endodontics, Faculty of Dentistry, McGill University,
Montreal, QC, Canada
Abdul Samad Khan Department of Restorative Dental Sciences, College of
Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Erum Khan Bhitai Dental and Medical College, Liaquat University of Medical
and Health Sciences, Jamshoro, Pakistan; Faculty of Dentistry, King Abdulaziz
University, Jeddah, Saudi Arabia
Zohaib Khurshid Department of Prosthodontics and Dental Implantology, College
of Dentistry, King Faisal University, Al-Ahsa, Saudi Arabia
Tiantong Lou Faculty of Dentistry, University of Toronto, Toronto, ON,
United States
Maria Mali Department of Orthodontics, Islamic International Dental College &
Hospital, Riphah International University, Islamabad, Pakistan
xxiv
List of contributors
Jukka P. Matinlinna Dental Materials Science, Applied Oral Sciences, Faculty of
Dentistry, The University of Hong Kong, Prince Philip Dental Hospital, Sai Ying
Pun, Hong Kong SAR, P.R. China
Kyung-san Min School of Dentistry, Chonbuk National University, Jeonju, South
Korea
Masoud Mozafari Bioengineering Research Group, Nanotechnology and
Advanced Materials Department, Materials and Energy Research Centre (MERC),
Tehran, Iran; Department of Tissue Engineering & Regenerative Medicine, Faculty
of Advanced Technologies in Medicine, Iran University of Medical Sciences
(IUMS), Tehran, Iran; Cellular and Molecular Research Center, Iran University of
Medical Sciences, Tehran, Iran
Shariq Najeeb Independent Researcher and Private Practitioner, Alberta,
Canada; National Center for Proteomics, University of Karachi, Pakistan
Seung Yun Nam Interdisciplinary Program of Marine-Biomedical, Electrical and
Mechanical Engineering, Center for Marine-Integrated Biomedical Technology
(BK21 Plus), Pukyong National University, Busan, South Korea; Department of
Biomedical Engineering, Pukyong National University, Busan, South Korea
Hafiz Muhammad Owais Nasim Department of Dental Materials, Sharif Medical
and Dental College, Lahore, Pakistan
Touraj Nejatian Eastman Dental Institute, University College of London, London,
United Kingdom; Nottingham Dental Clinic, Nottingham, United Kingdom; Royal
College of Surgeons of England, London, United Kingdom
Rafael Rocha Pacheco School of Dentistry, University of Detroit Mercy, Detroit,
MI, United States
Brouki Milan Peiman Cellular and Molecular Research Center, Iran University of
Medical Sciences, Tehran, Iran; Department of Tissue Engineering & Regenerative
Medicine, Faculty of Advanced Technologies in Medicine, Iran University of
Medical Sciences, Tehran, Iran
Sajjad Pezeshki Babol University of Medical Sciences, Babol, Iran
Zeeshan Qamar Department of Oral and Maxillofacial Surgery, Riyadh Elm
University, Riyadh, Saudi Arabia
Jean-Marc Retrouvey Division of Orthodontics, Faculty of Dentistry, McGill
University, Montreal, QC, Canada
List of contributors
xxv
Sahba Rezaei School of Chemical Engineering, College of Engineering,
University of Tehran, Tehran, Iran
Francisco Javier Rodrı́guez-Lozano School of Dentistry, University of Murcia,
Murcia, Spain
Vinicius Rosa Faculty of Dentistry, National University of Singapore, Singapore,
Singapore; Centre for Advanced 2D Materials and Graphene Research Centre,
National University of Singapore, Singapore, Singapore
Mahsa Roshandel Department of Anatomy and Pathology, University of Siena,
Siena, Italy
Mohammad Reza Saeb Color and Polymer Research Center (CPRC), Amirkabir
University of Technology, Tehran, Iran; Advanced Materials Group, Iranian Color
Society (ICS), Tehran, Iran; Department of Resin and Additive, Institute for Color
Science and Technology, Tehran, Iran
Farshid Sefat Biomedical and Electrical Engineering Department, School of
Engineering, University of Bradford, Bradford, United Kingdom; Interdisciplinary
Research Center in Polymer Science & Technology (IRC Polymer), University of
Bradford, Bradford, United Kingdom
Saroash Shahid Centre for Oral Bioengineering, Institute of Dentistry, Queen
Mary University of London, London, United Kingdom
Zeeshan Sheikh Faculty of Dentistry, University of Toronto, Toronto, ON,
Canada; Lunenfeld-Tanenbaum Research Institute, Mount Sinai Hospital, Toronto,
ON, Canada; Department of Laboratory Medicine and Pathobiology, University of
Toronto, Toronto, ON, Canada
Dalia Sherief Dental Biomaterials Department, Faculty of Dentistry, Ain-Shams
University, Cairo, Egypt
Sunjay Suri Division of Orthodontics, Faculty of Dentistry, University of Toronto,
Toronto, ON, United States
Ahmed Talal Department of Restorative Dental Sciences, College of Dentistry,
Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Waqas Tanveer Maxillofacial Prosthetic Service, Department of Prosthodontics,
Faculty of Dentistry, Mahidol University, Bangkok, Thailand
xxvi
List of contributors
James K.H. Tsoi Dental Materials Science, Discipline of Applied Oral Sciences,
Faculty of Dentistry, The University of Hong Kong, Pokfulam, Hong Kong SAR,
P.R. China
Rizwan Ullah Department of Oral Biology, Sindh Institute of Oral Health
Sciences, Jinnah Sindh Medical University, Karachi, Pakistan
Daniel Varley Medical Engineering Department, Faculty of Engineering and
Informatics, University of Bradford, Bradford, United Kingdom
Gaurav Vasudeva School of Dentistry, James Cook University, Townsville, QLD,
Australia; Oral Health Services, Hobart, TAS, Australia
Jayachandran Venkatesan Yenepoya Research Centre, Yenepoya University,
Mangalore, India
Rafael Pino Vitti Department of Dentistry, University of Taubaté, Taubaté,
Brazil; Department of Dentistry, Araras Dental School (FHO|UNIARARAS),
Araras, Brazil
Syed Azeem Ul Yaqin Department of Prosthodontics and Dental Implantology,
College of Dentistry, King Faisal University, Al-Ahsa, Saudi Arabia
Safiyya Yousaf Medical Engineering Department, Faculty of Engineering and
Informatics, University of Bradford, Bradford, United Kingdom
Mansour Youseffi Medical Engineering Department, Faculty of Engineering and
Informatics, University of Bradford, Bradford, United Kingdom
Muhammad S. Zafar Department of Dental Materials, Islamic International
Dental College, Riphah International University, Islamabad, Pakistan; Department
of Restorative Dentistry, College of Dentistry, Taibah University, Medina,
Saudi Arabia
Muhammad Sohail Zafar Department of Restorative Dentistry, College of
Dentistry, Taibah University, Almadinah Almunawwarah, Saudi Arabia
Payam Zarrintaj Polymer Engineering Department, Faculty of Engineering,
Urmia University, Urmia, Iran; Color and Polymer Research Center (CPRC),
Amirkabir University of Technology, Tehran, Iran; Advanced Materials Group,
Iranian Color Society (ICS), Tehran, Iran
Introduction to dental
biomaterials and their advances
1
Zohaib Khurshid1, Muhammad S. Zafar2,3, Shariq Najeeb4,
Touraj Nejatian5,6 and Farshid Sefat7
1
Department of Prosthodontics and Dental Implantology, College of Dentistry, King Faisal
University, Al-Ahsa, Saudi Arabia, 2Department of Restorative Dentistry, College of
Dentistry, Taibah University, Medina, Saudi Arabia, 3Department of Dental Materials,
Islamic International Dental College, Riphah International University, Islamabad, Pakistan,
4
National Center for Proteomics, University of Karachi, Pakistan, 5Royal College of
Surgeons of England, London, United Kingdom, 6Nottingham Dental Clinic, Nottingham,
United Kingdom, 7Biomedical and Electrical Engineering Department, School of
Engineering, University of Bradford, Bradford, United Kingdom
Chapter Outline
References 3
Further reading
5
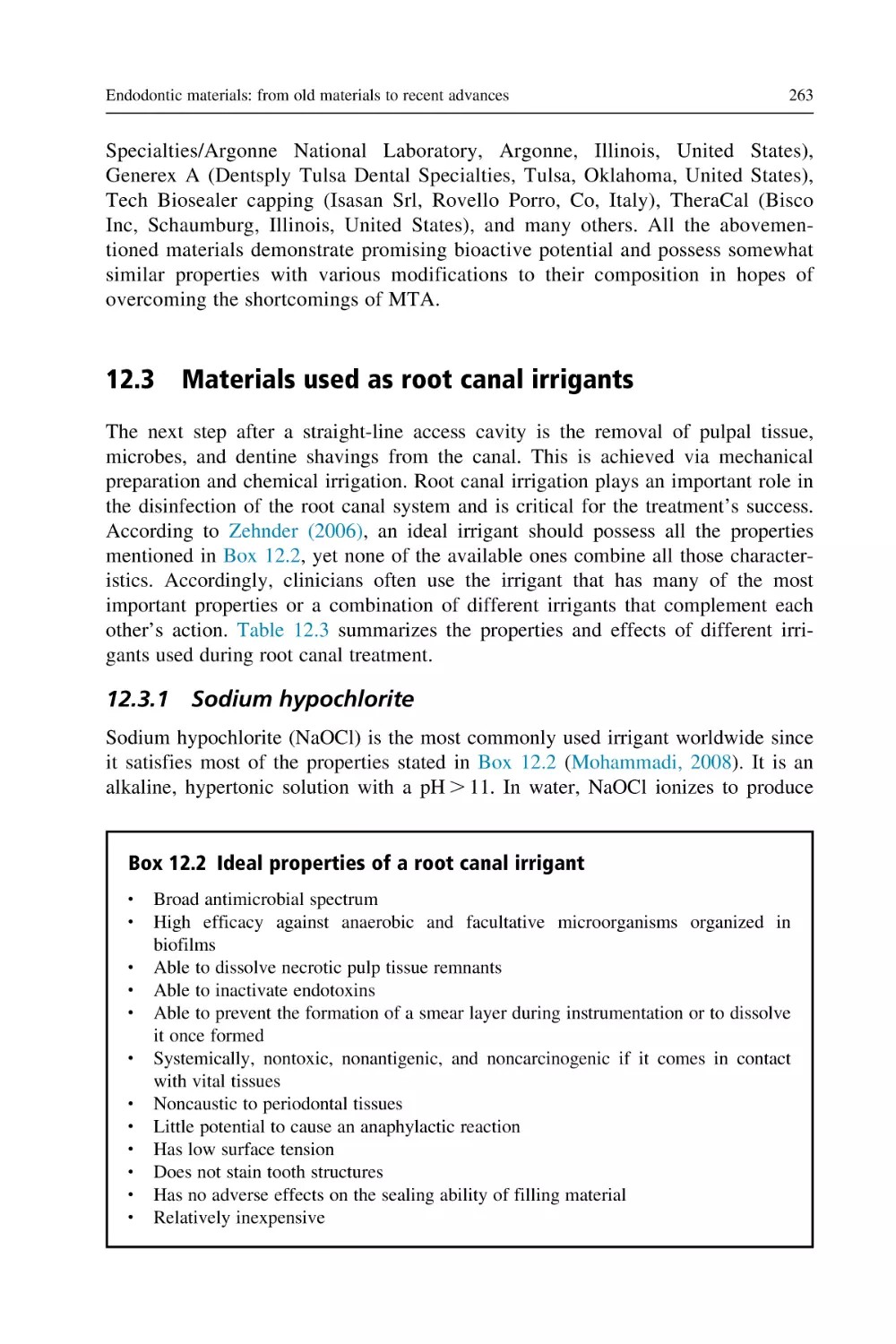
Dental biomaterials and tissue engineering are rapidly developing approaches being
used for the production of new organs and body tissues, particularly for bone
implants or dental tissue replacements. Yet, over the past few decades, there has
been a wide range of research conducted on the provision of tissue engineered dental grafts that has led to a significant improvement in the production of scaffolds
with similar characteristics to a natural tooth (Zafar and Ahmed, 2015).
Tissue engineering in the 21st century has become a cutting-edge science in the
field of medicine and it is expected in the near future to replace traditional therapies
which cause enormous side effects. In the tissue engineering principles, one of the
main elements after cells, environmental factors, and signaling molecules is the biomaterial, which plays an important role in successful functional tissue engineered
products. In recent years significant improvement and progress have been reported
in the reconstruction of various human tissue replacements and prostheses, including bone (Sefat et al., 2010, 2014), cartilage (Daghigh Ahmadi et al., 2018; Raja
et al., 2018), skin (Mahjour et al., 2015; Bye et al., 2014), oral tissues (Nejatian
et al., 2017; Zafar and Ahmed, 2015; Qasim et al., 2018; Najeeb et al., 2017), cornea (Deshpande et al., 2013; Ortega et al., 2014), nerve (Mohamadi et al., 2017;
Mohammadi et al., 2018), and adipose tissue (Amini et al., 2018).
The most common methods used in the fabrication of tissue engineering scaffolds,
particularly as dental biomaterials, consist of hydrogels, molecular self-assembly, thermally induced phase separation, solvent casting, particulate-leaching techniques, and
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00001-3
Copyright © 2019 Elsevier Ltd. All rights reserved.
2
Advanced Dental Biomaterials
the electrospinning process (Gentile et al., 2017; Mahjour et al., 2016). In particular,
for dental tissue engineering much research has been carried out using electrospinning
(Zafar et al., 2016; Qasim et al., 2018), and this is the most widely used method in the
production of tissue engineered teeth.
Dentistry, similarly to medicine and other related subjects such as biomedical
engineering, biomedical science, pharmacy, and pharmacology, has been revolutionized by the introduction of new technologies, for example, dentists use digital
technology to carry out dental treatments. For this reason, we have included an
interesting chapter on digital dentistry in this book.
This book covers both the basic and clinical sciences of dental biomaterials with
the view to meeting the needs of researchers and practitioners. In this book, the
authors mainly look at various dental biomaterials’ properties and characterization
techniques, such as metal alloys, polymers, composites, and ceramics.
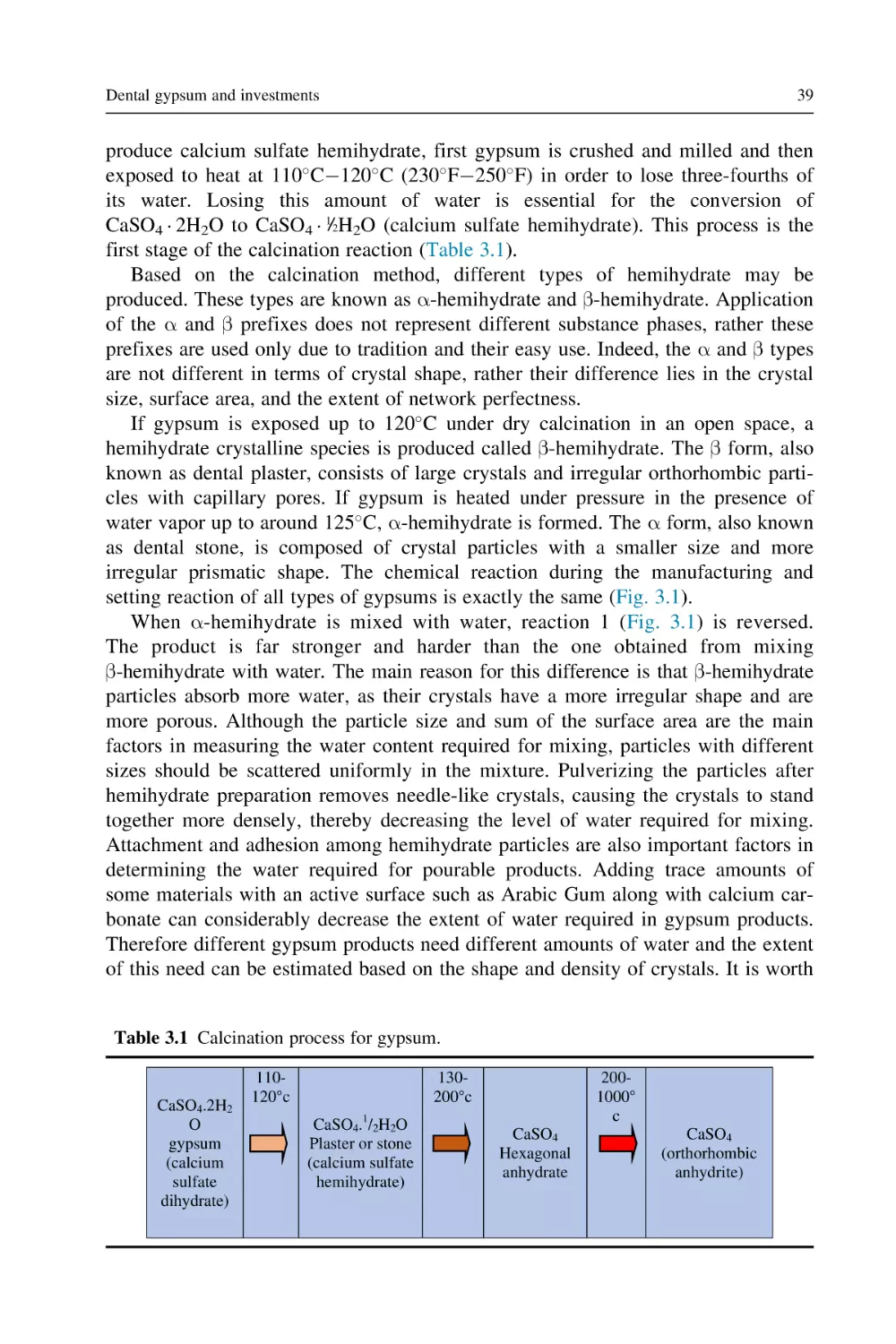
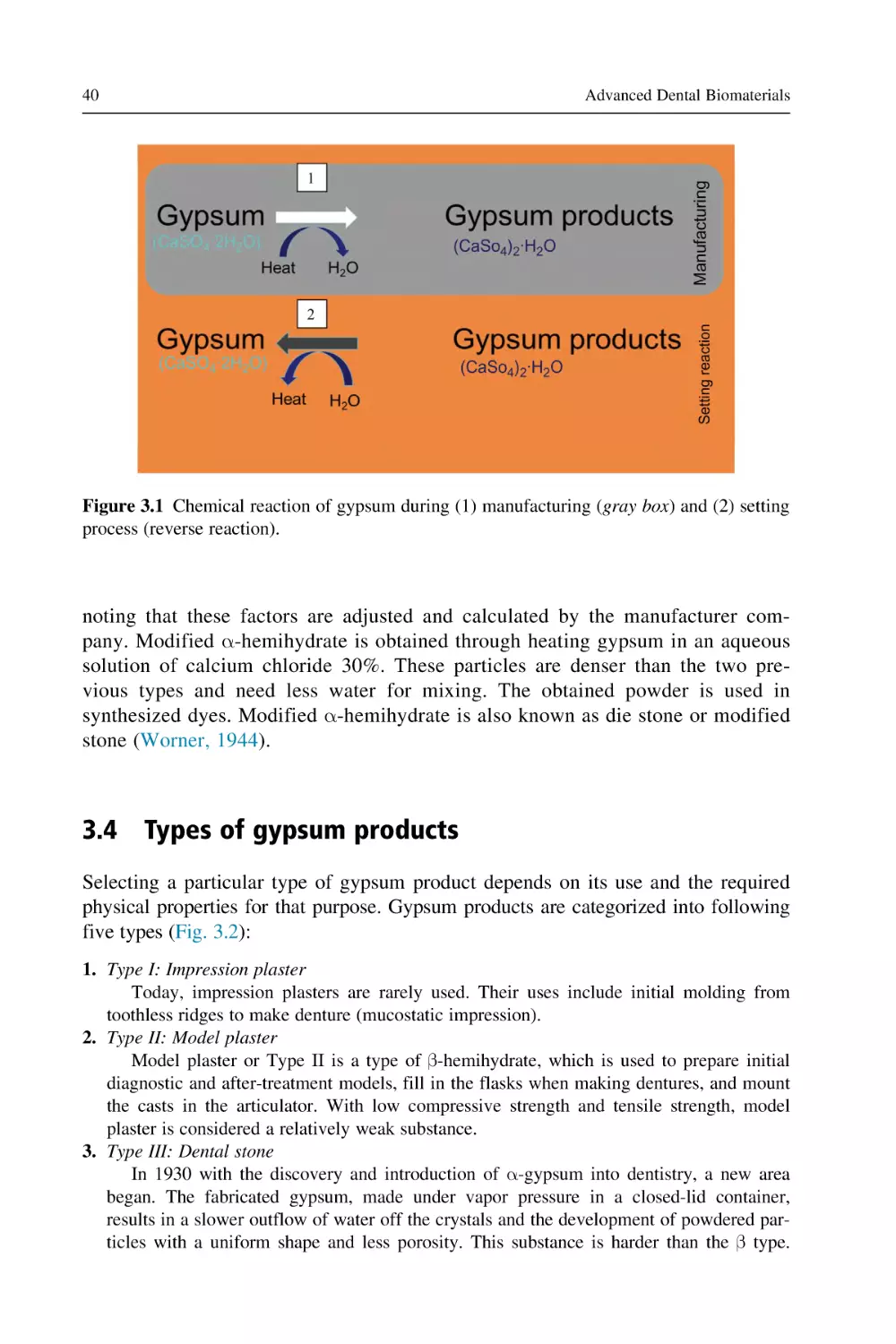
A chapter will focus on dental gypsum and investment materials covering composition, types, manufacturing, and applications. Gypsum products can be found as
a powder which forms a fluid mass once combined with water and, therefore, has
the capability to be shaped, before finally hardening into a rigid, stable mass. The
main application of gypsum products is to replicate the shape of oral structures,
which will be discussed in this chapter.
Acrylic resin is a biomaterial that has the required mechanical and physical properties (Zafar and Ahmed, 2014), and it has been used as a denture material both in
research and the clinic. Much research has been done on the biocompatibility and
biodegradability of this material (Nejatian et al., 2015). Acrylic resin will be discussed in a separate chapter in this book.
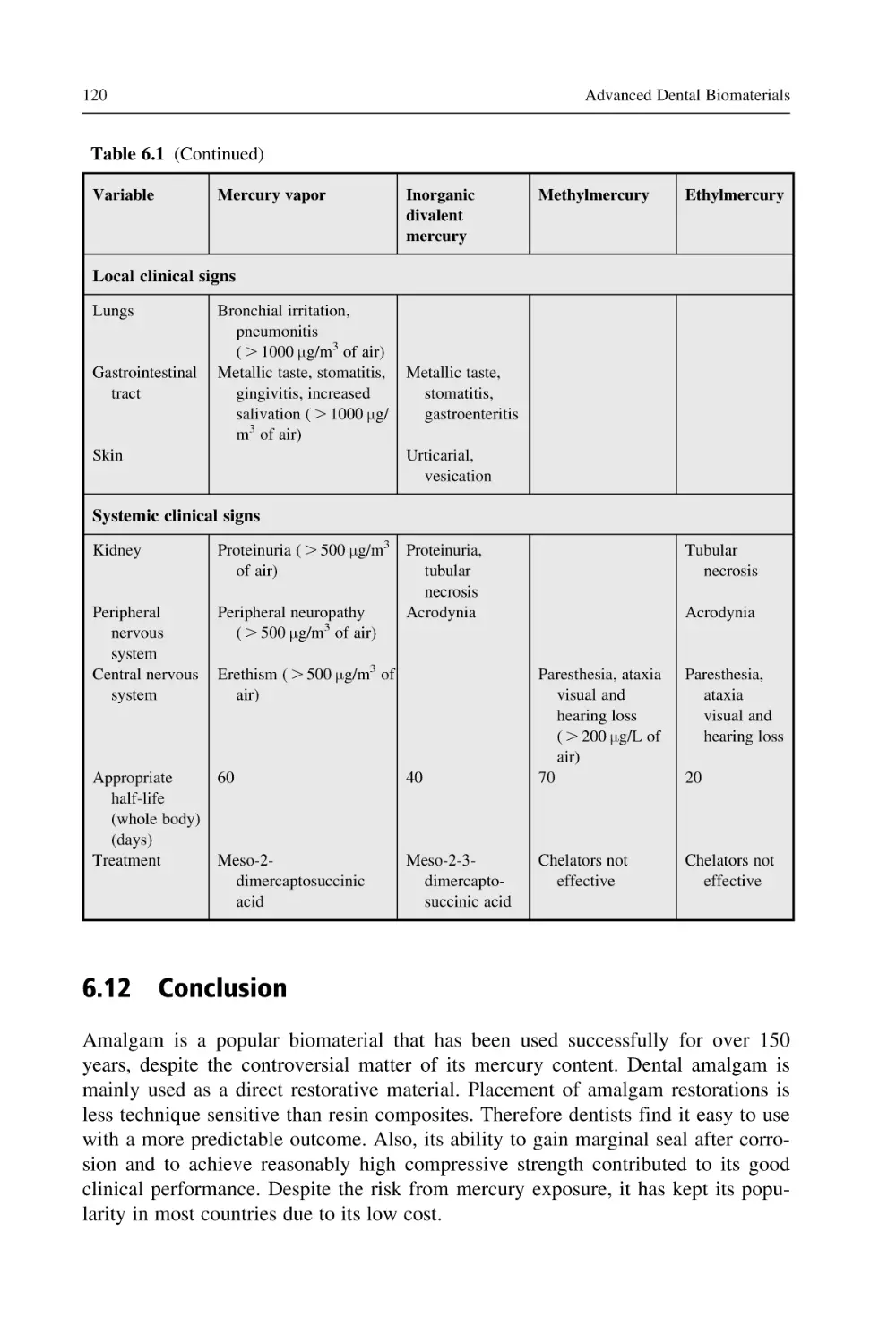
Another chapter is mainly focused on dental amalgam, which has been used successfully in the dental industry for decades. Dental amalgam is composed of a mixture of metal alloy and liquid mercury. Amalgam is mainly used for dental
restorations. The current trend in the United Kingdom is to phase-down amalgam
application due to the increasing concern over the safety of mercury, however, it is
still widely used in many other countries, including the United States. Amalgam
stays soft for a short period of time after it is mixed, which allows enough time for
it to be condensed and shaped onto the prepared tooth (Gay et al., 1979; Bates,
2006).
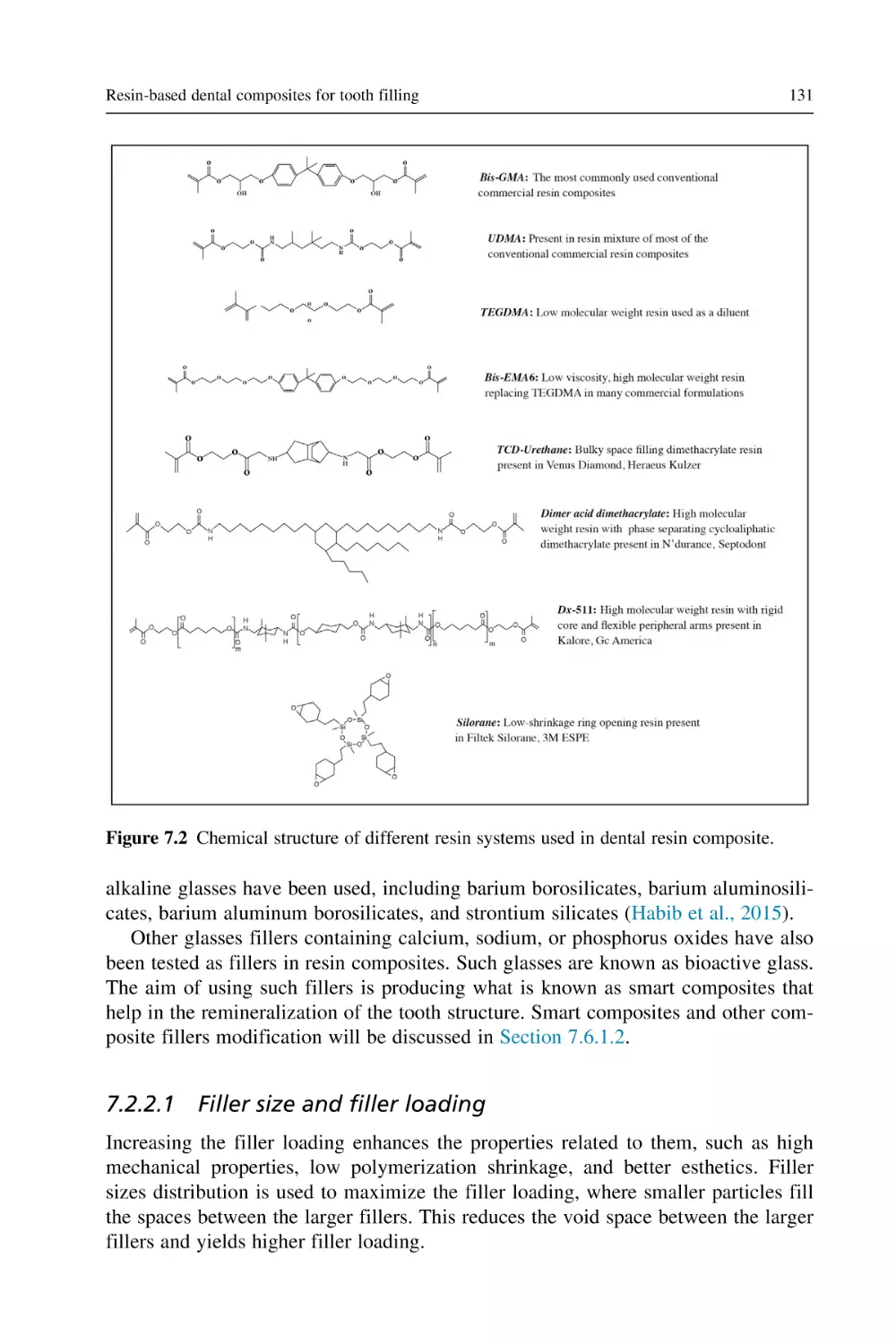
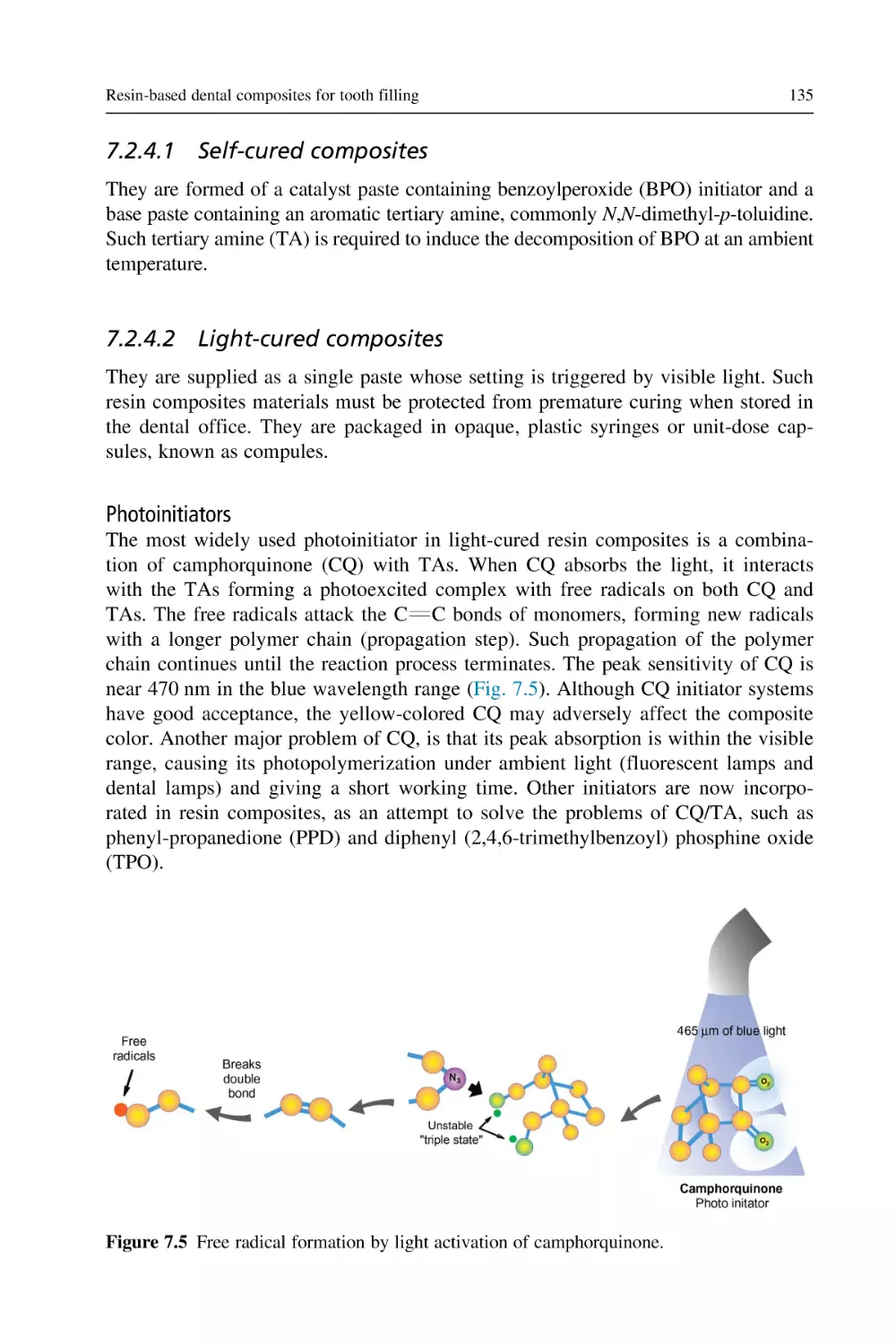
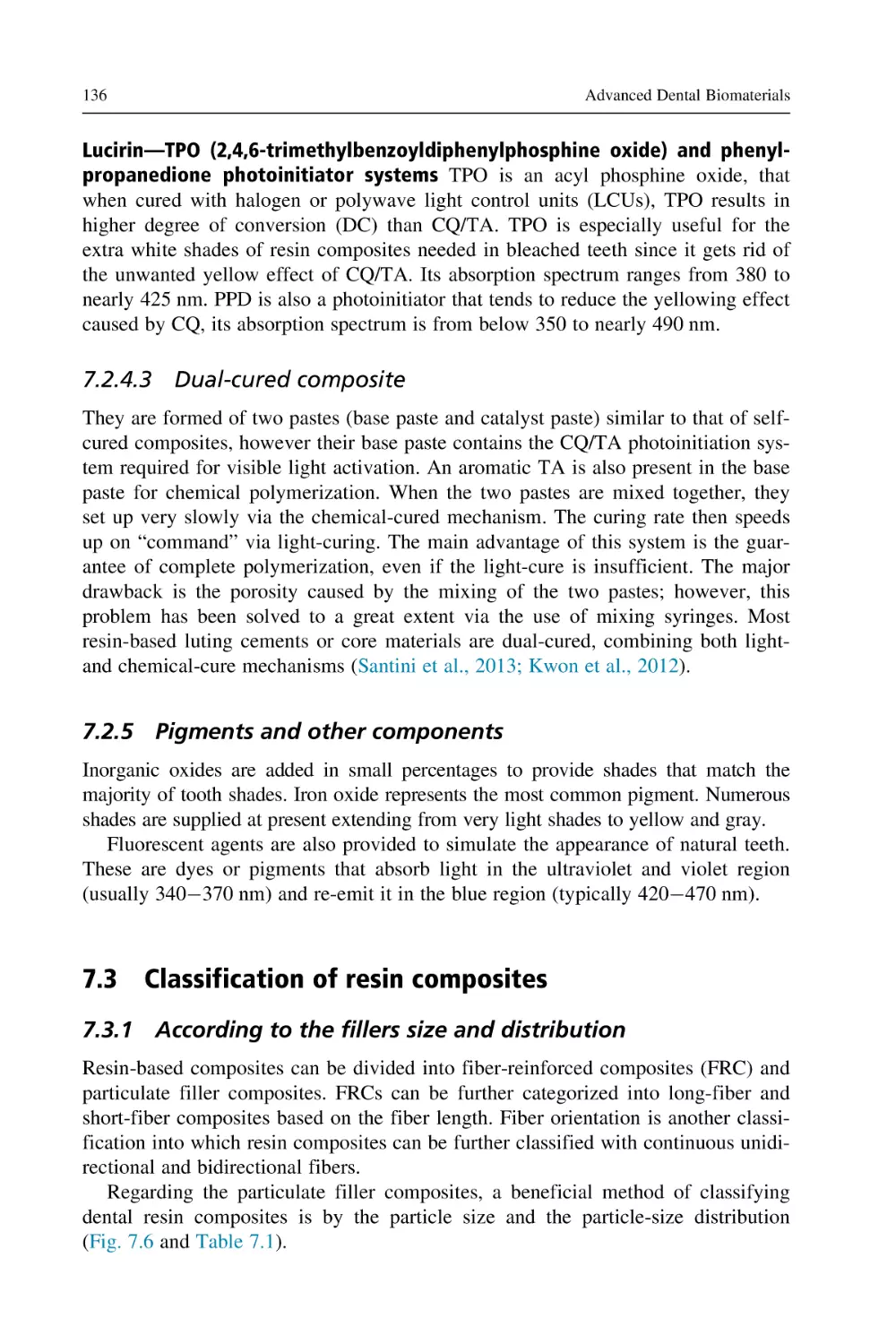
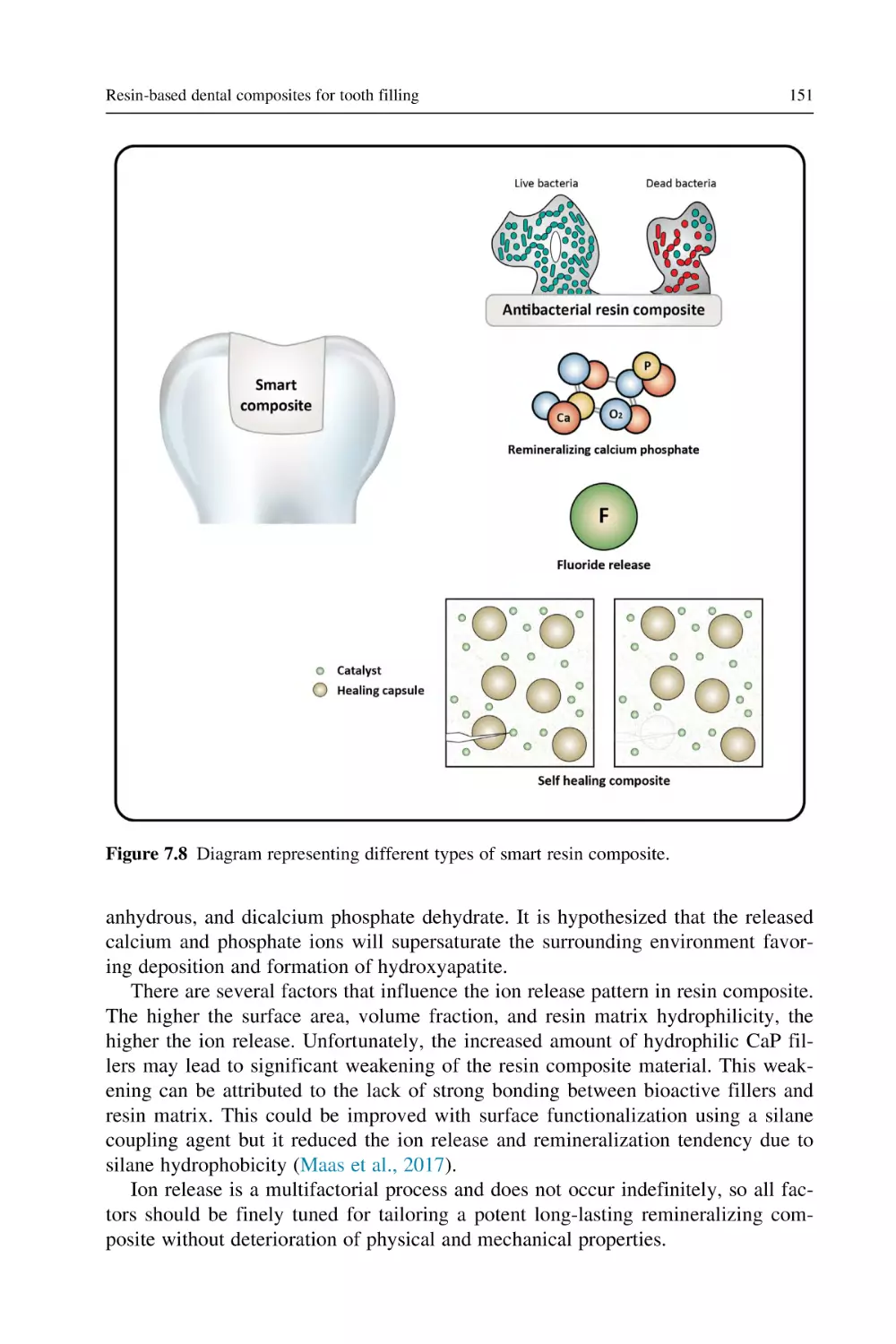
Dental resin composites are important biomaterials that have been increasingly
used as the main restorative materials (Nejatian et al., 2017; Khurshid et al., 2015).
In this book the specific types of composites as well as the potential biological
issues of dental composites are discussed in detail. In addition, resin-based dental
composites for tooth filling are addressed in a separate chapter due to their
importance.
Cements are another important group of biomaterials that have been explored
intensively by researchers and clinicians. A separate chapter is allocated to dental
cements, including base, liner, luting, and temporary cements, as well as pulp capping materials. Due to the high clinical demand for dental cements, the chemistry
and applications of glass ionomer cement (GIC) and nano-GIC have been discussed
broadly here in this book.
Introduction to dental biomaterials and their advances
3
Dental impression materials have been utilized as negative replicas to fabricate
dental models. Various natural and synthetic materials have been utilized as dental
impression materials, which are frequently classified on the basis of their properties
into two groups, that is, elastic and nonelastic families. In this book, impression
materials and their properties are discussed with the aim of providing a practical
guide for dentists and prosthodontists.
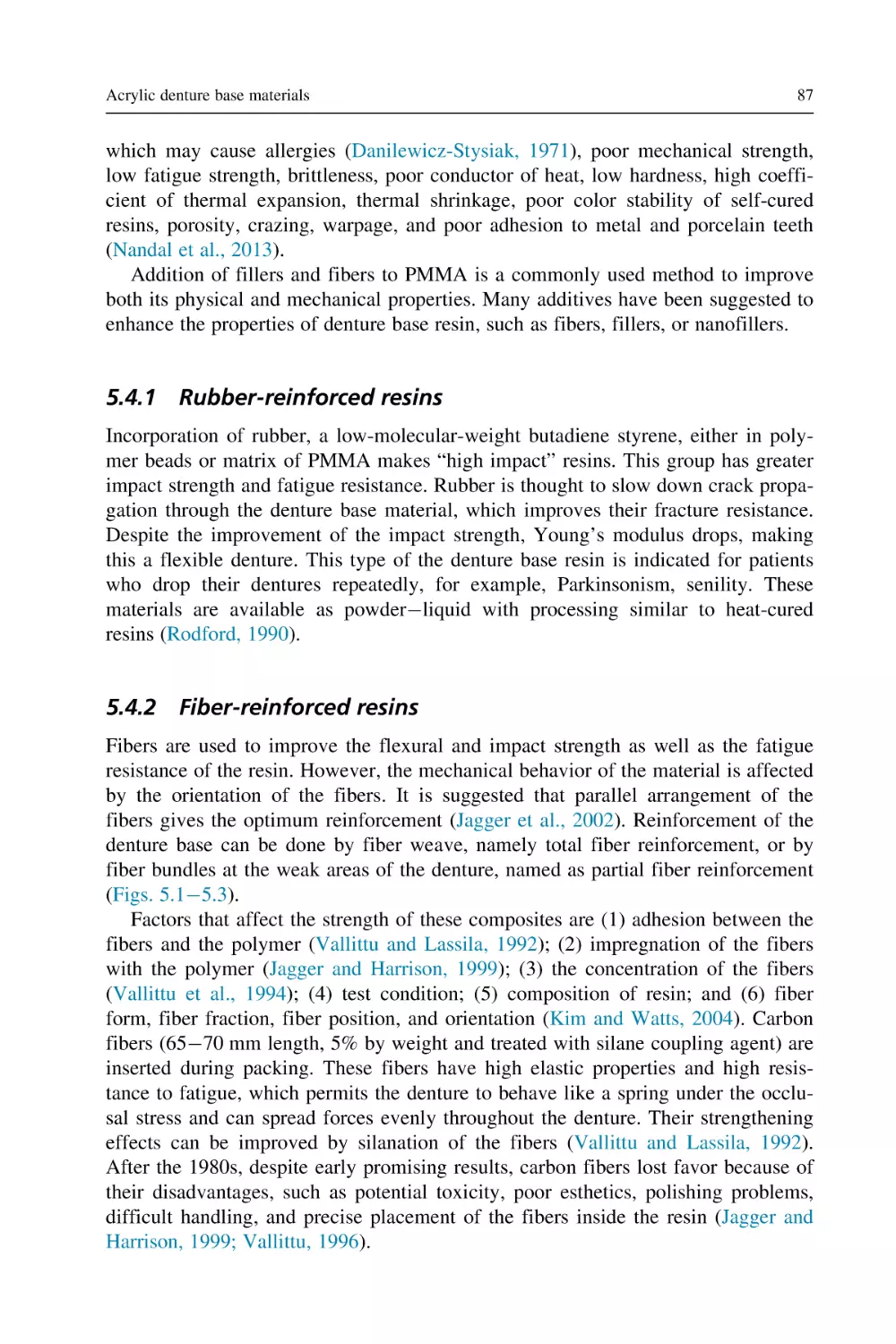
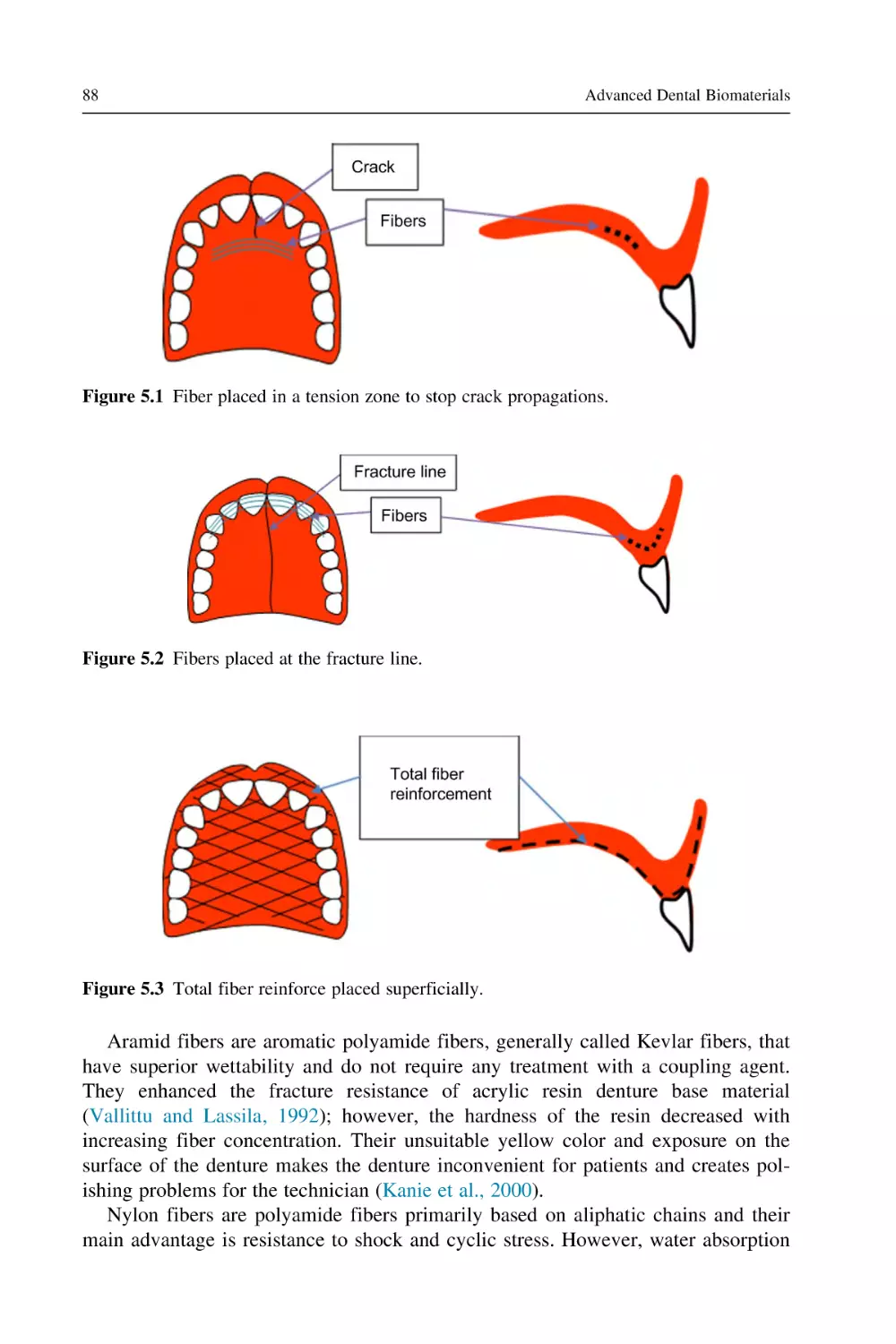
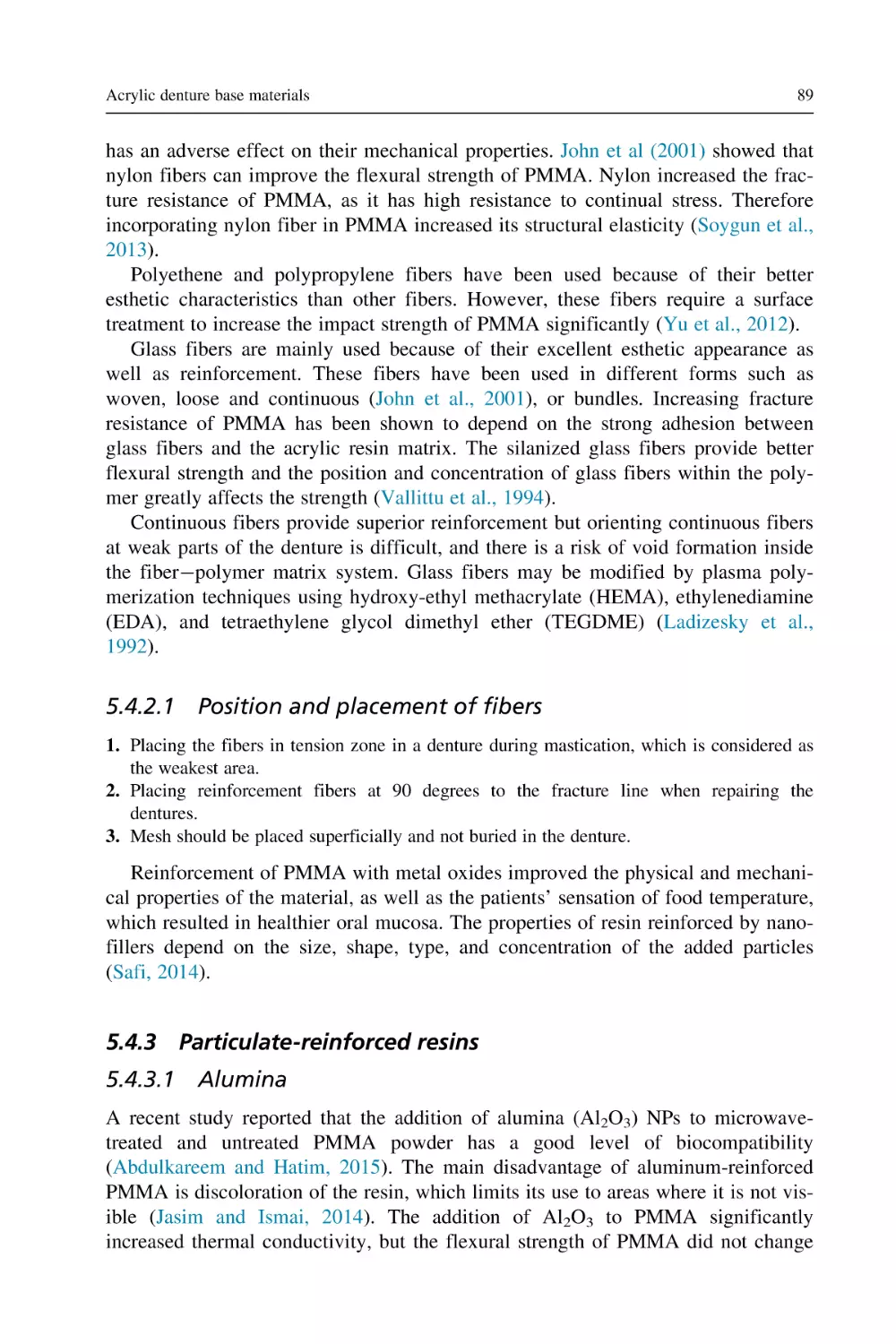
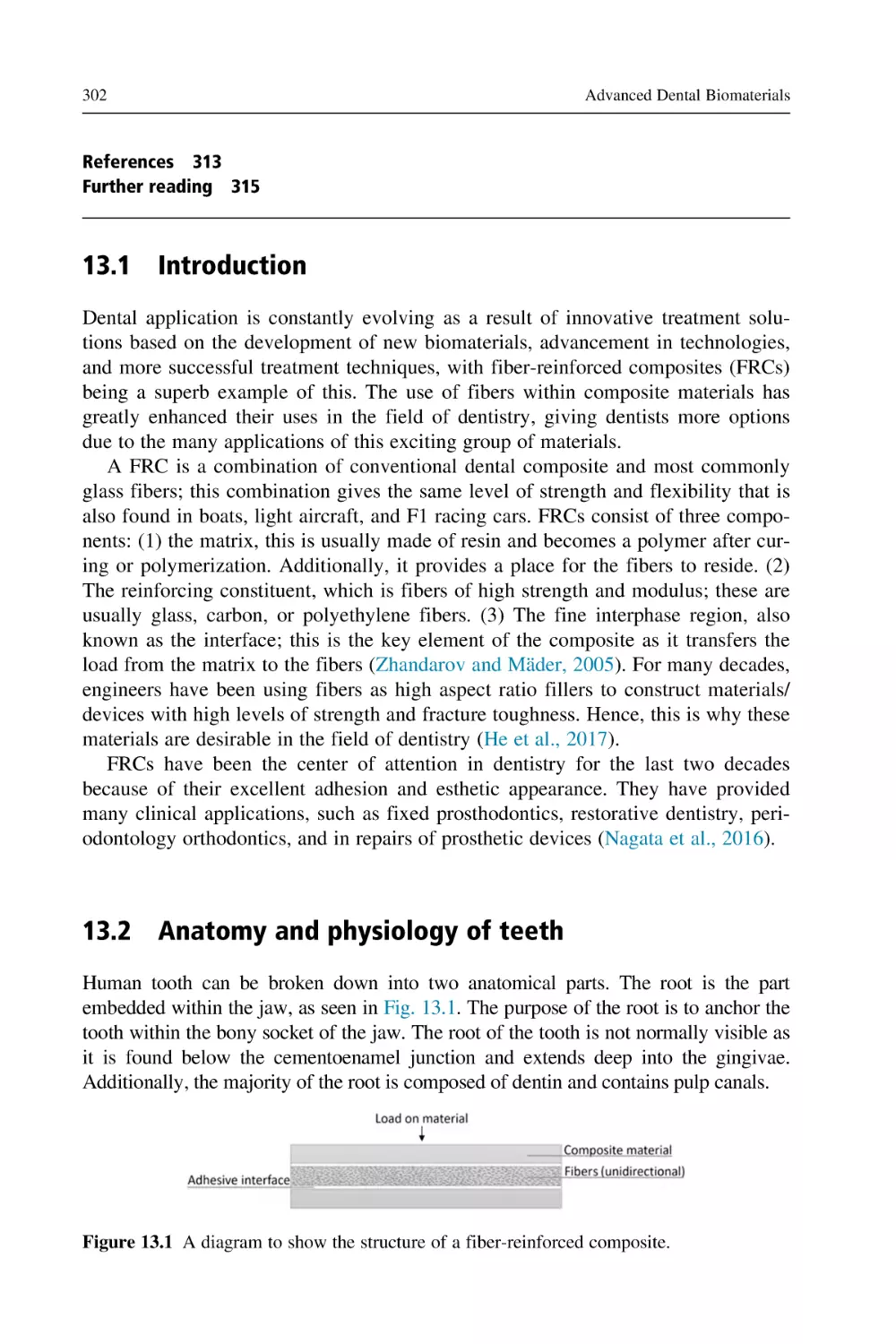
Fiber reinforced composites (FRCs) are combinations of conventional dental
resin composites and glass fibers. This combination provides a high level of
strength in the same way as that found in boats, light aircraft, and F1 racing cars.
For many decades, engineers have been using fibers as fillers to construct materials/devices with high levels of strength and fracture toughness. That is why these
materials attracted attention as desirable restorative materials in the field of dentistry (He et al., 2017). FRCs have been the center of attention in dentistry in the
21st century because of their excellent adhesion and appearance. Nowadays these
materials have many clinical applications, such as fixed prosthodontics, restorative
dentistry, periodontology, orthodontics, and repair of prosthetic devices (Nagata
et al., 2016). FRCs are discussed in detail in a chapter of this book. Additionally, a
number of emerging materials that have been extensively explored for various dental applications, such as nanomaterials (Najeeb et al., 2015, 2016a,b,c,d; Zafar
et al., 2017), polyether ether ketones (Najeeb et al., 2016a,b), natural silk (Zafar
and Ahmed, 2014), and antimicrobial peptides (Khurshid et al., 2016a,b, 2017,
2018), will be discussed in parts of various chapters.
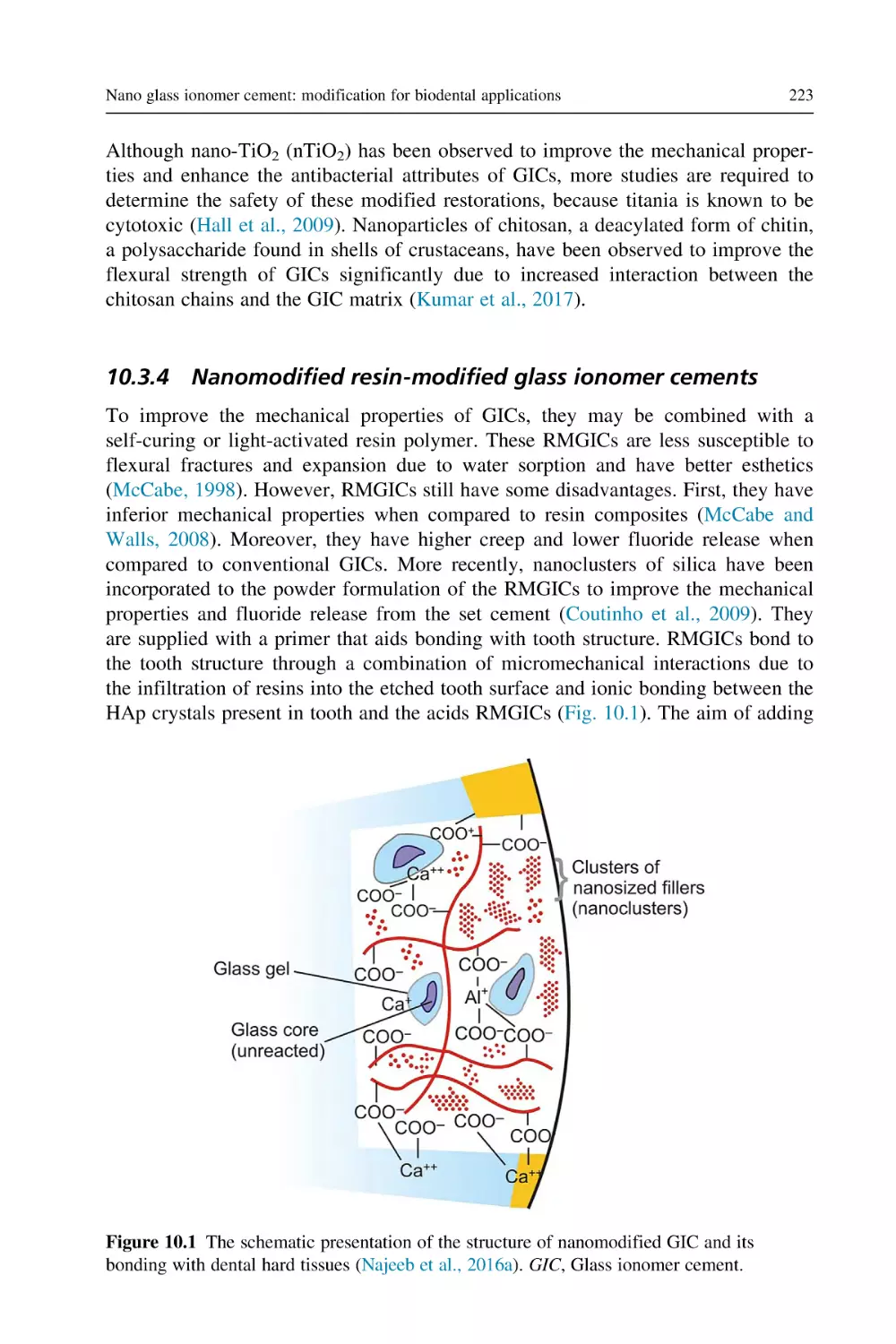
The use of GICs as direct restorative dental materials, which have been extensively studied and used in dentistry (Zafar and Ahmed, 2015; Najeeb et al., 2016a,
b,c,d), is also discussed in detail in this book. Other advanced dental biomaterials
are also covered in great detail including endodontic materials, advanced ceramics,
bone cements, calcium phosphate, bioactive glasses, graphene, and silicon, as well
as orthodontic materials including wires, orthodontic brackets, elastomeric ligatures,
and chains. The final chapter discusses biomaterials used for maxillofacial prosthetic rehabilitation/reconstruction, as well as biomaterials for craniofacial tissue
engineering and regenerative dentistry which are hot topics in the field of bioengineering and regenerative medicine.
References
Amini, N., Vousooghi, N., Alizade, A., Ramezani, S., Joghataei, M.T., Brouki Milan, P.,
et al., 2019. Transplantation of adipose tissue-derived stem cells into brain through cerebrospinal fluid in rat models: protocol development and initial outcome data. Curr. Stem
Cell Res. Ther. 14 (2), 191 195.
Bates, M.N., 2006. Mercury amalgam dental fillings: an epidemiologic assessment. Int. J.
Hyg. Environ. Health 209, 309 316.
Bye, F.J., Bullock, A.J., Singh, R., Sefat, F., Roman, S., Macneil, S., 2014. Development of a
basement membrane substitute incorporated into an electrospun scaffold for 3D skin tissue engineering. J. Biomater. Tissue Eng. 4, 1 7.
4
Advanced Dental Biomaterials
Daghigh Ahmadi, E., Raja, T.I., Khaghani, S.A., Soon, C.F., Mozafari, M., Youseffi, M.,
et al., 2018. The role of photonics and natural curing agents of TGF-β1 in treatment of
osteoarthritis. Mater. Today Procedia 5, 15540 15549.
Deshpande, P., Sefat, F., Ramchadaran, C., Mariappan, I., Johnson, C., Mckean, R., et al.,
2013. Simplifying corneal surface regeneration using a biodegradable synthetic membrane and limbal tissue explants. Biomaterials 34 (21), 5088 5106.
Gay, D.D., Cox, R.D., Reinhardt, J.W., 1979. Chewing releases mercury from fillings.
Lancet 1 (8123), 985 986.
Gentile, P., Mccolgan-Bannon, K., Ceretto, N., Sefat, F., Dalgarno, K., Ferreira, A.M., 2017.
Biosynthetic PCL-graft-collagen bulk material for tissue engineering applications.
Materials 10, 693.
He, J., Vallittu, P., Lassila, L.V., 2017. Preparation and characterization of high radio-opaque
E-glass fibre-reinforced composite with iodine containing methacrylate monomer. Dent.
Mater. 33 (2), 218 225.
Khurshid, Z., Zafar, M., Qasim, S., Shahab, S., Naseem, M., AbuReqaiba, A., 2015.
Advances in nanotechnology for restorative dentistry. Materials 8 (2), 717 731.
Khurshid, Z., Naseem, M., Sheikh, Z., Najeeb, S., Shahab, S., Zafar, M.S., 2016a. Oral antimicrobial peptides: types and role in the oral cavity. Saudi Pharm. J 24 (5), 515 524.
Khurshid, Z., Zohaib, S., Najeeb, S., Zafar, M.S., Rehman, R., Rehman, I.U., 2016b.
Advances of proteomic sciences in dentistry. Int. J. Mol. Sci. 17 (5), 728.
Khurshid, Z., Najeeb, S., Mali, M., Moin, S.F., Raza, S.Q., Zohaib, S., et al., 2017. Histatin
peptides: pharmacological functions and their applications in dentistry. Saudi Pharm. J.
25 (1), 25 31.
Khurshid, Z., Zafar, M.S., Naseem, M., Khan, R.S., Najeeb, S., 2018. Human Oral Defensins
antimicrobial peptides: a future promising antimicrobial drug. Curr. Pharm. Des. 24
(10), 1130 1137.
Mahjour, S.B., Fu, X., Yang, X., Fong, J., Sefat, F., Wang, H., 2015. Rapid creation of skin
substitutes from human skin cells and biomimetic nanofibers for acute full-thickness
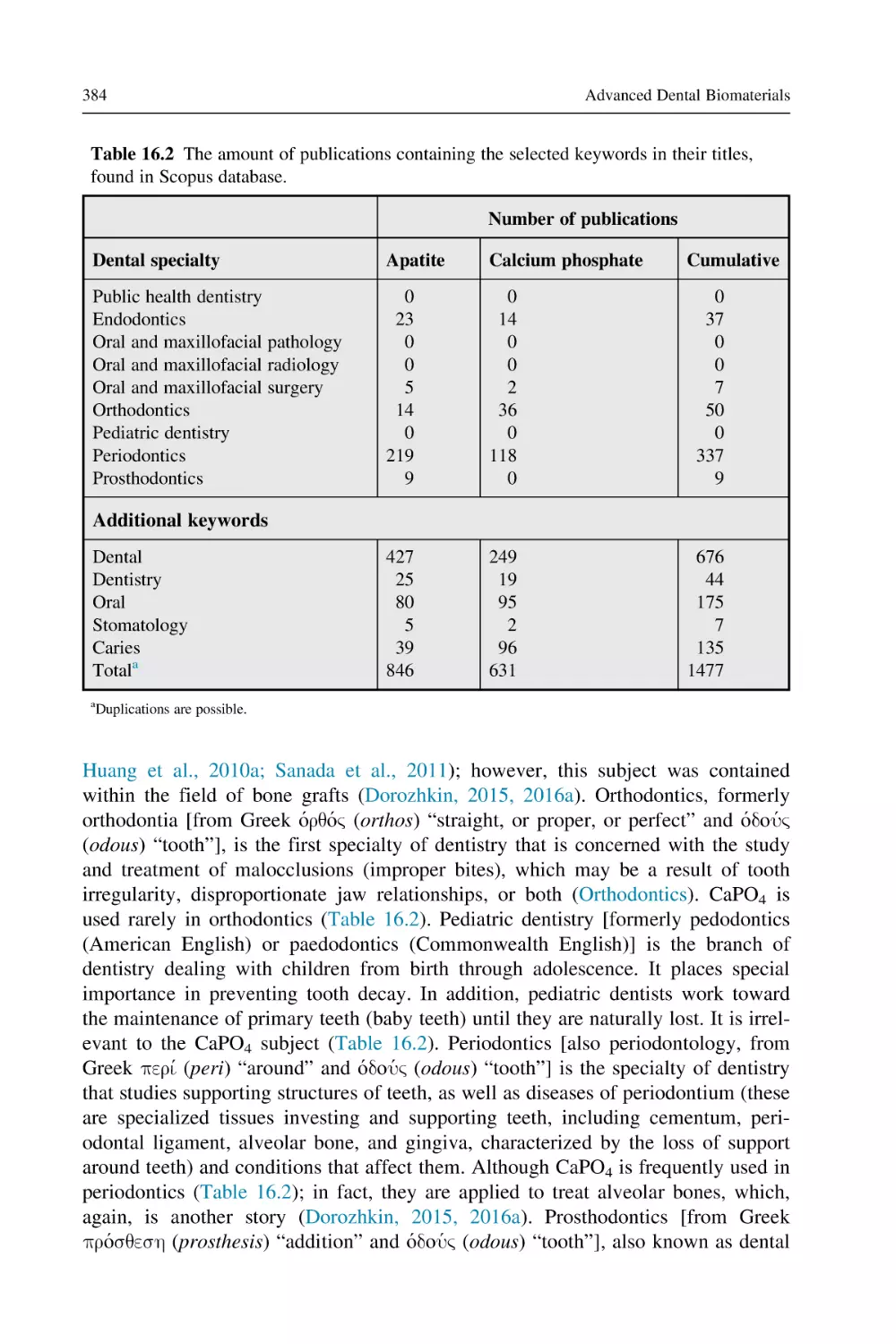
wound repair. Burns 41 (8), 1764 1774.
Mahjour, S.B., Sefat, F., Polunin, Y., Wang, L., Wang, H., 2016. Improved cell infiltration of
electrospun nanofiber mats for layered tissue constructs. J. Biomed. Mater. Res. Part A
104 (6), 1479 1488.
Mohamadi, F., Ebrahimi, S., Nourani, M.R., Mansoori, K., Alizadeh, A.A., Tavangar, S.M.,
et al., 2017. Enhanced sciatic nerve regeneration by human endometrial stem cells in an
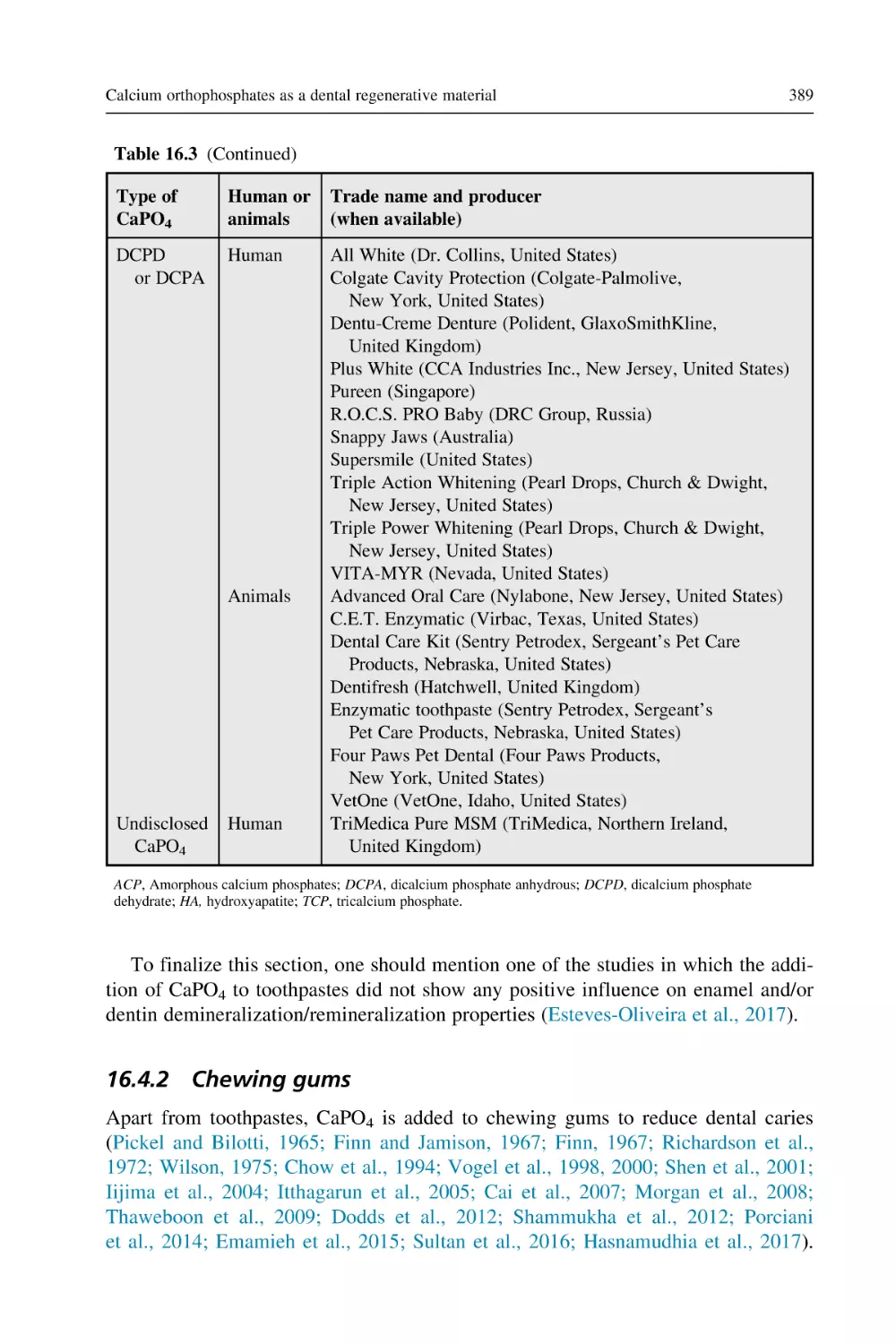
electrospun poly (ε-caprolactone)/collagen/NBG nerve conduit in rat. Artif. Cells
Nanomed. Biotechnol. 46 (8), 1731 1743.
Mohammadi, A., Maleki-Jamshid, A., Sanooghi, D., Brouki Milan, P., Rahmani, A., Sefat,
F., et al., 2018. Transplantation of human chorion-derived cholinergic progenitor cells: a
novel treatment for neurological disorders. Mol. Neurobiol. 56 (1), 307 318.
Nagata, K., Garoushi, S.K., Vallittu, P.K., Wakabayashi, N., Takahashi, H., Lassila, L.V.J.,
2016. Fracture behaviour of single-structure fibre-reinforced composite restorations.
Acta Biomater. Odontol. Scand. 2 (1), 118 124.
Najeeb, S., Khurshid, Z., Matinlinna, J.P., Siddiqui, F., Nassani, M.Z., Baroudi, K., 2015.
Nanomodified peek dental implants: bioactive composites and surface modification—a
review. Int. J. Dent. 2015, 381759.
Najeeb, S., Bds, Z.K., Bds, S.Z., Bds, M.S., 2016a. Bioactivity and osseointegration of PEEK
are inferior to those of titanium: a systematic review. J. Oral Implantol. 42 (6), 512 516.
Najeeb, S., Zafar, M.S., Khurshid, Z., Siddiqui, F., 2016b. Applications of polyetheretherketone
(PEEK) in oral implantology and prosthodontics. J. Prosthodont. Res. 60 (1), 12 19.
Introduction to dental biomaterials and their advances
5
Najeeb, S., Khurshid, Z., Zafar, M.S., Khan, A.S., Zohaib, S., Martı́, J.M., et al., 2016c.
Modifications in glass ionomer cements: nano-sized fillers and bioactive nanoceramics.
Int. J. Mol. Sci. 17 (7), 1134.
Najeeb, S., Khurshid, Z., Agwan, A.S., Zafar, M.S., Alrahabi, M., Qasim, S.B., et al., 2016d.
Dental applications of nanodiamonds. Sci. Adv. Mater. 8 (11), 2064 2070.
Najeeb, S., Khurshid, Z., Agwan, M.A., Ansari, S.A., Zafar, M.S., Matinlinna, J.P., 2017.
Regenerative potential of platelet rich fibrin (PRF) for curing intrabony periodontal
defects: a systematic review of clinical studies. Tissue Eng. Regener. Med 1, 1 8.
Nejatian, T., Sefat, F., Johnson, T., 2015. Impact of packing and processing technique on
mechanical properties of acrylic denture base materials. Materials 8 (5), 2093 2109.
Nejatian, T., Khurshid, Z., Zafar, M.S., Najeeb, S., Zohaib, S., Mozafari, M., et al., 2017.
Dental biocomposites (Chapter 5). Biomaterials for Oral and Dental Tissue Engineering.
Elsevier, pp. 65 83.
Ortega, I., Sefat, F., Paterson, T., Deshpande, P., Ramchadaran, C., Claeyssens, F., et al.,
2014. Combination of microstereolithography and electrospinning to produce membranes equipped with niches for corneal regeneration. J. Vis. Exp 91, e51826.
Qasim, S.,B., Zafar, M.S., Najeeb, S., Khurshid, Z., Shah, A.H., Husain, S., et al., 2018.
Electrospinning of chitosan-based solutions for tissue engineering and regenerative medicine. Int. J. Mol. Sci. 19 (2), 407.
Raja, T.I., Khaghani, S.A., Zafar, M.S., Khurshid, Z., Mozafari, M., Youseffi, M., et al.,
2018. Effect of TGF-β1 on water retention properties of healthy and osteoarthritic chondrocytes. Mater. Today Proc. 5 (7), 15717 15725.
Sefat, F., Youseffi, M., Denyer, M.C.T., 2010. Imaging via widefield surface plasmon resonance microscope for studying bone cell interactions with micro-patterned ECM proteins. J. Microsc. 241 (3), 282 290.
Sefat, F., Denyer, M.C.T., Youseffi, M., 2014. Effects of different transforming growth factor
beta (TGF-β) isomers on wound closure of bone cell monolayers. Cytokines 64, 75 86.
Zafar, M.S., Ahmed, N., 2014. Nanoindentation and surface roughness profilometry of poly
methyl methacrylate denture base materials. Technol. Health Care 22 (4), 573 581.
Zafar, M.S., Ahmed, N., 2015. Therapeutic roles of fluoride released from restorative dental
materials. Fluoride 48, 184 194.
Zafar, M.S., Najeeb, S., Khurshid, Z., Vazirzadeh, M., Zohaib, S., Najeeb, B., et al., 2016.
Potential of electrospun nanofibers for biomedical and dental applications. Materials 9
(2), 73.
Zafar, M.S., Khurshid, Z., Najeeb, S., Zohaib, S., Rehman, I.U., 2017. Therapeutic applications of nanotechnology in dentistry. Nanostructures for Oral Medicine. Elsevier,
pp. 833 862.
Further reading
Zafar, M.S., Al-Samadani, K.H., 2014. Potential use of natural silk for bio-dental applications. J. Taibah Univ. Med. Sci. 9 (3), 171 177.
Zafar, M.S., Khurshid, Z., Almas, K., 2015. Oral tissue engineering progress and challenges.
Tissue Eng. Regener. Med. 12 (6), 387 397.
Properties of dental biomaterials
2
Muhammad S. Zafar1,2, Rizwan Ullah3, Zeeshan Qamar4,
Muhammad A. Fareed5, Faiza Amin6, Zohaib Khurshid7 and Farshid Sefat8,9
1
Department of Restorative Dentistry, College of Dentistry, Taibah University, Medina,
Saudi Arabia, 2Department of Dental Materials, Islamic International Dental College,
Riphah International University, Islamabad, Pakistan, 3Department of Oral Biology, Sindh
Institute of Oral Health Sciences, Jinnah Sindh Medical University, Karachi, Pakistan,
4
Department of Oral and Maxillofacial Surgery, Riyadh Elm University, Riyadh, Saudi
Arabia, 5Adult Restorative Dentistry, Dental Biomaterials and Prosthodontics Oman
Dental College, Muscat, Sultanate of Oman, 6Department of Science of Dental Materials,
Dow Dental College, Dow University of Health Sciences, Karachi, Pakistan, 7Department
of Prosthodontics and Dental Implantology, College of Dentistry, King Faisal University,
Al-Ahsa, Saudi Arabia, 8Biomedical and Electrical Engineering Department, School of
Engineering, University of Bradford, Bradford, United Kingdom, 9Interdisciplinary
Research Centre in Polymer Science and Technology (IRC Polymer), University of
Bradford, Bradford, United Kingdom
Chapter Outline
2.1 Introduction 8
2.2 Optical properties (color)
2.3 Thermal properties 9
2.3.1
2.3.2
2.3.3
2.3.4
2.3.5
2.3.6
2.3.7
2.4
2.5
2.6
2.7
2.8
8
Temperature 9
Transition temperatures 9
Heat of fusion (L) 11
Thermal conductivity (K) 12
Specific heat (Cp) 13
Thermal diffusivity (Δ) 13
Coefficient of thermal expansion (α) 14
Viscosity 14
Electrical conductivity and resistivity 15
Mechanical properties and characterization methods
Limitation of mechanical testing methods 22
Biological properties 22
2.8.1
2.8.2
2.8.3
2.8.4
Biocompatibility 22
In vitro testing 23
In vivo testing 24
Usage tests 24
2.9 Toxicity and cytotoxicity
24
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00002-5
Copyright © 2019 Elsevier Ltd. All rights reserved.
16
8
Advanced Dental Biomaterials
2.10 Cytotoxicity tests 26
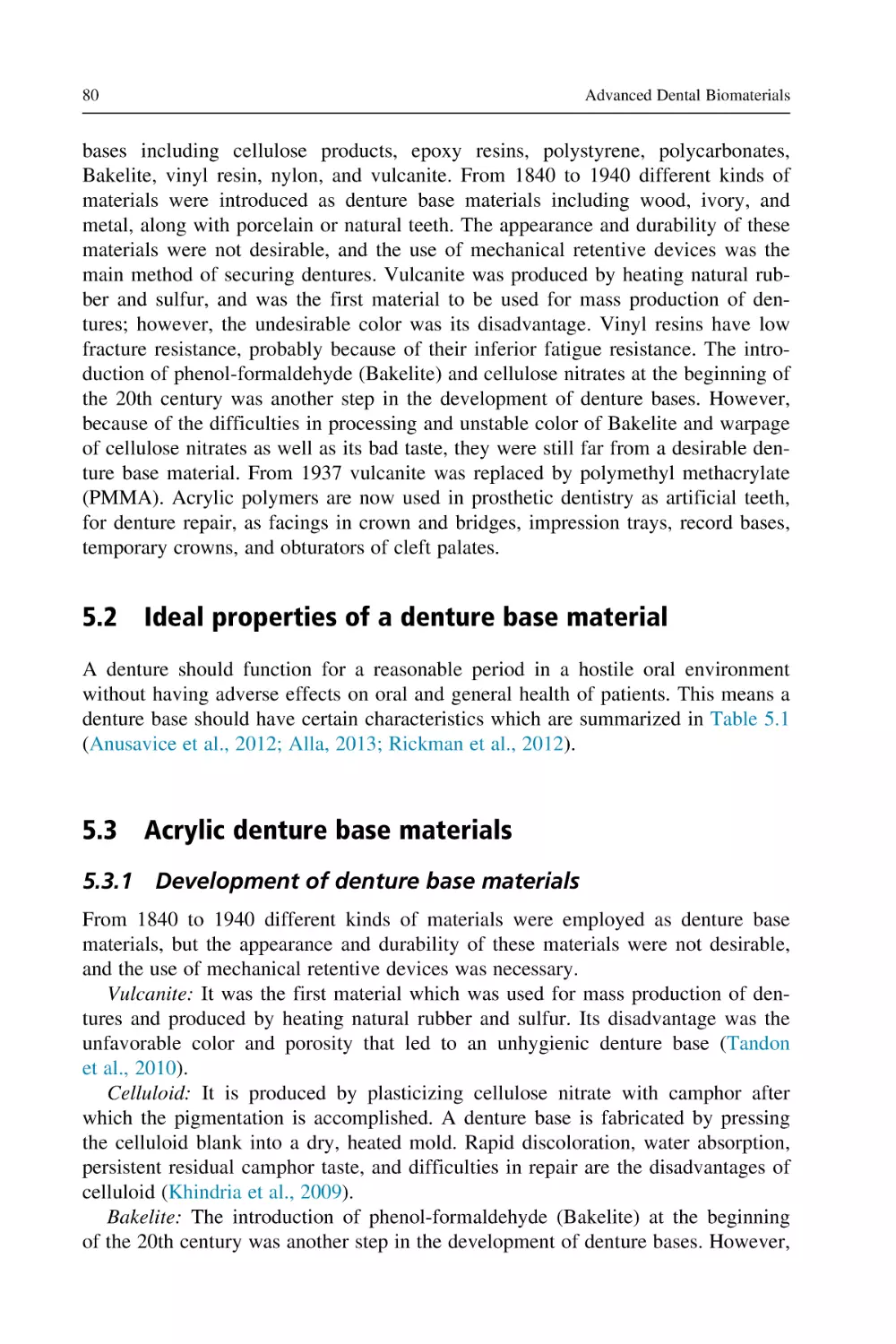
2.11 Fluoride and caries 26
2.11.1 Fluoride toxicity 27
2.12 Carcinogenicity 27
2.13 Biodegradation 28
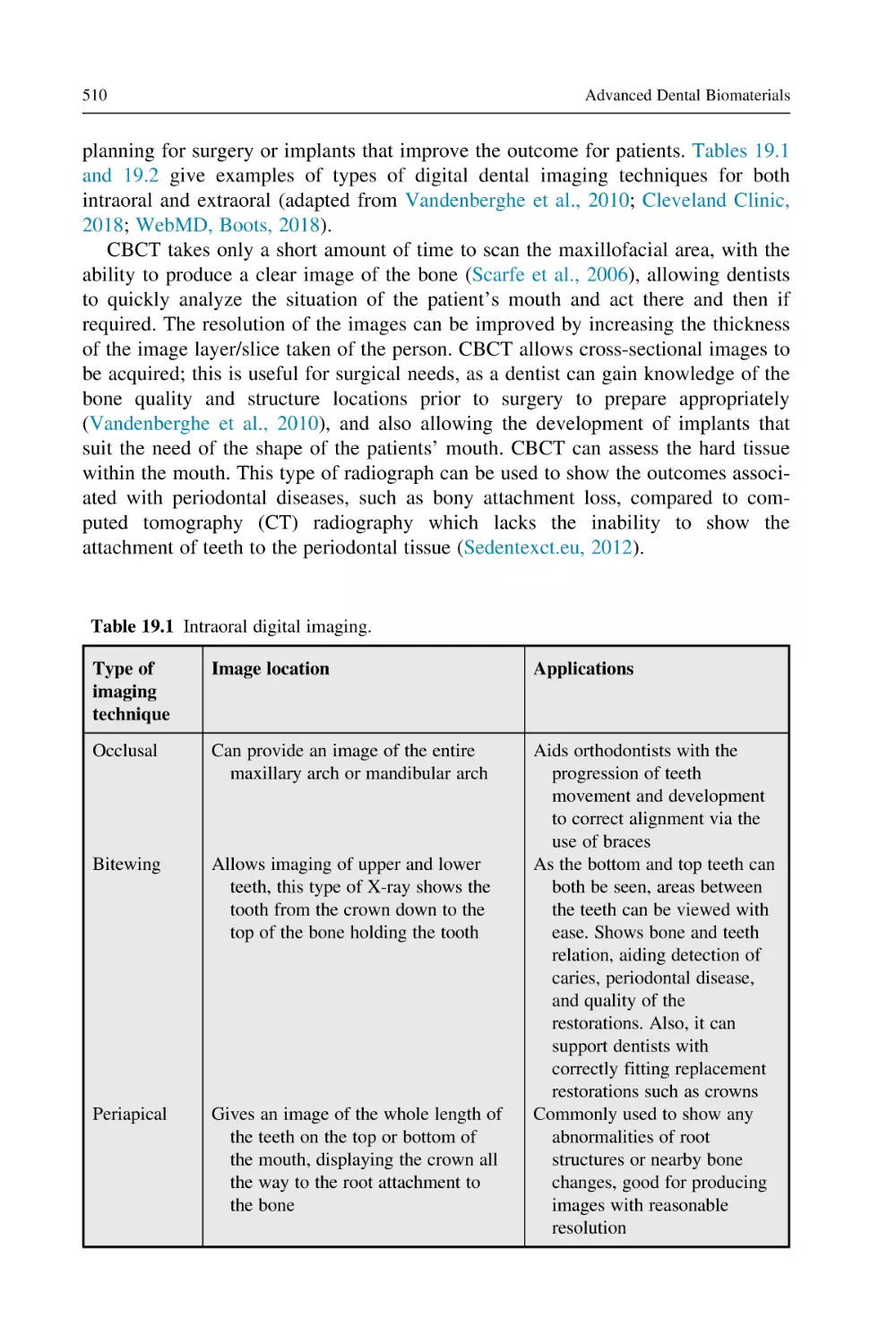
2.14 Bioactivity 28
2.15 Osseointegration 29
2.16 Osteoinduction 29
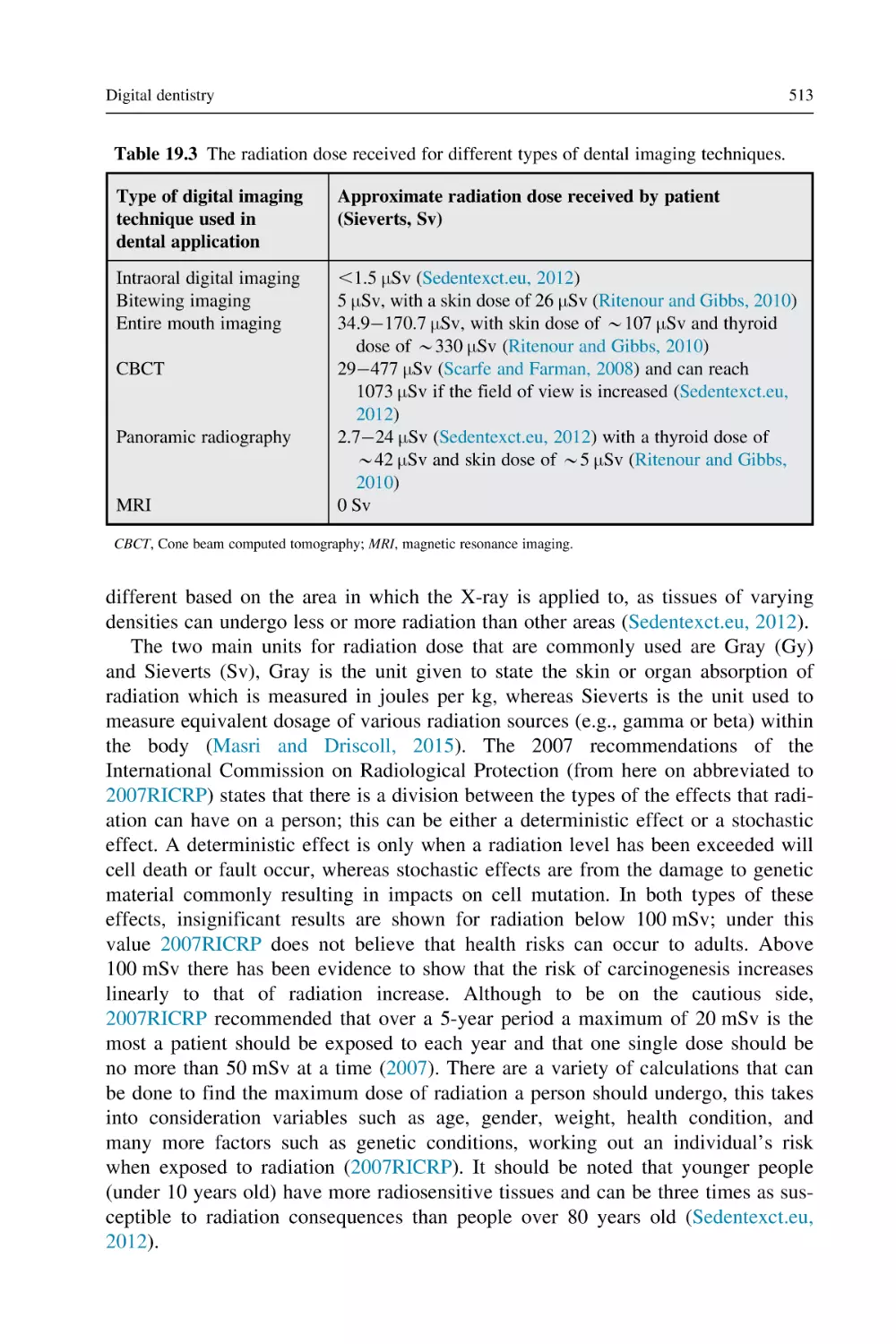
2.17 Foreign body reaction 29
2.18 Conclusive remarks 30
References 30
2.1
Introduction
Understanding the properties of dental biomaterials is important in order to compare
with the properties of oral hard and soft tissues prior to any clinical application.
Various dental restorations tend to fail due to a number of reasons such as distortion
or mechanical failure. The dental restorations are sometimes incompatible with the
supporting oral tissues due to the interface or substrate failure. Although no dental
biomaterial has been reported as having ideal properties to date, but it is worth
mentioning that the performance and clinical success of dental biomaterials is
strongly associated with their properties. In this chapter, various physical, mechanical, and biological properties of dental biomaterials and related interaction are
discussed.
2.2
Optical properties (color)
Color is perceived as an end result of the sensory response to light (Costa, 2016).
The physiological stimuli or sensory response is experienced by an individual,
whereas the light beam is considered as the physical stimuli which produce the sensory response. Color is perceived due to reflection or transmission (partial or complete) of white light. According to Grassmann’s law, the normal eye can
differentiate in three color parameters, which are dominant wavelengths, luminous
reflectance, and the excitation purity (Mausfeld, 1998; Grassmann, 1853). The dominant wavelength (λ) is the wavelength of a monochromatic light which on combination with achromatic color (gray) matches the perceived color (Klein and
Meyrath, 2010). Light with short (400 nm) and long (700 nm) wavelengths are violet and red in color, respectively (Klein and Meyrath, 2010). The wavelength range
of visible light (400700 nm) corresponds to specific colors (e.g., blue, green, yellow, and orange). This property of color that is distinguished by light’s wavelength
is called “hue.” Among all the colors and shades, there are only three primary colors i.e., red, green, and blue. These three colors when used in appropriate
Properties of dental biomaterials
9
proportions can produce different colors, for example, yellow color can be produced
by an appropriate combination of green and red.
The second parameter is luminous reflectance of color (value), which classifies
objects equivalent to a series of achromatic scale (López Camelo and Gómez,
2004). For the light diffusing objects, it ranges from black to white. While in the
case of transmitting objects, it ranges from black to clear or colorless. The black is
specified as a standard with luminous reflectance of 0 and the white assigned as
100. The third component (saturation of color, also called “Chroma”) defines the
degree of difference from achromatic color toward the color spectrum; it numerically ranges from 0 to 1 (Sakaguchi and Powers, 2012).
2.3
Thermal properties
Thermal properties are important in regulating the performance of dental materials.
At the molecular level, the structural arrangement and movements of atoms are
affected as a function of temperature variations. Therefore it is necessary to have an
understanding of different thermal techniques used to identify thermal properties of
dental materials.
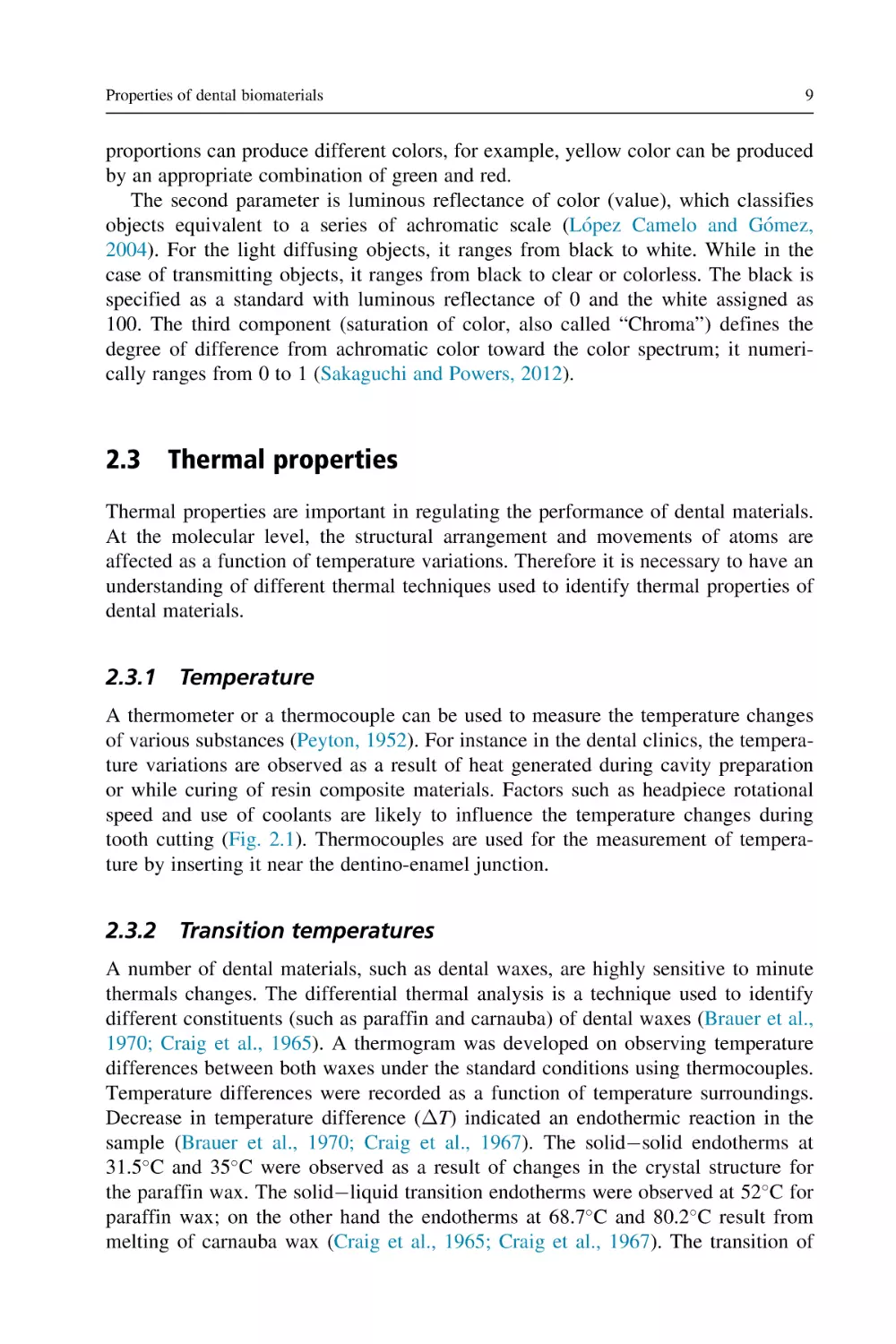
2.3.1 Temperature
A thermometer or a thermocouple can be used to measure the temperature changes
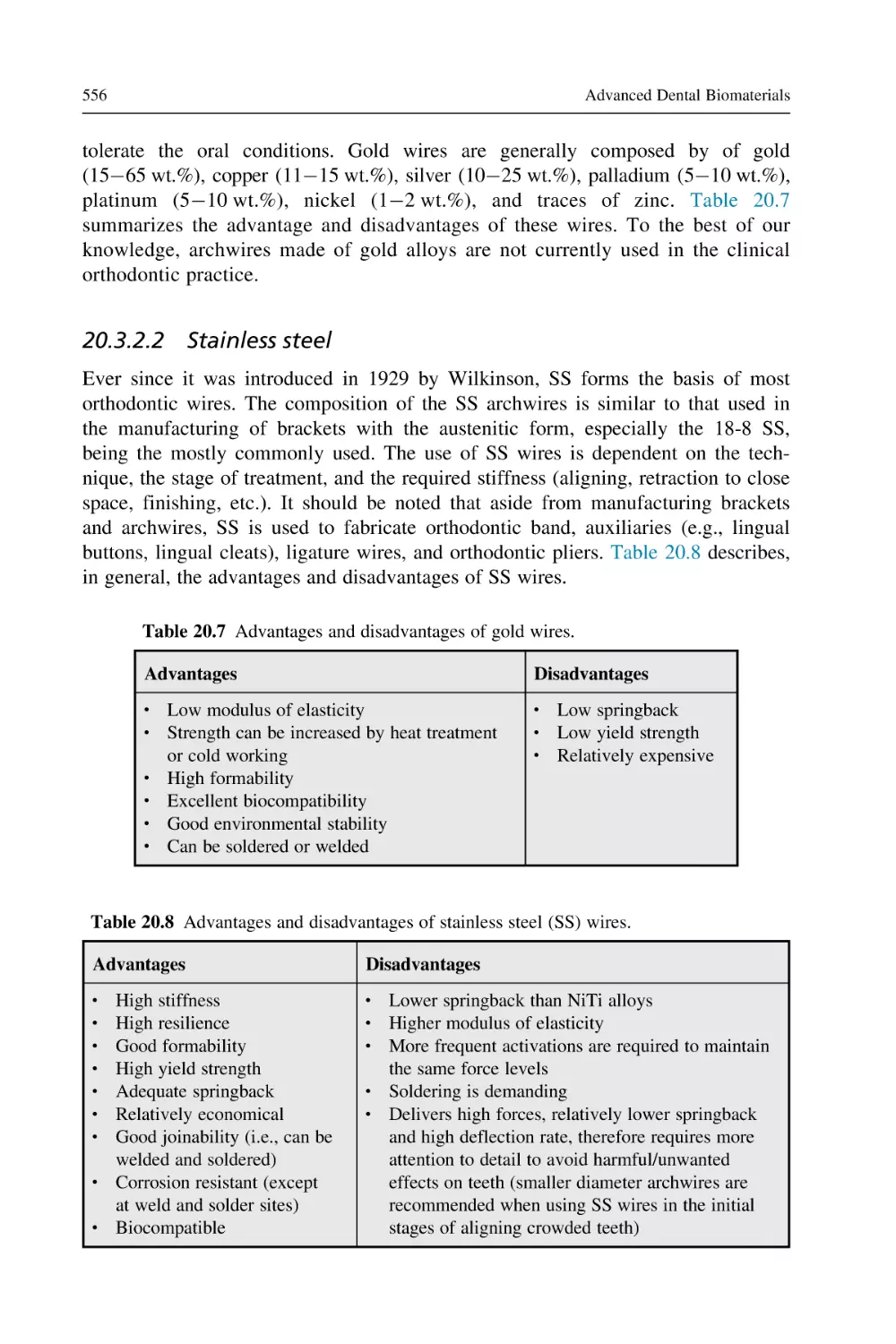
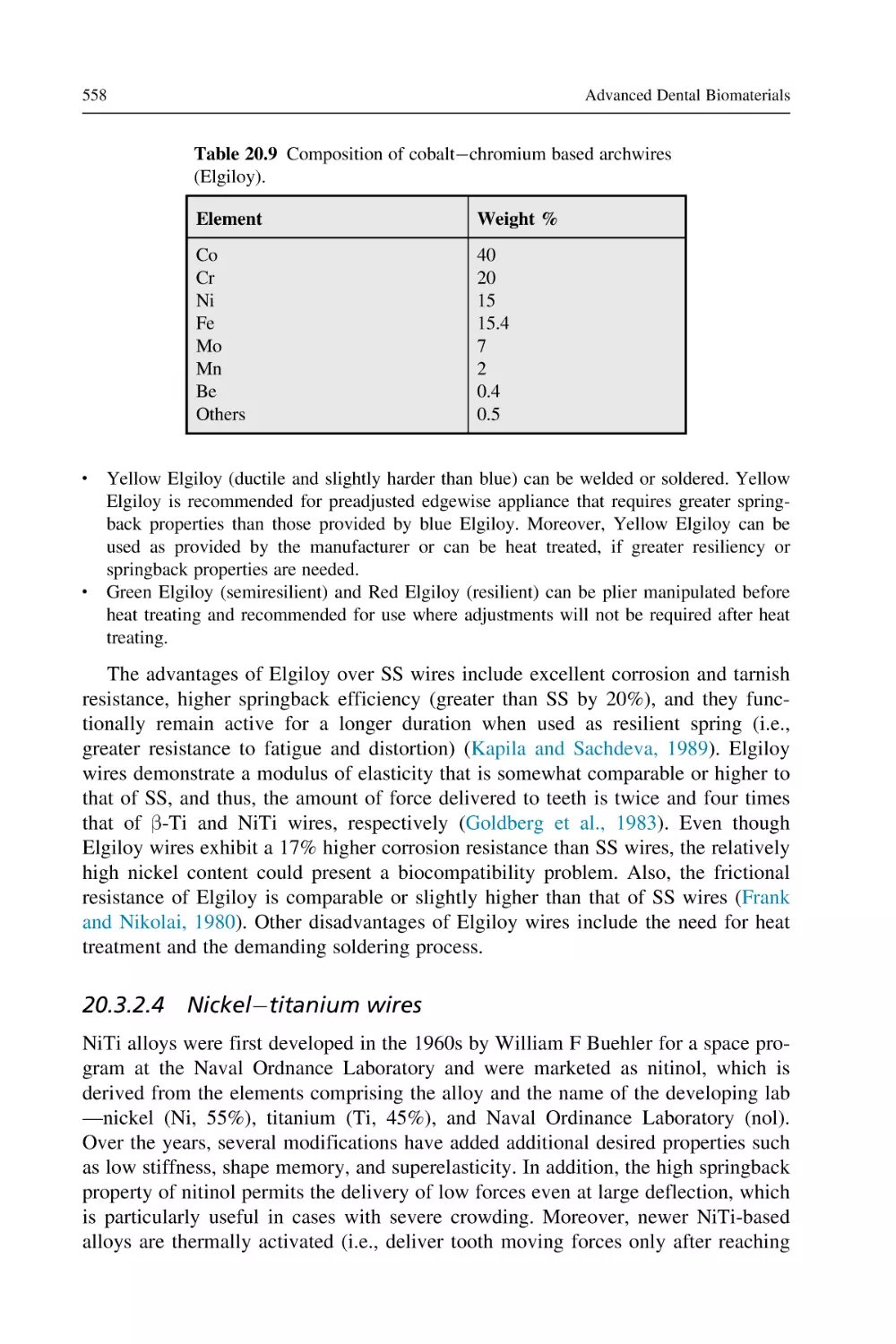
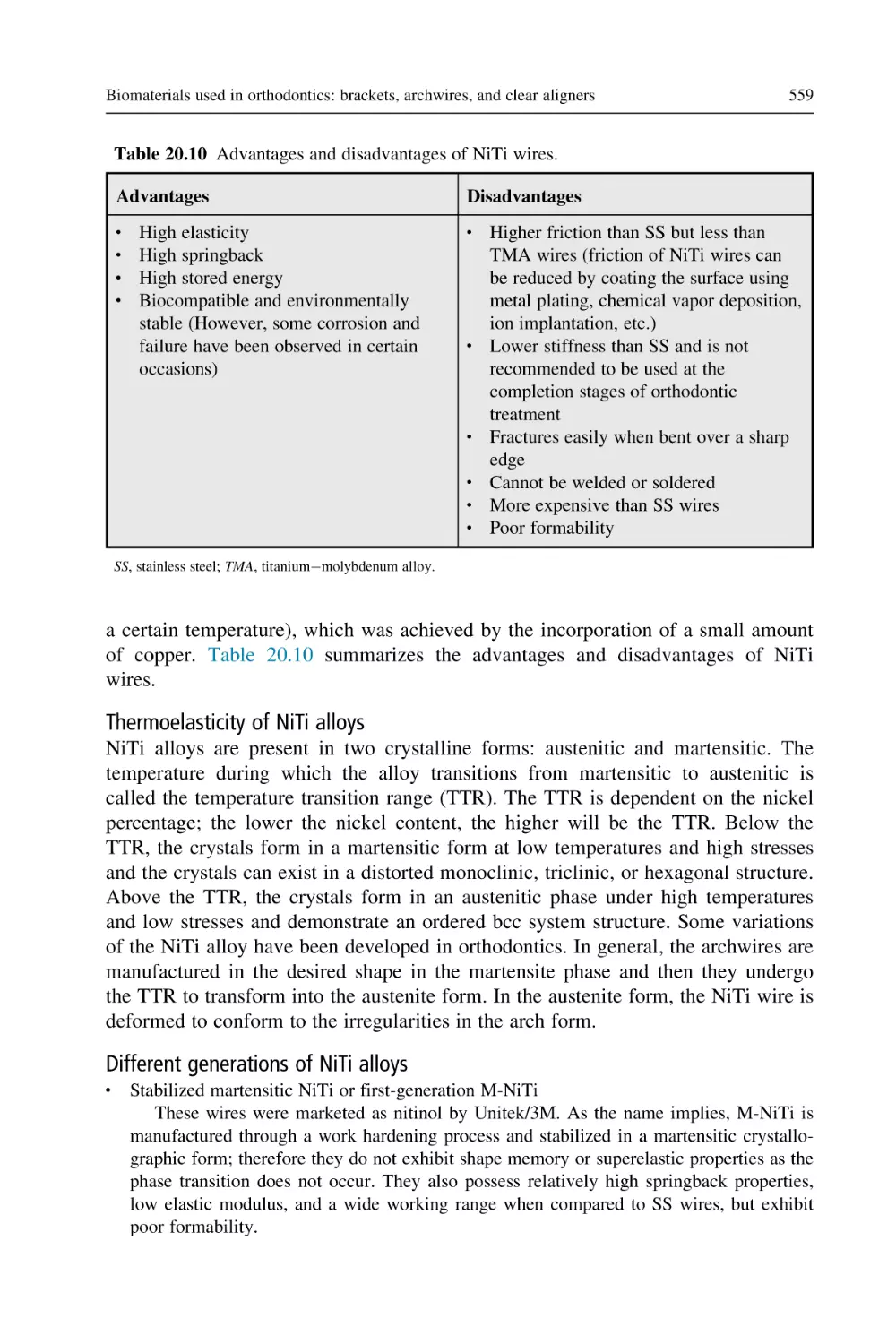
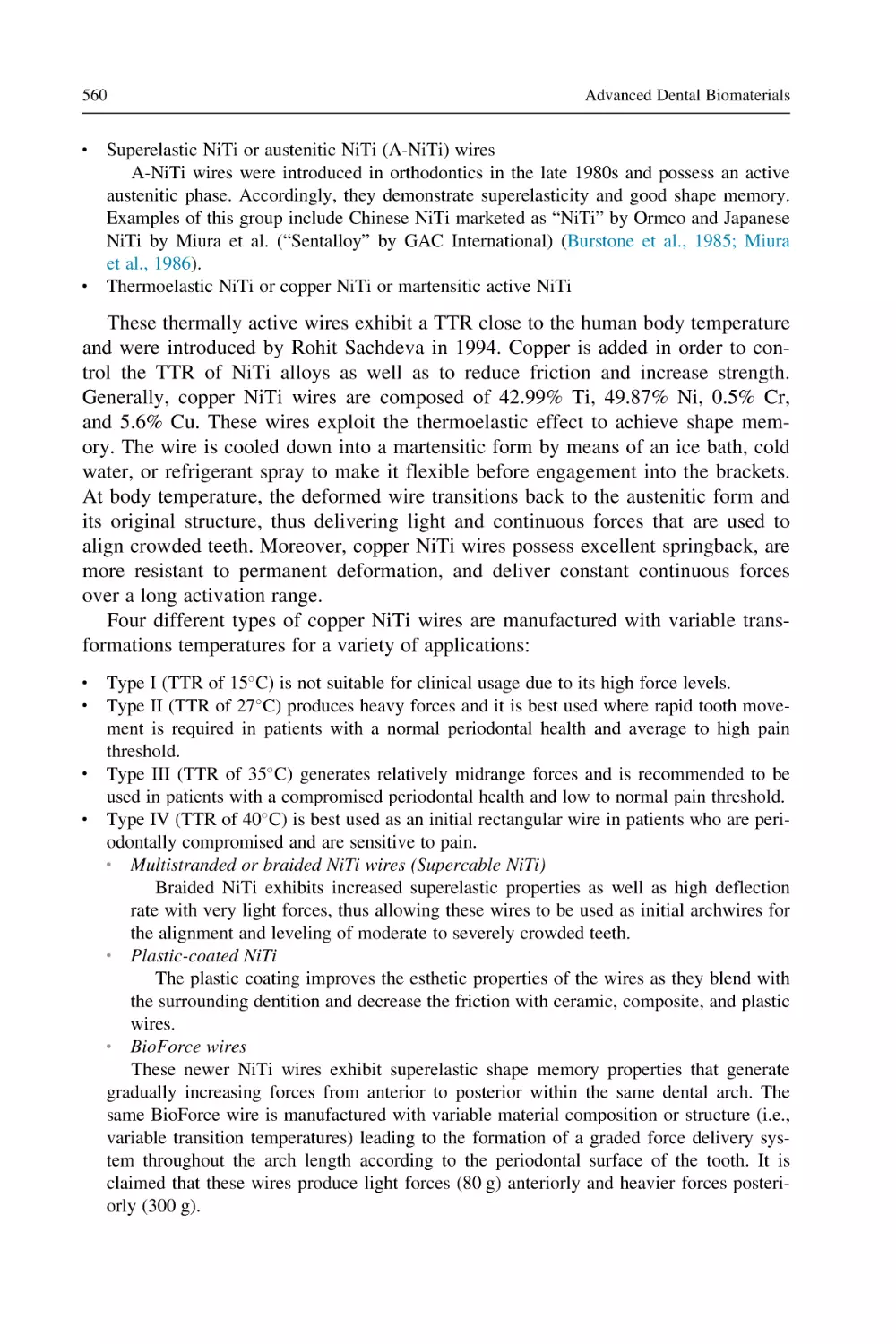
of various substances (Peyton, 1952). For instance in the dental clinics, the temperature variations are observed as a result of heat generated during cavity preparation
or while curing of resin composite materials. Factors such as headpiece rotational
speed and use of coolants are likely to influence the temperature changes during
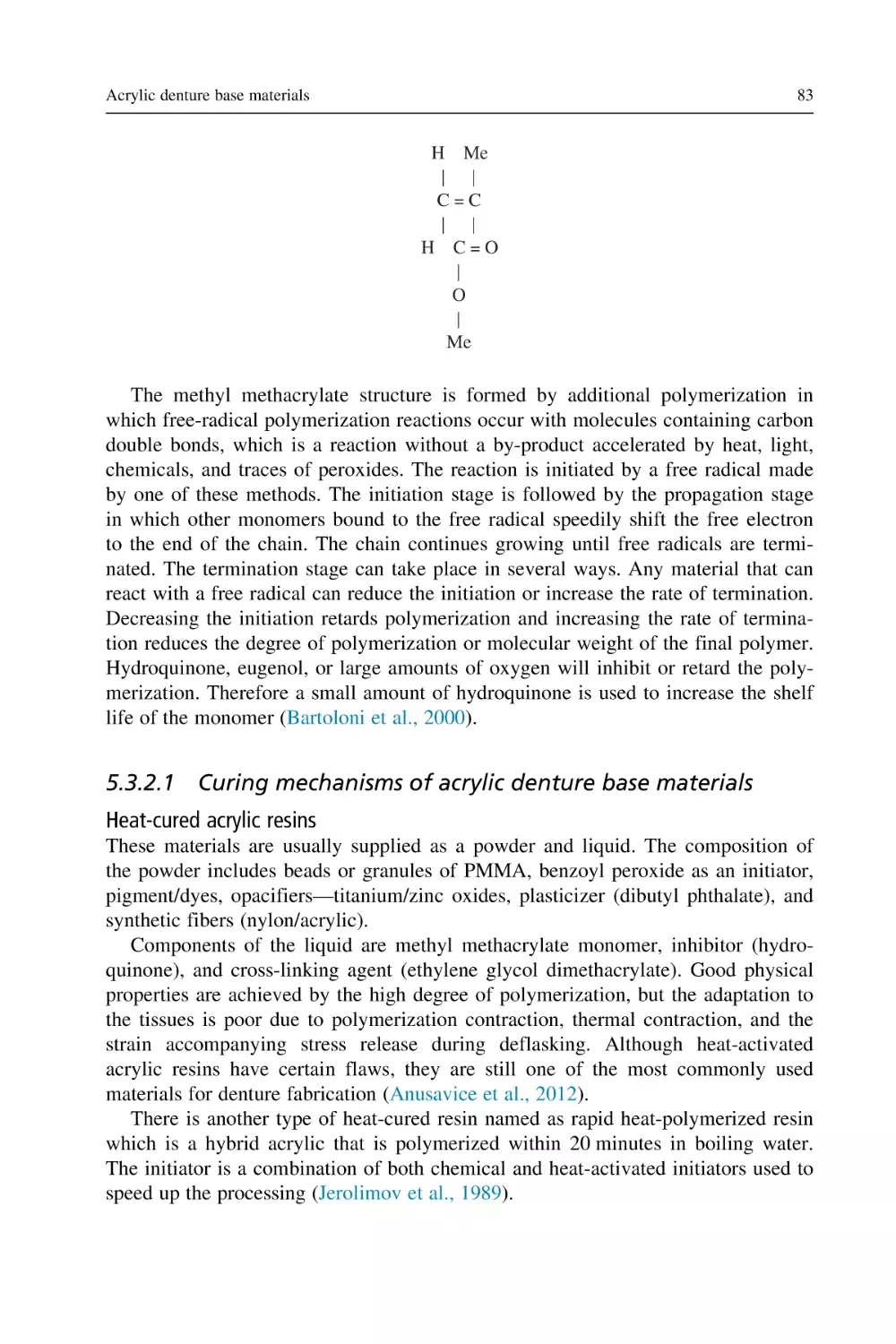
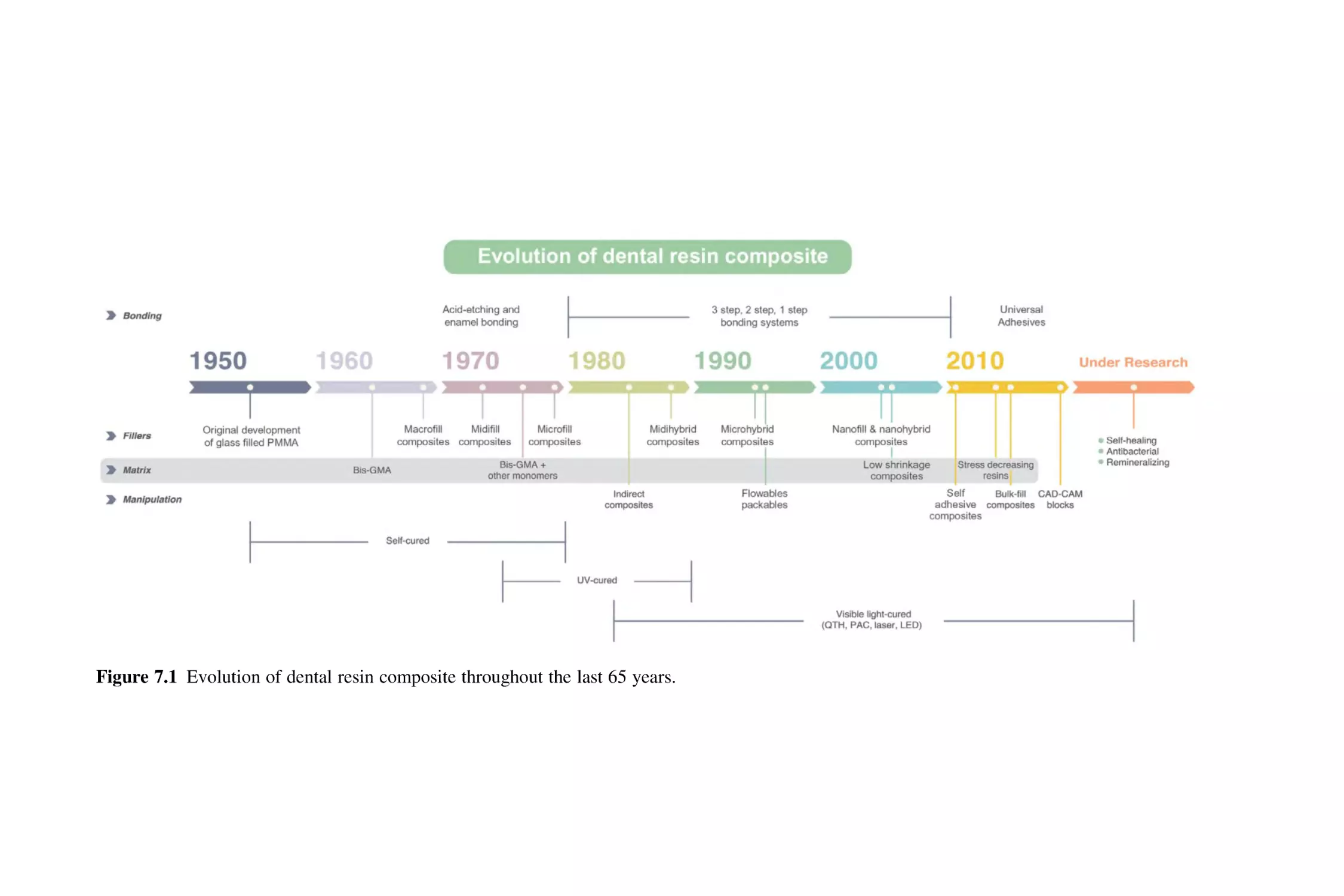
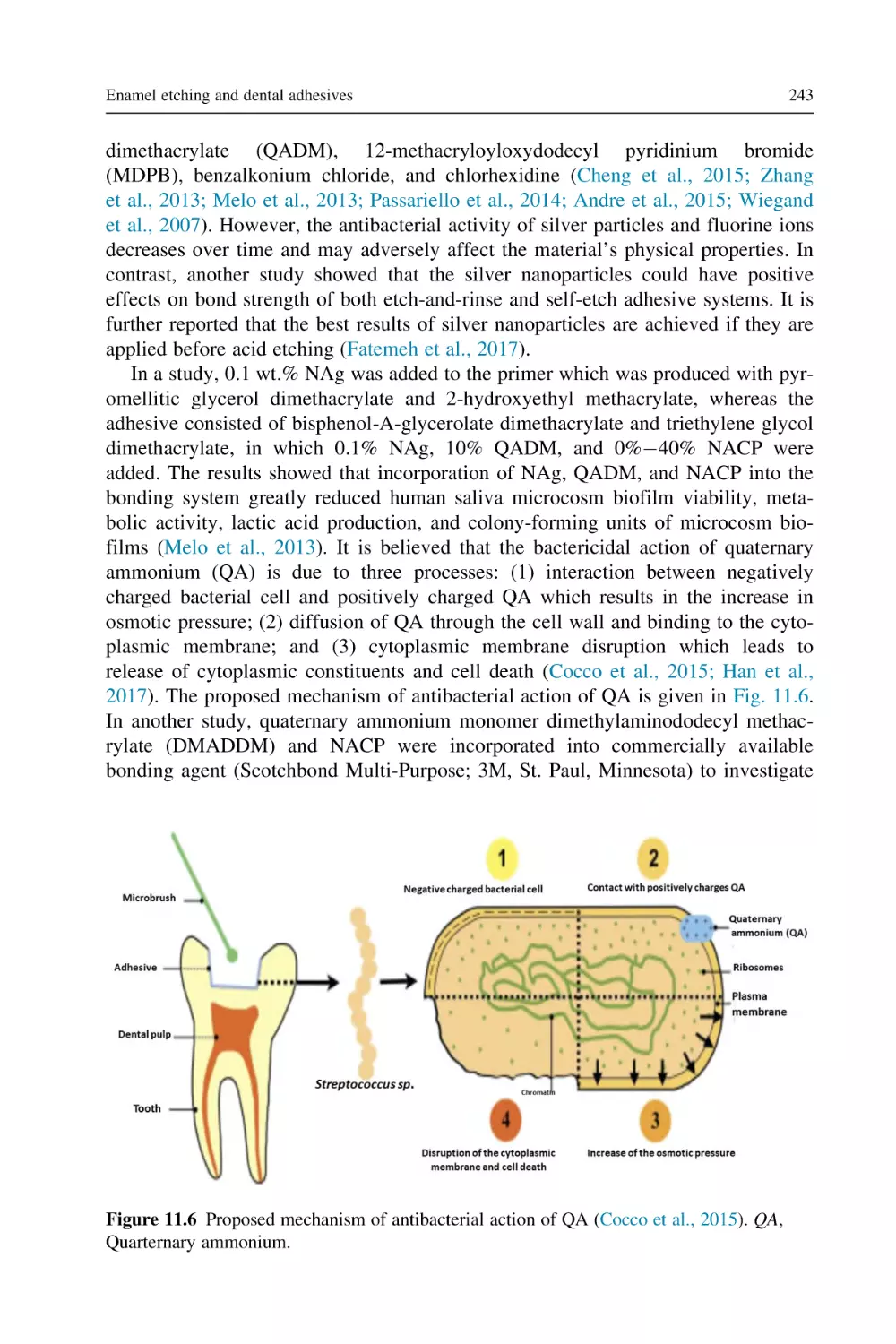
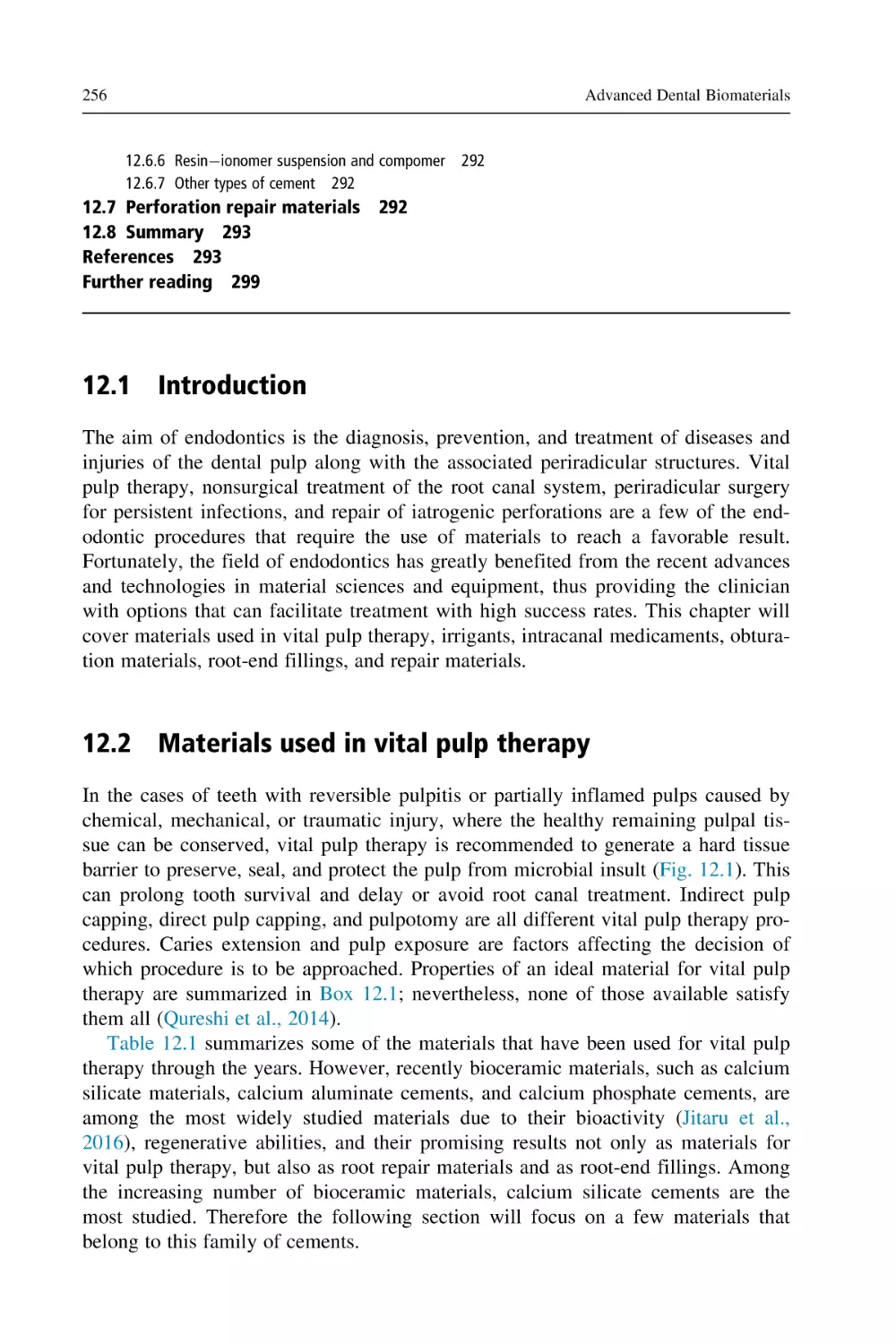
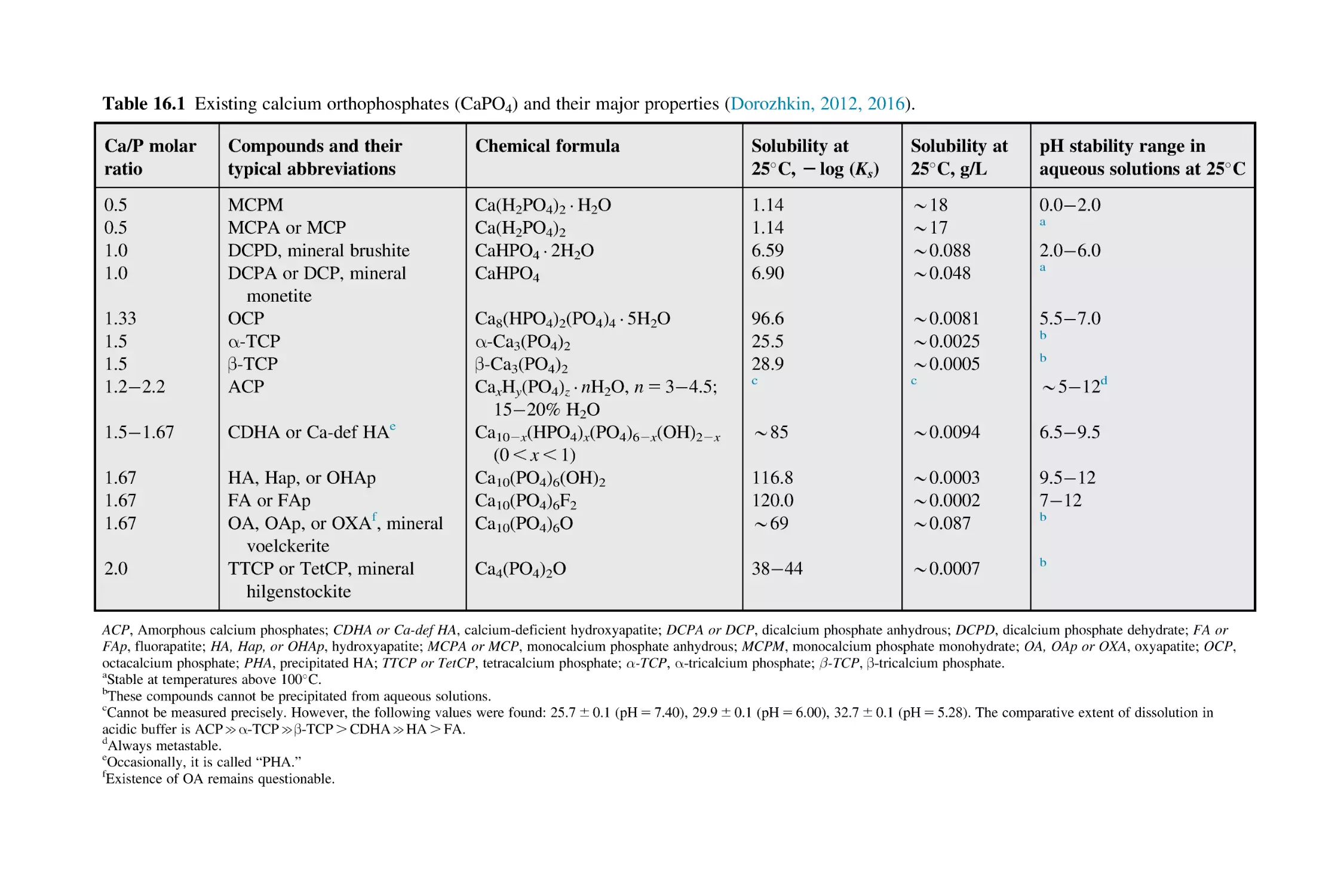
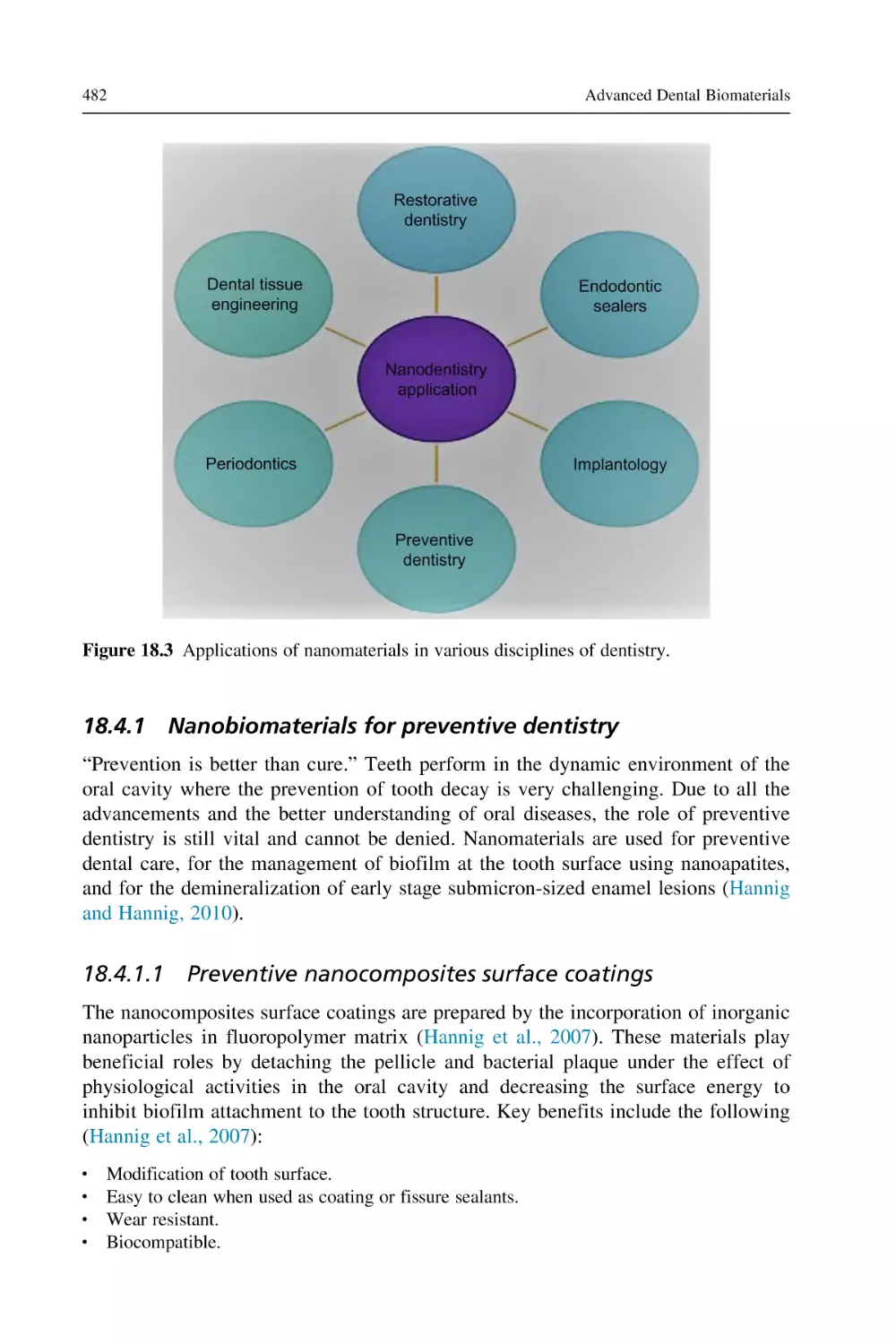
tooth cutting (Fig. 2.1). Thermocouples are used for the measurement of temperature by inserting it near the dentino-enamel junction.
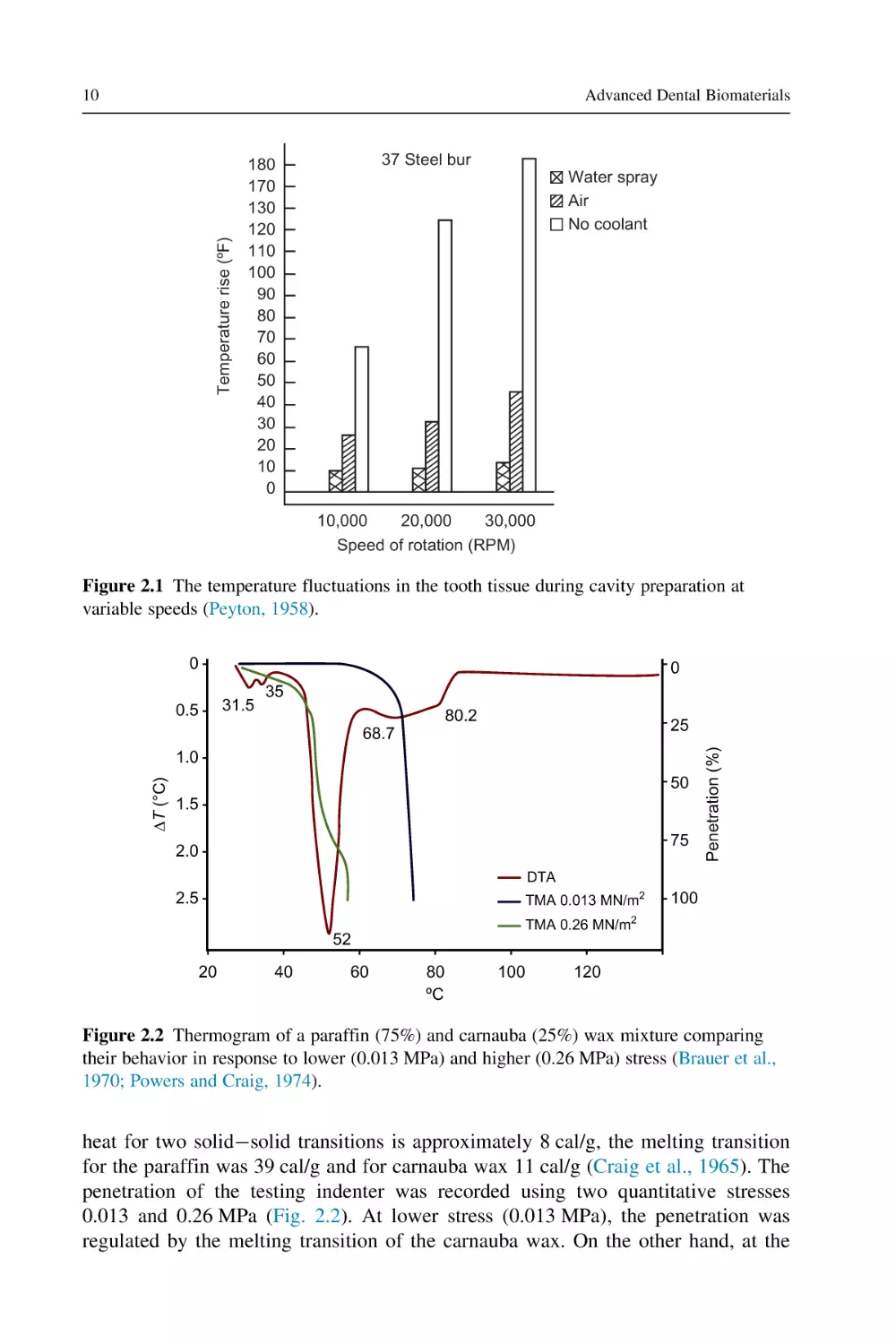
2.3.2 Transition temperatures
A number of dental materials, such as dental waxes, are highly sensitive to minute
thermals changes. The differential thermal analysis is a technique used to identify
different constituents (such as paraffin and carnauba) of dental waxes (Brauer et al.,
1970; Craig et al., 1965). A thermogram was developed on observing temperature
differences between both waxes under the standard conditions using thermocouples.
Temperature differences were recorded as a function of temperature surroundings.
Decrease in temperature difference (ΔT) indicated an endothermic reaction in the
sample (Brauer et al., 1970; Craig et al., 1967). The solidsolid endotherms at
31.5 C and 35 C were observed as a result of changes in the crystal structure for
the paraffin wax. The solidliquid transition endotherms were observed at 52 C for
paraffin wax; on the other hand the endotherms at 68.7 C and 80.2 C result from
melting of carnauba wax (Craig et al., 1965; Craig et al., 1967). The transition of
Advanced Dental Biomaterials
Temperature rise (ºF)
10
37 Steel bur
180
170
130
120
110
100
90
80
70
60
50
40
30
20
10
0
Water spray
Air
No coolant
10,000
20,000
30,000
Speed of rotation (RPM)
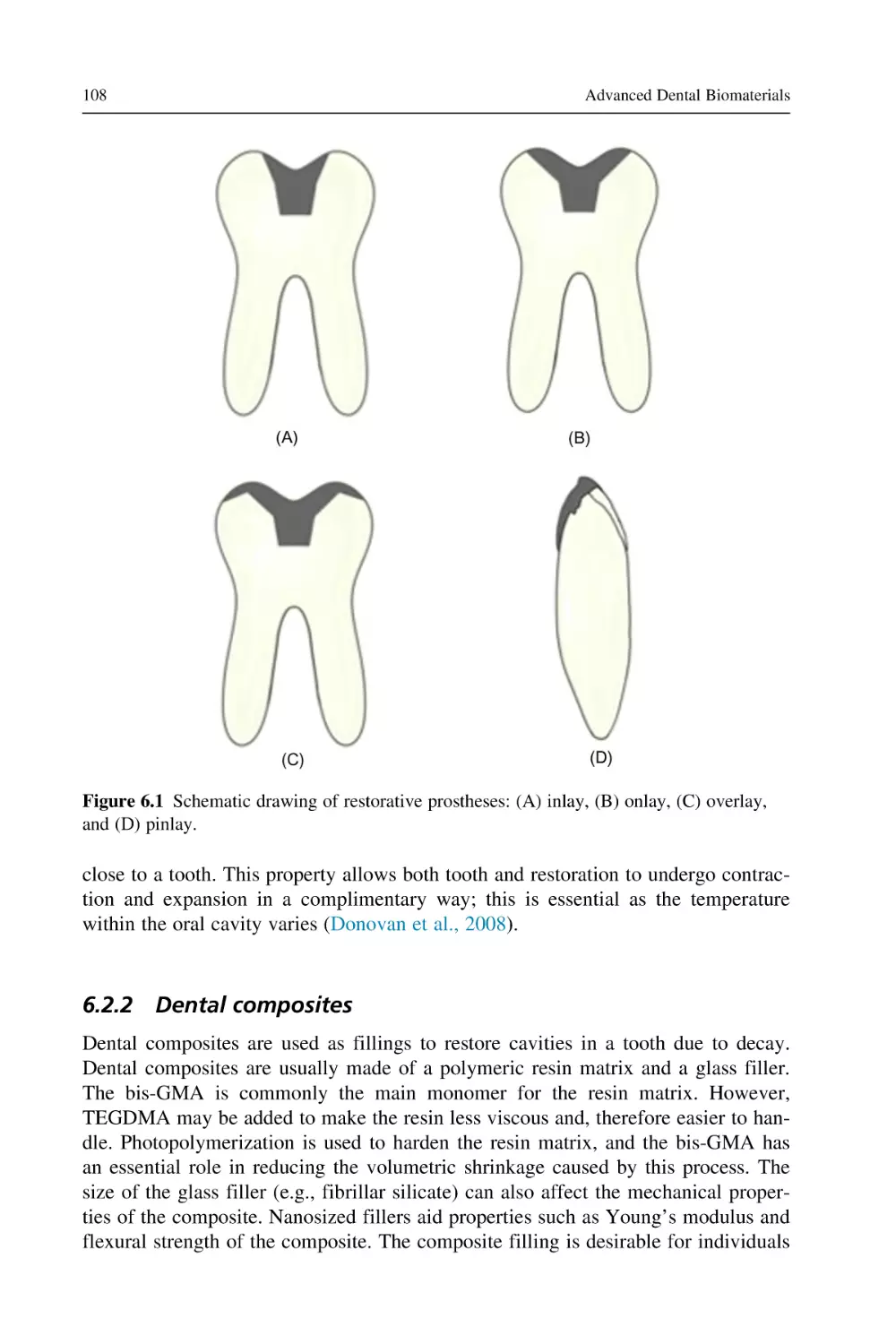
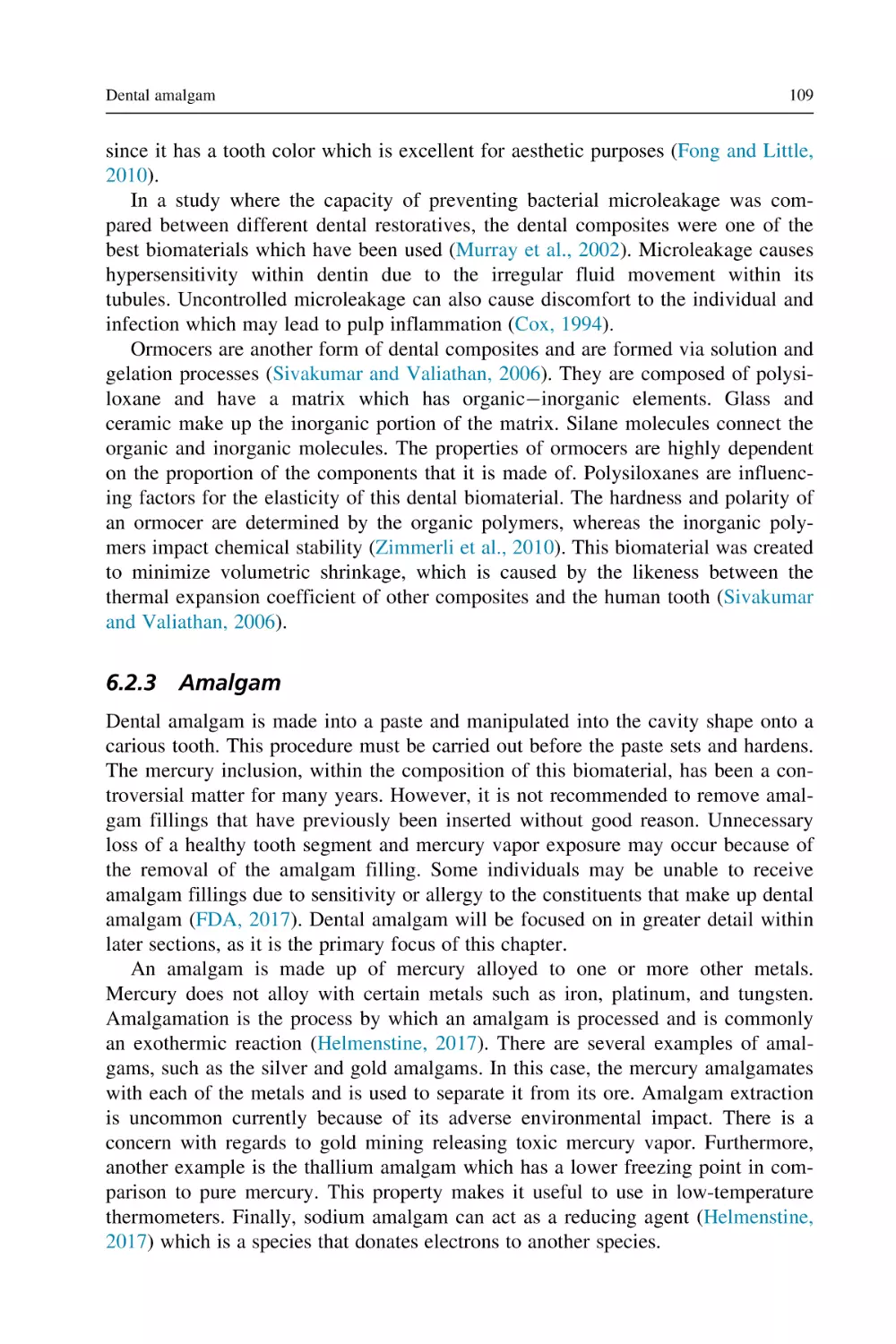
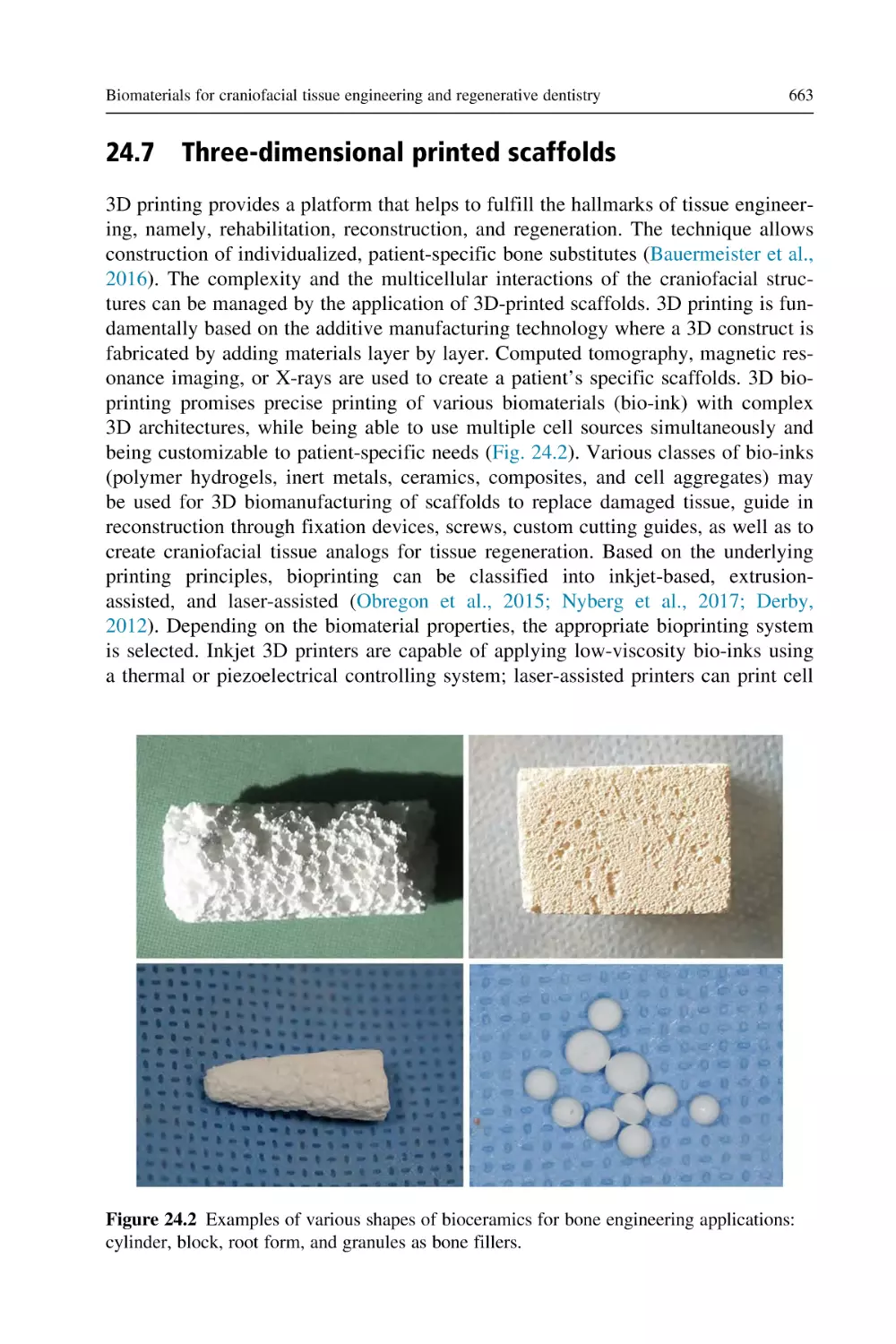
Figure 2.1 The temperature fluctuations in the tooth tissue during cavity preparation at
variable speeds (Peyton, 1958).
0
0
80.2
25
68.7
ΔT (°C)
1.0
50
1.5
75
2.0
Penetration (%)
31.5
0.5
35
DTA
2.5
TMA 0.013 MN/m2
100
2
TMA 0.26 MN/m
52
20
40
60
80
ºC
100
120
Figure 2.2 Thermogram of a paraffin (75%) and carnauba (25%) wax mixture comparing
their behavior in response to lower (0.013 MPa) and higher (0.26 MPa) stress (Brauer et al.,
1970; Powers and Craig, 1974).
heat for two solidsolid transitions is approximately 8 cal/g, the melting transition
for the paraffin was 39 cal/g and for carnauba wax 11 cal/g (Craig et al., 1965). The
penetration of the testing indenter was recorded using two quantitative stresses
0.013 and 0.26 MPa (Fig. 2.2). At lower stress (0.013 MPa), the penetration was
regulated by the melting transition of the carnauba wax. On the other hand, at the
Properties of dental biomaterials
11
higher stress (0.26 MPa), the penetration was facilitated mainly by solidsolid and
solidliquid transitions of paraffin wax. Nearly 44% of the wax penetration
occurred before the melting of paraffin wax, which is corresponding to its flowing
potential (Powers and Craig, 1974).
Another important property correlated with the thermograms is the coefficient of
thermal expansion. This coefficient is raised approximately from 300 3 1026/ C to
1400 3 1026/ C prior to solidsolid transition. The property of flow is also
observed to increase in this temperature range.
The dynamic mechanical analysis is another technique in order to analyze the
thermal properties of a material. For this purpose, a thin film of di-methacrylate
copolymer is subjected to tensile strain at a specific frequency of 11 Hz (Wilson
and Turner, 1987). The elastic modulus and loss of tangent are obtained by raising
the temperature. The glass transition temperature (Tg) is measured from the
decrease of elastic modulus with temperature changes. The Tg determines the temperature at which polymer is transformed to a softer, rubbery state on heating
(Wilson and Turner, 1987). The lower value of glass transition temperature can be
affected by the lower degree of alteration of double bonds, less cross-linking, and
better flexibility of networks. The coefficient of thermal expansion of a polymer is
altered at the glass transition temperature.
2.3.3 Heat of fusion (L)
The heat in calories (Cal) or Joules (J) which is required for conversion of 1 g of
material from the solid phase to the liquid phase (melting temperature) is referred
to as heat of fusion. The heat of fusion can be calculated by
L5
Q
m
where L is the heat of fusion, Q refers to the total amount of heat absorbed, and m
refers to the mass of the substance being melted. Thus, practically, the mass of material is directly proportional to the heat required in changing the total mass to liquid.
The heat of fusion of a material is correlated with melting or freezing. For the change
in the state from a solid mass to liquefaction it is important to add heat, as long the
heat of fusion is retained by the liquid, the mass remains molten. As soon as the heat
is liberated from the liquid state the material solidifies. The difference in the energy
content is of key importance in order to maintain the kinetic molecular motion, an
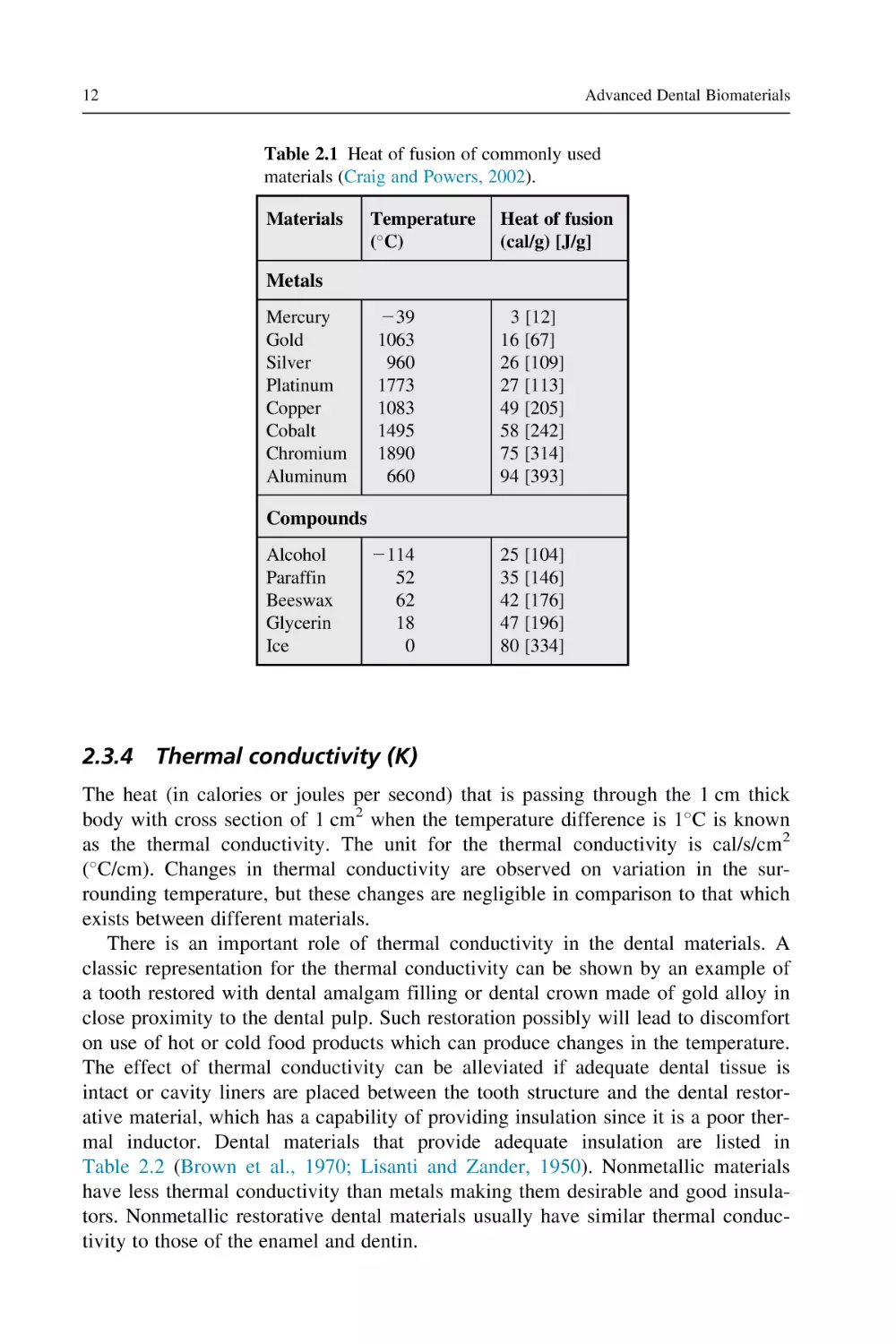
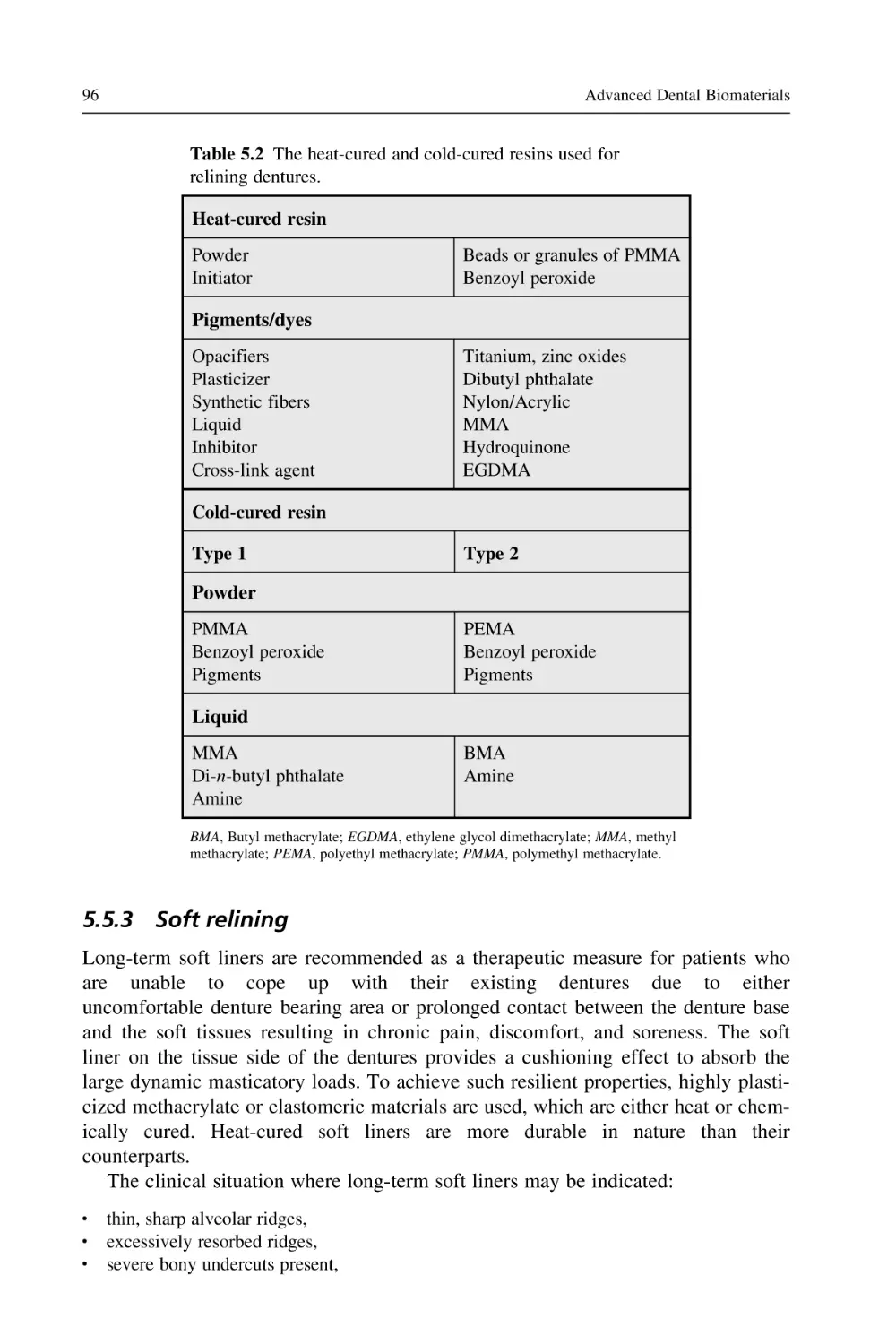
important property of a material in a liquid state. The heat of fusion values for commonly used materials are listed in the Table 2.1 (Craig and Powers, 2002). It can be
observed from Table 2.1 that the values for dental alloys, particularly silver, gold,
and copper, are lower than that of many other alloys and metals.
12
Advanced Dental Biomaterials
Table 2.1 Heat of fusion of commonly used
materials (Craig and Powers, 2002).
Materials
Temperature
( C)
Heat of fusion
(cal/g) [J/g]
Metals
Mercury
Gold
Silver
Platinum
Copper
Cobalt
Chromium
Aluminum
239
1063
960
1773
1083
1495
1890
660
3 [12]
16 [67]
26 [109]
27 [113]
49 [205]
58 [242]
75 [314]
94 [393]
2114
52
62
18
0
25 [104]
35 [146]
42 [176]
47 [196]
80 [334]
Compounds
Alcohol
Paraffin
Beeswax
Glycerin
Ice
2.3.4 Thermal conductivity (K)
The heat (in calories or joules per second) that is passing through the 1 cm thick
body with cross section of 1 cm2 when the temperature difference is 1 C is known
as the thermal conductivity. The unit for the thermal conductivity is cal/s/cm2
( C/cm). Changes in thermal conductivity are observed on variation in the surrounding temperature, but these changes are negligible in comparison to that which
exists between different materials.
There is an important role of thermal conductivity in the dental materials. A
classic representation for the thermal conductivity can be shown by an example of
a tooth restored with dental amalgam filling or dental crown made of gold alloy in
close proximity to the dental pulp. Such restoration possibly will lead to discomfort
on use of hot or cold food products which can produce changes in the temperature.
The effect of thermal conductivity can be alleviated if adequate dental tissue is
intact or cavity liners are placed between the tooth structure and the dental restorative material, which has a capability of providing insulation since it is a poor thermal inductor. Dental materials that provide adequate insulation are listed in
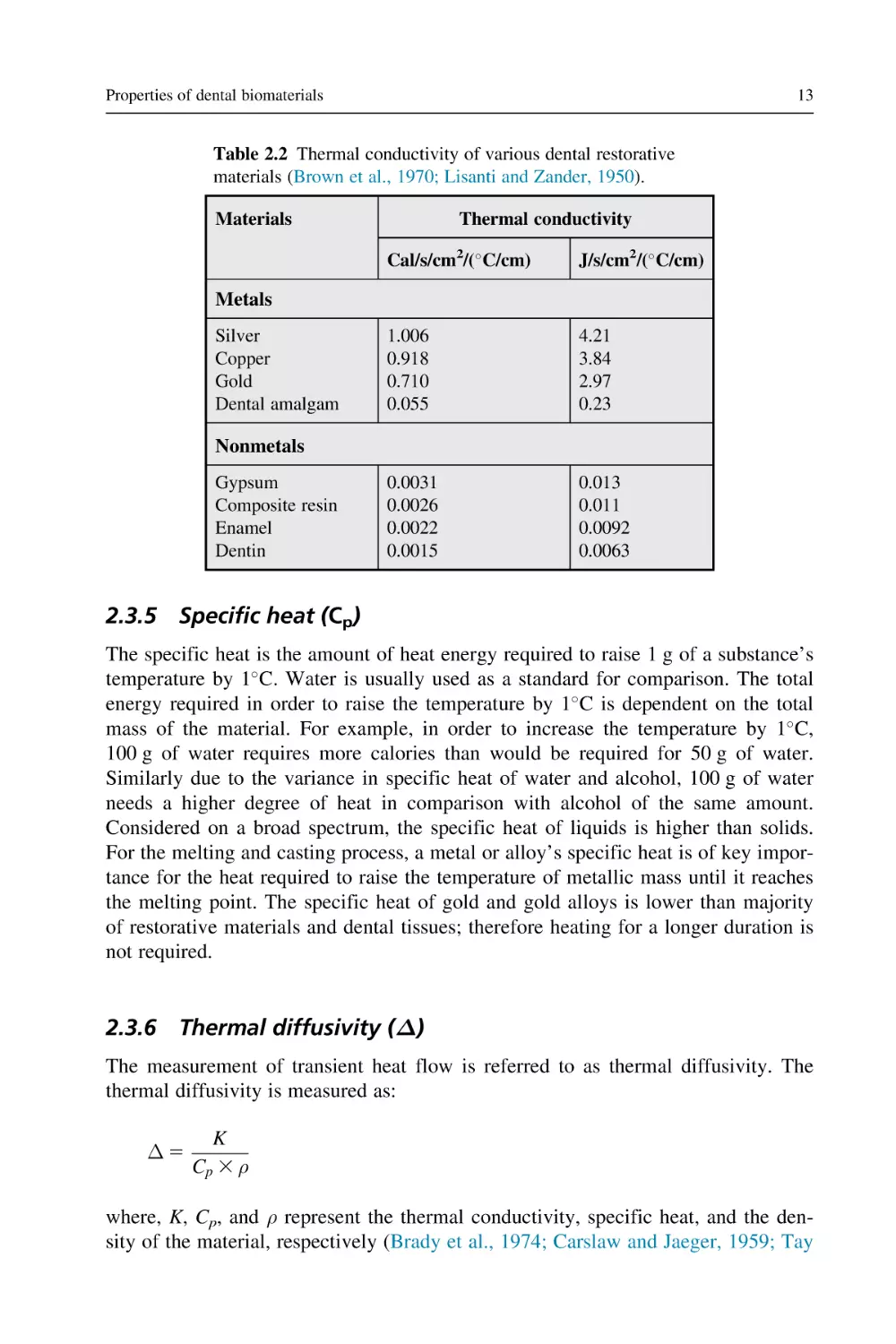
Table 2.2 (Brown et al., 1970; Lisanti and Zander, 1950). Nonmetallic materials
have less thermal conductivity than metals making them desirable and good insulators. Nonmetallic restorative dental materials usually have similar thermal conductivity to those of the enamel and dentin.
Properties of dental biomaterials
13
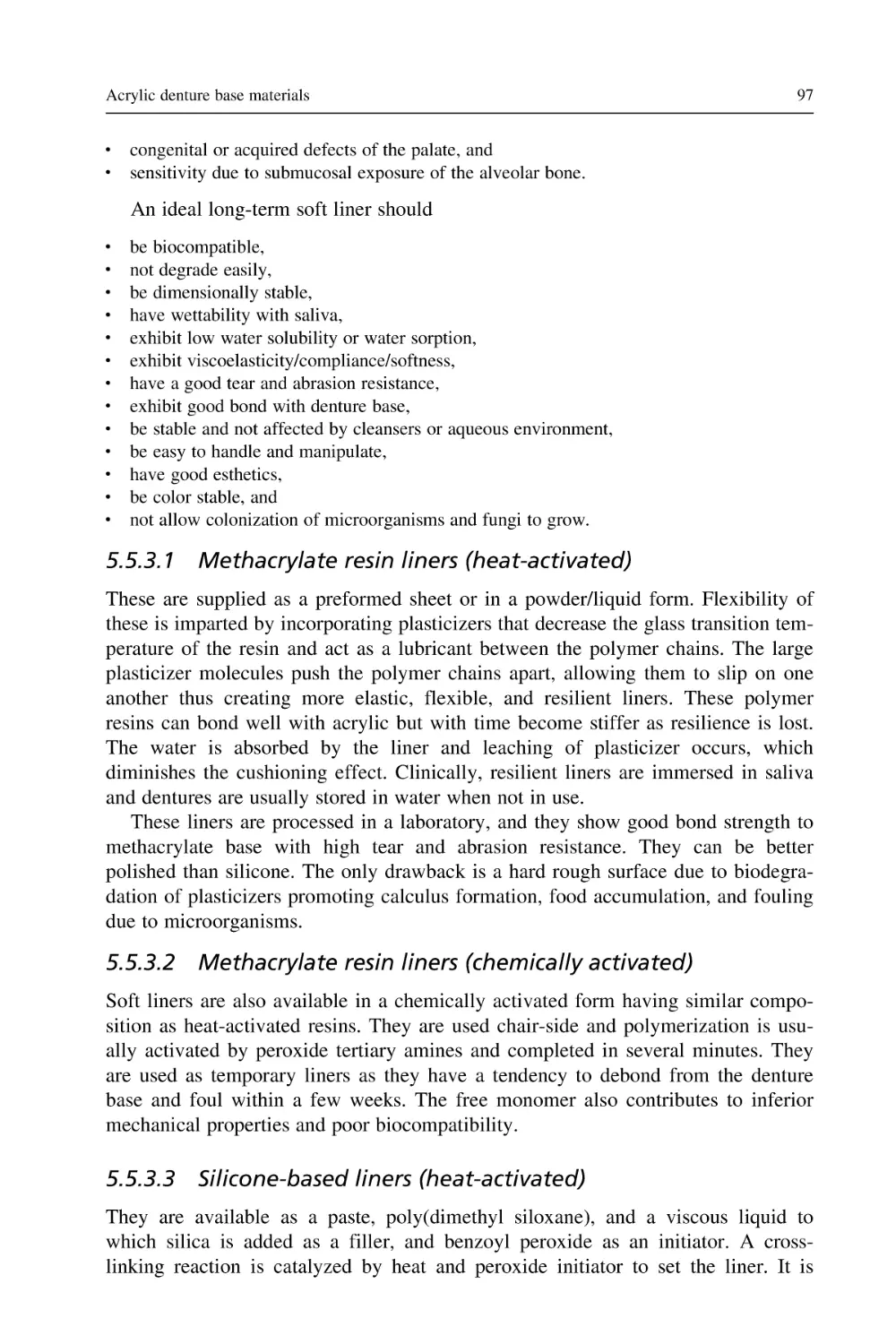
Table 2.2 Thermal conductivity of various dental restorative
materials (Brown et al., 1970; Lisanti and Zander, 1950).
Materials
Thermal conductivity
Cal/s/cm2/( C/cm)
J/s/cm2/( C/cm)
1.006
0.918
0.710
0.055
4.21
3.84
2.97
0.23
0.0031
0.0026
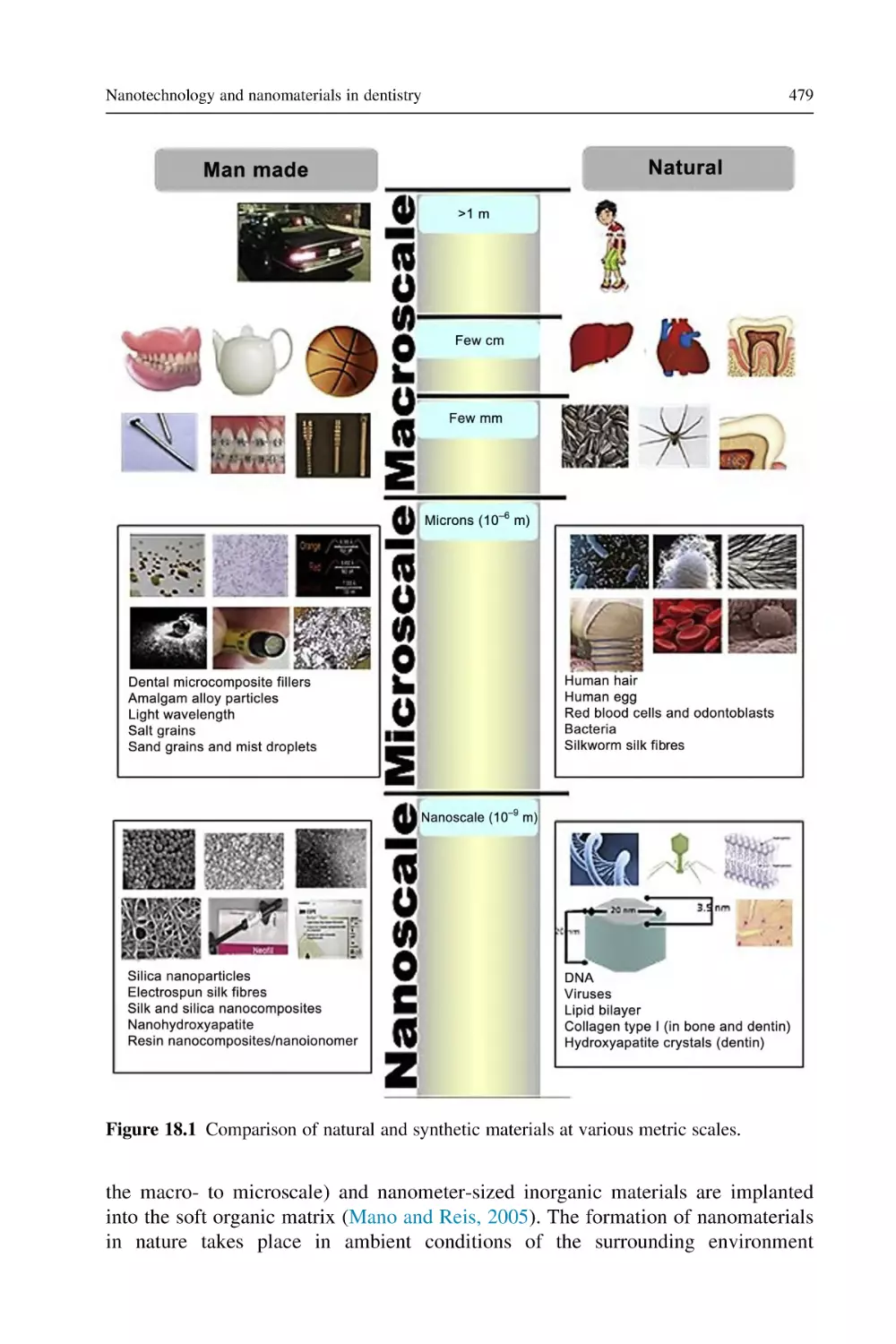
0.0022
0.0015
0.013
0.011
0.0092
0.0063
Metals
Silver
Copper
Gold
Dental amalgam
Nonmetals
Gypsum
Composite resin
Enamel
Dentin
2.3.5 Specific heat (Cp)
The specific heat is the amount of heat energy required to raise 1 g of a substance’s
temperature by 1 C. Water is usually used as a standard for comparison. The total
energy required in order to raise the temperature by 1 C is dependent on the total
mass of the material. For example, in order to increase the temperature by 1 C,
100 g of water requires more calories than would be required for 50 g of water.
Similarly due to the variance in specific heat of water and alcohol, 100 g of water
needs a higher degree of heat in comparison with alcohol of the same amount.
Considered on a broad spectrum, the specific heat of liquids is higher than solids.
For the melting and casting process, a metal or alloy’s specific heat is of key importance for the heat required to raise the temperature of metallic mass until it reaches
the melting point. The specific heat of gold and gold alloys is lower than majority
of restorative materials and dental tissues; therefore heating for a longer duration is
not required.
2.3.6 Thermal diffusivity (Δ)
The measurement of transient heat flow is referred to as thermal diffusivity. The
thermal diffusivity is measured as:
Δ5
K
Cp 3 ρ
where, K, Cp, and ρ represent the thermal conductivity, specific heat, and the density of the material, respectively (Brady et al., 1974; Carslaw and Jaeger, 1959; Tay
14
Advanced Dental Biomaterials
and Braden, 1987). The unit for the thermal diffusivity is mm2/s. The gold crown
or amalgam restorations have high thermal conductivity and low specific heat and
are likely to cause potent thermal shock in comparison with the normal tooth structure. Similar to thermal conductivity, the material thickness is important in regulating the thermal diffusivity (Brady et al., 1974).
2.3.7 Coefficient of thermal expansion (α)
The coefficient of thermal expansion is referred to as dimensional changes in a
material per unit for the change by 1 C in temperature (Fairhurst et al., 1980).
The coefficient of thermal expansion can be calculated using the following
equation:
α5
ðLfinal 2 Loriginal Þ
½Loriginal 3 Cfinal 2 Coriginal
The units for thermal expansion are expressed as the notation / C as the values
are small and they are therefore generally used in exponential form, for example,
12 3 1026/ C (Fairhurst et al., 1980).
2.4
Viscosity
The fluid viscosity is observed to have a direct relation with the shear rate; it
increases with increasing shear rate. The proportionality of the viscosity varies for
different fluids. The viscosity of the fluids may vary according to the shear rate;
therefore fluid can further be classified as Newtonian, pseudoplastic, or dilatant.
The Newtonian fluids are reported to have constant viscosity which is independent
of its shear rate. Classic examples for Newtonian fluids are dental cements and
impression materials. For the pseudoplastic fluid the viscosity decreases with an
increasing shear rate. The best example for the pseudoplastics is the monophase
elastomeric materials (Combe and Moser, 1978). These materials tend to have high
viscosity therefore on mixing or while placing the impression material containing
tray into the mouth, it remains in its place without flowing (Herfort et al., 1977).
Elastomeric materials can be used in syringes as they encounter higher shear rates
while passing through the syringe tip. On exiting the syringe the viscosity decreases
by 10-fold (Herfort et al., 1977). This property of material is referred to as thixotropy, although the term “thixotropy” particularly defines the alterations in the viscosity of a material with time. A material whose viscosity increases with increasing
shear rate is referred to as a dilatant fluid. In dentistry, a classic example for dilatant fluids is the denture base resins (Vermilyea et al., 1978).
Properties of dental biomaterials
2.5
15
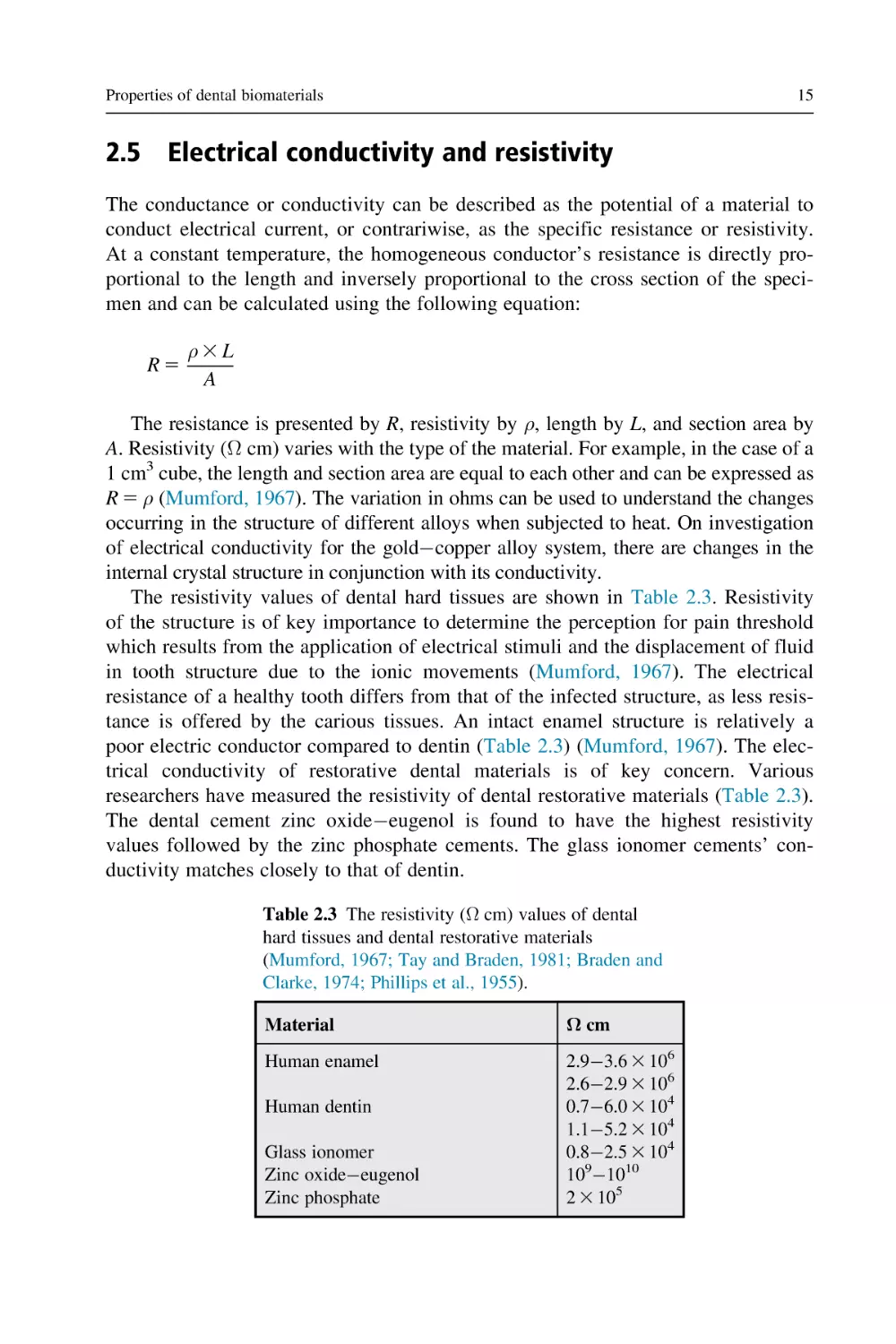
Electrical conductivity and resistivity
The conductance or conductivity can be described as the potential of a material to
conduct electrical current, or contrariwise, as the specific resistance or resistivity.
At a constant temperature, the homogeneous conductor’s resistance is directly proportional to the length and inversely proportional to the cross section of the specimen and can be calculated using the following equation:
R5
ρ3L
A
The resistance is presented by R, resistivity by ρ, length by L, and section area by
A. Resistivity (Ω cm) varies with the type of the material. For example, in the case of a
1 cm3 cube, the length and section area are equal to each other and can be expressed as
R 5 ρ (Mumford, 1967). The variation in ohms can be used to understand the changes
occurring in the structure of different alloys when subjected to heat. On investigation
of electrical conductivity for the goldcopper alloy system, there are changes in the
internal crystal structure in conjunction with its conductivity.
The resistivity values of dental hard tissues are shown in Table 2.3. Resistivity
of the structure is of key importance to determine the perception for pain threshold
which results from the application of electrical stimuli and the displacement of fluid
in tooth structure due to the ionic movements (Mumford, 1967). The electrical
resistance of a healthy tooth differs from that of the infected structure, as less resistance is offered by the carious tissues. An intact enamel structure is relatively a
poor electric conductor compared to dentin (Table 2.3) (Mumford, 1967). The electrical conductivity of restorative dental materials is of key concern. Various
researchers have measured the resistivity of dental restorative materials (Table 2.3).
The dental cement zinc oxideeugenol is found to have the highest resistivity
values followed by the zinc phosphate cements. The glass ionomer cements’ conductivity matches closely to that of dentin.
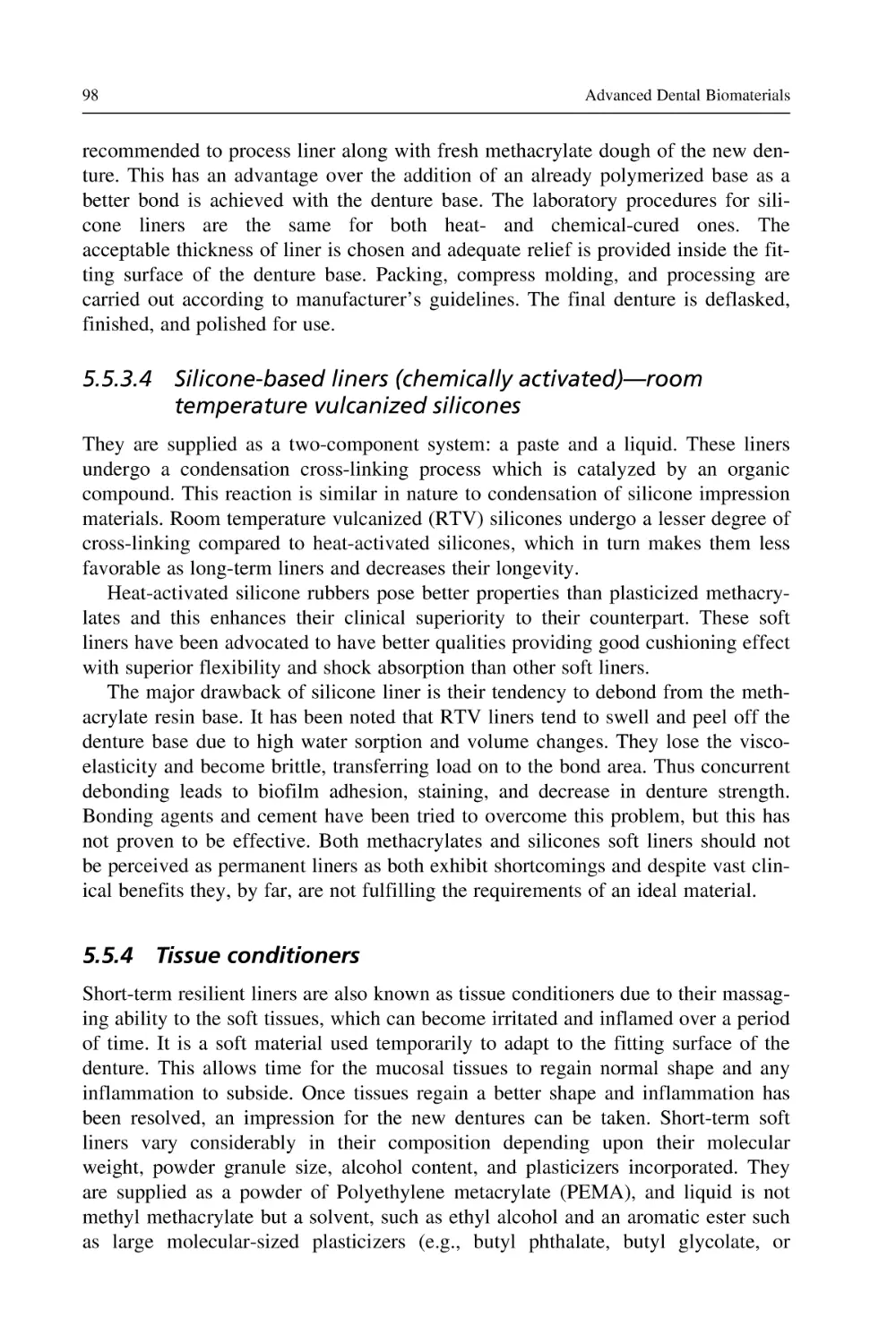
Table 2.3 The resistivity (Ω cm) values of dental
hard tissues and dental restorative materials
(Mumford, 1967; Tay and Braden, 1981; Braden and
Clarke, 1974; Phillips et al., 1955).
Material
Ω cm
Human enamel
2.93.6 3 106
2.62.9 3 106
0.76.0 3 104
1.15.2 3 104
0.82.5 3 104
1091010
2 3 105
Human dentin
Glass ionomer
Zinc oxideeugenol
Zinc phosphate
16
2.6
Advanced Dental Biomaterials
Mechanical properties and characterization methods
The vibrant human oral atmosphere is able to influence the dental biomaterials used
for tooth restoration. One of the key requirements of dental materials is to match
the properties of the tooth structure which are required in a particular application
(Tillberg et al., 2008). In order to identify the appropriate mechanical properties relevant to a particular use various test methods are employed. Therefore, an understanding of mechanical properties allows to distinguish the potential causes of
clinical deficiencies related to the mechanical failure of dental materials under oral
load. The basic parameter to determine mechanical behavior is to understand the
stressstrain relationship for deformation (Vaderhobli, 2011). Mechanical properties determine the resistance fracture or deformation under an applied force or pressure. Analysis of mechanical properties will help to understand the failure and
longevity of dental materials in the dynamic oral environment under various types
of stresses and forces (De Jager et al., 2006).
The mechanical behavior of a material is mainly related to the response to a
force or load (Zafar and Ahmed, 2014b,c) and this behavior ultimately decides the
usefulness of a material in a specific application. The mechanical testing and characterization are usually carried out according to existing standards set by various
international organizations such as american dental association (ADA), the British
Standards, or the Federation Dentaire Internationale (McCabe and Walls, 2008).
One of the main purposes of these standards is to provide the technical information
regarding an unbiased and dependable selection process for the materials used by
health care providers. Certain claims of the materials’ quality arise from manufacturers as a result of standard test methodologies for mechanical, physical, chemical,
and biological tests. The mechanical testing performed by the manufacturers to
measure mechanical properties such as compression strength (CS), tensile strength,
flexural strength (FS), wear, modulus, and biocompatibility must be performed
under the specific testing conditions to identify the safest and the most efficient
materials for specific clinical applications (Basu et al., 2010).
The mechanical properties demonstrate how a dental material and the tooth
structure react to the applied forces. Therefore it is important to understand the
application of force or stress and pressure on a material; such forces will change
the shape or structure of the materials if not resisted.
1. Force or pressure: Force is an applied energy to move or to deform a material. During
the normal function and biting, various types of forces are applied on the tooth structure,
alveolar socket, and periodontal complex (Van Noort and Barbour, 2013). For example,
axial, vertical forces, horizontal forces, torsion and bending forces, or any combination
of these forces (Fig. 2.3) are applied to the tooth or materials by the muscles of mastication while biting and through parafunctional habits. External forces due to dental trauma,
orthodontics, and tooth movement are also present. Three characteristics of force determine the outcome of the applied force, that is, the magnitude, the direction, and the point
of application of force and these result in various deformations of the materials
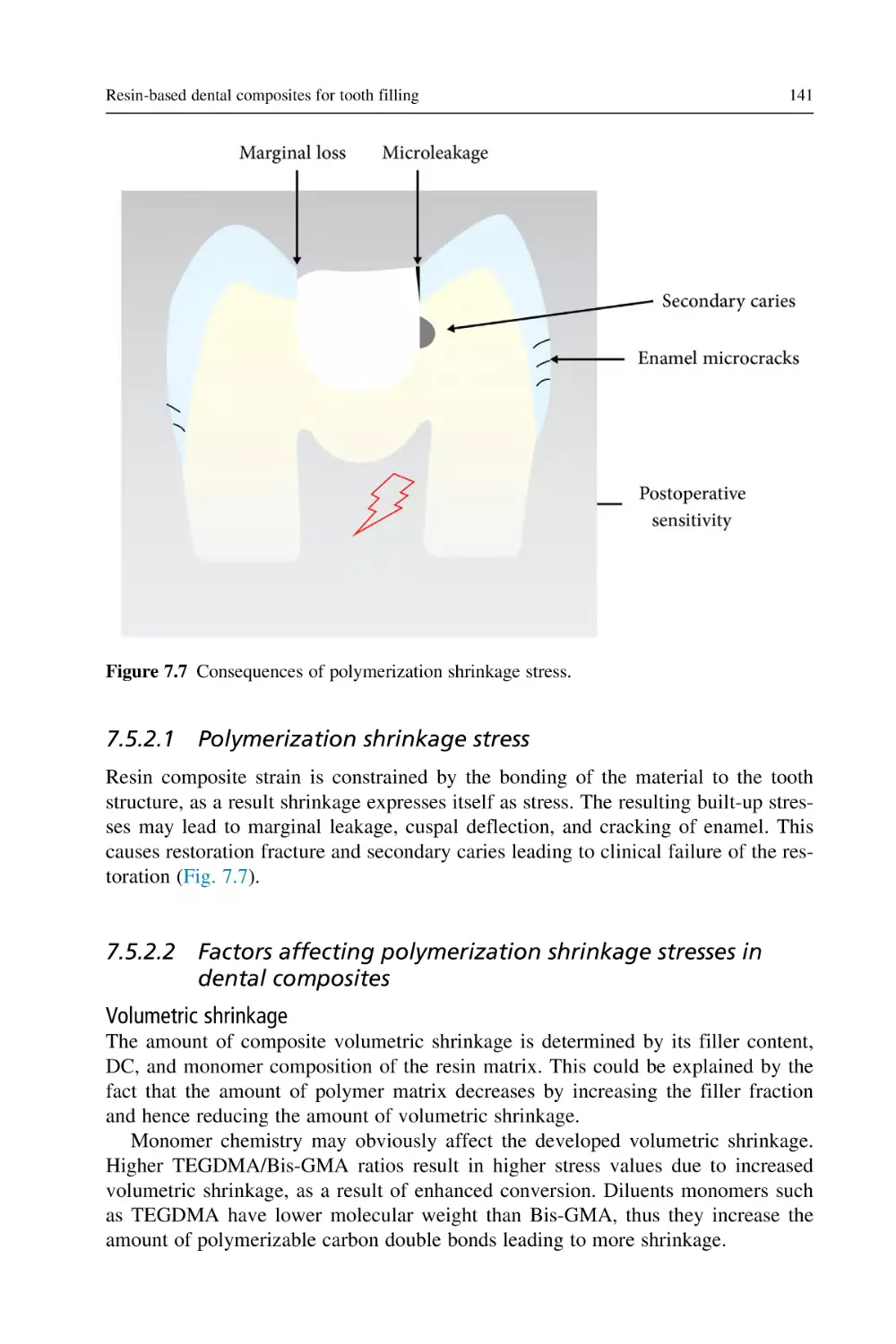
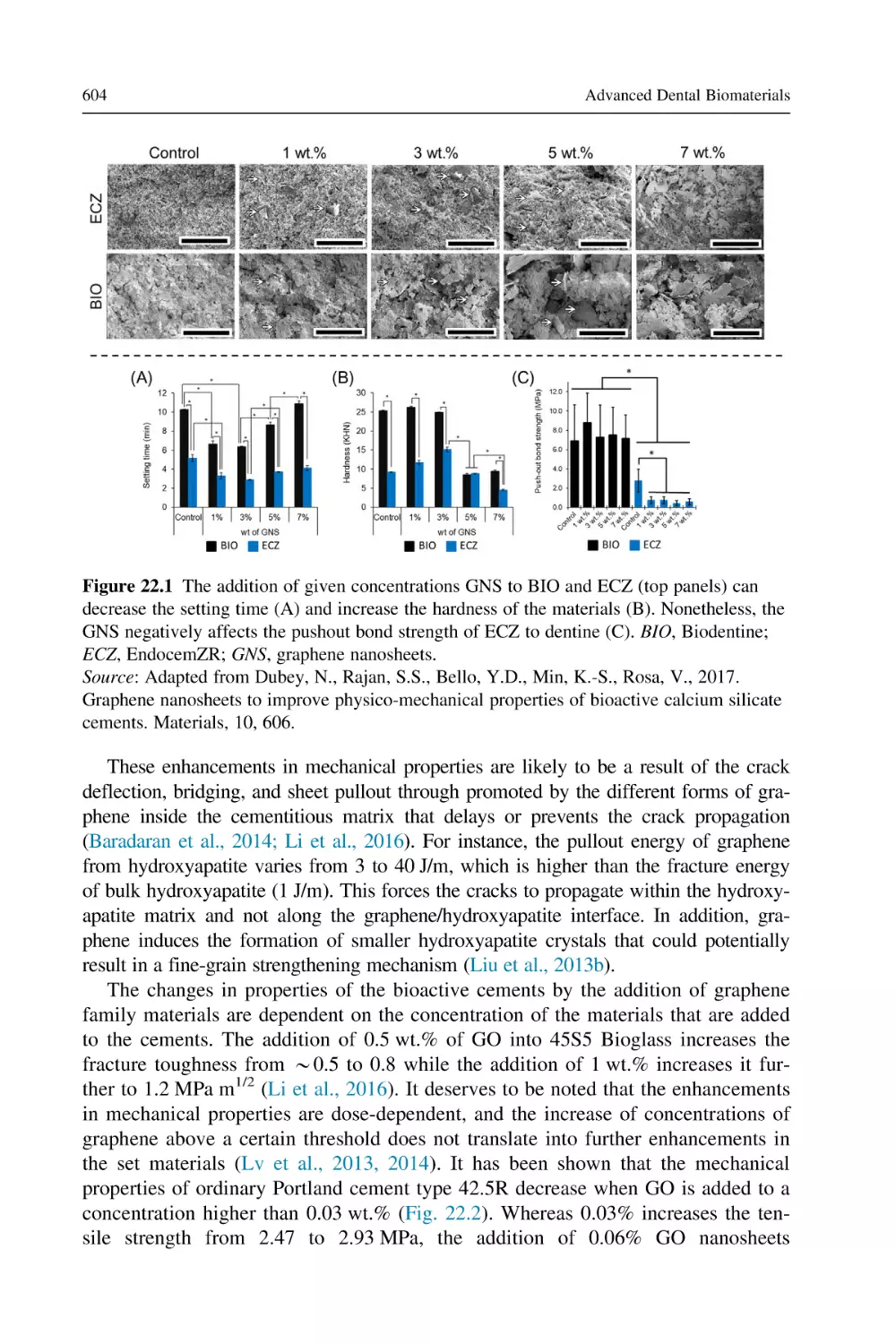
(Fig. 2.3).
Properties of dental biomaterials
17
Figure 2.3 Various types of forces and possible deformation according to force directions.
Several test methods are designed to measure the mechanical properties of dental
material by destructive testing methodologies, that is, compressive, tensile, impact tests,
hardness, brittleness, fatigue, and wear resistance. The unit of force is newton or pound.
2. Stress and strain: When a force is applied on a material, stress is equal to the force
applied divided by per unit area, that is, forces/unit area, and the unit is Newton/meter
square. Stress or a force that is applied to a material produces a strain which is opposite
to the external force but equal in magnitude. Strain is the change in the size (length) of
the material divided by the original size (length). The unit of stress is pascal (Pa) or
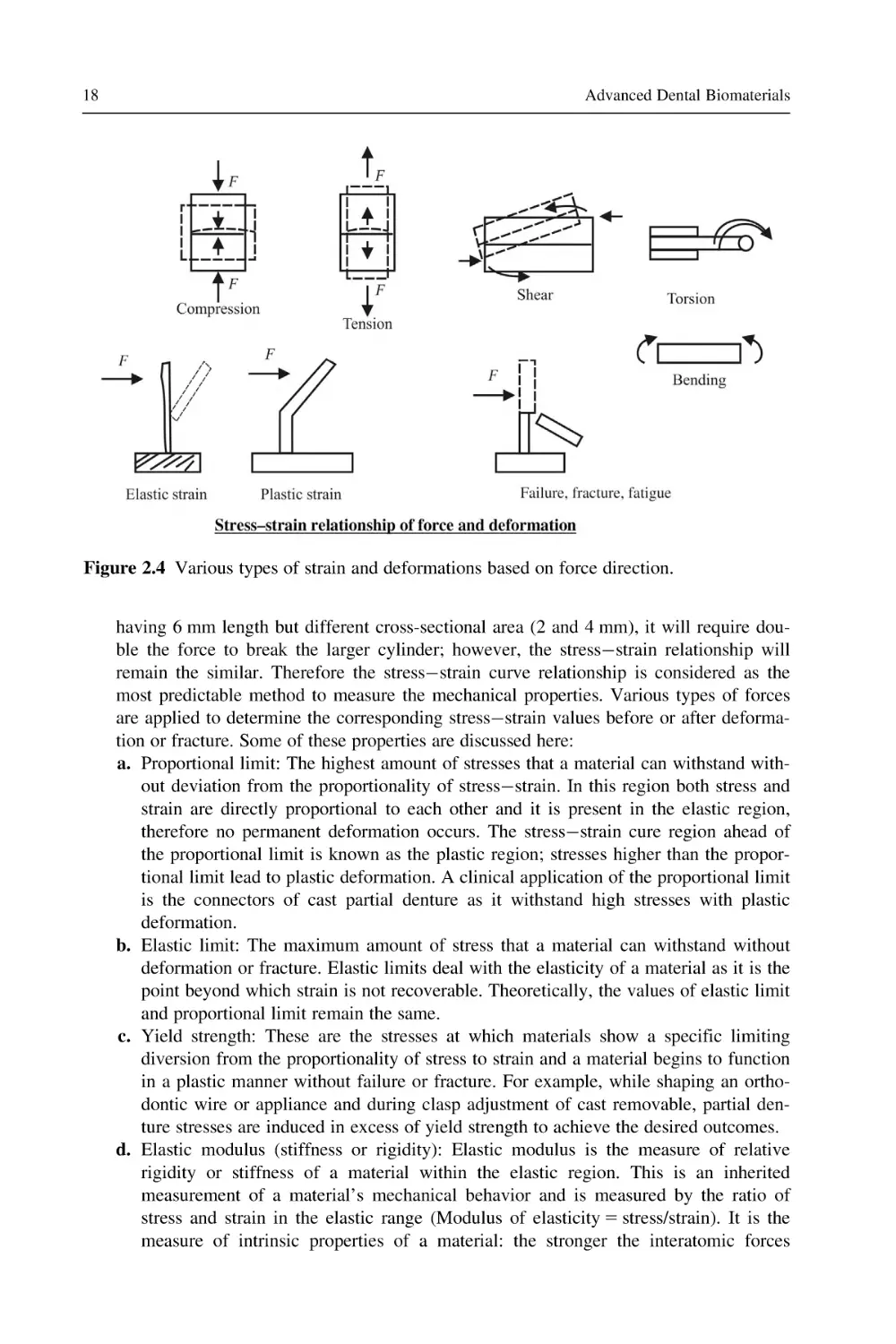
megapascal (MPa). Compressive stresses are produced when a material is subjected to
forces in a straight line directed in the same direction toward the center. Compressive
stress produces comprehensive strain (Sakaguchi and Powers, 2012), as shown in
Fig. 2.4. Tensile stress results in a material when two set of forces are applied in a
straight line but in opposite directions, that is, the material is pulled apart (Fig. 2.4).
Tensile stress produces tensile strain.
3. Elastic and plastic regions: In the stressstrain graph, two types of stresses are common,
elastic and plastic, which produce the corresponding elastic strain and plastic strain.
Elastic stresses do not produce any deformation; therefore after the removal of elastic
stress, a material will come back to its original dimension and it remains unchanged due
to elastic strain, whereas plastic stresses produce permanent deformation and the material
will not come back to its original size or shape (Sakaguchi and Powers, 2012). Several
mechanical behaviors are determined from elastic strain, for example, elastic modulus,
flexibility, resilience, and Poisson’s ratio. On the other hand, the initial plastic deformation region and/or the end of the elastic region of a stressstrain graph help to determine
the yield point, proportional limit, elastic limit, and yield strength.
It is important to understand stress and strain because they are independent of the
size of the material used. For example, for two cylindrical shape specimens of composite
18
Advanced Dental Biomaterials
Figure 2.4 Various types of strain and deformations based on force direction.
having 6 mm length but different cross-sectional area (2 and 4 mm), it will require double the force to break the larger cylinder; however, the stressstrain relationship will
remain the similar. Therefore the stressstrain curve relationship is considered as the
most predictable method to measure the mechanical properties. Various types of forces
are applied to determine the corresponding stressstrain values before or after deformation or fracture. Some of these properties are discussed here:
a. Proportional limit: The highest amount of stresses that a material can withstand without deviation from the proportionality of stressstrain. In this region both stress and
strain are directly proportional to each other and it is present in the elastic region,
therefore no permanent deformation occurs. The stressstrain cure region ahead of
the proportional limit is known as the plastic region; stresses higher than the proportional limit lead to plastic deformation. A clinical application of the proportional limit
is the connectors of cast partial denture as it withstand high stresses with plastic
deformation.
b. Elastic limit: The maximum amount of stress that a material can withstand without
deformation or fracture. Elastic limits deal with the elasticity of a material as it is the
point beyond which strain is not recoverable. Theoretically, the values of elastic limit
and proportional limit remain the same.
c. Yield strength: These are the stresses at which materials show a specific limiting
diversion from the proportionality of stress to strain and a material begins to function
in a plastic manner without failure or fracture. For example, while shaping an orthodontic wire or appliance and during clasp adjustment of cast removable, partial denture stresses are induced in excess of yield strength to achieve the desired outcomes.
d. Elastic modulus (stiffness or rigidity): Elastic modulus is the measure of relative
rigidity or stiffness of a material within the elastic region. This is an inherited
measurement of a material’s mechanical behavior and is measured by the ratio of
stress and strain in the elastic range (Modulus of elasticity 5 stress/strain). It is the
measure of intrinsic properties of a material: the stronger the interatomic forces
Properties of dental biomaterials
4.
5.
6.
7.
19
(basic interaction forces), the greater the value of elastic modulus, and therefore, the
materials would be more rigid and stiff (resistance to elastic deformation). Generally,
the modulus of elasticity of dental materials is directly related to hardness (Zafar and
Ahmed, 2014a,b; Zafar, 2014).
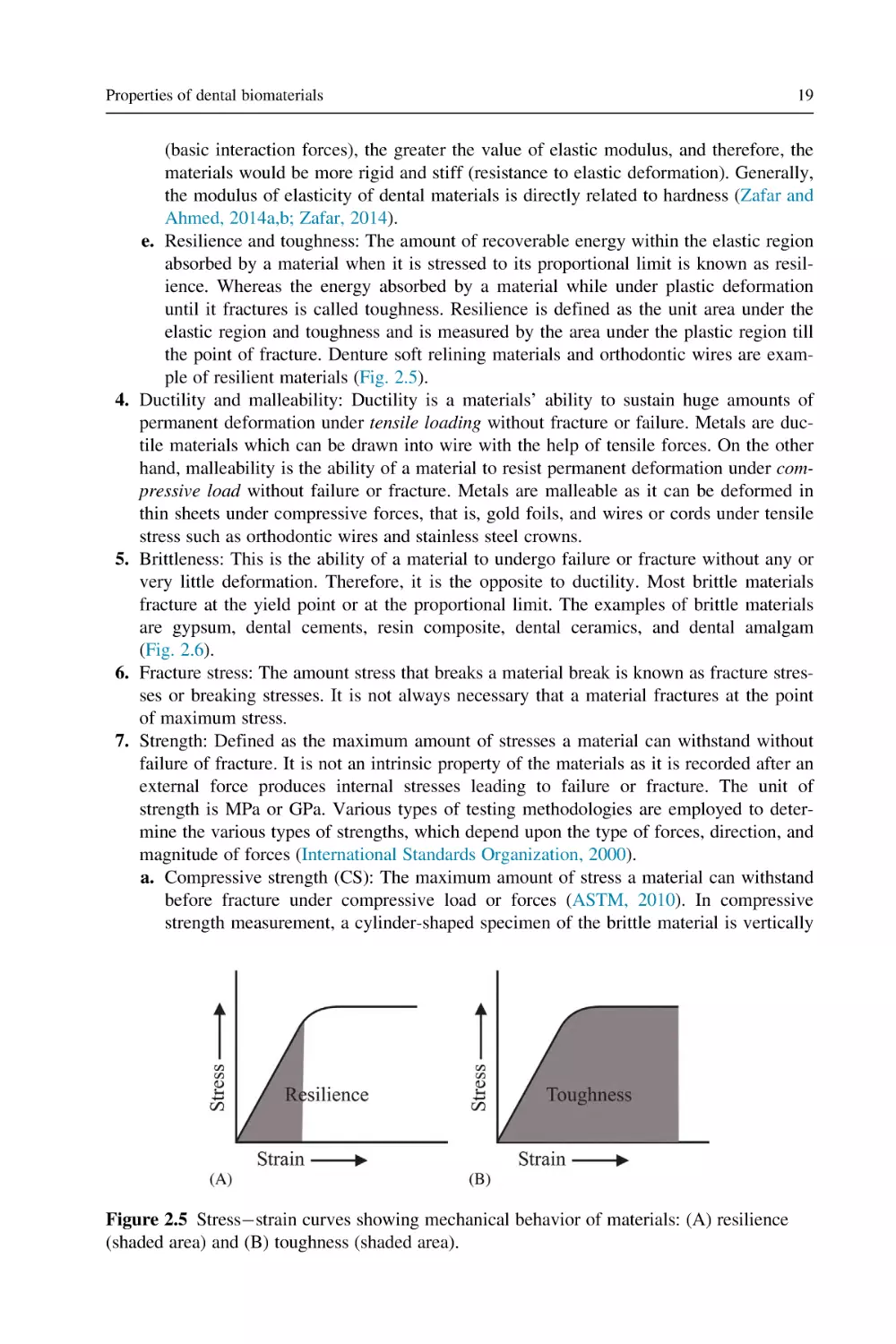
e. Resilience and toughness: The amount of recoverable energy within the elastic region
absorbed by a material when it is stressed to its proportional limit is known as resilience. Whereas the energy absorbed by a material while under plastic deformation
until it fractures is called toughness. Resilience is defined as the unit area under the
elastic region and toughness and is measured by the area under the plastic region till
the point of fracture. Denture soft relining materials and orthodontic wires are example of resilient materials (Fig. 2.5).
Ductility and malleability: Ductility is a materials’ ability to sustain huge amounts of
permanent deformation under tensile loading without fracture or failure. Metals are ductile materials which can be drawn into wire with the help of tensile forces. On the other
hand, malleability is the ability of a material to resist permanent deformation under compressive load without failure or fracture. Metals are malleable as it can be deformed in
thin sheets under compressive forces, that is, gold foils, and wires or cords under tensile
stress such as orthodontic wires and stainless steel crowns.
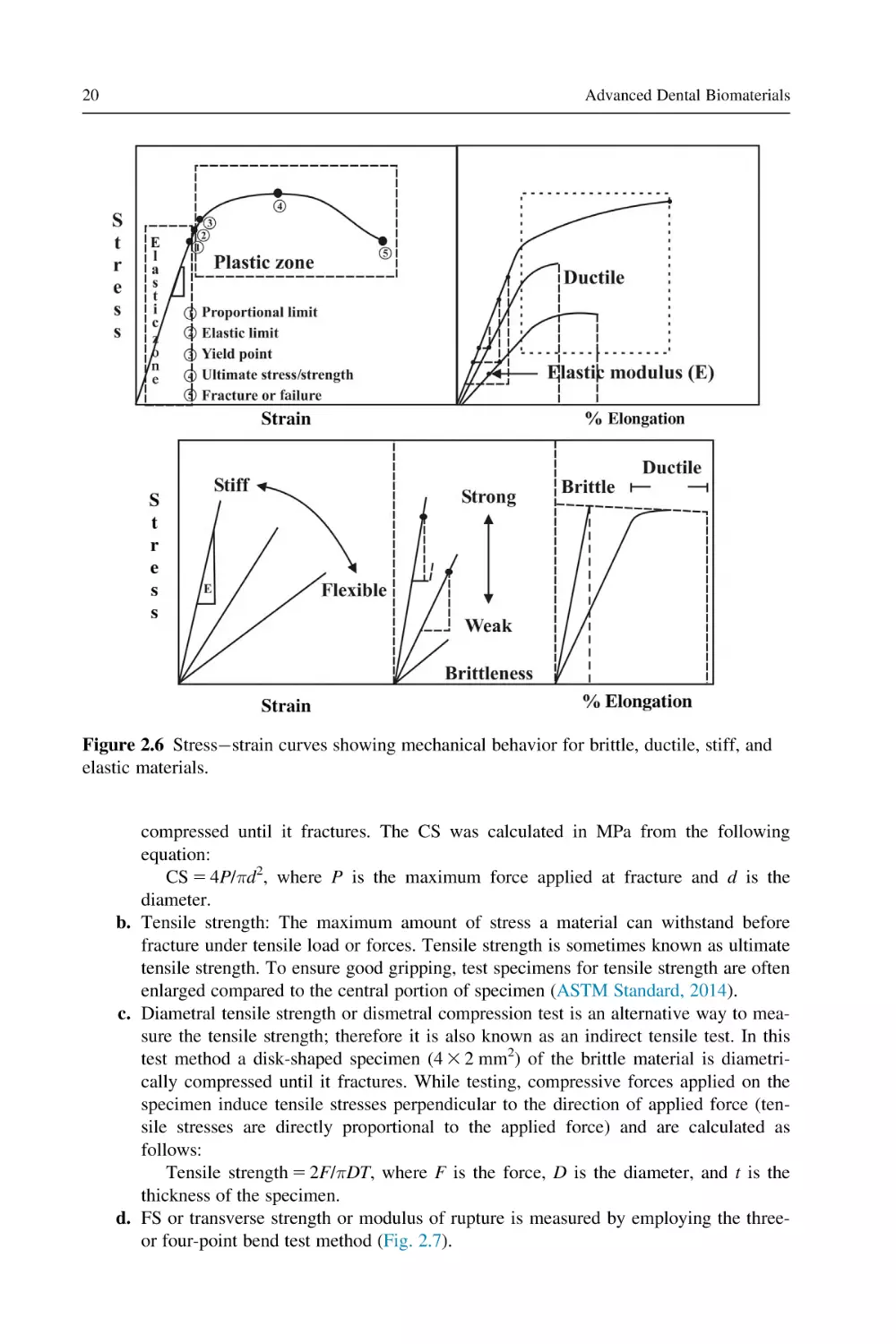
Brittleness: This is the ability of a material to undergo failure or fracture without any or
very little deformation. Therefore, it is the opposite to ductility. Most brittle materials
fracture at the yield point or at the proportional limit. The examples of brittle materials
are gypsum, dental cements, resin composite, dental ceramics, and dental amalgam
(Fig. 2.6).
Fracture stress: The amount stress that breaks a material break is known as fracture stresses or breaking stresses. It is not always necessary that a material fractures at the point
of maximum stress.
Strength: Defined as the maximum amount of stresses a material can withstand without
failure of fracture. It is not an intrinsic property of the materials as it is recorded after an
external force produces internal stresses leading to failure or fracture. The unit of
strength is MPa or GPa. Various types of testing methodologies are employed to determine the various types of strengths, which depend upon the type of forces, direction, and
magnitude of forces (International Standards Organization, 2000).
a. Compressive strength (CS): The maximum amount of stress a material can withstand
before fracture under compressive load or forces (ASTM, 2010). In compressive
strength measurement, a cylinder-shaped specimen of the brittle material is vertically
Figure 2.5 Stressstrain curves showing mechanical behavior of materials: (A) resilience
(shaded area) and (B) toughness (shaded area).
20
Advanced Dental Biomaterials
Figure 2.6 Stressstrain curves showing mechanical behavior for brittle, ductile, stiff, and
elastic materials.
compressed until it fractures. The CS was calculated in MPa from the following
equation:
CS 5 4P/πd2, where P is the maximum force applied at fracture and d is the
diameter.
b. Tensile strength: The maximum amount of stress a material can withstand before
fracture under tensile load or forces. Tensile strength is sometimes known as ultimate
tensile strength. To ensure good gripping, test specimens for tensile strength are often
enlarged compared to the central portion of specimen (ASTM Standard, 2014).
c. Diametral tensile strength or dismetral compression test is an alternative way to measure the tensile strength; therefore it is also known as an indirect tensile test. In this
test method a disk-shaped specimen (4 3 2 mm2) of the brittle material is diametrically compressed until it fractures. While testing, compressive forces applied on the
specimen induce tensile stresses perpendicular to the direction of applied force (tensile stresses are directly proportional to the applied force) and are calculated as
follows:
Tensile strength 5 2F/πDT, where F is the force, D is the diameter, and t is the
thickness of the specimen.
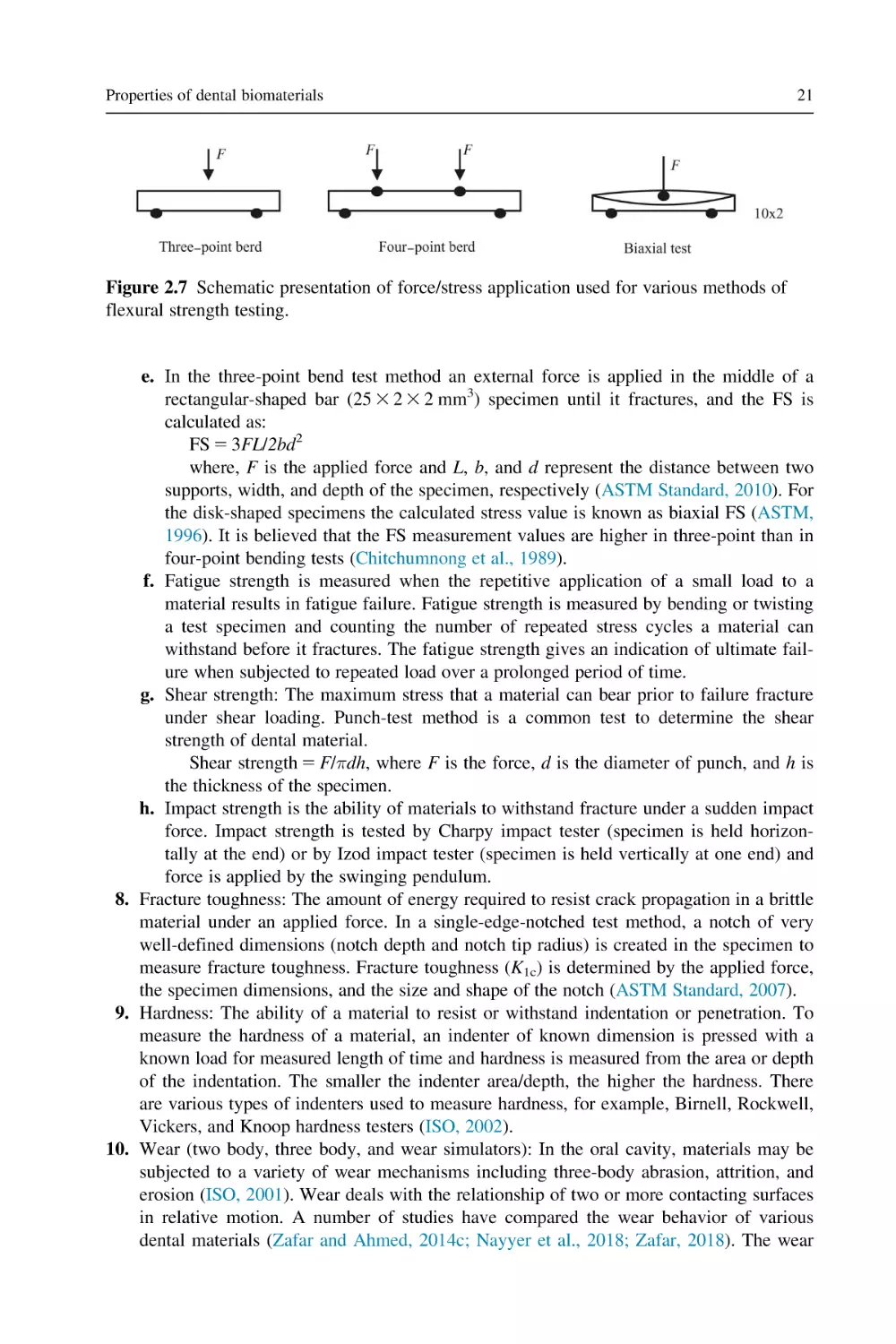
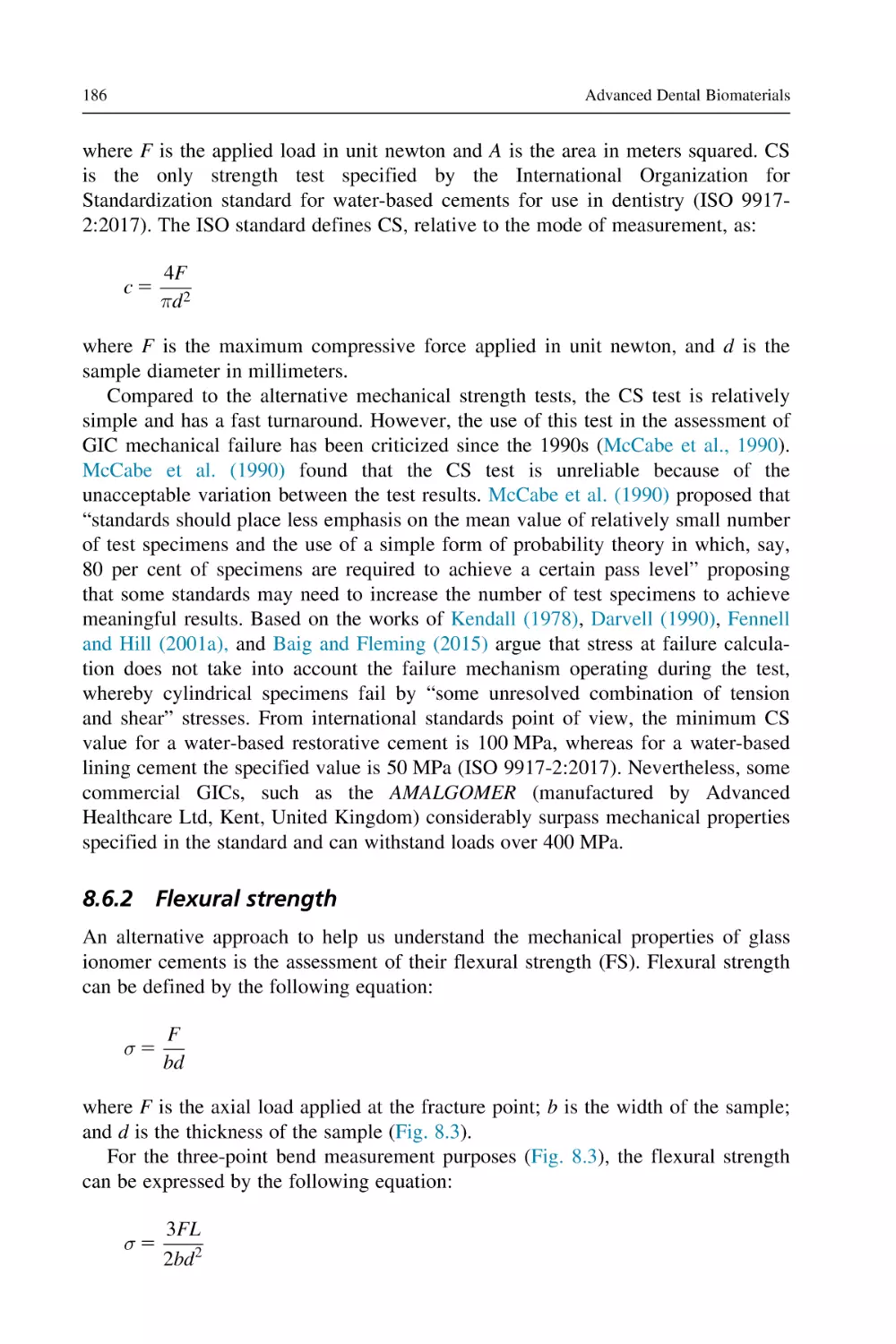
d. FS or transverse strength or modulus of rupture is measured by employing the threeor four-point bend test method (Fig. 2.7).
Properties of dental biomaterials
21
Figure 2.7 Schematic presentation of force/stress application used for various methods of
flexural strength testing.
e. In the three-point bend test method an external force is applied in the middle of a
rectangular-shaped bar (25 3 2 3 2 mm3) specimen until it fractures, and the FS is
calculated as:
FS 5 3FL/2bd2
where, F is the applied force and L, b, and d represent the distance between two
supports, width, and depth of the specimen, respectively (ASTM Standard, 2010). For
the disk-shaped specimens the calculated stress value is known as biaxial FS (ASTM,
1996). It is believed that the FS measurement values are higher in three-point than in
four-point bending tests (Chitchumnong et al., 1989).
f. Fatigue strength is measured when the repetitive application of a small load to a
material results in fatigue failure. Fatigue strength is measured by bending or twisting
a test specimen and counting the number of repeated stress cycles a material can
withstand before it fractures. The fatigue strength gives an indication of ultimate failure when subjected to repeated load over a prolonged period of time.
g. Shear strength: The maximum stress that a material can bear prior to failure fracture
under shear loading. Punch-test method is a common test to determine the shear
strength of dental material.
Shear strength 5 F/πdh, where F is the force, d is the diameter of punch, and h is
the thickness of the specimen.
h. Impact strength is the ability of materials to withstand fracture under a sudden impact
force. Impact strength is tested by Charpy impact tester (specimen is held horizontally at the end) or by Izod impact tester (specimen is held vertically at one end) and
force is applied by the swinging pendulum.
8. Fracture toughness: The amount of energy required to resist crack propagation in a brittle
material under an applied force. In a single-edge-notched test method, a notch of very
well-defined dimensions (notch depth and notch tip radius) is created in the specimen to
measure fracture toughness. Fracture toughness (K1c) is determined by the applied force,
the specimen dimensions, and the size and shape of the notch (ASTM Standard, 2007).
9. Hardness: The ability of a material to resist or withstand indentation or penetration. To
measure the hardness of a material, an indenter of known dimension is pressed with a
known load for measured length of time and hardness is measured from the area or depth
of the indentation. The smaller the indenter area/depth, the higher the hardness. There
are various types of indenters used to measure hardness, for example, Birnell, Rockwell,
Vickers, and Knoop hardness testers (ISO, 2002).
10. Wear (two body, three body, and wear simulators): In the oral cavity, materials may be
subjected to a variety of wear mechanisms including three-body abrasion, attrition, and
erosion (ISO, 2001). Wear deals with the relationship of two or more contacting surfaces
in relative motion. A number of studies have compared the wear behavior of various
dental materials (Zafar and Ahmed, 2014c; Nayyer et al., 2018; Zafar, 2018). The wear
22
Advanced Dental Biomaterials
behavior of dental materials is not only dependent on the material properties but also on
the contact conditions including the material itself, the surface roughness, motion pattern, the rate of loading, the shape and contour of the antagonist material, the local environment, and lubrication. The traditional methods of classifications of wear are based on
the type of motion and the mechanism of wear (adhesion, abrasion, attrition, surface
fatigue). In vitro wear test methods attempt to mimic the masticatory processes. The
wear assessment of restorative materials has been conducted using a variety of machines
which simulate diverse wear mechanisms. Most commonly used wear simulators include
the IVOCLAR wear simulator, the Zurich wear simulator, the MTS wear simulator, the
Oregon Health & Science University wear simulator, the Dento-munch-robo-simulator,
and the University of Alabama wear simulator (Heintze, 2006). However, due to complex oral biology and a limited number of internationally recognized standards for the
in vitro wear testing, simulating and interpreting complexity of the wear behavior
mechanisms is not straightforward (Heintze et al., 2012).
11. Standards of dental materials testing: Various studies reporting mechanical characterization
can only be compared if following certain standards of testing parameters, specimen preparation, and data interpretation. In addition, following standards facilitates the reproducibility
of results. Unfortunately, there are only a few standards available to describe the mechanical
testing parameters for dental restorative materials, specifically for glass ionomer cements
(GICs) and resin-based composites. For example, the specification standard for acidbase
cements (ISO 9917-1:2007) describes the CS, working time, and setting time specifications;
the standard for light activated system (ISO 9917-2:2000) describes FS, depth of cure,
shade, and color stability; the ISO 10477-2004 provides standard specification for bond
strength, FS, and water sorption; and the ISO 4049:2000 describes the specification for FS,
film thickness, depth of cure, working, and setting time.
2.7
Limitation of mechanical testing methods
It is very difficult to duplicate the human oral conditions in the laboratory and this
makes it difficult to properly test materials in a similar environment into which
they will be placed. In addition, the quality of the test specimens prepared for
mechanical testing may also influence the outcome of test results. All mechanical
test methods are limited as they address the individual properties without measuring
the interaction between various properties. Therefore the phenomenon of aging in
the oral cavity and the determination of the potential service of life of dental materials are challenging but an important factor to determine the mechanical properties.
2.8
Biological properties
2.8.1 Biocompatibility
Biocompatibility is an ability of a material to perform its desired function without
causing any local or systemic adverse response in the recipient of the material
(Perrotti et al., 2017; Schmalz, 2014). Biocompatibility is a dynamic process
because there is a change in properties of material and host response over the period
Properties of dental biomaterials
23
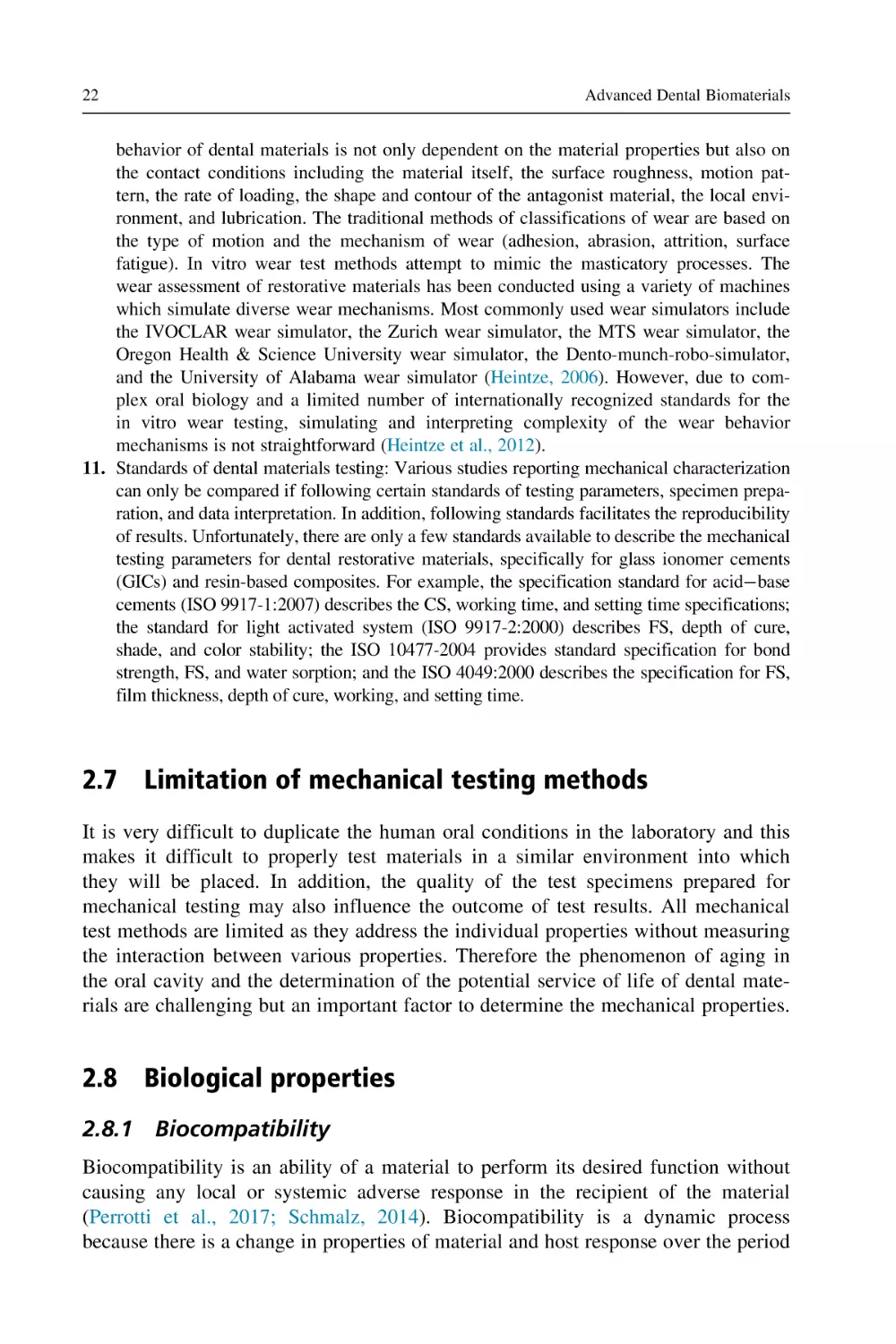
Table 2.4 Various types of tests used to assess the biocompatibility of
biomaterials (Perrotti et al., 2017; Moharamzadeh et al., 2009).
Tests
Testing methods
1
In vitro
2
In vivo
3
Usage
Cytotoxicity test
Membrane permeability test
Agar overlay method
Dentin barrier tests
Mucous membrane irritation test
Skin sensitization
Implantation tests
Dental pulp irritation tests
Periapical tissue damage and
Endodontic usage
Dental implantation in bone
of time, for instance due to corrosion, disease, and aging (Wataha, 2001).
Biocompatibility testing is not easy as new technologies are arriving. The simplest
way of classifying these tests is in vitro testing, in vivo testing on animal models,
and usage tests (Table 2.4).
2.8.2 In vitro testing
In vitro testing is performed outside a living organism in a laboratory setting using
cells of human or animal origin (Perrotti et al., 2017; Cintra et al., 2017). The
objective of in vitro testing is to predict the response and further improve the material before in vivo testing (de Souza Costa et al., 2014). The in vitro testing includes
the following:
G
G
Indirect contact tests, in which the viability of cell is assessed through indirect contact of
material, for instance, contact of elute or extract of material with the cells, mostly fibroblasts or keratinocytes (Perrotti et al., 2017; Cintra et al., 2017; Moharamzadeh et al.,
2009). Among the other methods of indirect contact are agar overlay method and dentin
slice technique (Moharamzadeh et al., 2009).
Direct contact tests, in which the material is in direct contact with the cell. The morphological features of cells are observed under a scanning electron microscope
(Moharamzadeh et al., 2009; Chan et al., 2017). The cell viability is also assessed by
methyl thiazol tetrazolium (MTT) assay in which the viable cells convert the MTT 3-[4,5dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide into formazan dye and the dye is
quantified using a reader at a specific wavelength (Chan et al., 2017).
The in vitro testing has numerous advantages, such as being faster and more
cost-effective compared to in vivo testing, with greater reproducibility of the
results, and no ethical and legal issues (Sakaguchi and Powers, 2012; Perrotti et al.,
2017; Wataha et al., 1999). The disadvantage of in vitro testing is that the exact tissue response of the material cannot be predicted (Sakaguchi and Powers, 2012;
Perrotti et al., 2017).
24
Advanced Dental Biomaterials
2.8.3 In vivo testing
In vivo testing is done in animal models (de Souza Costa et al., 2014). The in vivo
testing includes:
G
G
testing by implantation of the material subcutaneously in animals, followed by monitoring
the inflammatory response of the adjacent tissues by excising and examining the tissue
under the microscope (Cintra et al., 2017; Garcia Lda et al., 2010; Lacerda-Santos et al.,
2015) and
implantation test of the material into the experimental animal bone followed by histological evaluation (Chan et al., 2017).
The main advantages of in vivo testing is that the biological response is comprehensive and has lower costs compared to clinical studies (Perrotti et al., 2017; de
Souza Costa et al., 2014). The disadvantages that are associated with in vivo tests
are high costs as compared to in vitro testing, long duration, and ethical and legal
issues (Sakaguchi and Powers, 2012; Perrotti et al., 2017).
2.8.4 Usage tests
The usage tests are considered as gold standard and are performed on human volunteers. The material or device is placed in a situation that is similar to its intended
use (Perrotti et al., 2017; de Souza Costa et al., 2014; Moharamzadeh et al., 2009).
The advantage of the usage tests is that the results are clinically relevant and comprehensive (Perrotti et al., 2017; Moharamzadeh et al., 2009).
The major disadvantages that are associated with usage tests are their high costs,
prolonged duration, and legal and ethical issues (Perrotti et al., 2017; de Souza
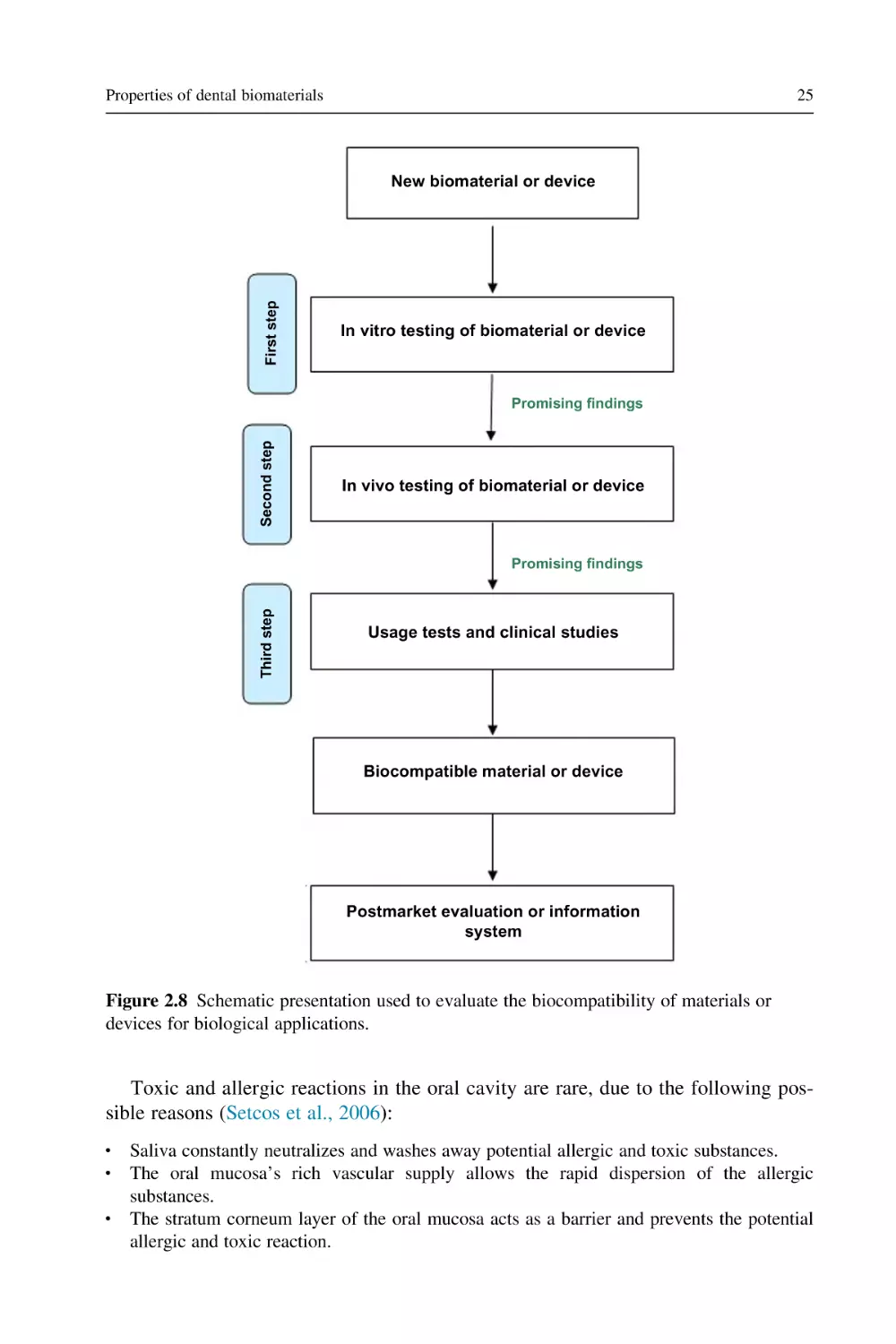
Costa et al., 2014). It is vital to understand that just one type of testing cannot
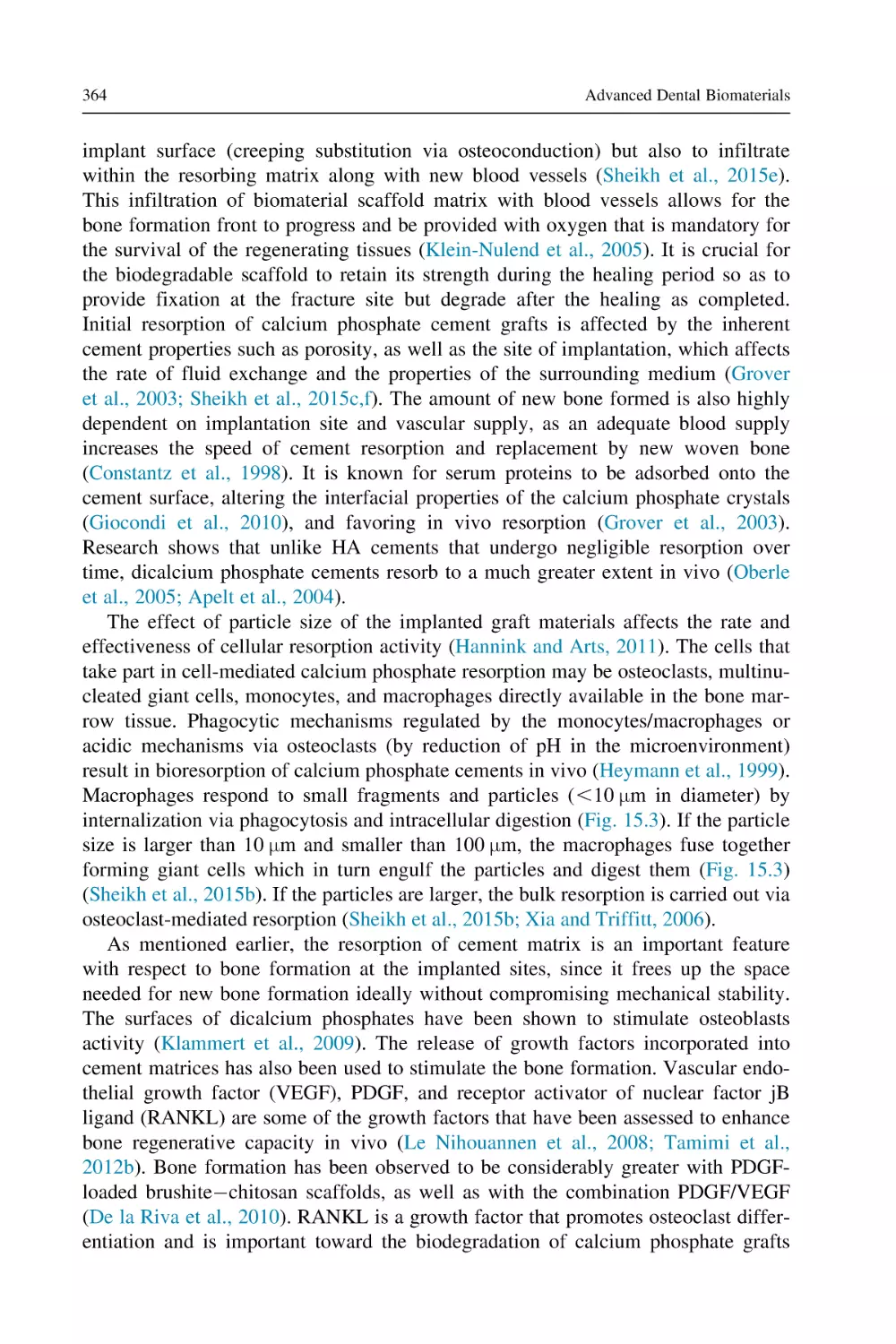
entirely predict the biocompatibility of a material and a combination of tests is usually carried out to evaluate the overall biocompatibility of the material. For any specific biological application, a systematic protocol (Fig. 2.8) is used to evaluate the
biocompatibility of materials or devices.
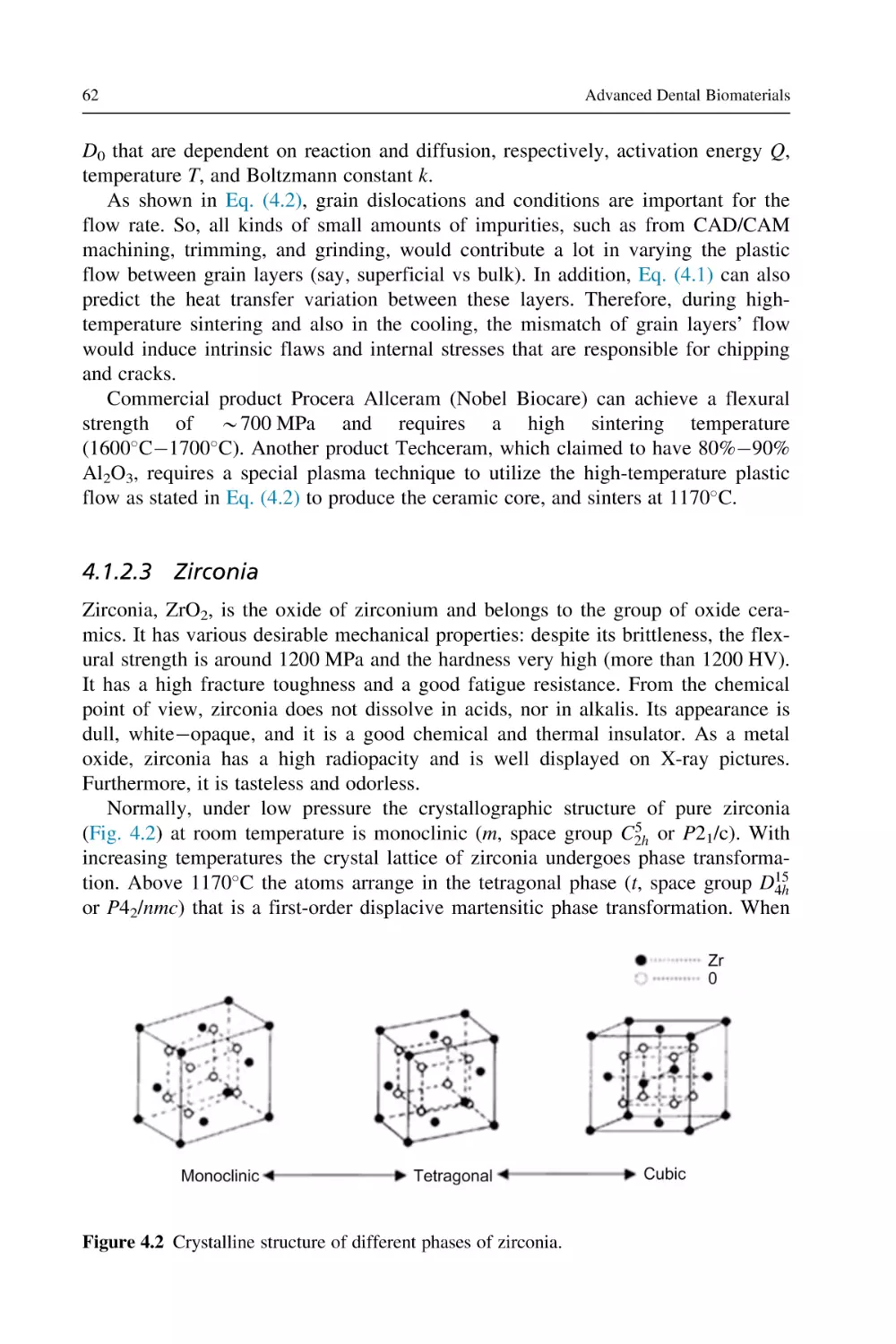
2.9
Toxicity and cytotoxicity
Toxicity is the ability of a material to damage a biological system by chemical
means (Schmalz, 2009a). In vitro cytotoxicity testing is assessed during the initial
screening of the material. In vitro studies have shown that when the setting reaction
in the restorative materials (such as resin modified glass ionomer cements and resin
composites) is incomplete, the cytotoxic effects are due to the release of ingredients
from the incompletely set material that alters the metabolic processes of the cell
(Goldberg, 2008). The toxicity is classified as local or the systemic toxicity.
Local toxicity: The damage occurs in the form of inflammation or necrosis at the
site of application of a biomaterial (Schmalz, 2009a).
Systemic toxicity: The damage occurs in an area that is distant from the site of
application of material (Schmalz, 2009a).
Properties of dental biomaterials
25
First step
New biomaterial or device
In vitro testing of biomaterial or device
Second step
Promising findings
In vivo testing of biomaterial or device
Third step
Promising findings
Usage tests and clinical studies
Biocompatible material or device
Postmarket evaluation or information
system
Figure 2.8 Schematic presentation used to evaluate the biocompatibility of materials or
devices for biological applications.
Toxic and allergic reactions in the oral cavity are rare, due to the following possible reasons (Setcos et al., 2006):
G
G
G
Saliva constantly neutralizes and washes away potential allergic and toxic substances.
The oral mucosa’s rich vascular supply allows the rapid dispersion of the allergic
substances.
The stratum corneum layer of the oral mucosa acts as a barrier and prevents the potential
allergic and toxic reaction.
26
2.10
Advanced Dental Biomaterials
Cytotoxicity tests
The cytotoxicity tests assess the cellular reaction by a material or its eluates and
in vitro testing assesses the cell viability, cell growth or function, enzyme activity,
membrane integrity, and formation of reactive oxygen species before and after
exposure of cells to the material (de Souza Costa et al., 2014; Moharamzadeh et al.,
2009; Goldberg, 2008).
The outcomes of these tests cannot exactly predict the behavior of the material
in vivo. The outcomes of cytotoxic tests depend on numerous factors, such as storage time of material before testing, material manipulation/mixing ratio, and polymerization method (Jorge et al., 2003). The test should be selected according to the
desired use of the material, for instance the in vitro cytotoxicity of denture adhesives should be evaluated by exposure of extracts of denture adhesives with the gingival fibroblasts, followed by evaluation of the cell density and metabolic activity
of the viable cells (Soares et al., 2018). The in vivo local cytotoxicity of oral
hygiene products can be assessed by the collection of oral mucosa cells of the individual, followed by scanning of nuclear anomalies under high magnification (Tadin
et al., 2018).
2.11
Fluoride and caries
Dental caries is one of the most prevalent and multifactorial community problems
in the developed as well as developing societies. The relationship of fluoride
administration and decreased incidence of dental caries is well documented and
fluoride has made an impact on the dental health of the population (Levine, 2010;
Tenuta and Cury, 2010). The anticaries effect of fluoride is dependent on the type
of fluoride compound, concentration and contact time of fluoride with oral tissues,
and the method of fluoride delivery (Goldberg, 2016). Fluoride is an ionic form of
a trace element that belongs to the halogen group of elements (McGrady et al.,
2010). It is one of the most abundant and highly reactive elements that are present
naturally in water, soil, plants, and animals (Harrison, 2005; Ullah et al., 2017).
Fluoride is recognized by the US Food and Drug Agency for the prevention of dental caries (Carey, 2014). Fluoride is naturally present in water and seafood
(Martı́nez-Mier, 2012). It has been delivered into the oral cavity by water fluoridation, food products (milk, salts, and juices), devices (fluoride nanoparticles), and
oral hygiene products (toothpastes, mouth rinses, gels, and varnishes containing
fluoride) (McGrady et al., 2010; Ullah and Zafar, 2015). In addition, fluoride has
been incorporated into various dental restorative materials such as conventional and
resin-modified glass ionomers and modified resin-based composites (Zafar and
Ahmed, 2015a; Zafar, 2013) that facilitate caries prevention by releasing fluoride
into the oral cavity.
The major effect of fluoride on caries prevention is primarily due to the topical
effect of fluoride after eruption. The caries preventing effect of fluoride is mainly
Properties of dental biomaterials
27
due to the inhibition of bacterial plaque metabolism and acid production by inhibiting bacterial enzyme enolase (Levine, 2010; Ullah and Zafar, 2015) and through
formation of a more stable mineral phase with less solubility. There is also incorporation of fluoride into the enamel prior to the eruption of teeth which also increases
the resistance of enamel against dental caries (Martı́nez-Mier, 2012).
2.11.1 Fluoride toxicity
The total fluoride dose of 0.050.07 mg/kg body weight is considered as safe
(Buzalaf and Levy, 2011). The fluoride containing products for the control of dental
caries should be prescribed carefully. During tooth development consumption of
fluoride above the safe dose is associated with numerous toxic effects (Tinanoff
and O’Sullivan, 1997). However, the primary focus here is dental fluorosis. Dental
fluorosis is a developmental disturbance in enamel formation, which occurs because
of exposure of fluoride above the safe dose. The enamel is hypomineralized with
increased porosity (Carey, 2014; Atia and May, 2013). The dental fluorosis risk is
related to the fluoride dose, duration of consumption, nutritional status, renal and
gastrointestinal function, genetics, and timing of intake (Tinanoff and O’Sullivan,
1997; Denbesten and Li, 2011). The clinical presentation of dental fluorosis may
range from chalky white areas of hypomineralization to dark stained surface with
pitting and brittle enamel (Carey, 2014; Tinanoff and O’Sullivan, 1997; Atia and
May, 2013). The severity of dental fluorosis depends on when and how long the
excess exposure to fluoride occurs (Atia and May, 2013).
2.12
Carcinogenicity
Carcinogenesis is the progression of a normal healthy cell to a potentially malignant
cell (Scully, 2011). Carcinogenicity is an ability of a material to cause cancer or
neoplasm in vivo and the carcinogens are the substances that are known to cause
cancer (Craig and Powers, 2002; Anusavice and Phillips, 2003). There are various
risk factors that are associated with carcinogenesis; the most commonly associated
factors are tobacco, alcohol consumption, Candida albicans, viruses such as human
papilloma, herpes simplex, and ionizing radiations. These factors either act alone or
in combination (Scully, 2011).
Formaldehyde is an antimicrobial compound. It is used in the manufacturing
industry (plywood, glue), agriculture (seed treatment), and cosmetics. Beside this it
is also present naturally in fruits and fishes. It is also a constituent of dental materials
such as composite resins, epoxy resin used in endodontic treatment, and formocresol
an agent for pulpotomy (Athanassiadis et al., 2015). Formaldehyde is considered as a
carcinogenic material but the amount of release in vivo is very negligible to cause
any significant risk (Athanassiadis et al., 2015). Nickel-containing alloys have
various applications in dentistry, such as crowns, bridges, partial dentures, metallic
brackets, wires, springs, and endodontic instruments (Setcos et al., 2006).
28
Advanced Dental Biomaterials
The nickel-containing alloys within restorations and appliances release a very negligible amount of nickel as compared to exposure through other routes, for instance
drinking water, occupational exposure, and intravenous exposure during drug administration (Setcos et al., 2006). Although there are concerns of carcinogenicity associated with nickel among laboratory personnel involved in the casting of alloys
containing nickel, which can be minimized if manufacturer’s instructions are followed (Setcos et al., 2006). Dental adhesives containing glutaraldehyde, TEGMA,
and bis-GMA products have been found to be mutagenic in vitro. However, the concentrations are very negligible in subjects with these restorations compared to those
concentrations necessary to cause these effects (Craig and Powers, 2002; Schmalz,
2009b).
2.13
Biodegradation
The degradation of material that is not harmful for the body is known as biodegradation. The products that are produced as a result are usually not toxic to the body
fluids. However, a high rate of biodegradation can have a few side effects
(Goharian, 2017b). Examples of the biodegradable materials include natural
polymer-based materials such as silk (Zafar and Al-Samadani, 2014; Cao and
Wang, 2009; Vasconcelos et al., 2008), chitosan (Husain et al., 2017; Qasim et al.,
2018), and synthetic polymers polylactic coglycolic acid, poly(urethanes), and polylactic acid. The advantages of the biodegradable materials are that their subsequent
removal from the patient’s body is not required and it is easier to deliver therapeutic agents locally (Goharian, 2017a).
2.14
Bioactivity
Bioactivity is the ability of a material to elicit a specific biological effect and form
a bond with the tissue. The term bioactivity is also defined as the cellular effects
induced because of release of bioactive substances and ions from the material
(Vallittu et al., 2018; Gerhardt and Boccaccini, 2010; Hoppe et al., 2011). The
incorporation of therapeutic substances favorably affects the behavior of the cells
and enhances bone and new blood vessels formation (Hoppe et al., 2011).
Examples of bioactive materials are bioactive glasses for bone regeneration and tissue engineering (Gorustovich et al., 2009), composite materials with bioactive inorganic components (Gerhardt and Boccaccini, 2010), glass ionomers (Najeeb et al.,
2016a), hydroxyapatite (HA) nanoparticles modified titanium implants (Vanzillotta
et al., 2006; Javed et al., 2014), and titanium dioxide nanoparticle-modified adhesives or coatings (Welch et al., 2010; Najeeb et al., 2016b).
Before in vivo testing of bioactivity, it is standard to conduct in vitro testing of
the bioactivity of the material by immersion of the material into simulated body
fluid and assessing the formation of HA on its surface using different surface
Properties of dental biomaterials
29
analysis characterization techniques such as X-ray diffraction and energy dispersive
spectroscopy (Loof et al., 2008). The bioactivity of a material depends on numerous
factors, among them the key factors are the chemical composition (presence of bioactive ions for instance Sr, Cu, Zn, F, and Mg), surface roughness or topography of
the material, and wettability of the material (Chan et al., 2017; Hoppe et al., 2011).
2.15
Osseointegration
It is defined as a direct anchorage or contact between the implant surface and bone
without any fibrous tissue in between that can be observed histologically
(Albrektsson and Johansson, 2001; De Meurechy et al., 2017). Osseointegration
depends on a number of factors, for instance (De Meurechy et al., 2017; Goharian
and Abdullah, 2017):
G
G
G
material related factors, such as biocompatibility, surface chemistry, roughness, topography, and laser ablation of material;
tissue related factors, such as bone quality and quantity; and
factors related to surgical procedures, including surgical trauma, sterilization, and primary
stability (De Meurechy et al., 2017).
Early in vitro assessment of the osteogenic differentiation was evaluated by measuring the in vitro activity of alkaline phosphatase (Chan et al., 2017).
Osseointegration is assessed in vivo by implantation of the material within the bone
of an animal model followed by micro-CT measurement to evaluate the bone volume density (Chan et al., 2017). Further assessments are done by evaluation of
bone implant histologically by assessment of new bone formation and the presence
of inflammatory cells (Chan et al., 2017).
2.16
Osteoinduction
The process by which the undifferentiated bone cells are stimulated to differentiate
into osteoblast cells or the process by which the bone formation is induced
(Albrektsson and Johansson, 2001). The materials reported to have osseoinductive
effects are poly-hydroxyethylmethacrylate, titanium, HA, biphasic calcium phosphate, carbonated apatite, and octacalcium phosphate (Barradas et al., 2010).
Implants with moderate surface roughness 12 μm are considered as optimal for
cell attachment. The bioactive glass fibers on the implant surface also improve
osseointegration (Chan et al., 2017).
2.17
Foreign body reaction
This is an inflammatory process and is marked by the deposition of an avascular
dense collagen capsule with inflammatory cells around the material or device that
is implanted (Trindade et al., 2016; Soto et al., 2018). These reactions are usually
30
Advanced Dental Biomaterials
reported with implant material or devices and less commonly it is associated with
local dressing materials (Tasoulas et al., 2017). The inflammatory cells that are
mainly present at the site of a foreign body reaction are monocytes, macrophages,
Langerhans, and giant cells (Vasiljević et al., 2018; Jordan et al., 2018). These reactions start as a result of an interaction between tissue fluid and blood with the material followed by an inflammatory reaction and granulated tissue formation (De
Meurechy et al., 2017). These reactions also lead to the degradation of the materials
as a result of which the material becomes brittle and more prone to physical damage (De Meurechy et al., 2017). The foreign body reaction is dependent on the
properties of the material, surface form, and topography of the biomaterial
(Vasiljević et al., 2018). The strategies that are employed to reduce the foreign
body reactions are to decrease surface porosity, incorporation of antiinflammatory
agents, and the release and delivery of growth factors (Soto et al., 2018).
2.18
Conclusive remarks
The properties of dental materials may vary vastly from one type to another.
Understanding the properties of dental biomaterials is important in order for comparison with the properties of the oral hard and soft tissues to be replaced. Ideally,
the biomaterials’ properties should closely match the properties of the lost tissues to
be replaced. For clinical performance and success, a biomaterial must pass the
required criteria for various physical, mechanical, and biological properties during
the characterization and testing phase.
References
Albrektsson, T., Johansson, C., 2001. Osteoinduction, osteoconduction and osseointegration.
Eur. Spine J. 10, S96S101.
Anusavice, K., Phillips, R., 2003. Phillips’ Science of Dental Materials. Saunders, St. Louis,
MO; Great Britain.
ASTM, 1996. 394-78, Standard test method for biaxial flexure strength (modulus of rupture)
of ceramic substrates. American Society for Testing and Materials, West Conshohocken,
PA (reapproved in 1996 and withdrawn in 2001).
ASTM, 2010. ASTM 695 Standard Test Method for Compressive Properties of Rigid
Plastics. ASTM Materials Standards.
ASTM Standard, 2007. Standard Test Methods for Determination of Fracture Toughness of
Advanced Ceramics at Ambient Temperature.
ASTM Standard, 2010. ASTMD790-10. Standard Test Methods for Flexural Properties of
Unreinforced and Reinforced Plastics and Electrical Insulating Materials. ASTM
International, West Conshohocken, PA.
ASTM Standard, 2014. ASTM D638-14 Standard Test Method for Tensile Properties of
Plastics; ASTM International. American Society for Testing and Materials, West
Conshohocken, PA.
Properties of dental biomaterials
31
Athanassiadis, B., George, G., Abbott, P., Wash, L., 2015. A review of the effects of formaldehyde release from endodontic materials. Int. Endod. J. 48, 829838.
Atia, G., May, J., 2013. Dental fluorosis in the paediatric patient. Dent. Update 40, 836839.
Barradas, A.M., Yuan, H., van Blitterswijk, C., Habibovic, P., 2010. Osteoinductive biomaterials: current knowledge of properties, experimental models and biological mechanisms. Eur. Cell. Mater. 21, 407429.
Basu, B., Katti, D.S., Kumar, A., 2010. Advanced Biomaterials: Fundamentals, Processing,
and Applications. John Wiley & Sons.
Braden, M., Clarke, R., 1974. Dielectric properties of zinc oxide-eugenol type cements. J.
Dent. Res. 53, 12631267.
Brady, A., Lee, H., Orlowski, J.A., 1974. Thermal conductivity studies of composite dental
restorative materials. J. Biomed. Mater. Res. 8, 471485.
Brauer, G., Termini, D., Burns, C., 1970. Characterization of components of dental materials and
components of tooth structure by differential thermal analysis. J. Dent. Res. 49, 100110.
Brown, W., Dewey, W., Jacobs, H., 1970. Thermal properties of teeth. J. Dent. Res. 49,
752755.
Buzalaf, M.A., Levy, S.M., 2011. Fluoride intake of children: considerations for dental caries
and dental fluorosis. Monogr. Oral Sci. 22, 119.
Cao, Y., Wang, B., 2009. Biodegradation of silk biomaterials. Int. J. Mol. Sci. 10, 15141524.
Carey, C.M., 2014. Focus on fluorides: update on the use of fluoride for the prevention of
dental caries. J. Evid. Based Dent. Pract. 14, 95102.
Carslaw, H.S., Jaeger, J.C., 1959. Conduction of Heat in Solids, second ed. Clarendon Press,
Oxford.
Chan, Y., Lew, W., Lu, E., Loretz, T., Lu, L., Lin, C., et al., 2017. An evaluation of the
biocompatibility and osseointegration of novel glass fiber reinforced composite
implants: in vitro and in vivo studies. Dent. Mater. 34, 470485.
Chitchumnong, P., Brooks, S.C., Stafford, G.D., 1989. Comparison of three- and four-point
flexural strength testing of denture-base polymers. Dent. Mater. 5, 25.
Cintra, L.T.A., Benetti, F., de Azevedo Queiroz, I.O., de Araujo Lopes, J.M., Penha de
Oliveira, S.H., Sivieri Araujo, G., et al., 2017. Cytotoxicity, biocompatibility, and
biomineralization of the new high-plasticity MTA material. J. Endod. 43, 774778.
Combe, E., Moser, J., 1978. The rheological characteristics of elastomeric impression materials. J. Dent. Res. 57, 221226.
Costa, M.F., 2016. Color vision sensation and perception. Front Psychol. 7, 1084.
Craig, R., Powers, J., 2002. Restorative Dental Materials. Mosby, St. Louis, MO; London.
Craig, R., Eick, J., Peyton, F., 1965. Properties of natural waxes used in dentistry. J. Dent.
Res. 44, 13081316.
Craig, R., Powers, J., Peyton, F., 1967. Differential thermal analysis of commercial and dental waxes. J. Dent. Res. 46, 10901097.
De Jager, N., de Kler, M., van der Zel, J.M., 2006. The influence of different core material
on the FEA-determined stress distribution in dental crowns. Dent. Mater. 22, 234242.
De Meurechy, N., Braem, A., Mommaerts, M., 2017. Biomaterials in temporomandibular
joint replacement: current status and future perspectives—a narrative review. Int. J. Oral
Maxillofac. Surg. 47, 518533.
Denbesten, P., Li, W., 2011. Chronic fluoride toxicity: dental fluorosis. Monogr. Oral Sci.
22, 8196.
de Souza Costa, C.A., Hebling, J., Scheffel, D.L., Soares, D.G., Basso, F.G., Ribeiro, A.P.,
2014. Methods to evaluate and strategies to improve the biocompatibility of dental materials and operative techniques. Dent. Mater. 30, 769784.
32
Advanced Dental Biomaterials
Fairhurst, C.W., Anusavice, K.J., Hashinger, D.T., Ringle, R.D., Warren Twiggs, S., 1980.
Thermal expansion of dental alloys and porcelains. J. Biomed. Mater. Res. 14,
435446.
Garcia Lda, F., Marques, A.A., Roselino Lde, M., Pires-de-Souza Fde, C., Consani, S., 2010.
Biocompatibility evaluation of Epiphany/Resilon root canal filling system in subcutaneous tissue of rats. J. Endod. 36, 110114.
Gerhardt, L., Boccaccini, A.R., 2010. Bioactive glass and glass-ceramic scaffolds for bone
tissue engineering. Materials 3, 38673910.
Goharian, A., 2017a. Further development of trauma plating fixation. In: Goharian, A. (Ed.),
Trauma Plating Systems. Elsevier.
Goharian, A., 2017b. General concepts. In: Goharian, A. (Ed.), Trauma Plating Systems.
Elsevier.
Goharian, A., Abdullah, M.R., 2017. 7—Bioinert Metals (Stainless Steel, Titanium, Cobalt
Chromium). Trauma Plating System. Elsevier, Amsterdam, pp. 115142.
Goldberg, M., 2008. In vitro and in vivo studies on the toxicity of dental resin components: a
review. Clin. Oral Investig. 12, 18.
Goldberg, M., 2016. Understanding Dental Caries: From Pathogenesis to Prevention and
Therapy. Springer.
Gorustovich, A.A., Roether, J.A., Boccaccini, A.R., 2009. Effect of bioactive glasses on
angiogenesis: a review of in vitro and in vivo evidences. Tissue Eng., B: Rev 16,
199207.
Grassmann, H., 1853. Zur theorie der farbenmischung. Annalen der Physik. 165, 6984.
Harrison, P.T., 2005. Fluoride in water: a UK perspective. J. Fluorine Chem. 126,
14481456.
Heintze, S.D., 2006. How to qualify and validate wear simulation devices and methods.
Dent. Mater. 22, 712734.
Heintze, S.D., Faouzi, M., Rousson, V., Ozcan, M., 2012. Correlation of wear in vivo and six
laboratory wear methods. Dent. Mater. 28, 961973.
Herfort, T.W., Gerberich, W.W., Macosko, C.W., Goodkind, R.J., 1977. Viscosity of elastomeric impression materials. J. Prosthet. Dent. 38, 396404.
Hoppe, A., Güldal, N.S., Boccaccini, A.R., 2011. A review of the biological response to ionic
dissolution products from bioactive glasses and glass-ceramics. Biomaterials 32,
27572774.
Husain, S., Al-Samadani, K.H., Najeeb, S., Zafar, M.S., Khurshid, Z., Zohaib, S., et al.,
2017. Chitosan biomaterials for current and potential dental applications. Materials 10,
602.
International Standards Organization, 2000. ISO 4049 Dentistry-Polymer-Based Filling,
Restorative and Luting Materials. International Organization for Standardization,
Geneva, Switzerland.
ISO, 2001. Dental materials—guidance on testing of wear—Part 2: Wear by two-and/or three
body contact. In: Technical Specification; No. 14569-14572.
ISO, 2002. ISO14577-1: metallic materials—instrumented indentation test for hardness and
materials. In: ISO/TC 164/SC 3.
Javed, F., Vohra, F., Zafar, S., Almas, K., 2014. Significance of osteogenic surface coatings
on implants to enhance osseointegration under osteoporotic-like conditions. Implant.
Dent. 23, 679686.
Jordan, S.W., Fligor, J.E., Janes, L.E., Dumanian, G.A., 2018. Implant porosity and the foreign body response. Plast. Reconstr. Surg. 141, 103e112e.
Properties of dental biomaterials
33
Jorge, J.H., Giampaolo, E.T., Machado, A.L., Vergani, C.E., 2003. Cytotoxicity of denture
base acrylic resins: a literature review. J. Prosthet. Dent. 90, 190193.
Klein, G.A., Meyrath, T., 2010. Industrial Color Physics. Springer.
Lacerda-Santos, R., de Meneses, I.H., de Morais Sampaio, G.A., Pithon, M.M., Alves, P.M.,
2015. Effect of degree of conversion on in vivo biocompatibility of flowable resin used
for bioprotection of mini-implants. Angle Orthod. 86, 157163.
Levine, M., 2010. Topics in Dental Biochemistry. Springer Science & Business Media.
Lisanti, V., Zander, H., 1950. Thermal conductivity of dentin. J. Dent. Res. 29, 493497.
Loof, J., Svahn, F., Jarmar, T., Engqvist, H., Pameijer, C.H., 2008. A comparative study of
the bioactivity of three materials for dental applications. Dent. Mater. 24, 653659.
López Camelo, A.F., Gómez, P.A., 2004. Comparison of color indexes for tomato ripening.
Hortic. Bras. 22, 534537.
Martı́nez-Mier, E.A., 2012. Fluoride its metabolism, toxicity, and role in dental health. J.
Evid. Based Complement. Alternat. Med. 17, 2832.
Mausfeld, R., 1998. 12. Color perception: from Grassmann codes to a dual code for object
and illumination colors. In: Color Vision: Perspectives From Different Disciplines.
Walter de Gruyter Berlin, New York, p. 231.
McCabe, J.F., Walls, A.W.G., 2008. Applied Dental Materials. Blackwell, Oxford.
McGrady, M.G., Ellwood, R.P., Pretty, I.A., 2010. Why fluoride? Dent. Update 37,
595598. 601602.
Moharamzadeh, K., Brook, I.M., Van Noort, R., 2009. Biocompatibility of resin-based dental
materials. Materials 2, 514548.
Mumford, J.M., 1967. Resistivity of human enamel and dentine. Arch. Oral Biol. 12,
925927.
Najeeb, S., Khurshid, Z., Zafar, M.S., Khan, A.S., Zohaib, S., Martı́, J.M.N., et al., 2016a.
Modifications in glass ionomer cements: nano-sized fillers and bioactive nanoceramics.
Int. J. Mol. Sci. 17, E1134.
Najeeb, S., Khurshid, Z., Zohaib, S., Zafar, M.S., 2016b. Bioactivity and osseointegration of
PEEK are inferior to those of titanium—a systematic review. J. Oral Implantol. 42,
512516.
Nayyer, M., Zahid, S., Hassan, S.H., Mian, S.A., Mehmood, S., Khan, H.A., et al., 2018.
Comparative abrasive wear resistance and surface analysis of dental resin-based materials. Eur. J. Dent. 12, 5766.
Perrotti, V., Piattelli, A., Quaranta, A., Gómez-Moreno, G., Iezzi, G., 2017. Biocompatibility
of dental biomaterials. In: Shelton, R. (Ed.), Biocompatibility of Dental Biomaterials.
Woodhead Publishing.
Peyton, F., 1952. Temperature rise and cutting efficiency of rotating instruments. New York
DJ. 18, 439.
Peyton, F., 1958. Effectiveness of water coolants with rotary cutting instruments. J. Am.
Dent. Assoc. 56, 664675.
Phillips, L.J., Phillips, R.W., Schnell, R.J., 1955. Measurement of the electric conductivity of
dental cement: IV. Extracted human teeth; in vivo tests; summary. J. Dent. Res. 34,
839848.
Powers, J., Craig, R., 1974. Penetration of commercial and dental waxes. J. Dent. Res. 53,
402409.
Qasim, S.B., Zafar, M.S., Najeeb, S., Khurshid, Z., Shah, A.H., Husain, S., et al., 2018.
Electrospinning of chitosan-based solutions for tissue engineering and regenerative medicine. Int. J. Mol. Sci. 19, 407.
34
Advanced Dental Biomaterials
Sakaguchi, R.L., Powers, J.M., 2012. Craig’s Restorative Dental Materials. Elsevier/Mosby,
Philadelphia, PA.
Schmalz, G., 2009a. Biocompatibility of Dental Materials. Springer, Berlin; London.
Schmalz, G., 2009b. Resin-based composites. In: Schmalz, G., Arenholt-Bindslev, D. (Eds.),
Biocompatibility of Dental Materials. Springer Berlin Heidelberg, Berlin, Heidelberg.
Schmalz, G., 2014. Strategies to improve biocompatibility of dental materials. Curr. Oral
Health Rep. 1, 222231.
Scully, C., 2011. Oral cancer aetiopathogenesis; past, present and future aspects. Med. Oral
Patol. Oral Cir. Bucal 16, e306e311.
Setcos, J.C., Babaei-Mahani, A., Silvio, L.D., Mjor, I.A., Wilson, N.H., 2006. The safety of
nickel containing dental alloys. Dent. Mater. 22, 11631168.
Soares, A.S., Scelza, M.Z., Spoladore, J., Gallito, M.A., Oliveira, F., Moraes, R.C.M., et al.,
2018. Comparison of primary human gingival fibroblasts from an older and a young
donor on the evaluation of cytotoxicity of denture adhesives. J. Appl. Oral Sci. 26,
e20160594.
Soto, R.J., Merricks, E.P., Bellinger, D.A., Nichols, T.C., Schoenfisch, M.H., 2018. Influence
of diabetes on the foreign body response to nitric oxide-releasing implants. Biomaterials
157, 7685.
Tadin, A., Gavic, L., Zeravica, A., Ugrin, K., Galic, N., Zeljezic, D., 2018. Assessment of
cytotoxic and genotoxic effects of conventional and whitening kinds of toothpaste on
oral mucosa cells. Acta Odontol. Scand. 76, 6470.
Tasoulas, J., Daskalopoulos, A., Droukas, C., Nonni, A., Nikitakis, N.G., 2017. An unusual
microscopic pattern of foreign body reaction as a complication of dry socket management. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 125, e118e123.
Tay, W., Braden, M., 1981. Materials science: dielectric properties of glass ionomer cements.
J. Dent. Res. 60, 13111314.
Tay, W., Braden, M., 1987. Thermal diffusivity of glass-ionomer cements. J. Dent. Res. 66,
10401043.
Tenuta, L.M.A., Cury, J.A., 2010. Fluoride: its role in dentistry. Braz. Oral Res. 24, 917.
Tillberg, A., Jarvholm, B., Berglund, A., 2008. Risks with dental materials. Dent. Mater. 24,
940943.
Tinanoff, N., O’Sullivan, D., 1997. Early childhood caries: overview and recent findings.
Pediatr. Dent. 19, 1216.
Trindade, R., Albrektsson, T., Tengvall, P., Wennerberg, A., 2016. Foreign body reaction to
biomaterials: on mechanisms for buildup and breakdown of osseointegration. Clin.
Implant. Dent. Relat. Res. 18, 192203.
Ullah, R., Zafar, M.S., 2015. Oral and dental delivery of fluoride: a review. Fluoride 48,
195204.
Ullah, R., Sohail Zafar, M., Shahani, N., 2017. Potential fluoride toxicity from oral medicaments: a review. Iran. J. Basic Med. Sci. 20, 841848.
Vaderhobli, R.M., 2011. Advances in dental materials. Dent. Clin. North Am. 55,
619625. x.
Vallittu, P.K., Boccaccini, A.R., Hupa, L., Watts, D.C., 2018. Bioactive dental materials—do
they exist and what does bioactivity mean? Dent. Mater. 34, 693694.
Van Noort, R., Barbour, M.E., 2013. Introduction to Dental Materials 4. Elsevier Health
Sciences.
Vanzillotta, P.S., Sader, M.S., Bastos, I.N., Soares Gde, A., 2006. Improvement of in vitro
titanium bioactivity by three different surface treatments. Dent. Mater. 22, 275282.
Properties of dental biomaterials
35
Vasconcelos, A., Freddi, G., Cavaco-Paulo, A., 2008. Biodegradable materials based on silk
fibroin and keratin. Biomacromolecules 9, 12991305.
Vasiljević, P.J., Živković, J., Vukelić-Nikolić, M., Najman, S., 2018. Determining the biological properties of biomaterials in vivo. Anonymous Biomaterials in Clinical Practice.
Springer.
Vermilyea, S., Powers, J., Koran, A., 1978. The rheological properties of fluid denture-base
resins. J. Dent. Res. 57, 227231.
Wataha, J.C., 2001. Principles of biocompatibility for dental practitioners. J. Prosthet. Dent.
86, 203209.
Wataha, J., Lockwood, P., Nelson, S., Rakich, D., 1999. In vitro cytotoxicity of dental casting alloys over 8 months. J. Oral Rehabil. 26, 379387.
Welch, K., Cai, Y., Engqvist, H., Stromme, M., 2010. Dental adhesives with bioactive and
on-demand bactericidal properties. Dent. Mater. 26, 491499.
Wilson, T., Turner, D., 1987. Characterization of polydimethacrylates and their composites
by dynamic mechanical analysis. J. Dent. Res. 66, 10321035.
Zafar, M.S., 2013. Effects of surface pre-reacted glass particles on fluoride release of dental
restorative materials. World Appl. Sci. J. 28, 457462.
Zafar, M.S., 2014. A comparison of dental restorative materials and mineralized dental tissues for surface nanomechanical properties. Life Sci. J. 11, 1924.
Zafar, M.S., 2018. Wear behavior of various dental restorative materials. Mater. Technol. 33,
2531.
Zafar, M.S., Ahmed, N., 2014a. Nanoindentation and surface roughness profilometry of poly
methyl methacrylate denture base materials. Technol. Health Care 22, 573581.
Zafar, M.S., Ahmed, N., 2014b. Nanomechanical characterization of exfoliated and retained
deciduous incisors. Technol. Health Care 22, 785793.
Zafar, M.S., Ahmed, N., 2014c. Effects of wear on hardness and stiffness of restorative dental materials. Life Sci. J. 11, 1118.
Zafar, M.S., Al-Samadani, K.H., 2014. Potential use of natural silk for bio-dental applications. J. Taibah Univ. Med. Sci. 9, 171177.
Zafar, M.S., Ahmed, N., 2015a. Therapeutic roles of fluoride released from restorative dental
materials. Fluoride 48, 184194.
Zafar, M.S., Ahmed, N., 2015b. The effects of acid etching time on surface mechanical properties of dental hard tissues. Dent. Mater. J. 34, 315320.
3
Dental gypsum and investments
Touraj Nejatian1,2, Pegah Firouzmanesh3 and Azeem Ajaz4
1
Eastman Dental Institute, University College of London, London, United Kingdom,
2
Nottingham Dental Clinic, Nottingham, United Kingdom, 3Babol University of Medical
Sciences, Babol, Iran, 4Department of Prosthodontics and Dental Implantology, College of
Dentistry, King Faisal University, Al-Ahsa, Kingdom of Saudi Arabia
Chapter Outline
3.1
3.2
3.3
3.4
3.5
Introduction 37
Desirable properties of gypsum products 38
Production of calcium sulfate hemihydrate 38
Types of gypsum products 40
The setting and manipulation characteristics of gypsum products
3.5.1
3.5.2
3.5.3
3.5.4
42
Mixing technique 42
Pouring the impression 43
The setting processes 44
Setting time 46
3.6 Setting expansion hygroscopic setting expansion 47
3.6.1
3.6.2
3.6.3
3.6.4
3.6.5
Reproduction of detail 49
Compressive strength 49
Tensile strength 50
Surface hardness and abrasion resistance 50
Dimensional stability 51
3.7 Dies and models produced from digital data
3.8 Conclusion 52
References 52
3.1
51
Introduction
Replicas of oral tissues are used in dentistry for the purpose of assessment, treatment planning, and manufacturing indirect restorations. They may also be used as
part of medicolegal records. These replicas are called Study Models when used for
assessment and treatment planning, whereas the ones used for manufacturing
removable appliances are classified as Casts. Dies are the third type and are more
accurate replicas which are used for making fixed restorations. The accuracy of the
replicas depends on the accuracy of both the impression and the replica materials.
Various materials are used to pour the impressions including gypsum products and
epoxy materials. Recently, polymers are being used by novel three-dimensional
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00003-7
Copyright © 2019 Elsevier Ltd. All rights reserved.
38
Advanced Dental Biomaterials
(3D) printing systems to make replicas. Gypsum products are the most commonly
used material to pour the impressions due to their versatile nature. There are five
types of gypsum products with the same chemical composition but differing physical
forms with different properties for different applications.
3.2
Desirable properties of gypsum products
A true replica of oral tissue is required to be reasonably accurate and dimensionally
stable to enable making an accurate restoration; however, the degree of accuracy
required varies depending on the application. For example, indirect fixed restoration
should be made with high accuracy and fine details, whereas a moderate level of
accuracy is acceptable for most of the study models. Strength, hardness, and resistance against scratching are other important properties of gypsum materials, especially for die materials as they are prone to damage during handling in a dental lab.
Compatibility with impression material is another requirement of the replica materials
as poor compatibility may result in imperfection in the replicas. Finally, like many
other materials in the clinical environment, gypsums should have a long shelf life,
short setting time, be easy and safe to use, inexpensive, and be easy to dispose of or
recycle. Gypsum products of five different types have a range of properties to meet
the various clinical needs, which have made it the most popular replica material in
dentistry.
For gypsum investment materials, the desirable properties should be same as
above along with some more detailed features (Luk and Darvell, 1991; Anusavice,
2013; Asaoka et al., 2012; Luk and Darvell, 2003):
G
G
G
G
G
G
G
G
G
G
Sufficient strength at room temperature and high temperatures to withstand the impact of
molten metal.
Easy to manipulate and become hard in a reasonably short period of time.
Stable and resistant to higher temperatures to prevent damage to the surface of the alloy
by releasing gas.
Sufficient expansion to compensate the shrinkage of the wax pattern and metal alloys.
Beneficial thermal expansion over a range of other casting temperatures.
Enough porosity to let off the gases produced during casting procedures.
Preserve all the fine details and margins.
Easily separated from the surface of the metal.
No chemical reaction with casting metals.
Inexpensive.
3.3
Production of calcium sulfate hemihydrate
The main constituent of gypsum-based products, including plasters and dental
stones, is calcium sulfate hemihydrate (CaSO4 1/2H2O) or [2(CaSO4) H2O]. As
gypsum is in the form of dihydrate calcium sulfate (CaSO4 2H2O), in order to
Dental gypsum and investments
39
produce calcium sulfate hemihydrate, first gypsum is crushed and milled and then
exposed to heat at 110 C 120 C (230 F 250 F) in order to lose three-fourths of
its water. Losing this amount of water is essential for the conversion of
CaSO4 2H2O to CaSO4 1/2H2O (calcium sulfate hemihydrate). This process is the
first stage of the calcination reaction (Table 3.1).
Based on the calcination method, different types of hemihydrate may be
produced. These types are known as α-hemihydrate and β-hemihydrate. Application
of the α and β prefixes does not represent different substance phases, rather these
prefixes are used only due to tradition and their easy use. Indeed, the α and β types
are not different in terms of crystal shape, rather their difference lies in the crystal
size, surface area, and the extent of network perfectness.
If gypsum is exposed up to 120 C under dry calcination in an open space, a
hemihydrate crystalline species is produced called β-hemihydrate. The β form, also
known as dental plaster, consists of large crystals and irregular orthorhombic particles with capillary pores. If gypsum is heated under pressure in the presence of
water vapor up to around 125 C, α-hemihydrate is formed. The α form, also known
as dental stone, is composed of crystal particles with a smaller size and more
irregular prismatic shape. The chemical reaction during the manufacturing and
setting reaction of all types of gypsums is exactly the same (Fig. 3.1).
When α-hemihydrate is mixed with water, reaction 1 (Fig. 3.1) is reversed.
The product is far stronger and harder than the one obtained from mixing
β-hemihydrate with water. The main reason for this difference is that β-hemihydrate
particles absorb more water, as their crystals have a more irregular shape and are
more porous. Although the particle size and sum of the surface area are the main
factors in measuring the water content required for mixing, particles with different
sizes should be scattered uniformly in the mixture. Pulverizing the particles after
hemihydrate preparation removes needle-like crystals, causing the crystals to stand
together more densely, thereby decreasing the level of water required for mixing.
Attachment and adhesion among hemihydrate particles are also important factors in
determining the water required for pourable products. Adding trace amounts of
some materials with an active surface such as Arabic Gum along with calcium carbonate can considerably decrease the extent of water required in gypsum products.
Therefore different gypsum products need different amounts of water and the extent
of this need can be estimated based on the shape and density of crystals. It is worth
Table 3.1 Calcination process for gypsum.
CaSO4.2H2
O
gypsum
(calcium
sulfate
dihydrate)
110120°c
130200°c
CaSO4.1/2H2O
Plaster or stone
(calcium sulfate
hemihydrate)
2001000°
c
CaSO4
Hexagonal
anhydrate
CaSO4
(orthorhombic
anhydrite)
40
Advanced Dental Biomaterials
Figure 3.1 Chemical reaction of gypsum during (1) manufacturing (gray box) and (2) setting
process (reverse reaction).
noting that these factors are adjusted and calculated by the manufacturer company. Modified α-hemihydrate is obtained through heating gypsum in an aqueous
solution of calcium chloride 30%. These particles are denser than the two previous types and need less water for mixing. The obtained powder is used in
synthesized dyes. Modified α-hemihydrate is also known as die stone or modified
stone (Worner, 1944).
3.4
Types of gypsum products
Selecting a particular type of gypsum product depends on its use and the required
physical properties for that purpose. Gypsum products are categorized into following
five types (Fig. 3.2):
1. Type I: Impression plaster
Today, impression plasters are rarely used. Their uses include initial molding from
toothless ridges to make denture (mucostatic impression).
2. Type II: Model plaster
Model plaster or Type II is a type of β-hemihydrate, which is used to prepare initial
diagnostic and after-treatment models, fill in the flasks when making dentures, and mount
the casts in the articulator. With low compressive strength and tensile strength, model
plaster is considered a relatively weak substance.
3. Type III: Dental stone
In 1930 with the discovery and introduction of α-gypsum into dentistry, a new area
began. The fabricated gypsum, made under vapor pressure in a closed-lid container,
results in a slower outflow of water off the crystals and the development of powdered particles with a uniform shape and less porosity. This substance is harder than the β type.
Dental gypsum and investments
41
Figure 3.2 Different types of gypsum products.
Thus in the vicinity of hydrocolloid molding materials, it loses its superficial strength to a
lesser extent and allows for fabricating indirect pattern. Dental stone is suitable for synthesizing acrylic dentures and making diagnostic casts.
4. Type IV: Dental stone, high strength
Stone Type IV is a modified α-hemihydrate which is obtained by calcination of gypsum in calcium chloride solution and has very dense and cubic-shaped particles. They
have a great strength, hardness, and resistance to abrasion, while their setting expansion is
low. As a result, they are suitable for preparing die.
5. Type V: Dental stone, high strength, high expansion
Dental stone Type V has the maximum compressive strength. In this type, expansion
occurs during setting leading to a larger mold, which compensates for the solidification
shrinkage of base-metal alloys during the later casting (Mccabe and Walls, 2013)
(Fig. 3.3).
42
Advanced Dental Biomaterials
Figure 3.3 Setting expansion of Type V gypsum utilized to compensate for solidification
shrinkage of base-metal alloys during casting.
3.5
The setting and manipulation characteristics of
gypsum products
The technique to use gypsum products is relatively simple. The required equipment includes mixing bowl, mixing spatula, room-temperature water, and correct
powder/water ratio. To achieve the optimum properties powder and water should
be mixed with each other at the correct ratio. It is important that the mixing bowl
and other mixing equipment used for dental gypsum be used only for mixing
dental gypsum. Use of this equipment for mixing phosphate investment or molding
substances causes contamination that may alter the dental stone properties later. It is
also important that all mixing equipment be cleaned after the job and no dry gypsum
remains on the bowl or spatula.
3.5.1 Mixing technique
3.5.1.1 Measuring the water
The best outcome is obtained by distilled water, though mixing with normal tap water
also leads to favorable results. The water should be at ambient temperature. Water is
usually measured by a graduated cylinder, as 1 g water has almost a volume of 1 mL.
3.5.1.2 Measuring the powder
The powder weight is measured by an accurate scale. The powder volume should
not be measured by a cup, as different powders become dense at different levels.
Dental gypsum and investments
43
3.5.1.3 Adding powder and water
The preferred method for mixing involves adding the measured level of water
into the container. Then, the preweighed powder should be gradually added to
it. Approximation-based addition of water and gypsum for reaching the desired
consolidation should be avoided, as it can result in a low strength and inconsistent expansion. Gypsum should be added to water slowly to avoid entrapment of
large amounts of air. The powder should be left to soak in water for at least
30 seconds while moving the bowl around to wet the powder before mixing.
Using hand mixing, back and forth strokes are used. Typically, the bowl is
rotated so that all nonmixed and dry substances enter the mixture. This continues until a creamy homogenous mixture is obtained. Mechanical mixing
accelerates the setting reaction and reduces work and setting time of gypsums.
The strength and hardness obtained under conditions where mixing is done
mechanically and in a vacuum are usually greater than when mixing has been
done by hand. As mechanical mixers are faster, the powder is added to water
and it is stirred by hand until complete soaking of powder. It is then placed in a
mechanical mixer and is mixed for a shorter time of 10 30 seconds (Mccabe
and Walls, 2013).
3.5.2 Pouring the impression
It begins by holding the impression tray so that the handle rests against the vibrator.
Start at one end of the arch and place a small amount of gypsum mixture into the
impression letting it flow slowly enough to fill each tooth imprint one after another.
After the impression is filled, the remaining bubbles should be popped with a small
instrument. After covering all the critical surfaces of the impression, you may safely
add progressively the larger amount of the mix. Do not flow stone over the outside
of the tray, because it must be removed before the impression can be separated
from the cast. Now let this first pour set for about 45 minutes or at least until the
stone loses its glazed appearance before making the cast base. Continue filling the
impression stone to the level slightly above the height of the impression walls
(about 2 mm thick). Lastly, add retention nodules to this first pour to retain the base
mechanically. Place the handle of the tray in a holding device; do not lay the
impression on the counter or the cast will be distorted. Add stone around the retention nodules and invert the first pour into the patty. Use your spatula to shape the
sides of the cast base. Take care not to bring stone up onto the tray embedding
the tray into the base. With a mandibular cast, you must take time to smooth and
contour the tongue space while the second mix is still soft. There is a rate of vibration that is best for each mix’s ability to flow. The vibration intensity should be set
high enough to make the material move across the surface of the impression. If the
vibrator is set too high the impression “jumps” in your hand and gypsum moves so
fast that it skips over surface detail, or vibration wave patterns develop on the
surface of the mix (O’Brien, 2008).
44
Advanced Dental Biomaterials
3.5.3 The setting processes
The precursor substance for production of casts and gypsum models and some casting
investments and molding gypsum is calcium sulfate hemihydrate, which is converted to
calcium sulfate dehydrate through an exothermic reaction when setting (Fig. 3.4).
Three theories of gypsum setting exist:
1. crystalline 5 dissolution 2 precipitation;
2. gel; and
3. hydration.
Nowadays, the most accepted theory is crystalline theory, which is based on the
dissolution of hemihydrate powder and instant recrystallization of gypsum followed
by the interlocking of the crystal to form the set solid. Calcium sulfate dehydrate
has a relatively low solubility compared to calcium sulfate hemihydrate, which
causes the setting of these substances. When hemihydrate powder is mixed with a
proper ratio of water, it changes into a thick slurry. Dissolution of hemihydrate
continues until it turns into a saturated solution. Thereafter, the saturated solution
of hemihydrate mixes with water and converts to supersaturated dehydrate mixture
and precipitates as needle-like crystals of nucleation type in the solution. At room
temperature (20 C), the solubility of hemihydrate is four times greater than that of
dehydrate forms. With the precipitation of calcium sulfate dehydrate, the solution is
no longer saturated with hemihydrate. Thus hemihydrate continues to dissolve.
Next, while new crystals are being formed or previous crystals are growing further,
the dissolution of hemihydrate and precipitation of the dehydrate form continues.
The links of the needle-like crystals which have been distorted cause the final
consistent structure (Docking, 1965; Winkler et al., 1998).
3.5.3.1 Stages of setting
The setting process is continuous, from the beginning of mixing until the setting
reaction is complete, by which time the material has reached its full wet strength.
However, important physical changes can be recognized during this process. The
stages in setting may be described as fluid, plastic, friable, and carvable.
3.5.3.2 The rate of setting reaction
G
G
G
G
G
Water/powder ratio (W/P ratio)
Spatulation
Temperature
Colloidal system and pH
Additives: (1) accelerates and (2) retarders
Figure 3.4 Setting reaction of calcium sulfate hemihydrate.
Dental gypsum and investments
45
3.5.3.3 Water/powder ratio
In general, the effects of using less water (less W/P ratio) can be summarized as
follows:
G
G
G
G
G
thickening of the mixture and making it harder to work;
retaining more air bubbles by reducing the amount of water to fill the space between
particles;
strengthening of the mixture;
enhancing the dimensional changes; and
decreasing the number of nuclei per unit resulting in a longer setting time.
3.5.3.4 Spatulation
The setting time will be shorter by prolonging and increasing the rate of gypsum
mixing. This is probably due to the fact that when the stone or plasters are in contact with water, some gypsum crystals will form immediately. The formation of
these crystals increases with the onset of mixing. At the same time, the crystals are
broken down through spatula stirrer and dispersed within the mixture, causing an
increase in the number of crystalline nuclei and thus shortening the setting time
(Mccabe and Walls, 2013).
3.5.3.5 Temperature
Increasing temperature has complex effects on the setting time of gypsum products,
including a decrease in the relative solubility of calcium sulfate hemihydrate and
calcium sulfate dihydrate. Reducing the lower solubility ratio leads to a slower
reaction and longer setting times. On the other hand, increasing the temperature
will accelerate the reaction rate and shorten the setting time. In practice the effects
of these two phenomena accumulate together, to reveal the overall effect.
Increasing the temperature to about 40 C enhances the solubility of hemihydrate
and thus accelerates the setting reaction. Increasing the temperature over 40 C leads
to a decrease in the solubility of hemihydrate and slows down the setting reaction
until the solubility of hemihydrate and dihydrate is equal at 100 C, where no reaction occurs and the plasters will not set (Singh and Garg, 1997).
3.5.3.6 Modifying agents
One of the methods of controlling the setting time is adding certain modifiers to
the dental stone and plaster mix. If the added chemical reduces the setting time, it
will be known as an accelerator, and if it increases the setting time, it will be
considered as a retarder. The retarders usually reduce the solubility of a layer
absorbed on the surface of the hemihydrate and prevent further growth of the
gypsum crystals by coating their surface. The organic materials such as glues,
gelatin, and some gums act in this manner. Other types of retarders consist of salts
forming a layer of calcium salt on the plaster surface, which is less soluble in
comparison to sulfate, including borax, potassium citrate, and calcium chloride. It
should be noted that many alkaline mineral salts, such as sodium chloride, act as
46
Advanced Dental Biomaterials
accelerators in low concentrations but as retarders in high concentrations (more
than 20%). Less than 2% potassium sulfate or sodium chloride can be added to
the gypsum mixture to accelerate the setting reaction rate and reduce the setting
time. The gypsum is usually appended by adding a small amount of slurry to the
water, but not a lot of powder to accelerate the reaction because it will be very
difficult to produce a mixture with the desired viscosity. It is better to choose a
product that essentially has longer setting time when a prolonged setting time is
required. It should be kept in mind that the use of colder water has no major effect
on the setting time. To ensure achieving the longest working time, it is better,
therefore, to use a product with a regular setting time or to use the shortest time
and rate of mixing.
3.5.3.7 Fineness
Minimizing the size of hemihydrate particles leads to an increase in the hemihydrate dissolution rate, the number of gypsum nuclei and setting rate.
3.5.3.8 Effect of pH
Fluids with a low pH (such as saliva) delay the setting reaction (Earnshaw and
Marks, 1964). If the mold taken from the patient’s mouth is not washed properly
and is still contaminated with saliva, it will slow down the setting reaction.
3.5.4 Setting time
3.5.4.1 Initial setting time
Initial setting time or working time is the interval between the onset of mixing and
the setting mass reaching the semihard stage. Initial setting time is clinically the
period when the plaster loses its gloss.
3.5.4.2 Final setting time
This is the interval between the start of mixing the powder and water to the completion
of the substance reaction and setting, when the material can be removed from the mold
without deformation or break. The final setting time is chemically the period when all
water required for hydration is consumed by hemihydrate.
The following tests are used to measure the setting time:
G
G
Loss of gloss
As the reaction progresses, part of the excess water is absorbed and the dihydrate is
produced; as a result, the mixture loses its gloss. This happens usually in the ninth minute,
but the plaster setting is still incomplete and cannot be removed from the mold.
Initial Gilmore test
In the initial Gilmore test the mixture is spread over the target area and the needle is
placed on the surface. The initial setting time will be when the needle no longer makes
any track on the material surface.
Dental gypsum and investments
G
47
Vicat test for setting time
A needle with a diameter of 1 mm and a pressure of 300 g is used in this test. The
setting time is obtained when the needle no longer penetrates to a depth of 2 mm in the
material. This test can be also employed to control the quality of the mixture.
The measurement of Vicat and initial Gilmore occur simultaneously in some cases,
while there is a little difference at other times.
3.5.4.3 Gilmore test for final setting time
This is similar to the initial Gilmore test, but a heavier Gilmore needle is used. The
final setting time will be when the needle leaves an only minor barely visible
trace on the surface (Dental Science, 2017; Sanad et al., 1982; Williams and
Williams, 1984).
3.6
Setting expansion hygroscopic setting expansion
Gypsum products, when mixed with water and allowed to set, exhibit measurable
linear expansion along their extremities, which is known as “normal setting expansion.” When during setting additional water is brought into contact, an increased
expansion is observed due to the outward thrust of the growing crystals. This
phenomenon of expansion is known as “hygroscopic setting expansion” (Mahler
and Bruce Ady, 1960). All gypsum products show some linear expansion, the
percentage of this expansion varies from one type of gypsum product to another
(Table 3.2).
Under normal conditions the round particles of hemihydrate are surrounded by
water and the crystals of dihydrate begin to form on the nuclei (Mahler and Bruce
Ady, 1960; Lyon et al., 1955). Hydration helps reduce water around the particles
while the surface tension of water draws the particles closer. The crystals of dihydrate begin to grow and contact each other, further decreasing the water around the
particles. Furthermore, water is also consumed by dihydrate growth which should
bring the crystals closer as before, but the outward thrust of the growing crystals
repels this contraction and ultimately the crystals are entangled and intermeshed
(Mahler and Bruce Ady, 1960; Lyon et al., 1955). Consequently, gypsum products
when setting under water have been observed with more setting expansion than
gypsum products which set under air (Fig. 3.5).
Table 3.2 Setting expansion by volumetric percentage of different gypsum products when
mixed with water.
Gypsum products
Setting expansion (%)
Plaster
Low moderate strength dental stone
High-strength dental stone
High-strength, high-expansion dental stone
0.2 0.3
0.15 0.25
0.08 0.10
0.10 0.20
48
Advanced Dental Biomaterials
I
Water
1
2
II
3
Water
Water
Water
1
2
3
Figure 3.5 Illustration of the setting expansion of gypsum products. (I) The gypsum product
is mixed with water and left to set. The crystal growth is restricted by the surface tension of
water surrounding the growing crystals. (II) Hygroscopic expansion occurred when the
mixture is exposed to water during the setting reaction which provides room for longer
crystal growth (Mahler and Bruce Ady, 1960).
The hygroscopic setting expansion is purely a physical phenomenon and is not a
result of any chemical reaction other than the normal setting expansion. Therefore
variables that will have an effect on normal setting expansion will be liable for
changes in hygroscopic expansion as well. For example, the higher hygroscopic
expansion will be a result of a reduction in W/P ratio and increased speculation
(Cesar et al., 2015; Cunningham et al., 1952; Garber et al., 1985). The hygroscopic
expansion achieved during the setting of dental plaster or stone is double the time
compared to the normal setting expansion. The higher hygroscopic expansion is
required for gypsum-bonded casting investments used in the fabrication of cast gold
alloy restorations. Other investment materials have also shown a similar expansion
pattern when they set under hydrated conditions (Michalakis et al., 2009).
It is important to note that hygroscopy is the ability of a substance to attract
water molecules from the environment either by absorption or adsorption. For gypsum products, the hygroscopic expansion that has been described here is not a result
of absorption or adsorption and, therefore, the term hygroscopic setting expansion
is technically incorrect (Mahler and Bruce Ady, 1960; Michalakis et al., 2009).
Nevertheless this term will be used whenever explaining the setting expansion of
gypsum.
Dental gypsum and investments
49
3.6.1 Reproduction of detail
The American National Standards Institute/American Dental Association Specification
nos. 19 and 25 evaluate the compatibility of impression materials with dental stone
by the presence of a 20-μm-wide line produced on a dental stone cast of calcium
sulfate dehydrate (ADA, 1972, 1977). Surface details less than 20 μm are not
recorded due to the porous nature of gypsum products, but macroscopic details are
very well reproduced. There is some loss of surface details contributed by the
production of air bubbles. It is advisable to use surface vibration and tapping techniques while pouring a cast to reduce air bubbles. Since the gypsum is soluble in
water in minute degrees, care must be taken to avoid repeated drying and wetting
of the surface when waxing up a mold for casting (Malaviya and Shrestha, 2016). It
has been well established that gypsum dies do not reproduce surface details better
than electroformed or epoxy dies due to their surface being porous at the microscopic level. There have been surface details record issues when silicon impressions
are used as the gypsum does not wet these materials (Chang et al., 2016). Therefore
nonionic surfactants are used to improve the wettability of these impression materials
by water slurry. Contamination with saliva or blood can also affect surface detail
reproduction. Therefore care must be taken when pouring impressions with gypsum
to achieve good surface details.
3.6.2 Compressive strength
The most common mechanical property for assessing the strength of gypsum
products is the compressive strength. The compressive strength decreases from
high-strength dental stone at 38 MPa to model stone at 30 MPa and down to plaster
at 12 MPa (Noort and Barbour, 2013). The compressive strength is inversely
proportional to the W/P ratio. The greater the amount of water used to mix, the lower
is the compressive strength. Model plaster with a greater quantity of excess water
exhibits a compressive strength of 12 MPa, whereas high-strength dental stone consisting of the least amount of excess water has a compressive strength around
38 MPa. The excess water only contributes to the volume and not the strength of
the material (Earnshaw and Smith, 2009; Peyton et al., 1952; Noort, 2002). For
example, if the stone is mixed with the same W/P ratio as model plaster its strength
will be decreased to similar to that of the model plaster (Fig. 3.6). Thus the compressive strength of the set material is affected significantly if the recommended
powder liquid ratio is not used. More water has the advantage of a uniform mix and
air bubbles can be easily released by vibration action, but compressive strength
becomes inferior. On the other hand, using less water makes a thick mix incorporated
with air which in turn increases the porosity and significantly reduces the overall
strength. Therefore it is highly recommended to follow the manufacturer’s guidelines.
In general, a dry mix may increase the compressive strength up to twice that of the
wet one, but the excessive reduction of water will result in inferior properties
(Earnshaw and Smith, 2009; Peyton et al., 1952; Noort, 2002).
50
Advanced Dental Biomaterials
Figure 3.6 Effect of W/P ratio on compressive strength of different gypsum products:
plaster, model stone, and high-strength dental stone. W/P ratio, Water/powder ratio.
Source: Data from Ronald, L.S., John, M.P., 2012. Craig’s Restorative Dental Materials,
13th ed. Mosby Elsevier.
3.6.3 Tensile strength
Plaster’s tensile strength is very low (approximately 2 MPa) due to the porous and
brittle nature of the material. This has the disadvantage of the teeth and margins
being damaged if handled roughly. This is why dental stone, which has twice the
tensile strength of plaster is preferred for the production of crown and bridge
models and dies (Earnshaw and Smith, 2009; Padevět et al., 2011).
3.6.4 Surface hardness and abrasion resistance
Gypsum products are highly susceptible to scratching and loss of surface details
due to low surface hardness and abrasion resistance. The surface hardness is
directly proportional to the compressive strength of the gypsum products. Therefore
the greater the compressive strength, the greater the hardness. It has been noted that
surface hardness increases at a much faster rate than the compressive strength for a
final set material due to the surface mass of the hardened material reaching a dry
state earlier than the mass of the inner portion (Peyton et al., 1952).
Gypsum products have been tested again and again and attempts have been
made to improve their hardness by incorporating set gypsum with epoxy or methylmethacrylate monomer that polymerizes when setting (Robert et al., 2004; Williams
et al., 1983). Epoxy resin does show better detail reproduction, abrasion resistance,
and transverse strength than gypsum products but undergoes polymerization shrinkage. This, in turn, can affect and compromise the fit of the castings unless taken
into account before processing. Dental plaster with epoxy resin showed an increase
in the strength but this was not the case for dental stone or high-strength dental
stones (Paquette et al., 2000; Robert et al., 2004). Generally, abrasive resistance
was improved by 15% 41% when epoxy resin was added to dental stone but compressive strength and surface hardness decreased.
Drying molds, casts, or dies to achieve compressive strength and surface hardness rapidly has been rejected as it makes the gypsum dehydrated and therefore
weakens the overall structure. Some other methods, such as soaking in glycerin or
Dental gypsum and investments
51
different oils that have been used to increase surface hardness, have also been
rejected as this would not improve the surface hardness and would just smoothen
the surface which makes the carver or wax knife slide over it when in contact.
Surface hardness can be improved and increased using commercial hardening solutions containing colloidal silica (30%) (Robert et al., 2004; Williams et al., 1983).
However, it should be noted that increased surface hardness does not mean
increased abrasion resistance as that is only one of the many factors that can affect
wear resistance. Studies for two-body abrasion resistance showed that there is no
improvement in abrasion resistance when high-strength stone is commercially hardened using different solutions (Robert et al., 2004; Hollenback and Smith, 1967;
von Fraunhofer and Spiers, 1983).
Further studies and methods for the measurement of abrasion resistance are
required as two-body abrasion tests are not well established for gypsum products. It
is worth noting that disinfectants used on gypsum products have shown to adversely
affect the surface hardness making the surface susceptible to erosion and wear.
3.6.5 Dimensional stability
Dimensional stability of the set gypsum products is excellent; there is no or very
little dimensional change of the set material (Chan and Darvell, 2001). These materials can be stored for a long period of time under dry conditions as the material is
still slightly soluble in water. Therefore it is recommended not to wash the surface
of the set material with hot water.
3.7
Dies and models produced from digital data
Computer-assisted technologies such as 3D technologies have been increasingly
used in dentistry, where a layer-by-layer replica or a designed restoration is formed.
This is so-called additive manufacturing or rapid prototyping employed to make
dental replicas as well as restorations. To manufacture the replicas a digital image
of the oral tissue or an object is obtained either directly from the patient’s mouth or
indirectly from a conventional impression and then sent to a 3D printer after processing the data. In order to make restorations, a virtual restoration is designed on the
virtual model in the computer and sent to a 3D printer. This technology facilitates
and accelerates manufacturing of replicas and restorations with higher accuracy and
reduces material waste. However, the high initial investment makes adoption of this
technology by dental practices or most dental labs very slow.
Different materials have been used for 3D printing including ABS plastics, polyamide (nylon), glass-reinforced polyamide, epoxy resins, titanium, steel, photopolymers, waxes, and polycarbonates. Formlabs has recently introduced a long-term
biocompatible 3D printing resin called Dental LT Clear for orthodontic appliances
and devices (TESS, 2017). PolyJest dental materials are specially designed for
dental application, and these include three types (Table 3.1).
52
Advanced Dental Biomaterials
1. Clear Biocompatible (MED 610)
Used to produce orthodontic appliances as well as delivery and positioning trays and
surgical guides.
2. Vero Dent Plus (MED 690)
A dark beige material that creates amazingly fine features and finishes with great accuracy, strength, and durability.
3. Vero Glaze (MED620)
An opaque material with A2 shading designed to provide the suitable color match for
veneer try-ins and diagnostic wax-ups (Mahamood et al., 2016). These materials are
used by various systems such as Object260 and Object500 Dental Selection (by
Stratasys) to manufacture dental replicas and restorations.
3.8
Conclusion
Gypsum products have been used in dentistry for many years, mostly to make replicas of oral tissue for various purposes, due to their desirable properties. However,
computer-assisted technologies are enabling us to produce dental replicas and
restorations by shortening the stages, increasing the accuracy, and reducing the
wastes. Further work is required to reduce the initial cost and production time
before they are routinely used in dental practices and dental laboratories.
References
Dental Science, 2017. Gypsum Products in Dentistry: Types, Uses, Properties. Available
from ,http://www.dental-science.com/gypsum-materials/. (accessed 21.01.18.).
ADA, 1972. New American Dental Association specification no. 25 for dental gypsum
products. J. Am. Dent. Assoc. 84, 640 644.
ADA, 1977. Revised American Dental Association specification no. 19 for non-aqueous,
elastomeric dental impression materials. J. Am. Dent. Assoc. 94, 733 741.
Anusavice, K.J., 2013. Philip’s Science of Dental Materials. Elsevier/Saunders, St. Louis, MO.
Asaoka, K., Bae, J.Y., Lee, H.H., 2012. Porosity of dental gypsum-bonded investments in
setting and heating process. Dent. Mater. J. 31, 120 124.
Cesar, A.F., Tatiana, S.Z., Fabio, A.R., Yoshio, F., Marcia, F., 2015. Linear setting expansion
of different gypsum products. RSBO 12, 61 67.
Chan, T.K., Darvell, B.W., 2001. Effect of storage conditions on calcium sulphate
hemihydrate-containing products. Dent. Mater. 17, 134 141.
Chang, Y.-C., Yu, C.-H., Liang, W.-M., Tu, M.-G., Chen, S.-Y., 2016. Comparison of the
surface roughness of gypsum models constructed using various impression materials and
gypsum products. J. Dent. Sci. 11, 23 28.
Cunningham, W.A., Dunham, R.M., Antes, L.L., 1952. Hydration of gypsum plaster. Ind.
Eng. Chem. 44, 2402 2408.
Docking, A.R., 1965. Gypsum research in Australia—the setting process. Int. Dent. J. 15,
372 376.
Earnshaw, R., Smith, D.C., 2009. The tensile and compressive strength of plaster and stone.
Aust. Dent. J. 11, 415 422.
Dental gypsum and investments
53
Earnshaw, R., Marks, B., 1964. The measurement of setting time of gypsum products. Aust.
Dent. J. 1 (9), 17 26.
Garber, D.K., Powers, J.M., Brandau, H.E., 1985. Effect of spatulation on the properties of
high-strength dental stones. J. Mich. Dent. Assoc. 67, 133 136.
Hollenback, G.M., Smith, D.D., 1967. A further investigation of the physical properties of
hard gypsums. J. Calif. Dent. Assoc. 43, 221 227.
Luk, H.W.K., Darvell, B.W., 1991. Strength of phosphate-bonded investments at high
temperature. Dent. Mater. 7, 99 102.
Luk, W.K., Darvell, B.W., 2003. Effect of burnout temperature on strength of gypsumbonded investments. Dent. Mater. 19, 552 557.
Lyon, H.W., George, D., Schoonover, I.C., 1955. The mechanism of hygroscopic expansion
in dental casting investments. J. Dent. Res. 34, 44 50.
Mahamood, S., Abdul Khader, M., Ali, H., 2016. Applications of 3-D printing in orthodontics: a review. Int. J. Sci. Study 3, 267 270.
Mahler, D.B., Bruce Ady, A., 1960. An explanation for the hygroscopic setting expansion of
dental gypsum products. J. Dent. Res. 39, 578 589.
Mccabe, J.F., Walls, A., 2013. Applied Dental Materials. John Wiley & Sons.
Michalakis, K.X., Stratos, A., Hirayama, H., Pissiotis, A.L., Touloumi, F., 2009. Delayed
setting and hygroscopic linear expansion of three gypsum products used for cast articulation. J. Prosthet. Dent. 102, 313 318.
Malaviya, N., Shrestha, A., 2016. Comparative evaluation of surface detail changes and
compressive strength of gypsum casts and dies after immersion in hypochlorite solution and microwave irradiation—an in vitro study. Int. J. Contemp. Med. Res. 3,
1547 1551.
Noort, R.V., 2002. Introduction to Dental Materials. Mosby, Edinburgh.
Noort, R.V., Barbour, M.E., 2013. Introduction to dental materials. Mosby Elsevier,
Edinburgh; New York.
O’Brien, W.J., 2008. Dental Materials and Their Selection. Quintessence Pub. Co., Hanover
Park, IL; London.
Padevět, P., Tesarek, P., Plachý, T., 2011. Evolution of mechanical properties of gypsum in
time. Int. J. Mech. 5 (1), 1 9.
Paquette, J.M., Taniguchi, T., White, S.N., 2000. Dimensional accuracy of an epoxy resin die
material using two setting methods. J. Prosthet. Dent. 83, 301 305.
Peyton, F.A., Leibold, J.P., Ridgley, G.V., 1952. Surface hardness, compressive strength, and
abrasion resistance of indirect die stones. J. Prosthet. Dent. 2, 381 389.
Robert, G.C., John, M.P., John, C.W., 2004. Dental Materials. Mosby, St. Louis, MO.
Sanad, M.E.E., Combe, E.C., Grant, A.A., 1982. The use of additives to improve the mechanical properties of gypsum products. J. Dent. Res. 61, 808 810.
Singh, M., Garg, M., 1997. Retarding action of various chemicals on setting and hardening
characteristics of gypsum plaster at different pH. Cem. Concr. Res. 27, 947 950.
TESS, 2017. Formlabs Releases New Dental LT Clear Orthodontic 3D Printing Resin,
Updates Dental SG Resin. ,www.3ders.org. (accessed 05.05.18.).
von Fraunhofer, J.A., Spiers, R.R., 1983. Strength testing of dental stone: a comparison of
compressive, tensile, transverse, and shear strength tests. J. Biomed. Mater. Res. 17,
293 299.
Williams, G.J., Bates, J.F., Wild, S., 1983. The effect of surface treatment of dental stone
with resins. Quintessence Dent. Technol. 7, 41 45.
Williams, K.R., Williams, G.J., 1984. The setting of dental plasters: an electron microscopical
study. J. Mater. Sci. 19, 929 938.
54
Advanced Dental Biomaterials
Winkler, M.M., Monaghan, P., Gilbert, J.L., Lautenschlager, E.P., 1998. Comparison of four
techniques for monitoring the setting kinetics of gypsum. J. Prosthet. Dent. 79,
532 536.
Worner, H.K., 1944. The effect of temperature on the rate of setting of plaster of Paris.
J. Dent. Res. 23, 305 308.
Ceramic materials in dentistry
4
James K.H. Tsoi
Dental Materials Science, Discipline of Applied Oral Sciences, Faculty of Dentistry, The
University of Hong Kong, Pokfulam, Hong Kong SAR, P.R. China
Chapter Outline
4.1 Introduction 55
4.1.1 Glass ceramics 56
4.1.2 Oxide ceramics 61
4.1.3 Polymer-containing ceramics 64
4.2 Ceramic bonding
65
4.2.1 Mechanism 65
4.2.2 Bond strength evaluation 71
4.2.3 Fatigue 73
4.3 Ceramic biological interaction
74
4.3.1 Surface chemistry 74
4.3.2 Physical parameters 76
4.3.3 Sterilization methods 77
4.4 Conclusion 77
References 77
4.1
Introduction
Ceramic, being a composite material, is defined as a (IUPAC Goldbook, 2007):
Rigid material that consists of an infinite three-dimensional network of sintered
crystalline grains comprising metals bonded to carbon, nitrogen or oxygen
Generally speaking, the term ceramic is applicable to any class of inorganic,
nonmetallic product that consists of two or more phases, which is different to a
glass (that is amorphous), and commonly requires a high temperature during the
manufacturing process. Ceramics are capable of withstanding high strength and
stiffness. However, they are often brittle and are low in tensile strength. These properties limit the application of ceramics. Nevertheless, ceramics can mimic natural
teeth well esthetically. Thus, while limitations still need to be overcome, the application of ceramics in dentistry is somewhat multifold.
Ceramics in modern dentistry can be generally classified into glass ceramics
and oxide ceramics based on chemical composition. Glass ceramics, also termed
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00004-9
Copyright © 2019 Elsevier Ltd. All rights reserved.
56
Advanced Dental Biomaterials
silica-based ceramics, are a group of materials that have been widely used in
all-ceramic restorations since the 1970s. These can be further classified as
porcelain-based (e.g. feldspathic and leucite-reinforced) or non-porcelain-based
(e.g. fluormica glass and lithium disilicate) ceramics. Oxide ceramics are defined as
a group of ceramics containing no more than 15% silica with little or no glass
phase. They can be subclassified into (1) aluminium-oxide/alumina ceramics,
including glass-infiltrated alumina ceramics, densely sintered alumina ceramic
systems and (2) zirconium-oxide/zirconia ceramics, including glass-infiltrated and
densely sintered zirconia ceramic systems. Because of their stable chemical
structure, oxide ceramics have significantly improved mechanical properties and
can be regarded as “high-strength ceramics.”
4.1.1 Glass ceramics
4.1.1.1 Feldspathic porcelain
As aforementioned, the classification of glass ceramics can be based on “porcelain”.
Porcelain was originally developed in China 12002000 years ago and then
exported to Europe. Chemically speaking, porcelain contains a number common
components such as kaolin, feldspar, and quartz. When these components are heated
to a sufficiently high temperature, some components are melted and a silica-based
glassy matrix embedding a crystalline core is created. This process is called vitrification. Thus, the porosity (i.e. the flaws) decreased and accompanied by general
increase in hardness, mechanical strength, and translucency.
In terms of dental feldspathic porcelain, various components exist, typically
70%75% potash feldspar (K2O Al2O3 6SiO2), few percentage of kaolin
(Al2O3 2SiO2 2H2O) as binder, 15%20% quartz (SiO2) as crystalline phase, and
minute amounts of pigments for different shades. These components are melted or
react at various temperatures to form different compounds:
Al2 O3 2SiO2 2H2 O ! Al2 O3 2SiO2 ðmetakaoliniteÞ12H2 OðgÞ @ 450o C
k
(4.i)
3Al2 O3 2SiO2 ðmulliteÞ 1SiO2
(4.ii)
@ . 1000o C
K2 O Al2 O3 6SiO2 ! K2 O Al2 O3 4SiO2 ðleuciteÞ12SiO2 @1150o C
(4.iii)
It should be noted that these reactions will never complete unless a sufficiently
long enough time is given. Thus, the overall entity is a partially melted (softened,
because the temperature is less than the melting point in its pure form) mass consisting of multispecies with reactants and products. This is a sintering process that
is defined as (Darvell, 2011):
Heating a powder below the melting point of any component such as to permit
agglomeration and welding of particles by diffusion alone, with or without applied
pressure.
Ceramic materials in dentistry
57
Continuation of heating of the mass would let the amorphous SiO2 [as generated
in Eqs. (4.ii) and (4.iii)] to become liquid and chemically cross-link with metal ions
in the system, for example, Al31 and K1, to form a 3D network. In addition, the Al
atom could chemically react with SiO2 on the surface of crystalline quartz. This
newly formed aluminosilicate can effectively form a chemical (covalent) bond
between crystalline and amorphous phases. During the cooling process, crystallization would not happen on this partially melted mass due to (1) the high viscosity of
the liquid phase and (2) crystallization that requires high activation energy.
Ultimately, the final structure is a glassy silicate matrix embedded with (1) a core
in mixture form that consists largely of quartz and unreacted feldspar and (2) a dispersion of the separated mullite.
Despite quartz being in the crystalline phase, which is deemed to contribute to
the overall strength, quartz per se is not a high-strength material. Some additives,
such as alumina (Al2O3), can be added in order to improve the mechanical performance. However, caution should be taken for such an addition because the coefficients of thermal expansion (CTE) between different particles are different.
Residual stress would happen at the particles’ interface if the CTEs are not
matched. On the other hand, as natural feldspar is commonly used by manufacturers, other feldspar analogs that contain sodium, rubidium, and calcium are also
found in dental feldspathic porcelain. These compounds will affect the transformation temperatures in the whole system, and thus quality control is an important
aspect in making the final product. For example, soda feldspar
(Na2O Al2O3 6SiO2) is able to decrease the softening temperature but increase the
pyroplastic flow that will slump and distort the shape of the material.
As you might notice, the sintering process can be closely controlled by time and
temperature. These technique-sensitive procedural parameters allow (if proper!) diffusion between particles and phases, which can reduce the porosity, the total surface
area, and the total surface energy, thereby producing ideally a pore-free high-fusing
product. These temperature and time parameters, as well as the dimension of the
porcelain, can be generally described using the Biot number (Bi):
B i 5 Lc
h
kb
(4.1)
where Lc is the characteristic length (i.e. volume of body divided by the surface
area of the body), h the heat transfer coefficient (i.e. heat flux divided by temperature difference between solid and surrounding fluid such as air), and kb the thermal
conductivity.
Bi is an index stating the ratio of heat transfer resistance inside and on the surface of the material. So, a small Bi means less heat transfer, while a large Bi means
good heat transfer. When considering an object under heating with time, there is no
way for heat to be evenly distributed at every single point inside and at the surface.
Commonly, at the surface, maximum tensile stress would be encountered and at the
center there would be compressive stress. The overall magnitude of the stresses
increases with increasing Bi. This said, at the extreme case of Bi 5 0, every test
point would be stress free; conversely Bi 5 N would be highly stressed. As a result,
58
Advanced Dental Biomaterials
if there is a steep temperature gradient as a sudden deposition of energy from the
object to the surrounding or vice versa, thermal stress would be developed. If the
thermal stress is larger than the strength of material, failure will occur and this is
called thermal shock.
Another issue is shrinkage. To control the shrinkage, particle size distribution is
important so as to pack the particles as tightly as possible. Nowadays, dental technicians can use manufacturer premixed, fused, and quenched porcelain powders, that
is, "cold-shocked", to produce low- and medium-fusing dental porcelain frits. Then,
there is no chemical reaction during the heating process since the powders simply
melt about the glass transition temperature and fuse together. Upon cooling, a solid
mass is produced. If cooling is carried out in the mold, a block can be produced
and this is used as a blank CAD/CAM (computer-aided design/computer-aided
machining) block.
Porcelain, due to its lower strength than other ceramics, is commonly used in
applications that have lower mechanical strength requirement, for example, veneer,
external facing of metal framework, inlay, and onlay.
4.1.1.2 Leucite-reinforced porcelain
As the name implies, this is a porcelain that is reinforced by leucite. With the incorporation of a high proportion of leucite, CTE is raised such that the chance of thermal mismatch with, say, metal during the application of PFM (porcelain-fused
metal) can be decreased. Leucite-reinforced porcelain also has a CAD/CAM block
version, and currently, there is a similar application with feldspathic porcelain.
4.1.1.3 Fluorine-containing glass ceramics
The dental representative for this type of ceramics is known as fluormica, which is
mainly based on glass with constituents of SiO2 K2O MgO Al2O3 ZrO2, and
also some fluorine-containing compounds. So, the final product is tetrasilica mica
crystals within the glass that has a casting temperature of 1380 C, together with a
flexural strength of 120150 MPa and a Knoop microhardness value of 360 (cf.
enamel: 340). Commercial examples include Dicor (Cast version) and Macor
(CAD/CAM version). Interestingly, Leung et al. (2015) have reported that an experimental fluorine-containing ceramic (fluorophlogopite, with K2SiF6) can be a more
reliable CAD/CAM material (as a result of Weibull modulus on flexural strength)
and can also produce less wear than other glass ceramics (feldspathic and lithium
disilicate) as well as polymer-infiltrated ceramic blocks (Table 4.1).
It should be noted that although a material may contain fluorinated compounds,
it does not imply it has a fluoride ion-releasing ability, although fluoride was
detected with the immersion of fluorophlogopite into water.
4.1.1.4 Lithium silicate
Lithium disilicate is a glass ceramic based on crystalline phase of Li2Si2O5, which
makes up 70 vol.%, and also has low vol.% of Li3PO4 crystalline phase. It has an
Table 4.1 Flexural strength, Vickers hardness, and Weibull modulus for fluorophlogopite, feldspathic porcelain, polymer-infiltrated polymer network, and
lithium disilicate computer-aided design/computer-aided machining blocks.
Characteristic
Experimental
fluorophlogopite
(1)
Feldspathic
porcelain (2)
Polymer-infiltrated ceramic
network (3)
Lithium disilicate (4)
Group
Multiple
comparison
Three-point
flexural
strength (MPa),
mean (SD)
Vickers hardness
(HV), mean
(SD)
Weibull modulus
Composition from
manufacturer
117.61 (7.62)
106.67 (18.50)
145.95 (12.65)
341.88 (40.25)
,0.001
(1), (2) ,
(3) , (4)
153.74 (23.62)
594.74 (25.22)
372.29 (51.23)
731.63 (30.64)
,0.001
(1) , (3) ,
(2) , (4)
18.34
K2SiF6, Al2O3,
MgO, SiO2,
B2O3
6.93
SiO2, Al2O3, Na2O,
K2O, CaO, TiO2,
coloring oxides
12.87
SiO2, Al2O3, Na2O, K2O, B2O3,
CaO, TiO2, coloring oxides,
methacrylate polymer
10.01
SiO2, Li2O, K2O, P2O5,
ZrO2, ZnO, Al2O3,
MgO, coloring oxides
Source: Modified from Leung, B.T.W., Tsoi, J.K.H., Matinlinna, J.P., Pow, E.H.N., 2015. Comparison of mechanical properties of three machinable ceramics with an experimental flurophlogopite glass
ceramic. J. Prosthet. Dent. 114 (3), 440446.
60
Advanced Dental Biomaterials
unusual microstructure that contains many randomly oriented small, interlocking,
plate-like, and needle-like crystals. Such a microstructure (Fig. 4.1) is good to arrest
cracks and provide substantial increase of flexural strength. It is quite user-friendly
in that the processing temperature is 920 C, and flexural strength is achievable to
350450 MPa. Both hot press and CAD/CAM versions are available. However, it
is worth noting that these two versions of ceramics are different in crystal size.
Thus, they have different mechanical properties (Fig. 4.1). In addition, a study
(Fabian Fonzar et al., 2017) revealed different translucencies of the lithium disilicate would show a difference in mechanical strength, particularly in CAD/CAM
blocks. The reason is unknown but the formulation might contribute to this
difference.
Another type of lithium silicate ceramic is zirconia-lithium silicate, which has
added, and is claimed to be reinforced by zirconia fine particles (B10 wt.%) in lithium silicate. It could achieve a higher flexural strength than lithium disilicate.
Figure 4.1 SEM images of lithium disilicate hot press and CAD/CAM versions. NB: The
particle sizes of hot press are larger than CAD/CAM, which might yield a better mechanical
performance. CAD, Computer-aided design; CAM, computer-aided machining; SEM,
scanning electron microscope.
Ceramic materials in dentistry
61
Limited scientific literature about this material is available. The commercially
available CAD/CAM blocks are
1. Vita Surprinity (unsintered)
2. Dentsply Celtra DUO (sintered)
4.1.2 Oxide ceramics
4.1.2.1 Glass-infiltrated aluminium-oxide ceramic
The need for improved fracture strength is vital for all-ceramic restorations. So,
increasing the alumina (Al2O3) content can be functional as a reinforcement of the
glassy matrix, that is, comparable to leucite crystals. Hence, ceramics that are based
on aluminium oxide have been produced and are indicated in multiple areas for restoration, such as copings, frameworks, crowns, and fixed partial denture (FPDs). To
use such copings and frameworks the alumina should be veneered with feldspathic
porcelain so as to serve two purposes: (1) obtaining better physical strength and (2)
esthetics.
Glass-infiltrated aluminium-oxide ceramic utilizes a dry-sintered B85% Al2O3
core that is infused with B15% molten lanthanum glass. Commonly, this kind of
core can achieve a flexural strength of 400500 MPa after glass infiltration. The
commercial representative product is In-Ceram Alumina (VITA).
4.1.2.2 Densely sintered aluminium-oxide ceramic
Densely sintered high-purity aluminium-oxide ceramic, as the name implies, utilizes 80.0%99.5% Al2O3 to sinter and does not contain any silica. It should be
noted that, given the alumina has a hexagonal close-packed structure with Al31 and
other metal ions in two-third of octahedral sites, the alumina is elastic and not viscoplastic at temperature ,1000 C (Ionascu, 2008). However, at the alleviation of
temperature, alumina (and many other polycrystalline ceramics such as zirconia)
will reduce its brittleness and allow viscoplastic deformation like metal. In this case
the grain boundaries sliding and diffusion creep are commonly recognized as the
mechanism for this high-temperature viscoplasticity. Such a so-called high-temperature superplastic behavior in polycrystalline ceramics is essential in stress-related
densification processes, such as “hot isostatic pressing” and “hot pressing.” As
such, the creep rate (plastic flow), ε_ , for the superplasticity of ceramics can be generalized in Arrhenius relationship of
ε_ ðσ; T Þ 5 A
σ2σ n bp
0
G
d
D0 expQ=KT
(4.2)
where σ is the stress applied, σ0 is the threshold stress that is dependent of grain
boundaries, shear modulus G, stress component n, Burger’s vector b that represents
the magnitude and direction of the lattice distortion resulting from a dislocation in a
crystal lattice, grain size d, grain size component p, preexponential constants A and
62
Advanced Dental Biomaterials
D0 that are dependent on reaction and diffusion, respectively, activation energy Q,
temperature T, and Boltzmann constant k.
As shown in Eq. (4.2), grain dislocations and conditions are important for the
flow rate. So, all kinds of small amounts of impurities, such as from CAD/CAM
machining, trimming, and grinding, would contribute a lot in varying the plastic
flow between grain layers (say, superficial vs bulk). In addition, Eq. (4.1) can also
predict the heat transfer variation between these layers. Therefore, during hightemperature sintering and also in the cooling, the mismatch of grain layers’ flow
would induce intrinsic flaws and internal stresses that are responsible for chipping
and cracks.
Commercial product Procera Allceram (Nobel Biocare) can achieve a flexural
strength of B700 MPa and requires a high sintering temperature
(1600 C1700 C). Another product Techceram, which claimed to have 80%90%
Al2O3, requires a special plasma technique to utilize the high-temperature plastic
flow as stated in Eq. (4.2) to produce the ceramic core, and sinters at 1170 C.
4.1.2.3 Zirconia
Zirconia, ZrO2, is the oxide of zirconium and belongs to the group of oxide ceramics. It has various desirable mechanical properties: despite its brittleness, the flexural strength is around 1200 MPa and the hardness very high (more than 1200 HV).
It has a high fracture toughness and a good fatigue resistance. From the chemical
point of view, zirconia does not dissolve in acids, nor in alkalis. Its appearance is
dull, whiteopaque, and it is a good chemical and thermal insulator. As a metal
oxide, zirconia has a high radiopacity and is well displayed on X-ray pictures.
Furthermore, it is tasteless and odorless.
Normally, under low pressure the crystallographic structure of pure zirconia
5
(Fig. 4.2) at room temperature is monoclinic (m, space group C2h
or P21/c). With
increasing temperatures the crystal lattice of zirconia undergoes phase transformation. Above 1170 C the atoms arrange in the tetragonal phase (t, space group D15
4h
or P42/nmc) that is a first-order displacive martensitic phase transformation. When
Figure 4.2 Crystalline structure of different phases of zirconia.
Ceramic materials in dentistry
63
zirconia is heated to temperatures higher than 2370 C, a second transformation
occurs, which turns tetragonal phase into the cubic form (c, space group O5h or
Fm3m) (Botelho et al., 2018).
The changes in the crystal lattice of the dimension change from m to t and from
t to c is approximately 3%5% for each transformation. However, when cooling
the heated zirconia to room temperature, the opposite dimensional changes cause
high stresses. So, pure zirconia forms cracks while cooling. To prevent this, some
chemicals such as magnesia (MgO), lime (calcium oxide, CaO), ceria (cerium trioxide, Ce2O3), and yttria (Y2O3) are added. These chemicals are able to inhibit crack
formation and crack propagation by stabilizing the zirconia at t phase. In principle,
when zirconia is subjected to an increase of external stress, microcracks would
appear and the stress is the highest at the tip of a crack. If the crystalline structure
of zirconia is stabilized in tetragonal form, phase transformation from t to m can
happen. Due to the new arrangement of the atoms, the material volume around the
tip of the crack increases by 3%5%. So, this makes the crack tip less sharp and
also increases the crack path length (i.e. toughened). Therefore, effectively speaking, tetragonal phase stabilization can inhibit crack propagations by t to m transformation. Such a toughening mechanism by phase transformation is able to capture
cracks under compressive stresses but is less effective under tension. Therefore
yttria-stabilized tetragonal zirconia crystal (Y-TZP) has poor resistance to tensile
stresses.
Currently, the most commonly used zirconia-based polycrystalline ceramic in
dentistry is room temperature stabilized at t phase by adding 36 wt.% or 23 mol
% of Y2O3, which is called Y-TZP. Y-TZP is the only zirconia that is listed on the
ISO standard for surgical applications and therefore can be used as an implant
material.
However, there are some negative effects of such phase transformation. In particular, different kinds of stress can cause the t to m transformation and one of them is
temperature, which is so-called low temperature degeneration (LTD). As such, the
mechanism to inhibit crack propagation no longer works and this effectively
decreases the mechanical properties of Y-TZP. The particular reasons for LTD are
still controversially discussed in the literature. In general, some reasons are sound,
for example, the absorption of water into the surface of zirconia, stabilizers, grain
size of the zirconia, the residual stresses after sintering, and any other external stresses. Apparently, the real LTD mechanism could be a combination of various
factors.
It should be also noticed that, under a pressurized environment the monoclinic
phase zirconia can be transited to orthorhombic brookite phase at 311 GPa, or to
orthorhombic cotunnite phase at 915 GPa. So, caution should be taken during the
manufacturing of zirconia CAD/CAM discs or blocks using the press technique.
As a matter of fact, the first generation of Y-TZP is a dull and white material,
which cannot mimic the translucency of natural teeth, and is not even comparable
to porcelain. The secondary generation of dental zirconia added some colorants to
make the monolithic zirconia. Although the shade is there, the material is still opaque because the incident light is (1) reflected at the material interface between air
64
Advanced Dental Biomaterials
and ceramic, (2) scattered at grain boundaries, and (3) scattered at pores. So, the
final in-line transmission (TIT) would become weaker and thus reduce the translucency. To allow zirconia to achieve the translucency of dental porcelain, a Rayleigh
approximation could be used
(
TIT 5 ð1 2 RÞexp
128π4 r 3
2
18λ4
)
Δnave ð2n1Δnave Þ 2
t
2
(4.3)
where Δnave is the average birefringence, 2n is the grain size, t is the thickness, and
λ is the wavelength. The loss of reflection at two surfaces is given by R 5 1 2 2n/
(n2 1 1) where n is the refractive index. Using this calculation, a study (Zhang,
2014) revealed that the grain size should be down to 82 nm (for 1.3 mm thickness),
77 nm (for 1.5 mm thickness), and even 70 nm (for 2 mm thickness). Obviously,
such small sizes of zirconia grains are not easy (or not economical) to obtain. So,
the easiest way to tackle this is to laminate a layer of porcelain (with similar CTE)
such as the PFM. However, chipping might occur which can ultimately lead to fracture. Removing bonded zirconia prostheses, such as crowns or bridges, is difficult
and causes damage to the ceramic.
Recently, another approach that has been put into practice was the addition of
small amounts of the cubic phase zirconia (with isotropic refractive index) into YTZP so as to avoid scattering from the grain boundaries. In fact the manufacturers
are not simply adding cubic phase zirconia powders into TZP, but they add the preprocessed B1 μm crystal powders with high amounts of (B50%) cubic zirconia
and high yttria content (B5 mol%) into TZP. While the third generation of zirconia
seems to have high translucency that matches with current dental porcelain, the
strength (flexural strength: 650800 MPa) was compromised because the grain
boundaries might not be well attached [in particular during high temperature, the
grain boundaries slide, as shown in Eq. (4.2)], and also the t to m toughening may
not be so effective.
4.1.3 Polymer-containing ceramics
As the name implies, this type of ceramic (in CAD/CAM block form) does not contain solely the ceramic. Commonly, polymeric phase is added so as to increase the
crack length, that is, it gives the onset of plasticity under the load and demonstrates
a Dugdale cracking model in a way that displacement happens around the crack
tips. So, the crack resistance is increased and this effectively lowered the scattering
of the strength data. Thus, the Weibull modulus is increased (Table 4.1).
Currently, in the market, there are some brands of products named “Hybrid
Ceramics.” Indeed, first, whether the CAD/CAM block can be claimed ceramic
depends on the existence of an infinite three-dimensional network of crystalline
grains. Second, whether it can be named “hybrid” material depends on the interfacial intimate interactions at the nanoscale that has happened between the phases. If
the polymeric and ceramic components are separated, we should term these blocks
Ceramic materials in dentistry
65
as “composites.” Therefore if the CAD/CAM block is made by compression of
resin-coated ceramic powders, then this is a “composite” material, neither hybrid
nor ceramic.
One more issue is, in the literature both CAD/CAM and CAD-CAM are used.
Although they look the same, slash (/) and hyphen (-) conventionally have different
meanings in instrumentation. Accordingly, in the process, if the CAD and CAM are
different, for example, operated by different equipment, a slash is preferred. If
CAD and CAM are hyphenated (-) that means this is a combined or integrative process. However, in dentistry, it seems to be that both CAD/CAM and CAD-CAM
are used interchangeably.
4.2
Ceramic bonding
Nowadays, various ceramic restorations, for example, veneers, inlays/onlays,
crowns, implants, and resin-bonded bridges exist and a long-term success of the restoration relies heavily on the quality of bonding. To achieve this, resin luting
cements were introduced to aid all-ceramic restoration retention. Resin cements not
only provide stronger and more durable bonding between ceramics and teeth but
can also achieve better esthetic outcomes and maintain higher ceramic strength
(Tian et al., 2014).
4.2.1 Mechanism
It is generally accepted that adhesion between ceramics and resin cements is provided
by two major mechanisms: micromechanical attachment and chemical bonding.
Micromechanical attachment can be created by etching and/or grit-blasting, while coupling agents can provide a chemical bond. All these mechanisms rely on the surface
treatments/conditioning methods in order to provide a suitable surface for adherent
and substrates. As various ceramics differ in chemical conformation and microstructure, it is necessary to establish bonding procedures according to the ceramic type.
4.2.1.1 Chemical surface conditioning
Hydrofluoric acid etching
Hydrofluoric acid (HF) is an aqueous solution of hydrogen fluoride. HF has a long
history in the surface pretreatment of silica-based ceramics before bonding. Such an
etching process can increase the roughness of the ceramic surface and consequently
creates a micromechanical interlock between the ceramic and resin luting cement.
HF is a weak acid compare to the same concentration of, say, HCl. In fact, HF can
react with SiO2:
SiO2 ðsÞ 1 4HF ðaqÞ ! SiF4 ðgÞ 12H2 O
(4.iv)
4SiF4 ðgÞ 1 3H2 OðlÞ 1 2HFðaqÞ ! 3H2 SiF6 ðaqÞ 1 H2 SiO3 ðaqÞ
(4.v)
66
Advanced Dental Biomaterials
So, the etching process induced by HF does not rely on the “acidic” property of HF
but rather the fluoride substitution to oxygen due to electronegativity in glass that
forms the Si F glass. Thus, the term “HF etching” should be used, as “acid etching” is misleading.
Various glass ceramics and composite can be HF etched to create the roughness
for adhesion, as illustrated in Fig. 4.3. For feldspathic porcelain, it was found that
the longer the etching time, the rougher the surface will become (Table 4.2), but
the biaxial flexural strengths are no different (Liu et al., 2015). So, this result
Figure 4.3 SEM images of various CAD/CAM materials before and after HF etching. Mark
II: feldspathic porcelain; e.max: lithium disilicate; Suprinity: zirconia-reinforced lithium
silicate; Enamic: PICN. CAD, Computer-aided design; CAM, computer-aided machining; HF,
hydrofluoric acid; PICN, polymer-infiltrated ceramic network; SEM, scanning electron
microscope.
Ceramic materials in dentistry
67
Table 4.2 Comparison between different hydrofluoric acid etching time on feldspathic
porcelain.
Surface
treatment
Surface
roughness
(µm)
Biaxial flexural
strength (MPa)
Shear bond
strength (MPa)
Weibull
modulus
of shear bond
strength
Control
Etching for 30 s
Etching for 1 min
Etching for 2 min
0.11 6 0.02a
0.25 6 0.04b
0.50 6 0.07c,d
0.52 6 0.09d
90.0 6 5.5e
89.0 6 4.8e
86.3 6 7.4e
86.8 6 9.6e
11.60 6 1.93f
10.58 6 1.27f,g
10.37 6 2.32f,g
10.26 6 1.46g
7.38
9.99
5.36
8.11
Different superscript letters indicate the significant differences (P , .05).
Source: From Liu, D., Tsoi, J.K.H., Pow, E.H.N., Wong, H.M., 2015. Influence of different etching protocols on the reliability of resin
bonding to CAD/CAM feldspathic porcelain. Int. J. Adhes. Adhes. 62, 1824.
suggested that the HF etching would change the superficial surface only. On the
other hand, the longer etching time, despite increasing the surface roughness, would
decrease the shear bond strength. Again, the Weibull moduli as shown in Table 4.2
can demonstrate the bond reliability. Thus, there is a need to follow the manufacturers’ recommendation for the HF etching procedure. Nonetheless, different dosage
forms (liquid vs gel), HF concentrations, and components in the formulation would
affect the overall outcome. In addition, different test methods, due to the variation
in setup, would have different sensitivity for the effects. For example, HF etching
on lithium disilicate for 60 seconds may show the same tensile bond strength as
20 seconds. However, a bending test setup would show 60 seconds of HF etching to
have significantly lower bond strength than 20 seconds (Wong et al., 2017).
Therefore, the test setup would be influential on test sensitivity.
Early studies have shown that zirconia surface cannot be etched by HF, and zirconia is termed an “acid-resistant ceramic.” However, recent studies have revealed
that some drastic (and very dangerous!) conditions, for example, hot HF, can etch
the zirconia. Such a condition can create a higher roughness (Fig. 4.4), comparable
bond strength, and no t to m transformation as revealed in grit-blasting. HF-etched
zirconia is also shown to be bacteriostatic according a study (Han et al., 2017), possibly due to the sharp and spiky micro-/nanotopographical features on the surface
being not favorable for bacterial attachment.
Primer
Primer, by definition is a (Darvell, 2011):
Material used to treat a surface in order to prepare it for subsequent coating or
bonding, especially through the deposition of an intermediate layer.
In general, primers are used to unite two dissimilar materials by providing chemical bonds between them. In dental ceramics the most commonly used are silane
and phosphate coupling agents. These two coupling agents can change the surface
chemistry of ceramics, so that the resin cements are able to chemically bond to the
68
Advanced Dental Biomaterials
Figure 4.4 SEM images of zirconia without treatment, grit-blasted by silica-coated alumina,
and HF etched. XRD on bottomright revealed the monoclinic phase was presented in gritblasted zirconia surface, but only tetragonal phase was found in untreated and HF-etched
zirconia. NB: HF-etched zirconia created some nanospiky structures that are bacteriostatic.
HF, Hydrofluoric acid; SEM, scanning electron microscope; XRD, X-ray diffraction.
Source: From Liu, D., Tsoi, J.K.H., Pow, E.H.N., Wong, H.M., 2015. Influence of different
etching protocols on the reliability of resin bonding to CAD/CAM feldspathic porcelain. Int.
J. Adhes. Adhes. 62, 1824.
ceramics. Given the difference in chemical nature, these coupling agents are used
for different ceramics.
Recently, a study (Lung et al., 2018) has comprehensively reviewed the dental
silane adhesion mechanism. The most commonly used dental silane is 3-(methacryloyloxy)propyltrimethoxysilane (MPS). To have a successful silane adhesion on
ceramics the hydroxyl group (OH) on the ceramic surface plays an important role
(Fig. 4.5).
In terms of glass ceramics, hydroxyl groups come from the equilibrium reaction
between the chemisorbed water in atmosphere and SiO2. However, the amount of
OH is low. So, another aspect of HF etching is about the formation of silica gel
from the metasilicic acid (H2SiO3) upon dehydration [as revealed in Eq. (4.iv)].
The thin silica gel is highly active with a high amount of hydroxyl group.
For an oxide ceramic such as zirconia, as revealed in Fig. 4.4, it could not be
easily etched by HF, but it can be grit-blasted. The types of grits are influential for
Figure 4.5 Schematic diagram to illustrate the mechanism of silane coupling agent on ceramic surface.
70
Advanced Dental Biomaterials
the selection of a proper coupling agent. For example, to use silane as a primer for
zirconia, the grits should be silica-coated alumina. Such grits would enable a formation of silica layer on the zirconia surface which is reactable with silane. If ordinary
alumina is used for grit-blasting, then the primer of choice should be 10-MDP (10methacryloyloxydecyl dihydrogen phosphate), which is a phosphate coupling agent.
The reason is simple: 10-MDP can chemically react with ZrO2, ZrOH, and even
Zr41 as revealed on the zirconia surface in a study (Nagaoka et al., 2017).
Ideally, the primer layer should be as thin as possible because
the primer is shown to be the weakest (in strength) in an adhesive joint system
(substrateprimersubstrate). So, to control the thickness, various techniques
could be used. For example, using a flow of hot air on the primer layer deposited
on lithium disilicate was shown to yield a higher bond strength (Tian et al., 2014).
However, it should be noted that, achieving the single primer monolayer (i.e. only
one layer) in ordinary dental surface is not feasible. We should term the dental
primer layer as ultrathin film.
4.2.1.2 Mechanical surface conditioning
Grit-blasting
There are various reasons for blasting surfaces with grits in dentistry, for example,
to cleanse and to increase their surface roughness. Commonly, surface roughness is
one of the surface topographical parameters, which is measurable by profiling at a
microlevel (e.g. profilometer) or at a nanolevel (e.g. atomic force microscopy).
Grit-blasting can effectively increase the surface roughness and (also increase) the
surface area. As such, the micromechanical interlocking between two dissimilar
materials could be enhanced. Various grits are available for blasting the dental
ceramic surfaces, and the most commonly used are alumina (Al2O3) and silicacoated alumina. These grits are available in different sizes, and in dentistry, the
most commonly used are “marked” as 25, 50, and 110 μm, which indicate the average particule size within an acceptable range.
These particles also come with different shapes. Obviously, spherical grits are
effective in transferring the kinetic energy but not effective for abrasive actions
(plowing, cutting, and gouging) compared to sharp and angular grits. Also, the angle
and the distance between the blasting tip and ceramic substrate would also yield a
difference in adhesion (Ho et al., 2015). Thus, care should be taken in operation and
selection of grit-blasting parameters. For example, in the case of glass ceramics,
2550 μm alumina powders are commonly used at a pressure of 0.28 MPa. Zirconia
might need a higher pressure, say 23.5 bar, and be blasted with 30 μm (chairside)
or 110 μm (laboratory) grits that should be coupled with the suitable primers.
The ultimate drawback of grit-blasting is that it could also create sharp micro- or
nanocracks on the surface, and the heat generated during the blasting might be able
to partially melt the tip of cracks. One possible solution is to use HF to further etch
the surface and hence smoothen the crack tips. For zirconia the t to m transformation on zirconia happens during the blasting and is not easily detected (Liu et al.,
2013). Nevertheless, normally zirconia cracks from stress concentration areas, for
Ceramic materials in dentistry
71
example, cusps, thin margin, and also connectors. Therefore for the adhesion area,
grit-blasting appears to have no or little/minimal damaging effects.
Laser
Laser (light amplification by stimulated emission of radiation) has also been utilized as one of the surface treatment methods in ceramics. Various parameters, for
example, mode of action, irradiation (power), and wavelength, can be adjusted in
order to optimize the operation. A study (Liu et al., 2013) has successfully used a
high-power CO2 laser to make certain patterns on zirconia surface and improve porcelainzirconia bonding without t to m transformation. It should be noticed that
chipping from zirconia or porcelain is a crucial issue that is a catastrophic failure
and not reversible.
Polishing/grinding
A recent study (Ho et al., 2018) has revealed that different surface grinding procedures on zirconia would affect the surface roughness, thickness, fracture strength,
and biaxial flexural strength in various ways (Table 4.3).
Obviously, tungsten carbide should not be used in trimming or grinding zirconia
because the treatment will weaken the material. Diamond is preferred, and it does
not cause a huge reduction in zirconia thickness.
4.2.2 Bond strength evaluation
The oral cavity is a complex environment that is influenced by numerous intrinsic
and extrinsic factors, for example, temperature change, saliva, daily food and drink
intake, biting force, and other habits. Thus, in the evaluation of ceramic and its
adhesion, laboratory testing should take these variables into account so as to provide additional insights about the problems and solutions.
Common methods to evaluate resinceramic bond strength include shear, tensile, and four-point flexural bond strength tests. In particular the shear motion of
the crosshead applied on the resin at the resinceramic joint cannot give a “pure
shear” at the interface between resin and ceramic surfaces. Although it is true that
the tensile component could be reduced by placing the crosshead as close as possible to the ceramic substrate, there is no way to get a zero distance between the
crosshead and the ceramic substrate. Thus, “brittle shear” between two substrates
cannot be obtained, and “ductile” or “brittle-ductile” shears are observed, which
might contribute nonadhesive failures (Jin et al., 2016). So, despite the simplicity in
preparing the sample, the shear bond strength test has become less popular now. To
test the shear component more accurately, mold-enclosed shear bond strength and
lever-induced mold-enclosed shear bond strength tests are recommended.
Tensile bond strength test is currently a popular test to evaluate resinceramic
bond, and it is so far the best to evaluate tensile component (as the shear component is
minimal). Various bond configurations can be set, for example, two-substrate
(resinceramic) and three-substrate (ceramicresinceramic or ceramicresin
dentine) systems. A report (Tian et al., 2014) has shown the three-substrate
Table 4.3 Effects of different surface grinding procedures on zirconia’s thickness, roughness, breaking force, and biaxial flexural strength.
Groups
Mean thickness
reduction (mm)
Mean surface
roughness (µm)
Mean breaking
force (N)
Mean biaxial flexural
strength (MPa)
Coarse diamond
Fine diamond
Tungsten carbide
Fine tungsten carbide
Coarse diamond 1 fine tungsten carbide
Coarse diamond 1 air particle abrasion
Air particle abrasion
Control
0.14 6 0.03
0.05 6 0.02
0.07 6 0.01
0.13 6 0.04
0.27 6 0.04
0.21 6 0.04
0.09 6 0.02
0.88 6 0.01
(mean thickness)
5.76 6 0.75
2.52 6 1.22
3.52 6 0.53
2.27 6 0.87
4.49 6 0.40
6.05 6 0.79
3.28 6 0.67
0.44 6 0.16
337.39 6 69.17a
301.97 6 117.86
202.83 6 27.02a
145.26 6 30.72a
137.85 6 9.53a
349.52 6 66.76
372.63 6 68.96
453.25 6 56.59
840.57 6 181.37
598.89 6 241.19
412.01 6 43.13a
352.07 6 65.37a
495.15 6 62.28a
1070.41 6 199.59
840.38 6 176.62
788.34 6 92.32
a
The mean difference is significant at the 0.05 level (GamesHowell post hoc test) compared to dry control group.
Source: From Ho, C.M.B., Ding, H., Chen, X., Tsoi, J.K.H., Botelho, M., 2018. The effects of dry and wet trimming on the strength of dental zirconia. Ceram. Int. 44 (9),
1045110462.
Ceramic materials in dentistry
73
(ceramicresinceramic) system is a more reliable method to evaluate resinceramic
bond strength than the two-substrate (resinceramic) system, since the bond strength
value is higher and the Weibull modulus slightly higher. To “make” the bond test sensitive the area of tensile test should be small, say B1 mm2. This dimension is easily
achievable for lower strength ceramics such as glass ceramics. However, for highstrength ceramics, such as zirconia, cutting the specimen would not be that easy.
The four-point flexural bond strength is a new concept, which uses the threesubstrate system (e.g. ceramicresinceramic) and places the specimen on the
four-point bending test jig. The results are promising for the evaluation of
resinzirconia (Sanli et al., 2015) and resinlithium disilicate (Wong et al., 2017)
bonding. In particular, four-point flexural strength is more sensitive in the evaluation of the effects of different surface treatments on bonds. The comparison of
Weibull moduli and relative standard deviation has shown this method to be more
reliable than tensile bond strength test (Wong et al., 2017), even when the physical
size of the specimen is large. So, the sample preparation (especially for zirconia) is
easier.
4.2.3 Fatigue
A study (Homaei et al., 2016a) noticed that dental ceramics have a fatigue life distribution that can be fitted with Basquin formula:
σa 5 AðN ÞB
(4.4)
where σa is the stress amplitude, N is the cycles of failure, A is the coefficient constant, and B is the exponent constant. In addition, the fatigue limit of the maximum
load (σmax) can be calculated:
σmax 5 2σa 1 σmin
(4.5)
where σmin is the minimum load applied.
Table 4.4 revealed a summary between static and fatigue properties of zirconia,
lithium disilicate, and polymer-infiltrated ceramic network (PICN). It could be seen
that the fatigue limit of ceramics was approximately 45%55% of mean flexural
strength.
It should be noted that the ceramic fracture surfaces due to fatigue are much
smoother than under static loading. This is because of the second stage of fatigue
failure in which the crack propagates perpendicular to the tensile stress. Despite the
fact the ceramic fatigue happens in laboratory tests, in clinical situation, the ceramic
is bonded on the teeth. So, to evaluate the ceramic fatigue or fracture, ceramics
bonded on extracted teeth could give a good prediction on the materialteeth interaction. In another study (Homaei et al., 2016b), a ball indentation model on cyclic
fatigued CAD/CAM ceramic crowns on human premolars revealed that the average
fatigue limit for lithium disilicate is B900k cycles (for 1400 N), and B380k cycles
74
Advanced Dental Biomaterials
Table 4.4 Static and fatigue properties of zirconia, lithium disilicate, and polymerinfiltrated ceramic network (PICN).
vis-v
Four-point
flexural strength
σ 0 (MPa)
Fatigue of stress
amplitude σa (MPa)
Fatigue limit of
maximum load
σ max (MPa)
Zirconia
Lithium dilisilicate
PICN
886.9
356.7
135.8
247.1
81.2
33.9
500.1
168.4
73.8
Source: From Homaei, E., Farhangdoost, K., Tsoi, J.K.H., Matinlinna, J.P., Pow, E.H.N., 2016a. Static and fatigue mechanical behavior
of three dental CAD/CAM ceramics. J. Mech. Behav. Biomed. Mat. 59, 304313; Homaei, E., Farhangdoost, K., Pow, E.H.N.,
Matinlinna, J.P., Akbari, M., Tsoi, J.K.H., 2016b. Fatigue resistance of monolithic CAD/CAM ceramic crowns on human premolars.
Ceram. Int. 42, 1570915717.
for PICN (for 870 N). This said, both materials can survive under normal masticatory forces, and interestingly both materials would mostly fracture above the
cementoenamel junction which means it is restorable.
In addition, a new attempt (Homaei et al., 2018) using finite element method
with the fatigue Eq. (4.4) has demonstrated that the development of shear stress
concentration in the margin is important in resinceramic bonding failure because
the enamel failed in the adjacent area to the interface. This is in agreement with
some of the experimental data and also signifies the importance of shear component
in bond strength test.
4.3
Ceramic biological interaction
Biological substances, such as cells and bacteria, can attach on any surface in any
favorable conditions, such as temperature and humidity. The surface characteristics,
cell/bacterial types and properties, as well as the serum proteins and oral environments play significant roles in the growth of these biological substances. In particular, in the case of oral bacteria, there are more than 700 species of microbes
existing in the oral cavity, and they can form biofilm that is defined as
(Samaranayake, 2018)
Complex, functional community of one or more species of microbes, encased in an
exopolysaccharide matrix and attached to one another or to a solid surface
In terms of ceramics, various surface parameters would contribute to the bacterial attachment. These are either (1) chemically or (2) physically related.
4.3.1 Surface chemistry
As illustrated in Fig. 4.5, the ceramic surface has a lot of hydroxyl (OH) groups.
Under different pH together with different content of salivary ions and molecules,
2
the hydroxyl groups would be protonated (2OH1
2 ), deprotonated (O ), or stay as
Ceramic materials in dentistry
75
they are, all due to chemical equilibrium. These chemical groups can attract various
bacteria with van der Waals forces, electrostatic or Coulomb interactions. Most of
the time, the ceramic substrate would be firstly coated with proteins and then bacteria. In terms of cells, the OH is attractive to osteoblasts. For example in zirconia,
due to the adsorption of water molecules, a partially hydroxylated surface is formed
(Fig. 4.6).
With the addition of the OH on zirconia, the crystalline structure at the surface
is no longer intact. Chemically speaking, the bond lengths between ZrO and
ZrOH are different. Thus, the volume (V) at the surface that contains both ZrO
and ZrOH is different from its original form. According to thermodynamic principle, that is,
G 5 U 1 pV TS
(4.6)
where G the Gibbs free energy would be increased with increase of V, given that U
the internal energy, p the pressure, T the temperature, and S the entropy are
unchanged. This said, the partially hydroxylated surface is not that stable and therefore “activated.”
It is also interesting to note that such a hydroxylated surface contains “clusters”,
such that different sizes of the clusters would yield different energy (Eg) between
the highest occupied (HOMO) and the lowest unoccupied molecular orbitals
(LUMO). Fig. 4.7 illustrates the HOMO and LUMO for ZrO2 clusters for Zr number of 12.
In fact the zirconia surface shows Eg with 4.55.5 eV, which is a semiconductor
range and similar to other chemicals that have osseointegration effect such as titania
(TiO2) and hafnia (HfO2). Although the biological knowledge on this aspect is
Figure 4.6 Schematic diagram to illustrate the partially hydroxylated (in red square) surface
on zirconia.
76
Advanced Dental Biomaterials
Figure 4.7 HOMOLUMO illustration for ZrO2 clusters (Zr atom number 5 12). Redblue
paired dumbbell-shaped orbitals are the orbitals. We can see the orbitals are confined mainly
at the oxygen atoms (in red) rather than zirconium atoms (gray). HOMO, Highest occupied
molecular orbitals; LUMO, lowest unoccupied molecular orbitals.
limited, such a capacitor-like material would be able to show a certain kind of electrical stimulation that provides another pathway for osseointegration or at least
induces the levels of proteins via van der Waals force guidance (Zhuang et al.,
1997). Therefore, the biological interaction is enhanced.
Some silanes, such as 3-MPS, have been proven to diminish the amount and viability of Candida albicans on zirconia. However, some other silanes, such as 3acryloxypropyltrimethoxysilane (ACPS), may not give the same effects (Villard
et al., 2014). Interestingly, MPS on zirconia would make the surface hydrophilic
and decrease the surface free energy, but not ACPS. The reason is unknown and
worth further investigation.
4.3.2 Physical parameters
Various factors, such as roughness and texture, belong to the physical parameters
that will contribute to the bacterial and cellular adhesion, in particular during the
initial stage. In general a rougher surface would attach more biological substances
because the surface can easily trap the substances physically. Therefore, the ceramics should be treated in different ways depending on the application.
If applied for veneer, crown, and bridges, the inner surface should be rough in
order to bond well. However, the esthetic surface should be smooth or even glazed
to make sure the surface cannot be easily attached by bacteria. For an implant body
(such as screw), obviously the zirconia should be roughened in order to promote the
Ceramic materials in dentistry
77
osteoblastic reaction. Nevertheless, to prevent periimplantitis, the screw neck part
should be smoothened. Another approach could be using hot HF to etch the neck
part so as to actively shred the bacteria (Han et al., 2017) by the nanospiky surface.
4.3.3 Sterilization methods
In implant application, a sterilization procedure is necessary for all implant components. Ultraviolet light (UV), autoclave, and gamma waves are commonly used in
dental industry for the sterilization of implants. A laboratory study (Han et al.,
2018) has compared the biofilm formation on different sterilization methods on zirconia. The results revealed that a dry heat-autoclaved sample has a significantly
lower bacteria content than other groups, even better than UV-C and gamma ray.
High-energy UV-C and gamma ray would even change the color of zirconia, possibly due to the electrons in the quantized energy levels of ZrO being excited. This
is also an important indication for a laboratory that a proper sterilization method
should be adopted for testing the antibacterial property.
4.4
Conclusion
This chapter has provided a quick summary on the classification of dental ceramics,
adhesion, and biological interaction. In particular, glass ceramics and zirconia play
a major role nowadays with some new developments from polymer-infiltrated
ceramic networks. In terms of resinceramic adhesion, HF is useful to etch glasscontaining ceramics and grit-blasting can roughen the oxide ceramic surfaces. A
successful adhesion also relies on primer (coupling agents). Bacteria and cells can
attach onto ceramic surfaces. We can conclude that ceramic materials are very useful in dentistry, and a proper understanding is essential.
References
Botelho, M.G., Dangay, S., Shih, K., Lam, W.Y.H., 2018. The effect of surface treatments on
dental zirconia: an analysis of biaxial flexural strength, surface roughness and phase
transformation. J. Dent. (in press).
Darvell, B.W., 2011. A Glossary of Terms in Dental Materials Science, eleventh ed.
Fabian Fonzar, R., Carrabba, M., Sedda, M., Ferrari, M., Goracci, C., Vichi, A., 2017.
Flexural resistance of heat-pressed and CAD-CAM lithium disilicate with different
translucencies. Dent. Mater. 33, 6370.
Han, A., Tsoi, J.K.H., Matinlinna, J.P., Chen, Z., 2017. Influence of grit-blasting and hydrofluoric acid etching treatment on surface characteristics and biofilm formation on zirconia. Coatings 7 (8), 130.
Han, A., Tsoi, J.K.H., Matinlinna, J.P., Zhang, Y., Chen, Z., 2018. Effects of different sterilization methods on surface characteristics and biofilm formation on zirconia in vitro.
Dent. Mater. 34 (2), 272281.
Ho, B.J., Tsoi, J.K.H., Liu, D., Lung, C.Y.K., Wong, H.M., Matinlinna, J.P., 2015. Effects of
sandblasting distance and angles on resin cement bonding to zirconia and titanium. Int.
J. Adhes. Adhes. 62, 2531.
78
Advanced Dental Biomaterials
Ho, C.M.B., Ding, H., Chen, X., Tsoi, J.K.H., Botelho, M., 2018. The effects of dry and wet
trimming on the strength of dental zirconia. Ceram. Int. 44 (9), 1045110462.
Homaei, E., Farhangdoost, K., Tsoi, J.K.H., Matinlinna, J.P., Pow, E.H.N., 2016a. Static and
fatigue mechanical behavior of three dental CAD/CAM ceramics. J. Mech. Behav.
Biomed. Mat. 59, 304313.
Homaei, E., Farhangdoost, K., Pow, E.H.N., Matinlinna, J.P., Akbari, M., Tsoi, J.K.H.,
2016b. Fatigue resistance of monolithic CAD/CAM ceramic crowns on human premolars. Ceram. Int. 42, 1570915717.
Homaei, E., Jin, X.Z., Pow, E.H.N., Matinlinna, J.P., Tsoi, J.K.H., Farhangdoost, K., 2018.
Numerical fatigue analysis of premolars restored by CAD/CAM ceramic crowns. Dent.
Mater. (in press).
Ionascu, C., 2008. High Temperature Mechanical Spectroscopy of Fine-Grained Zirconia and
Alumina Containing Nano-Sized Reinforcements (Ph.D. thesis). Lausanne, EPFL.
IUPAC Goldbook, 2007. Definitions of Terms Relating to the Structure and Processing of
Sols, Gels, Networks, and Inorganic-Organic Hybrid Materials (IUPAC
Recommendations 2007), vol. 79, p. 1801.
Jin, X.Z., Homaei, E., Matinlinna, J.P., Tsoi, J.K.H., 2016. A new concept and finite-element
study on dental bond strength tests. Dent. Mater. 32, e238e250.
Leung, B.T.W., Tsoi, J.K.H., Matinlinna, J.P., Pow, E.H.N., 2015. Comparison of mechanical
properties of three machinable ceramics with an experimental flurophlogopite glass
ceramic. J. Prosthet. Dent. 114 (3), 440446.
Liu, D., Matinlinna, J.P., Tsoi, J.K.H., Pow, E.H.N., Miyazaki, T., Shibata, Y., et al., 2013. A
new modified laser pretreatment for porcelain zirconia bonding. Dent. Mater. 29,
559565.
Liu, D., Tsoi, J.K.H., Pow, E.H.N., Wong, H.M., 2015. Influence of different etching protocols on the reliability of resin bonding to CAD/CAM feldspathic porcelain. Int. J.
Adhes. Adhes. 62, 1824.
Lung, C.Y.K., Matinlinna, J.P., Tsoi, J.K.H., 2018. Silane adhesion mechanism in dental
applications and surface treatments: a review. Dent. Mater. 31 (1), 1328.
Nagaoka, N., Yoshihara, K., Feitosa, V.P., Tamada, Y., Irie, M., Yoshida, Y., et al., 2017.
Chemical interaction mechanism of 10-MDP with zirconia. Sci. Rep. 7, 45563.
Samaranayake, L.P., 2018. Essential Microbiology for Dentistry (5th Edition), Elsevier.
Sanli, S., Comlekoglu, M., Comlekoglu, E., Sonugelen, M., Pamir, T., Darvell, B.W., 2015.
Influence of surface treatment on theresin-bonding of zirconia. Dent. Mater. 31,
657668.
Tian, T., Tsoi, J.K.H., Matinlinna, J.P., Burrow, M.F., 2014. Evaluation of microtensile bond
strength on ceramic-resin adhesion using two specimen testing substrates. Int. J. Adhes.
Adhes. 54, 165171.
Villard, N., Seneviratne, C., Tsoi, J.K.H., Heinonen, M., Matinlinna, J.P., 2014. Candida
albicans aspects of novel silane systemcoated titanium and zirconia implant surfaces.
Clin. Oral Imp. Res. 26, 332341.
Wong, A.C.H., Tian, T., Tsoi, J.K.H., Burrow, M.F., Matinlinna, J.P., 2017. Aspects of adhesion tests on resin-glass ceramic bonding. Dent. Mater. 33, 10451055.
Zhang, Y., 2014. Making yttria-stabilized tetragonal zirconia translucent. Dent. Mater. 30,
11951203.
Zhuang, H., Wang, W., Seldes, R.M., Tahernia, A.D., Fan, H., Brighton, C.T., 1997.
Electrical stimulation induces the level of TGF-b mRNA in osteoblastic cells by a mechanism involving calcium/calmodulin pathway. Biochem. Biophy. Res. Commun. 237,
225229.
Acrylic denture base materials
5
Touraj Nejatian1,2, Sajjad Pezeshki3 and Azeem Ajaz4
1
Eastman Dental Institute, University College of London, London, United Kingdom,
2
Nottingham Dental Clinic, Nottingham, United Kingdom, 3Babol University of Medical
Sciences, Babol, Iran, 4Department of Prosthodontics and Dental Implantology, College of
Dentistry, King Faisal University, Al-Ahsa, Kingdom of Saudi Arabia
Chapter Outline
5.1 Introduction 79
5.2 Ideal properties of a denture base material 80
5.3 Acrylic denture base materials 80
5.3.1 Development of denture base materials 80
5.3.2 Chemical structure and mechanism of polymerization
5.3.3 Commercial forms and composition 85
82
5.4 Modified and novel denture base materials and manufacturing
technologies 86
5.4.1
5.4.2
5.4.3
5.4.4
5.4.5
5.4.6
5.4.7
Rubber-reinforced resins 87
Fiber-reinforced resins 87
Particulate-reinforced resins 89
Hybrid reinforcement 91
Hypoallergenic resins 91
Thermoplastic resins 92
Novel technologies in manufacturing removable denture base
5.5 Denture lining materials
5.5.1
5.5.2
5.5.3
5.5.4
Clinical indication 94
Hard relining 95
Soft relining 96
Tissue conditioners 98
5.6 Acrylic artificial teeth
5.7 Conclusion 100
References 100
Further reading 104
5.1
93
94
99
Introduction
A denture base is a part of a denture that rests on soft tissue, replaces lost soft tissue, and retains the artificial teeth, which require the endurance of various types of
stresses. Various types of materials have been used in the construction of denture
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00005-0
Copyright © 2019 Elsevier Ltd. All rights reserved.
80
Advanced Dental Biomaterials
bases including cellulose products, epoxy resins, polystyrene, polycarbonates,
Bakelite, vinyl resin, nylon, and vulcanite. From 1840 to 1940 different kinds of
materials were introduced as denture base materials including wood, ivory, and
metal, along with porcelain or natural teeth. The appearance and durability of these
materials were not desirable, and the use of mechanical retentive devices was the
main method of securing dentures. Vulcanite was produced by heating natural rubber and sulfur, and was the first material to be used for mass production of dentures; however, the undesirable color was its disadvantage. Vinyl resins have low
fracture resistance, probably because of their inferior fatigue resistance. The introduction of phenol-formaldehyde (Bakelite) and cellulose nitrates at the beginning of
the 20th century was another step in the development of denture bases. However,
because of the difficulties in processing and unstable color of Bakelite and warpage
of cellulose nitrates as well as its bad taste, they were still far from a desirable denture base material. From 1937 vulcanite was replaced by polymethyl methacrylate
(PMMA). Acrylic polymers are now used in prosthetic dentistry as artificial teeth,
for denture repair, as facings in crown and bridges, impression trays, record bases,
temporary crowns, and obturators of cleft palates.
5.2
Ideal properties of a denture base material
A denture should function for a reasonable period in a hostile oral environment
without having adverse effects on oral and general health of patients. This means a
denture base should have certain characteristics which are summarized in Table 5.1
(Anusavice et al., 2012; Alla, 2013; Rickman et al., 2012).
5.3
Acrylic denture base materials
5.3.1 Development of denture base materials
From 1840 to 1940 different kinds of materials were employed as denture base
materials, but the appearance and durability of these materials were not desirable,
and the use of mechanical retentive devices was necessary.
Vulcanite: It was the first material which was used for mass production of dentures and produced by heating natural rubber and sulfur. Its disadvantage was the
unfavorable color and porosity that led to an unhygienic denture base (Tandon
et al., 2010).
Celluloid: It is produced by plasticizing cellulose nitrate with camphor after
which the pigmentation is accomplished. A denture base is fabricated by pressing
the celluloid blank into a dry, heated mold. Rapid discoloration, water absorption,
persistent residual camphor taste, and difficulties in repair are the disadvantages of
celluloid (Khindria et al., 2009).
Bakelite: The introduction of phenol-formaldehyde (Bakelite) at the beginning
of the 20th century was another step in the development of denture bases. However,
Acrylic denture base materials
81
Table 5.1 Requirements of a denture base material.
Property
Biological
Chemical
Requirements
G
G
G
G
Mechanical
G
G
G
G
G
G
G
G
Thermal
G
G
G
Esthetic
G
G
Other
G
G
G
G
G
G
G
Should be neutral, nontoxic, nonirritant, and noncarcinogenic
Should be insoluble and nonreactive in the oral fluids or any other food
ingredient
Should not absorb fluids which cause dimensional changes
Should be compatible and bond very well with artificial teeth and liners
Should have a high modulus of elasticity and rigid enough against
masticatory forces
Should be resilient enough to absorb masticatory force to protect the
underlying soft tissues
Should have a high elastic limit and proportional
Limit to prevent the permanent deformation against stresses
Should have adequate fatigue resistance and impact strength to
withstand the cyclic masticatory force and impact forces, respectively
Should be dimensionally stable
Should have adequate abrasion resistance
Specific gravity should be low (especially for maxillary dentures)
Should be a good thermal conductor to encourage natural stimuli and
avoid accidental burning of oral tissue
COTE should match with that of the artificial teeth to avoid
concentration of stress on the toothdenture interface
Should have a softening temperature above boiling temperature of
water
Should exhibit sufficient translucency so that it can be made to match
the appearance of the oral tissues
Should be capable of being tinted or pigmented
Should maintain the desirable properties for an extended period after
manufacture
Should be inexpensive
Should be easy to manipulate
Should be radiopaque so that they can be detected if some part of the
denture is accidentally swallowed
Should be easy to repair
Should be easy to clean
Should have a long shelf life
COTE, Coefficient of thermal expansion.
because of the difficulties in processing and repair, and unstable color of Bakelite
and its bad taste, it was still far from a desirable denture base material (Noort and
Barbour, 2013). From 1937 vulcanite was replaced by PMMA.
Polyvinyl chloride (PVC): PVC is still being used as a denture lining material
and for the construction of athletic mouth guards. Vinyl resins have low fracture
resistance, probably because of their inferior fatigue resistance. They harden over
time because the plasticizer leaches out during service.
82
Advanced Dental Biomaterials
Its polishing is difficult; therefore, it results in poor denture hygiene and acts as
an irritant to the oral mucosal tissues (Munksgaard, 2004).
PMMA: In prosthetic dentistry, there are multiple applications for acrylic resins
such as artificial teeth, for denture repair, as facings in crown and bridges, impression trays, record bases, temporary crowns, and obturators of cleft palates.
Completely polymerized PMMA is highly transparent. Heat-cured acrylic resin dentures contain 0.2%0.5% and the self-cured acrylic resin dentures contain 2%5%
(Bahrani et al., 2012) methyl methacrylate as a residual monomer. This residual
monomer has the potential to evoke irritation, inflammation, and allergic response
of the oral mucosa. Further, the residual monomer can produce both stomatitis and
angular cheilitis. Toxic and allergic effects of acrylics depend on several variables,
including polymermonomer ratio, storage time and water immersion, type of
polymerization cycle, and polymerization method used (Jorge et al., 2003).
Acrylic resins are soluble in aromatic hydrocarbons, ketones, and esters and
much less soluble in water comparatively. Alcohol functions as a plasticizer and
reduces the glass transition temperature. Therefore solutions containing alcohol
should not be used for cleaning or storing the dentures. The water absorption of the
PMMA changes the dimension of the denture when alternately soaked in water and
dried which leads to crazing (Rimple et al., 2011). Due to ease of processing, low
cost, light weight, excellent esthetic properties, low water sorption and solubility,
and ability to be repaired easily, PMMA is a popular denture base material.
However, low thermal conductivity, inferior mechanical strength, brittleness, high
coefficient of thermal expansion, and relatively low modulus of elasticity are its
weakness during the clinical service (Sakaguchi and Powers, 2007). Research in
this area is aimed at modifying the composition or reinforcing the PMMA with
stronger materials and developing new materials with better properties. The
approaches include modifying the composition with copolymers, reinforcing the
dentures with various fibers such as aramid fibers, carbon/graphite fibers, polyethylene fibers, and glass fibers, and also reinforcing with various metallic fillers and
nanoparticles (NPs), such as silica and titania NPs. Almost all denture materials are
radiolucent. An addition of bismuth (10%15%) or uranyl salts provides adequate
radiodensity but at the cost of the increased transverse deflection and water sorption. Producing clinically acceptable levels of radiopacity without degrading physical and esthetic properties of the acrylic resin still remains a challenge (Bloodworth
and Render, 1992).
5.3.2 Chemical structure and mechanism of polymerization
Methyl methacrylate monomers (the formula is shown below), by using the process
of free-radical addition polymerization, make PMMA, which is the main component
of acrylic resin denture bases. This process includes the sequence of activation, initiation, propagation, and termination. Depending on the activation process, they are
classified as heat-cured, cold-cured, light-activated, and microwave-cured acrylic
resins (Sakaguchi and Powers, 2007).
Acrylic denture base materials
83
H Me
C=C
H C=O
O
Me
The methyl methacrylate structure is formed by additional polymerization in
which free-radical polymerization reactions occur with molecules containing carbon
double bonds, which is a reaction without a by-product accelerated by heat, light,
chemicals, and traces of peroxides. The reaction is initiated by a free radical made
by one of these methods. The initiation stage is followed by the propagation stage
in which other monomers bound to the free radical speedily shift the free electron
to the end of the chain. The chain continues growing until free radicals are terminated. The termination stage can take place in several ways. Any material that can
react with a free radical can reduce the initiation or increase the rate of termination.
Decreasing the initiation retards polymerization and increasing the rate of termination reduces the degree of polymerization or molecular weight of the final polymer.
Hydroquinone, eugenol, or large amounts of oxygen will inhibit or retard the polymerization. Therefore a small amount of hydroquinone is used to increase the shelf
life of the monomer (Bartoloni et al., 2000).
5.3.2.1 Curing mechanisms of acrylic denture base materials
Heat-cured acrylic resins
These materials are usually supplied as a powder and liquid. The composition of
the powder includes beads or granules of PMMA, benzoyl peroxide as an initiator,
pigment/dyes, opacifiers—titanium/zinc oxides, plasticizer (dibutyl phthalate), and
synthetic fibers (nylon/acrylic).
Components of the liquid are methyl methacrylate monomer, inhibitor (hydroquinone), and cross-linking agent (ethylene glycol dimethacrylate). Good physical
properties are achieved by the high degree of polymerization, but the adaptation to
the tissues is poor due to polymerization contraction, thermal contraction, and the
strain accompanying stress release during deflasking. Although heat-activated
acrylic resins have certain flaws, they are still one of the most commonly used
materials for denture fabrication (Anusavice et al., 2012).
There is another type of heat-cured resin named as rapid heat-polymerized resin
which is a hybrid acrylic that is polymerized within 20 minutes in boiling water.
The initiator is a combination of both chemical and heat-activated initiators used to
speed up the processing (Jerolimov et al., 1989).
84
Advanced Dental Biomaterials
Cold-cured acrylic resins
The chemistry of this kind of acrylic resin is similar to that of heat-cured resins
except that the cured is initiated by a tertiary amine (e.g., dimethyl-p-toluidine or sulfinic acid) instead of heat. The size of the polymer beads is smaller than the heatcured resin to ease the dissolution in the monomer to produce the dough before going
to that level of curing reaction, which prevents proper adaptation of the mixture to
the mold. Also, because the method of curing is not as efficient as the heat curing
technique, the outcome is lower molecular weight polymers which in turn results in
a lower strength property, higher residual monomer, lower color stability, and lower
glass transition temperature of the resin (with Tg being typically 75 C80 C).
Therefore these materials are highly susceptible to creep, and this can contribute significantly to the eventual distortion of the denture when in use (van Noort, 2012).
The radical polymerization of the surface layer is inhibited by oxygen due to deactivation of free radicals produced by the initiator. It was proposed that the polymerization process should be carried out in water in order to obtain an adequate degree of
polymerization on the surface of autopolymerizing PMMA resin (Vallittu, 1999).
Advantage: Greater dimensional accuracy due to reduced polymerization shrinkage.
Visible lightcured resins
The composition of these resins is more similar to restorative composites than denture base materials because of their matrix, which is urethane dimethacrylate
(UDMA), which contains a small amount of colloidal silica to control the flowability. Their filler consists of acrylic beads that become part of an interpenetrating
polymer network structure when cured. Camphorquinone, as a photoinitiator, is
included in this composition, so it needs special equipment for polymerization
(Anusavice et al., 2012). The acrylic is polymerized in a light chamber with blue
light at the wavelength of 400500 nm (Sakaguchi and Powers, 2007).
According to Takamata and Setcos (1989), mechanical characteristics of these
denture base materials are slightly lower than those of the conventional PMMA.
Visible lightactivated acrylic resins provide dentures that have an accurate fit and
superior strength. They allow for complete polymerization without residual compounds, ease of fabrication, and manipulation ability to bond with other denture
base resins and low bacterial adherence (Ogle et al., 1986). However, visible lightactivated acrylic resin is more brittle than PMMA denture resin. Therefore it is
commonly used for relines and repairs rather than for laboratory fabrication of the
entire denture base.
Advantages: Nontoxic and methyl methacrylate-free denture base resins, less
porous than chemically activated denture base resins, facilitate fabrication and final
adjustment of the mouth, decreased polymerization shrinkage.
Disadvantages: In the conventional manner the resins are opaque and cannot be
used, and this system is technique sensitive (Tandon et al., 2010).
Microwave-cured acrylic resins
In 1968 a microwave-activated denture base material was introduced. Metallic
flasks cannot be used as microwaves do not pass through them. Specially designed
Acrylic denture base materials
85
plastic flasks and special microwave machines are needed for this procedure. Some
studies showed comparable results to heat-cured acrylic resins, and some even
showed more accuracy of fit and lower residual monomer (Sakaguchi and Powers,
2007).
Advantages: Reduced curing time (3 minutes), and dough-forming time, color
stability, less fracture of artificial teeth and resin bases, and superior denture base
adaptation, lower residual monomer, most stable.
Disadvantages: Less bond strength to the denture teeth. Increased porosity due to
heat entrapment in the nonmetallic flasks. The plastic flasks and polycarbon bolts
are relatively expensive and tend to break down on exceeding packing pressure
(1200 psi) and after processing several dentures (Tandon et al., 2010).
Pour-type denture resins
This is a type of cold-cured resin, which commonly named as fluid resins. After
mixing, the resulting slurry is so flowable that it can be poured into agar hydrocolloid or silicone or modified plaster molds. The small sizes of beads or powder of
pour-type resins are the main difference between them and cold-cured resins
(Sakaguchi and Powers, 2007). Centrifugal casting and injection mold methods are
techniques used to inject the slurry into the mold. In comparison with heat and
cold-cured ones, these offered improved adaptation, dimensional stability, reduced
cost, and simple procedure but had low strength, higher solubility, and high residual
monomer levels (Tandon et al., 2010).
5.3.3 Commercial forms and composition
5.3.3.1 Powderliquid form
There are three reasons for the particular formulation of a powderliquid system:
1. By reaching the dough stage, the processing and packing of the resin under pressure is
possible. In addition, in cold-cured types the manipulation and adaptation of the dough on
the model and trimming off any excess to produce special trays are more convenient.
2. The polymerization shrinkage is reduced in comparison with monomer because the material being used (i.e., the beads or granules) has already been polymerized. Granules dissolve more readily in monomer than beads and go quickly to the doughy stage.
3. Exothermic reaction of polymerization caused by converting CQC to CC is reduced
due to the previous substantial polymerization (Noort and Barbour, 2013).
Powder
1. Acrylic polymer (PMMA) may be modified with ethyl, butyl, or other alkyl methacrylates
to improve its strength.
2. Initiator such as benzoyl peroxide or diisobutylazonitrile to initiate the polymerization of
monomer liquid after being added to the powder.
3. Tissue-like shades of pigments such as mercuric sulfide, ferric oxide, or carbon black.
These pigments may be combined into the polymer beads by adding them during the polymerization or mechanically mixed with the polymer beads after polymerization.
4. Zinc or titanium dioxides are used as opacifiers.
86
Advanced Dental Biomaterials
5. Dyed synthetic fibers made from nylon or acrylic are usually added to make natural oral
mucosa and simulate the shape of blood vessels.
6. Dibutyl phthalate may be added to powder or monomer as a plasticizer.
7. Heavy metal compounds of elements such as barium or radiopaque glass fillers are added
to improve the radiopacity. Desirable radiopacity can be achieved by adding 20% by
weight of these compounds, which leads to a reduction in the strength of the material and
changes in the appearance of the denture. Also, bismuth or uranyl salts at concentrations
of 10%15% and zirconyl dimethacrylate at 35% have been used. Recently, a new radiopaque terpolymer has been synthesized containing 20 30 50 -triodobenzyoyl ethyl methacrylates, methyl methacrylates, and 2-hydroxyethyl methacrylates, which may be used as
denture-based materials (Sakaguchi and Powers, 2007).
Liquid
1. The liquid part of the powderliquid-type acrylic resin is methyl methacrylate.
2. The inhibitor, which is added to prevent early polymerization, is generally hydroquinone
in a concentration of 0.003%0.1%.
3. In self-curing resins, tertiary amines, sulfinic acids, or the more stable salts of sulfinic
acid are used as an accelerator and may be added to increase the speed of peroxide
decomposition and enable the polymerization of the monomer at room temperature. The
commonly used amines are N,N-dimethyl-para-toluidine and N,N-dihydroxyethyl-paratoluidine. These types of resins may be called cold-curing or autopolymerizing resins.
4. Plasticizers are sometimes included to make the polymer softer and more resilient and are
commonly low-molecular-weight esters, such as dibutyl phthalate. The mechanism of the
effect of these molecules is that they interfere with the interaction between polymer molecules not entering the polymerization reaction. Unfortunately, the release of these materials into the oral fluid hardens the denture base. Some higher esters such as butyl or octyl
methacrylate have been used to cope with the problem. They polymerize making an internal plasticizer and do not leach out in oral fluids. Thus the denture remains flexible.
5. Some cross-linking materials that have reactive CR 5 CH groups at opposite ends of
the molecules can link long polymers together which is desirable. Glycol dimethacrylate
is one of these “cross-linking” materials. Cross-linking materials increase resistance to
minute surface cracking, termed crazing (Sakaguchi and Powers, 2007).
5.3.3.2 Gel form
Some of the denture materials such as vinyl acrylics can be supplied in a gel form;
their composition is the same as powderliquid types except for their chemical
accelerators, which cannot be used with the initiator in the monomer. They need a
light resource as an alternative curing route.
5.4
Modified and novel denture base materials and
manufacturing technologies
PMMA is the most popular denture base material because of its excellent properties, such as good esthetics, ease of processing and repair, and low cost. However,
it is still far from an ideal denture base material because of residual monomers
Acrylic denture base materials
87
which may cause allergies (Danilewicz-Stysiak, 1971), poor mechanical strength,
low fatigue strength, brittleness, poor conductor of heat, low hardness, high coefficient of thermal expansion, thermal shrinkage, poor color stability of self-cured
resins, porosity, crazing, warpage, and poor adhesion to metal and porcelain teeth
(Nandal et al., 2013).
Addition of fillers and fibers to PMMA is a commonly used method to improve
both its physical and mechanical properties. Many additives have been suggested to
enhance the properties of denture base resin, such as fibers, fillers, or nanofillers.
5.4.1 Rubber-reinforced resins
Incorporation of rubber, a low-molecular-weight butadiene styrene, either in polymer beads or matrix of PMMA makes “high impact” resins. This group has greater
impact strength and fatigue resistance. Rubber is thought to slow down crack propagation through the denture base material, which improves their fracture resistance.
Despite the improvement of the impact strength, Young’s modulus drops, making
this a flexible denture. This type of the denture base resin is indicated for patients
who drop their dentures repeatedly, for example, Parkinsonism, senility. These
materials are available as powderliquid with processing similar to heat-cured
resins (Rodford, 1990).
5.4.2 Fiber-reinforced resins
Fibers are used to improve the flexural and impact strength as well as the fatigue
resistance of the resin. However, the mechanical behavior of the material is affected
by the orientation of the fibers. It is suggested that parallel arrangement of the
fibers gives the optimum reinforcement (Jagger et al., 2002). Reinforcement of the
denture base can be done by fiber weave, namely total fiber reinforcement, or by
fiber bundles at the weak areas of the denture, named as partial fiber reinforcement
(Figs. 5.15.3).
Factors that affect the strength of these composites are (1) adhesion between the
fibers and the polymer (Vallittu and Lassila, 1992); (2) impregnation of the fibers
with the polymer (Jagger and Harrison, 1999); (3) the concentration of the fibers
(Vallittu et al., 1994); (4) test condition; (5) composition of resin; and (6) fiber
form, fiber fraction, fiber position, and orientation (Kim and Watts, 2004). Carbon
fibers (6570 mm length, 5% by weight and treated with silane coupling agent) are
inserted during packing. These fibers have high elastic properties and high resistance to fatigue, which permits the denture to behave like a spring under the occlusal stress and can spread forces evenly throughout the denture. Their strengthening
effects can be improved by silanation of the fibers (Vallittu and Lassila, 1992).
After the 1980s, despite early promising results, carbon fibers lost favor because of
their disadvantages, such as potential toxicity, poor esthetics, polishing problems,
difficult handling, and precise placement of the fibers inside the resin (Jagger and
Harrison, 1999; Vallittu, 1996).
88
Advanced Dental Biomaterials
Figure 5.1 Fiber placed in a tension zone to stop crack propagations.
Figure 5.2 Fibers placed at the fracture line.
Figure 5.3 Total fiber reinforce placed superficially.
Aramid fibers are aromatic polyamide fibers, generally called Kevlar fibers, that
have superior wettability and do not require any treatment with a coupling agent.
They enhanced the fracture resistance of acrylic resin denture base material
(Vallittu and Lassila, 1992); however, the hardness of the resin decreased with
increasing fiber concentration. Their unsuitable yellow color and exposure on the
surface of the denture makes the denture inconvenient for patients and creates polishing problems for the technician (Kanie et al., 2000).
Nylon fibers are polyamide fibers primarily based on aliphatic chains and their
main advantage is resistance to shock and cyclic stress. However, water absorption
Acrylic denture base materials
89
has an adverse effect on their mechanical properties. John et al (2001) showed that
nylon fibers can improve the flexural strength of PMMA. Nylon increased the fracture resistance of PMMA, as it has high resistance to continual stress. Therefore
incorporating nylon fiber in PMMA increased its structural elasticity (Soygun et al.,
2013).
Polyethene and polypropylene fibers have been used because of their better
esthetic characteristics than other fibers. However, these fibers require a surface
treatment to increase the impact strength of PMMA significantly (Yu et al., 2012).
Glass fibers are mainly used because of their excellent esthetic appearance as
well as reinforcement. These fibers have been used in different forms such as
woven, loose and continuous (John et al., 2001), or bundles. Increasing fracture
resistance of PMMA has been shown to depend on the strong adhesion between
glass fibers and the acrylic resin matrix. The silanized glass fibers provide better
flexural strength and the position and concentration of glass fibers within the polymer greatly affects the strength (Vallittu et al., 1994).
Continuous fibers provide superior reinforcement but orienting continuous fibers
at weak parts of the denture is difficult, and there is a risk of void formation inside
the fiberpolymer matrix system. Glass fibers may be modified by plasma polymerization techniques using hydroxy-ethyl methacrylate (HEMA), ethylenediamine
(EDA), and tetraethylene glycol dimethyl ether (TEGDME) (Ladizesky et al.,
1992).
5.4.2.1 Position and placement of fibers
1. Placing the fibers in tension zone in a denture during mastication, which is considered as
the weakest area.
2. Placing reinforcement fibers at 90 degrees to the fracture line when repairing the
dentures.
3. Mesh should be placed superficially and not buried in the denture.
Reinforcement of PMMA with metal oxides improved the physical and mechanical properties of the material, as well as the patients’ sensation of food temperature,
which resulted in healthier oral mucosa. The properties of resin reinforced by nanofillers depend on the size, shape, type, and concentration of the added particles
(Safi, 2014).
5.4.3 Particulate-reinforced resins
5.4.3.1 Alumina
A recent study reported that the addition of alumina (Al2O3) NPs to microwavetreated and untreated PMMA powder has a good level of biocompatibility
(Abdulkareem and Hatim, 2015). The main disadvantage of aluminum-reinforced
PMMA is discoloration of the resin, which limits its use to areas where it is not visible (Jasim and Ismai, 2014). The addition of Al2O3 to PMMA significantly
increased thermal conductivity, but the flexural strength of PMMA did not change
90
Advanced Dental Biomaterials
significantly (Kul et al., 2016). Also, the addition of silane-treated aluminum particles to PMMA powder significantly increased the compressive, tensile, and flexural
strength and the wear resistance of denture base resin (Chaijareenont et al., 2012).
Surface roughness and water sorption of aluminum-reinforced PMMA were not significantly changed (Vojdani et al., 2012).
5.4.3.2 Zirconia
Incorporating zirconia (ZrO2) NPs in PMMA increased its thermal conductivity,
impact strength, and flexural strength (Gad et al., 2016). Also, compressive
strength, fatigue strength, as well as fracture toughness and hardness of the polymer
were improved (Salih et al., 2015; Nejatian et al., 2006). The adhesion between the
resin matrix and filler particles is very important to enhance the composite’s properties. Therefore a silane coupling agent could be useful to improve the bond strength
between zirconia NPs and PMMA. The flexural strength and impact strength of
acrylic resin increased, but its tensile strength was not improved. The effect of
ZrO2 on the water sorption and solubility of PMMA was different (Bian et al.,
2007). In addition, zirconia nanotubes showed a better reinforcing effect than zirconia NPs but, in contrast to zirconia NPs, surface treatment would decrease the reinforcing effect of zirconia nanotubes (Yu et al., 2014).
5.4.3.3 Titanium
Adding titanium (TiO2) particles could improve fracture toughness and hardness of
PMMA as well as thermal conductivity at the cost of flexural strength (Nejatian
et al., 2006). In addition, there is a significant increase in impact strength (Ahmed
et al., 2016). The improvement of the physical and mechanical properties of
PMMA is limited by poor wettability between fillers and the resin matrix. For this
reason, a titanium coupling agent was used for improving the properties of
titanium-reinforced PMMA (Elshereksi et al., 2014). The incorporation of silanized
TiO2 NPs in PMMA improved the impact strength, transverse strength, and surface
hardness of the resin but decreased its water sorption and solubility. Moreover, surface roughness increased with the addition of 3 wt.% of silanized TiO2 NPs to the
acrylic resin (Alwan and Alameer, 2015). Adding apatite-coated titanium dioxide
and fluoridated apatite-coated titanium dioxide inhibited Candida adhesion due to
the antifungal effect (Sawada et al., 2014; Shibata et al., 2007). The addition of barium titanate (BaTiO3) as a radiopacifier to PMMA showed a slight decrease in fracture toughness properties (Elshereks et al., 2009).
Silver
The addition of silver (Ag) in PMMA could reduce microbial adhesion and colonization because silver has an antimicrobial effect. Also, the addition of silver NPs
(Ag NPs) to denture base acrylic resin showed antifungal properties (Casemiro
et al., 2007; Monteiro et al., 2012). Incorporating silver powder to PMMA significantly increased thermal conductivity, but the flexural strength values of PMMA
were not significantly changed (Kul et al., 2016). The physical and mechanical
Acrylic denture base materials
91
properties of PMMA were improved by the addition of silver NPs, including the
increase of thermal conductivity and compressive strength. Therefore it is recommended to be used in the palatal area of maxillary acrylic resin dentures (HamediRad et al., 2014; Ghafari et al., 2014).
Hydroxyapatite fillers
Hydroxyapatite fillers added to PMMA enhanced the mechanical properties of
PMMA. They increased the flexural strength as well as the flexural modulus of
PMMA (Tham et al., 2010).
Silicon dioxide
The mechanical and thermal properties of PMMA were improved by the incorporation of silicon dioxide (SiO2) NPs (Safi, 2014). The addition of SiO2 NPs has
increased PMMA impact and transverse strength. Surface hardness also increased
with a higher SiO2 NP concentration (Alnamel and Mudhaffer, 2014).
Silica-based filler
Incorporation of mica in PMMA increased the hardness of acrylic resin and
improved the mechanical and thermal properties, as well as the dimensional stability of PMMA, but its flexural strength was reduced because of the weak bond
between mica and acrylic resin (Mansour et al., 2013). The incorporation of fluoride glass fillers to PMMA decreased its microbial adhesion at the cost of surface
roughness (Al-Bakri et al., 2014; Tsutsumi et al., 2016), whereas nanoclay particles
improved the thermal conductivity, but negatively affected the flexural strength
(Ghaffari et al., 2016).
5.4.4 Hybrid reinforcement
Reinforcement of PMMA by more than one type of fiber was first suggested by
Vallittu in 1997. A combination of fibers improves mechanical and physical properties of the material, such as surface roughness (Aljafery and Basima, 2015), tensile
strength, flexural modulus (Alhareb and Ahmad, 2011), hardness, thermal conductivity, and radiopacity (Salman and Khalaf, 2015), as well as reducing polymerization shrinkage (Safarabadia et al., 2014; Alhareb et al., 2015).
5.4.5 Hypoallergenic resins
Hypoallergenic denture base materials such as diurethane dimethacrylate, polyurethane, polyethylene terephthalate, and polybutylene terephthalate exhibit significantly lower residual monomer content than PMMA (Uzun and Hersek, 1999); thus
they could act as an alternative denture base material in allergic patients.
Enterephthalate-based dentures show low water solubility than PMMA (Pfeiffer and
Rosenbauer, 2004). Light-cured indirect composite containing urethane dimethacrylate (UDMA) is another alternative to PMMA for patients hypersensitive to PMMA
(Pfeiffer and Rosenbauer, 2004).
92
Advanced Dental Biomaterials
5.4.6 Thermoplastic resins
In this procedure, a fully polymerized basic material is softened by heat (without
chemical changes) and injected afterward. These materials have opened a new
chapter in making dentures (Philip, 1998) Thermoplastic resins have many advantages over the conventional powderliquid systems. They are very resistant to heat,
solvents, and chain degradation as well as being comfortable for the patients. They
are also esthetically pleasing and have high fatigue, creep, and wear resistance.
Nonporous structure of the material makes them more resistant to bacterial growth.
Relining and repairing through repressing is possible. This group includes thermoplastic nylon (polyamide), thermoplastic acetal, thermoplastic acrylic, and thermoplastic polycarbonate (Rawls et al., 1992).
5.4.6.1 Thermoplastic nylon
The basic material of thermoplastic nylon is polyamide (derived from diamine and
dibasic acid monomers). Thermoplastic nylon, which was introduced to dentistry in
the 1950s, was later used by Rapid Injection System (currently known as The
Flexite Company, United States) in 1962 as the first flexite thermoplastic (a fluoropolymer—a Teflon-type plastic). Thermoplastic nylon is injected at temperatures of
274 C293 C. This material generally replaces the metal and the pink acrylic denture material used to build the framework for removable partial dentures. Valplast
and Flexiplast are two polyamide materials used to make partial dentures. In 1992
The Flexite Company developed the first preformed nylon clasps known as ClaspEze, which are available in pink and clear shades. Nylon is not brittle, has a light
weight, does not warp, and provides better esthetics. Nylon is nonporous and more
durable against discoloration, and it still retains a slight amount of moisture to keep
it comfortable against mucosa (Phoenix et al., 2004). However, nylon is not strong
enough to be used as partial denture rests or in occlusal force bearing areas and is
also not easy to adjust and polish (Lowe, 2004).
5.4.6.2 Thermoplastic acetal
Acetal was first introduced as an unbreakable thermoplastic denture resin in 1971.
Rapid Injection System developed the first tooth-colored clasps with thermoplastic
fluoropolymer (Keenan et al., 2003). In 1986 Dental “D” reintroduced a homopolymer called acetal as tooth-colored clasps with good short-term mechanical properties, better long-term stability, that were hypoallergic (monomer-free), and had
desirable esthetics. The artificial teeth and clasps can be injected together in resin
or into the existing denture and polished by a dedicated polishing kit. However,
overtrimmed dentures cannot be repaired easily as it requires injection, and poor
adhesion between the denture base and the artificial teeth may result in leakage of
saliva around the teeth, resulting in debonding (Keenan et al., 2003). Also, a major
connector is required to be rigid. Therefore an injected resin major connector for
temporary partials is no longer recommended due to high flexibility.
Acrylic denture base materials
93
5.4.6.3 Thermoplastic acrylic
Heat-cured PMMA has high porosity, high water absorption, volumetric changes,
and residual monomer. Thermoplastic acrylic demonstrates poor impact resistance
but has adequate tensile and flexural strength and also provides excellent esthetics
due to good translucency and vitality. In addition, it is easy to adjust, reline, repair,
and polish at the chair-side. However, acrylic wear resistance is less than acetal
especially when subjected to occlusal forces and as a consequence it cannot maintain its vertical dimension for as long. Flexite M.P., a thermoplastic acrylic, is a
special blend of polymers with the highest impact strength among this group and
resistance to fracture against impact forces, for example, when the dentures are
dropped on the floor (Negrutiu et al., 2005).
5.4.6.4 Thermoplastic polycarbonate
Polycarbonate is a polymer chain of bisphenol-A carbonate. Similar to acetal resin,
polycarbonate resin is also very strong, fracture resistant, and flexible. However,
due to low wear resistance, it should not be used on occlusal surfaces.
Polycarbonate is not suitable for full or partial dentures, but it is ideal for provisional crown and bridges. Having natural translucency and good finishing, polycarbonate provides excellent esthetics and function in the short or mid-term. This
material exhibits little water absorption and no unpleasant smell of saliva absorption. Good adherence and coherence of this material with saliva provides a good
affinity with mucous membrane. In addition, it has high impact, crack, and abrasive
resistance (Negrutiu et al., 2005).
5.4.7 Novel technologies in manufacturing removable
denture base
Computer-aided design/computer-aided manufacturing (CAD/CAM) techniques are
employed for fabricating fixed and removable partial dental prostheses. Generally,
two technological approaches were used for fabricating dentures: CAD/CAM and
rapid prototyping (RP) (Lima et al., 2014). In both approaches, a clinical impression
procedure for obtaining the morphology of denture bases and the muscular and phonetic positions of the denture teeth is necessary. After making gypsum models,
acrylic bases are made, and occlusal rims for each model are fabricated with previously determined standard vertical and centric relationships. Subsequently, the
recorded information is scanned, and the complete denture bases are virtually
designed. The maxillary and mandibular teeth alignment is verified, and the teeth in
each arch are fabricated in one piece, or set, by CAM or RP. Of course, CAD/CAM
systems have not completely replaced traditional impression taking, because
dynamic movements of the soft tissues influence the quality of the direct digital
impression. At present, there are five CAD/CAM systems available for production
of dentures: AvaDent (Global Dental Science), Baltic Denture System (Merz Dental
GmbH), Ceramill Full Denture System (Amann Girrbach AG), DENTCA/Whole
94
Advanced Dental Biomaterials
You (DENTCA, Inc.; Whole You, Inc.), and Wieland Digital Denture (Ivoclar
Vivadent, Inc.).
Advantages of digital fabrication of dentures:
G
G
G
G
G
G
G
decreased number of appointments,
reduced shrinkage and improved strength,
decreased manufacturing time,
decreased risk of microorganism colonization on the denture surfaces,
advances in standardization for clinical research on removable prostheses,
easy reproduction of the denture and manufacture of a trial denture using stored digital
data, and
superior quality control by clinicians and technicians (Min et al., 2014; Kattadiyil et al.,
2015).
Limitations and disadvantages of digital fabrication of dentures:
G
G
G
G
manufacturing challenges used by impression-taking and OVD-recording procedures,
MMR transfer, and maintenance of lip support, which is all similar to the procedures used
in the conventional process,
inability to define the mandibular occlusal plane,
expensive materials and increased laboratory cost compared with those for conventional
methods, and
lack of trial denture, which precludes the evaluation of dentures by patients and dentists
before final denture fabrication (Sirirungrojying et al., 1998).
5.5
Denture lining materials
The anatomy of the denture bearing area remains under constant change due to variables such as the load, physiological conditions, and tissue tolerance. Therefore
edentulous patients should be made aware of the residual ridge resorption which is
inevitable, and the prosthesis needs to be modified in a timely manner. Ill-fitting
dentures due to the bone and soft tissue changes result in significantly abused tissues. Traumatized and abused tissues are conditioned in a time-dependent manner
providing a cushioning effect with the provision of denture lining materials. This
not only involves the refitting of the surfaces within complete dentures but also aids
in retention of the extra and intraoral prosthesis.
5.5.1 Clinical indication
The general indications for relining are as follows:
G
G
G
G
loss of fit surface, retention, and stability due to alveolar bone resorption,
loss of vertical dimension of occlusion (VDO),
degradation of denture base,
denture extension not covering the mucobuccal fold areas, retromolar pad in the mandibular region, and hamular notch area in the maxillary region,
Acrylic denture base materials
G
G
95
for elderly patients where new dentures are suspected not to work due to old denture
habituation, and
patients with the psychological unwillingness to new dentures.
The earliest lining materials were made from natural rubber until the 1945s
when the synthetic resin was first used as a resilient liner. By 1958 silicone rubbers
were introduced as liners.
Relining materials are selected and used according to the clinical need. These
materials can be classified into three types:
G
G
G
Hard reline materials: permanent type (Requirements ADA 13 and 17)
Soft liners: semipermanent type (Requirements ADA 17)
Tissue conditioners: temporary soft relining materials (Requirements ADA 17).
5.5.2 Hard relining
A complete denture may be expected a mean life of about 45 years, depending on
the rate of resorption of the alveolar bone. When soft tissue changes arise due to
bone resorption, the fit surface of the dentures can be improved by employing a
hard reline material. This becomes more challenging with mandibular dentures than
maxillary dentures.
There are principally two techniques of lining the dentures: direct and indirect.
The direct technique involves the relining of the denture with a cold-cured acrylic
resin at the chair-side, whereas the indirect technique involves the denture being
sent to the laboratory for relining with a heat-cured acrylic.
Heat-cured acrylics (polymer powder and monomer liquid) used for relining are
identical to the ones used for denture construction (Table 5.2). However, the fabrication differs from the normal construction of dentures. The impression is made
using the defective or old denture as a special tray where changed oral tissues are
recorded and a stone cast is prepared. The stone cast along with the impression and
denture is invested in the flask; after setting, the two halves are separated and the
impression material removed. Separating media is applied and polymer powder
(PMMA) and liquid (methyl methacrylate) are mixed (Table 5.2). A resin dough is
achieved which is packed into the old denture space (previously occupied by
impression material) and curing is performed. After curing, the modified denture is
obtained for which slight finishing is done.
Cold-cured resins are available in two types (Table 5.2). The second type is preferred over the first due to MMA being an irritant to the soft tissues, and it also can
sensitize the patients. The only disadvantage of using PEMA and BMA is that they
reduce the Tg, and this causes the possibility of dimensional instability. The chairside procedure is straightforward and just needs to follow the recommended manufacturer’s guidelines. Care must be taken, as poorly controlled chair-side relining
may result in increased VD. Also, these materials have shown to have an
unacceptable taste, high exothermic reactions, and diminished color stability over
time.
96
Advanced Dental Biomaterials
Table 5.2 The heat-cured and cold-cured resins used for
relining dentures.
Heat-cured resin
Powder
Initiator
Beads or granules of PMMA
Benzoyl peroxide
Pigments/dyes
Opacifiers
Plasticizer
Synthetic fibers
Liquid
Inhibitor
Cross-link agent
Titanium, zinc oxides
Dibutyl phthalate
Nylon/Acrylic
MMA
Hydroquinone
EGDMA
Cold-cured resin
Type 1
Type 2
Powder
PMMA
Benzoyl peroxide
Pigments
PEMA
Benzoyl peroxide
Pigments
Liquid
MMA
Di-n-butyl phthalate
Amine
BMA
Amine
BMA, Butyl methacrylate; EGDMA, ethylene glycol dimethacrylate; MMA, methyl
methacrylate; PEMA, polyethyl methacrylate; PMMA, polymethyl methacrylate.
5.5.3 Soft relining
Long-term soft liners are recommended as a therapeutic measure for patients who
are unable to cope up with their existing dentures due to either
uncomfortable denture bearing area or prolonged contact between the denture base
and the soft tissues resulting in chronic pain, discomfort, and soreness. The soft
liner on the tissue side of the dentures provides a cushioning effect to absorb the
large dynamic masticatory loads. To achieve such resilient properties, highly plasticized methacrylate or elastomeric materials are used, which are either heat or chemically cured. Heat-cured soft liners are more durable in nature than their
counterparts.
The clinical situation where long-term soft liners may be indicated:
G
G
G
thin, sharp alveolar ridges,
excessively resorbed ridges,
severe bony undercuts present,
Acrylic denture base materials
G
G
97
congenital or acquired defects of the palate, and
sensitivity due to submucosal exposure of the alveolar bone.
An ideal long-term soft liner should
G
G
G
G
G
G
G
G
G
G
G
G
G
be biocompatible,
not degrade easily,
be dimensionally stable,
have wettability with saliva,
exhibit low water solubility or water sorption,
exhibit viscoelasticity/compliance/softness,
have a good tear and abrasion resistance,
exhibit good bond with denture base,
be stable and not affected by cleansers or aqueous environment,
be easy to handle and manipulate,
have good esthetics,
be color stable, and
not allow colonization of microorganisms and fungi to grow.
5.5.3.1 Methacrylate resin liners (heat-activated)
These are supplied as a preformed sheet or in a powder/liquid form. Flexibility of
these is imparted by incorporating plasticizers that decrease the glass transition temperature of the resin and act as a lubricant between the polymer chains. The large
plasticizer molecules push the polymer chains apart, allowing them to slip on one
another thus creating more elastic, flexible, and resilient liners. These polymer
resins can bond well with acrylic but with time become stiffer as resilience is lost.
The water is absorbed by the liner and leaching of plasticizer occurs, which
diminishes the cushioning effect. Clinically, resilient liners are immersed in saliva
and dentures are usually stored in water when not in use.
These liners are processed in a laboratory, and they show good bond strength to
methacrylate base with high tear and abrasion resistance. They can be better
polished than silicone. The only drawback is a hard rough surface due to biodegradation of plasticizers promoting calculus formation, food accumulation, and fouling
due to microorganisms.
5.5.3.2 Methacrylate resin liners (chemically activated)
Soft liners are also available in a chemically activated form having similar composition as heat-activated resins. They are used chair-side and polymerization is usually activated by peroxide tertiary amines and completed in several minutes. They
are used as temporary liners as they have a tendency to debond from the denture
base and foul within a few weeks. The free monomer also contributes to inferior
mechanical properties and poor biocompatibility.
5.5.3.3 Silicone-based liners (heat-activated)
They are available as a paste, poly(dimethyl siloxane), and a viscous liquid to
which silica is added as a filler, and benzoyl peroxide as an initiator. A crosslinking reaction is catalyzed by heat and peroxide initiator to set the liner. It is
98
Advanced Dental Biomaterials
recommended to process liner along with fresh methacrylate dough of the new denture. This has an advantage over the addition of an already polymerized base as a
better bond is achieved with the denture base. The laboratory procedures for silicone liners are the same for both heat- and chemical-cured ones. The
acceptable thickness of liner is chosen and adequate relief is provided inside the fitting surface of the denture base. Packing, compress molding, and processing are
carried out according to manufacturer’s guidelines. The final denture is deflasked,
finished, and polished for use.
5.5.3.4 Silicone-based liners (chemically activated)—room
temperature vulcanized silicones
They are supplied as a two-component system: a paste and a liquid. These liners
undergo a condensation cross-linking process which is catalyzed by an organic
compound. This reaction is similar in nature to condensation of silicone impression
materials. Room temperature vulcanized (RTV) silicones undergo a lesser degree of
cross-linking compared to heat-activated silicones, which in turn makes them less
favorable as long-term liners and decreases their longevity.
Heat-activated silicone rubbers pose better properties than plasticized methacrylates and this enhances their clinical superiority to their counterpart. These soft
liners have been advocated to have better qualities providing good cushioning effect
with superior flexibility and shock absorption than other soft liners.
The major drawback of silicone liner is their tendency to debond from the methacrylate resin base. It has been noted that RTV liners tend to swell and peel off the
denture base due to high water sorption and volume changes. They lose the viscoelasticity and become brittle, transferring load on to the bond area. Thus concurrent
debonding leads to biofilm adhesion, staining, and decrease in denture strength.
Bonding agents and cement have been tried to overcome this problem, but this has
not proven to be effective. Both methacrylates and silicones soft liners should not
be perceived as permanent liners as both exhibit shortcomings and despite vast clinical benefits they, by far, are not fulfilling the requirements of an ideal material.
5.5.4 Tissue conditioners
Short-term resilient liners are also known as tissue conditioners due to their massaging ability to the soft tissues, which can become irritated and inflamed over a period
of time. It is a soft material used temporarily to adapt to the fitting surface of the
denture. This allows time for the mucosal tissues to regain normal shape and any
inflammation to subside. Once tissues regain a better shape and inflammation has
been resolved, an impression for the new dentures can be taken. Short-term soft
liners vary considerably in their composition depending upon their molecular
weight, powder granule size, alcohol content, and plasticizers incorporated. They
are supplied as a powder of Polyethylene metacrylate (PEMA), and liquid is not
methyl methacrylate but a solvent, such as ethyl alcohol and an aromatic ester such
as large molecular-sized plasticizers (e.g., butyl phthalate, butyl glycolate, or
Acrylic denture base materials
99
dibutyl phthalates). They are mixed at chair-side and gelation of tissue conditioner
takes place. This is a physical process, devoid of any chemical reaction. Upon mixing the large molecule plasticizers decreases the entanglement process; thereby the
softness increases and the Tg decreases.
Indications for tissue conditioners/short-term soft liners include the following:
G
G
G
G
G
G
G
G
to treat irritated and inflamed denture-supporting tissues,
used for diagnostic purposes to stabilize the vertical dimension of occlusion (VDO),
used as an adjunct to correct the occlusion of the old prosthesis in relation to VDO,
temporary lining for surgical splints,
temporary lining for immediate dentures,
relining for obturators,
during implant healing as tissue conditioners, and
as an adjunct material for functional impressions.
Tissue-conditioner requirements differ when used as functional impression materials. For a traumatized tissue, a tissue conditioner should be able to exhibit flow
and elastic properties, thus conditioning the tissues with its viscoelastic behavior,
which has viscous fluid and elastic solid properties. On the other hand, a functional
impression material should exhibit good flow but with no or minimal elastic recovery. This property of the material is of prime importance as under functional stresses it should flow readily to encompass the underlying soft tissues, which are
altered under stress conditions.
The impression materials must exhibit dimensional stability in regard to solubility, water sorption, and weight change. They should be compliant for many weeks
and have a good bond with resin bases. Elastic recovery should be minimal for the
success of these as impression materials. To obtain optimum results, functional
impressions are removed after 57 days and casts are poured immediately.
5.6
Acrylic artificial teeth
Acrylic teeth are supplied as anatomical and nonanatomical zero-degree acrylic
resin teeth-sets. There are supplied in different sizes and there are various color
shades to select from. Acrylic (methacrylate-based) resin (PMMA) denture teeth are
either manufactured by compression dough molding technique or injection molding.
The heat-cured acrylic is available in powder and liquid forms for the preparation
and to improve the properties and decrease crazing large volumes of cross-linking
agents (glycol or other dimethacrylates) are used. Some of the resin-based teeth
available in the market are the multiplex polymer matrix resin teeth, resin teeth
with Interpenetrating polymer network (IPN) of polymers, and double cross-linked
resins.
Properties of the acrylic teeth:
G
G
They have adequate biocompatibility.
They have good esthetics (different color shades).
100
G
G
G
G
G
G
G
G
G
G
G
G
G
G
Advanced Dental Biomaterials
Their color is stable for good period of time.
Crazing can be avoided if cross-linked.
Low surface hardness (20 KHN).
Abrasive resistance is moderate, tend to wear out by opposing teeth.
They have excellent resistance to fracture.
They are highly resilient and flexible.
They do not produce “click” sound like porcelain teeth.
Their bonding to acrylic denture is by chemical means.
Their thermal expansion is similar to denture bases (80120 ppm/ C).
They are easy to grind and polish.
The water sorption causes dimensional changes.
The fabrication is a simple and easy procedure.
They do not dissolve in solvents.
Newer generations of resin teeth are much more stable (wear) and do not get stained.
5.7
Conclusion
PMMA has been used as the most popular denture base material for many years
due to its unique properties. Efforts have been made to modify or employ novel
materials to meet specific needs of the patients. Also, modern technologies have
been introduced to the dentistry to reduce the cost and improve the quality and
facilitate manufacturing of the dentures. The initial outcome of these advanced
technologies is promising; however, further development in technology and material is still required to allow them to be used routinely and replace the conventional
techniques and materials.
References
Abdulkareem, M., Hatim, N., 2015. Evaluation the biological effect of adding aluminum
oxide, silver nanoparticles into microwave treated PMMA powder. Int. J. Enhanced Res.
Sci. Technol. Eng. 4, 172178.
Ahmed, M., El-shennawy, M., Althomali, Y., Omar, A., 2016. Effect of titanium dioxide
nano particles incorporation on mechanical and physical properties on two different
types of acrylic resin denture base. World J. Nano Sci. Eng. 6, 1111119.
Al-bakri, I., Harty, D., Al-omari, W., Swain, M., Chrzanowski, W., Ellakwa, A., 2014.
Surface characteristics and microbial adherence ability of modified polymethylmethacrylate by fluoridated glass fillers. Aust. Dent. J. 59, 482489.
Alhareb, A., Ahmad, Z., 2011. Effect of Al2O3/ZrO2 reinforcement on the mechanical properties of PMMA denture base. J. Reinf. Plast. Compos. 30, 8693.
Alhareb, A., Akil, H., Ahmad, Z., 2015. Mechanical properties of PMMA denture base reinforced by nitrile rubber particles with Al2O3/YSZ fillers. Procedia Manuf. 2, 301306.
Aljafery, M., Basima, M., 2015. Effect of addition ZrO2-Al2O3 nanoparticles mixture on
some properties and denture base adaptation of heat cured acrylic resin denture base
material. J. Baghdad Coll. Dent. 27, 1521.
Acrylic denture base materials
101
Alla, R., 2013. Dental Materials Science. Jaypee Brothers Medical Publishers (Pvt) Ltd, New
Delhi.
Alnamel, H., Mudhaffer, M., 2014. The effect of silicon dioxide nano-fillers reinforcement
on some properties of heat-cure polymethylmethacrylate denture base material.
J. Baghdad Coll. Dent. 26, 3236.
Alwan, S., Alameer, S., 2015. The effect of the addition of silanized nano titania fillers on
some physical and mechanical properties of heat cured acrylic denture base materials.
J. Baghdad Coll. Dent. 27, 8691.
Anusavice, K., Shen, C., Rawls, H.R., 2012. Phillips’ Science of Dental Materials,
twelfth ed. Saunders.
Bahrani, F., Safari, A., Vojdani, M., Karampoor, G., 2012. Comparison of hardness and surface roughness of two denture bases polymerized by different methods. World J. Dent.
3, 171175.
Bartoloni, J.A., Murchison, D.F., Wofford, D.T., Sarkar, N.K., 2000. Degree of conversion in
denture base materials for varied polymerization techniques. J. Oral. Rehabil. 27,
488493.
Bian, Y., Zhang, X., Zhu, B., Yu, W., Ruan, D., Min, M., 2007. Influence of different amount
of silane coupling agent on the flexural strength of PMMA/nanometer ZrO2 composites.
Shanghai Kou Qiang Yi Xue 163, 319323.
Bloodworth, K.E., Render, P.J., 1992. Dental acrylic resin radiopacity: literature review and
survey of practitioners’ attitudes. J. Prosthet. Dent. 67, 121123.
Casemiro, L., Gomes Martins, C., Pires-de-Souza Fde, C., Panzeri, H., 2007. Antimicrobial
and mechanical properties of acrylic resins with incorporated silver-zinc zeolite—Part I.
Gerodontology 25, 187194.
Chaijareenont, P., Takahashi, H., Nishiyama, N., Arksornnukit, M., 2012. Effect of different
amounts of 3-methacryloxypropyltrimethoxy silane on the flexural properties and wear
resistance of alumina reinforced PMMA. Dent. Mater. J. 3, 623628.
Danilewicz-stysiak, Z., 1971. Allergy as a cause of denture sore mouth. J. Prosthet. Dent. 25,
1618.
Elshereks, I.N., Mohamed, S., Arifin, A., Mohd Ishak, Z., 2009. Effect of filler incorporation
on the fracture toughness properties of denture base polymethylmethacrylate. J. Phys.
Sci. 20, 112.
Elshereksi, N., Ghazali, M., Muchtar, A., Azhari, C., 2014. Perspectives for titanium-derived
fillers usage on denture base composite construction: a review article. Adv. Mater. Sci.
Eng. 1, 114.
Gad, M., Arrejaie, A., Abdel-Halim, M., Rahoma, A., 2016. The reinforcement effect of
nano-zirconia on the transverse strength of repaired acrylic denture base. Int. J. Dent.
2016, 7094056.
Ghafari, T., Hamedi-Rad, F., Ezzati, B., 2014. Does addition of silver nanoparticles to denture base resin increase its thermal conductivity? J. Dent. Sch. 32, 139144.
Ghaffari, T., Barzegar, A., Hamedi Rad, F., Moslehifard, E., 2016. Effect of nanoclay on
thermal conductivity and flexural strength of polymethyl methacrylate acrylic resin.
J. Dent. (Shiraz) 17, 121127.
Hamedi-Rad, F., Ghaffari, T., Rezaii, F., Ramazani, A., 2014. Effect of nanosilver on thermal
and mechanical properties of acrylic base complete dentures. J. Dent. (Tehran) 11,
495505.
Jagger, D.C., Harrison, A., 1999. The effect of chopped poly(methyl methacrylate) fibers on
some properties of acrylic resin denture base material. Int. J. Prosthodont. 12, 542546.
102
Advanced Dental Biomaterials
Jagger, D.C., Jagger, R.G., Allen, S.M., Harrison, A., 2002. An investigation into the transverse and impact strength of “high strength” denture base acrylic resins. J. Oral.
Rehabil. 29, 263267.
Jasim, B., Ismai, L.I., 2014. The effect of silanized alumina nano-fillers addition on some
physical and mechanical properties of heat cured polymethylmethacrylate denture base
material. J. Baghdad Coll. Dent. 26, 1823.
Jerolimov, V., Brooks, S.C., Huggett, R., Bates, J.F., 1989. Rapid curing of acrylic denturebase materials. Dent. Mater. 5, 1822.
John, J., Gangadhar, S.A., Shah, I., 2001. Flexural strength of heat-polymerized polymethyl
methacrylate denture resin reinforced with glass, aramid, or nylon fibers. J. Prosthet.
Dent. 86, 424427.
Jorge, J.H., Giampaolo, E.T., Machado, A.L., Vergani, C.E., 2003. Cytotoxicity of denture
base acrylic resins: a literature review. J. Prosthet. Dent. 90, 190193.
Kanie, T., Fujii, K., Arikawa, H., Inoue, K., 2000. Flexural properties and impact strength of
denture base polymer reinforced with woven glass fibers. Dent. Mater. 16, 150158.
Kattadiyil, M.T., Jekki, R., Goodacre, C.J., Baba, N.Z., 2015. Comparison of treatment outcomes in digital and conventional complete removable dental prosthesis fabrications in
a predoctoral setting. J. Prosthet. Dent. 114, 818825.
Keenan, P.L., Radford, D.R., Clark, R.K., 2003. Dimensional change in complete dentures
fabricated by injection molding and microwave processing. J. Prosthet. Dent. 89,
3744.
Khindria, S., Mittal, S., Sukhija, U., 2009. Evolution of denture base materials. J. Indian
Prosthodont. Soc. 9, 6469.
Kim, S.H., Watts, D.C., 2004. The effect of reinforcement with woven e-glass fibers on the
impact strength of complete dentures fabricated with high-impact acrylic resin.
J. Prosthet. Dent. 91, 274280.
Kul, E., Aladağ, L., Yeşildal, R., 2016. Evaluation of thermal conductivity and flexural
strength properties of poly(methyl methacrylate denture) base material reinforced with
different fillers. J. Prosthet. Dent. 116, 803810.
Ladizesky, N.H., Ho, C.F., Chow, T.W., 1992. Reinforcement of complete denture bases
with continuous high performance polyethylene fibers. J. Prosthet. Dent. 68, 934939.
Lima, J.M., Anami, L.C., Araujo, R.M., Pavanelli, C.A., 2014. Removable partial dentures:
use of rapid prototyping. J. Prosthodont. 23, 588591.
Lowe, L.G., 2004. Flexible denture flanges for patients exhibiting undercut tuberosities and
reduced width of the buccal vestibule: a clinical report. J. Prosthet. Dent. 92, 128131.
Mansour, M., Wagner, W., Chu, T., 2013. Effect of mica reinforcement on the flexural
strength and microhardness of polymethylmethacrylate denture resin. J. Prosthodont. 22,
179183.
Min, K., Silberstein, M., Aluru, N.R., 2014. Crosslinking PMMA: molecular dynamics investigation of the shear response. J. Polym. Sci. B Polym. Phys. 52, 444449.
Monteiro, D., Gorup, L., Takamiya, A., de Camargo, E., Filho, A., Barbosa, D., 2012. Silver
distribution and release from an antimicrobial denture base resin containing silver colloidal nanoparticles. J. Prosthodont. 21, 715.
Munksgaard, E.C., 2004. Leaching of plasticizers from temporary denture soft lining materials. Eur. J. Oral Sci. 112, 101104.
Nandal, S., Ghalaut, P., Shekhawat, H., Gulati, M.S., 2013. New era in denture base resins.
Dent. J. Adv. Stud. 1, 136143.
Negrutiu, M., Sinescu, C., Romanu, M., Pop, D., Lakatos, S., 2005. Thermoplastic resins for
flexible framework removable partial dentures. TMJ 55, 295299.
Acrylic denture base materials
103
Nejatian, T., Johnson, A., Van Noort, R., 2006. Reinforcement of denture base resin. Adv.
Sci. Technol. 49, 109118.
Noort, R.V., Barbour, M.E., 2013. Introduction to Dental Materials. Mosby Elsevier,
Edinburgh; New York.
Ogle, R.E., Sorensen, S.E., Lewis, E.A., 1986. A new visible light-cured resin system applied
to removable prosthodontics. J. Prosthet. Dent. 56, 497506.
Pfeiffer, P., Rosenbauer, E., 2004. Residual methyl methacrylate monomer, water sorption,
and water solubility of hypoallergenic denture base materials. J. Prosthet. Dent. 92,
7278.
Philip, B., 1998. The new acrylic resin with improved thermal diffusivity. J. Prosthet. Dent.
79, 278284.
Phoenix, R.D., Mansueto, M.A., Ackerman, N.A., Jones, R.E., 2004. Evaluation of mechanical and thermal properties of commonly used denture base resins. J. Prosthodont. 13,
1727.
Rawls, H., Marshall, M., Cardenas, H., Bhagat, H., 1992. Cytotoxicity evaluation of a new
radiopaque resin additive-triphenyl bismuth. Dent. Mater. 8, 5459.
Rickman, L.J., Padipatvuthikul, P., Satterthwaite, J.D., 2012. Contemporary denture base
resins: Part 1. Dent. Update 39, 25.
Rimple, Gupta, A., Kamra, M., 2011. An evaluation of the effect of water sorption on dimensional stability of the acrylic resin denture bases. Int. J. Contemp. Dent. 2, 4348.
Rodford, R.A., 1990. Further development and evaluation of high impact strength denture
base materials. J. Dent. 18, 151157.
Safarabadia, M., Khansarib, N., Rezaeic, A., 2014. An experimental investigation of HA/
Al2O3 nanoparticles on mechanical properties of restoration materials. Eng. Solid Mech.
2, 173182.
Safi, I., 2014. Evaluation the effect of nano-fillers (TiO2, Al2O3, SiO2) addition on glass transition temperature. E-modulus and coefficient of thermal expansion of acrylic denture
base material. J. Baghdad Coll. Dent. 26, 3741.
Sakaguchi, R.L., Powers, J.M., 2007. Craig’s Restorative Dental Materials. Elsevier, Mosby,
a Division of Reed Elsevier, India Pvt Ltd, New Delhi.
Salih, S., Oleiwi, J., Hamad, Q., 2015. Investigation of fatigue and compression strength for
the PMMA reinforced by different system for denture applications. Int. J. Biomed.
Mater. Res. 3, 513.
Salman, T., Khalaf, H., 2015. The influence of adding of modified ZrO2-TiO2 nanoparticles
on certain physical and mechanical properties of heat polymerized acrylic resin.
J. Baghdad Coll. Dent. 27, 3339.
Sawada, T., Sawada, T., Kumasaka, T., Hamada, N., Shibata, T., Nonami, T., et al., 2014.
Self-cleaning effects of acrylic resin containing fluoridated apatite-coated titanium dioxide. Gerodontology 31, 6875.
Shibata, T., Hamada, N., Kimoto, K., Umemoto, T., Toyoda, M., 2007. Antifungal effect of
acrylic resin containing apatite-coated TiO2 photocatalyst. Dent. Mater. J. 26, 437444.
Sirirungrojying, S., Srisintorn, S., Akkayanont, P., 1998. Psychometric profiles of temporomandibular disorder patients in southern Thailand. J. Oral. Rehabil. 25, 541544.
Soygun, K., Bolayir, G., Boztug, A., 2013. Mechanical and thermal properties of polyamide
versus reinforced PMMA denture base materials. J. Adv. Prosthodont. 5, 153160.
Takamata, T., Setcos, J.C., 1989. Resin denture bases: review of accuracy and methods of
polymerization. Int. J. Prosthodont. 2, 555562.
Tandon,, R., Gupta,, S.,, Samarth Kumar, A.,, 2010. Denture base materials: from past to
future. Indian J. Dent. Sci. 2, 3339.
104
Advanced Dental Biomaterials
Tham, W., Chow, W., Mohd Ishak, Z., 2010. Simulated body fluid and water absorption
effects on poly(methyl methacrylate)/hydroxyapatite denture base composites. Expr.
Polym. Lett. 4, 517528.
Tsutsumi, C., Takakuda, K., Wakabayashi, N., 2016. Reduction of candida biofilm adhesion
by incorporation of prereacted glass ionomer filler in denture base resin. J. Dent. 44,
3743.
Uzun, G., Hersek, N., 1999. Tinçer effect of five woven fiber reinforcements on the impact
& transverse strength of a denture base resin. J. Prosthet. Dent. 81, 616620.
Vallittu, P.K., 1996. Comparison of the in vitro fatigue resistance of an acrylic resin removable partial denture reinforced with continuous glass fibers or metal wires.
J. Prosthodont. 5, 115121.
Vallittu, P.K., 1999. Unpolymerized surface layer of autopolymerizing polymethyl methacrylate resin. J. Oral. Rehabil. 26, 208212.
Vallittu, P.K., Lassila, V.P., 1992. Reinforcement of acrylic resin denture base material with
metal or fibre strengtheners. J. Oral. Rehabil. 19, 225230.
Vallittu, P.K., Lassila, V.P., Lappalainen, R., 1994. Acrylic resin-fiber composite—Part I:
The effect of fiber concentration on fracture resistance. J. Prosthet. Dent. 71, 607612.
van Noort, R., 2012. The future of dental devices is digital. Dent. Mater. 28, 312.
Vojdani, M., Bagheri, R., Khaledi, A., 2012. Effects of aluminum oxide addition on the flexural strength, surface hardness, and roughness of heat-polymerized acrylic resin. J. Dent.
Sci. 7, 238244.
Yu, S.H., Lee, Y., Oh, S., Cho, H.W., Oda, Y., Bae, J.M., 2012. Reinforcing effects of different fibers on denture base resin based on the fiber type, concentration, and combination.
Dent. Mater. J. 31, 10391046.
Yu, W., Wang, X., Tang, Q., Guo, M., Zhao, J., 2014. Reinforcement of denture base
PMMA with ZrO2 nanotubes. J. Mech. Behav. Biomed. Mater. 32, 192197.
Further reading
Glossary of Prosthodontic Terms Committee of the Academy of Prosthodontics. The glossary
of prosthodontic terms. J. Prosthet. Dent. 117, e1e105.
6
Dental amalgam
Nasira Haque1, Safiyya Yousaf2, Touraj Nejatian3, Mansour Youseffi2,
Masoud Mozafari4,5 and Farshid Sefat6,7
1
Department of Biomedical and Electronics Engineering, School of Engineering,
University of Bradford, Bradford, United Kingdom, 2Medical Engineering Department,
Faculty of Engineering and Informatics, University of Bradford, Bradford, United Kingdom,
3
Eastman Dental Institute, University College of London, London, United Kingdom,
4
Bioengineering Research Group, Nanotechnology and Advanced Materials Department,
Materials and Energy Research Centre (MERC), Tehran, Iran, 5Department of Tissue
Engineering & Regenerative Medicine, Faculty of Advanced Technologies in Medicine,
Iran University of Medical Sciences (IUMS), Tehran, Iran, 6Interdisciplinary Research
Centre in Polymer Science & Technology (IRC Polymer), University of Bradford, Bradford,
United Kingdom, 7Biomedical and Electrical Engineering Department, School of
Engineering, University of Bradford, Bradford, United Kingdom
Chapter Outline
6.1 Introduction 106
6.2 Dental filling biomaterials
107
6.2.1 Gold fillings 107
6.2.2 Dental composites 108
6.2.3 Amalgam 109
6.3 History of amalgam 111
6.4 Composition of amalgam 112
6.4.1 Low-copper dental amalgam 112
6.4.2 High-copper dental amalgam 112
6.5 Amalgam bonding
113
6.5.1 Nonbonded amalgam restorations 113
6.5.2 Bonded amalgam restorations 114
6.5.3 Nonbonded versus adhesively bonded amalgam restorations 114
6.6 Material properties of amalgam
114
6.6.1 Compressive and tensile strength 114
6.6.2 Creep 115
6.6.3 Tarnish and corrosion 116
6.7
6.8
6.9
6.10
6.11
Dimensional change 117
Hardness 117
Young’s modulus 118
Failure mode 118
Biocompatibility 118
6.11.1 Toxicology of mercury 118
6.12 Conclusion
120
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00006-2
Copyright © 2019 Elsevier Ltd. All rights reserved.
106
Advanced Dental Biomaterials
References 121
Further reading 123
6.1
Introduction
Dentistry is the branch of medicine which deals with oral health. Services in this field
very much depend on the biomaterials, which have developed remarkably over the
years. The biomaterials are either directly prepared and placed in a tooth cavity or
indirectly made in a laboratory and cemented in the cavity. Various types of biomaterials such as polymer composites, glass ionomer cement, resin cement, gold, and
dental amalgams have been used as directed restorative materials. Dental amalgam as
a metallic direct restorative material is the primary focus of this chapter.
Dental amalgam is a popular biomaterial which has been used successfully in
the dental industry for decades. It is composed of a mixture of metal alloy and liquid mercury. Amalgam is mainly used for dental restorations. The metal alloy portion of this biomaterial has a composition made up of silver, tin, copper, and traces
of other metals. The unique composition of amalgam gives rise to many useful
properties such as excellent durability and strength. These are some of the many
factors behind the long service life of amalgam with an average of 810 years
(Delta Dental, 2012a,b).
The main application of dental amalgam is the restoration of tooth cavities. After
removing infected tooth tissue, the cavity is modified to the required shape to receive
the amalgam filling. The constituents of amalgam are then mixed to form an amalgam
paste, which is then placed in the cavity and left to complete the chemical reaction and
become hard (FDA, 2017). Amalgam stays soft for a short period after it is mixed,
enough to condense and shape onto the prepared tooth (Gay et al., 1979; Bates, 2006).
This biomaterial is relatively cost-effective and widely used. Despite the benefits
of amalgam fillings, the safety of them has been a very controversial subject over
the years. This is due to the inclusion of elemental mercury within the composition
of amalgam. Analytical chemistry techniques were used to investigate dental amalgam, and it has been established that mercury is released continuously (Gay et al.,
1979; Bates, 2006). Mechanical friction from the teeth onto the amalgam and mercury being dissolved in saliva, aid the release of mercury. An epidemiological
assessment found that there was little to no evidence linking this biomaterial to any
effect mortality rates or chronic diseases (Gay et al., 1979; Bates, 2006).
A global treaty known as the Minamata Convention on Mercury has been put into
place by UNEP (United Nations Environment Programme) to decrease and where possible eliminate the use of mercury. This is to ensure the adverse effects that mercury
has on the environment and the human population are decreased. Under this treaty dental amalgam is undergoing a “phase down” of usage. The reason behind this decision
is to reduce the adverse effects of using this element, yet to still provide safe healthcare
(FDI World Dental Federation, 2017). This book chapter aims to investigate the application of amalgam as a dental biomaterial as well as the composition, biocompatibility,
bonding, and material properties of amalgam.
Dental amalgam
6.2
107
Dental filling biomaterials
6.2.1 Gold fillings
Gold has been used for over 4000 years as a dental restorative. During the early use
of gold in dentistry, a higher importance was given to the aesthetics it had to offer,
rather than its contribution to mastication. Gold fillings can be used to restore the
function of a tooth affected by dental caries. It is thought that alloyed gold is an
excellent choice for fillings, as it has excellent biocompatibility, is easy to manufacture, and lasts over an extended period (Knosp et al., 2003).
Pure gold is usually only used for the direct filling of cavities on the tooth surface. Only small cavities may have gold inserted onto them as gold fillings are
unable to withstand forces expelled during mastication. Pure gold is soft. Hence it
has nearly 50% elongation and a low-stress enduring capacity. These properties
allow the pure gold to be cold worked, which is necessary to place it into the cavity
easily. Alloyed gold may also be used as a restorative material, and gold is commonly alloyed with base metals (such as indium and copper) and noble metals
(Knosp et al., 2003). Cavities can also be filled with an investment cast gold alloy.
This material is cemented and used in both dental onlays and inlays (as shown in
Fig. 6.1). Alloys with 65%75% gold are commonly used. In addition, gold can be
electroformed and covered with porcelain, after which it may be cemented into the
designated cavity. Restorative dentistry involves dental bridges and crowns, and
involves applying electroformed gold onto porcelain veneers. Electroforming is
advantageous because it prevents gold from changing dimensions when it is fired
with porcelain, which then minimizes the number of steps required to achieve the
desired product. The electroformed gold produced high hardness which is
suitable for this application (Knosp et al., 2003).
Gold is a noble metal that has a high market value. Gold fillings are costly and
therefore unavailable to patients from all socioeconomic backgrounds. Gold casting
requires at least two appointments since the cavity must be prepared without undercuts and then the filling must be inserted, which adds to the expense. In comparison
to the longevity of a gold filling, the cost is not very significant. The process of
insertion is technique sensitive and requires skill from the dentist. In addition, since
gold is not tooth colored, it is, therefore, seldom used for anterior tooth restorations
(Donovan et al., 2008).
The gold casting is created in a laboratory where a replica of the opposing teeth
is present, which allows the filling to be shaped, so it aids mastication. It is easier
to achieve a smooth finish on a gold restoration, rather than other restorative materials since it is fabricated in the laboratory and is not affected by the oral environment. The smooth finish is advantageous as it is comfortable for the patient and
reduces plaque build-up (Donovan et al., 2008).
Gold is a “permanent” filling, in contrast to amalgam and resin composites, this
is because when it is properly prepared it will not marginally wear or fracture. The
gold filling protects the enamel at the edges of the restorations since it can be
placed with precision to support the enamel. The coefficient of expansion of gold is
108
Advanced Dental Biomaterials
Figure 6.1 Schematic drawing of restorative prostheses: (A) inlay, (B) onlay, (C) overlay,
and (D) pinlay.
close to a tooth. This property allows both tooth and restoration to undergo contraction and expansion in a complimentary way; this is essential as the temperature
within the oral cavity varies (Donovan et al., 2008).
6.2.2 Dental composites
Dental composites are used as fillings to restore cavities in a tooth due to decay.
Dental composites are usually made of a polymeric resin matrix and a glass filler.
The bis-GMA is commonly the main monomer for the resin matrix. However,
TEGDMA may be added to make the resin less viscous and, therefore easier to handle. Photopolymerization is used to harden the resin matrix, and the bis-GMA has
an essential role in reducing the volumetric shrinkage caused by this process. The
size of the glass filler (e.g., fibrillar silicate) can also affect the mechanical properties of the composite. Nanosized fillers aid properties such as Young’s modulus and
flexural strength of the composite. The composite filling is desirable for individuals
Dental amalgam
109
since it has a tooth color which is excellent for aesthetic purposes (Fong and Little,
2010).
In a study where the capacity of preventing bacterial microleakage was compared between different dental restoratives, the dental composites were one of the
best biomaterials which have been used (Murray et al., 2002). Microleakage causes
hypersensitivity within dentin due to the irregular fluid movement within its
tubules. Uncontrolled microleakage can also cause discomfort to the individual and
infection which may lead to pulp inflammation (Cox, 1994).
Ormocers are another form of dental composites and are formed via solution and
gelation processes (Sivakumar and Valiathan, 2006). They are composed of polysiloxane and have a matrix which has organicinorganic elements. Glass and
ceramic make up the inorganic portion of the matrix. Silane molecules connect the
organic and inorganic molecules. The properties of ormocers are highly dependent
on the proportion of the components that it is made of. Polysiloxanes are influencing factors for the elasticity of this dental biomaterial. The hardness and polarity of
an ormocer are determined by the organic polymers, whereas the inorganic polymers impact chemical stability (Zimmerli et al., 2010). This biomaterial was created
to minimize volumetric shrinkage, which is caused by the likeness between the
thermal expansion coefficient of other composites and the human tooth (Sivakumar
and Valiathan, 2006).
6.2.3 Amalgam
Dental amalgam is made into a paste and manipulated into the cavity shape onto a
carious tooth. This procedure must be carried out before the paste sets and hardens.
The mercury inclusion, within the composition of this biomaterial, has been a controversial matter for many years. However, it is not recommended to remove amalgam fillings that have previously been inserted without good reason. Unnecessary
loss of a healthy tooth segment and mercury vapor exposure may occur because of
the removal of the amalgam filling. Some individuals may be unable to receive
amalgam fillings due to sensitivity or allergy to the constituents that make up dental
amalgam (FDA, 2017). Dental amalgam will be focused on in greater detail within
later sections, as it is the primary focus of this chapter.
An amalgam is made up of mercury alloyed to one or more other metals.
Mercury does not alloy with certain metals such as iron, platinum, and tungsten.
Amalgamation is the process by which an amalgam is processed and is commonly
an exothermic reaction (Helmenstine, 2017). There are several examples of amalgams, such as the silver and gold amalgams. In this case, the mercury amalgamates
with each of the metals and is used to separate it from its ore. Amalgam extraction
is uncommon currently because of its adverse environmental impact. There is a
concern with regards to gold mining releasing toxic mercury vapor. Furthermore,
another example is the thallium amalgam which has a lower freezing point in comparison to pure mercury. This property makes it useful to use in low-temperature
thermometers. Finally, sodium amalgam can act as a reducing agent (Helmenstine,
2017) which is a species that donates electrons to another species.
110
Advanced Dental Biomaterials
Dental amalgam is commonly known as “silver fillings” since it has a gray
appearance. The main application of dental amalgam is, within dentistry, as a restoration material. The scientific research that has been reviewed by the FDA displays
no link between health issues and amalgam fillings. The FDA has deemed dental
amalgam fillings safe for use on both adults and children (aged 6 or above).
Furthermore, it has been established from limited evidence that this filling does not
have an adverse effect on the fetus during pregnancy. Also the levels of mercury in
breast milk, due to the mother having amalgam fillings, are acceptable since it is
lower than the value considered safe (FDA, 2017). The study that supports this
statement (Lygre et al., 2016) included many volunteers and found no substantial
evidence to support prenatal amalgam exposure caused health issues for the child.
Pereira (2016) conducted a study which compared dental amalgam to glass ionomers, composites, and resin ionomers. When compared to the other direct placement restorations, it was established that amalgam requires a more significant
amount of healthy tooth structure removed during cavity preparation. It was seen
that the other methods did not require this since they all included an adhesive bonding mechanism. Though this was the case, amalgam is still widely used in clinical
conditions since it has a broader tolerance range than the other methods.
In an age where aesthetics are becoming more vital, dental amalgam is inadequate since it has a nontooth color. This limitation usually leads to the use of amalgam fillings on mainly posterior teeth. However, in contrast to other direct
restoration methods, the cost of amalgam is significantly lower (Pereira, 2016).
This is beneficial in poorer countries where people are likely to choose dental
restorations, with costs being a more crucial factor in aesthetics. Failure rates of
amalgam are low; therefore they require replacement less often than other restoration methods (Pereira, 2016). The durability of amalgam ranges from “good to
excellent,” and this factor adds to the longevity of the dental restoration.
Mastication expends many forces onto the restorations, and therefore this is an
advantageous property. Amalgam also has a superior lifetime of approximately 10
years, which is a longer life span than the glass ionomer, composite, and resin ionomer. Although amalgam has the highest wear resistance in contrast to the other restoration methods, it is also the only one of a brittle nature, since it fragments
around the edges (Pereira, 2016).
Direct dental restorations must be placed into the cavity by a dental professional.
Amalgam filling placement is not technique sensitive. Therefore extensive experience is not be required by the dentist. Amalgam can be easily manipulated, and it is
possible to rectify mistakes carried out by the dentist. In addition, as opposed to
composites, the placement time of amalgam is short. These factors combined help
to make the dentist more comfortable and confident with amalgam usage (Pereira,
2016).
To see if there is a trend of amalgam usage worldwide, Burke (2004) reviewed
government guidelines on amalgam. Results displayed that there is a decrease in
usage worldwide, but the rate of depreciation cannot be identified due to insufficiently available publications. The use of amalgam has declined more slowly in the
United Kingdom, in comparison to the United States and Australia. One of the
Dental amalgam
111
main factors influencing this decline in use is the release of mercury. Limited studies have linked the toxic mercury release to Alzheimer’s disease and multiple sclerosis (Bates, 2006).
In extremely rare cases, individuals may have an allergic reaction to amalgam
fillings. Metal constituents of the filling, such as the elemental mercury, can be the
cause of this reaction. Individuals, who have a family history of this issue, are the
most susceptible to this condition. Symptoms of this allergic reaction can include
skin rashes (Oral Health Centre, 2016b). Amalgam restorations can also lead to
amalgam tattoos. These tattoos can occur during the insertion of the amalgam
restorations if any of the constituents are accidentally implanted onto neighboring
palatal, buccal, gingival, or lingual mucosa. The accumulation of these constituents
may leave a gray/black oral lesion behind. Though they are benign, they may
resemble oral lesions which are caused by melanoma or Kaposi’s sarcoma. These
causes are more severe, but they can be quickly ruled out by biopsy (Dubach and
Caversaccio, 2011).
6.3
History of amalgam
The exact origin of dental amalgam is unknown, but in 1826 it was recorded that
the Frenchman Monsieur Travaux introduced this material. During this period, dental amalgam consisted of mercury combined with finely ground silver coins. In the
United States during 1895, a dental amalgam alloy which had a silvertin composition was founded by Dr. G.V. Black. The silvertin alloy particles were combined
with mercury. Once the alloy particles and mercury reacted, the initial plastic
behavior allowed it to be shaped onto the tooth and then harden into place
(Hollenback, 1969; Pereira, 2016).
During the early 19th century, amalgam was also used for dental restorations in
Europe. During this period there were other metallic restorations available which
included hammered lead and gold. In contrast to amalgam, the other restorations
had an absence of toxic mercury and had an intricate insertion technique. These factors made the usage of amalgam questionable within the dental field (Greener,
1979; Nicholson, 2002).
The controversy over amalgam usage led to the “amalgam wars” in the United
States. Dentists during this period had a divided opinion about the safety of amalgam fillings. Some dentists ceased amalgam usage since the mercury had a toxic
nature and it was seen to be unethical to put patients at unnecessary risk. The
American Society of Dental Surgeons, a professional body at the time, supported
the prevention of amalgam usage. They grouped together dentists who did not use
amalgam against the dentists who were still using amalgam. Specifications which
included thorough testing of amalgam were released in 1929, by the American
Dental Association. This aided in making more desirable amalgams, that not only
carried out their function but also put patients at a lower risk (Greener, 1979;
Nicholson, 2002).
112
Advanced Dental Biomaterials
Many figures had an impact on dental amalgam advancements. Notably in 1896,
Dr. G.V. Black established the formulae of a balanced dental amalgam composition.
This composition has a likeness to the modern-day dental amalgam. The formulae
considered the level of contraction and expansion that the amalgam would go
through during its lifetime. The cavity preparation techniques which he established
made the insertion of amalgam simpler and still act as guidance to dentists today
(Singh, 2015).
6.4
Composition of amalgam
The alloy segment of dental amalgam can be formed using techniques such as lathe
cutting and gas atomization which produces lathe cut or spherical particles, respectively. Various criteria are used for classification of dental amalgams. Among those,
the classification based on copper content is probably the most popular one due to
the significant effect that copper has on properties of dental amalgam. The traditional amalgam which has a copper particle concentration lower than 6 wt.% is classified as low-copper amalgam, whereas when the alloy portion of the amalgam
contains greater than 810 wt.% copper particles, it is classified as high-copper
amalgam (Okabe and Cahn, 1990; Hooghan et al., 1996).
6.4.1 Low-copper dental amalgam
Low-copper amalgam was initially used for fillings and has a composition of
approximately 24.327.6 wt.% tin, 66.772.5 wt.% silver, 1.25.5 wt.% of copper, and occasionally other metals were included (Okabe and Cahn, 1990; Hooghan
et al., 1996). High-copper amalgam has now replaced this compound because it has
better suited qualities to function as a dental filling (Dental Science, 2016).
Hooghan et al. (1996) used transmission electron microscopy to investigate the
microstructure of low-copper amalgam. The analysis displayed that the unreacted γ
(Ag3Sn) phase was surrounded by the γ1 (Ag2Hg3) and γ 2 (HgSn7) phases. It was also
noticed that the reaction layer between γ and γ1 phase included a mixture of β1
(AgHgSn) and some of the Cu6Sn5 (η) phase. The γ1 phase holds the amalgam
together and has a similar strength and corrosion resistance to the γ phase, though it has
a brittle nature. The γ2 phase is the weakest structure, and if this phase is large it may
lead to corrosion (Dental Science, 2016). The amalgamation reaction of low-copper
amalgams can be summarized into the following equation (Dental Science, 2016):
Excess γ-Ag3 Sn 1 Hg ! Unreacted γ-Ag3 Sn 1 γ1 -Ag2 Hg3 1 γ2 -Sn7 Hg
6.4.2 High-copper dental amalgam
High-copper amalgam alloy consists of 17.030.2 wt.% tin, 39.970.1 wt.% silver,
9.529.9 wt.% copper, and may include 0.012.0 wt.% zinc (Okabe and Cahn, 1990;
Dental amalgam
113
Hooghan et al., 1996). Admixed or single-composition alloys are used to prepare this
type of amalgam. An admixed composition consists of both lathe cut and spherical
particles, whereas single-composition alloys contain the same shape of particles
throughout (Dental Science, 2016).
The γ2 phase (Sn7Hg) is found in the majority of silvertin alloys (Sarkar and
Eyer, 1987; Yap et al., 2004). These alloys were created to reduce the weak γ2
phase (Sn7Hg) by forming more of the (Cu6Sn5) η phase (Beech, 1982). The highcopper amalgam has superior corrosion and creep resistance properties when compared to its predecessor (Sarkar and Eyer, 1987; Yap et al., 2004). Acciari et al.
(2005) have suggested that another beneficial quality of the high-copper amalgam
is that it decreases toxicity due to mercury vapor emission.
During the amalgamation of high-copper dental amalgam, mercury reacts with a
powdered amalgam alloy and forms a metallurgical structure. The amalgam alloy is
usually made up of copper, silver, tin, and other metals. The solubility of the elements involved is different. Therefore this gives rise to the dissolving of compounds. The mercury defuses into silvertin particles and dissolves them partially.
Silvercopper particles, however, are less reactive with mercury (Craig, 1985;
Acciari et al., 2005).
The γ1 (Ag2Hg3) and γ2 (Sn7Hg) phases are formulated when silvertin particles
are partially dissolved in the mercury. The γ2 phase surrounding the silvertin particles and the γ1 phase surrounding the silvercopper particles react to form the η
phase (Cu6Sn5). During this process, some silvertin particles (γ phase) are left
unreacted (Craig, 1985; Acciari et al., 2005). In other words, high-copper converts
the weak and corrosive γ2 phase to a stronger and less corrosive γ1 phase. A structure with up to six phases is produced, and the following equations display the
amalgamation process (Craig, 1985; Acciari et al., 2005):
γ-Ag3 Sn 1 AgCu 1 Hg ! γ1 -Ag2 Hg3 1 γ2 -Sn7 Hg 1 γ-Ag3 Sn 1 AgCu
γ2 -Sn7 Hg 1 AgCu ! η-Cu6 Sn5 1 γ1 -Ag2 Hg3
Although high-copper amalgam is preferred today, the increased content of copper does not always mean an improved clinical performance. When comparing a
modified low-copper amalgam to a high-copper amalgam, it is possible that they
can show similar clinical performance (Beech, 1982).
6.5
Amalgam bonding
6.5.1 Nonbonded amalgam restorations
Dental amalgam does not naturally bond to the tooth surface. The amalgam must be
mechanically retained to the tooth via cavity preparation. Retention methods of
amalgam may include mechanical devices to aid adherence. Generally, the process
of cavity preparation for nonbonded amalgam is less conservative and can lead
to loss of healthy tooth structure, which is the main disadvantage of this method.
114
Advanced Dental Biomaterials
This leads to the remaining tooth structure becoming weakened; therefore fracture
may occur (Dean, 2016).
6.5.2 Bonded amalgam restorations
Bonded amalgam restorations are made via an adhesive lining material that is
placed under the amalgam. This dental lining has dentin bonding ability and amalgam is placed over it before the adhesive sets. A mechanical bond forms between
amalgam and the bonding as the two materials intermix (Dean, 2016). Bonded
amalgam restorations reduce the need for cavity preparation to retain the amalgam
restoration. This is highly beneficial because the healthy remains of the tooth structure can be salvaged (Bonsor, 2011). Microleakage is the passage of bacteria, molecules, and fluids between the restorative material and tooth (Muliyar et al., 2014). It
is beneficial as the restoration will have a low possibility of microleakage and bacterial invasion through the toothmaterial interface. This decreases the risk of sensitivity after restoration and recurrent caries in the long term. Bonding can help
with maintaining the integrity of tooth structure which in turn reduces the probability of tooth fracture (Bonsor, 2011).
6.5.3 Nonbonded versus adhesively bonded amalgam
restorations
A study reviewed articles investigating the bonding of amalgam, and their main
findings included an investigation on 31 patients, who in total received 113 amalgam restorations. These restorations were made of either adhesively bonded or nonbonded amalgam. After 2 years there was a follow-up examination, which found no
significant difference between the two groups, in marginal change or sensitivity
after insertion. Although a small sample size was used and the study was carried
out in a university dental clinic, the data may not be representable. This may show
that there is limited evidence to show nonbonded amalgam restorations perform
worse than adhesively bonded amalgam. The review also suggested dentists may
have to consider the additional costs for the adhesively bonded amalgam
(Agnihotry et al., 2016). Vanishree et al. (2015) found that bonded amalgam has
less probability of microleakage when compared to composite resins and nonbonded amalgam restorations. Also, the study showed that the samples restored by
bonded amalgam and composite resins had an inconsistent fracture resistance in
comparison to nonbonded amalgam.
6.6
Material properties of amalgam
6.6.1 Compressive and tensile strength
An amalgam restoration must be able to withstand biting forces acting during mastication. Therefore it is essential that it has a high compressive strength. The
Dental amalgam
115
compressive strength of the high-copper amalgam is 414 MPa, whereas low-copper
amalgam is considerably lower, 380 MPa (Thomas et al., 2013). Jayanthi and
Vinod (2013) carried out a study to compare the compressive and flexural strength
of dental materials used as core build-up procedures. This study included amalgam
(DPI), Fluorocore composite (DENTSPLY, Caulk), Vitremer glass ionomer (3 M),
and nanocomposite Filtek (3 M). The flexural strength of amalgam was found to be
the lowest of all materials being tested. It had also been established that the compressive strength of amalgam as core build-up material was higher than Vitremer
but lower than that of the composites tested. Dental amalgam is unable to withstand
high tensile stresses, and therefore to avoid fracture the positioning of it within the
cavity must be carefully thought out. This means the tooth cavity should be prepared in a way that the restoration is subjected to the least tensile and shear forces
possible. Low-copper amalgam can withstand 60 MPa of a shear force or tension
(Manappallil, 2016).
During the initial placement of amalgam, since it has a low strength, patients are
advised to not bite down hard on it for the first 8 hours. During the setting process
when the amalgam begins to solidify, the strength of the amalgam also begins to
increase. After these initial 8 hours, the amalgam has nearly reached its complete
strength. It is essential for the amalgam to meet the ISO specifications of having a
specified compressive strength after 1 hour (100 MPa) and 24 hours (350 MPa).
Certain amalgams continue increasing in strength even after 6 months, and this may
suggest a continuous reaction between the alloy particles and matrix. The composition is also a factor which affects strength. High-copper single-composition amalgams have the advantage of achieving a high strength (262 MPa) within the first
hour of placement (Manappallil, 2016), which will reduce the risk of immature failure of the restoration and patients’ discomfort. Hasheminezhad et al. (2012) investigated whether the compressive strength of amalgam is affected by copper content.
They found that high-copper content in amalgam leads to higher compressive
strength, due to the elimination of the γ2 phase. There is a positive correlation
between strain rate and fracture stress for a copper amalgam. In addition, amalgam
alloy particles may change shape from lathe cut into spherical during the processing
due to the increase of copper within their composition.
6.6.2 Creep
Amalgam suffers from creep when oral forces cause stress and gradually changes
its shape. This can occur under constant or intermittent stress (Manappallil, 2016).
A high creep rate occurs when there is a gradual failure at the margins of the amalgam filling (Powers and Wataha, 2017). The amalgam begins to flow, which results
in parts of it slightly detaching from the cavity and protruding. The protruded edges
are unsupported and may fracture under the occlusal forces leaving marginal
ditches. The unsupported edges and ditches may also trap food and lead to decay
(Thomas et al., 2013).
Creep is affected by microstructure in low-copper amalgam. Larger γ1 (Ag2Hg3)
phase particles display a lower creep rate, whereas higher creep rates are linked to
116
Advanced Dental Biomaterials
the γ2 (Sn7Hg) phase. Low-copper lathe cut amalgam can have up to 6% creep
which exceeds the allowable limit. Due to the lack of γ2 phase, single-composition
high-copper amalgams, in contrast, have a lower creep rate. Another creep preventative factor in high-copper amalgam is the (η phase) Cu6Sn5 rods stopping the γ1
phase from breaking down. To produce an amalgam with a low creep rate and high
strength, it is essential to keep the mercury to alloy ratio low (Manappallil, 2016).
The creep values of currently used amalgams are very low (Powers and Wataha,
2017).
6.6.3 Tarnish and corrosion
Amalgam restorations that are placed into tooth cavities are susceptible to tarnish
and corrosion (Manappallil, 2016). Tarnishing of the amalgam occurs at the surface
level; it can be recognized by discoloration from chemical reactions with food.
Whereas corrosion can chemically degrade both the surface and the bulk of a tooth,
internal corrosion can decrease the strength and affect the shape of the amalgam,
which inevitably can lead to failure of the filling (Powers and Wataha, 2017). Lowcopper amalgam restorations are more likely to undergo corrosion since they have a
larger γ2 phase. The finding of a study (Amin, 2007) supported low-copper amalgam having a lower corrosion resistance when compared to high-copper amalgam.
The study also found that corrosion resistance improved for both types of amalgam
when they were left to age in an artificial oral environment. A factor which can
increase corrosion levels are patients who are on high sulfur diets, which
encourages the formation of black silver sulfide on the surface of the filling. High
residual mercury and scratched surface texture of the restoration are the other contributing factors. After the amalgam restoration has been placed into the cavity, polishing the restoration slows down its corrosion. In addition to this, it is crucial to
mix the correct proportions of mercury to alloy, since it is possible that excess corrosion may otherwise be caused (Manappallil, 2016).
6.6.3.1 Marginal sealing
Upon the initial placement of amalgam, there is a slight gap between the amalgam
and cavity walls (Mahler et al., 2009). This gap contains fluid containing molecules,
ions, and bacteria (Ben-Amar et al., 1995). Amalgam has a unique ability to seal its
marginal gap. This occurs since the margins of amalgam fillings naturally corrode
while in service and this leads to corrosive deposits forming. Microleakage is
decreased, as the corrosion products build up to fill the gap around the restoration,
and seal it. Sealing can reduce chances of bacterial invasion. It is difficult to judge,
solely from the appearance of the amalgam’s margins, whether the amalgam filling
is sealed and if there is a chance of secondary caries. This is because despite having
worn down margins, it is possible to have a well-sealed amalgam filling (Dental
Science, 2016).
High-copper amalgam has a higher corrosion resistance when compared to lowcopper amalgam. A study investigated whether it would take high-copper amalgam
longer to create a seal, due to a slower formation of corrosive deposits. The results
Dental amalgam
117
suggested that it is difficult to anticipate the sealing behavior of amalgam based on
corrosion resistance alone. Factors such as the gap size and inclusion of zinc within
the amalgams composition, also play a vital role. It was found that it is possible for
high-copper amalgam to seal at a similar speed as its low-copper counterpart if the
initial gap between the cavity wall and amalgam was small (Mahler et al., 2009). In
addition, sealing via corrosive deposits can occur more rapidly if the amalgam is
adapted to fit the cavity walls when placed (Ben-Amar et al., 1995).
6.7
Dimensional change
Amalgam undergoes dimensional changes during the setting period (Espevik,
1977). Powers and Wataha (2017) defined the overall expansion or contraction of
amalgam during its initial setting reaction to be dimensional change. During the initial setting reaction, commonly expansion occurs due to matrix formation, whereas
contraction is the result of a reaction between the amalgam alloy particles and mercury. Factors such as the proportion of amalgam alloy to mercury and trituration/
condensation procedures can affect dimensional change. Improper mixing force/
time can adversely affect this factor. Expansion during the setting reaction of amalgam is sought after (Powers and Wataha, 2017). Commonly trituration time of the
amalgam alloy can be modified to favor the expansion of amalgam, although it is
not advised since other vital properties may become compromised (Espevik, 1977).
Once an ideal amalgam is placed into the prepared cavity, it would not expand
or contract (Powers and Wataha, 2017). Therefore it is preferred for amalgam to
have little dimensional change upon insertion. This is mainly because postoperative
sensitivity can be the result of both excessive expansion and contraction. Leakage
and decay could also occur if the amalgam underwent excessive contraction (Dental
Science, 2016), because this would create a gap between the amalgam and cavity
wall. Excessive expansion can also cause the amalgam to move out of the prepared
cavity and bulge (Powers and Wataha, 2017). Each type of amalgam behaves differently. However, adherence to the manufacturer’s instructions will positively impact
dimensional change (Dental Science, 2016). The requirement for dimensional
change, ruled by the American Dental Association (ADA) is 20 μm/cm or less.
Most modern amalgams have a dimensional change of zero (Powers and Wataha,
2017). The size of the amalgam restoration can affect the life expectancy. Smaller
restorations usually undergo less stress, and therefore their life expectancy
increases. Class I amalgam can last between 15 and 18 years, whereas Class II
amalgam has a life expectancy of 1215 years. The patient’s oral hygiene and diet
largely impact the life expectancy of amalgam restorations (Dental Science, 2016).
6.8
Hardness
Optimal hardness in dental amalgam also contributes to the success of amalgam
restorations. Although hardness is defined as the resistance of the materials against
118
Advanced Dental Biomaterials
scratches, hardness tests actually measure the resistance of a material against indentation from a harder material onto its surface. A study was carried out to see how
the addition of zinc oxide (ZnO) and aluminum oxide (Al2O3) nanoparticles
affected the hardness of dental amalgam. It was found that when the 40% ZnO filler
(the highest proportion) was added to the composition, the hardness increased the
greatest, to a value of 0.95 GPa on the Vickers scale. It was observed that different
annealing temperatures of ZnO affected the hardness of the dental amalgam. More
excellent grain size is created when the ZnO nanoparticles undergo a lower annealing temperature. It was observed that a finer grain size gave better material hardness. In addition, it was observed that adding a more significant proportion of
Al2O3 filler produced larger increments in hardness than increasing the ZnO filler
(Yahya et al., 2013).
6.9
Young’s modulus
Beatty and Pidapartil (1993) established that amalgam has almost 3.5 times greater
elastic modulus in tension in comparison to compression. This is greater than the
composite resin tested, which had double the elastic modulus in tension in contrast
to its compression. This factor was thought to decrease the tensile stress upon the
dental amalgam bending. A study carried out by Kumar and Shivrayan (2015)
found that high-copper amalgam (named Hi-Aristaloy) possessed the highest value
for elastic modulus (17.28 GPa) when compared to other direct core dental biomaterials. In addition, it was found that the γ (Ag3Sn), γ1 (Ag2Hg3), and γ2 (Sn8Hg)
phases in amalgam have different values of elastic modulus, where γ was seen to
have the highest value (Davies et al., 2010).
6.10
Failure mode
Wang and Darvell (2007) conducted a study on the failure mode of dental biomaterials, including amalgam. When the amalgam was subjected to Hertzian indentation,
it failed primarily from plastic deformation as the thickness of amalgam became
larger or radial cracking originated from its underside. An amalgam of a range of
different thicknesses failed. Also, it was reported that a correlation was found
between failure load and thickness of amalgam, excluding extremities.
6.11
Biocompatibility
6.11.1 Toxicology of mercury
The composition of dental amalgam includes approximately 50% mercury. This
inclusion is very controversial since mercury has been linked to many diseases
Dental amalgam
119
(Bates, 2006). Mercury is a naturally occurring element in the environment, and it
can also be found in the Earth’s crust. Though amalgam fillings are a source of
mercury exposure (Rathore et al., 2012), Clarkson et al. (2003) reported that the
other main exposure sources are fish consumption and vaccines. Fish consumption
is a source of methylmercury, whereas vaccines can cause exposure to ethyl mercury. These are both organic forms of mercury.
Mercury exposure mainly occurs during the removal or insertion of the dental
amalgam filling. After the filling has hardened, the mercury vapor release decreases
to a value that is below the acceptable threshold. An individual may undergo
delayed hypersensitivity because of the insertion of the amalgam filling, the chance
of this occurring can be reduced if mercury hygiene procedures are performed
(Rathore et al., 2012). The mercury vapor produced is mostly inhaled, and it may
also be absorbed into the blood. Dentists are occupationally exposed while they are
placing the restorations (Clarkson et al., 2003). Ucar and Brantley (2011) conducted
a study to review the literature regarding the toxicology of mercury from dental
amalgam. They concluded that the termination of dental amalgam use could not be
justified from the literature.
Mercury is continuously released from the inserted amalgam filling (Bates,
2006). Ucar and Brantley (2011) reported that factors such as age, amalgam composition, and individual mastication style affect the release of mercury into the oral
cavity. Once the mercury has been released, it is dissolved in saliva and passes into
the individual. This can occur if intraoral air containing mercury vapor is inhaled
and if the filling particles that wear away during mastication are ingested. In addition, swallowing saliva, which has environmental mercury alongside dissolved particles, can pass mercury into an individual. Table 6.1 displays significant forms of
mercury exposure, the path the mercury takes within the body, and treatment
options.
Table 6.1 Major forms of mercury exposure, the path the mercury takes within the body,
and treatment options.
Variable
Mercury vapor
Inorganic
divalent
mercury
Methylmercury
Ethylmercury
Route of
exposure
Inhalation
Oral
Oral (from fish
consumption)
Target organ
Central nervous system,
peripheral nervous
system, kidney
Kidney
Central nervous
system
Parenteral
(through
vaccines)
Central
nervous
system,
kidney
(Continued)
120
Advanced Dental Biomaterials
Table 6.1 (Continued)
Variable
Mercury vapor
Inorganic
divalent
mercury
Methylmercury
Ethylmercury
Local clinical signs
Lungs
Gastrointestinal
tract
Bronchial irritation,
pneumonitis
( . 1000 μg/m3 of air)
Metallic taste, stomatitis,
gingivitis, increased
salivation ( . 1000 μg/
m3 of air)
Skin
Metallic taste,
stomatitis,
gastroenteritis
Urticarial,
vesication
Systemic clinical signs
Kidney
Peripheral
nervous
system
Central nervous
system
Appropriate
half-life
(whole body)
(days)
Treatment
6.12
Proteinuria ( . 500 μg/m3 Proteinuria,
of air)
tubular
necrosis
Acrodynia
Peripheral neuropathy
( . 500 μg/m3 of air)
Erethism ( . 500 μg/m3 of
air)
60
40
Meso-2dimercaptosuccinic
acid
Meso-2-3dimercaptosuccinic acid
Tubular
necrosis
Acrodynia
Paresthesia,
ataxia
visual and
hearing loss
Paresthesia, ataxia
visual and
hearing loss
( . 200 μg/L of
air)
70
20
Chelators not
effective
Chelators not
effective
Conclusion
Amalgam is a popular biomaterial that has been used successfully for over 150
years, despite the controversial matter of its mercury content. Dental amalgam is
mainly used as a direct restorative material. Placement of amalgam restorations is
less technique sensitive than resin composites. Therefore dentists find it easy to use
with a more predictable outcome. Also, its ability to gain marginal seal after corrosion and to achieve reasonably high compressive strength contributed to its good
clinical performance. Despite the risk from mercury exposure, it has kept its popularity in most countries due to its low cost.
Dental amalgam
121
References
Acciari, H.A., Guastaldi, A.C., Brett, C.M.A., 2005. Corrosion of the component phases presents in high copper dental amalgams. Application of electrochemical impedance spectroscopy and electrochemical noise analysis. Corros. Sci. 47 (3), 635647.
Agnihotry, A., Fedorowicz, Z., Nasser, M., 2016. Adhesively bonded versus non-bonded
amalgam restorations for dental caries. Cochrane Database Syst. Rev. (3), CD007517.
Amin, W.M., 2007. Comparative electrochemical investigation of the effect of aging on corrosion of dental amalgam. Quintessence Int. 38 (7), e417e424.
Bates, M.N., 2006. Mercury amalgam dental fillings: an epidemiologic assessment. Int. J.
Hyg. Environ. Health 209 (4), 309316.
Beatty, M.W., Pidapartil, R.M.V., 1993. Elastic and fracture properties of dental direct filling
materials. Biomaterials 14 (13). Available from: https://www.sciencedirect.com/science/
article/pii/0142961293901925 (accessed 9.03.18.).
Beech, D.R., 1982. High copper alloys for dental amalgam. Int. Dent. J. 32 (3), 240251.
Ben-Amar, A., Cardash, H.S., Judes, H., 1995. The sealing of the tooth/amalgam interface by
corrosion products. J. Oral Rehabil. 22 (2), 101104.
Bonsor, S.J., 2011. Bonded amalgams and their use in clinical practice. Dent. Update 38 (4),
222224. 226-8, 230.
Burke, F.J.T., 2004. Amalgam to tooth-coloured materials—implications for clinical practice
and dental education: governmental restrictions and amalgam-usage survey results. J.
Dent. 32 (5), 343350. Available from: https://www-sciencedirect-com.brad.idm.oclc.
org/science/article/pii/S0300571204000430?via%3Dihub.
Clarkson, T.W., Magos, L., Myers, G.J., 2003. The toxicology of mercury—current exposures and clinical manifestations. N. Engl. J. Med. 349 (18), 17311737.
Cox, C.F., 1994. Evaluation and treatment of bacterial microleakage. Am. J. Dent. 7 (5),
293295. Available from: https://www.ncbi.nlm.nih.gov/pubmed/7986455.
Craig, R.G., 1985. Restorative Dental Materials, seventh ed. Mosby.
Davies, R.A., Ardalan, S., Mu, W., Tian, K., Farsaikiya, F., Darvell, B.W., et al., 2010.
Geometric, electronic and elastic properties of dental silver amalgam γ-(Ag3Sn), γ1(Ag2Hg3), γ2-(Sn8Hg) phases, comparison of experiment and theory. Intermetallics 18
(5), 756760. Available from: https://doi.org/10.1016/j.intermet.2009.12.004 (accessed
10.03.18.).
Dean, J.A., 2016. McDonald and Avery’s Dentistry for the Child and Adolescent, 10th ed.
Elsevier.
Delta Dental, 2012a. Dental amalgam or resin composite fillings?. ,https://www.deltadentalins.com/oral_health/amalgam.html..
Delta Dental, 2012b. What is plaque?. ,https://www.deltadentalins.com/oral_health/plaque.
html..
Dental Science, 2016. Amalgam: properties, uses, toxicity and advantages. ,http://www.dental-science.com/amalgam/..
Donovan, T., Simonsen, R.J., Guertin, G., Tucker, R.V., 2008. Why gold castings are excellent restorations. J. Oper. Dent. 33 (2), 113115. Available from: https://www.jopdent.
com/journal/editorial/openFile.php?takeFile 5 Volume_33__Issue_2.txt.
Dubach, P., Caversaccio, M., 2011. Amalgam tattoo. N. Engl. J. Med. 364, e29. Available
from: https://doi.org/10.1056/NEJMicm1011669.
Espevik, S., 1977. Effect of trituration on dimensional changes of dental amalgam. Acta
Odontol. Scand. 35 (5), 251255.
122
Advanced Dental Biomaterials
FDA, 2017. About dental amalgam fillings. ,https://www.fda.gov/MedicalDevices/
ProductsandMedicalProcedures/DentalProducts/DentalAmalgam/ucm171094.htm#1..
FDI World Dental Federation, 2017. Minamata convention on mercury comes into force in
august affecting use of dental amalgam. ,https://www.fdiworlddental.org/news/
20170606/minamata-convention-on-mercury-comes-into-force-in-august-affecting-useof-dental..
Fong, H., Little, M.J., 2010. Dental Composites with Nano-Scaled Fillers. Nova Science
Publishers, Inc. Available from: https://ebookcentral-proquest-com.brad.idm.oclc.org/lib/
bradford/detail.action?docID 5 3018712.
Gay, D.D., Cox, R.D., Reinhardt, J.W., 1979. Chewing releases mercury from fillings.
Lancet 1 (8123), 985986.
Greener, E.H., 1979. Amalgam—yesterday, today, and tomorrow. Oper. Dent. 4 (1), 2435.
Hasheminezhad, A., Zebarjad, S.M., Sajjadi, S.A., Rahanjam, L., 2012. Effect of copper content on compressive strength and microstructure of dental amalgams. Sci. Res. 4,
155159. Available from: https://doi.org/10.4236/eng.2012.43020.
Helmenstine, A.M., 2017. Amalgam Definition and Uses. ThoughtCo. Available from:
https://www.thoughtco.com/amalgam-definition-4142083.
Hollenback, G.M., 1969. A consideration of amalgam. J. Calif. Dent. Assoc. 45, 1518.
Hooghan, T.K., Pinizzotto, R.F., Watkins, J.H., Okabe, T., 1996. A study of a low copper
dental amalgam by analytical transmission electron microscopy. J. Mater. Res. 11 (10),
24742485.
Jayanthi, N., Vinod, V., 2013. Comparative evaluation of compressive strength and flexural
strength of conventional core materials with nanohybrid composite resin core material
an in vitro study. J. Indian Prosthodontic Soc. 13 (3), 281289.
Knosp, H., Holliday, R.J., Corti, C.W., 2003. Gold in dentistry: alloys, uses and performance.
Gold Bull. 36 (3), 93102. Available from: https://link.springer.com/content/pdf/
10.1007/bf03215496.pdf (accessed 23.02.18.).
Lygre, G.B., Haug, K., Skjærven, R., Björkman, L., 2016. Prenatal exposure to dental amalgam and pregnancy outcome. Community Dent. Oral Epidemiol. 44 (5), 442449.
Available from: https://doi.org/10.1111/cdoe.12233.
Mahler, D.B., Pham, B.V., Adey, J.D., 2009. Corrosion sealing of amalgam restorations
in vitro. Oper. Dent. 34 (3), 312320. Available from: https://doi.org/10.2341/08-94.
Manappallil, J.J., 2016. Basic Dental Materials., fourth ed. Jaypee Brothers Medical
Publishers (P) Ltd..
Muliyar, S., Shameem, K.A., Thankachan, R.P., Francis, P.G., Jayapalan, C.S., Hafiz, K.A.
A., 2014. Microleakage in endodontics. J. Int. Oral Health 6 (6), 99104.
Murray, P.E., Hafez, A.A., Smith, A.J., Cox, C.F., 2002. Bacterial microleakage and pulp
inflammation associated with various restorative materials. Dent. Mater. 18 (6),
470478. Available from: https://www.ncbi.nlm.nih.gov/pubmed/12098576.
Nicholson, J.W., 2002. The Chemistry of Medical and Dental Materials, Royal Society of
Chemistry.. Royal Society of Chemistry. Available from: https://ebookcentral-proquestcom.brad.idm.oclc.org/lib/bradford/reader.action?docID 5 1185355&query.
Okabe, T., Cahn, R.W., 1990. Encyclopedia of Materials Science and Engineering. Pergamon
Press, Oxford.
Oral Health Centre, 2016b. Problems After Dental Fillings. Boots Web MD.. Available from:
https://www.webmd.boots.com/oral-health/guide/problems-dental-fillings.
Pereira, T., 2016. Silver amalgam: a clinician’s perspective. J. Dent. Res. 4 (2), 2530.
Available
from:
http://www.jresdent.org/article.asp?issn 5 2321-4619;year 5 2016;
volume 5 4;issue 5 2;spage 5 25;epage 5 30;aulast 5 Pereira.
Dental amalgam
123
Powers, J.M., Wataha, J.C., 2017. Dental Materials, Foundations and Applications., 11th ed.
Elsevier.
Rathore, M., Singh, A., Pant, V.A., 2012. The dental amalgam toxicity fear: a myth or actuality. Toxicol. Int. 19 (2), 8188. Available from: https://doi.org/10.4103/09716580.97191.
Sarkar, N.K., Eyer, C.S., 1987. The microstructural basis of creep of c1 in dental amalgam. J.
Oral Rehabil. 14 (27).
Shivrayan, A., Kumar, G., 2015. Comparative study of mechanical properties of direct core
build-up materials. Contemp. Clin. Dent. 6 (1), 16.
Singh, H., 2015. Remembering Sir G.V. Black. Indian J. Dent. 6 (3), 147148. Available
from: https://doi.org/10.4103/0975-962X.163047.
Sivakumar, A., Valiathan, A., 2006. Dental ceramics and ormocer technology—navigating
the future. Trends Biomater. Artif. Organs 20 (1), 4043.
Thomas, G.P., 2013. Amalgam-chemical composition, mechanical properties and common
applications. AZO Materials. Available from: https://www.azom.com/article.aspx?
ArticleID 5 8081. (accessed 19.01.18.).
Ucar, Y., Brantley, W.A., 2011. Review article, biocompatibility of dental amalgams. Int. J.
Dent. 2011, 17. Available from: https://doi.org/10.1155/2011/981595.
Vanishree, H.S., Shanthala, B.M., Bobby, W., 2015. The comparative evaluation of fracture
resistance and microleakage in bonded amalgam, amalgam, and composite resins in primary molars. Indian J. Dent. Res. 26 (5), 446450.
Wang, Y., Darvell, B., 2007. Failure mode of dental restorative materials under Hertzian
indentation. Dent. Mater. 23 (10), 12361244.
Yahya, N., Puspitasari, P., Latiff, N.R.A., 2013. Hardness improvement of dental amalgam
using zinc oxide and aluminium oxide nanoparticles. In: Ochsner, A., da Silva, L.,
Altenbach, H. (Eds.), Characterization and Development of Biosystems and
Biomaterials. Advanced Structured Materials, vol. 29. Springer, pp. 932.
Yap, A.U.J., Ng, B.L., Blackwood, D.J., 2004. Corrosion behaviour of high copper dental
amalgams. J. Oral Rehabil. 31, 595599.
Zimmerli, B., Strub, M., Jeger, F., Stadler, O., Lussi, A., 2010. Composite materials: composition, properties and clinical applications, a literature review. Schweiz Monatsschr
Zahnmed 120, 972979.
Further reading
Ajlan, S.A., Aldahmash, A.M., Ashri, N.Y., 2015. Dental pulp stem cells, biology and use
for periodontal tissue engineering. Saudi Med. J. 36 (12), 13911399.
Amalgam-chemical composition, mechanical properties and common applications. AZO
Mater. ,https://www.azom.com/article.aspx?ArticleID 5 8081..
American Dental Association, 2012a. Primary tooth development [Image]. ,http://www.
mouthhealthy.org/en/az-topics/e/eruption-charts..
American Dental Association, 2012b. Permanent tooth development [Image]. ,http://www.
mouthhealthy.org/en/az-topics/e/eruption-charts..
Beek, G.C.V., 1983. Dental Morphology, an Illustrated Guide, second ed. Billing & sons Ltd,
Worcester, pp. 4547.
Berkovitz, B.K.B., Holland, G.R., Moxham, B.J., 2018. Oral Anatomy, Histology and
Embryology., fifth ed. Elsevier.
124
Advanced Dental Biomaterials
British Orthodontic Society, 2014. Patient information leaflet, tooth transplants. https://www.
bos.org.uk/Portals/0/Public/docs/PILs/toothtransplantsmarch14.pdf.
Chano, L., Clokie, C.M.L., Yau, D.M., 2001. Autogenous tooth transplantation: an alternative
to dental implant placement. J. Can. Dent. Assoc. 67 (2), 9296.
Cohen, A.S., Pogrel, M.A., Shen, T.C., 1995. Transplanting teeth successfully: autografts and
allografts that work. J. Am. Dent. Assoc. 126 (4), 481485.
Davenport, T., 2017. What are the most common dental problems?. ,https://www.verywell.
com/top-common-dental-problems-1059461..
Dentagama, 2016. Image of the restorative prothesis: inlay, onlay, overlay, pinlay. ,https://
dentagama.com/news/what-is-the-difference-between-inlay-onlay-overlay-and-pinlay.
(accessed 25.02.18.).
D’Aguino, R., Graziano, A., Laino, G., Papaccio, G., 2008. Dental pulp stem cells: a promising tool for bone regeneration. Stem Cells Rev. 4 (1), 2126.
Harris, E.F., 2016. Odontogenesis. In: Irish, J.D., Scott, G.R. (Eds.), A Companion to Dental
Anthropology. John Wiley & Sons, pp. 145149.
Healthline, 2015. Incisors. ,https://www.healthline.com/human-body-maps/incisor..
Hoffman, M., 2009. Picture of the Teeth. WebMD [Image] . Available from: https://www.
webmd.com/oral-health/picture-of-the-teeth#1.
Hu, J.C.-C., Simmer, J.P., 2001. Dental enamel formation and its impact on clinical dentistry.
J. Dent. Educ. 65 (9), 896905.
Huang, G.T.J., 2009. Pulp and dentin tissue engineering and regeneration: current progress.
Regener. Med. 4 (5), 697707. Available from: https://doi.org/10.2217/rme.09.45.
Jethmalani, Y.D., Potdar, P.D., 2015. Human dental pulp stem cells: applications in future
regenerative medicine. World J. Stem Cells 7 (5), 839851.
Keels and The American Academy of Pediatrics Section on Oral Health, 2014. Management
of dental trauma in a primary care setting, the section on oral health. Pediatrics 133 (2),
e468. Available from: http://pediatrics.aappublications.org/content/133/2/e466.
Kim, N., Cho, S.G., 2013. Clinical applications of mesenchymal stem cells. Korean J. Intern.
Med. 28 (4), 387402. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/
PMC3712145/.
Konigsberg, S., Northway, W.M., 1980. Autogenic tooth transplantation: the “state of the
art”. Am. J. Orthod. Dentofacial Orthop. 77 (2), 146162.
MacConaill, M.A., 2017. Joint. Encyclopaedia Britannica, Inc. Available from: https://www.
britannica.com/science/joint-skeleton/Fibrous-joints#ref470986.
Marrelli, M., Tatullo, M., Shakesheff, K.,M., White, L.J., 2015. Dental pulp stem cells: function, isolation and applications in regenerative medicine. J. Tissue Eng. Regener. Med. 9
(11), 12051216.
Matalova, E., Antonarakis, G.S., Sharpe, P.T., Tucker, A.S., 2005. Cell lineage of primary
and secondary enamel knots. Dev. Dyn. 233 (3), 754759.
Mayo Clinic, 2017a. TMJ Disorders. Mayo Clinic. Available from: https://www.mayoclinic.
org/diseases-conditions/tmj/symptoms-causes/syc-20350941.
Mayo Clinic, 2017b. Mouth cancer. ,https://www.mayoclinic.org/diseases-conditions/
mouth-cancer/symptoms-causes/syc-20350997..
Mayo Clinic, 2017c. Periodontitis. ,https://www.mayoclinic.org/diseases-conditions/periodontitis/symptoms-causes/syc-20354473..
NHS Choices, 2016. Tooth decay. ,https://www.nhs.uk/conditions/tooth-decay/..
National Institute of Dental and Craniofacial Research, 2015. Oral cancer: causes and symptoms & the oral cancer exam. ,https://www.nidcr.nih.gov/OralHealth/Topics/
OralCancer/AfricanAmericanMen/CausesSymptoms.htm..
Dental amalgam
125
Newman, T., 2016. Bad breath (halitosis): causes, diagnosis and treatment. Medical News
Today . Available from: https://www.medicalnewstoday.com/articles/166636.php.
Norris, J., 2010. Tooth Enamel: Nature’s Crowning Achievement. University of California
San Francisco. Available from: https://www.ucsf.edu/news/2010/08/6000/tooth-enamelresearch-combines-science-and-engineering.
Open Stax, 2016. Anatomy & physiology. Open Stax CNX. Available from: http://cnx.org/
contents/14fb4ad7-39a1-4eee-ab6e-3ef2482e3e22@8.24.
Oral Health Centre, 2016a. Tooth Enamel Erosion and Restoration. Boots Web MD.
Available from: https://www.webmd.boots.com/oral-health/guide/tooth-enamel-erosionrestoration.
Oral Health Centre, 2017. Temporomandibular Joint Disorders (TMJ and TMD). Boots Web
MD. Available from: https://www.webmd.boots.com/oral-health/guide/temporomandibular-joint-disorders-tmj-tmd?page 5 3.
Science Learning Hub, 2011. Rate of digestion. ,https://www.sciencelearn.org.nz/resources/
1834-rate-of-digestion..
Skaria, S., 2016. Fibrous Joint—Gomphosis [Image]. ,https://www.slideshare.net/
SajanScaria/artrology..
Slootweg, P.J., 2007. Dental Pathology: A Practical Introduction.. Springer.
Stay, F., 2014. How your teeth affect your digestive system. ,http://www.totalhealthmagazine.com/Dental-Health/How-Your-Teeth-Affect-Your-Digestive-System.html..
Swindler, D.R., 2002. Primate Dentition: An Introduction to the Teeth of Non-human
Primates.. Cambridge University Press, Cambridge.
The editors of Encyclopaedia Britannica, 2007. Cementum. Encyclopaedia Britannica, Inc.
Available from: https://www.britannica.com/science/cementum.
The editors of Encyclopaedia Britannica, 2014. Dentin. Encyclopaedia Britannica, Inc.
Available from: https://www.britannica.com/science/dentin.
Watson, S., 2017. What is the Function of Tooth Pulp. Very Well. Available from: https://
www.verywell.com/tooth-pulp-dental-terms-1059180.
Yau, E.C.K., 2009. Tooth autotransplantation as a treatment option. Dent. Bull. 14 (6),
2124. Available from: http://www.fmshk.org/database/articles/03db05_2.pdf.
Zimmermann, K.A., 2016. Digestive System: Facts, Function & Diseases. Live Science.
Available from: https://www.livescience.com/22367-digestive-system.html.
Resin-based dental composites
for tooth filling
7
Ahmed El-Banna1, Dalia Sherief1 and Amr S. Fawzy2
1
Dental Biomaterials Department, Faculty of Dentistry, Ain-Shams University, Cairo,
Egypt, 2UWA Dental School, University of Western Australia, Nedlands, WA, Australia
Chapter Outline
7.1 Introduction 128
7.2 General composition
7.2.1
7.2.2
7.2.3
7.2.4
7.2.5
128
The resin matrix 128
Fillers 130
Silane coupling agent 134
Initiatoraccelerator system 134
Pigments and other components 136
7.3 Classification of resin composites
7.3.1
7.3.2
7.3.3
7.3.4
136
According to the fillers size and distribution 136
According to the composite consistency 137
According to the packing (placement) technique 138
According to the curing techniques 138
7.4 Clinical indications of resin composites
7.5 Properties and limitations 139
7.5.1
7.5.2
7.5.3
7.5.4
7.5.5
7.5.6
7.5.7
7.5.8
138
Degree of conversion 139
Polymerization shrinkage and polymerization shrinkage stresses
Physical properties 144
Esthetic properties 144
Mechanical properties 145
Biocompatibility 145
Degradation 147
Clinical durability 147
140
7.6 Attempts for resin composite improvement 148
7.6.1 Regarding material formulation 148
7.6.2 Regarding manipulation 154
7.6.3 Regarding both material formulation and manipulation 156
7.7 Guidelines and recommendations for future laboratory and clinical
researches 165
7.7.1 Guidelines for laboratory evaluation of resin composite (mechanical behavior and technique
sensitivity) 166
7.7.2 Recommendations for future clinical studies 166
References
171
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00007-4
Copyright © 2019 Elsevier Ltd. All rights reserved.
128
7.1
Advanced Dental Biomaterials
Introduction
In the mid-20th century acrylic resins were launched in the field of esthetic restorative dentistry to overcome the limitations of silicate cement. In 1955 Buonocore
developed the concept of using phosphoric acid as an attempt to enhance the bonding of acrylic resin restorations to enamel. Phosphoric acid induced selective dissolution within the enamel creating microporosities into which resin flows and
polymerizes creating micromechanical interlocking. In 1962 Bowen developed the
high molecular-weight bisphenol-aglycidyldimethacrylate (Bis-GMA) monomer as
a trial to upgrade the physical properties of acrylic resins, as their monomers only
allowed linear chain polymers to be formed. Resin composites were developed in
1962 by combining dimethacrylates (epoxy resin and methacrylic acid) with silanized quartz powder.
Early chemically cured composites required the mixing of both base and catalyst
pastes together leading to inaccurate proportioning and mixing thus affecting the
properties. From 1970, composite materials cured by electromagnetic radiation
emerged, eliminating the need for mixing and its drawbacks. Ultraviolet light
sources were used first to provide the required polymerization energy. The limited
polymerization depth and induced side effects of ultraviolet radiation led to its
replacement by visible light (427491 nm), which is currently in use and undergoing further development (Fig. 7.1) (Leprince et al., 2013; Ferracane, 2011).
During the past decade, resin composites have become the most widely used
restorative materials, gradually replacing amalgam restorations, which have been the
standard restorative material for more than 100 years. Such transition was not only
due to the favorable esthetics of resin composites but also due to the highly conservative cavity preparation compared to that of amalgam. Since amalgam toxicity is still a
point of debate, there is a trend toward reducing the use of mercury or even banning
mercury-containing products in some countries, thus dental resin composites remain a
main interest of dental material research (Rasines Alcaraz et al., 2014).
7.2
General composition
Resin composites consist of three main components which are the resin matrix
(organic part), the inorganic fillers (inorganic part), and the coupling agent. The
resin matrix includes the monomers, initiators, inhibitors, pigments, and modifiers.
7.2.1 The resin matrix
The monomer systems are considered as the primary foundation of the composite
resin formulation. Bis-GMA remains to be the widely used monomer for constructing today’s composites; whether alone or in combination with urethane dimethacrylate (UDMA). Such monomers are slightly viscous and have to be mixed with low
molecular-weight diluent monomers so that a clinically workable consistency may
Figure 7.1 Evolution of dental resin composite throughout the last 65 years.
130
Advanced Dental Biomaterials
be produced upon addition of the fillers. Low molecular-weight compounds with
difunctional carbon double bonds, for example, triethylene glycol dimethacrylate
(TEGDMA), are added by the manufacturer to reduce and control the viscosity of
the composite.
In addition to the conventional dimethacrylates, composite resin matrix may contain acidic carboxylic groups. Such composites are known as compomers. The
name is derived from the terms composite and glass ionomer. Self-adhesive composite resin cements is another group of acidic monomers containing composites.
Resin cements are formed by a combination of usually dimethacrylate monomers
and acid-functionalized monomers, such as methacryloyloxydecyl dihydrogen phosphate (MDP), glycerol phosphate-dimethacrylate (GPDM), or dipentaerythritol
Penta acrylate phosphate (PENTA). Another category of resin composites is those
containing anionically ring-opening polymerizable cycloaliphatic epoxides. The
term “silorane” was introduced to represent such composites whose monomer systems include both siloxane and oxirane structural units. The main advantage of
these resins is the reduced polymerization shrinkage. Attempts to modify and
improve the properties of resin composite matrix (Fig. 7.2) will be discussed later
in Section 7.6 (Baroudi and Rodrigues, 2015).
7.2.2 Fillers
Inorganic fillers represent the dispersed phase of resin-based composites whose
nature plays a significant role in determining their physical and mechanical properties. Fillers vary according to their chemistry, shape, and size; such variations are
reflected in the properties of composites. Inorganic fillers are generally added to
enhance the strength and modulus of the organic resin matrix. However fillers also
reduce the thermal expansion coefficient, water sorption, and polymerization
shrinkage, as well as imparting radiopacity and enhancing the esthetic properties.
Silicon dioxide was the first filler used in dental resin composites. It is termed
silica, or quartz when present in its crystalline form. It is also considered the basis
for other types of glass fillers that are formed of different silicate compounds.
Silica has a refractive index which is lower than that of the traditional BisGMA/TEGDMA resin matrix, making it more opaque than other fillers used in
such a resin system. Alkaline glass fillers are also used in many of the currently
available commercial composites such as TetricEvoCeram (IvoclarVivadent,
Liechtenstein), Grandio (Voco, Germany), Esthet-X (Dentsply Caulk, United
States), and Herculite XRV (Kerr, United States). They are composed mainly of
silion dioxide, however they contain a fraction of alkaline oxides such as barium
oxide (BaO) and strontium oxide (SrO), which incorporate into the silica network
causing interruption of the structure. The main advantage of this material, however,
is the inclusion of heavier elements into the filler imparting radiopacity of the material without needing to add separate radiopacity agents, such as ytterbium or yttrium
fluoride. Another important advantage of such particles is superior optical properties since they have a refractive index higher than silica, making it closer to that of
traditional resin matrix, producing more transparent composites. Many forms of
Resin-based dental composites for tooth filling
131
Figure 7.2 Chemical structure of different resin systems used in dental resin composite.
alkaline glasses have been used, including barium borosilicates, barium aluminosilicates, barium aluminum borosilicates, and strontium silicates (Habib et al., 2015).
Other glasses fillers containing calcium, sodium, or phosphorus oxides have also
been tested as fillers in resin composites. Such glasses are known as bioactive glass.
The aim of using such fillers is producing what is known as smart composites that
help in the remineralization of the tooth structure. Smart composites and other composite fillers modification will be discussed in Section 7.6.1.2.
7.2.2.1 Filler size and filler loading
Increasing the filler loading enhances the properties related to them, such as high
mechanical properties, low polymerization shrinkage, and better esthetics. Filler
sizes distribution is used to maximize the filler loading, where smaller particles fill
the spaces between the larger fillers. This reduces the void space between the larger
fillers and yields higher filler loading.
132
Advanced Dental Biomaterials
Using small particles also improve esthetics and polishability of the resin composite restoration. Filler sizes larger than the visible light wavelength were found to
cause light scattering. Such scattering enhances opacity and produces a rough surface when the fillers are exposed at the resin composite surface. Surface roughness
of the resin composite restoration causes accumulation of food debris, stains, and
dental plaque.
It should be considered that the smaller the filler particle size the higher the surface/volume ratio present to form hydrogen bonding with the resin matrix. This
increases the viscosity of the resin composite and in turn its resistance to mixing
and manipulation. Thus the smaller the fillers size the less the filler fraction that
can be added.
7.2.2.2 Prepolymerized filler particles
These specialized fillers are produced by adding very high concentrations of inorganic micro- or nanofillers to a resin monomer under high heat and pressure. Once
polymerized, the resultant blocks are ground into macrosized filler particles, with
size ranging from 30 to 65 μm. The resin composite material is made up by adding
a combination of these larger macrosized filler particles and individual microfillers
in a quantity of uncured monomer. This dramatically minimizes the amount of
uncured monomer, thus decreasing polymerization shrinkage (Fig. 7.3).
7.2.2.3 Nanofilled resin composite
Nanofilled composites have been introduced to the dental market as a product of
nanofiller technology. They are formulated with nanomer and nanocluster filler particles. Nanomers are distinct nonagglomerated particles of 2075 nm in size, while
nanoclusters are slightly bound agglomerates of nano-sized particles (Fig. 7.4). The
mixture of nano-sized particles and nanoclusters decreases the interstitial spacing of
the filler particles, thus allowing higher filler loading, better physical properties, and
high surface polish retained for a considerable period of time. The first commercial
nanofilled resin composite (Filtek Supreme, 3M ESPE) was launched in 2002.
As for nanohybrid composites, they contain large-sized fillers (0.45 μm)
together with nanometer-sized fillers. They are considered hybrid composites rather
than true nanofilled composites (Ferracane, 2011).
Figure 7.3 Diagrammatic representation of prepolymerized fillers fabrication.
Resin-based dental composites for tooth filling
133
Figure 7.4 Schematic diagram for nanofillers and nanoclusters.
Source: Courtesy 3M ESPE.
There are several aims behind incorporating nanofillers in dental composites. First,
the size of nanofillers is less than the wavelength of visible light (400800 nm),
which provides the ability to develop highly translucent resin composites.
Using nanoparticles alone to form highly filled composites will result in poor rheological properties (high viscosity). In order to overcome such problem nanoclusters
were designed. The nanoclusters are made of lightly sintered nanomers. The clusters
allow having a wide size distribution varying from 100 nm to submicron.
Nanofilled composites have mechanical strength similar to that of microhybrid
composites, and at the same time retain a high surface finish like microfilled composites. In the nanofilled composite, the nanoclusters shear at a similar rate as the
resin matrix during wear process, thus maintaining a long-term polished surface
(Ferracane, 2011).
7.2.2.4 Fiber-reinforced composites
The wide use of fiber-reinforced polymers in many industrial fields encouraged the
investigation of such materials in dental composites. Glass fibers are the most commonly used fibers in dental composites due to their low cost as well as their chemical composition and refractive index that are nearly similar to that of the silica
fillers. Glass fibers also showed good adhesion to the resin matrix when treated
with silane coupling agents. Electrical or E-glass fibers are those most commonly
used in dental composites; they are characterized by their high strength and high
electrical resistivity.
Different types of polymeric fibers were also investigated to improve the overall
properties of the composites, such as polyethylene fibers and aramid fibers. Aramid
fibers significantly increased the strength properties of resin-based composites;
however, the yellow color of these fibers affected the esthetic appearance, limiting
their use in resin-based composites. The incorporation of polyethylene fibers generally enhanced the mechanical properties of the resin composites; however, their low
surface energy and poor adhesion of the resin matrix limited their reinforcing effect.
Plasma etching was an attempt to improve the wetting of these fibers and their
mechanical interlocking with the resin matrix.
Various kinds of nanotubes have been also investigated as reinforcements for
dental resin composites. Carbon nanotubes were the most commonly used. The
134
Advanced Dental Biomaterials
addition of small percentages of these carbon nanotubes to a commercial composite
increased the flexural strength by 23%. Double-walled halloysite nanotubes were
also explored to reinforce unfilled and glass-filled dental resin composites. The
addition 12.5 wt.% of halloysite nanotubes showed a twofold increase in the fracture resistance of these composites; however, it produced a slight increase in the
flexural strength. More rigid whiskers were also attempted. These whiskers
included ceramics, carbides, zinc oxide, zirconia/silica, silicon nitride, and silicon
carbide. Whiskers fused with silica nanoparticles were also tried as resin composite
fillers. These silica-fused whiskers showed 33% decrease in wear and a twofold
increase in flexural strength compared to the control (Nayar et al., 2015; Khan
et al., 2015).
7.2.3 Silane coupling agent
Surface treatment of the resin composites’ filler particles with silane coupling agents
is essential to maintain a strong and durable bond between the polymer matrix and
the filler particles. Silanized fillers were shown to enhance tensile strength and tensile
bond strength of resin composites compared to nonsilanized filler particles.
Filler particles showed improved wettability and dispersion within the resin
matrix thus improving the physical and mechanical properties of resin composites.
The water uptake by silanized filler particles was also found to be significantly
lower than nonsilanized filler particles.
The chemical formulation of organofunctional silanes is as below:
XUUUSiUUUðORÞ3
where X is an organofunctional (methoxy) group and R is a hydrolyzable alkyl
group. The alkyl group is hydrolyzed to silanol to react with the fillers’ mineral surface, on the other hand the organofunctional group copolymerizes with the resin
matrix. Dental silane products are based on 3-methacryloxypropyltrimethoxy silane,
an organofunctional trialkoxysilane which reacts via its alkoxysilane groups with
the filler and itself, and with the resin matrix via its methacrylate functional group.
An important factor affecting the efficiency of the silanation process is the thickness of the silane film. The closest monolayer to the filler surface chemically bonds
to this surface. As the silane thickness increases, its layers become more disorganized and physicosorbed on the surface of the fillers increasing the risk of weak
bond formation. A critical thickness of the silane layers is thus required, which is
controlled by the quantity of silane used.
7.2.4 Initiatoraccelerator system
The function of the initiatoraccelerator system is to polymerize and cross-link the
composite resin into a hardened form. The polymerization reaction can be triggered
by light (light-cured), chemicals (self-cured, auto-cured), or both chemical and
light-curing (dual-cured).
Resin-based dental composites for tooth filling
135
7.2.4.1 Self-cured composites
They are formed of a catalyst paste containing benzoylperoxide (BPO) initiator and a
base paste containing an aromatic tertiary amine, commonly N,N-dimethyl-p-toluidine.
Such tertiary amine (TA) is required to induce the decomposition of BPO at an ambient
temperature.
7.2.4.2 Light-cured composites
They are supplied as a single paste whose setting is triggered by visible light. Such
resin composites materials must be protected from premature curing when stored in
the dental office. They are packaged in opaque, plastic syringes or unit-dose capsules, known as compules.
Photoinitiators
The most widely used photoinitiator in light-cured resin composites is a combination of camphorquinone (CQ) with TAs. When CQ absorbs the light, it interacts
with the TAs forming a photoexcited complex with free radicals on both CQ and
TAs. The free radicals attack the CQC bonds of monomers, forming new radicals
with a longer polymer chain (propagation step). Such propagation of the polymer
chain continues until the reaction process terminates. The peak sensitivity of CQ is
near 470 nm in the blue wavelength range (Fig. 7.5). Although CQ initiator systems
have good acceptance, the yellow-colored CQ may adversely affect the composite
color. Another major problem of CQ, is that its peak absorption is within the visible
range, causing its photopolymerization under ambient light (fluorescent lamps and
dental lamps) and giving a short working time. Other initiators are now incorporated in resin composites, as an attempt to solve the problems of CQ/TA, such as
phenyl-propanedione (PPD) and diphenyl (2,4,6-trimethylbenzoyl) phosphine oxide
(TPO).
Figure 7.5 Free radical formation by light activation of camphorquinone.
136
Advanced Dental Biomaterials
Lucirin—TPO (2,4,6-trimethylbenzoyldiphenylphosphine oxide) and phenylpropanedione photoinitiator systems TPO is an acyl phosphine oxide, that
when cured with halogen or polywave light control units (LCUs), TPO results in
higher degree of conversion (DC) than CQ/TA. TPO is especially useful for the
extra white shades of resin composites needed in bleached teeth since it gets rid of
the unwanted yellow effect of CQ/TA. Its absorption spectrum ranges from 380 to
nearly 425 nm. PPD is also a photoinitiator that tends to reduce the yellowing effect
caused by CQ, its absorption spectrum is from below 350 to nearly 490 nm.
7.2.4.3 Dual-cured composite
They are formed of two pastes (base paste and catalyst paste) similar to that of selfcured composites, however their base paste contains the CQ/TA photoinitiation system required for visible light activation. An aromatic TA is also present in the base
paste for chemical polymerization. When the two pastes are mixed together, they
set up very slowly via the chemical-cured mechanism. The curing rate then speeds
up on “command” via light-curing. The main advantage of this system is the guarantee of complete polymerization, even if the light-cure is insufficient. The major
drawback is the porosity caused by the mixing of the two pastes; however, this
problem has been solved to a great extent via the use of mixing syringes. Most
resin-based luting cements or core materials are dual-cured, combining both lightand chemical-cure mechanisms (Santini et al., 2013; Kwon et al., 2012).
7.2.5 Pigments and other components
Inorganic oxides are added in small percentages to provide shades that match the
majority of tooth shades. Iron oxide represents the most common pigment. Numerous
shades are supplied at present extending from very light shades to yellow and gray.
Fluorescent agents are also provided to simulate the appearance of natural teeth.
These are dyes or pigments that absorb light in the ultraviolet and violet region
(usually 340370 nm) and re-emit it in the blue region (typically 420470 nm).
7.3
Classification of resin composites
7.3.1 According to the fillers size and distribution
Resin-based composites can be divided into fiber-reinforced composites (FRC) and
particulate filler composites. FRCs can be further categorized into long-fiber and
short-fiber composites based on the fiber length. Fiber orientation is another classification into which resin composites can be further classified with continuous unidirectional and bidirectional fibers.
Regarding the particulate filler composites, a beneficial method of classifying
dental resin composites is by the particle size and the particle-size distribution
(Fig. 7.6 and Table 7.1).
Resin-based dental composites for tooth filling
137
Figure 7.6 Classification of resin composites based on filler size, shape, and distribution.
Table 7.1 Classification of resin composites based on particle size and particle-size
distribution.
Type of composite
Filler size
Conventional (large
fillers)
Hybrid (large
fillers)
Small/fine filled
Midfilled
Hybrid (midfilled)
Minifilled
Hybrid (minifilled)
Homogeneous
microfilled
Heterogeneous
microfilled
Nanofilled
composites
Nanohybrid
150-μm silica or glass fillers
A combination of 120 μm glass fillers and 40 nm silica fillers
0.110 μm
110 μm
A combination of 0.110 μm glass fillers and 40 nm silica fillers
0.11 μm
A combination of 0.12 μm glass fillers and 40 nm silica fillers
40-nm silica
A combination of 40-nm silica particles together with
prepolymerized resin particles containing 40-nm silica
,100-nm silica or zirconia nanoparticles together with
nanoclusters
A combination of 0.12-μm glass or prepolymerized resin
microparticles together with # 100-nm nanoparticles
7.3.2 According to the composite consistency
Composite materials could also be classified according to their consistency into
flowable and packable composites. Flowable composites are designed to be dispensed from very fine bore syringes into limited spaces providing better adaptation.
Reducing the filler content and/or addition of other modifying agents, such as surfactants, are the main methods used to reduce consistency of flowable composites.
Large reduction in filler content should be avoided as it would significantly reduce
138
Advanced Dental Biomaterials
the mechanical properties and increase the polymerization shrinkage of flowable
composites.
Packable composites are designed to provide adequate resistance to condensation
in order to avoid slumping and allow the formation of tight interproximal contacts.
Packable composites develop their thicker consistency through modification in filler
size distributions or the addition of other types of fillers, such as fibers, but not
through increasing the filler loading (Lutz et al., 1983).
7.3.3 According to the packing (placement) technique
Based on the packing technique resin composites may be also classified into incremental and bulk-packed composite. Polymerization shrinkage, as well as the limited
curing depth makes it generally recommended to place composite resin in 2 mm
increments or less. Incremental placement however may be accompanied with
porosity and voids especially within large posterior composite restorations. In order
to simplify and speed up the placement of large posterior RBCs, manufacturers
have produced resin composite materials that can be placed as single thick increments (4 mm or more). Such resin composites are known as bulk-fill RBCs.
7.3.4 According to the curing techniques
Resin composites may be further classified according to the curing techniques into
light-cured, chemical-cured, and dual-cured composites (previously mentioned in
Section 7.2.4).
Resin composites can be categorized into direct and indirect resin composites.
Recent direct composite resins show superior optical and mechanical properties,
however their use in larger posterior restorations is still a challenge since polymerization shrinkage exists as a problem in cavities with high C-factor. Indirect composites are fabricated on a die and additionally cured extraorally using combinations
of light, pressure, and heat to increase the degree of polymerization, mechanical
properties, wear resistance, and also lessen the polymerization shrinkage. Such indirect restorations are bonded using resin cements (Kwon et al., 2012).
7.4
Clinical indications of resin composites
Resin-based composite restorations are widely used in the dental field. The clinical
indications of each type of resin composite are dictated by the amount of stresses
applied on the restoration as well as the esthetic requirements.
Regarding high stress bearing areas requiring adequate polishability (classes I,
II, III, IV), either hybrid large fillers or hybrid midifil resin composites are used. As
for moderate stress bearing areas requiring optimal polishability (classes III, IV),
hybrid minifilled and nanohybrid composites are indicated. For low stress and subgingival areas that require high luster and polishability, microfilled resin composite
Resin-based dental composites for tooth filling
139
is the choice. Nanofilled composites are used as anterior restorations that require
high translucency and surface finish
Packable composites are indicated in situations where good condensability is
required (classes I, II). On the other hand flowable composites are required where
improved flow is needed in areas of limited accessibility (class II) (Hervas-Garcia
et al., 2006).
7.5
Properties and limitations
7.5.1 Degree of conversion
Properly cured resin is considered the principle factor for a successful resin-based
restoration. This is accomplished mainly by having an adequate DC, which is presented by the percentage of carboncarbon double bonds (CQC) that are transformed to carboncarbon single bonds (CaC).
DC for dimethacrylate polymers ranges between 43% and 75%. A high DC is
essential to improve the physical, mechanical, and biological properties of the
resin-based composites. Several factors affect the degree of polymerization of resin
composites (Braden, 1974).
7.5.1.1 Effect of resin shade
Various shades and translucencies of resin composites are available to allow better
matching with adjacent tooth structures, thus improving the esthetic appearance of
the restoration. Resin composites with darker and more opaque shades prevent adequate light transmission and thus will have a lesser DC.
7.5.1.2 Effect of resin increment thickness
Placement of resin composites in more than 2 mm increment thickness causes significant reduction in DC. This is due to the limited curing depth of light-curing
units since they do not exceed 2 mm. Bulk-fill composites however permits resin
composite placement in increments up to 4 mm while preserving an adequate DC.
This is due to higher translucency of bulk-fill RBC that allows more light transmission compared to conventional resin composites.
7.5.1.3 Effect of light-curing system
Quartz Tungsten Halogen (QTH) is formed of a quartz bulb containing halogen,
iodine, or bromine gas, and a tungsten filament. Light is produced when electric
current passes through the tungsten filament. The light emitted is a white light with
a wavelength of broad spectrum.
Light is filtered by a filter present inside the LCU to eliminate the ineffective
wavelengths. Filtered light has a wavelength of 400500 nm, which is compatible
with CQ, the most commonly used photoinitiator. A major disadvantage of the
140
Advanced Dental Biomaterials
QTH LCU is that the useless light produced by the bulb results in an elevated operating temperature, reducing the lifetime of the bulb (to 100 hours). Fans are essential to reduce such elevated temperature.
The light-emitting diode (LED) is the latest light-curing unit submitted to the dental market. LED technology uses junctions of doped semiconductors rather than a
bulb to produce light. The light emitted has a narrower spectrum with less heat generation than a QTH LCU, but is within the range of CQ. Filters and fans are therefore,
not required in LED LCUs. A LED light unit has a life span of about 10,000 hours.
Newly introduced LED LCUs emit lights with two or more wavelength ranges
(polywave LED LCUs). They produce both a shorter violet wavelength and a longer
blue wavelength. Violet light activates photoinitiators sensitive to light within the
range of 350420 nm wavelength while blue light activates photoinitiators (mainly
CQ), with maximum absorbance near 468 nm. These polywave LED LCUs are the
method of choice to activate a broader range of photoinitiators (Santini, 2010).
7.5.1.4 Effect of light-curing tip distance from RBC surface
A decrease in radiant exposure of the light occurs on increasing the curing distance
between the composite surface and the light cure. This reduction is due to cusp
height and cavity depth, thus causing the curing tip to be at a distance from the
cured resin composite. The distance from the light-curing tip and the gingival floor
of a proximal box in deep Class II RBC restorations may reach 6 mm or more; a
50% reduction of light irradiance was reported by increasing the curing distance
from 0 to 6 mm.
7.5.1.5 Effect of cavity location
The location of some resin-based restorations, such as on the buccal or lingual surfaces
of the second molar, makes it impossible to position the LCU tip directly and at 90
over the RBC restoration surface. This can affect the DC of the cured RBC increment.
7.5.1.6 Effect of light-curing duration
For a 2-mm resin composite increment to have adequate polymerization, it should
receive a radiant exposure within the range of 1624 J/cm2. This energy (E) is determined by multiplying the irradiance level (I) coming from the LCU (mW/cm2) by its
duration (T). A longer curing time is thus needed when the irradiance level is lower.
7.5.2 Polymerization shrinkage and polymerization shrinkage
stresses
Polymerization shrinkage is one of the main drawbacks of resin-based composite
restorations. During polymerization the conversion of monomer molecules into a
closely packed polymer network results in volumetric shrinkage. Polymerization of
dimethacrylate-based composites is associated with approximately 2%6% volumetric shrinkage (Braga et al., 2005).
Resin-based dental composites for tooth filling
141
Figure 7.7 Consequences of polymerization shrinkage stress.
7.5.2.1 Polymerization shrinkage stress
Resin composite strain is constrained by the bonding of the material to the tooth
structure, as a result shrinkage expresses itself as stress. The resulting built-up stresses may lead to marginal leakage, cuspal deflection, and cracking of enamel. This
causes restoration fracture and secondary caries leading to clinical failure of the restoration (Fig. 7.7).
7.5.2.2 Factors affecting polymerization shrinkage stresses in
dental composites
Volumetric shrinkage
The amount of composite volumetric shrinkage is determined by its filler content,
DC, and monomer composition of the resin matrix. This could be explained by the
fact that the amount of polymer matrix decreases by increasing the filler fraction
and hence reducing the amount of volumetric shrinkage.
Monomer chemistry may obviously affect the developed volumetric shrinkage.
Higher TEGDMA/Bis-GMA ratios result in higher stress values due to increased
volumetric shrinkage, as a result of enhanced conversion. Diluents monomers such
as TEGDMA have lower molecular weight than Bis-GMA, thus they increase the
amount of polymerizable carbon double bonds leading to more shrinkage.
142
Advanced Dental Biomaterials
Several modifications have been made in the monomer systems of resin composite
materials to decrease the polymerization shrinkage. Various low-shrinkage dental
composites have been commercially marketed (discussed in Section 7.6.1.1).
Viscoelastic behavior and polymerization kinetics
Resin composites are solids with a unique viscoelastic behavior. They are characterized by their ability to flow at early polymerization stages followed by an increased
elastic modulus on further polymerization.
At the start of the polymerization reaction, composite resin is in aplastic viscous
form allowing it to flow. This stage is known as the pre-gel stage, during which the
resin monomers can still move or “slip” within the organic matrix. Larger molecules are formed as the polymerization process proceeds and the composite hardens
into a solid form. At a certain point no further monomer movement is possible;
such point is known as the gel point. It denotes the transition of resin composites
from the pre-gel to post-gel stage. Within the post-gel stage resin composites experience and increase in the elastic modulus, but are still contracting due to further
polymerization. Such polymerization shrinkage with an increased elastic modulus
and minimal monomer slippage causes stresses to develop. The most rigid material
(the material having the highest elastic modulus) will result in the highest stress.
C-factor and substrate compliance
Since composite shrinkage strain is limited by its bonding to the cavity walls, two
factors must be considered. The first factor is the amount of confinement exploited
on the material, which is calculated by the percentage of composite surface bonded
to the substrate in relation to the total surface area. This ratio is known as the “cavity configuration factor” (C-factor). It is defined as the ratio between bonded and
unbonded surfaces of the composite sample.
The second factor is the bonding substrate’s compliance. The substrate’s compliance refers to the degree of stiffness of the substrate walls. Using a near-zero compliance system during testing and higher C-factors are usually related to higher
stress values.
Water sorption
Water sorption of resin composites and their resultant expansion might compensate
for the resin composite shrinkage. However relief caused by water sorption expansion occurs slowly in comparison to the rapid polymerization shrinkage stresses.
Although water sorption lessens polymerization shrinkage stresses, it causes a series
of negative consequences such as deterioration of mechanical properties and color
stability of resin composites.
7.5.2.3 Management of polymerization shrinkage stress
Light-curing modes
Initial light exposure at lower irradiance values was found to reduce the reaction
rate and stress development. This is due to the extended pre-gel stage that increases
the chance for resin flow before the vitrification stage.
Resin-based dental composites for tooth filling
143
The “soft-start” protocol involves an initial light exposure with lower irradiance
for a certain period of time, followed by full irradiance.
Another protocol involves a few seconds initial exposure with reduced light irradiance followed a waiting period without irradiance then full light irradiance later.
Such protocol is known as “pulse-delay.”
Such alternative light-curing protocols may not profoundly influence the shrinkage stresses and the final properties of the hardened composite resin. This may be
due to that: (1) most shrinkage stress is developed during the post-gel stage; (2)
soft-start irradiation procedures may result in reduced DC levels, which in turn lead
to decreased cross-link density, thus adversely affecting the properties of resin composites in terms of solubility and elastic modulus (Santini, 2010).
Incremental layering technique
Incremental layering of resin composites has been highly recommended as it
reduces the effects of shrinkage stresses caused by high C-factor, thus enhancing
the bond strength and reducing interfacial microleakage, cuspal deflection, and
postoperative pain. Despite the importance of incremental placement of light-cured
resin composites to achieve adequate light penetration and maximum depth of cure,
it may lead to void entrapment between layers, as well as increased chair time.
Low elastic modulus liners
Flowable composites have an elastic modulus 20%30% less than conventional
hybrid composites. According to the “elastic cavity wall concept,” the shrinkage
stress generated by a higher modulus resin composite can be absorbed by an elastic
intermediate layer of flowable composite. This is claimed to help in lessening the
stress at the toothrestoration interface displayed clinically as a reduction in cuspal
deflection.
Lower shrinkage stress monomer chemistry
The evolution of low-volumetric shrinkage monomers such as Silorane or DX-511
has not necessarily led to a similar decrease in shrinkage stresses. This has provoked the development of “lower contraction stress” monomers such as SureFil
SDR flow and another novel low-shrinkage stress monomer TCD-DI-HEA (bis
(acryloyloxymethyl)tricyclo[5.2.1.02,6]decane), which is found, for example, in
Venus Diamond Nanohybrid Composite (Heraeus Kulzer). This will be discussed
later in detail (Section 7.6.1.1).
Preheating
Preheating of resin composites has been presented as a technique used to increase
composite flow, marginal adaptation, and monomer conversion.
Higher resin composite temperature reduces system viscosity and enhances radical mobility, resulting in additional polymerization and higher conversion before
the vitrification point, decreasing the magnitude of stress. This technique will be
discussed in detail in Section 7.6.2.2.
144
Advanced Dental Biomaterials
7.5.3 Physical properties
7.5.3.1 Thermal properties
In general, the linear coefficient of the thermal expansion (α) values for composites
are less than the mean of its components (fillers and matrix) summed together;
however, the values exceed those for dentin and enamel. The α of fine composites
is less than that of microfilled composites. Higher values for microfilled composites
are mainly due to the greater amount of polymer matrices.
Thermal stresses place an extra strain on the interfacial bonding between the restoration and tooth structure, which adds to the damaging effect of the polymerization shrinkage. During cyclic application of either hot or cold stimuli, the high
difference between the thermal coefficient of expansion of composites and teeth
may cause percolation of oral fluids and early bond failure.
The thermal conductivity of fine composites is greater than that of microfilled
composites because of the higher filler loading of fine composites. Inorganic fillers
have higher thermal conductivity compared to the polymer matrix.
7.5.3.2 Solubility
Inadequate light-curing intensity and duration may lead to insufficient polymerization, especially within the deeper increments. Improperly polymerized composites
have greater water sorption and solubility, displayed clinically as early discoloration. Water storage of resin composites may lead to the breakdown of interfacial
bonding between the fillers and resin matrix accompanied by the leaching of inorganic ions. During the first 30 days of storage in water, silicon leaches in the highest quantity (1517 μg/mL) but decreases later with time. Barium, boron, and
strontium, which are present in glass fillers, also leach out to various degrees. Wear
and abrasion of composites are mainly caused by the breakdown of the fillers/
matrix bonding (Braden, 1974).
7.5.4 Esthetic properties
Esthetic restoration of anterior teeth is quite challenging as it mandates dealing with
optically complex natural tooth structure with variation in optical behavior among
enamel, dentine, and pulp. Enamel is translucent with approximately 70% light transmission, whereas dentine is opaque with 52% light transmission (Franco et al., 2007).
An impeccable esthetic outcome with resin composite depends on different factors
related to both technique and materials. Regarding techniques, esthetic restoration is
influenced by shade mapping, meticulous isolation, design of teeth preparation, proper
bonding protocol, as well as anatomical shaping and contouring to mimic natural
teeth. The execution of perfect esthetic restoration is dependent on various materialrelated factors, such as available shades, fluorescence, translucency, chameleon effect,
polishability, wear resistance, and gloss retention (Nahsan et al., 2012).
Resin composite translucency and color are related to compositional structure
and formulation, including pigments and opacifiers, filler size and loading, the
Resin-based dental composites for tooth filling
145
mismatch in refractive index between fillers and matrix, and photoinitiator system,
as well as resin type and its curing quality (Mikhail and Johnston, 2014).
Early brands of resin composite offered only single body translucency with different Vita shades, whereas later on manufacturers produced composite kits with
variable translucencies (enamel, body, dentine) in addition to characterization stains
and special effects (transparent incisal, opalescent halo, white spots). It should be
usually considered that understanding the optical properties is more important than
having several commercial kits in order to select the appropriate composite resin
(Nahsan et al., 2012).
Surface smoothness and high gloss improve the natural appearance of the final
restoration. Surface smoothness is influenced by the filler size and finishing and
polishing protocol. It is believed that resin with smaller fillers (microfilled and
nanofilled) produces a smoother surface and greater luster compared to large particles (microhybrid). Recently, systematic review of influence of filler size on the
surface finish of composite revealed that there is no in vitro evidence for superiority
of submicron or nanofilled composites over microhybrid with regard to surface
smoothness and gloss retention (Kaizer et al., 2014).
Regarding the esthetics of a posterior composite, it is mainly dependent on
proper bonding and adaptation with the cavity margin with proper anatomical
reconstruction.
7.5.5 Mechanical properties
Advancements in dental resin composites over the years have focused on the
enhancement of the mechanical properties. Generally, current dental resin composites show satisfactory mechanical behavior to be used in most of the clinical restorative procedures. Concern regarding placement of resin composite in high stress
situations still exists. This concern is justified as one of the main reasons for composite failures is fracture. Composite mechanical properties rely mainly on the filler
loading (percentage, distribution, size and type of fillers) and bonding between
fillers and matrix. Generally, the higher the filler loading the higher the strength,
stiffness, and toughness.
There is considerable data in literature showing great variability in mechanical
properties of dental resin composite commercial products even within the same category (Ferracane, 2011; Ilie and Hickel, 2009). So it is difficult to predict mechanical performance of a dental composite from its category alone. But generally the
in vitro mechanical evaluation is essential as a primary screening and prediction of
clinical performance and durability. Guidelines for mechanical evaluation and its
correlation to clinical outcomes will be discussed later in this chapter (Table 7.2).
7.5.6 Biocompatibility
Biocompatibility considerations for resin composite include cytotoxicity and
allergic reactions for both patient and dentist. Several factors affect the biocompatibility of composite restoration such as composition (type of resin, fillers,
146
Advanced Dental Biomaterials
Table 7.2 List of mechanical properties for various resin composite categories.
Material type
Flexural
strength
(MPa)
Flexural
modulus
(GPa)
Diametral
tensile strength
(MPa)
Compressive
strength
(MPa)
Hybrid
composites
Packable
composites
Ormocer-based
composites
Nanohybrid
composites
Compomers
Flowable
compomers
Flowable
composites
Microfilled
composites
116.6 ( 6 23.9)
7.3 ( 6 2.3)
32.5 ( 6 8.0)
79.0 ( 6 3.2)
105.9 ( 6 28.1)
8.4 ( 6 2.5)
34.3 ( 6 8.8)
80.3 ( 6 3.5)
104.3 ( 6 21.6)
7.5 ( 6 2.4)
35.2 ( 6 9.5)
77.0 (0)
103.1 ( 6 19)
5.0 ( 6 0.8)
40.5 ( 6 8.3)
78.4 ( 6 2.5)
94.7 ( 6 34)
89.1 ( 6 25.2)
9.2 ( 6 1.9)
4.2 ( 6 1.1)
33.9 ( 6 9.4)
33.5 ( 6 8.3)
74.9 ( 6 5.6)
64.4 ( 6 4.1)
99.8 ( 6 27.4)
4.4 ( 6 1.6)
38.3 ( 6 10)
66.1 ( 6 4.3)
73.5 ( 6 10.9)
3.8 ( 6 0.8)
24.2 ( 6 3.8)
60.7 ( 6 4.0)
Source: Adapted from Ilie, N., Hickel, R., 2009. Investigations on mechanical behaviour of dental composites. Clin.
Oral Investig. 13, 427438.
bonding between matrix and fillers, and initiator system), method and quality of
polymerization, as well as proper manipulation (cavity management, proper
restorative technique, finishing and polishing). As biocompatibility concerns
regarding composite are highly dependent on how much the composite leaches,
so the compositional factor and high quality polymerization can be considered
the key factors for reducing any harmful effects from composite restorations
(Mallineni et al., 2013).
Laboratory evaluation of freshly set methacrylate resins shows moderate cytotoxicity on directly exposed cultured cells over 2472 hours, however recent types
of resins cause minimal cytotoxicity with higher quality polymerization and less
leachants. The cytotoxicity is significantly reduced within 2448 hours after polymerization and significantly diminished by the presence of a dentine barrier.
Generally, properly light-cured resins are less cytotoxic compared to chemically
cured resins. DC of light-cured resins was found to range from 55%75% and can
be increased up to 80% with further postcuring (Mallineni et al., 2013).
In vivo usage tests revealed low to moderate pulpal inflammation after 3 days
with about 0.5 remaining dentine thickness. Within 58 weeks, the reaction
diminishes and reparative dentine formation was observed. Pulpal inflammatory
response was minimal with use of protective liner or stable bonding agent. Polished
composites show significantly less cytotoxic effect in laboratory testing. Also, the
extent of the restoration especially its surface area is considered one of the factors
that can affect the leaching procedure clinically (Mallineni et al., 2013).
Resin-based dental composites for tooth filling
147
In addition to short-term leaching, resin composite is susceptible to the combined
effect of mechanical, hydrolytic, and enzymatic degradation leading to long-term
elution of degradation products with varying extent. This long-term elution is considered of more biological significance, as it theoretically occurs throughout the service life of the restorations (Bakopoulou et al., 2009).
Controversy about estrogen-like response (xenoestrogenic effect) of residual BisGMA resin has been raised. It was found that Bis-GMA can cause xenoestrogenic
effect in vitro. However, there is no clinical evidence for an estrogen-like effect of
any current commercial products (Mallineni et al., 2013).
7.5.7 Degradation
As mentioned previously, degradation over time can caused elution of different products from resin composite. Resin degradation may be caused by different stimuli,
such as thermal, photocatalytic, and/or chemical effects.
For example, it has been found that biologically derived enzymes can degrade
the monomer components of composite resins, which may then result in the liberation of methacrylic substances.
Various environmental challenges face composite restorations during service
causing significant changes due to aging and degradation. Aging-derived changes
can be due to chemical breakdown by hydrolysis and enzymatic degradation by
cholesterol esterase and pseudo-cholinesterase. Degradation also can be influenced
by the applied stresses associated with swelling of resin leading to formation of
voids and microcracks and premature failure (Drummond, 2008).
The nature and actual extent of these changes are not clear. However, degradation effects should be considered during materials evaluation and characterization
as it is not appropriate to evaluate only the initial properties. Current evidence supports the leading roles of the organic phase and the matrix/filler interface in the
degradation of strength and toughness (Lohbauer et al., 2013). Accordingly, recent
research directions have focused on development of degradation-resistant restorative materials. The recent modification and enhancement trials to develop fatigue
resistant materials will be discussed later in this chapter.
7.5.8 Clinical durability
Success and longevity of dental restorations are dependent factors related to the
material, patient (oral hygiene, masticatory forces, and abnormal habits), dentist
(skills, isolation, techniques), and cavity size and complexity. Since the introduction
of resin composite, the improvement of its clinical performance and durability has
been highly challenging, especially in stress bearing posterior restorations.
Recently, the marked improvement in composite resin materials have significantly
enhanced its clinical performance in different clinical situations.
A systematic review of different clinical trials over the last two decades has
revealed overall satisfactory success rates of posterior composite restorations. The
overall success rate between 1995 and 2005 was 89.41%,while for 200616 it was
148
Advanced Dental Biomaterials
86.87% for all studied restorations. The reported overall success rates for long-term
studies improved in the 200616 decade ranging from 64% to 96.9% compared with
the 50% to 83% for the 19952005 decade. The annual failure rate of posterior composite ranges from 1.5% to 2.4%. This trend indicates that the clinical performance
and durability of posterior composite have improved (Alvanforoush et al., 2017).
The main reasons for failure in the first 4 years of a composite restoration’s service life were fracture, marginal defects, and secondary caries. In contrast, for
restorations older than 5 years, secondary caries and fracture were the predominant
failures. There is an important shift in failure reasons from recurrent caries, wear,
and postoperative sensitivity toward mechanical failure and endodontic treatment.
This shift may be related to the increased frequency of placing composite restoration in more complex cavities (Alvanforoush et al., 2017).
According to Cochrane clinical reviews, there is low-quality evidence to suggest
that amalgam is more durable than resin composite restorations. There is insufficient evidence to support or refute any adverse effects amalgam or composite
restorations may have on patients (Rasines Alcaraz et al., 2014).
Regarding anterior composite restoration, there is proven good clinical performance with long-term follow-up periods with annual failure rates ranging from 0%
to 4.1%. Failure behavior in anterior composite restorations differs from posterior
teeth, with more restoration replacement due to esthetic reasons and less secondary
caries. However there is still the need for long-term well-designed clinical trials to
evaluate the durability and clinical performance of resin composite restorations,
especially with the rapid development of investigation techniques and the improvement of restorative and adhesive technologies (Demarco et al., 2015).
7.6
Attempts for resin composite improvement
7.6.1 Regarding material formulation
7.6.1.1 Low-shrinkage composites
Different strategies have been evolved to reduce polymerization shrinkage of resin
composites which include:
G
G
Reduction of resin matrix through addition of more fillers
Nanofilled, hybrid filler loading, prepolymerized fillers
This approach is discussed in detail earlier in Section 7.2.2
Synthesis of low-shrinking resins (Fig. 7.2)
Ring-opening polymerization (Silorane, 3M ESPE)
High molecular-weight resin (DX-511, Kalore, GC)
Low-shrinkage TCD resin (Venus diamond, HeraeusKulzer)
Dimer acidbased dimethacrylate resin (N’Durance, Septodont).
Ring-opening epoxy siloxane (Silorane)
In 2007 an interesting ring-opening monomer was introduced called Silorane (3M
ESPE), which is named for the two chemical subunits that make up the
Resin-based dental composites for tooth filling
149
molecule: siloxanes and oxiranes. Siloxanes provide an inorganic backbone of alternating silicon and oxygen atoms (SiOSiO) that has either an hydrogen or
an organic side group attached to the Si atoms. Siloxanes can be branched,
unbranched, or cyclic and are best known for imparting hydrophobic properties. In
Silorane, the siloxane backbone is cyclic and the organic side groups are oxiranes.
Oxiranes are three-member rings consisting of two carbons and one oxygen, which
is the simplest epoxide, and are members of the epoxy resin group. Polymers
formed from oxiranes are known for low-shrinkage and excellent physical properties (Pitel, 2013).
Silorane polymerizes via cationic ring-opening of the oxirane groups, leading to
very minimal overall shrinkage. According to the manufacturer, the volumetric
shrinkage obtainable with the silorane-based composite is approximately 0.9%
when evaluated by the bonded disk method, also known as the Watt’s method. This
was significant because it was the first time a commercially available direct composite has reported a shrinkage factor ,1. However, when using other generally
accepted test methods, the actual polymerization shrinkage stresses may not be significantly lower than that possible with more conventional resin-based composites
(Pitel, 2013).
Although it was a fascinating idea to have a low-shrinkage Silorane, it has several serious limitations. It was not compatible with other resins, it was extremely
hydrophobic, and it required special proprietary bonding agents. In addition, the
claimed lower shrinkage did not lead to either reduced stresses in the cavity or clinically significant superiority over conventional resins.
High molecular-weight resin (DX-511, Kalore, GC)
Limitations of the Silorane monomer have led to research focusing on developing
another strategy. Since volumetric shrinkage has been linked to molecular sites
where there is a conversion of an electrostatic van der Waals interaction to a covalent bond, it stands to reason that reducing the total number of such conversions
should effectively reduce the total volumetric shrinkage. This can be accomplished
by utilizing monomer molecules with higher molecular weights, which also typically occupy a larger volume of space. With fewer total monomer molecules to
occupy the same potential space compared to smaller monomers, there is a reduction in the number of covalent bonds formed per unit space. This will ultimately
reduce the total polymerization shrinkage and shrinkage stress.
An example of this strategy is found in Kalore (GC America, Inc.), which was
introduced in 2009. Kalore is 82% filled by weight and has a reported volumetric
shrinkage of approximately 1.7% (by mercury dilatometer). It replaces the BisGMA monomer with DX-511, a new lower shrinking monomer chemically
related to UDMA that has been developed by DuPont. Thus Kalore is able to
retain full methacrylate compatibility. DX-511 has a much higher molecular
weight (895 g/mol) than Bis-GMA (513 g/mol) and has both stiff and flexible
segments in the monomer, the latter of which reduces the monomer viscosity, permitting lower amounts of diluent monomers to be used in the formulation
(Pitel, 2013).
150
Advanced Dental Biomaterials
Dimer acidbased dimethacrylate monomer (N’Durance, Septodont)
Septodont introduced phase separating low-shrinkage dimerbased dimethacrylate
resin in N’Durance composite. The core structure of the dimer acidbased monomer is composed of both linear and cyclic aliphatic structures (Fig. 7.2). “Dimer
acid” means any of the class of cycloaliphatic carboxylic acids that are highmolecular-weight dibasic acids which are viscous liquid and can be polymerized
directly with alcohols and polyols to form polyesters. The manufacturer claims both
low-volumetric shrinkage, and high DC. The high conversion degree limits the elution of any residual monomer and thus enhances the biocompatibility of the material. The low shrinkage combined with high DC can be explained by the high
molecular weight with bulky nature of the core structure of the dimer acidbased
dimethacrylates. Also, it is claimed that phase separation occurs during polymerization leading to reduced shrinkage stresses.
Low-shrinkage TCD urethanebased monomer (Venus Diamond, Heraeus Kulzer)
Another novel low-shrinkage/stress monomer is TCD urethanebased resin, patented by Heraeus Kulzer in 2008 and introduced as Venus Diamond resin composite. The TCD monomer applies several strategies to reduce volumetric shrinkage
and shrinkage stress. First, it has a backbone similar to Bis-GMA, which helps
reduce molecular vibrations during polymerization. In addition, it lacks the polar
hydroxyl groups found in Bis-GMA. Both of these properties help reduce the intermolecular distances between monomer molecules in the uncured state. Therefore
the change between the uncured and cured states is minimized, which would help
impart lower volumetric shrinkage. TCD resin also has an elastic urethane side
chain allowing stress absorption and compensation of the volumetric shrinkage.
7.6.1.2 Smart composites
Smart materials have been promoted widely as a key technology that will underpin
all manner of novel products with unique capabilities. Indeed, in 2013, the World
Economic Forum’s Global Agenda Council on Emerging technologies identified a
class of smart materials, as one of the top 10 most promising technological trends.
Smart materials can respond by changing some properties with external stimuli
such as stress, pH, and temperature.
As secondary caries is considered one of the most common causes of resin composite failure, recent conservative emerging trends focus on the development of
smart bioactive remineralizing antibacterial resin composites. The therapeutic conservative treatment aims to improve resin durability with more tooth structure conservation. Different approaches to develop such material will be reviewed and
clarified (Maas et al., 2017) (Fig. 7.8).
Bioactive remineralizing composites
Composites containing calcium phosphate (CaP) particles are considered “smart
materials” as its ion release increases with more acidic conditions.
Different CaP phases have been inserted in dental composite as bioactive fillers
such as tetracalcium phosphate, amorphous calcium phosphate dicalcium phosphate
Resin-based dental composites for tooth filling
151
Figure 7.8 Diagram representing different types of smart resin composite.
anhydrous, and dicalcium phosphate dehydrate. It is hypothesized that the released
calcium and phosphate ions will supersaturate the surrounding environment favoring deposition and formation of hydroxyapatite.
There are several factors that influence the ion release pattern in resin composite.
The higher the surface area, volume fraction, and resin matrix hydrophilicity, the
higher the ion release. Unfortunately, the increased amount of hydrophilic CaP fillers may lead to significant weakening of the resin composite material. This weakening can be attributed to the lack of strong bonding between bioactive fillers and
resin matrix. This could be improved with surface functionalization using a silane
coupling agent but it reduced the ion release and remineralization tendency due to
silane hydrophobicity (Maas et al., 2017).
Ion release is a multifactorial process and does not occur indefinitely, so all factors should be finely tuned for tailoring a potent long-lasting remineralizing composite without deterioration of physical and mechanical properties.
152
Advanced Dental Biomaterials
Table 7.3 Different antimicrobial agents added to resin composite.
Filler modification
Nonreleased antibacterial
agents
G
G
Released antibacterial agents
G
G
G
G
Silver-supported
fillers
MDPB
SrF2
Silver ions
Silversilica glass
ZnO
Matrix modifications
G
G
G
G
G
G
G
G
G
Triclosan
QPEI
Acrylic-amine-HF salts
Methacryloyl acidfluoride
Acrylic-amine-BF3
Chlorhexidine
Benzalkonium chloride
Cetylpyridinium
chloride
Chitosan
HF, Hydrogen fluoride; MDPB, 12-Methacryloyloxydodecylpyridinium bromide; QPEI, quaternary ammonium
polyethyleneimine; SrF2, strontium fluoride; ZnO, zinc oxide.
Antibacterial composites
Resin composites have more tendency for plaque accumulation compared to other
restorative materials and intact tooth structure. This bacterial affinity is believed to
increase frequency of secondary caries around composite restorations (Ferracane,
2017).
Antibacterial composite formulations rely on modification of either matrix and/
or fillers with an antibacterial component. The antimicrobial strategies can be
divided into stationary nonreleased additives or soluble released agent (Beyth et al.,
2014) (Table 7.3).
Fluoride anticariogenic potential through its antibacterial effect and formation of
acid-resistant fluoroapatite is well documented. Accordingly, there have been different attempts to add these anticariogenic qualities to resin composite. Fluoride can
be added in the form of fluoridated silicate glass particles, such as barium-aluminofluoride glass, or addition of inorganic fluoride compounds, such as ytterbium trifluoride (YbF3), sodium fluoride (NaF), and strontium fluoride (SrF2), to the filler
system. Another approach to add a fluoride-releasing property to a composite is
incorporation of prereacted glass ionomer particles, this led to the production of a
commercial giomer called Beautifil from Shofu (Nedeljkovic et al., 2015).
Fluoride release from fillers occurs through water diffusion into the resin matrix
and exchange reaction. It is a challenging problem to achieve adequate fluoride
release over time without compromising the physical properties of composite.
Different promising approaches have been tried to overcome this challenge through
incorporation of calcium fluoride nanoparticles to filler system. Also, using organic
fluoride compounds, such as methacryloyl fluoride methyl acrylate and acrylic the
amine-HF salt in the resin matrix which have revealed promising results. However,
the leached fluoride form composite is still much lower and less effective compared
to resin-modified glass ionomer.
Resin-based dental composites for tooth filling
153
Silver is another well-known antimicrobial agent that has been used either as
a releasing or nonreleasing additive in resin composite. Silver can be added in
different forms such as a glass filler releasing silver ions, silver nanoparticles,
silver-supported apatite, and silver-supported zeolite. Two other silver carriers
incorporated in composites, silver-supported silica gel and silver-supported zirconium phosphate, showed potent contact antibacterial effect without silver ion
release. This showed potent in vitro antimicrobial effect without compromising
mechanical properties. Zinc oxide nanoparticles have been added to composite, but
they exhibited only a short-term contact inhibition of bacterial growth, without the
release of zinc ions.
Another simple approach to develop antimicrobial composites is modification of
the resin matrix with a soluble disinfectant, such as triclosan, chlorhexidine, quaternary ammonium compounds (benzalconium chloride and cetylpyridinium chloride),
biopolymer chitosan, antibiotics (vancomycin and metronidazole), and green tea
extract (epigallocatechin-3-gallate). Unfortunately, all soluble antibacterial additives
in composites showed “burst effect,” which means an initial large amount of leaching for a few days followed by a significant decrease in the remaining antimicrobial. Moreover, the antimicrobial release led to a porous structure with significant
compromise of the material’s mechanical properties. To overcome these drawbacks,
the synthesis and copolymerization of an antibacterial resin with the methacrylate
resin was extensively investigated. This would exhibit a long-term contact antibacterial effect without leaching or compromising the mechanical properties.
Methacryloyloxydodecyl pyridinium bromide is the most extensively studied antibacterial resin with highly promising results. It was incorporated as a prepolymerized resin filler. Quaternary ammonium polyethyleneimine (QPEI) is another
antibacterial monomer that has been incorporated as nanoparticles to provide a
large surface area for a potent antibacterial effect. QPEI includes for example, quaternary ammonium dimethacrylate and methacryloxylethyl-cetyldimethyl ammonium chloride (DMAE-CB). Macromolecular resins also have the advantage of
being chemically stable, nonvolatile, and sustaining long-term antibacterial potential (Cheng et al., 2017).
To develop solid evidence regarding new generations of therapeutic, bioactive,
and antimicrobial composite resins, more clinical studies are highly needed as most
of the current studies are in vitro. Nonetheless, the multidisciplinary research concerning these material categories is expected to offer tremendous benefits to oral
and dental health.
Polyacid modified composite (compomer)
In the early 1990s, compomer was introduced as a new material class trying to
combine the esthetics of resin composite with adhesion and fluoride release of glass
ionomer. It is composed of methacrylate resin (UDMA) as a traditional composite
modified with polymerizable dicarboxylic acid. The fluoroaluminum silicate glass
of glass ionomer is added in the form of glass filler embedded in the resin matrix.
There is not sufficient water for a glass ionomer acidbase reaction to occur and
compomer setting is dependent only on free radical polymerization as per
154
Advanced Dental Biomaterials
conventional composites. Surface pretreatment of tooth structure with adhesive
resins is essential for bonding as the compomer was not able to bond chemically
with the tooth structure as a glass ionomer. Fluoride release and recharge of compomer was found to be much lower than glass ionomer cement. This may be attributed
to the hydrophobic nature of the resin matrix compared to hydrophilic glass ionomer. The clinical use of compomer is limited to pediatric restoration and low stress
bearing areas in adults as its mechanical performance is much lower than conventional resin composites (Zimmerli et al., 2010).
Self-healing composites
Self-healing materials are another example of smart material that responds to
mechanical stimulus and extends its survival by restoring mechanical integrity after
damage. Self-healing composite relies on an encapsulated polymerizable solution
with reactants which are released when the capsule is ruptured by crack propagation. Then et al. (2011) described the first experimental self-healing dental resin
composite using the microcapsule technique. They made it using a synthesized
dicyclopentadiene (DCPD) capsule filled with urea formaldehyde (UF) dispersed in
Bis-GMA/UDMA/TEGDMA resin with 55 wt.% of silanated silica fillers and 2 wt.
% of catalyst. It should be noted that the presence of the capsules within the resin
may provide some benefit in terms of mechanical properties, regardless of the selfhealing effect. It revealed a significant recovery of fracture toughness without
compromising biocompatibility.
Concerns regarding the biological safety of DCPD led to the development of different experimental self-healing systems in dental composite. Microcapsules of poly
urea formaldehyde filled with TEGDMA resin and TA activator were used. This
self-healing system utilizes BPO in resin matrix to initiate polymerization of the
healing resin (Fugolin and Pfeifer, 2017).
Several recent studies using microcapsule self-healing mechanisms with various
healing resins revealed a minimum of 65% recovery of the fracture toughness with
minimal cytotoxicity (Fugolin and Pfeifer, 2017; Maas et al., 2017).
7.6.2 Regarding manipulation
7.6.2.1 Layering technique
Traditionally, direct composite restoration is recommended to be laid in 2 mm
increments for proper polymerization and reduction of shrinkage stresses.
Incremental application of composite can be placed in either horizontal or oblique successive layers. Oblique increments are placed in such a way to try to avoid
bonding of opposite walls. This technique is claimed to result in less cuspal deflection and reduced shrinkage stresses as a result of the controlled C-factor (ratio of
bonded to unbonded restoration surfaces) by bonding to single cusp with each
increment application. However, the subsequent increments will eventually bond to
opposite walls producing significant stresses. Also the C-factor concept is too simple to explain shrinkage stresses which are a multifactorial complex phenomenon.
Resin-based dental composites for tooth filling
155
Finite element stress analysis compared oblique and horizontal incremental
application of a premolar restoration and revealed that oblique increments produced
less stresses along the compositeenamel interface, and higher stresses along the
compositedentin interface. Two millimeters increment seems to produce adequate
mechanical properties with low-shrinkage stresses. It is extremely important to note
that an increased number of increments give more chance of voids and porosity.
Although there is no conclusive evidence in the literature concerning the incremental layering advantages regarding polymerization shrinkage, it is recommended
as the standard technique for composite placement, claiming dissipation of shrinkage stresses and with proper polymerization.
7.6.2.2 Composite preheating
Composite preheating before insertion in the cavity offers several advantages. It
reduces composite viscosity and allows injection molding of highly filled viscous
composite into the cavity with better adaptation, polymerization quality, and fewer
voids. This advantage allows handling of the composite like a flowable restorative
material while maintaining the superior properties of packable composites. The
warm composite shows enhanced molecular mobility leading to improved mechanical properties after curing. There was some concern regarding injecting warm composite inside the cavity with fears of pulp thermal injury. However, composite cools
immediately after placement and results in only slight temperature elevation compared to intraoral temperature. Although composite preheating requires additional
equipment (Fig. 7.9) and some training for mastering placement technique, the cost
is relatively low and the learning curve is shallow with high benefits and very limited adverse events (da Costa et al., 2011).
The most popular heating devices present on the market are Calset and
Thermaflo. Some simpler methods have been used for composite warming instead
of these devices such as hot air blower, hot water bath, and microwave oven.
Modified glass bead sterilizer and wax warmer are also promising suggested innovations especially where economic condition and availability are the major concerns to implement these techniques.
7.6.2.3 Use of lining material
As mentioned previously, polymerization shrinkage stresses are multifactorial and
elastic modulus of the composite material is one of the factors that can affect it. It
is believed that low elastic modulus materials generate less shrinkage stresses compared to rigid materials. Based on this assumption, the concept of “elastic cavity
wall” and “sandwich technique” have been evolved by placing less rigid material as
a cavity liner under composite restoration. Several studies have investigated different resilient lining materials such as thick adhesive layer, glass ionomer, resinmodified glass ionomer, or flowable composite. This approach is claimed to reduce
the polymerization shrinkage stresses with its deleterious consequences and increase
the durability and success rate of composite restoration (Soares et al., 2017).
156
Advanced Dental Biomaterials
Figure 7.9 Calset composite heating device.
Nevertheless, there is inconsistent evidence concerning the claimed advantages
of the use of lining material under composite. There is no evidence of enhanced
performance or durability when comparing restorations with and without elastic
cavity liners. Accordingly, there is no need to add cost and/or unnecessary clinical
step by placing lining material underneath composite restorations (Schenkel et al.,
2016).
7.6.3 Regarding both material formulation and manipulation
Much effort has been concentrated on developing materials that are simpler to use
by virtue of requiring fewer application steps, such as bulk-fill and self-adhesive
composites.
7.6.3.1 Self-adhesive composites
Self-adhesive flowable composites were introduced in 2009. Currently, there are
three commercially available products (Table 7.4). These materials are currently
recommended for liners and small restorations but with simplified application without separate bonding protocol pretreatment. Self-adhesive composite technology is
relevant to self-etch adhesive systems as it relies on the presence of acidic
functional monomers such as trimelitic acid methacrylate (4-MET), GPDMs, or
Resin-based dental composites for tooth filling
157
Table 7.4 Different products, manufacturers, and compositions of the commercially
available self-adhesive composites.
Product
Manufacturer
Composition
Fusio
Liquid
Dentin
Pentron Clinical,
Orange, CA,
United States
Vertise
Flow
Kerr, Orange, CA,
United States
Embrace
Wetbond
Pulpdent,
Watertown, MA,
United States
Resin: UEDMA, TEGDMA, HEMA, 4MET, catalyst
Fillers: SiO2 (65 wt.%), silanated barium
glass, NaF
Resin: GPDMA, HEMA, Bis-GMA,
catalysts
Fillers: Prepolymerized filler, silanated
barium glass, nano-sized colloidal SiO2,
YF3 (70 wt.%)
Resin: UEDMA, BMEP, TMPTMA,
HEMA, water, catalysts
Fillers: SiO2, NaF (37 wt.%)
4-MET, Trimelitic acid methacrylate; Bis-GMA, bisphenol glycidil dimethacrylate; BMEP, bis-methacryloyloxy ethyl
phosphate; GPDMA, glycerolphosphoric acid dimethacrylate; HEMA, hydroxyethyl methacrylate; TEGDMA,
triethylene glycol dimethacrylate; TMPTMA, trimethyloyl propane trimethacrylate; UEDMA, aliphatic diurethane
dimethacrylate.
bis-methacryloyloxy ethyl phosphate (BMEP), in addition to hydroxyethyl methacrylate (HEMA). These monomers vary in acidity and are responsible for partially
etching the tooth structure and penetrating through the smear layer, forming a
hybrid layer. HEMA is added to increase the wettability and allow better hybridization with the moist tooth structure. These composite formulas were designed with
the aim of getting the benefits of the advancing technology of micromechanical and
chemical bonding of the recent simplified self-etch adhesive systems (Maas et al.,
2017) (Fig. 7.10).
Under the limitations of the present studies, there is overall agreement that selfadhesive flowable composite are less efficient than conventional restorative systems
with few exceptions. This is attributed to the relative high viscosity limiting the diffusion into the tooth substrate in addition to the limited extent of decalcification.
Some researchers found that application of phosphoric acid pre-etch and/or selfetch universal adhesives increased the bond strength significantly. Unfortunately,
the different surface pretreatment deprived the self-adhesive composites of its main
advantage. Accordingly, routine application of self-adhesive flowable composites
should be carefully considered.
7.6.3.2 Bulk-fill composites
Bulk-fill resin composites have been introduced to the market in both flowable and
conventional/sculptable viscosities, with the premise of simplified application
(Fig. 7.11).
Different concerns were raised with this concept such as ensuring proper polymerization, depth of cure, adaptation of the material to cavity walls and margins, in
158
Advanced Dental Biomaterials
Figure 7.10 Chemical structure of glycerol phosphate-dimethacrylate (GPDM) resin with
acidic side chain for self-adhesive composite.
Figure 7.11 Different packing techniques comparing conventional incremental packing to
bulk-fill composite either single 4 mm increment or 4 mm base with capping composite.
addition to polymerization shrinkage and shrinkage stresses. These concerns should
be considered while tailoring the material composition and evaluating its laboratory
and clinical performance. Regarding proper polymerization and depth of cure, it has
been achieved through different approaches, which include modified initiators,
translucent fillers, and modification of resin chemistry.
Different modifications have been invented to reduce polymerization shrinkage
and its stresses. Among these approaches are high molecular-weight resins, stress
decreasing modulators, and addition fragmentation polymer, in addition to stress
absorbing fillers.
Flowable bulk-fill materials generally have lower filler loading than nonflowable, sculptable materials and require that the occlusal layer be filled with a “cap”
of a more highly filled composite that is expected to be stronger and more wear
resistant under occlusal loading (Chesterman et al., 2017).
The mechanical properties, esthetic outcomes, and placement techniques vary
significantly between the available bulk-fill composite materials. Bulk-fill materials
are highly beneficial in the restoration of posterior teeth with difficult patient control and limited time available at present, for example, in children, anxious patients,
and large posterior cavities.
Overall there are early promising in vitro studies supporting the use of bulk-fill
composites which confirm the manufacturer’s claims. However, there is very little
clinical research on the long-term outcomes of these materials. Such evidence is
Resin-based dental composites for tooth filling
159
highly necessary before the real effectiveness of these materials can be confirmed.
Until further data are available, it is recommended that clinicians carefully select
materials and strictly follow the current recommendations in application
(Table 7.5).
Indirect composite
There are three main restorative techniques available, namely direct, indirect, and
semidirect. Indirect technique allows better control and easier restoration of occlusal anatomy and proximal contours. In addition, it is expected to provide better margins due to the limitation of the polymerization shrinkage stresses into the confined
thin layer of the resin cement. Moreover, the highly controlled polymerization and
sometimes combination of different polymerization protocols produces restorations
with better polymerization quality and hence improved physical and mechanical
properties. However, conventional indirect technique requires two visits, additional
clinical steps as recording impression, provisional restoration fabrication, and laboratory contribution, leading to increased time and cost (Alharbi et al., 2014).
Indirect composites can be differentiated according to:
1.
2.
3.
4.
manufacturing process (manual layering vs machinable CAD/CAM),
microstructure (dispersed filler vs polymer infiltrated ceramic network “PICN”),
polymerization (light, high temperature, or high temperature with high pressure), and
composition (matrix and filler technology).
Different types of indirect composites are summarized in Table 7.6.
Manual indirect composites have similar structures, compositions, and layering
techniques to the direct composite. The key difference is that it is built up extraorally on a model in the lab and subjected to additional highly controlled polymerization, improving the DC.
Digital computerized techniques have recently revolutionized the world of dentistry, introducing digital designing and computerized milling of different industrial
high-performance materials blocks. CAD/CAM industrially processed blocks offer
homogenous materials with less flaws and extremely high filler loading up to levels
that couldn’t be possible with direct composite. Recent CAD/CAM blocks are BisGMA-free, and they are no longer photopolymerized. They are processed using
industrial grade high temperature and sometimes high pressure. CAD/CAM blocks’
microstructure can be either formed of a high amount of dispersed fillers or a PICN
(Mainjot et al., 2016).
PICN blocks are inspired by glass-infiltrated ceramics produced by Vita in the
1980s. In 1997, R. Giordano patented the idea of the infiltration of presintered
glassceramic scaffold with resin to produce PICN. PICNs differ significantly
from composite materials with dispersed fillers classically incorporated by mixing.
In contrast to dispersed fillers, the ceramic network forms a three-dimensional scaffold of interconnected particles forming a real skeleton which helps in a more effective stress distribution in all directions, thus resisting mechanical breakdown. In
2012, Vita produced the first commercial PICN blocks called Vita Enamic. The
high volume fraction of ceramic has led to introduction of the confusing
Table 7.5 Summary of commercially available bulk-fill resin composite with the manufacturers, claimed depth of cure, application technique,
composition, and claimed technology.
Product
Manufacturer
Type
Available shades
Claimed
depth of
cure
(mm)
Composition
Claimed technology
Surefil SDR
Dentsply
Flowable base
Universal
4
Resin: Modified UDMA,
TEGDMA, EBPADMA
Fillers: 68 wt.%, 44 vol.%;
barium and strontium
fluoroaluminosilicate glass
Initiator: CQ, BHT
photoaccelerator
Resin: Bis-EMA, UDMA,
TEGDMA, TMPTMA
Fillers: 86 wt.%, 66 vol.%
silanated strontium
aluminum sodium fluoride
phosphate silicate glass
Initiator: CQ
Resin: Bis-GMA, Bis-EMA,
UDMA
Fillers: 81 wt.% 61 vol.%
barium glass, ytterbium
trifluoride, mixed oxide,
prepolymer
Initiators: CQ, TPO, Ivocerin
Resin: Bis-GMA, Bis-EMA,
UDMA
Fillers: 68 wt.%,46 vol.%
barium glass, ytterbium
trifluoride, mixed oxide,
prepolymer
Initiator: CQ, TPO, Ivocerin
G
Quixfil
Tetric
EvoCeram
Bulk-fill
Tetric EvoFlow
Bulk-fill
Dentsply
Ivoclar
Vivadent
Ivoclar
Vivadent
Viscous full
depth filling
Viscous full
depth filling
nanohybrid
Flowable base
Universal
IVA
IVB
IVW
IVA
IVB
IVW
4
4
4
G
G
G
G
G
G
Lower filler content
Novel high molecular UDMA-based
monomer (849 g/mol) with stress
decreasing modulator
Increased filler loading reducing
shrinkage
Increased translucency and amount
of photoinitiator increasing the depth
of cure
Photoinitiator system containing
Ivocerin makes it more efficient in
promoting polymerization depth
Prepolymerized fillers reducing
shrinkage and relive stresses
The main difference between these
different products in filler loading
which controls viscosity of the
material either flowable or viscous
Tetric NCeram
Bulk-fill
Ivoclar
Vivadent
Viscous full
depth filling
nanohybrid
IVA
IVB
IVW
4
Tetric N-Flow
Bulk-fill
Ivoclar
Vivadent
Flowable base
IVA
IVB
IVW
4
SonicFill
Kerr
Sonic activated
full depth
filling
A1, A2, A3, B1
5
Resin: Bis-GMA, Bis-EMA,
UDMA
Filler: 78 wt.%, barium glass,
ytterbium trifluoride, mixed
oxide, prepolymer
Initiators: CQ, TPO, Ivocerin
Resin: Bis-GMA, Bis-EMA,
UDMA
Filler: 78 wt.%,barium glass,
ytterbium trifluoride, mixed
oxide, prepolymer
Initiators: CQ, TPO, Ivocerin
Resin: Bis-GMA, Bis-EMA,
TEGDMA
Fillers: 83.5 wt.% 69 vol.%
Silanated barium boron
aluminum silicate glass,
silica
G
G
G
Filtek Bulk-fill
Filtek Bulk-fill
flowable
3M ESPE
3M ESPE
Viscous full
depth filling
Flowable base
A1, A2, A3, B1,
C3
U, A1, A2, A3
4 (Class I)
5(ClassII)
4
Resin: Bis-GMA, AUDMA,
UDMA, and 1, 12dodecane-DMA
Fillers: 76.5 wt.%, 58.4 vol.%
Nano silica, nano zirconia,
zirconia/silica nanocluster,
ytterbium trifluoride
Initiators: CQ, EDMAB
Resin: Bis-GMA, Bis-EMA
(6), procrylate, and UDMA
Fillers: 64.5 wt.%, 42.5 vol.%
zirconia/silica fillers,
ytterbium trifluoride
Initiators: CQ, EDMAB
G
G
G
G
Sonic activation of the composite
dramatically lowers the viscosity
during placement
High translucency and increased
amount of photoinitiator for deeper
polymerization
High amount of filler loading
High molecular-weight AUDMA
reduce polymerization shrinkage
Addition fragmentation resin
reducing shrinkage stresses by
photocleavage during polymerization
Nanofiller technology reducing
shrinkage
Enhanced photoinitiators for deeper
curing
(Continued)
Table 7.5 (Continued)
Product
Manufacturer
Type
Available shades
Claimed
depth of
cure
(mm)
Composition
Claimed technology
X-tra fil
VOCO
Viscous full
depth filling
Universal
4
Resin: Bis-GMA, UDMA,
TEGDMA
Fillers: 86 wt.%, 70 vol.%
barium boron aluminum
silicate glass
Resin: Bis-GMA, UDMA,
TEGDMA
Fillers: 75 wt.%, barium boron
aluminum silicate glass
Resin: UDMA, Bis-EMA
Fillers: 65 wt.% 38 vol%
barium glass filler,
ytterbium fluoride and
silica
Bis-GMA, TEGDMA, PMMA
Hybrid filler, fractions, and Eglass fibers
G
X-tra base
VOCO
Flowable base
Universal, A2
4
Venus Bulk-fill
Heraeus
Kulzer,
Flowable base
Universal
4
Gc
Fiberreinforced
bulk-fill
base
Everx posterior
G
High filler loading to reduce
shrinkage
High translucency for deeper light
penetration
G
4
The fibers may conduct and scatter the
light over longer distances, explaining
the relatively deep and wide
polymerization observed
BHT, Butylated hydroxyl toluene; Bis-EMA, ethoxylated bisphenol A dimethacrylate; Bis-GMA, bisphenol glycidil dimethacrylate; CQ, camphorquinone; TEGDMA, triethylene glycol dimethacrylate; TMPTMA, trimethyloyl propane
trimethacrylate; TPO, diphenyl (2,4,6-trimethylbenzoyl) phosphine oxide; UDMA, urethane dimethacrylate.
Table 7.6 Different types of indirect composite materials, microstructure, manufacturers, polymerization modes, and compositions.
Manufacturing
process
Manual layering
Microstructure
Dispersed
fillers
Polymerization
mode
Light
Light 1 temperature
complement
Material
Manufacturer
Composition
Matrix
Fillers
Ceramage and
Ceramage up
Gradia
Shofu
UDMA, HEMA
Silica-based glass
GC Corp
UDMA, other DMA
Signum
Heraeus Kulzer
Sinfony
3M ESPE
UDMA, TEGDMA,
other DMA
UDMA, other DMA
Solidex
Shofu
UDMA
SR Nexeco
Ivoclar Vivadent
UDMA, other DMA
Silica powder, silicate glass
powder, prepolymerized
filler (75 wt.%)
Silica-based glass fillers
(74 wt.%)
Strontium aluminum
borosilicate glass, silica,
and 5% glass ionomer
fillers 50 wt.%
More than 53% ceramic
fillers
Silica (1050 nm),
Zirconia, silica-based
glass (7080 wt.%)
VITAVM LC
Estenia C&B
VITA
Zahnfabrick
Kuraray
SR adoro
Ivoclar Vivadent
Twiny
Yamamoto,
Precious Metal
Co
BPA, TEGDMA,
other DMA
Unknown DMA
(1Bis-GMA in
opaque paste)
UDMA 1 other
DMA
UDMA 1 TEGDMA
Silica-based glass, alumina
(2 μm and 2 nm) (92 wt.%)
Silica-based composite
Silica (20100 nm),
zirconia, alumina, silicaparticles (200600 nm),
zirconia aluminasilicaclusters (16 μm)
(Continued)
Table 7.6 (Continued)
Manufacturing
process
Machinable
blocks
Microstructure
Dispersed
fillers
Polymerization
mode
Light
High temperature
PICN
High temperature and
high pressure
Material
Manufacturer
3M ESPE
Composition
Matrix
Fillers
Silica (0.6 μm), zirconia
(0.6 μm) (85 wt.%)
Silica-based glass, silica (20
and 300 nm) (71 wt.%)
Silica (20 nm) zirconia
(411 nm), zirconiasilica clusters
(0.610 μm) (79 wt.%)
Silica-based glass, silica
(61 wt.%)
Glassceramic sintered
network (86 wt.%)
Paradigm MZ 100
block
Cerasmart
GC America
Lava Ultimate
3M ESPE
Bis-GMA,
TEGDMA
UDMA 1 other
DMA
UDMA
Shofu block HC
Shofu
UDMA, TEGDMA
VITA Enamic
VITA Zahnfabrik
UDMA, TEGDMA
AUDMA, Aromatic Urethane dimethacrylate; BPA, Bisphenol A; Bis-GMA, Bisphenol glycidil dimethacrylate; DMA, Dimethacrylate; EBPADMA, ethoxylatedbisphenol Adimethacrylate; EDMAB, ethyl 4-dimethyl
aminobenzoate; HEMA, hydroxyethyl methacrylate; PICN, polymer infiltrated ceramic network TEGDMA, triethylene glycol dimethacrylate; UDMA, urethane dimethacrylate.
Resin-based dental composites for tooth filling
165
commercial name “hybrid ceramic” to describe this material. “Hybrid ceramic” is a
common confusing commercial name that does not conform to materials science
and does not reflect the actual properties of the material. Different descriptive
names are present for PICNs such as double-network materials, interpenetrating
phase ceramicresin composites, or ceramic-based interpenetrating phase
materials.
Among CAD/CAM composites, PICN materials constitute an innovative and
promising class of materials with benefits in term of high flexural strength, hardness
value between enamel and dentin (thus reducing tooth wear), elastic modulus intermediate between enamel and dentin, and minimal toxicity and resin leaching.
Recent advances with CAD/CAM composites are promising according to the current in vitro studies. Unfortunately, there is limited clinical evidence regarding this
category of materials and consequently no evidence-based recommendations can be
supported for clinical practice at the moment (Mainjot et al., 2016; Angeletaki
et al., 2016).
Regarding selection of the suitable restorative protocol in clinical practice
according to the current evidence, there is no difference in terms of clinical durability between direct and indirect resin composite restorations in different clinical
situations. Given the current level of evidence, it appears reasonable to suggest that
the less costly and less time-consuming technique of placing direct resin restorations should be the preference when guiding patient decision-making (Farsai, 2017;
Radford, 2017).
7.7
Guidelines and recommendations for future
laboratory and clinical researches
There are always confusing gaps and difficulty in correlating the standardized
in vitro evaluations with clinical performance of the restorative materials. Different
trials to make such correlations are often criticized for lack of evidence for significant correlation with clinical performance.
Although most of the laboratory methods are standardized and validated, there is
interinstitute variability and different values can be presented for the same product
even with ISO testing. Clinical studies show greater variability and a lack of standardization with the risk of different types of bias. Reasons for this variation may
be accounted for by factors related to the patient, materials, skills, treated teeth,
procedure complexity, and/or type of outcome and its assessment method.
Correlations between laboratory and clinical outcomes were found to be moderately positive with a few significant results. Restoration fracture was found to be
mostly correlated to the material’s fracture toughness, while clinical wear was correlated with flexural strength. No clinical correlations were found for compressive
strength and flexural modulus. Unfortunately, these conclusions should be carefully
considered as they are based on a huge amount of variable studies with inadequate
descriptions or studies with a high risk of bias (Heintze et al., 2017).
166
Advanced Dental Biomaterials
For better standardized and comparable future outcomes, eminent dental
researchers with the Academy of Dental Materials have set guidelines for resin
composite laboratory testing and recommendations for future randomized clinical
trials.
7.7.1 Guidelines for laboratory evaluation of resin composite
(mechanical behavior and technique sensitivity)
In 2017 the Academy of Dental Materials set an initiative to review and critically
appraise the different laboratory testing methodologies to evaluate resin composite
mechanical performance and technique sensitivity, in an attempt to develop guidelines for in vitro composite evaluation. Test methods have been ranked on the priority of the specific property being tested, as well as on the specific test methods for
evaluating that property. Focus was placed on the methods that are considered to be
of the highest priority in terms of being the most applicable, useful, supported by
the literature, and clinical correlation.
The properties for evaluating resin composites were ranked in the priority of
measurement regarding mechanical performance and technique sensitivity and are
listed in Table 7.7. These guidelines were meant to help the researchers in choosing
the proper method to assess the key properties of dental resin composites with
regard to their mechanical behavior and technique sensitivity (Ilie et al., 2017;
Ferracane et al., 2017) (Table 7.8).
7.7.2 Recommendations for future clinical studies
Clinical research in restorative dentistry is confounded by various problems of
study designs, trials length, and collected information in addition to high cost.
Opdam et al. reviewed and discussed the pros and cons of different study designs
and outcomes for the evaluation of dental restorations and set recommendations for
future clinical trials.
They recommended that clinical trials should have control groups, include confounders, such as patient risk factors, in the data, and analysis with assessment of
patient-centered outcomes with relevance to the profession and patients.
For further development of restorative dentistry, there is plenty of room for different research questions to be studied with well-designed and executed trials.
Studies comparing new materials to their predecessors are needed before launching
new products but it is not of prime importance. Randomized clinical trials comparing different treatment protocols are much more valuable. For example, comparison
of direct versus indirect restorations, tooth replacement versus tooth retention, restoration repair versus replacement, bridge versus implant, all need to be assessed.
Comparing materials with each other should be done against the gold standard. For
material testing trials, clarifying any conflict of interest or sponsorship is mandatory. The primary outcome should be valuable and of relevance to patients, dentists,
and stakeholders. The use of globally agreed outcomes for future trials would be
Table 7.7 Summary of the available methods for mechanical evaluation of resin composite.
Clinical issue/requirement
Properties
Property rank
Method
Test rank
Fracture and deformation resistance
Strength
1
Toughness
2
Fracture toughness
1
Edge strength—
chipping
Fatigue
2
3-Point bending (ISO 4049)
4-Point bending
Biaxial flexural (ASTM F394-78)
Compression (ASTM D695)
Tensile (ASTM D638)
Diametral tensile (ANSI/ADA Spec 27)
Impact (ISO 179/1961)
Transverse impact (DIN 53 453)
Shear
Shear punch (ASTM D732-46)
Calculated from strength test
Impact (ISO 179/1961)
Transverse impact (DIN 53 453)
Double torsion
Indentation—Vickers
Chevron notched specimens (ASTM E1304-97)
Single-edge notched beam (ASTM E399-12)
Compact tension (ASTM E399-12)
CK10 instrument (with acoustic emission)
1
2
2
3
1
4
2
2
4
2
1
2
2
2
3
2
1
2
1
1
Elastic modulus
1
Fatigue strength—Staircase
Fatigue resistance—uniaxial loading (ASTM E606/E606M-12)
3-Point bending (ISO 4049)
4-Point bending
Biaxial flexural strength (ASTM F394-78)
Compression (ASTM D695)
Tensile
Diametral tensile (ANSI/ADA Spec 27)
2
2
2
1
3
3
1
4
Indentation hardness
1
Indentation (ISO/FDIS 14577-1)
Martens (universal) (E DIN 50359)
Vickers (ISO 6507-1)
Knoop (ISO 6507-1)
Rockwell (ISO 2039-2)
Brinell (ISO 6506-1:200)
1
1
3
3
3
3
(Continued)
Table 7.7 (Continued)
Clinical issue/requirement
Properties
Property rank
Method
Test rank
Wear resistance
Wear—abrasion/three
body
1
Wear—attrition/
contact/two body
1
Wear—toothbrush
3
OHSU abrasion (ISO TS No. 14569-2)
Alabama generalized (ISO TS No. 14569-2)
ACTA (ISO TS No. 14569-2)
OHSU attrition (ISO TS No. 14569-2)
Alabama localized (ISO TS No. 14569-2)
Ivoclar-Willytec simulator
Munich-Willytec simulator
Toothbrush/toothpaste(ISO TS No. 14569-2)
1
2
3
2
3
2
2
3
Source: Adapted from Academy of Dental Materials’ guidance.
Table 7.8 Summary of available tests for evaluation of resin composite handling, polymerization, and dimensional stability.
Clinical issue/requirement
Properties
Property
rank
Method
Test
rank
Technique sensitivity: handling
—placement
Stickiness
2
Slump resistance
2
Viscosity
2
Porosity
1
Radiopacity
Sensitivity to ambient light
Degree of conversion
1
1
1
Polymerization kinetics—rate
1
Depth of cure
1
Unplugging force, unplugging work
Measure length/area of withdrawn composite
Extrude and cure
Imprint and cure (SRI)
Rheology (with Viscometer)
Pressing under standard load and measure size
Section—assess under magnification
3D microtomography
Archimedes method, ASTM D3171-11
X-ray
ISO 4049 (vs aluminum step wedge) and ISO13116
ISO 4049 (Xenon light box)
FT-IR spectroscopy
Near IR
FT-Raman
DSC
NMR
FT-IR, NIR, Raman
DSC
Shrinkage/dilatometry
Optical—interferometry, fluorescent probes
Elastic modulus—DMA, rheometer
Acoustic
DEA
ISO 4049—scraping
Microhardness vs depth
Chemical vs depth (FT-IR, NIR, Raman)
Penetrometer
Solvent dissolution
Transition in translucency
1
2
1
1
1
2
1
2
2
2
1
1
1
1
2
2
4
1
1
2
2
3
2
2
2
1
1
2
3
3
Polymerization
(Continued)
Table 7.8 (Continued)
Clinical issue/requirement
Properties
Property
rank
Method
Test
rank
Dimensional stability
Polymerization shrinkage
1
Polymerization shrinkage rate/
kinetics and gel point
Polymerization stress
1
Bonded disk
SSA
Linometer
Dilatometer (e.g., Hg)
Pyknometer
Archimedes method—ISO (17304)
Accuvol camera imaging
Strain gage
Digital image correlation
E.g., from bonded disk or SSA
1
1
2
2
2
1
2
2
2
1
1
Hygro (swelling) expansion
1
Via UTM
Bioman method
Tensilometer (cantilever beam)
SSA
Photoelastic method
Thin ring
Indentation crack analysis
Laser scanning of disk—stored for 3 months or more
in water or other solvent.
Calipers or dial gage
Measuring microscope
Displacement measured over a temperature range
1
1
1
1
2
2
3
1
Thermal expansion
3
2
2
2
DEA, Dielectric analysis; DSC, Differential scanning calorimetry; FTIR, Fourier transform infrared; NIR, Fourier transform near-infrared spectroscopy; NMR, Nuclear magnetic resonance; SRI, slump resistance
index; SSA, stressstrain analyzer; UTM, universal testing machine.
Source: Adapted from Academy of Dental Materials’ guidance.
Resin-based dental composites for tooth filling
171
desirable also to reduce the risk of selective reporting. Different patient-related risks
such as caries risk and bruxism should be recorded and considered in analysis. The
time and causes for any interventions should also be recorded to allow differentiation between success, failure, and survival. Different trial designs should be considered when planning to compare restorative treatments and materials: while
randomized clinical trials reduce selection bias, their observation times are usually
short and sample sizes limited. Retrospective and prospective practice-based studies
circumvent these limitations, but have considerable risk of indication bias and confounding which need to be dealt with appropriately. Perhaps the answer lies in coordinated, multicenter studies of different design, no one design being capable of
yielding all the required outcomes. Whatever the way forward, funders and sponsors of clinical research in restorative dentistry should encourage investigators to
come forward with new innovative approaches to answer priority questions (Opdam
et al., 2017).
References
Alharbi, A., Rocca, G.T., Dietschi, D., Krejci, I., 2014. Semidirect composite onlay with cavity sealing: a review of clinical procedures. J. Esthet. Restor. Dent. 26, 97106.
Alvanforoush, N., Palamara, J., Wong, R.H., Burrow, M.F., 2017. Comparison between published clinical success of direct resin composite restorations in vital posterior teeth in
19952005 and 20062016 periods. Aust. Dent. J. 62, 132145.
Angeletaki, F., Gkogkos, A., Papazoglou, E., Kloukos, D., 2016. Direct versus indirect inlay/
onlay composite restorations in posterior teeth. A systematic review and meta-analysis.
J. Dentistry 53, 1221.
Bakopoulou, A., Papadopoulos, T., Garefis, P., 2009. Molecular toxicology of substances
released from resin-based dental restorative materials. Int. J. Mol. Sci. 10, 38613899.
Baroudi, K., Rodrigues, J.C., 2015. Flowable resin composites: a systematic review and clinical considerations. J. Clin. Diagn. Res. 9, Ze18Ze24.
Beyth, N., Farah, S., Domb, A.J., Weiss, E.I., 2014. Antibacterial dental resin composites.
React. Funct. Polym. 75, 8188.
Braden, M., 1974. Selection and properties of some new dental materials. Dent. Update 1,
489501.
Braga, R.R., Ballester, R.Y., Ferracane, J.L., 2005. Factors involved in the development of
polymerization shrinkage stress in resin-composites: a systematic review. Dent. Mater.
21, 962970.
Cheng, L., Zhang, K., Zhang, N., Melo, M.A.S., Weir, M.D., Zhou, X.D., et al., 2017.
Developing a new generation of antimicrobial and bioactive dental resins. J. Dent. Res.
96, 855863.
Chesterman, J., Jowett, A., Gallacher, A., Nixon, P., 2017. Bulk-fill resin-based composite
restorative materials: a review. Br. Dent. J. 222, 337344.
da Costa, J.B., Hilton, T.J., Swift Jr., E.J., 2011. Critical appraisal: preheating composites. J.
Esthet. Restor. Dent. 23, 269275.
Demarco, F.F., Collares, K., Coelho-De-Souza, F.H., Correa, M.B., Cenci, M.S., Moraes, R.
R., et al., 2015. Anterior composite restorations: a systematic review on long-term survival and reasons for failure. Dent. Mater. 31, 12141224.
172
Advanced Dental Biomaterials
Drummond, J.L., 2008. Degradation, fatigue, and failure of resin dental composite materials.
J. Dent. Res. 87, 710719.
Farsai, P.S., 2017. Longevity of direct and indirect resin composite restorations in permanent
posterior teeth: a systematic review and meta-analysis. J. Evid.-Based Dent. Pract. 17,
110112.
Ferracane, J.L., 2011. Resin composite—state of the art. Dent. Mater. 27, 2938.
Ferracane, J.L., 2017. Models of caries formation around dental composite restorations. J.
Dent. Res. 96, 364371.
Ferracane, J.L., Hilton, T.J., Stansbury, J.W., Watts, D.C., Silikas, N., Ilie, N., et al., 2017.
Academy of dental materials guidance-resin composites: Part II-Technique sensitivity
(handling, polymerization, dimensional changes). Dent. Mater. 33, 11711191.
Franco, E.B., Francischone, C.E., Medina-Valdivia, J.R., Baseggio, W., 2007. Reproducing
the natural aspects of dental tissues with resin composites in proximoincisal restorations.
Quintessence Int. 38, 505510.
Fugolin, A.P.P., Pfeifer, C.S., 2017. New resins for dental composites. J. Dent. Res. 96,
10851091.
Habib, E., Wang, R., Wang, Y., Zhu, M., Zhu, X., 2015. Inorganic fillers for dental resin
composites: present and future. ACS Biomater. Sci. Eng. 2, 111.
Heintze, S.D., Ilie, N., Hickel, R., Reis, A., Loguercio, A., Rousson, V., 2017. Laboratory
mechanical parameters of composite resins and their relation to fractures and wear in
clinical trials—a systematic review Siegward. Dent. Mater. 33, E101E114.
Hervas-Garcia, A., Martinez-Lozano, M.A., Cabanes-Vila, J., Barjau-Escribano, A., FosGalve, P., 2006. Composite resins. A review of the materials and clinical indications.
Med. Oral Patol. Oral Cir. Bucal 11, E215E220.
Ilie, N., Hickel, R., 2009. Investigations on mechanical behaviour of dental composites. Clin.
Oral Investig. 13, 427438.
Ilie, N., Hilton, T.J., Heintze, S.D., Hickel, R., Watts, D.C., Silikas, N., et al., 2017.
Academy of dental materials guidance-resin composites: Part I—Mechanical properties.
Dent. Mater. 33, 880894.
Kaizer, M.R., DE Oliveira-Ogliari, A., Cenci, M.S., Opdam, N.J.M., Moraes, R.R., 2014. Do
nanofill or submicron composites show improved smoothness and gloss? A systematic
review of in vitro studies. Dent. Mater. 30, e41e78.
Khan, A.S., Azam, M.T., Khan, M., Mian, S.A., Ur rehman, I., 2015. An update on glass
fiber dental restorative composites: a systematic review. Mater. Sci. Eng. C, Mater.
Biol. Appl. 47, 2639.
Kwon, T.Y., Bagheri, R., Kim, Y.K., Kim, K.H., Burrow, M.F., 2012. Cure mechanisms in
materials for use in esthetic dentistry. J. Investig. Clin. Dent. 3, 316.
Leprince, J.G., Palin, W.M., Hadis, M.A., Devaux, J., Leloup, G., 2013. Progress in
dimethacrylate-based dental composite technology and curing efficiency. Dent. Mater.
29, 139156.
Lohbauer, U., Belli, R., Ferracane, J.L., 2013. Factors involved in mechanical fatigue degradation of dental resin composites. J. Dent. Res. 92, 584591.
Lutz, F., Setcos, J., Phillips, R., Roulet, J., 1983. Dental restorative resins. Types and characteristics. Dent. Clin. N. Am. 27, 697712.
Maas, M.S., Alania, Y., Natale, L.C., Rodrigues, M.C., Watts, D.C., Braga, R.R., 2017. Trends
in restorative composites research: what is in the future? Braz. Oral Res. 31, e55.
Mainjot, A.K., Dupont, N.M., Oudkerk, J.C., Dewael, T.Y., Sadoun, M.J., 2016. From artisanal to CAD-CAM blocks: state of the art of indirect composites. J. Dent. Res. 95,
487495.
Resin-based dental composites for tooth filling
173
Mallineni, S.K., Nuvvula, S., Matinlinna, J.P., Yiu, C.K., King, N.M., 2013. Biocompatibility
of various dental materials in contemporary dentistry: a narrative insight. J. Investig.
Clin. Dent. 4, 919.
Mikhail, S.S., Johnston, W.M., 2014. Confirmation of theoretical colour predictions for layering dental composite materials. J. Dent. 42, 419424.
Nahsan, F.P.S., Mondelli, R.F.L., Franco, E.B., Naufel, F.S., Ueda, J.K., Schmitt, V.L., et al.,
2012. Clinical strategies for esthetic excellence in anterior tooth restorations: understanding color and composite resin selection. J. Appl. Oral Sci. 20, 151156.
Nayar, S., Ganesh, R., Santhosh, S., 2015. Fiber reinforced composites in prosthodontics—a
systematic review. J. Pharm. Bioallied Sci. 7, S220.
Nedeljkovic, I., Teughels, W., De munck, J., Van meerbeek, B., Van landuyt, K.L., 2015. Is
secondary caries with composites a material-based problem?. Dent. Mater. 31,
e247e277.
Opdam, N.J.M., Collares, K., Hickel, R., Bayne, S.C., Loomans, B.A., Cenci, M.S., et al.,
2017. Clinical studies in restorative dentistry: new directions and new demands. Dent.
Mater.
Pitel, M.L., 2013. Low-shrink composite resins: a review of their history, strategies for managing shrinkage, and clinical significance. Compend. Contin. Educ. Dent. 34, 578590.
Radford, J.R., 2017. Longevity of direct and indirect resin composite restorations in permanent posterior teeth: a systematic review and meta-analysis. BDJ 222, 30.
Rasines Alcaraz, M.G., Veitz-Keenan, A., Sahrmann, P., Schmidlin, P.R., Davis, D., IheozorEjiofor, Z., 2014. Direct composite resin fillings versus amalgam fillings for permanent
or adult posterior teeth. Cochrane Database Syst. Rev. 31, Cd005620.
Santini, A., 2010. Current status of visible light activation units and the curing of lightactivated resin-based composite materials. Dent. Update 37, 214216. 218-20, 223-7.
Santini, A., Gallegos, I.T., Felix, C.M., 2013. Photoinitiators in dentistry: a review. Prim.
Dent. J. 2, 3033.
Schenkel, A.B., Peltz, I., Veitz-Keenan, A., 2016. Dental cavity liners for class I and class II
resin-based composite restorations. Cochrane Database Syst. Rev. 10, Cd010526.
Soares, C.J., Faria, E.S.A.L., Rodrigues, M.P., Vilela, A.B.F., Pfeifer, C.S., Tantbirojn, D.,
et al., 2017. Polymerization shrinkage stress of composite resins and resin cements—
what do we need to know? Braz. Oral Res. 31, e62.
Then, S., Neon, G.S., Abu kasim, N.H., 2011. Performance of melamine modified ureaformaldehyde microcapsules in a dental host material. J. Appl. Polym. Sci. 122,
25572562.
Zimmerli, B., Strub, M., Jeger, F., Stadler, O., Lussi, A., 2010. Composite materials: composition, properties and clinical applications. A literature review. Schweiz Monatsschr
Zahnmed 120, 972986.
8
Glass-ionomer cement: chemistry
and its applications in dentistry
Saroash Shahid1 and Tomas Duminis2
1
Centre for Oral Bioengineering, Institute of Dentistry, Queen Mary University of London,
London, United Kingdom, 2Centre for Oral Bioengineering, Institute of Dentistry, Barts
and the London School of Medicine and Dentistry, London, United Kingdom
Chapter Outline
8.1 Introduction 175
8.2 Development of glass-ionomer cements 176
8.3 Components of glass-ionomer cements 178
8.3.1 Composition and nature of the glass component 178
8.3.2 Composition and nature of the acid component 180
8.3.3 Water: the reaction medium 181
8.4 Chemistry of the setting reaction
181
8.4.1 Decomposition of the glass powder 182
8.4.2 Gelation phase 182
8.4.3 Maturation phase 183
8.5 Fluoride release from glass-ionomer cements
183
8.5.1 Source of fluoride 183
8.5.2 Mechanism of fluoride release 184
8.5.3 Factors effecting fluoride release 184
8.6 Mechanical properties
185
8.6.1 Compressive strength 185
8.6.2 Flexural strength 186
8.7 Esthetics 188
8.8 Chemical adhesion with tooth 188
8.9 Moisture sensitivity of glass-ionomer cements 189
8.10 Use of glass-ionomer cements in alternative restorative technique
8.11 Nanoapatite-filled glass ionomers 189
8.12 Thermo-cured glass ionomers 190
8.13 Resin-modified glass-ionomer cements 190
8.14 Glass ionomer as a “nondental” cement 191
References 191
Further reading 194
8.1
189
Introduction
It has been almost 50 years since the first glass-ionomer cements (GICs), now officially termed as “glass polyalkenoate cements,” were introduced into the dental
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00008-6
Copyright © 2019 Elsevier Ltd. All rights reserved.
176
Advanced Dental Biomaterials
world. In recent years this material has undergone further development resulting in
the availability of a range of materials which undergo setting or “curing” via different proportions of acidbase and free-radical reactions. In the wake of these developments it seems essential to define what GICs are. To serve this purpose, the
following definition seems an adequate description of the chemistry and properties
of the material:
The term glass-ionomer cement is reserved exclusively for a material consisting of
acid-decomposable glass and a water-soluble acid that sets by neutralisation
reaction which takes place within a clinically acceptable time.
McLean (1994)
Ever since its advent, GIC has received a mixed response from clinicians. It is
acknowledged for its chemical adhesion with the tooth and continuing fluoride release
(Wilson, 1989; Smith, 1998), but also it is subjected to criticism due to its lack of physical strength and translucency (Crisp et al., 1974; Mount and Makinson, 1982). Despite
this criticism, the material has found its place in a broad spectrum of applications such
as luting/lining cement; base, or dentine substitute under composite resin; sealant over
an active carious lesion; and a restoration in its own right. The driving force in all these
aforementioned applications is indeed the chemical adhesion with tooth and the longterm fluoride release (Anusavice, 2003; Mount and Hume, 1998; Mount, 1998).
8.2
Development of glass-ionomer cements
The inspiration for the development of GIC can be traced back to the era of clinical
dentistry which was governed by the use of amalgam, gold, and porcelain as restorative materials. The limitations of these materials drove the need for new materials,
which could be used for luting/lining purposes and which also had a better esthetic
appeal. This paved the way for the development of the zinc phosphate cement by
Pierce in 1879 which was later further modified by Ames and Fleck (Ames, 1892;
Fleck, 1902) to give the modern-day zinc-phosphate cement. Coinciding with Pierce’s
discovery was Foster’s zinc oxideeugenol cement which soon gained popularity due
to its obtundant effect on the pulp (Smith, 1998). Despite all these developments, the
first breakthrough on the esthetics front was the silicate cement. Developed originally
in 1873 by Thomas Fletcher, the silicate became famous in 1904, only after it had
been modified by Steenbock of Berlin. Due to these ongoing developments, the end of
the first quarter of the 20th century saw three basic types of dental cements, namely,
zinc phosphate cement, zinc oxideeugenol cement, and silicate cement. Over the
next 50 years, these cements underwent considerable technical improvement, but generally, the fundamentals of their setting chemistry remained unchanged.
In 1963 the idea of polyelectrolyte cement was developed, which involved the
reaction of metal oxide with reactive water-soluble polymers. Based on this concept, Smith produced the first zinc polyacrylate cement using zinc oxide and poly
Glass-ionomer cement: chemistry and its applications in dentistry
177
(acrylic acid). By 1964, this cement had been developed into a usable system. It
was capable of chemically bonding to the tooth structure due to the use of poly
(acrylic acid) which has the ability to complex calcium ions and form hydrogen
bonds with collagen. After undergoing technological improvements and clinical
trials, the material became commercially available in 1968. In the next decade the
material underwent considerable development and materials containing fluorides
and using copolymers became commercially available.
In spite of the novel properties of these polyacrylate cements, the metal oxide
component rendered them opaque and hence not esthetically acceptable. This led to
the development of formulations using zinc-containing glass ceramics and silicate
cement powders, but these had problems such as the prolonged setting time when
mixed with poly(acrylic acid). Wilson and Kent made a major development in this
direction by taking poly(acrylic acid) and mixing it with an ion-leachable glass
(Wilson and Kent, 1972). The resultant product was given the name ASPA that was
an acronym for aluminosilicate polyacrylate. ASPA (Fig. 8.1) was a hybrid of the
dental silicate cement and the carboxylate cement. The development of more reactive glasses with high fluorine content and the discovery of the effect of tartaric
acid in improving the setting properties resulted in the first practical GIC in 1972.
These earlier materials, however, had drawbacks mainly related to their sluggish
setting. They showed prolonged sensitivity to moisture and when set they were
slightly opaque. However, since these early materials appeared various modifications had been carried out which have led to materials with better characteristics.
These modifications included the following:
1. Use of alternative polymers such as acrylic/maleic acid as the polyacid component
(Nicholson, 1998).
2. The use of vacuum-dried polymer powders blended with the glass and activated by the
addition of water (Prosser et al., 1984).
3. The development of cermet containing cements in which the filler consists of a cermet
which is silver sintered to the surface of calcium fluoroaluminosilicate glass. These
Figure 8.1 Aluminosilicate polyacrylate (ASPA), the first commercial glass-ionomer cement
(GIC).
178
Advanced Dental Biomaterials
materials have their use in situations where radiopacity is required and for core buildup
under crowns (McLean and Gasser, 1985).
4. Metal-reinforced cements in which a metal such as a silver tin alloy or stainless steel is
added as an inert filler to conventional glass-ionomer in an attempt to reinforce the set
cement (Williams et al., 1992).
5. Resin-modified cements in which the conventional acidbase reaction of GIC are complemented by photochemical polymerization of added monomers and initiators.
8.3
Components of glass-ionomer cements
Conventional GICs have the following constituents:
G
G
G
Glass powder: A specially formulated acid-degradable fluoroaluminosilicate glass.
Acid: The acid is a homopolymer of acrylic acid or a related copolymer. (1)Tartaric acid
is added to improve the working and sharpen the setting time.
Water: The reaction medium.
8.3.1 Composition and nature of the glass component
The glasses used in GIC are fluoroaluminosilicates. These are different from glasses
we see around us, for example in windows, which are mainly soda lime silica
glasses. Window glasses possess highly cross-linked OSiO linkages and are
chemically stable in nature and do not react with conventional acids. Such glasses
would serve no purpose in GIC since in order to produce set cement it is essential
that the glass is reactive in nature and capable of releasing metal cations. However,
the addition of network modifying cations to these glasses disrupts the OSiO
linkages to produce nonbridging oxygens (BOs) (NBOs). The resulting glass then
represents an ionic polymer where the positive charge of the cation balances the
negative charge on the network (produced by NBO). For glasses used in GIC, alumina acts as the intermediate oxide, that is, it can take part in glass structure but
cannot form glass on its own. The addition of alumina produces negative sites such
as the AlO2
4 tetrahedra makes these glasses “acid decomposable,” hence allowing
them to be used in cement formation. Fluoroaluminosilicates are produced by the
fusion of silica, alumina, calcium fluoride, and calcium oxide with aluminum fluoride, aluminum phosphate, and cryolite (Na3AlF6) added in minor quantities.
Structurally, these glasses are based on AlO4 and SiO4 tetrahedra with a threedimensional glass structure (Fig. 8.2). O is at the vertex and Si and Al are at the
center of the tetrahedron.
Alkaline ions or alkaline earth ions such as Na1, Ca21, and Sr21 exist near the
31
Al ion in order to charge balance AlO2
4 tetrahedra. These modifying ions can
also result in the formation of NBO. It was originally believed that fluoride and
phosphate ions included in the glass structure do not form a part of the skeletal
structure of the silicate network (Davidson and Mjör, 1999); however, some studies
Glass-ionomer cement: chemistry and its applications in dentistry
179
Figure 8.2 Skeletal structure of fluoroaluminosilicate glass (a tetrahedron) (Davidson and
Mjör, 1999). (Note: The structure is 3D but is drawn in 2D for simplicity.)
Table 8.1 Components of fluoroaluminosilicate glass and their effects.
Component
Percentage
Effects
SiO2
29.0
Al2O3
16.6
CaF2
34.2
These are three essential components of the glass which
fuse to form the calcium fluoroaluminosilicate glass.
Glasses higher in SiO2 (more than 40%) are more
translucent, whereas those high in CaF2 or Al2O3 are
more opaque.
Complements the fluxing action of CaF2, i.e., reduce
fusion temperature
Improves translucency and adds body to the cement paste
Used to replace calcium fully or partially to give
radiopacity to the glass
Na3AlF6
AlPO4
Sr, Ba, La,
salts
5.0
9.9
Source: Compiled from Mount G.J., Hume W.R., 1998. Preservation and Restoration of Tooth Structure. Mosby,
London; Wilson A.D., McLean J.W., 1988. Glass-Ionomer Cement. Quintessence, Chicago, IL.
have shown the existence of phosphate as a network former, and there is strong evidence that PO41 tetrahedra locally charge balance AlO2
4 tetrahedra.
The glasses are commercially prepared by fusing the mixture of its ingredients
(Table 8.1) at 1200 C1550 C. In the next step the melt glass is shock cooled
resulting in the formation of coarse granules which are then ground by dry milling
in a ball mill to produce a particle size depending upon its application. Generally, a
particle size of ,50 µm is preferred for restorative cements, whereas ,20 µm is
produced for the luting type of material (Wilson and McLean, 1988). In either case
ball milling is often followed by acid-washing of the glasses with 5% aqueous
acetic acid. This is done in order to reduce the reactivity of the glass.
Early work on simple glasses suggests that the Al2O3/SiO2 ratio is crucial in
determining the glass reactivity (Wilson et al., 1979); however, more recently
180
Advanced Dental Biomaterials
Griffin and Hill (1999) have provided evidence that this ratio has no significant
influence on the properties of GICs derived from fluoro-alumino-phosphosilicate
glasses. Fluoride fluxes (CaF2 and Na3AlF6) apart from lowering the fusion temperature of the glass, impart the unique property of fluoride release from the cement.
Griffin and Hill (2000) reported that the glass transition temperature, Tg, for glasses
prepared in their experiments falls by approximately 200 C when the amount of
fluorine is increased. They explained that the reduction in the temperature is caused
by the replacement of BOs by fluorines to form NBOs in the glass. Thus it disrupts
the network and allows the relaxation phenomena to take place at a lower temperature. In addition, fluorine converts Ca21 to F-Ca(n) reducing the number of NBOs
attached to Si. The presence of fluorine in the glass structure also affects the rheological and setting properties of GIC. Fluorine-containing glass will be more “network disrupted” and hence more susceptible to acid attack. Crisp and Wilson
(1974a,b) found that increasing the fluoride content aids in the extraction of ions
from the glass. De Barra and Hill (2000) also found that increasing the content of
fluorine in a glass reduces the working and setting times of the cement.
In most commercial formulations, calcium is wholly or partially replaced by
strontium, barium, or lanthanum to impart radiopacity to the set cement. Strontium
seems to be an ideal candidate since it has a similar ionic radius to that of calcium
and hence can replace it without disrupting the glass and produce any loss of translucency (Deb and Nicholson, 1999).
8.3.2 Composition and nature of the acid component
Acids used in the conventional glass-ionomer system are polyelectrolytes. These, as
the name denotes, are both polymers and electrolytes and hence are soluble in
water. Polyelectrolytes used in GIC are the poly(alkenoics). These polyacids
include the homopolymers and copolymers of unsaturated mono-, di-, and tricarboxylic acids. Of these, the most important used to date have been poly(acrylic
acid)s, copolymers of acrylic and itaconic acids (Crisp et al., 1980), and copolymers
of acrylic and maleic acids. The polyacids are generally prepared by free-radical
polymerization of the appropriate monomers in aqueous solution in the presence of
a chain transfer agent and an initiator such as ammonium persulfate. These polyacids consist of linear chains with no cross-linking but have pendant acid groups
(Wilson and McLean, 1988). To produce a cement of adequate mechanical properties it is essential that the polyacids used have a molecular weight in the range of
40,000 to 60,000—the higher the molecular weight the better will be the mechanical properties—however, in practice molecular weight is limited by viscosity, and
some balance has to be achieved between concentration, viscosity, and molecular
weight (Wilson et al., 1989).
The polyacid used in the original glass ionomer was 50% by weight aqueous
solution of poly(acrylic acid) (Crisp et al., 1975). However, poly(acrylic acid) molecules being flexible and mobile are capable of intermolecular hydrogen bonding.
This results in gelation of poly(acrylic acid) solutions on storage prepared at a concentration greater than 45% by weight. It was found that methylation of the poly
Glass-ionomer cement: chemistry and its applications in dentistry
181
(acrylic acid) inhibits the gelation process (Crisp et al., 1975); however, cements
prepared from such a liquid stained in the mouth. Crisp and Wilson (1974a,b)
hypothesized that the copolymers of acrylic acid with other saturated carboxylic
acids would be less susceptible to gelation due to reduced stereoregularity. Based
on this assumption, they synthesized a copolymer of acrylic and itaconic acid which
proved to be indefinitely stable to gelation at a concentration of 50% m/m. Due to a
greater number of carboxylic acid groups, cements produced from copolymers with
higher acid functionality were found to be harder than those of poly(acrylic acid)
(Mount and Makinson, 1982). However, it was also observed that cements based on
acrylic acid copolymers show less adhesion with tooth structure (Aboush and
Jenkins, 1986) and are less resistant to acid attack (Setchell et al., 1985; Wilson
et al., 1986) than cements of poly(acrylic acid). Tartaric acid (1) is an essential
additive in the glass-ionomer system. It is added at a level of 5% or 10% in order
to improve the handling properties, which it does by extending the working time
and sharpening the setting time (Crisp et al., 1975). Using fourier transform infrared
spectrsocopy (FTIR) analysis, Nicholson (1998) suggested that this is because (1)
tartaric acid delays the formation of calcium carboxylate. Raman analysis also confirms this finding. An increase in compressive strength (CS) has also been reported
with the use of tartaric acid (Crisp et al., 1975).
8.3.3 Water: the reaction medium
GICs are water-based materials, and hence water plays an important role in their
setting and structure. It serves as a solvent and a medium for transporting the ions.
Apart from this, water also hydrates the siliceous hydrogel and the metal poly(acrylate) salts formed (Wilson and Mclean, 1988). Water is present in the set cement in
at least two different states depending on whether they can be removed or not by
desiccation over a suitable desiccant. These states have been classified as “evaporable” and “nonevaporable” or more commonly referred to as “loosely bound” and
“tightly bound” water, respectively (Wilson et al., 1979). Loss of loosely bound
water during initial setting stages retards the setting and produces surface crazing
and cracks, whereas moisture contamination at this stage results in loss of soluble
ions producing weak cements (Wilson et al., 1979; Causton, 1981). As the cement
matures, the ratio of tightly bound water to loosely bound water increases, decreasing its susceptibility to desiccation accompanied by an increase in strength and
modulus and a decrease in plasticity (Paddon and Wilson, 1976; Wilson and Kent,
1972).
8.4
Chemistry of the setting reaction
The setting reaction is an acidbase reaction with the ion-leachable glass acting as
a base and the acid being poly(acrylic acid) or its copolymer (Crisp and Wilson,
1974a,b).
182
Advanced Dental Biomaterials
The setting process is in three overlapping stages (Crisp and Wilson, 1974a,b):
Stage 1: The decomposition of the glass powder;
Stage 2: Gelationprecipitation of cations and anions;
Stage 3: Maturation phase.
8.4.1 Decomposition of the glass powder
This phase may be best described as the ion leaching or extraction phase. During
this stage, ionization of the carboxylic acid liberates protons (H1) from the carboxyl (COOH) group. These protons attack the surface of the glass liberating Al31,
Ca21, Na1, F2 (if present), and H2PO24 ions into the aqueous phase (Wilson and
Prosser, 1982). Barry et al. (1979) found that this attack was not uniform but
seemed to take place more at calcium-rich sites in the glass since these areas are
more basic. Whatever the nature of the attack, it results in the formation of silicic
acid which later condenses to form silica gel (Wasson and Nicholson, 1990, 1993).
Crisp and Wilson (1974a,b) predicted that as a result of this attack, 20%30% of
the glass particles are degraded. However, Billington et al. (2006) argue that
approximately 7% of the glass is consumed to produce the cement matrix. This degradation of the glass surface and cross-linking of polyacids is accompanied by a
rise in pH (Crisp and Wilson, 1974a,b) and the viscosity of the cement paste
(Wilson and Mclean, 1988).
8.4.2 Gelation phase
As the reaction continues, ions released from the glass accumulate and are removed
by precipitation as insoluble polyacrylates. Al31, Ca21, and F2 form metallic salt
bridges with free (COO2) groups resulting in the cross-linking of the polycarboxylate chains and ultimately leading to the setting. This process continues until all the
ions are insoluble. It is important to note that not all COOH groups lose their
hydrogen ions to form COO2 ions. This is because when most of the carboxylic
groups have ionized, the negative charge on the polymer chain increases. This
results in the positively charged ions becoming more strongly bound to the polymer
chains, hence making it difficult for the metal ions to replace them. Furthermore, as
the density of the cross-links increases, it hinders the movement of metal ions
toward carboxyl sites. Due to these reasons, the neutralization reaction does not
quite go to completion.
It has been shown that calcium polyacrylate is largely responsible for the initial
gelation and setting of the cement in phase-separated glasses producing a clinically
hard material within 410 minutes of mixing. This is followed by a slower formation of aluminum salts which may take up to 48 hours for completion (Crisp et al.,
1974a,b; Barry et al., 1979). However, FTIR analysis has shown that, finally, both
salts are present in equal quantities.
The fluoride and phosphate ions form insoluble salts and complexes. Na1 contributes to the formation of orthosilicic acid on the surface of the glass particles which
converts to silica gel as the pH rises. The silica gel assists in binding the powder to
the matrix (Mount and Hume, 1998).
Glass-ionomer cement: chemistry and its applications in dentistry
183
8.4.3 Maturation phase
Soon after the gelation phase, the material undergoes what is commonly known as
the “maturation phase.” During this stage, the material has been shown to increase
in CS. According to Wilson and Prosser (1982), this is due to the less mobile aluminum cross-linking the remaining the COOH acids or by replacing the already
cross-linked calcium ions. More recently, Pires et al. (2004) have pointed at the
maturation-related release of the more covalently bound “network forming” aluminum ions to complement the cross-linking phenomenon. Interestingly, Boyd and
Towler (2005) have observed a maturation phenomenon in a GIC formulated from
aluminum-free calcium-zinc-silicate glasses. Since the glass did not contain any
“less mobile” aluminum ions, it suggests the existence of other mechanisms to be
associated with improvements in mechanical properties as a result of maturation
phenomenon.
Wasson and Nicholson (1990) using inductively coupled plasma—optical emission spectrometry (ICP-OES) found that silica is released in large amounts during
the decomposition of the glass and hypothesized its role in cement formation. Such
a release has also been observed by De Maeyer et al. (2002) using FTIR analysis.
Wasson and Nicholson (1993) demonstrated the role of silica in the maturation process and associated it with the increase in CS of the cements. Although a possible
candidate, the authors did not look at the presence of factors other than silica.
Using IR and NMR analysis, Matsuya et al. (1996) have also related the increase in
CS with the silica phase in the matrix, but they too ignored the presence of any
complimentary mechanisms.
Apart from the above factors, hydration has also been associated with the maturation phenomenon. Wilson et al. (1979) found an increase in the ratio of bound to
unbound water with maturation and have correlated it with the increase in CS. The
presence of free and bound water has also been observed in silica desiccants. Since
the posthardened silica network formed in GIC has been found to be similar to that
of amorphous silica (Matsuya et al., 1996), it may give a possible explanation for
this phenomenon of free and bound water in GIC.
8.5
Fluoride release from glass-ionomer cements
GICs are known to release clinically beneficial amounts of fluoride (Guida et al,
2002; Khouw-Liu et al., 1999; Jones et al., 2003). The irony, however, is that leachable fluoride had not been intentionally included to make the cement suitable for
dental use, but it occurred as a constituent of several chemicals used in the manufacture of the glass (Williams et al., 2002).
8.5.1 Source of fluoride
It is not clear as to how and from where the fluoride ion arrives at the surface of
the cement. However, it is hypothesized that all intrinsic fluoride must initially
come from the glass (Williams et al., 2002). Fluoride in the glass is released into
184
Advanced Dental Biomaterials
the matrix during the setting reaction. An important point to note here is that the
fluoride is released from the cement along with sodium and perhaps calcium ions in
order to maintain the electrical neutrality of the cement, and due to this dependency
on other ions the amount of fluoride released from the cement cannot be determined
solely by the quantity of fluoride in the initial glass (Thevadass et al., 1996).
8.5.2 Mechanism of fluoride release
During the setting of GIC, the fluoride ions arise initially from the surface of the
glass particles which are then held in the siliceous gel of the matrix. Since fluoride
ions do not form part of the cement matrix, thus a continuous exchange of fluoride
can occur from the cement depending on the gradient of fluoride in the oral environment at any given time. However, the mechanism behind the release of fluoride
from GICs has not been understood completely, but all researchers seem to agree
on the kinetics associated with the fluoride release according to which at least two
processes are occurring simultaneously, that is, a short-term fluoride burst release
and a long-term fluoride release. This can be demonstrated by the equation below
which adequately and accurately describes the cumulative fluoride [F]c release
from a restorative glass ionomer in distilled water (De Moor and Verbeeck, 1998).
pffi
ð½FI tÞ
1β t
½Fc 5
t 1 t1=2
where [F]I 5 maximum value of fluoride released during short-term reaction;
t 5 time; t1/2 5 “half-life” of short-term release, that is, the time required for the
fluoride released by short-term reaction to reach half of its maximum value; β 5 a
constant which is measure for the driving force of the long-term release.
A large amount of the fluoride released from GICs is during the “short-term
release” phase which occurs within a few days of placement in the oral cavity. This
amount then declines sharply during the first week and stabilizes after 23 months.
The long-term release of fluoride is substantially lower, but it appears to be sufficient to prevent caries (Mount and Hume, 1998).
The process of diffusion seems to be associated with the long-term release of
fluoride from glass ionomers. This is evident by Forsten’s (1990) study which
showed the existence of a linear relationship between the amounts of fluoride
released and the square root of time, thus following the theory of simple diffusion.
Another study, by Williams et al. (1999), also pointed toward a relationship
between the surface area and the amount of fluoride released, which again shows
the existence of a diffusion mechanism. However, an erosive mechanism also seems
to complement the fluoride release since studies have shown an increase in fluoride
release in an acidic environment (Thevadass et al., 1996). This may account for the
morphological changes which are frequently observed.
8.5.3 Factors effecting fluoride release
Fluoride release has been shown to be dependent upon variables such as the composition of the glass and polyalkenoic acid, the relative proportions of the constituents
Glass-ionomer cement: chemistry and its applications in dentistry
185
in the cement mix, the mixing process, and the elution medium (De Witte et al.,
2000). The relationship between the composition of aluminosilicate glasses and its
effect on fluoride release can be observed from Williams et al.’s (2002) study
where a sodium-free glass LG26 released lower fluoride than a sodium-containing
glass G338. This may be attributed to the high solubility of sodium. However, in
glasses where calcium is substituted with strontium for the purpose of radiopacity,
a substantial increase in fluoride has not been observed. The only slight increase by
strontium has been attributed to its increased density which affects the powder/liquid mixing ratio (Guida et al., 2002).
The amount of fluoride release in different elution media is an interesting phenomenon to observe since the oral cavity provides an environment of varying pH
and ionic concentration. Various researchers have concurred that there is an
increase in fluoride release in an acidic environment, due to surface degradation
(De Moor and Verbeeck, 1998; Czarnecka et al., 2002). This increase in fluoride
release at a lower pH enhances the anticariogenic properties of GIC since the caries
process also decreases the pH of the environment surrounding the tooth.
Furthermore, their study also showed the release of more fluoride in an acidic environment. This increase in fluoride release was also previously observed by De
Moor and Verbeeck (1998). Hadley et al. (2000, 2001) have also observed the phenomenon of surface degradation on exposure of GICs to neutral NaF solution.
Since the solution used in this case was a neutral one, the presence of ions in the
elution medium may be a possible explanation for the surface roughness.
Among the various elution media used for fluoride release, artificial saliva is an
important one since it provides a close emulation of the oral environment. Mallakh
and Sarkar (1990) found that glass ionomers released more fluoride in deionized water
than in artificial saliva. This pattern of fluoride release was also observed by Williams
et al. (1997, 2001) using the same artificial saliva. Although the mechanism behind the
reduction has not been understood, but it has been proposed to be either due to the
higher ionic strength of the artificial saliva or probably the calcium in the artificial
saliva forms an insoluble calcium fluoride layer on the surface of the cement
(Williams et al., 2001). The findings of Williams et al. (1997, 2001) and Mallakh and
Sarkar highlights the difference in fluoride release in artificial saliva compared with
that in deionized water. This not only questions the clinical correlation of studies in
deionized water, but it also suggests that further work is required in this area in order
to understand the pattern of fluoride release in the oral environment.
8.6
Mechanical properties
8.6.1 Compressive strength
Compressive strength (CS) is the maximum stress a material can withstand under a
constant load over a given area. CS can be expressed by the following equation:
σ5
F
A
186
Advanced Dental Biomaterials
where F is the applied load in unit newton and A is the area in meters squared. CS
is the only strength test specified by the International Organization for
Standardization standard for water-based cements for use in dentistry (ISO 99172:2017). The ISO standard defines CS, relative to the mode of measurement, as:
c5
4F
πd2
where F is the maximum compressive force applied in unit newton, and d is the
sample diameter in millimeters.
Compared to the alternative mechanical strength tests, the CS test is relatively
simple and has a fast turnaround. However, the use of this test in the assessment of
GIC mechanical failure has been criticized since the 1990s (McCabe et al., 1990).
McCabe et al. (1990) found that the CS test is unreliable because of the
unacceptable variation between the test results. McCabe et al. (1990) proposed that
“standards should place less emphasis on the mean value of relatively small number
of test specimens and the use of a simple form of probability theory in which, say,
80 per cent of specimens are required to achieve a certain pass level” proposing
that some standards may need to increase the number of test specimens to achieve
meaningful results. Based on the works of Kendall (1978), Darvell (1990), Fennell
and Hill (2001a), and Baig and Fleming (2015) argue that stress at failure calculation does not take into account the failure mechanism operating during the test,
whereby cylindrical specimens fail by “some unresolved combination of tension
and shear” stresses. From international standards point of view, the minimum CS
value for a water-based restorative cement is 100 MPa, whereas for a water-based
lining cement the specified value is 50 MPa (ISO 9917-2:2017). Nevertheless, some
commercial GICs, such as the AMALGOMER (manufactured by Advanced
Healthcare Ltd, Kent, United Kingdom) considerably surpass mechanical properties
specified in the standard and can withstand loads over 400 MPa.
8.6.2 Flexural strength
An alternative approach to help us understand the mechanical properties of glass
ionomer cements is the assessment of their flexural strength (FS). Flexural strength
can be defined by the following equation:
σ5
F
bd
where F is the axial load applied at the fracture point; b is the width of the sample;
and d is the thickness of the sample (Fig. 8.3).
For the three-point bend measurement purposes (Fig. 8.3), the flexural strength
can be expressed by the following equation:
σ5
3FL
2bd2
Glass-ionomer cement: chemistry and its applications in dentistry
187
Figure 8.3 Schematic representation of three-point flexural bend test.
Figure 8.4 Flexural strength versus PAA molar mass (Fennell and Hill, 2001c).
where F is the axial load force applied, in unit newton; L is the length of the sample
support span; b is the width of the sample; and d is the thickness of the sample. In
the flexural strength measurement, fracture occurs at midpoint under tension. In a
study by Fennell and Hill (2001a) it was concluded that the dominant parameters
which have an effect on the FS of GICs are the poly(acrylic acid) (PAA) molar
mass (Fig. 8.4) and the PAA concentration (Fig. 8.5).
Prosser et al. (1984) also reported that the flexural strength of GICs depends on
the glass composition and the polyelectrolyte used to prepare them. The authors
noted that opaque and opal glasses containing crystallites tended to yield cements
with high FS. FS was also found to increase with increasing molecular weight of
the poly(acrylic acid). In water-setting cements, the strength of the cements was
shown to be critically dependent on the glass/polyacid ratio. In a study by Dowling
et al. (2012), compressive strength, three-point flexural strength (TFS), and biaxial
flexural strength (BFS) data from three commercially available GICs were
188
Advanced Dental Biomaterials
Figure 8.5 Flexural strength versus PAA concentration (Fennell and Hill, 2001b).
statistically compared for reproducibility (P 5 .05). Based on the statistical analysis
of this data, Dowling et al. (2012) found that TFS and BFS were reproducible; however, the experimental data were found to vary significantly, and as such the study
concluded that CS measurement is not a statistically valid measurement. The
authors could not show any statistical difference between TFS and BFS. The
authors also noted that the specimen fabrication for BFS is relatively simple and
less operator-dependent as compared to the specimen fabrication for TFS.
8.7
Esthetics
The development of the first glass ionomer cement in 1968 was considered to be a
big breakthrough in esthetic dentistry because the new cement was translucent.
Since the development of the first generation of GICs, the esthetics of modern
GICs have improved, mainly as a result of better understanding of the structureproperty relationship. Highly translucent glass ionomer cements are produced by
matching the refractive index (RI) of the glass component to the liquid component
to avoid light scattering at the glass-polysalt interfaces. However, other factors such
as the poly(acrylic acid) concentration and the particle size can also influence the
esthetics as well as other properties of the cement. Most commercial and model laboratory GIC glass compositions contain a significant amount of fluoride. It has
been shown that fluoride content in GIC glasses can be correlated to the refractive
index of the glasses (Duminis et al., 2018). Therefore, varying the fluoride content
in GIC glasses can be used as a tool to fine-tune the refractive index of the core
glass component so that it closely matches to the liquid component.
8.8
Chemical adhesion with tooth
One of the important properties of GICs is their chemical adhesion with the tooth
without the use of intermediate bonding material. The process of chemical adhesion
Glass-ionomer cement: chemistry and its applications in dentistry
189
is through two mechanisms. First is an ion exchange process where the polyacrylic
acid reacts with the hydroxyapatite in the tooth and forms bonds with calcium and
phosphate. The second mechanism is by hydrogen bonding with the collagen present in dentine. Although bond strength between GIC and tooth is weak, evidence
suggests that the bond is “self-healing,” that is, it can reform if it is broken.
8.9
Moisture sensitivity of glass-ionomer cements
During the early stages of setting, GICs are very sensitive to moisture/saliva contamination and desiccation as these can disrupt the matrix resulting in a weak
cement. It is essential that GICs be protected up to at least 24 hours after placement.
This can be achieved by applying Vaseline, cocoa butter, or varnishes over the surface of the material soon after placement.
8.10
Use of glass-ionomer cements in alternative
restorative technique
Alternative restorative treatment (ART), formerly known as atraumatic restorative
treatment, is defined as “a dental caries treatment procedure involving the removal
of soft, demineralised tooth tissue using hand instrument alone, followed by restoration of the tooth with an adhesive restorative material, routinely glass ionomer.”
This technique has been endorsed by the World Health Organization and the
International Association for Dental Research as a means of restoring and preventing caries. ART may be used to restore and prevent caries in young patients, uncooperative patients, or patients with special healthcare needs, or when traditional
cavity preparation and/or placement of traditional dental restorations are not feasible. GIC is the material of choice for ART, because of its bonding to enamel and
dentin, fluoride release, and ease of use. Van Hof et al. concluded, based on a
meta-analysis, that single-surface ART restorations using high-viscosity GIC in
both primary and permanent dentitions showed high survival rates, and that
medium-viscosity (traditional) GIC should not be used for ART restorations.
8.11
Nanoapatite-filled glass ionomers
GICs have undergone extensive developments and modifications since it was first
developed as ASPA. These include improvements in radiopacity, esthetics, and
mechanical properties. Of notable mention among these recent developments is
Glass Carbomer by GCP Dental, Netherlands. The glass ionomer contains nanofluorapatite/hydroxyapatite as a secondary filler in the formulation to enhance the
remineralization of the tooth tissue. Phosphate ions are essential in the remineralization of the tooth, however including too much phosphate in the glass composition
190
Advanced Dental Biomaterials
results in a slow setting material. In Glass Carbomer the manufacturers overcome
this problem by including apatite phase as a secondary filler. The nanofluor/
hydroxyapatite in the material acts as nuclei for apatite formation, thus promoting
remineralization. The enhanced remineralization is evident through the formation of
a “pseudo-enamel” apatite phase which has been reported by an in vivo study
(Duinen et al., 2004).
8.12
Thermo-cured glass ionomers
Thermo-curing is a relatively new technique which uses radiant heat to accelerate
the setting reaction of conventional GICs. This technique helps overcome the problem of early moisture sensitivity of GICs. Glass Carbomer is a commercially available GIC which has been specifically developed for use with thermo-curing.
Thermo-curing is achieved by a special light curing device which emits heat. These
portable handheld devices are available from Glass Carbomer manufacturer and are
like the LED light curing units used for dental composites. In a clinical setting,
thermo-curing is performed soon after placing the filling in the cavity by placing
the tip of the light-cured unit on the surface of the GIC. In the case of Glass
Carbomer, the manufacturer recommends a curing time of 90 seconds. Various
researchers have investigated the effects of thermo-curing on mechanical properties
of various GICs and have reported an increase in surface microhardness and FS.
One clinical study has reported the beneficial effect of thermo-curing on the success
rate of ART restorations for up to 18 months.
8.13
Resin-modified glass-ionomer cements
Resin-modified GICs (RMGICs) can be regarded as fast setting GICs with immediate resistance to water uptake and some protection from water loss. Their composition consists of calcium fluoroaluminosilicate glass powder which is mixed with the
liquid-containing hydroxyethylmethacrylate (HEMA), polyacrylic acid, and polymerization initiators. On mixing the powder with the liquid, two distinct types of
setting reactions occur:
G
G
acidbase neutralization and
free-radical addition polymerization.
These reactions may lead to the formation of two matrices, an ionomer salt
hydrogel and polyHEMA matrix with multiple cross-linking. Full properties
reached after maturation occurs as in an autocure system. Due to the presence of
resin phase, RMGIC is prone to polymerization exotherm and polymerization
shrinkage. Furthermore, since RMGICs contain less polyacrylic acid as compared
to conventional GICs, there may be an effect on the chemical adhesion with the
tooth. Although RMGICs initially provide improved mechanical properties, over
Glass-ionomer cement: chemistry and its applications in dentistry
191
time these properties tend to deteriorate due to water absorption by polyHEMA.
The water uptake also makes the RMGIC prone to intrinsic staining which cannot
be removed by polishing.
8.14
Glass ionomer as a “nondental” cement
Glass ionomers received considerable attention during the early 1990s as cements
in other branches of medicine. Excellent biocompatibility was reported
(Sasanaluckit et al., 1993), and in one study Meyer et al. (1993) argued that
although aluminum had found its way into the cells, there was no evidence of cytotoxicity, possibly due to the formation of nontoxic complexes with silica. Clinical
trials reported good results for use in procedures such as alveolar ridge to build up,
reconstruction following removal of bone tumors (Lindeque and Jonck, 1993), fixation of cochlear implants (Ramsden et al., 1992), and craniofacial reconstruction
surgery (Zollner et al., 1994). However, these materials received a major setback
when they were withdrawn from clinical use in France in 1994 (Renard et al.,
1994). This was following severe postoperative problems with two patients who
underwent translabrynthic otoneosurgery and bone reconstruction with GICs.
Extremely high levels of aluminum were observed in the lumbar cerebrospinal
fluid, serum, and urine. Since the case report of this incident is poorly written, it is
unclear if this event may have occurred due to operator error in the surgical technique. Following this series of events, researchers have produced several formulations of aluminum-free glasses for use in glass ionomers for such purposes. These
glasses either use zinc (Boyd and Towler, 2005) or iron to replace aluminum.
References
Aboush, Y.E., Jenkins, C.B., 1986. An evaluation of the bonding of glass-ionomer restoratives to dentine and enamel. Br. Dent. J. 161 (5), 179184.
Ames, W.V.B., 1892. A new oxyphosphate cement for crown setting. Dent. Cosmos. 24, 906.
Anusavice, K.J., 2003. Philips’ Science of Dental Materials, 11th ed. Elsevier, India.
Baig, M.S., Fleming, G.J., 2015. Conventional glass-ionomer materials: a review of the
developments in glass powder, polyacid liquid and the strategies of reinforcement. J.
Dent. 43 (8), 897912.
Barry, T.I., Clinton, D.J., Wilson, A.D., 1979. The structure of a glass-ionomer cement and
its relationship to the setting process. J. Dent. Res. 58, 10721079.
Boyd, D., Towler, M.R., 2005. The processing, mechanical properties and bioactivity of zinc
based glass ionomer cements. J. Mater. Sci. Mater. Med. 16 (9), 843850.
Causton, B.E., 1981. The physico-mechanical consequences of exposing glass ionomer
cements to water during setting. Biomaterials 2 (2), 112115.
Crisp, S., Wilson, A.D., 1974a. Reactions in glass ionomer cements: I. Decomposition of the
powder. J. Dent. Res. 53 (6), 14081413.
192
Advanced Dental Biomaterials
Crisp, S., Wilson, A.D., 1974b. Reactions in glass ionomer cements: III. The precipitation
reaction. J. Dent. Res. 53 (6), 14201424.
Crisp, S., Pringuer, M.A., Wardleworth, D., Wilson, A.D., 1974. Reactions in glass ionomer
cements: II. An infrared spectroscopic study. J. Dent. Res. 53 (6), 14141419.
Crisp, S., Ferner, A.J., Lewis, B.G., Wilson, A.D., 1975. Properties of improved glassionomer cement formulations. J. Dent. 3 (3), 125130.
Crisp, S., Kent, B.E., Lewis, B.G., Ferner, A.J., Wilson, A.D., 1980. Glass-ionomer cement
formulations. II. The synthesis of novel polycarobxylic acids. J. Dent. Res. 59,
10551063.
Czarnecka, B., Limanowska-Shaw, H., Nicholson, J.W., 2002. Buffering and ion-release by a
glass-ionomer cement under near-neutral and acidic conditions. Biomaterials 23,
27832788.
Darvell, B., 1990. Uniaxial compression tests and the validity of indirect tensile-strength. J.
Mater. Sci. 25 (2A), 757780.
Davidson, C.L., Mjör, I.A., 1999. Advances in Glass-Ionomer Cements. Quintessence Pub. Co.
Deb, S., Nicholson, J.W., 1999. The effect of strontium oxide in glass-ionomer cements. J.
Mater. Sci. Mater. Med. 10, 471474.
De Maeyer, E.A., Verbeeck, R.M., Vercruysse, C.W., 2002. Infrared spectrometric study of
acid-degradable glasses. J. Dent. Res. 81 (8), 552555.
De Moor, R.J., Verbeeck, R.M., 1998. Effect of acetic acid on the fluoride release profiles of
restorative glass ionomer cements. Dent. Mater. 14, 261268.
De Witte, A.M., De Maeyer, E.A., Verbeeck, R.M., Martens, L.C., 2000. Fluoride release
profiles of mature restorative glass ionomer cements after fluoride application.
Biomaterials 21, 475482.
Duminis, T., Shahid, S., Karpukhina, N.G., Hill, R.G., 2018. Predicting refractive index of
fluoride containing glasses. Dent Mater. 34 (5), e83e88. Available from: https://doi.
org/10.1016/j.dental.2018.01.024.
el Mallakh, B.F., Sarkar, N.K., 1990. Fluoride release from glass-ionomer cements in deionized water and artificial saliva. Dent. Mater. 6, 118122.
Fennell, B., Hill, R., 2001a. The influence of poly(acrylic acid) molar mass and concentration
on the properties of polyalkenoate cements—Part II Young’s modulus and flexural
strength. J. Mater. Sci. 36 (21), 51775183.
Fennell, B., Hill, R., 2001b. The influence of poly(acrylic acid) molar mass and concentration
on the properties of polyalkenoate cements—Part III—Fracture toughness and toughness. J. Mater. Sci. 36 (21), 51855192.
Fennell, B., Hill, R., 2001c. The influence of poly(acrylic acid) molar mass and concentration
on the properties of polyalkenoate cements—Part I—Compressive strength. J. Mater.
Sci. 36 (21), 51935202.
Fleck, D.J., 1902. The chemistry of oxyphosphates. Dent. Items Int. 24, 906.
Forsten, L., 1990. Short- and long-term fluoride release from glass ionomers and other
fluoride-containing filling materials in vitro. Scand. J. Dent. Res. 98, 179185.
Guida, A., Hill, R.G., Towler, M.R., Eramo, S., 2002. Fluoride release from model glass
ionomer cements. J. Mater. Sci. Mater. Med. 13, 645649.
Hadley, P.C., Billington, R.W., Pearson, G.J., Williams, J.A., 2000. Effect of monovalent
ions in glass ionomer cements on their interaction with sodium fluoride solution.
Biomaterials 21, 97102.
Hadley, P.C., Billington, R.W., Williams, J.A., Pearson, G.J., 2001. Interactions between
glass ionomer cement and alkali metal fluoride solutions: the effect of different cations.
Biomaterials 22, 31333138.
Glass-ionomer cement: chemistry and its applications in dentistry
193
Jones, F.H., Hutton, B.M., Hadley, P.C., Eccles, A.J., Steele, T.A., Billington, R.W., et al.,
2003. Fluoride uptake by glass ionomer cements: a surface analysis approach.
Biomaterials 24, 107119.
Kendall, K., 1978. Complexities of compression failure. Proc. R. Soc. London, Ser. A—
Math. Phys. Eng. Sci. 361 (1705), 245263.
Khouw-Liu, V.H., Anstice, H.M., Pearson, G.J., 1999. An in vitro investigation of a poly
(vinyl phosphonic acid) based cement with four conventional glass-ionomer cements.
Part 1: Flexural strength and fluoride release. J. Dent. 27, 351357.
Lindeque, B.G., Jonck, L.M., 1993. Ionogran—an ionomeric micro implant in bone tumour
reconstruction. A clinical evaluation. Clin. Mater. 14 (1), 4956.
Matsuya, S., Maeda, T., Ohta, M., 1996. IR and NMR analyses of hardening and maturation
of glass-ionomer cement. J. Dent. Res. 75 (12), 19201927.
McCabe, J., Watts, D., Wilson, H., Worthington, H., 1990. An investigation of test-house
variability in the mechanical testing of dental materials and the statistical treatment of
results. J. Dent. 18 (2), 9097.
McLean, J.W., Gasser, O., 1985. Glass-cermet cements. Quintessence Int. 16, 333343.
McLean, J.W., Nicholson, J.W., Wilson, A.D., 1994. Proposed nomenclature for glassionomer dental cements and related materials. Quintessence Int. 25, 587589.
Meyer, U., Szulczewski, D.H., Barckhaus, R.H., Atkinson, M., Jones, D.B., 1993. Biological
evaluation of an ionomeric bone cement by osteoblast cell culture methods.
Biomaterials 14 (12), 917924.
Mount, G.J., 1998. Clinical performance of glass-ionomers. Biomaterials 19, 573579.
Review.
Mount, G.J., Hume, W.R., 1998. Preservation and Restoration of Tooth Structure. Mosby,
London.
Mount, G.J., Makinson, O.F., 1982. Glass-ionomer restorative cements: clinical implications
of the setting reaction. Oper. Dent. 7, 134141.
Nicholson, J.W., 1998. Chemistry of glass-ionomer cements: a review. Biomaterials 19,
485494. Review.
Paddon, J.M., Wilson, A.D., 1976. Stress relaxation studies on dental materials. 1. Dental
cements. J. Dent. 4 (4), 183189.
Pires, R., Nunes, T.G., Abrahams, I., Hawkes, G.E., Morais, C.M., Fernandez, C., 2004.
Stray-field imaging and multinuclear magnetic resonance spectroscopy studies on the
setting of a commercial glass-ionomer cement. J. Mater. Sci. Mater. Med. 15 (3),
201208.
Prosser, H.J., Powis, D.R., Brant, P., Wilson, A.D., 1984. Characterization of glass-ionomer
cements. 7. The physical properties of current materials. J. Dent. 12, 231240.
Ramsden, R.T., Herdman, R.C., Lye, R.H., 1992. Ionomeric bone cement in neuro-otological
surgery. J. Laryngol. Otol. 106 (11), 949953.
Renard, J.L., Felten, D., Bequet, D., 1994. Post-otoneurosurgery aluminium encephalopathy.
Lancet 344 (8914), 6364.
Rudel, C., Zollner, W., 1994. Ionomeric cement—a bone glue for device fixation. Ear Nose
Throat J. 73 (3), 189191. Review.
Sasanaluckit, P., Albustany, K.R., Doherty, P.J., Williams, D.F., 1993. Biocompatibility of
glass ionomer cements. Biomaterials 14 (12), 906916.
Setchell, D.J., Teo, C.K., Khun, A.T., 1985. The relative solubilities of four modern glassionomer cements. Br. Dent. J. 158 (6), 220222.
Smith, D.C., 1998. Development of glass-ionomer cement systems. Biomaterials 19,
467478.
194
Advanced Dental Biomaterials
Thevadass, K.P., Pearson, G.J., Anstice, H.M., Davies, E.H., 1996. Method for enhancing the
fluoride release of a glass-ionomer cement. Biomaterials 17, 425429.
Van Duinen, R.N., Davidson, C.L., De Gee, A.J., Feilzer, A.J., 2004. In situ transformation
of glass-ionomer into an enamel-like material. Am. J. dent. 17, 223227.
Wasson, E.A., Nicholson, J.W., 1990. A study of the relationship between setting chemistry
and properties of modified glass-poly(alkenoate) cements. Br. Polym. J. 23, 179183.
Wasson, E.A., Nicholson, J.W., 1993. New aspects of the setting of glass-ionomer cements.
J. Dent. Res. 72 (2), 481483.
Williams, J.A., Billington, R.W., Pearson, G.J., 1992. The comparative strengths of commercial glass-ionomer cements with and without metal additions. Br. Dent. J. 172,
279282.
Williams, J.A., Billington, R.W., Pearson, G., 1997. Silver and fluoride ion release from
metal-reinforced glass-ionomer filling materials. J. Oral Rehabil. 24, 369375.
Williams, J.A., Billington, R.W., Pearson, G.J., 1999. The influence of sample dimensions on
fluoride ion release from a glass ionomer restorative cement. Biomaterials 20,
13271337.
Williams, J.A., Billington, R.W., Pearson, G.J., 2001. A long term study of fluoride release
from metal-containing conventional and resin-modified glass-ionomer cements. J. Oral
Rehabil. 28, 4147.
Williams, J.A., Billington, R.W., Pearson, G.J., 2002. The glass ionomer cement: the sources
of soluble fluoride. Biomaterials 23, 21912200.
Wilson, A.D., 1989. Developments in glass-ionomer cements. Int. J. Prosthodont. 2,
438446.
Wilson, A.D., Kent, B.E., 1972. A new translucent cement for dentistry. The glass ionomer
cement. Br. Dent. J. 132, 133135.
Wilson A.D., McLean J.W., 1988. Glass-Ionomer Cement. Quintessence, Chicago, IL.
Wilson, A.D., Prosser, H.J., 1982. Biocompatibility of the glass ionomer cement. J. Dent.
Assoc. S. Afr. 37 (12), 872879.
Wilson, A.D., Groffman, D.M., Powis, D.R., Scott, R.P., 1986. A study of variables affecting
the impinging jet method for measuring the erosion of dental cements. Biomaterials 7
(3), 217220.
Wilson, A.D., Hill, R.G., Warrens, C.P., Lewis, B.G., 1989. The influence of polyacid molecular weight on some properties of glass-ionomer cements. J. Dent. Res. 68 (2), 8994.
Wilson, A.D., Paddon, J.M., Crisp, S., 1979. The hydration of dental cements. J. Dent. Res.
58 (3), 10651071.
Further reading
Brune, D., 1982. Heat treatment of glass ionomer, silicate, zinc phosphate and zinc polycarboxylate cements. Scand. J. Dent. Res. 90 (5), 409412.
Fejerskov, O., Ekstrand, J., Burt, B.A. (Eds.), 1996. Fluoride in Dentistry. second ed.
Munksgaard, Copenhagen.
Fusayama, T., Katayori, T., Nomoto, S., 1963. Corrosion of gold and amalgam placed in contact with each other. J. Dent. Res. 42, 11831197.
Hellwig, E., Lennon, A.M., 2004. Systemic versus topical fluoride. Caries Res. 38, 258262.
Jenkins, G.N., 1999. Review of fluoride research since 1959. Arch. Oral. Biol. 44, 985992.
Glass-ionomer cement: chemistry and its applications in dentistry
195
Nicholson, J.W., Czarnecka, B., 2004. The interaction of lactic acid-glass cements with aqueous solutions. J. Mater. Sci. Mater. Med. 15 (2), 151154.
Nicholson, J.W., Tawfik, H., Czarnecka, B., 2002. A study of cements formed by aqueous
lactic acid and aluminosilicate glass. J. Mater. Sci. Mater. Med. 13 (4), 417419.
Schmidt, W., Purmann, R., Jochum, P., Gasser, O., 1980. Mixing compounds for glassionomer cements and use of a copolymer for preparing the mixing components. Eur.
Pat. Appl. 24, 056.
Ten Cate, J.M., 2004. Fluorides in caries prevention and control: empiricism or science.
Caries Res. 3825438257.
Towler, M.R., Bushby, A.J., Billington, R.W., Hill, R.G., 2001. A preliminary comparison of
the mechanical properties of chemically cured and ultrasonically cured glass ionomer
cements, using nano-indentation techniques. Biomaterials 22 (11), 14011406.
Wilson, A.D., Crisp, S., Abel, G., 1977. Characterization of glass-ionomer cements. 4. Effect
of molecular weight on physical properties. J. Dent. 5 (2), 117120.
Impression materials for dental
prosthesis
9
Payam Zarrintaj1,2,3, Sahba Rezaei4, Seyed Hassan Jafari4,
Mohammad Reza Saeb2,3,5, Shadi Ghalami6, Mahsa Roshandel6,
Brouki Milan Peiman7,8, Daghigh Ahmadi Ehsaneh9, Farshid Sefat10,11
and Masoud Mozafari7,8
1
Polymer Engineering Department, Faculty of Engineering, Urmia University, Urmia, Iran,
2
Color and Polymer Research Center (CPRC), Amirkabir University of Technology, Tehran,
Iran, 3Advanced Materials Group, Iranian Color Society (ICS), Tehran, Iran, 4School of
Chemical Engineering, College of Engineering, University of Tehran, Tehran, Iran,
5
Department of Resin and Additive, Institute for Color Science and Technology, Tehran,
Iran, 6Department of Anatomy and Pathology, University of Siena, Siena, Italy, 7Cellular
and Molecular Research Center, Iran University of Medical Sciences, Tehran, Iran,
8
Department of Tissue Engineering & Regenerative Medicine, Faculty of Advanced
Technologies in Medicine, Iran University of Medical Sciences, Tehran, Iran, 9Centre for
Nanohealth, College of Engineering, Swansea University, Swansea, United Kingdom,
10
Biomedical and Electrical Engineering Department, School of Engineering,
University of Bradford, Bradford, United Kingdom, 11Interdisciplinary Research Centre
in Polymer Science & Technology (IRC Polymer), University of Bradford, Bradford,
United Kingdom
Chapter Outline
9.1 Introduction 198
9.2 Elastic impression materials
9.2.1
9.2.2
9.2.3
9.2.4
9.2.5
9.3 Inelastic impression materials
9.3.1
9.3.2
9.3.3
9.3.4
200
Polyethers 200
Polysulfide 201
Alginate 201
Agar 202
Silicones 202
204
Impression wax 204
Impression compound 205
Impression plaster 205
Metallic oxide pastes (zinc oxideeugenol impression paste) 206
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00009-8
Copyright © 2019 Elsevier Ltd. All rights reserved.
198
Advanced Dental Biomaterials
9.4 Characteristics of impression materials
9.4.1
9.4.2
9.4.3
9.4.4
9.4.5
9.5 Conclusion and future perspective
References 212
9.1
207
Dimensional accuracy/dimensional stability 207
Wettability 208
Elastic recovery/flexibility 208
Mechanical properties 209
Miscellaneous 209
212
Introduction
Biomedical scientists have endeavored to repair the organs, mainly with the aid of
regeneration or implanting strategies (Chiu et al., 2017; Zarrintaj et al., 2017b;
Bakhshandeh et al., 2017). Dental health issues are related to the esthetic features of
people who naturally desire for being perfectly evaluated for their beauty; hence, a
wide range of materials have been utilized in dentistry with miscellaneous features
from both beauty and health-care views (Hafshejani et al., 2017; Zamanian et al.,
2013; Zarrintaj et al., 2018a). Indeed the key imprints of such concerns are impression
materials (IMs) that have been widely used in dentistry. IMs have been utilized in
prosthodontics (e.g., denture), orthodontics, restoration, maxillofacial prosthetics, diagnosis/treatment planning, and dental implants. IMs have been known as negative
imprints of the mouth tissues, which are utilized for the positive formation of the teeth
and juxtaposing tissues model. Various materials exhibit the appropriate properties as
candidates for IMs, these can be classified into elastic (nonrigid) and inelastic (rigid)
materials. Common elastic materials, when examined clinically, are reversible hydrocolloids, such as agar, which work on the basis of phase change caused by temperature
rise; irreversible hydrocolloids such as alginate salt; elastomeric materials such as silicones; and polyethers. Plasters, zinc oxide, and eugenol-based impression pastes are
categorized as rigid/inelastic IMs. Such materials are used for the dental arches using
dental impression trays (Ting-shu and Jian, 2015). Fig. 9.1 depicts the restoration the
lost teeth using IMs (Bhakta et al., 2011).
Typically, choosing the appropriate substance for a particular clinical usage/
application depends on either expense or precision. For designing more precise
materials, when they are needed for a special purpose and not routinely, particular
considerations are required. For cases where undercuts are not present among the
recording surfaces, stiff substances are preferred. Rigid IMs can also be utilized in
edentulous subjects, where soft tissue (compressible) undercuts are present
(McCabe and Walls, 2013). The reason for using the impression tray is to prepare
the supporting matrix for the IMs before simply inserting the impression into the
mouth. In general, two types of trays are available: custom-made and stock trays
(Marotti et al., 2014). Stock trays are supplied in various shapes and size in order to
help the clinician to choose the tray that fits well to the patient’s mouth. Such trays
are often either under- or overextended in relation to the extent of the oral soft and
Impression materials for dental prosthesis
199
Figure 9.1 Exposed fixture head after removal of the healing abutment (A); closed tray
impression coping screwed in place (B); light-bodied IM syringed around impression coping
(C); impression taken in a stock tray (D); impression with details of soft tissue around the
implant and adjacent teeth (E); and impression coping repositioned into the impression (F)
(Bhakta et al., 2011).
hard tissues, which need to be recorded for the clinical purposes so as to facilitate
modification if needed (Pastoret et al., 2017). On the other hand, custom-made trays
are constructed on the study casts of a patient’s mouth that have been obtained with
IMs, thus having a greater accuracy when compared to the stock trays. For recording
the oral soft tissues, such trays should be suitably extended in all orientations. Some
methods are used to stick IMs to the trays including puncturing perforation in the tray,
utilizing adhesives, and rim lock (McCabe and Walls, 2013; Tripathi et al., 2017).
IMs can be applied in liquid state or solid-like state to form the shape of dentition and
the surrounding structures of the oral cavity before being set. Materials used should
possess the following acceptable features: they should have pleasant esthetic color/
taste/odor with no releasable toxic ingredients, should be biocompatible with no irritation to the tissue, have an appropriate shelf-life, be affordable, be dimensionally stable,
and have sufficient mechanical strength. Techniques for taking impressions can be
defined as mucostatic (normal resting position), mucocompressive (compression
position), and selective pressure techniques (Oh and Morris, 2017). In order to
construct a proper cast, IMs should be scrutinized; fulfilling this aim, in this overview,
IMs and their properties are discussed. In the following sections, first, we focus on
elastic IMs, followed by inelastic IMs, and finally their characteristics.
200
9.2
Advanced Dental Biomaterials
Elastic impression materials
9.2.1 Polyethers
Among the elastomers, polyethers are the least hydrophilic; therefore they are
preferably chosen for moisture condition uses to capture preparation margins adequately; moreover, their wetting feature facilitates the fabrication of a gypsum
cast. It can be prepared by the monophase impression technique or syringe-andtray method (Fig. 9.2) (Rafael and Liebermann, 2017; Livaditis, 1998). Polyether
has some advantages, such as highly hydrophilic, high-to-moderate stability, good
accuracy, impressible in a monophase transition state, available in wide range of
viscosity, appropriate tear resistance, high modulus, and proper elastic recovery.
On the other hand, it suffers from being too stiff, susceptible to moisture absorption, and with potential for allergic reactions (Von Fraunhofer, 2013). Cationic
ring-opening polymerization of ethylene imine controls the polyether setting
behavior (Sakaguchi and Powers, 2012). New emerging polyethers exhibit proper
flexibility that is essential for its facile removal from the mouth. Because of water
absorption characteristics, polyethers should not be fully immersed in the water to
prevent distortion (Powers and Wataha, 2017). It was observed that exposing
polyether to immersion disinfection deteriorates its wettability potential. Sodium
hypochlorite and phenol enhance its wettability, while iodophor has the inverse
effect (Shetty et al., 2013).
Figure 9.2 Matrix filled with high-viscosity polyether impression material by the use of
impression syringe to minimize entrapment of air (Livaditis, 1998).
Impression materials for dental prosthesis
201
9.2.2 Polysulfide
Polysulfide, because of its nauseous taste, is not solely preferable for a dental prosthesis. It has been introduced as a paste to the two-component systems after mixing.
Condensation polymerization helps the polysulfide setting process to yield a crosslinked rubbery polymer with high molecular weight, while together with polysulfide
water forms as a by-product (Shoemaker et al., 2012; Guiraldo et al., 2017).
Polysulfide enjoys the advantages of proper tear resistance, dimension stability,
appropriate accuracy, and flexibility, whereas unpleasant taste, prolonged setting
time, and mixing difficulties limit its capabilities (Levartovsky et al., 2011). Silica
and TiO2 are being added as fillers to the base paste and have revealed promise in
altering polysulfide viscosity. The set reaction consists of the oxidation of the SH
groups that cause cross-linking and chain extension to yield elastomeric properties,
which can be easily removed from the mouth, comparably easier than that of polyether (Hamalian et al., 2011; Yang et al., 2016). Its prolonged reaction results in a
long-term dimensional change, while its setting time takes a value around 10 minutes with setting shrinkage (Von Fraunhofer, 2013). Due to the hydrophobic nature
of polysulfide, it has been desirable to be utilized in milieu therapy without saliva
and blood (Hamalian et al., 2011).
9.2.3 Alginate
Alginate is an irreversible hydrocolloid resulting from a solgel transition caused
by chemical reaction (Serrano-Aroca et al., 2017). Alginate is a polysaccharide presenting excellent biocompatibility with tissues (Atoufi et al., 2017). When exposed
to calcium ions (Ca21), alginate aqueous solution cross-links. Sodium phosphate
can be used as a retarder for regulating the setting time that has been found to vary
from 1 to 5 minutes with a mild rise in water temperature (Fokkinga et al., 2017).
Alginate is normally utilized when the accuracy is not so important. Elastomeric
materials can be used as a secondary layer over the alginate. Thanks to its low
price, easy flow, swift setting time, and minimal displacement, alginate can play
the role of an IM. On the other hand, low-dimensional stability, inappropriate tear
strength, and bubbling during mixing place some questions on alginate usage. The
fraction of powder regulates the properties of the final product, such as gel strength,
setting reaction, flow, and stability (Al-Enazi and Naik, 2016). It was reported that
the gelation time is governed by the secondary materials such as disinfection
liquids. For instance, chlorhexidine increases gelation time increment, while sodium
hypochlorite decreases the gelation time. Alginate gelation is related to ion availability so that a higher content of ions results in fast gelation; moreover, ion concentration affects the mechanical stability (de Azevedo Cubas et al., 2014).
Chlorhexidine will consume the ions and reduce the cross-link density (CLD);
hence, the mechanical stability of alginate plunges down. On the other hand,
sodium hypochlorite generates ions leading to the amelioration of the CLD and
mechanical stability enhancement (Amalan et al., 2013). Operational conditions,
202
Advanced Dental Biomaterials
such as temperature and humidity in storage and transport, manipulation of instructions, and ingredients ratio, govern the final product properties, such as distortion
and stability (Kulkarni and Thombare, 2015).
9.2.4 Agar
Agar is a kind of polysaccharide obtained from seaweed. It is a reversible hydrocolloids yielded via solgel transition under the influence of temperature, so that exhibits thermogelling behavior (Han et al., 2017; Zarrintaj et al., 2017a). Agar
provides high accuracy that makes it effective for use in crowns and bridges (fixed
prosthodontics); moreover, because of its thermoreversible behavior it can be used
several times. Because of the hydrophilicity of agar, dental drying is not mandatory,
and it can be used in the wet state. Agar formation necessitates the water bath and
rim-lock trays with coiled edges, which can allow water to pass through to cool
down the agar for the sake of setting (Iwasaki et al., 2016). Agar exhibits viscoelastic behavior, and its elastic recovery can be promoted by removing the impression
quickly so that the material tolerates the stress for a concise time; furthermore, agar
can be torn by applying a very low amount of stress because of poor mechanical
properties. The dimensional stability of materials is not desirable due to high water
uptake of gel (McCabe and Walls, 2013; Atoufi et al., 2017). Pouring the impression at several time intervals may bring about dimensional fluctuations. On this
issue, sequential pouring of the IMs (alginate, agar, and polyvinyl siloxane) for several times on dimensional precision of the impressions was recommended. It was
shown that when the materials were poured instantly, their dimensional exactness
did not differ noticeably, while when the same materials were repoured after
30 minutes (the second pour), dimensional accuracy of alginate indicated the most
alteration compared to the other aforementioned materials (Craig, 1988).
9.2.5 Silicones
9.2.5.1 Polysiloxanes
Polysiloxane (PVS), usually called addition silicone, has been utilized widely in
advanced restorative dentistry. Its grades are classified based on the filler content
that controls its properties, such as thickness and flowability (Wang, 2016). The
most well-known forms are extra light-bodied (low filler content), light-bodied, universal or medium-bodied, heavy-bodied, and putty (high filler content). A paste-topaste system and additional polymerization (without by-product) have been used
for synthesizing such silicone leading to a stable production. However, the hydrophobicity of such material necessitates accurate moisture control in applying time
(Goodall et al., 2015). Monophase polyvinyl siloxane and polyether elastomeric
IMs have been widely studied. It was revealed that impregum, Penta, and aquasil
acted better under the dry state; also, impregum acted better than the aquasil in
both situations (Vadapalli et al., 2016). New hydrophilic elastomeric IMs have been
recommended for diminishing the voids and distortion in the impressions. Soft
Impression materials for dental prosthesis
203
Figure 9.3 Polysiloxane (PVS) impression in a custom tray for fixed prosthodontics (Punj
et al., 2017).
polyether exhibited higher strain and lower tensile strength in comparison with
addition silicones. Moreover, the tear and tensile strength of heavy-bodied materials
were higher than those of light-bodies (Lu et al., 2004). Cole et al. synthesized
thiol- and allyl-functionalized siloxane oligomers using radical-mediated polymerizations to gain swift set elastomeric dental IMs. Thiol-ene siloxane was crosslinked through the redox-initiated reaction. Properties of such dental impression
were adjusted with plasticizer and kaolin filler; moreover, it exhibited a high accuracy (Cole et al., 2014). PVS should be cast in appropriate trays to use as an IM
(Fig. 9.3) (Punj et al., 2017).
9.2.5.2 Condensation silicone
The main materials of condensation silicones are dimethyl siloxane with CaCO3 or
silica as a filler. Stannous octoate and alkyl silicate act as catalysts. Ethyl alcohol is
the polymerization by-product that leads to high shrinkage during setting. Such silicones set quickly down on the tooth and are considered to get rigid to some extent
(Von Fraunhofer, 2013). The condensation silicones are available in putty, paste, or
light-bodied forms to be formed accurately. Hydrophobicity, shrinkage, and releasing their by-products, however, are disadvantages of condensation silicones to be
taken into account before choosing them for dental treatments. Disinfectant within
the silicone-based impression should be carefully controlled because it was reported
that the dimensional stability of such products varies formulation to formulation. It
is noteworthy that disinfectants containing benzalkonium chloride and glutaraldehyde are not deteriorative to the dimensional consistency of the aforementioned
elastomeric materials (Sinobad et al., 2014).
204
Advanced Dental Biomaterials
9.2.5.3 Vinyl polyether siloxane
This substrate is a novel IM receiving attention because of the simplicity of removal
of additional silicone and the hydrophilicity of polyether simultaneously. Based on
such specifications, it is a useful material for certain cases, such as narrow, deep
gingival crevices (Punj et al., 2017). It was reported that VPS exhibited the appropriate dimensional stability (Nassar et al., 2013). Vinyl polyether silicone (VPES)
and vinylpolysiloxane (VPS) were comparable regarding dimensional stability and
surface detail reproduction after the disinfection process and long-time storage (Din
et al., 2017). Investigations demonstrated that these materials are stable after
2-week storage; however, VPES showed less dimensional alteration compared to
the VPS. Also, the disinfected species of both substrates were more consistent than
the pristine ones. In vitro setting revealed that the VPES had enough dimensional
stability and surface accuracy (Nassar and Chow, 2015).
9.3
Inelastic impression materials
9.3.1 Impression wax
Varieties of natural waxes and resins have been utilized in dentistry for defined
applications. Waxes refer to thermoplastic materials solidifying at ambient temperature and being molten without decomposition, which consist of two or more
ingredients for the construction of nonmetallic denture bases (Powers and Craig,
1978). Dental waxes have a large thermal expansion coefficient. They can be
expanded upon temperature rise and vice versa. The mechanical features of waxes
depend inversely with temperature, but overall, their compressive strength and
elastic modulus are poor. Waxes can be derived from natural sources, such as
mineral (paraffin, microcrystalline, and montan), plant (carnauba, cocoa butter),
insect (beeswax), animals (spermaceti), or from synthetic materials such as polyethylene, polyoxyethylene glycol, halogenated hydrocarbon, and hydrogenated
(Tinto et al., 2017). Waxes, based on their usage, can be categorized into three
groups in dentistry including pattern wax (inlay wax, casting wax, and base plate
wax), processing wax (boxing wax, utility wax, and sticky wax), and impression
wax (corrective wax and bite plate wax). The greatest disadvantage of wax is its
distortion (Tinto et al., 2017). Conventional waxes consist of a paraffin wax with
a low melting point and beeswax in a ratio of 3:1. This proportion assures that at
mouth temperature, an appropriate flow is expectable. This kind of IM is not
common in recording thorough impressions; in fact, they are used for the modification of small defects in other impressions, especially the zinc oxideeugenol
impressions (Von Fraunhofer, 2013). Waxes belong to the thermoplastic substances that are able to flow at mouth temperature. These waxes can fill the sections of the impressions not receiving adequate material or imperfections caused
by the air blow with the aid of brushing. Prior to utilizing the wax in defective
Impression materials for dental prosthesis
205
parts of the impressions or impression trays, it should be melted. It is necessary
to give the material enough time when it is in the mouth to reach the oral temperature as it should undergo plastic flow to record the denture bearing area more
precisely (McCabe and Walls, 2013).
9.3.2 Impression compound
Impression compounds (ICs) are categorized as thermoplastic substances available
in sheet or stick form. Such compounds have been produced by combining waxes,
thermoplastic resins, fillers, and coloring agents. Some additives, such as shellac,
stearic acid, and gutta-percha, can be added to the compound for plasticity enhancement. ICs softening takes a long time to complete because of low thermal conductivity of the ICs. It was observed that the shrinkage occurs after removal due to the
high thermal expansion coefficient of ICs. Low thermal conductivity and high thermal expansion coefficient lead to the creation of internal stresses during the temperature fall form softening to the ambient degree resulting in distortion (Mete et al.,
2017). Low-fusing substances have been used as IMs to aid flow at temperatures
above 45 C and are available in sheet or stick form. In order to record the impressions of edentulous ridges, the sheet form is preferable, while the stick form is
suitable for recording the impressions of single crowns. The method for softening
the stick form is using a flame, whereas to soften the sheet a water bath is used. It
is important to notice that during softening the stick material’s direct exposure to
flame should be avoided to avoid ignition or boiling. Regarding the sheet forms, the
softening time in water bath should be controlled, since if the submerged time is
long, some important components, such as stearic acid, may be leached out. Higher
fusing ICs can be applied for fabricating impression trays (McCabe and Walls,
2013; Von Fraunhofer, 2013; Anusavice et al., 2013).
9.3.3 Impression plaster
Impression plasters (IPs) have conventionally been utilized as casting materials and
IMs for edentate patients. The components of the IP are calcined, β-calcium sulfate
hemihydrate that is mixed with water to trigger a reaction resulting in the formation of
calcium sulfate dehydrate (Oppedisano, 2013). The ratio of water/powder affects mixture constancy and setting time. Controlling the behavior of IPs is an important factor;
hence, some additives have been added to the compound. In order to decrease the setting expansion of the plasters, antiexpansion agents, such as potassium sulfate
(K2SO4), have been utilized. It is reported that such agents speed up the setting reaction. Borax is also combined as a retarder to provide the dentist with an opportunity to
control the setting features. Pigments, such as alizarin, can be utilized to make a difference between the impression and the mold (Dai et al., 2014). Conventional plaster
casting materials, due to the adhesion to the mold, necessitate the use of releasing
agents, but newly blended plaster is fabricated from acrylic resin or shellac to allow
206
Advanced Dental Biomaterials
easy separation. The disinfection process of IPs involves immersion in sodium hypochlorite. These materials are fragile, and whenever the pressure or tensile force is
applied, they fracture; thus, they cannot be used in undercut conditions. IPs have been
used for recording impressions of highly mobile soft tissues overlying the residual
alveolar bone. Moreover, IPs should be preserved in the dry state, as water absorbed
from the humid state causes setting time extension (Von Fraunhofer, 2013).
9.3.4 Metallic oxide pastes (zinc oxideeugenol impression
paste)
Impression paste has been utilized to take the secondary impressions for a complete
denture and consists of base part (zinc oxide) and catalyst paste (eugenol), which
are mixed with a stainless steel spatula for about 1 minute. Zinc oxide is accompanied with vegetable or mineral oil, used for plasticizing, and also helps to neutralize
the irritation caused by eugenol. Eugenol is usually available with rosin leading to
smooth and homogeneous materials and also facilitating the reaction pace. The
color of the zinc oxide paste is white, while eugenol paste is reddish brown. The
color contrast helps in determining the perfect mixing, since in this state, the mixture should show a homogenous color (Manappallil, 2015). These substrates are
divided into two main groups: hard paste (Type 1) for which the terminal set comes
to pass within 10 minutes and soft paste (Type 2) that indicates a final set occurrence within 15 minutes. After the final set the impression can be removed from the
mouth. The setting reaction is ionic in nature. Hence, ion concentration is an important factor in the reaction proceeding that can be affected by temperature and
humidity, and ionizable salt also affects the reaction rate. Initially, ZnO
hydrolyzes and reacts with eugenol to achieve zinc eugenolate salt
(2C10H12O2 1 ZnO!Zn(C10H11O2)2 1 H2O) (Luengo et al., 2017). It was reported
that an allergic response to the irritation can occur in some patients, as the eugenol
leaches out and reaches the soft tissue. In such cases, ZOE-like materials, that is,
eugenol-free zinc oxide impression pastes, are useful. ZOE-like materials are the
products of the reaction between zinc oxide and different carboxylic acids, such as
orthoethoxybenzoic acid. These acids are utilized instead of eugenol. In order to
diminish the tissue burning sensation, oil of cloves (including 70%85% eugenol)
can be used instead of pure eugenol in the first tube. Regarding disinfection, a 2%
alkaline glutaraldehyde is utilized through the steps as previously stated for ICs. In
the case of dimensional accuracy the impression pastes are reliable materials as less
than 0.1% shrinkage happens during setting. The impression pastes can be maintained without any change in shape arising from the relaxation or another motive of
the distortion. This state can be assured if the material used in the tray structure
shows dimensional stability (Anusavice et al., 2013). All the mentioned materials
should be used with the appropriate tray to exhibit the functional performance. 3Dprinted trays showed better properties, such as uniform thickness distribution of
IMs, than conventional ones (Fig. 9.4) (Sun et al., 2017).
Impression materials for dental prosthesis
207
Figure 9.4 Design process of the digital 3D-printed tray [(AD) maxilla and (EH)
mandible]. (A and E) The scanned data of the primary impression. (B) and (F) The
impression is trimmed to the appropriate range. (C and G) The main part of the tray and the
tissue stop. (D and H) A handle is added to the tray. The finished trays [(AiDi) manual tray
and (EiHi) digital tray]. (Ai and Ei) A maxillary tray with a tissue stop. (Bi and Fi) A
mandibular tray with a tissue stop. (Ci and Gi) A maxillary tray without a tissue stop. (Di and
Hi) A mandibular tray without a tissue stop (Sun et al., 2017).
9.4
Characteristics of impression materials
9.4.1 Dimensional accuracy/dimensional stability
Viscosity has a crucial role in determining the accuracy of the detail reproduction.
In fact, a low viscosity or degree of pseudoplasticity helps to record the surface segments precisely (Hamalian et al., 2011). When fixing the IM into the patient’s
mouth, it should be in the fluid state. The capability of the IMs to preserve the
material accuracy over time indicates their dimensional stability; however, by the
phrase dimensional accuracy, the absence of dimensional change for a short time
after removing from the mouth and during setting is considered (Anusavice et al.,
2013). The dimensional accuracy of some materials is time dependent, reported for
the case of elastomeric IMs, including polyvinyl siloxane, polyether, and polysulfide. In other words the highest level of dimensional accuracy corresponds to the
product collected right after the polymerization is completed, while it diminishes
during the storage of IMs over a prolonged period (Rubel, 2007). Materials with
low shrinkage have been chosen to be utilized as dental impressions (Hamalian
208
Advanced Dental Biomaterials
et al., 2011). For instance, polyvinyl siloxane and polyether can keep their dimensional accuracy for about 12 weeks after making the impression (Rubel, 2007).
PVS can be infinitesimally poured into the mold during the operation period,
whereas since polyether can absorb humidity from the environment and swell, it is
better for polyether to be poured within 1 hour after ejection from the mouth.
Regarding polysulfide and condensation silicone, as by-products accompany their
polymerization during the setting reaction, water and volatile ethyl alcohol should
be poured within 30 minutes after ejection from the mouth because such byproducts volatilize from the set impression and cause distortion. All of the elastomeric IMs shrink during polymerization; moreover, because of the generation of
by-products during the setting, they show more constriction. Overall, the greatest
dimensional change during setting refers to the polysulfide and polyvinyl silicone,
and the smallest one pertains to the PVS (Hamalian et al., 2011).
9.4.2 Wettability
A hydrophilic nature is one of the essential characteristics an actual IM needs, as
this substance is in continuity with the wet tissue. Affinity toward spreading on
hydrophilic substances results in flow capability into tiny areas or splitting and
recording partial details. IMs with low contact angle flow easily into small gaps
and make impressions with fewer voids. Hence, such materials are reliable for utilization in fixed prosthodontics (Hamalian et al., 2011). The sort of IMs that can
flow into partial segments in the scale of 2070 μm have been required in the field
of fixed partial dentures; on the other hand, IMs that can reproduce details in the
scale of 100150 μm are useful in the fields of removable prosthodontics (Rubel,
2007). Hydrophilic IMs enable dental stone to flow smoothly. Accordingly, the
casts without bubbles can be obtained. In order to produce more precise casts when
the IMs have high contact angle, both the particular pouring technique and attention
should be considered. Hydrophobic materials necessitate the surfactant utilization
to reduce the contact angle prior to pouring casts; on the contrary, polyether, polysulfide, and hydrocolloids are hydrophilic IMs with low contact angle (Rubel,
2007).
9.4.3 Elastic recovery/flexibility
It is of paramount importance for IMs to have an elastic recovery property, allowing it to return to its main dimensions without noticeable distortion upon removal
from the mouth (Re et al., 2015). It was indicated that PVS exhibited foremost elastic behavior (with over 99% elastic recovery), followed by polyether and then polysulfide. Instantly after mixing, PVS, because of swift elasticity development, should
be applied promptly, particularly at high temperatures. Conversely, polyether kept
the plasticity for the more extended duration after mixing. Also, the ultimate stiffness of the polyether is greater than that of PVS and may affect the ease of removing the material from the mouth (Mehta et al., 2014). The flexibility of the
impressions can facilitate the removal of the materials from the mouth. Polyether is
Impression materials for dental prosthesis
209
the stiffest IM. Polyvinyl siloxane is moderately rigid, and the rigidity relies on the
viscosity of the material (Hamalian et al., 2011). Alginate is evaluated as the most
flexible IM (Rubel, 2007). The investigations demonstrated that the viscosity is an
important factor in fabricating impressions and die with the least bubbles and maximal details. The increase in the amount of deformation and the time spent for
removal of the impression from the mouth have an influence on the accuracy of the
impression (Hamalian et al., 2011).
9.4.4 Mechanical properties
The main three relevant mechanical features of IMs in clinical terms having a functional impact on dental impression applications are yield strength, strain at yield
point, and tear energy. The yield strength is attributed to the point in which the
material can tolerate the stress without permanent deformation. The strain at yield
illustrates the quantity of undercut that an impression can defeat without permanent
deformation (Re et al., 2015). The tear energy determines and shows the degree to
which a material maintains resistance against tearing after setting. The material
should provide some properties such as appropriate and sufficient elastic recovery
and consumption of much energy to commence and spread tearing. Polysulfides are
incredibly resistant to tearing but show permanent deformation and do not indicate
complete elastic recovery after a critical point of permanent deformation (Al-Enazi
and Naik, 2016). Hydrocolloids show low tear strength. Both PVS and polyether
have the greatest tear strength, and they tear before they reach their perennial deformation point. Hence, they are more appropriate for clinical use (Hamalian et al.,
2011). Since producers have their exclusive formulations, various viscosities and
flow features exist. As different producers produce the materials, they also are at
various working times available according to standard-set versus quick-set IMs
(Rubel, 2007).
9.4.5 Miscellaneous
In addition to all the general properties that have been mentioned in previous sections, some other criteria are essential, including evaluating whether the materials
are tolerable for the patients, gaining the best consequences for low costs, and utilizing the disinfectants that cause the least dimensional changes. Disinfection of
some materials, for example, hydrocolloids, polyethers, and methacrylates, need
particular protocols to prevent distortion taking place after setting (Rubel, 2007;
Zarrintaj et al., 2018b). Various antibacterials and disinfectants can be used for dental impressions (Hafshejani et al., 2017; Maller et al., 2012). Diluted sodium hypochlorite is a disinfectant but not a sterilizer, accepted by the American Dental
Association for all materials except zinc oxideeugenol paste. Disinfection of zinc
oxideeugenol impression paste is done using glutaraldehyde (Rubel, 2007). In
Table 9.1 the properties of IMs are described.
Table 9.1 Comparison of various types of dental impression properties.
Impression
materials
Type
Advantage
Polyether
Elastic
G
G
G
G
G
G
G
Polysulfide
Elastic
G
G
G
G
Hydrophilic elastomeric
Dimensionally stable
Minimal shrinkage
Proper accuracy
Monophase impression
Good tear resistance
Low shrinkage
Good tear resistance
Stable dimensional
Proper accuracy
Most flexible elastomer
Disadvantage
G
G
G
G
G
G
G
G
Agar
Elastic
G
G
G
Alginate
Elastic
G
G
G
G
G
Addition
silicone
Elastic
G
G
G
G
G
High accuracy
Hydrophilic
Reusable
Easy flow
Cheap
Reproduction of adequate detail
Fast setting time
Minimal tissue displacement in the
mouth
G
Good detail reproduction
Excellent dimensional stability
No shrinkage on set
High patient acceptance
More than one model can be poured
from one cast
G
G
G
G
G
G
G
G
G
G
G
Ref.
Too stiff
Short working time
Guiraldo et al.
(2017)
Low patient satisfaction
Unpleasant taste and odor
Long setting time
Requires excellent moisture control
Difficult to mix
Some shrinkage on set with the release of by-product
Complex procedural steps
Significant start-up cost of the hardware
Punj et al. (2017)
Poor dimensional stability
Poor tear strength
Unsupported
Distortion
Easy to include air during mixing
A minimum thickness of 3 mm is required, which is
hard to achieve in thin areas in between the teeth
Hydrophobic
Too accurate
Poor tear resistance
Expensive
Khalid et al.
(2015)
Iwasaki et al.
(2016)
Punj et al. (2017)
(Continued)
Table 9.1 (Continued)
Impression
materials
Type
Advantage
Condensation
silicone
Elastic
G
G
Accurate
High patient acceptance
Disadvantage
G
G
G
G
G
Plaster
Inelastic
G
G
G
G
G
Impression
compound
Inelastic
G
G
G
G
Zinc oxide
eugenol
plaster
Inelastic
G
G
G
G
Hydrophilic
Good detail reproduction
Excellent dimensional stability
(contraction on setting)
Good patient tolerance
23 min working time
Primary impressions of complete
dentures
Border molding of trays
Extension of trays
Achieving mucocompression in the
postdam area when working
impressions are taken for complete
dentures
Thermoplastic
Can be heated to aid removal from
the casting material
Good detail reproduction
Excellent dimensional stability
(0.15% shrinkage on setting)
G
G
G
Hydrophobic
Requires excellent moisture control
Unreliable dimensional stability
Difficult to accurately proportion components leading to
variable results
Marked shrinkage on setting with the release of byproduct
Brittle
No recovery from deformation. Therefore if an undercut
is present, the material will have to be broken off the
impression and then glued back together before casting
Excess salivation by the patient could have an adverse
effect on detail reproduction
Ref.
Punj et al. (2017)
Von Fraunhofer
(2013)
Von Fraunhofer
(2013)
G
G
Rigid
Presence of undercuts can distort the final material or
cause the section engaged to separate from the resultant
impression
Luengo et al.
(2017)
212
9.5
Advanced Dental Biomaterials
Conclusion and future perspective
Dental IMs have been utilized for developing the numerous dental and orthodontic
applications. They are the first stage in the chain of a dental prosthesis or the initial
level of placing a crown or bridge. Due to such aims, various materials have been
examined for dental prostheses purposes ranging from elastic to rigid materials. To
preventing contamination, various disinfection materials have been added to
the IMs to reach a desired product. The maintenance of properties, such as
dimensional stability, is found to be among the major properties needed for the
suitable functioning of IM. Various properties, such as setting time, accuracy, wettability, and recovery, should be considered in IM usage. IMs preparation necessitates the tray involved in IM casting. Recently, a digital technique has been utilized
for the preparation of IMs and to optimize the process by shortening the process
time, enhancing the accuracy, and facilitating the setting procedure. To reach the
best dental impression, however, the material should be designed so as to meet several requirements simultaneously including low shrinkage, high accuracy, high stability, and proper hydrophilicity, and it must be applied with modern techniques to
achieve the appropriate product. In this regard the current chapter gives some
insights into the status of IMs used for dental prostheses. In the near future, digital
dentistry will cover all aspects of this. The new emerging digital devices are starting to be used in the IM field, and they will become more user friendly, more precise, and smaller in size of wand/equipment. Tomography is used for capturing the
basic graph to construct proper restorative implants. Hence, the digital methods in
IMs preparation should be evaluated in more detail in future studies to design a
road map for IMs selection for the next generation of restorative materials.
References
Al-Enazi, T.A., Naik, A.V., 2016. Disinfection of alginate and addition silicon rubber-based
impression materials. Int. J. Stomatol. Occlusion Med. 8 (1), 4448.
Amalan, A., Ginjupalli, K., Upadhya, N., 2013. Evaluation of properties of irreversible hydrocolloid impression materials mixed with disinfectant liquids. Dent. Res. J. 10 (1), 65.
Anusavice, K.J., Shen, C., Rawls, H.R., 2013. Phillips’ Science of Dental Materials. Elsevier
Health Sciences.
Atoufi, Z., Zarrintaj, P., Motlagh, G.H., Amiri, A., Bagher, Z., Kamrava, S.K., 2017. A novel
bio electro active alginate-aniline tetramer/agarose scaffold for tissue engineering: synthesis, characterization, drug release and cell culture study. J. Biomater. Sci., Polym. Ed.
143. just accepted.
Bakhshandeh, B., Zarrintaj, P., Oftadeh, M.O., Keramati, F., Fouladiha, H., Sohrabi-jahromi,
S., et al., 2017. Tissue engineering; strategies, tissues, and biomaterials. Biotechnol.
Genet. Eng. Rev. 33 (2), 144172.
Bhakta, S., Vere, J., Calder, I., Patel, R., 2011. Impressions in implant dentistry. Br. Dent. J.
211 (8), 361367.
Impression materials for dental prosthesis
213
Craig, R.G., 1988. Review of dental impression materials. Adv. Dent. Res. 2 (1), 5164.
Chiu, L.L.Y., Chu, Z., Radisic, M., Mozafari, M., 2017. Tissue engineering. Reference
Module in Materials Science and Materials Engineering. Elsevier.
Cole, M.A., Jankousky, K.C., Bowman, C.N., 2014. Thiol-ene functionalized siloxanes for
use as elastomeric dental impression materials. Dent. Mater. 30 (4), 449455.
Dai, J., Cheng, N., Miron, R.J., Shi, B., Cheng, X., Zhang, Y., 2014. Effect of decreased
implant healing time on bone (re)modeling adjacent to plateaued implants under functional loading in a dog model. Clin. Oral. Invest. 18 (1), 7786.
de Azevedo Cubas, G.B., Valentini, F., Camacho, G.B., Leite, F.R.M., Cenci, M.S., PereiraCenci, T., 2014. Antibacterial efficacy and effect of chlorhexidine mixed with irreversible hydrocolloid for dental impressions: a randomized controlled trial. Int. J.
Prosthodont. 27 (4), 363365.
Din, S.U., Parker, S., Braden, M., Tomlins, P., Patel, M., 2017. Experimental hydrophilic
vinyl polysiloxane (VPS) impression materials incorporating a novel surfactant compared with commercial VPS. Dent. Mater. 33, e301e309.
Fokkinga, W.A., Witter, D.J., Bronkhorst, E.M., Creugers, N.H., 2017. Clinical fit of partial
removable dental prostheses based on alginate or polyvinyl siloxane impressions. Int. J.
Prosthodont. 30 (1), 3337.
Goodall, R.H., Darras, L.P., Purnell, M.A., 2015. Accuracy and precision of silicon based
impression media for quantitative areal texture analysis, Sci. Rep., 5. p. 10800.
Guiraldo, R.D., Berger, S.B., Siqueira, R.M., Grandi, V.H., Lopes, M.B., Gonini-Júnior, A.,
et al., 2017. Surface detail reproduction and dimensional accuracy of molds: influence
of disinfectant solutions and elastomeric impression materials. Acta Odontol. Latinoam.
30 (1), 1318.
Hafshejani, T.M., Zamanian, A., Venugopal, J.R., Rezvani, Z., Sefat, F., Saeb, M.R., et al.,
2017. Antibacterial glass-ionomer cement restorative materials: a critical review on the
current status of extended release formulations. J. Control. Release 262, 317328.
Hamalian, T.A., Nasr, E., Chidiac, J.J., 2011. Impression materials in fixed prosthodontics:
influence of choice on clinical procedure. J. Prosthodont. 20 (2), 153160.
Han, M., Li, Q.-L., Cao, Y., Fang, H., Xia, R., Zhang, Z.-H., 2017. In vivo remineralization of
dentin using an agarose hydrogel biomimetic mineralization system. Sci. Rep. 7, 41955.
Iwasaki, Y., Hiraguchi, H., Iwasaki, E., Yoneyama, T., 2016. Effects of immersion disinfection of agar-alginate combined impressions on the surface properties of stone casts.
Dent. Mater. J. 35 (1), 4550.
Khalid, M., Shah, S.N., Chughtai, M.A., 2015. Comparison of mean dimensional measurement of alginate impression using sodium hypochlorite versus gluteraldehyde and benzalkonium chloride for disinfection. Cell 321, 9001101.
Kulkarni, M.M., Thombare, R.U., 2015. Dimensional changes of alginate dental impression
materials—an in vitro study. J. Clin. Diagn. Res.: JCDR. 9 (8), ZC98ZC102.
Levartovsky, S., Folkman, M., Alter, E., Pilo, R., 2011. Elastomeric impression materials.
Refu’at ha-peh veha-shinayim (1993) 28 (2), 5464.
Livaditis, G.J., 1998. Comparison of the new matrix system with traditional fixed prosthodontic impression procedures. J. Prosthet. Dent. 79 (2), 200207.
Lu, H., Nguyen, B., Powers, J.M., 2004. Mechanical properties of 3 hydrophilic addition silicone and polyether elastomeric impression materials. J. Prosthet. Dent. 92 (2), 151154.
Luengo, J., Reyes, H., Toscano, I., Garcia, Y., Anaya, M., 2017. Clinical and radiographic
evaluation of CTZ (chloramphenicol-tetracycline-zinc eugenol oxide) antibiotic paste in
pulp treatment of primary molars. J. Dent. Health Oral Disord. Ther. 8 (1), 00272.
214
Advanced Dental Biomaterials
Maller, S.V., Karthik, K., Maller, U.S., Abraham, M.C., Kumar, R.N., Manikandan, R., 2012.
Drug and dental impression materials. J. Pharm. Bioallied Sci. 4 (Suppl 2), S316.
Manappallil, J.J., 2015. Basic Dental Materials. JP Medical Ltd.
Marotti, J., Tortamano, P., Castilho, T.R., Steagall, W., Wolfart, S., Haselhuhn, K., 2014.
Accuracy of a self-perforating impression tray for dental implants. J. Prosthet. Dent. 112
(4), 843848.
McCabe, J.F., Walls, A.W., 2013. Applied Dental Materials. John Wiley & Sons.
Mehta, R., Dahiya, A., Mahesh, G., Kumar, A., Wadhwa, S., Duggal, N., et al., 2014.
Influence of delayed pours of addition silicone impressions on the dimensional accuracy
of casts. J. Oral Health Commun. Dent. 8, 3.
Mete, J.J., Rajguru, V.L., Dange, S.P., 2017. Aluminum barrier laminate or plastic tube as a
dispenser for modeling plastic impression compound for border molding. J. Prosthet.
Dent. 119, 676677.
Nassar, U., Chow, A.K., 2015. Surface detail reproduction and effect of disinfectant and
long-term storage on the dimensional stability of a novel vinyl polyether silicone
impression material. J. Prosthodont. 24 (6), 494498.
Nassar, U., Oko, A., Adeeb, S., El-Rich, M., Flores-Mir, C., 2013. An in vitro study on the
dimensional stability of a vinyl polyether silicone impression material over a prolonged
storage period. J. Prosthet. Dent. 109 (3), 172178.
Oh, W., Morris, H., 2017. The principles of functional and mucostatic impressions for complete denture bases: a review. Compend. Continuing Educ. Dent. (Jamesburg, NJ: 1995)
38 (10), 664.
Oppedisano, M., 2013. Delayed Linear Expansion of Two Ultra-low Expansion Dental
Stones (Doctoral dissertation).
Pastoret, M.-H., Krastl, G., Bühler, J., Weiger, R., Zitzmann, N.U., 2017. Accuracy of a separating foil impression using a novel polyolefin foil compared to a custom tray and a
stock tray technique. J. Adv. Prosthodont. 9 (4), 287293.
Powers, J.M., Craig, R.G., 1978. Thermal analysis of dental impression waxes. J. Dent. Res.
57 (1), 3741.
Powers, J.M., Wataha, J.C., 2017. Dental Materials: Foundations and Applications. Elsevier.
Punj, A., Bompolaki, D., Garaicoa, J., 2017. Dental impression materials and techniques.
Dent. Clin. North Am. 61 (4), 779796.
Rafael, C.F., Liebermann, A., 2017. Clinical characteristics of an allergic reaction to a polyether dental impression material. J. Prosthet. Dent. 117 (4), 470472.
Re, D., De Angelis, F., Augusti, G., Augusti, D., Caputi, S., D’Amario, M., et al., 2015.
Mechanical properties of elastomeric impression materials: an in vitro comparison. Int.
J. Dent. 2015, 428286.
Rubel, B.S., 2007. Impression materials: a comparative review of impression materials most
commonly used in restorative dentistry. Dent. Clin. North Am. 51 (3), 629642.
Sakaguchi, R.L., Powers, J.M., 2012. Craig’s Restorative Dental Materials-E-Book. Elsevier
Health Sciences.
Serrano-Aroca, Á., Ruiz-Pividal, J.-F., Llorens-Gámez, M., 2017. Enhancement of water diffusion and compression performance of crosslinked alginate films with a minuscule
amount of graphene oxide. Sci. Rep. 7 (1), 11684.
Shetty, S., Kamat, G., Shetty, R., 2013. Wettability changes in polyether impression materials
subjected to immersion disinfection. Dent. Res. J. 10 (4), 539.
Shoemaker, D.P., Chung, D.Y., Mitchell, J., Bray, T.H., Soderholm, L., Chupas, P.J., et al.,
2012. Understanding fluxes as media for directed synthesis: in situ local structure of
molten potassium polysulfides. J. Am. Chem. Soc. 134 (22), 94569463.
Impression materials for dental prosthesis
215
Sinobad, T., Obradović-Ðuričić, K., Nikolić, Z., Dodić, S., Lazić, V., Sinobad, V., et al.,
2014. The effect of disinfectants on dimensional stability of addition and condensation
silicone impressions. Vojnosanit. Pregl. 71 (3), 251258.
Sun, Y., Chen, H., Li, H., Deng, K., Zhao, T., Wang, Y., et al., 2017. Clinical evaluation of
final impressions from three-dimensional printed custom trays. Sci. Rep. 7 (1), 14958.
Ting-shu, S., Jian, S., 2015. Intraoral digital impression technique: a review. J. Prosthodont.
24 (4), 313321.
Tinto, W., Elufioye, T., Waxes, R.J., 2017. Pharmacognosy. Elsevier, pp. 443455.
Tripathi,, A., Singh,, S.V., Aggarwal,, H., Gupta,, A., Arya,, D., 2017. A technique to preserve spacer thickness during custom tray fabrication with autopolymerizing polymethylmethacrylate. Int. J. Dent. Res. 2 (1), 12.
Vadapalli, S.B., Atluri, K., Putcha, M.S., Kondreddi, S., Kumar, N.S., Tadi, D.P., 2016.
Evaluation of surface detail reproduction, dimensional stability and gypsum compatibility of monophase polyvinyl-siloxane and polyether elastomeric impression materials
under dry and moist conditions. J. Int. Soc. Prev. Commun. Dent. 6 (4), 302.
Von Fraunhofer, J.A., 2013. Dental Materials at a Glance. John Wiley & Sons.
Wang, Z., 2016. Comparison of dimensional accuracies using two elastomeric impression
materials in casting three-dimensional tool marks. J. Forensic. Sci. 61 (3), 792797.
Yang, Z.-Z., Wang, H.-Y., Lu, L., Wang, C., Zhong, X.-B., Wang, J.-G., et al., 2016.
Hierarchical TiO2 spheres as highly efficient polysulfide host for lithium-sulfur batteries. Sci. Rep. 6, 22990.
Zamanian, A., Yasaei, M., Ghaffari, M., Mozafari, M., 2013. Calcium hydroxide-modified
zinc polycarboxylate dental cements. Ceram. Int. 39 (8), 95259532.
Zarrintaj, P., Bakhshandeh, B., Rezaeian, I., Heshmatian, B., Ganjali, M.R., 2017a. A novel
electroactive agarose-aniline pentamer platform as a potential candidate for neural tissue
engineering. Sci. Rep. 7, 17187.
Zarrintaj, P., Moghaddam, A.S., Manouchehri, S., Atoufi, Z., Amiri, A., Amirkhani, M.A.,
et al., 2017b. Can regenerative medicine and nanotechnology combine to heal wounds?
The search for the ideal wound dressing. Nanomedicine 12 (19), 24032422.
Zarrintaj, P., Manouchehri, S., Ahmadi, Z., Saeb, M.R., Urbanska, A.M., Kaplan, D.L., et al.,
2018a. Agarose-based biomaterials for tissue engineering. Carbohydr. Polym. 187,
6684.
Zarrintaj, P., Urbanska, A., Gholizadeh, S.S., Goodarzi, V., Saeb, M.R., Mozafari, M.,
2018b. A facile route to the synthesis of anilinic electroactive colloidal hydrogels for
neural tissue engineering applications. J. Colloid Interface Sci. 516, 5766.
10
Nano glass ionomer cement:
modification for biodental
applications
Shariq Najeeb1, Zohaib Khurshid2, Hani Ghabbani3,
Muhammad S. Zafar3,4 and Farshid Sefat5,6
1
Independent Researcher and Private Practitioner, Alberta, Canada, 2Department of
Prosthodontics and Dental Implantology, College of Dentistry, King Faisal University,
Al-Ahsa, Saudi Arabia, 3Department of Restorative Dentistry, College of Dentistry, Taibah
University, Medina, Saudi Arabia, 4Department of Dental Materials, Islamic International
Dental College, Riphah International University, Islamabad, Pakistan, 5Biomedical and
Electrical Engineering Department, School of Engineering, University of Bradford,
Bradford, United Kingdom, 6Interdisciplinary Research Centre in Polymer Science and
Technology (IRC Polymer), University of Bradford, Bradford, United Kingdom
Chapter Outline
10.1 Introduction 217
10.2 Applications of glass ionomer cements 219
10.3 Nanomodifications of glass ionomer cement powders
10.3.1
10.3.2
10.3.3
10.3.4
219
Powder-based nanomodification of glass ionomer cements 220
Nanohydroxyapatite and ionomers 220
Glass ionomer cements modified with other nanoparticles 222
Nanomodified resin-modified glass ionomer cements 223
10.4 Conclusion 224
References 224
10.1
Introduction
A variety of synthetic and natural biomaterials are used to restore diseased or damaged tissues (Zafar et al., 2015; Husain et al., 2017). Materials such as metals and
alloys have been used in dentistry to repair teeth for thousands of years. Historical
records indicated that Plaster of Paris might have been used as a bone substitute
material in as early as the 19th century. Alloys of silver, called dental amalgams,
have been used since the late 1800s. More recently, a variety of materials, such as
titanium, zirconia, and polyetheretherketone (Najeeb et al., 2016b,c), have been
used as dental implant materials. Dental materials are used to replace or restore
hard and soft oral tissues. There are two main types of dental materials: direct
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00010-4
Copyright © 2019 Elsevier Ltd. All rights reserved.
218
Advanced Dental Biomaterials
dental materials and indirect dental materials. Direct dental materials are used
directly in the oral cavity to restore dental tissues; they do not need major processing or modification in the dental laboratory before use. Some examples of direct
dental materials are resin composites, glass ionomer cement (GIC), compomer, fissure sealants, and topical fluoride. Indirect dental materials have been modified,
physically and/or chemically, in the dental laboratory or chair-side before being
used in the oral cavity. Examples of indirect materials are acrylic dentures, dental
implants, indirect resin composite crowns and veneers, and maxillofacial prostheses. Indeed, modern dentistry involves the combined use of these indirect and direct
materials, along with natural biomaterials to improve the functions, esthetics, and
biomechanics of oral tissues.
GICs are mainly used as direct restorative dental materials. Directly speaking,
GICs are a group of restorative materials which contain aluminofluorosilicate
glasses as the vital component. First developed by Wilson and Kent in the early
1970s (Wilson and Kent, 1971), GICs have come a long way since their inception.
A number of modifications in their composition, introduction of various bioactive
fillers, and changing the particle size of the powders have been combined to tailor
the physical, chemical, and optical properties of GICs. Conventionally, GICs have
been composed of two main components: a fluoroaluminosilicate glass and an aqueous solution of polyacids (Sakaguchi and Powers, 2012). In addition to the main
ingredients, other acids such as maleic acid and itaconic acid (IA) may be added to
the formulation to improve the handling properties by altering the setting time.
Incorporation of salts of radiopaque metals such as barium and strontium makes
GICs visible in radiographs, making a clinical diagnosis and posttreatment assessment of restorations easier. The presence of fluoride ions in the glass component of
GICs may impart antibacterial properties by releasing fluoride into the oral cavity
(Zafar and Ahmed, 2015; Zafar, 2013). Therefore fluoride-releasing restorative
materials are used as vehicles for delivering fluoride to the oral cavity (Zafar and
Ahmed, 2015; Ullah and Zafar, 2015). Indeed, the inherent adhesive qualities of
GICs, coupled with their white color and translucency, make them an
acceptable material for restoring deciduous teeth.
Conventional glass ionomers are set via a reaction between polyacrylic acid
(PAA) and the glass particles. The reaction initially results in the gelation of the
acid and glass components (Sakaguchi and Powers, 2012). The structure can be
best described as unreacted glass particles embedded in the silica gel. Indeed,
changing the particle size, the type of the acid and adding other additives to the
glass and/or acid component of the cement can alter the physical, mechanical, and
chemical properties. The hardening phase of the GIC takes place when the polyacid
chains cross-link with calcium and aluminum ions in the powder (Anusavice and
Phillips, 2003). Research has indicated that the majority of sodium and fluoride
ions remain unreacted in the set GIC. The final stage of GIC setting is called “maturation.” During this stage, which may last for up to 1 year, water is bound by the
acid and glasses. Additionally, aluminum may also slowly leach out. In addition to
dental applications, research is being conducted to make GICs suitable for bone
applications. Their bioactive and adhesive properties are an advantage which may
Nano glass ionomer cement: modification for biodental applications
219
prove to be useful in bone regeneration and implant applications. However, there
are several limitations such as poor surface mechanical properties and wear resistance (Zafar and Ahmed, 2014; Zafar, 2018), that may impede the use of GICs. In
this chapter, we discuss various modifications that have been made to GICs to
improve their biological and mechanical properties.
10.2
Applications of glass ionomer cements
Over the last several decades, GICs have seen a variety of applications in dentistry.
GICs have been used to restore deciduous (milk) teeth due to ease of application.
Because of their white color and translucency, GICs have also been used to restore
anterior (front) teeth, either alone or in combination with other tooth-colored
materials, such as resin composites. Due to their adhesive properties, they may also
be used for the temporary or permanent cementation of crowns and bridges, in
addition to luting of orthodontic devices. Indeed, their bioactive properties have
also allowed them to be placed in deep carious lesions, following removal of
infected dentine.
Because infected dentine is removed, but bacteria-free and caries-affected dentine is left as much as possible, this technique is termed as atraumatic restorative
treatment. Due to its special dentine bonding properties, glass ionomers can be used
in endodontic treatment (obturation) as a sealer and as a core material. Activ GP
(gutta percha) contains gutta percha cones saturated with GIC on the external
surface. Although the sealer has minimal antimicrobial activity compared to other
sealers (Heling and Chandler, 1996), it creates a monoblock and allows adhesion
with canal walls. Also, obturating the root canal with a glass ionomer based sealer
makes the root more resistant to vertical root fracture because of its ability of dentin
bonding (Trope and Ray, 1992).
10.3
Nanomodifications of glass ionomer cement
powders
Nanotechnology is best described as the use of systems and modifications of
materials in the size range of 1 100 nm to improve their mechanical properties,
function, and esthetic attributes (Zafar et al., 2016, 2017; Khurshid et al., 2015).
Over the past few years, nanotechnology has been used to enhance osseointegration
of implants (Najeeb et al., 2015), reinforcement of polymeric materials (Najeeb
et al., 2016d), prevention of dental caries (Huang et al., 2011), and to enhance the
efficacy of tissue regeneration and drug delivery (Qasim et al., 2017).
Two main techniques have been employed for the production of nanosized materials. “Top-down” is the production of particles or systems in the nanometer range
by removal of bulk material, leaving behind nanometer-sized particles. Milling,
lithography, and machining are examples of top-down manufacturing. Conversely,
220
Advanced Dental Biomaterials
“bottom-up” nanomanufacturing would be best described as fabrication of
nanometer-sized materials atom by atom, such as in the case of the coating of dental implants, tissue regeneration, and additive 3D printing. Nanomodification
of GICs is mainly produced by the top-down nanofabrication of glasses, oxides,
and bioceramics.
A composite material is a material composed of two or more materials with
vastly different chemical and physical properties. Teeth and bone are an example of
natural composites. They both are composites of inorganic apatites embedded in an
organic matrix. In dentistry and surgery, a wide variety of synthetic and natural
composite materials are used. Resin composites, dental implants, and regenerative
tissue materials are just some of several composites used. Indeed, technically
speaking, GICs are also composite materials. Unreacted glass particles are embedded in a cross-linked matrix of organic acids, much akin to bone and teeth. Hence,
modification of the particle size and chemistry has a significant effect on the
mechanical, physical, and optical properties of GICs. Several nanomodifications
have been proposed to improve the quality, life, and function of GICs. This chapter
aims to summarize these modifications and ascertain their present status and the
clinical use of these nanomodified GIC formulations.
10.3.1 Powder-based nanomodification of glass ionomer
cements
Nanomodification of GICs has been achieved in three ways. First, the size of the
glass powder itself is altered to change the mechanical and physical properties of
GICs. Indeed, the initial study by De Caluwe et al. (2014) demonstrated the effect
of introducing nanosized glass powder on the setting characteristics and mechanical
properties of GIC. They observed that the addition of nanosized fluoroaluminosilicate glass not only decreased the setting time but also improved the mechanical
properties of the set GIC. A number of procedures are used to replicate the
detrimental effect of the oral environment on the restorative materials. It has been
observed that thermocycling has a more negative impact on the mechanical
properties of nanomodified materials than those of conventional ionomers. Over
the past few years, several modifications have been suggested, aimed at
increasing the mechanical, physical, biological, and optical properties of GICs.
Nanomodification of GICs mainly involves the incorporation of nanosized fillers to
the powder component. Significant nanomodifications are presented below, and a
summary of the mechanical properties of various nanomodified GICs are presented
in Table 10.1.
10.3.2 Nanohydroxyapatite and ionomers
Hydroxyapatite (HAp) is found in bone and teeth as the mineral component. Due
to its osteoconductive effects and remineralizing attributes, HAp has been used as
a dental implant coating to prevent dental caries and in regenerative therapy
Table 10.1 A summary of the mechanical properties of nanomodified glass ionomer cements (GICs) compared with those of conventional
GICs.
Liquid
Powder
Nanoparticles
(% and size)
Compressive
strength (MPa)
Tensile
strength
(MPa)
Flexural
strength
(MPa)
Reference
PAA copolymer
PAA copolymer
FAS
FAS
161
178
11.8
19
14.8
31
Moshaverinia et al. (2008a)
Moshaverinia et al. (2008b)
PAA copolymer
FAS
179
23
33
Moshaverinia et al. (2008b)
Polymer of AA,
NVP, IA
PAA copolymer
FAS
183.8
23.5
36
Moshaverinia et al. (2008a)
FAS
None
nHAp (5 wt.%
100 200 nm)
nFAp (5 wt.%
100 200 nm)
HAp (5 wt.%
100 200 nm)
3%
23.17
PAA copolymer
FAS
Garcia-Contreras et al.
(2015); Elsaka et al.
(2011)
Kumar et al. (2017)
Chitosan (10 wt.%
110 235 nm)
176.27
21.26
FAS, Fluoroaluminosilicate; HAp, hydroxyapatite; IA, itaconic acid; nHAp, nanohydroxyapatite; NVP, N-vinylpyrrolidone; PAA, polyacrylic acid.
222
Advanced Dental Biomaterials
(Huang et al., 2011; Kettenberger et al., 2017). Utilizing their bioactive nature, both
HAp and fluorapatite (FAp) have been incorporated into resin composites and glass
ionomers (Moshaverinia et al., 2008b; Zakir et al., 2013). Indeed, the addition of
nano-HAp (nHAp) and nano-FAp (nFAp) to the GIC powder results in significantly
improved flexural, tensile, and compressive strengths of the set GIC (Moshaverinia
et al., 2008b).
There are several mechanisms by which apatites may improve the mechanical
properties of the GICs. Spectroscopic studies have revealed that incorporation of
apatites decreases the solubility of the set GIC by increasing the crystallinity of the
composite (Moshaverinia et al., 2008a,b). When compared with nHAp-modified
GICs, nFAp-modified GICs have demonstrated higher crystallinity leading to better
mechanical properties (Moshaverinia et al., 2008a,b). Fractures and sensitivity to
moisture are two of the most common causes of their failure. Hence, the addition of
nanoapatites to GICs may overcome their limitations and prolong their intraoral
life. The mechanical properties of nFAp-modified GICs can be further enhanced by
substituting the PAA copolymer with a mixture of IA and N-vinylpyrrolidone
(NVP) copolymers. The mechanism behind this improvement is the interaction
between the apatite and the NVP chains, resulting in a more crystalline, stronger
chemical structure (Moshaverinia et al., 2008a). Another advantage of incorporating
nanoapatites is the increased adhesive bond strength between the tooth and the GIC
restoration. This is thought to be a result of two observations. First, the chemical
similarity of apatites present in teeth and the nanoapatites incorporated in the
GIC may give rise to the ionic interactions between the tooth and the GIC
structures (Lucas et al., 2003). Second, the small size of the nanometer-sized apatite
crystals makes it easier for them to infiltrate dentinal tubules and enamel pores
(Lee et al., 2010).
10.3.3 Glass ionomer cements modified with other nanoparticles
Zirconia (zirconium oxide, ZrO2) is a ceramic which has been used in dentistry for
the production of crowns (Kolbeck et al., 2008), dentures, and dental implants
(Calvo-Guirado et al., 2015). A study by Gu et al. (2005) evaluated the effect on
the mechanical properties of incorporating nanosized HAp and zirconia (nZrO2) to
conventional GIC. In the study, it was observed that the addition of nHAp and
nZrO2 at a concentration of 4% by volume resulted in significant improvement in
the mechanical properties of the cement. Nevertheless, in the same study, when
scanning electron micrographs of conventional set GIC and set nHAp/nZrO2modified GIC were compared, more cracks were observed in the latter (Gu et al.,
2005). This could have a detrimental effect on the long-term viability of these
modified cements, because the cracks may lead to marginal failure and subsequent
failure of the restorations.
Other nanosized particles, such as calcium fluoride (CaF2) and titania (titanium
oxide; TiO2), have also been used to modify GICs (Elsaka et al., 2011; Moreau and
Xu, 2010). Addition of CaF2 to resin-modified GICs (RMGICs) may prolong the
longevity of these cements by improving the mechanical properties, but it may also
have an adverse effect on fluoride release from the cement (Xu et al., 2010).
Nano glass ionomer cement: modification for biodental applications
223
Although nano-TiO2 (nTiO2) has been observed to improve the mechanical properties and enhance the antibacterial attributes of GICs, more studies are required to
determine the safety of these modified restorations, because titania is known to be
cytotoxic (Hall et al., 2009). Nanoparticles of chitosan, a deacylated form of chitin,
a polysaccharide found in shells of crustaceans, have been observed to improve the
flexural strength of GICs significantly due to increased interaction between the
chitosan chains and the GIC matrix (Kumar et al., 2017).
10.3.4 Nanomodified resin-modified glass ionomer cements
To improve the mechanical properties of GICs, they may be combined with a
self-curing or light-activated resin polymer. These RMGICs are less susceptible to
flexural fractures and expansion due to water sorption and have better esthetics
(McCabe, 1998). However, RMGICs still have some disadvantages. First, they have
inferior mechanical properties when compared to resin composites (McCabe and
Walls, 2008). Moreover, they have higher creep and lower fluoride release when
compared to conventional GICs. More recently, nanoclusters of silica have been
incorporated to the powder formulation of the RMGICs to improve the mechanical
properties and fluoride release from the set cement (Coutinho et al., 2009). They
are supplied with a primer that aids bonding with tooth structure. RMGICs bond to
the tooth structure through a combination of micromechanical interactions due to
the infiltration of resins into the etched tooth surface and ionic bonding between the
HAp crystals present in tooth and the acids RMGICs (Fig. 10.1). The aim of adding
Figure 10.1 The schematic presentation of the structure of nanomodified GIC and its
bonding with dental hard tissues (Najeeb et al., 2016a). GIC, Glass ionomer cement.
224
Advanced Dental Biomaterials
nanofillers to the RMGICs is to increase the infiltration of resin into the pores in
the etched tooth surface and enhance the binding. However, studies indicate that
there is no significant difference between the tensile bond strength of nanoRMGICs and conventional GIC (Coutinho et al., 2009). Indeed, clinical studies also
showed that there is no difference between the survival rates of RMGICs and
nano-RMGICs (Perdigao et al., 2012). Although nano-RMGIC is available
commercially (e.g., Ketac N100/Ketac Nano; 3M ESPE, St. Paul, Minnesota,
United States), more research is needed before nano-RMGICs find more use in the
clinical setting. Abrasion produced by toothbrush simulation produces less surface
roughness on the surface of nano-RMGICs than on conventional RMGICs;
degradation produced by bacteria and chemicals produce comparable surface roughnesses on both (de Paula et al., 2011, 2014; de Fúcio et al., 2012). This indicates
that in long-term use, nano-RMGICs do not hold any significant advantage over
conventional RMGICs as far as the surface properties are concerned. To date, no
statistically significant difference has been observed between the fluoride release
from nano-RMGICs and conventional RMGICs.
10.4
Conclusion
Although some nanomodifications have been proposed for GICs, more studies and
long-term clinical trials are vital to ascertain their advantages over conventional
GICs and RMGICs. The failure of the bioceramic glass interface in the set GICs is
thought to be a major concern that should be studied more. Not many studies have
been carried out to observe the effect of nanomodified GICs on dental pulp cells.
However, with the recent improvements in the resins and fillers, nanomodified
GICs may find widespread usage in dental clinics.
References
Anusavice, K., Phillips, R., 2003. Phillips’ Science of Dental Materials. Saunders, St. Louis,
MO, Great Britain.
Calvo-Guirado, J.L., Aguilar Salvatierra, A., Gargallo-Albiol, J., Delgado-Ruiz, R.A., Maté
Sanchez, J.E., Satorres-Nieto, M., 2015. Zirconia with laser-modified microgrooved surface vs. titanium implants covered with melatonin stimulates bone formation.
Experimental study in tibia rabbits. Clin. Oral Implants Res. 26, 1421 1429.
Coutinho, E., Cardoso, M.V., De Munck, J., Neves, A.A., Van Landuyt, K.L., Poitevin, A.,
et al., 2009. Bonding effectiveness and interfacial characterization of a nano-filled resinmodified glass-ionomer. Dent. Mater. 25, 1347 1357.
De Caluwe, T., Vercruysse, C.W., Fraeyman, S., Verbeeck, R.M., 2014. The influence of
particle size and fluorine content of aluminosilicate glass on the glass ionomer cement
properties. Dent. Mater. 30, 1029 1038.
Nano glass ionomer cement: modification for biodental applications
225
de Fúcio, S.B., de Paula, A.B., de Carvalho, F.G., Feitosa, V.P., Ambrosano, G.M.,
Puppin-Rontani, R., 2012. Biomechanical degradation of the nano-filled resin-modified
glass-ionomer surface. Am. J. Dent. 25, 315 320.
de Paula, A.B., Fucio, S.B., Ambrosano, G.M., Alonso, R.C., Sardi, J.C., Puppin-Rontani, R.,
2011. Biodegradation and abrasive wear of nano restorative materials. Oper. Dent. 36,
670 677.
de Paula, A.B., de Fucio, S.B., Alonso, R.C., Ambrosano, G.M., Puppin-Rontani, R., 2014.
Influence of chemical degradation on the surface properties of nano restorative materials. Oper. Dent. 39, E109 E117.
Elsaka, S.E., Hamouda, I.M., Swain, M.V., 2011. Titanium dioxide nanoparticles addition to
a conventional glass-ionomer restorative: influence on physical and antibacterial
properties. J. Dent. 39, 589 598.
Garcia-Contreras, R., Scougall-Vilchis, R., Contreras-Bulnes, R., Sakagami, H., MoralesLuckie, R., Nakajima, H., 2015. Mechanical, antibacterial and bond strength properties
of nano-titanium-enriched glass ionomer cement. J. Appl. Oral Sci. 23, 321 328.
Gu, Y.W., Yap, A.U., Cheang, P., Khor, K.A., 2005. Effects of incorporation of HA/ZrO(2)
into glass ionomer cement (GIC). Biomaterials 26, 713 720.
Hall, S., Bradley, T., Moore, J.T., Kuykindall, T., Minella, L., 2009. Acute and chronic toxicity of nano-scale TiO2 particles to freshwater fish, cladocerans, and green algae, and
effects of organic and inorganic substrate on TiO2 toxicity. Nanotoxicology 3, 91 97.
Heling, I., Chandler, N.P., 1996. The antimicrobial effect within dentinal tubules of four root
canal sealers. J. Endod. 22, 257 259.
Huang, S., Gao, S., Cheng, L., Yu, H., 2011. Remineralization potential of nanohydroxyapatite on initial enamel lesions: an in vitro study. Caries Res. 45, 460 468.
Husain, S., Al-Samadani, K.H., Najeeb, S., Zafar, M.S., Khurshid, Z., Zohaib, S., et al.,
2017. Chitosan biomaterials for current and potential dental applications. Materials 10,
602.
Kettenberger, U., Luginbuehl, V., Procter, P., Pioletti, D.P., 2017. In vitro and in vivo
investigation of bisphosphonate-loaded hydroxyapatite particles for peri-implant bone
augmentation. J. Tissue Eng. Regen. Med. 11, 1974 1985.
Khurshid, Z., Zafar, M., Qasim, S., Shahab, S., Naseem, M., AbuReqaiba, A., 2015.
Advances in nanotechnology for restorative dentistry. Materials 8, 717 731.
Kolbeck, C., Behr, M., Rosentritt, M., Handel, G., 2008. Fracture force of tooth tooth-and
implant tooth-supported all-ceramic fixed partial dentures using titanium vs. customised zirconia implant abutments. Clin. Oral Implants Res. 19, 1049 1053.
Kumar, R.S., Ravikumar, N., Kavitha, S., Mahalaxmi, S., Jayasree, R., Kumar, T.S., et al.,
2017. Nanochitosan modified glass ionomer cement with enhanced mechanical properties and fluoride release. Int. J. Biol. Macromol. 104, 1860 1865.
Lee, J., Lee, Y., Choi, B., Lee, J., Choi, H., Son, H., et al., 2010. Physical properties of
resin-reinforced glass ionomer cement modified with micro and nano-hydroxyapatite.
J. Nanosci. Nanotechnol. 10, 5270 5276.
Lucas, M.E., Arita, K., Nishino, M., 2003. Toughness, bonding and fluoride-release properties of hydroxyapatite-added glass ionomer cement. Biomaterials 24, 3787 3794.
McCabe, J.F., 1998. Resin-modified glass-ionomers. Biomaterials 19, 521 527.
McCabe, J.F., Walls, A.W.G., 2008. Applied Dental Materials. Oxford, Blackwell.
Moreau, J.L., Xu, H.H., 2010. Pmc2948642; fluoride releasing restorative materials: effects
of pH on mechanical properties and ion release. Dent. Mater. 26, e227 e235.
226
Advanced Dental Biomaterials
Moshaverinia, A., Ansari, S., Movasaghi, Z., Billington, R.W., Darr, J.A., Rehman, I.U.,
2008a. Modification of conventional glass-ionomer cements with N-vinylpyrrolidone
containing polyacids, nano-hydroxy and fluoroapatite to improve mechanical properties.
Dent. Mater. 24, 1381 1390.
Moshaverinia, A., Ansari, S., Moshaverinia, M., Roohpour, N., Darr, J.A., Rehman, I.,
2008b. Effects of incorporation of hydroxyapatite and fluoroapatite nanobioceramics
into conventional glass ionomer cements (GIC). Acta Biomater. 4, 432 440.
Najeeb, S., Khurshid, Z., Matinlinna, J.P., Siddiqui, F., Nassani, M.Z., Baroudi, K., 2015.
Nanomodified peek dental implants: bioactive composites and surface modification—a
review. Int. J. Dent 2015, 381759.
Najeeb, S., Khurshid, Z., Zafar, M.S., Khan, A.S., Zohaib, S., Martı́, J.M.N., et al., 2016a.
Modifications in glass ionomer cements: nano-sized fillers and bioactive nanoceramics.
Int. J. Mol. Sci. 17, 1134.
Najeeb, S., Khurshid, Z., Zohaib, S., Zafar, M.S., 2016b. Bioactivity and osseointegration of
PEEK are inferior to those of titanium—a systematic review. J. Oral Implantol. 42,
512 516.
Najeeb, S., Zafar, M.S., Khurshid, Z., Siddiqui, F., 2016c. Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J. Prosthodont. Res. 60, 12 19.
Najeeb, S., Khurshid, Z., Agwan, A.S., Zafar, M.S., Alrahabi, M., Qasim, S.B., et al., 2016d.
Dental applications of nanodiamonds. Sci. Adv. Mater. 8, 2064 2070.
Perdigao, J., Dutra-Correa, M., Saraceni, S.H., Ciaramicoli, M.T., Kiyan, V.H., 2012.
Randomized clinical trial of two resin-modified glass ionomer materials: 1-year results.
Oper. Dent. 37, 591 601.
Qasim, S.B., Najeeb, S., Delaine-Smith, R.M., Rawlinson, A., Rehman, I.U., 2017. Potential
of electrospun chitosan fibers as a surface layer in functionally graded GTR membrane
for periodontal regeneration. Dent. Mater. 33, 71 83.
Sakaguchi, R.L., Powers, J.M., 2012. Craig’s Restorative Dental Materials. Elsevier/Mosby,
Philadelphia, PA.
Trope, M., Ray, H.L., 1992. Resistance to fracture of endodontically treated roots. Oral Surg.
Oral Med. Oral Pathol. Oral Radiol. 73, 99 102.
Ullah, R., Zafar, M.S., 2015. Oral and dental delivery of fluoride: a review. Fluoride 48,
195 204.
Wilson, A.D., Kent, B.E., 1971. The glass-ionomer cement, a new translucent dental filling
material. J. Appl. Chem. Biotechnol. 21, 313.
Xu, H.H., Moreau, J.L., Sun, L., Chow, L.C., 2010. Pmc3077944; novel CaF(2) nanocomposite with high strength and fluoride ion release. J. Dent. Res. 89, 739 745.
Zafar, M.S., 2013. Effects of surface pre-reacted glass particles on fluoride release of dental
restorative materials. World Appl. Sci. J. 28, 457 462.
Zafar, M.S., 2018. Wear behavior of various dental restorative materials. Mater. Technol. 33,
25 31.
Zafar, M.S., Ahmed, N., 2014. Effects of wear on hardness and stiffness of restorative dental
materials. Life Sci. J. 11, 11 18.
Zafar, M.S., Ahmed, N., 2015. Therapeutic roles of fluoride released from restorative dental
materials. Fluoride 48, 184 194.
Zafar, M.S., Khurshid, Z., Almas, K., 2015. Oral tissue engineering progress and challenges.
Tissue Eng. Regener. Med. 12, 387 397.
Zafar, M.S., Najeeb, S., Khurshid, Z., Vazirzadeh, M., Zohaib, S., Najeeb, B., et al., 2016.
Potential of electrospun nanofibers for biomedical and dental applications. Materials
9, 73.
Nano glass ionomer cement: modification for biodental applications
227
Zafar, M.S., Khurshid, Z., Najeeb, S., Zohaib, S., Rehman, I.U., 2017. Chapter 26—
Therapeutic applications of nanotechnology in dentistry. In: Andronescu, E.,
Grumezescu, A.M. (Eds.), Nanostructures for Oral Medicine. Elsevier.
Zakir, M., Al Kheraif, A.A., Asif, M., Wong, F.S., Rehman, I.U., 2013. A comparison of the
mechanical properties of a modified silorane based dental composite with those of commercially available composite material. Dent. Mater. 29, e53 e59.
Enamel etching and dental
adhesives
11
Ahmed Talal1, Hafiz Muhammad Owais Nasim2 and
Abdul Samad Khan1
1
Department of Restorative Dental Sciences, College of Dentistry, Imam Abdulrahman
Bin Faisal University, Dammam, Saudi Arabia, 2Department of Dental Materials, Sharif
Medical and Dental College, Lahore, Pakistan
Chapter Outline
11.1 Introduction 229
11.2 Indications of adhesives 230
11.3 Composition of adhesives 231
11.3.1 Etchant 231
11.3.2 Primer 231
11.3.3 Bonding 231
11.4 Types of enamel etching
232
11.4.1 Acid etching 232
11.4.2 Laser etching 235
11.4.3 Self-etching 236
11.5 Classifications of adhesives
237
11.5.1 Classification based on generations 237
11.5.2 Classification based on clinical steps 240
11.5.3 Classification based on interaction with smear layer 241
11.6 Dentin bonding 241
11.7 Advancement in adhesives
242
11.7.1 Antibacterial properties 242
11.7.2 Bioactive properties 245
11.8 Conclusion 247
References 248
11.1
Introduction
The development of adhesives was a turning point in dentistry that revolutionized
restorative and preventive dentistry. The concept of cavity preparation changed
with the use of adhesives, and it was no longer required to extend the cavity preparation for resistance and retention of form at the cost of sound tooth structure. In
addition, advancements in adhesives substantially reduced recurrent caries which is
a major cause of restorations failure (Sofan et al., 2017a; Van Meerbeek et al.,
1992).
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00011-6
Copyright © 2019 Elsevier Ltd. All rights reserved.
230
Advanced Dental Biomaterials
The mineralized tooth structure, that is, enamel and dentin, has a unique composition and morphology. Enamel consists of hydroxyapatite (HA) (96 wt.%), water
(3 wt.%), and organic matrix, that is, proteins and lipids (1 wt.%) and has a solid
homogeneous crystalline structure with strong intermolecular forces and high surface energy which makes bonding relatively easy and predictable (Baier, 1992),
whereas dentin consists of HA (70 wt.%; 40% 45% in vol.), water (10 wt.%;
20% 25% in vol.), and organic matrix (20 wt.%; 30% in vol.) and presents a challenge to achieve optimal adhesion due to its chemical composition, level of moisture, and morphological variation. In addition, morphological and biomechanical
changes which occur in the dentin due to the physiological and pathological processes can make the adhesion process complex and challenging (Vinagre and
Ramos, 2016).
The success or failure of resin restorations is substantially dependent on the quality of adhesives which in turn is crucially dependent on the correct isolation of the
operative site from the fluid (dentinal fluid and saliva) and water. The main goals
of adhesion are (1) restoration retention and stability; (2) absorption and counteraction of shrinkage stresses; (3) pulp dentin complex sealing; (4) postoperative sensitivity reduction; (5) tooth structure reinforcement; and (6) reduction or elimination
of microleakage (Barkmeier and Cooley, 1992; Lutz et al., 1996).
Adhesives used in restorations perform the following functions (Brenna, 2012;
Bowen and Marjenhoff, 1992):
G
G
G
Long-term durability of the restoration by providing a perfect seal
Functional rehabilitation of the tooth by distributing forces
Provide retention to the restoration and counter shrinkage stresses
In the last three decades, much progress has been made in dental adhesives with
substantial improvement in their properties and ease of application. However, still,
bond failure and recurrent caries at the restoration tooth interface constitute the
major cause of restoration replacement. New developments in dental adhesives are
focused on imparting antibacterial and bioactive properties to improve their clinical
performance further.
11.2
Indications of adhesives
With the advancement in adhesives and development of restorative materials, the
use of adhesives has widened substantially, and they are being used in numerous
dental procedures, listed as follows (Perdigão and Sezinando, 2013):
1.
2.
3.
4.
5.
6.
restoration of carious and noncarious defects;
bonding of indirect restorations (crowns, inlay, and onlay);
bonding of partial and full resin veneers
in diastema closure;
pit and fissure sealant;
orthodontic bracket cementation;
Enamel etching and dental adhesives
231
7. desensitizing of the exposed tooth root;
8. sealing of root canal; and
9. bonding of fiber or metal posts.
11.3
Composition of adhesives
The main components of adhesive systems include the one described in the following subsections (Sofan et al., 2017a; Erickson, 1992).
11.3.1 Etchant
The etchant used in adhesive systems demineralizes the tooth structure and produces microporosities in which primer and bonding flow to produce micromechanical bonding. The etchant used in etch-and-rinse systems is 35% 37% phosphoric
acid. Whereas in self-etch systems an acidic monomer acts as both an etchant and a
primer.
11.3.2 Primer
Hydrophilic monomers in water-soluble solvents (acetone, ethanol, and water) for
improved flow and penetration into porous tooth substrate are used as primers.
These primers increase the wettability of adhesives on the etch tooth surface.
11.3.3 Bonding
Unfilled fluid resins have been used as a bonding agent between the tooth and composite and are mostly light-cured. The basic mechanism behind the bonding of dental restorations with the dentin and enamel is by the exchange of minerals or ions
from the dental hard tissue with resin of the restoration. To fulfill this concept, etching is the first line of action. Enamel etching technique is used to remove the smear
layer and create a rough surface. The “smear layer” term was first introduced by
McComb and Smith (1975). According to them, an amorphous smear layer was produced due to the instrumentation during the cutting and shaping of enamel and dentin. This smear layer consists of inorganic and organic parts of the dental tissue.
The bonding between the restoration and the dentin is compromised due to the presence of the smear layer, which is 0.5 5.0 μm thick and has the ability to block the
dentinal tubules. On the other hand, it reduces the permeability of the dentin and
acts as a “diffusion barrier.” Some studies showed that the presence of a smear
layer might reduce or inhibit the bacterial growth due to reduced dentin permeability. A study showed that with the application of sodium hypochlorite (NaOCl) and
mild hypochlorous acid (HOCl) solutions, the organic component on the smear
layer-covered dentin could be removed, which could eliminate the hybridized smear
layer created by self-etch adhesive, leading to the reduction of nanoleakage within
232
Advanced Dental Biomaterials
the hybrid layer (HL) (Thanatvarakorn et al., 2014). Therefore the main objective
of enamel etching is to remove the smear layer and produce a rough surface by dissolving the enamel rods or prisms. It encourages the adhesive to flow between the
indentations and provide the micromechanical retention for the resin-based composite materials and restorations. However, there is no scientific consensus on the efficacy of the removal of the smear layer in the root canal treatment (Moszner et al.,
2005).
11.4
Types of enamel etching
Mainly, enamel etching has been divided into the following:
G
G
acid etching and
laser etching.
11.4.1 Acid etching
The acid etching technique was first presented by Buonocore in 1955 for etching
the enamel surface of the tooth (Buonocore et al., 1968). According to his hypothesis, industrial phosphoric acid, which was used in paints and acrylic coating for
metals, can be used to adhere the acrylic resin with the enamel of the tooth after
etching with 85% phosphoric acid for 30 seconds. The acid etching technique can
remove the superficial layer of enamel up to 10 μm and produce a rough porous
surface, where it is expected that the average pore size is 5 50 μm, which helps in
the formation of “resin tags” and also increases the wettability of the enamel surface (Devarasa et al., 2012).
It is important to know the pattern of acid etching of enamel. There are three
major types of pattern produced by acid etching (Gwinnett, 1994), which are as
follows:
G
G
G
Type 1: Removal of the enamel prism core, the peripheral prism remains intact.
Type 2: Reverse of the type 1 process; the peripheries of the cores are removed, leaving
the enamel prism core intact.
Type 3: A somewhat total-etch technique in which prism morphology is less distinctive.
Furthermore, acid etching increases the bond strength between the restoration
and the dental hard tissue. It also reduces the microleakage around the restoration
and reduces the chances of secondary caries. However, a drawback associated with
etching is that the outermost strongest layer of the enamel surface is lost, which
makes it more prone to acid attacks. Acid etching procedure needs to be further
simplified, with a reduction in the steps and the amount of enamel loss should be
reduced, as the conservative approach is appreciated in the modern restorative dentistry (Peumans et al., 2005). To etch the enamel surface, many types of inorganic
acids and chelators have been used; however, it is important to determine which
acid treatments would yield favorable results consistently on tooth surfaces. Among
Enamel etching and dental adhesives
233
the many types of etchants that have been used clinically, phosphoric acid-based
etchants have gained popularity.
11.4.1.1 Phosphoric acid
In the etch-and-rinse technique, 30% 40% phosphoric acid is applied on the tooth
surface for 30 60 seconds and then rinsed off. A range of concentrations of the
phosphoric acid have been used in the etching process. By using 37% phosphoric
acid the prismatic and interprismatic crystal on the enamel surface is dissolved and
a rough and porous surface is formed, which may be 5 50 μm in depth. If the phosphoric acid concentration is less than 27%, then it forms dicalcium phosphate dihydrate precipitate which is difficult to remove. In contrast, if the concentration of the
phosphoric acid is increased to more than 40% it reduces the dissolution of the calcium which results in the shallow etching pattern (Silverstone, 1974). Therefore
commercially available etchant contains phosphoric acid in a 37% concentration.
The recommended time for acid etching is 15 20 seconds; however, a comparative
study showed that the 15 seconds etching provided similar surface roughness as
compared to 60 seconds. However, a shorter etching time resulted in less bonding
strength. It is important to know that the acid-treated surfaces are more prone to
caries and the strength of the enamel may reduce (Swift et al., 1995). Another
application of the 37% phosphoric acid is to apply it onto the tooth surface for
60 seconds before bleaching. It helps in better penetration of the bleaching agent
into the enamel surface and gives better results.
It is established that there are morphological and histological differences
between the primary and permanent teeth; therefore the infiltration of resins is
reduced in primary dentition due to aprismatic enamels. It is reported that no significant differences in the micromorphology of the enamel surface of primary teeth
were found for etching times ranging from 15 to 120 seconds (Garcia-Godoy and
Gwinnett, 1991). Another study reported no significant difference in bond strength
for primary enamel when etched for 60 240 seconds (Smutka et al., 1978).
However, Bozalis et al. (1979) suggested that primary enamel should not be etched
for more than 180 seconds.
11.4.1.2 Citric acid
Citric acid is considered as a weak organic acid and is used in periodontal infection
or diseases after the flap surgeries or on instrumentation to recover the cementum
and reduce the healing time. It has been applied as a conditioner and weak etchant
and it is reported that the use of 50% citric acid is effective and significantly
removes the surface smear layer (Prado et al., 2011). It can also be used as an irrigating material for the root canal treatment, where the best results can be obtained
by using citric acid of pH 1.1 to remove the smear layer (Haznedaroğlu, 2003).
Another study showed that the most effective pH of citric acid used for the complete removal of smear layer is between pH 1.1 and 1.9 (Di Lenarda et al., 2000).
The advantages the citric acid are (1) antibacterial properties; (2) cytotoxic effect;
234
Advanced Dental Biomaterials
Figure 11.1 SEM of dentin surface etched with 50 wt.% citric acid at a pH of 0.7, the acid
has produced a porous and clean dentinal surface (Breschi et al., 2002).
and (3) removal of the smear layer (Hennequin and Douillard, 1995). Fig. 11.1
shows the SEM image of dentinal tubules after etching with 50% citric acid of pH
0.7 and it exhibits good etching of the smear layer with the production of porous
and clean intertubular dentin. Other alternative materials for acid etching are 10%
melic acid and 2.5% nitric acid which are as effective as the above. Melic acid is
used for conditioning dentin and enamel surfaces.
11.4.1.3 Ferric chloride solution
Though the effect of ferric chloride is not completely understood, 3% ferric chloride solution has been used for acid etching before applying the adhesive and the
placement of the restoration. It is suggested that the use of ferric chloride may have
the following advantages (Saeki et al., 2001):
G
G
G
G
It can promote polymerization (Bowen, 1980).
It may help in the cross-linking and stabilizing the etch collagen network.
It protects the demineralized matrix from degradation during the drying procedure.
It helps in the denaturation of the collagen matrix during the process of etching
(Mizunuma, 1986).
Amalgambond (Parkell Dental, United States) was first developed by
Nakabayashi et al. (1982) and used in the dentin bonding system containing 10%
citric acid and 3% ferric chloride. Amalgambond has the ability to remove the
smear layer over the dentin and produce the rough surface up to 2 μm in depth. It
can also be used to bond the amalgam with the dentin. The shear bond strength of
this bond system is less than or equal to 20 MPa (Barbour and Rees, 2004).
Enamel etching and dental adhesives
235
11.4.1.4 Sodium hypochlorite
The first bleaching agent proposed was sodium hypochlorite which has been used
as a microabrasive material to remove the superficial layer of the enamel. It has
been used to remove superficial stains on the tooth surface which do not extend to
the deeper layer of the enamel. In the case of moderate to severe fluorosis, the conservative treatment of surficial discoloration includes treatment by using sodium
hypochlorite alone or with the bleaching agent. However, it is not an alternative to
the definitive restorative management including veneers, which are placed by
reducing the enamel surface. This sodium hypochlorite etching technique can be
useful in treating young patients who are more concerned about the esthetic and
color of teeth.
The sodium hypochlorite solution has been used extensively to remove or clean
the organic structure by oxidizing it. The hypomineralized enamel lesion can be
degraded, and the chromogenic organic materials present on the enamel surface can
be removed by applying the sodium hypochlorite. It is recommended to apply 5%
sodium hypochlorite to the superficial layer of the enamel for 5 10 minutes with
the bleaching agent, if the staining or discoloration persists then reetch for 60 seconds and rinse.
11.4.1.5 Ethylenediamine tetra-acetic acid
In older patients, the mineral content, tertiary dentin and/or “sclerotic dentin,”
become resistant to acid etching techniques. At the microscopic level, the dentinal
tubules are constricted due to the calcification and thickening of peripheral dentin.
For complete removal of the smear layer, a mixture of hypochlorite, chelating
agents (ethylene diamine tetra-acetic acid (EDTA) or quaternary ammonium bromide (cetrimide) added EDTA), and acids (maleic, citric, and polyacrylic acid)
have been used to dissolve the organic and inorganic part of the dental hard tissue.
Sodium hypochlorite and EDTA can be used as an alternative for the irrigation in
root canal treatment. It is proven that the EDTA completely removes the smear
layer if applied for 2 3 minutes on the tooth structure. The main drawback of the
EDTA is prolonged working time for etching or endodontic treatment (Prado et al.,
2011). Moreover the EDTA with aqueous citric acid can also be used to irrigate the
root canal in endodontic treatment (Yamaguchi et al., 1996).
11.4.2 Laser etching
Due to the limitation of the acid etch techniques, “laser irradiations” can be used to
remove the smear layer after preparation of the tooth cavity. One of the alternatives
is the erbium, chromium:yttrium scandium gallium garnet (Er,Cr:YSGG) radiation from the laser which creates many small pores or a rough surface by melting
the superficial layer of the enamel and recrystallizing the enamel rods or prisms.
The pattern obtained after the laser etching is somewhat similar to that seen in the
type 3 acid etching technique (Ghaffari et al., 2017). The recrystallization of the
236
Advanced Dental Biomaterials
Figure 11.2 Er,Cr:YSGG laser-irradiated dentin surface showing scaly, irregular, and rugged
appearance (Tseng et al., 2007). Er,Cr:YSGG, Erbium, chromium:
yttrium scandium gallium garnet.
enamel surface shows the fungiform appearance of the enamel surface, which sufficiently increases the micromechanical or chemical retention of the restoration with
the tooth structure. Fig. 11.2 shows the Er,Cr:YSGG laser-irradiated dentin surface
with a scaly, irregular, and rugged appearance (Tseng et al., 2007). Due to these
properties, it may be a good alternative to the conventional acid etching technique
because it does not induce any pain, heat, or vibration (Lee et al., 2003). The results
of bond strength between the restoration and tooth structure by laser etching are still
controversial.
11.4.3 Self-etching
This is the new technique which contains acidic monomer in the polymerizable
form and has a dual function as conditioner and primer for enamel and dentin
(Moszner et al., 2005). By using the self-etching technique, the number of steps is
reduced, as rinsing of phosphoric acid from enamel and dentin is not required. Its
action is similar to the conventional etching and rinse technique to remove the
smear layer from the dental hard tissue, however, in comparison, the enamel surface
is less retentive, as shown in Fig. 11.3. Its application involves two steps: first
application of self-etching primer (SEP) on dentin and enamel followed by adhesive
resin application. These SEPs are known as sixth generation (Kugel and Ferrari,
2000). In recent advancements, one-bottle and one-step self-etching have been
introduced to the market, which is known as seventh generation (Cal-Neto and
Miguel, 2006). Methacrylate-based SEP or bonding agents having the pH 1.5 2.5
are currently used. There are some limitations or drawbacks in the one component
self-etching, that is, it tends to absorb more water and hydrolytically degrade the
dimethacrylate-based resins.
Enamel etching and dental adhesives
237
Figure 11.3 Enamel surface after etching with a self-etching primer solution; the enamel
surface is less retentive than that obtained with phosphoric acid (Kugel and Ferrari, 2000).
11.5
Classifications of adhesives
Dental adhesives can be classified based on various factors, which include the
following:
G
G
G
different generations as they developed;
number of clinical steps involved; and
their action on the smear layer.
11.5.1 Classification based on generations
11.5.1.1 First-generation adhesives
Developed in the 1960s by Bowen, Cervident (S White Burs, Inc, Lakewood, New
Jersey) was the first-generation dentin bonding agent. It consisted of N-phenylglycine-glycidyl methacrylate comonomer. It was claimed to have the ability to chelate
with calcium in the tooth structure. However, the clinical results were not very
promising with a bond strength of only 2 3 MPa (Kugel and Ferrari, 2000; Sofan
et al., 2017a; Barkmeier and Cooley, 1992).
11.5.1.2 Second-generation adhesives
Clearfil Bond System F introduced in 1978 was the first product of secondgeneration dentin adhesives. It was suggested that second-generation systems make
bonds to the dentin surface through an ionic bond between calcium and chlorophosphate groups. Although the produced bond was stronger than that of the first generation, however, the bond strength of second-generation dentin bonding agent was
1 5 MPa which was still below the 10 MPa required for acceptable in vivo retention. The bond produced by the second generation was prone to hydrolysis when
238
Advanced Dental Biomaterials
exposed to saliva or moisture in the dentin, which could result in debonding of restoration. In addition, as no etching was involved in earlier generations, the adhesion
was due to bonding to the smear layer which was weak and unreliable (Kugel and
Ferrari, 2000; Barkmeier and Cooley, 1992).
11.5.1.3 Third-generation adhesives
In 1979 Fusayama et al. introduced acid etching of dentin before application of
bonding agent. However, acid etching did not produce much improvement in the
dentin bonding due to the hydrophobic nature of bonding resin. In addition, it was
thought that acid etching might produce pulpal inflammation, which limited its use.
Most of the third-generation bonding systems developed at that time did not remove
the entire smear layer but modified it. These materials modify the smear layer and
slightly demineralize the underlying intertubular dentin. Third-generation adhesives
produced both poor and good results. Scotchbond 2 (3M ESPE, Germany) was the
first material of this kind which was fully accepted by American Dental
Association (ADA) (Kugel and Ferrari, 2000; Heymann et al., 2013).
11.5.1.4 Fourth-generation adhesives
Fourth-generation dentin adhesive systems were developed to be used on acidetched dentin and consisted of etchant, primer, and bonding, which were applied to
the tooth one after another. Acid application on dentin removes the smear layer,
demineralizes intertubular and peritubular dentin, opens the dentin tubules, and
exposes the collagen fiber network (Fig. 11.4). Acid etching changes the mineral
content of dentin substrate and reduces its surface free energy. As dissolved HA has
high surface energy and the exposed collagen network has low energy surface, the
primer used in these systems increases the surface energy of dentin. The bonding
mechanism between the adhesive material and etched dentin substrate is achieved
by the formation of resin tags and adhesive lateral branches in the dentin porosities.
Figure 11.4 Scanning electron micrograph of etched dentin showing exposed collagen fibers
and open dental tubules (Pashley et al., 2011).
Enamel etching and dental adhesives
239
Figure 11.5 SEM image of the resin dentin interface, showing RC, the AR, HL, adhesive
resin tags (T), and dentin (D) (Mortazavi et al., 2012). AR, Adhesive resin; HL, hybrid layer;
RC, resin composite.
Primer and bonding resin penetrate etched intertubular dentin producing a
resin dentin interdiffusion zone or HL (Fig. 11.5) (Mortazavi et al., 2012).
Depending on the acid type, concentration, and application time, dentin is demineralized up to 7.5 μm. These systems produce bond strength between 17 and 30 MPa.
These adhesives systems are however time-consuming and technique-sensitive. As
in the fourth-generation adhesives, enamel and dentin are etched simultaneously;
these systems were initially called the “total-etch” technique, now they are commonly known as the “three-step etch-and-rinse” technique (Kugel and Ferrari, 2000).
11.5.1.5 Fifth-generation adhesives
Fifth-generation adhesives are two-step etch-and-rinse systems. They simplify the
bonding procedure by combining the primer and bonding agent in a single solution
and are applied simultaneously. They are also called “one-bottle” systems.
However, a separate etching step is still required. They have an acceptable bond
strength, are less technique-sensitive, easy to use, and have reduced postoperative
sensitivity (Sofan et al., 2017a).
11.5.1.6 Sixth-generation adhesives
The sixth-generation adhesive systems are two-steps self-etch systems. Two-steps
self-etch systems employ SEPs which do not require rinsing. These systems are
also described as “nonrinsing conditioners” or “self-priming etchant.” In the SEP
system, etching and priming of enamel and dentin are done simultaneously. Since
the rinsing and drying step is eliminated in SEP, the chances of over- or underdrying of dentin are reduced. These systems are less technique sensitive than etch-andrinse systems. There are less chances of discrepancy between demineralization and
resin infiltration depth as both happen simultaneously. In addition, there may be
less chances of postoperative sensitivity with SEP as compared to an etch-and-rinse
240
Advanced Dental Biomaterials
system, as SEPs do not eradicate the smear layer. Although these adhesives produce
good bond strength to dentin, the bond strength to enamel is comparatively less
than that produced by fourth- and fifth-generation adhesives.
11.5.1.7 Seventh-generation adhesives
In seventh-generation systems, etching, priming, and bonding have been combined
in a single solution and as a single step. These are also called “one-step self-etch”
or “all-in-one” adhesive systems. Although the clinical procedure is simplified in
the seventh-generation systems, their highly hydrophilic nature makes them liable
to water degradation and the bond strength of seventh-generation adhesives is lowest among all the adhesives systems (Sofan et al., 2017b).
11.5.1.8 Eighth-generation adhesives
Futurabond DC (Voco, United States) containing nano-sized fillers were introduced in 2010 by Voco America as eighth-generation adhesives systems. These
adhesives systems, owing to the presence of nanofillers, have higher penetration
into the etched dentin and produce a thicker HL with improved mechanical properties. They have increased bond strength to enamel and dentin and better stress
absorption. As the filler acts as a cross-linking agent, these systems have better
dimensional stability (Sofan et al., 2017a). However, a study showed that increasing
the nanofiller content beyond 1 wt.% increases the viscosity of the adhesive which
may cause them to accumulate as clusters which can lead to cracks and bond disintegration (Kasraei et al., 2009).
11.5.2 Classification based on clinical steps
Dental adhesives can also be classified based on the number of clinical steps
involved. They are classified as either one-, two-, or three-step adhesive systems.
11.5.2.1 Three-step etch-and-rinse systems
These adhesive systems involve three steps, which include etching, priming, and
bonding, all of which done separately. These adhesives systems are supplied in
three bottles, each for etchant, bonding, and primer. Among all the adhesive systems, three-step etch-and-rinse systems produce the most durable bonding and are
considered the gold standard (Van Meerbeek et al., 2003a).
11.5.2.2 Two-step systems
Two-step adhesive systems simplified the bonding procedure by combining two
steps. These systems are further subdivided as follows:
G
Two-step etch-and-rinse system. In these systems the priming and bonding steps are combined, as primer and bonding are supplied together in one bottle which is applied after
etching and rinsing.
Enamel etching and dental adhesives
G
241
Two-step self-etch systems are also known as “self-priming etchant.” These systems combine etching and priming steps, which are followed by the application of bonding without
rinsing.
11.5.2.3 One-step self-etch system
One-step adhesive systems combine etching, priming, and bonding steps. SEP and
bonding are supplied as one solution, supplied in a single bottle. These systems further simplify the bonding process (Sofan et al., 2017a).
11.5.3 Classification based on interaction with smear layer
Mechanically prepared dentin is covered by loosely bound smear layer, for a reliable bond between restorative resin and dentin; this smear layer must either be
removed or modified (Asmussen and Uno, 1992). Adhesive systems can be classified according to their effect on the smear layer (Brenna, 2012).
11.5.3.1 Smear layer removing systems
The adhesive systems which involve etch-and-rinse technique can be regarded as
smear layer removing systems. They are either three-step systems (etching 1 primer 1 bonding) or two-step systems (etching, primer 1 bonding). These systems
involve phosphoric acid etching of tooth substrates (enamel and dentin), which is
followed by rinsing with water for complete removal of acid. Acid application with
subsequent rinsing removes the smear layer and exposes surface roughness, enamel
prisms, dentinal tubules, and collagen network.
11.5.3.2 Smear layer dissolving systems
The adhesive systems that incorporate SEPs can be regarded as smear layer dissolving systems. These systems include two-step self-etch systems and one-step selfetching “all-in-one” systems which do not involve rinsing after application. These
adhesive systems do not remove the smear layer completely, rather they dissolve
the smear layer by infiltration.
11.6
Dentin bonding
Dentin is composed of HA, water, and organic matrix. It has a heterogeneous structure with low intermolecular forces and low surface energy. In addition, it is structurally and chemically altered by pathological processes, all this and the wet
surface due to fluid seepage make the bonding between dentin and restorative resin
complicated. Moreover, the tubular build-up of dentin and the resulting outward
pulpal water current in vital teeth turn dentin into a complex substrate (Baier, 1992;
Erickson, 1992; Van Meerbeek et al., 2003b; Perdigão, 2010).
Tooth structure cutting during cavity preparation results in the formation of the
smear layer which is loosely attached to the tooth surface. This smear layer is
242
Advanced Dental Biomaterials
composed of organic and inorganic components from enamel, dentin, or cementum,
which in clinical conditions is usually contaminated with saliva, blood, and bacteria. It covers the dentin surface and blocks the dentinal tubules by forming smear
plugs (Tao et al., 1988). Two strategies are generally employed to address the presence of the smear layer; these include complete removal of the smear layer before
bonding or the use of bonding agents which can penetrate the smear layer while
incorporating it. However, the removal of the smear layer and smear plugs increases
the dentinal tubules permeability, allowing fluid flow from and to the pulp chamber
(Pashley and Carvalho, 1997; Van Meerbeek et al., 2003b).
Bond strength of resin monomer to caries-affected dentin is lower than in sound
dentin. The HL produced in caries-affected dentin is thicker than that produced in
normal dentin, as affected dentin is more susceptible to acid, which leads to deeper
penetration of adhesive resins, whereas the penetration of adhesive resin into the
dentinal tubules is obstructed by acid-resistant mineral deposits in the dentinal
tubules. Lack of resin tag hybridization to peritubular dentin, due to acid-resistant
mineral deposits, decreases the cohesive strength of caries-affected dentin and leads
to lower bond strength to affected dentin (Say et al., 2005; Wei et al., 2008).
Studies showed that dentin aging does not significantly affect the bond strength
between dentin and adhesive resins (Lopes et al., 2011; Ozer et al., 2005).
The inherently wet nature of dentin makes it difficult to clinically dry it
completely. Excessive drying of dentin can lead to the collapse of the collagen network which prevents the infiltration of adhesive resin into the nanochannels produced due to HA dissolution between collagen fibers. Subsequently, it results in
reduced bonding between the resin and dentin. This led to the development of the
“moist bonding” technique in which dental adhesives can be used on a moist dentin
surface. These adhesives incorporate organic solvents such as acetone and ethanol
with primers or adhesives. These solvents enhance the penetration of resin monomers into the dentin collagen network, as they displace water from the moist dentin
surface and intact collagen network, which results in enhancing bond strength
(Kanca, 1992; Perdigao, 2002).
11.7
Advancement in adhesives
11.7.1 Antibacterial properties
Secondary caries is the major cause of restoration failures and replacements.
Bacterial invasion between the restoration and tooth structure, due to microleakage
or the residual bacteria in the cavity, can lead to secondary caries formation (Kim
and Shin, 2014). It is desirable to have an adhesive system with antibacterial properties which can prevent colonization of bacteria and inhibit caries, resulting in
increased longevity of the restoration (Amin et al., 2014; Imazato et al., 2014; Chen
et al., 2014). Various studies investigated the antibacterial potential of adhesive systems by incorporating nanoparticles of silver (NAg), nanoparticles of amorphous
calcium phosphate (NACP), fluorine ions, zinc oxide, quaternary ammonium
Enamel etching and dental adhesives
243
dimethacrylate (QADM), 12-methacryloyloxydodecyl pyridinium bromide
(MDPB), benzalkonium chloride, and chlorhexidine (Cheng et al., 2015; Zhang
et al., 2013; Melo et al., 2013; Passariello et al., 2014; Andre et al., 2015; Wiegand
et al., 2007). However, the antibacterial activity of silver particles and fluorine ions
decreases over time and may adversely affect the material’s physical properties. In
contrast, another study showed that the silver nanoparticles could have positive
effects on bond strength of both etch-and-rinse and self-etch adhesive systems. It is
further reported that the best results of silver nanoparticles are achieved if they are
applied before acid etching (Fatemeh et al., 2017).
In a study, 0.1 wt.% NAg was added to the primer which was produced with pyromellitic glycerol dimethacrylate and 2-hydroxyethyl methacrylate, whereas the
adhesive consisted of bisphenol-A-glycerolate dimethacrylate and triethylene glycol
dimethacrylate, in which 0.1% NAg, 10% QADM, and 0% 40% NACP were
added. The results showed that incorporation of NAg, QADM, and NACP into the
bonding system greatly reduced human saliva microcosm biofilm viability, metabolic activity, lactic acid production, and colony-forming units of microcosm biofilms (Melo et al., 2013). It is believed that the bactericidal action of quaternary
ammonium (QA) is due to three processes: (1) interaction between negatively
charged bacterial cell and positively charged QA which results in the increase in
osmotic pressure; (2) diffusion of QA through the cell wall and binding to the cytoplasmic membrane; and (3) cytoplasmic membrane disruption which leads to
release of cytoplasmic constituents and cell death (Cocco et al., 2015; Han et al.,
2017). The proposed mechanism of antibacterial action of QA is given in Fig. 11.6.
In another study, quaternary ammonium monomer dimethylaminododecyl methacrylate (DMADDM) and NACP were incorporated into commercially available
bonding agent (Scotchbond Multi-Purpose; 3M, St. Paul, Minnesota) to investigate
Figure 11.6 Proposed mechanism of antibacterial action of QA (Cocco et al., 2015). QA,
Quarternary ammonium.
244
Advanced Dental Biomaterials
its antibacterial potential, the results showed that DMADDM and NACP substantially reduced metabolic activity, lactic acid formation, and the total streptococci
and Streptococcus mutans of the biofilm (Chen et al., 2014). Another in vitro study
also investigated the incorporation of 2-methacryloyloxyethyl phosphorylcholine,
dimethylaminohexadecyl methacrylate (DMAHDM), and NACP into Scotchbond
Multi-Purpose bonding agent for root dentin coating to prevent caries with promising antibacterial and remineralizations results (Zhang et al., 2015b). A recent study
showed that DMAHDM and NACP added into a bonding for root caries application
has a potent effect on periodontal and endodontic pathogens (Wang et al., 2016).
In an in vitro study, Passariello et al. (2014) compared antibacterial properties of
multiple bonding agents by placing disks samples in culture media seeded with
Streptococcus gordonii, Streptococcus sanguinis, S. mutans, or Lactobacillus acidophilus. The study showed that the bonding agents containing MDPB, benzalkonium chloride, and chlorhexidine have the highest antibacterial activities for the
longest duration of time among all the materials assessed. Another study compared
the antibacterial properties of three commercially available adhesives systems with
different antibacterial components. The adhesive systems compared were Gluma
2Bond (Glutaraldehyde), Clearfil SE Protect (MDPB), and Peak Universal Bond
(Chlorhexidine). These adhesives systems were applied on the dentin surface of
extracted teeth which were then restored with composites. The antibacterial activity
of these adhesives was evaluated by direct contact method against four strict anaerobic and four facultative bacteria for up to 24 hours. The results showed that among
the adhesive systems, MDPB coating adhesive systems have the highest antibacterial activity (Andre et al., 2015). Clearfil Protect Bond (Kuraray Medical,
Okayama, Japan), an antibacterial adhesive containing MDPB, has bactericidal
properties in uncured form and when applied into the cavity acts as a disinfectant.
Once cured it inhibits the growth of the bacteria by destroying their cell membranes
which come in direct contact with the restoration. When applied on the dentin surface Clearfil Protect Bond can penetrate to a depth of 500 μm. One of the major
causes of secondary dentin is residual bacteria. Since MDPB-containing adhesive
system has cavity disinfecting properties, it may improve the long-term prognosis
of the restoration (Andre et al., 2015; Imazato et al., 2014). In a clinical study,
Clearfil Protect Bond used for orthodontic bracket cementation showed reduced
enamel demineralization around orthodontic brackets compared to a conventional
adhesive (Transbond XT, 3M Unitek, Monrovia, California) during a 30-day period
(Uysal et al., 2010). It is reported that MDBP can be used to improve bonding durability by inhibiting matrix metalloproteases and cathepsins (Tezvergil-Mutluay
et al., 2011, 2015).
Li et al. (2009) incorporated QA groups, that is, methacryloxylethylcetyl dimethyl
ammonium chloride, into the dental adhesive and observed that the modified adhesive influenced the growth, adherence, and membrane integrity of S. mutans.
Jedrychowski et al. (1983) reported that the small concentrations of chlorhexidine
increased the antibacterial activity without compromising the mechanical properties.
Su et al. incorporated nisin (an antibacterial peptide) in dental adhesives. Nisin
has been approved as generally recognized as safe by the US Food and Drug
Enamel etching and dental adhesives
245
Administration since 1988 because of its long-term use in food preservation (E234)
without causing health problems. It has effective antibiotic activity against cariogenic microorganisms. The results of this study showed that the nisin-incorporated
adhesive significantly suppressed the growth of S. mutans. However, with the
increase in concentration of these peptides, the bond strength was decreased (Su
et al., 2018).
Zinc oxide (ZnO) has been widely used in health sciences (Sarwar et al., 2017).
In dental materials it shows antibacterial properties, inhibition of metalloproteinases, and biocompatibility (Wu et al., 2018; Henn et al., 2011; Toledano et al.,
2012). It is reported that the antibacterial activity of ZnO is higher at the nanoscale
(Mirzaei and Darroudi, 2017; Raghupathi et al., 2011); however, the mechanism
behind these results is not well established. ZnO has been synthesized at the nanometric dimension in quantum dots (QDs) and these presented enhanced properties
compared to material in the “bulk” form. Recently, ZnO QDs (ZnOQDs) were incorporated in experimental dental adhesive and investigated for antibacterial properties. It was found that the addition of ZnOQDs reduced biofilm formation in
experimental adhesive resin surface by about 50%. It is anticipated that ZnO nanoparticles bound on the microorganism’s surface and disorganized the bacterium
membrane by modifying the molecular structure of phospholipids, entering into the
cell matrix and leading to modification of the cell shape and to leakage of intracellular constituents (Garcia et al., 2018).
In another study, nanocapsules containing indomethacin and triclosan were
added to commercial and experimental dental adhesives and this study confirmed
the favorability of adding nanocapsules for achieving a reliable long-term bond performance. Addition of nanocapsules in dental adhesives can prevent the inflammatory process of pulp tissue in deep cavities and protect against caries through
controlled drug release via these nanocapsules. Furthermore, these experimental
adhesives had no influence on the in situ degree of conversion or the immediate
bond strength. However, the bond strength decreased after 1 year of aging (Genari
et al., 2018).
Geraldeli et al. introduced various concentrations of arginine in experimental
dental adhesives. Arginine is an amino acid found in a variety of foods and is also
naturally produced by the human body and secreted in saliva in free form or as salivary peptides. It was found that the adhesive system containing 7% arginine was
able to retain appropriate physical and mechanical properties. Moreover, it showed
controlled release and moderate recharge of arginine over a prolonged period of
time. Arginine was released from the adhesive system at a rate and concentration to
exhibit antibacterial effect (Geraldeli et al., 2017).
11.7.2 Bioactive properties
Since their development, dental adhesives have come a long way regarding their
bonding ability and ease of application. However, the tooth restoration interface
remains the weakest link in the restorations. Microgap formation at the interface
leads to microleakage, which results in secondary caries formation. To increase the
246
Advanced Dental Biomaterials
longevity of the restorations by further improving the clinical performance of adhesive, recent developments include imparting bioactive properties in addition to antibacterial properties to the bonding resins (Zhang et al., 2015a; Taubock et al.,
2014; Tay and Pashley, 2009; Chen et al., 2014).
Synthetic calcium phosphate materials, that is, amorphous calcium phosphate,
HA, monocalcium phosphate monohydrate, and β-tricalcium phosphate, have been
incorporated in dental adhesives (Eliaz and Metoki, 2017; Xie et al., 2017; Pei
et al., 2017; Sfalcin et al., 2017; Yokota et al., 2016). Bioactive glass (BAG) is
another type of bioceramic, which has gained popularity since its invention in 1969
by Prof. Hench. It consists mainly of silicon, calcium, sodium, phosphorous, and
oxygen (Yoshihara et al., 2017) and has also been used as dental adhesive to remineralize the tooth surface (De Morais et al., 2018). These bioactive fillers can bond
with the living tissue chemically by forming a calcium phosphate layer at the toothmaterial interface that renders the restoration durable and prevents it from bacterial
ingression (Khan et al., 2008).
Dental adhesives with remineralizing capabilities have been developed. An adhesive with the ability to release Ca and P ions may enhance the HA formation which
is the main mineral component of the tooth structure. Ca and P ions released from
the adhesive can facilitate in the remineralization of the dentin HL and at the margins of the restoration and the tooth surface. The remineralization of the HL can
make it more resistant to oral environment degradation and capable of neutralizing
biofilm acid. In addition, Ca and P released from an adhesive may contribute to the
remineralization of infected and affected cavity lesions (Imazato et al., 2014; Zhang
et al., 2015a). A 30-day in vitro study employed demineralization/remineralization
cyclic regimen to assess the remineralization potential of NACP nanocomposites.
The results showed that the remineralization effects of NACP nanocomposite on
human enamel were fourfold that of a commercial fluoride-releasing composite
(Weir et al., 2012). In another study, NACP was incorporated into commercially
available bonding agent (Scotchbond Multi-Purpose) and its remineralization potential was investigated. The results showed that incorporation of NACP at 40% filler
content resulted in increased release of Ca and P ions which have remineralization
potential (Chen et al., 2014).
BAGs have been widely used for bone defects repair and as an implant material
due to their bone regeneration ability. BAG has the ability to release calcium and
phosphate ions, which have remineralization effects on the demineralized tooth
structure. In addition, dissolution of BAG in an aqueous environment releases alkali
ions, resulting in an increase in pH which gives BAG antibacterial and acid neutralizing properties (Yang et al., 2013, 2016; Xie et al., 2008; Zehnder et al., 2004).
Remineralization of mineral-depleted areas by BAG reduces the micropermeability
along the dentin-bonded interface (Sauro et al., 2012). Formation of incipient caries,
known as white spot lesions (WSL) around orthodontic brackets, is a common side
effect of fixed orthodontic appliances. These lesions manifest demineralization of
enamel due to bacterial action. Cariogenic bacteria which surround orthodontic
appliances use fermentable carbohydrate to produce acids which lead to the reduction of the local plaque pH, resulting in the depletion of calcium and phosphate
Enamel etching and dental adhesives
247
ions from the enamel structure and resulting in WSL (Mitchell, 1992). Various
studies have reported on the incorporation of BAG in the adhesive systems for
orthodontic brackets. BAG addition in the adhesives has been shown to prevent
demineralization of enamel due to the Ca and P ion releasing ability, thereby preventing WSL (Yang et al., 2016; Brown et al., 2011; Manfred et al., 2013).
Sauro et al. (2012) investigated the beneficial effects of Bioglass 45S5 and zincpolycarboxylated BAG-based dental adhesives on the bonded dentin interface. The
concentration of these particles was 33 wt.%. The study showed an increase in
nanomechanical properties, while simultaneously reducing the micropermeability
along the dentin-bonded interface. This occurred by means of the therapeutic remineralization of imperfect mineral-depleted areas. Furthermore, the surface of the
specimen exhibited several “funneled” dentinal tubules with no exposed collagen
fibrils and it was mainly protected by residual resin and mineral crystals which
were embedded within a resin/collagen network. Both BAG and fluoride-based
BAG (F-BAG) resins induced the precipitation of mineral contents inside the dentinal tubules and onto the surface. Also, the F-BAG resins showed a higher modulus
of elasticity (13%) and an increase in stiffness of demineralized dentin when compared to BAG-based samples and control samples. This might be due to the release
of fluoride and phosphate ions, which can accelerate the remineralization process.
Recently, F-BAG and BAG have been added in dimethacrylate-based resins and it
has been found that F-BAG-based composite shows more bioactivity than conventional BAG, as well as accelerated dentin remineralization. F-BAG furthermore
showed a higher ability to reduce the solubilization of C-terminal cross-linked telopeptides and C-terminal telopeptides (Tezvergil-Mutluay et al., 2017). Khvostenko
et al. synthesized BAG (15 wt.%) and incorporated it into resin matrices along with
strontium glass, and their in vitro study showed a significant antimicrobial effect by
reducing the extent of bacterial biofilm penetration into preexisting marginal gaps.
Recently, niobium-based BAG has been incorporated in dental adhesives and results
showed that the commercial adhesive at 30% niobium-based BAG concentrations
did not compromise the bond strength of the dental adhesive, but did show high
radiopacity and presented mineral precipitation, which characterized the experimental adhesives as bioactive materials (Carneiro et al., 2018). Another study showed
that the incorporation of boron nitride nanotubes up to 0.15 wt.% improved the
chemical and mechanical properties of dental adhesives and promoted mineral
deposition (Degrazia et al., 2017). The dental adhesives based on these bioceramics
have shown their potential to be used in clinical dentistry.
11.8
Conclusion
It is well established that over time dental adhesives have shown quite
acceptable results. However, concern has been raised related to their mechanical
and physical properties. Therefore in the future, more research is required to
improve their physical and mechanical properties without decreasing the biological
248
Advanced Dental Biomaterials
potential. Furthermore, the improvement of their composition to enhance their antibacterial properties can help in minimizing the risks of secondary caries formation.
The use of bioceramics can improve biological and mechanical properties; an ionocovalent structural model of the calcium phosphate family seems promising as reinforcing fillers. Surface modification during in situ synthesis and doping with amine,
bromine, and with metal ions can also lead to improvements in the properties of fillers of dental adhesives. In conclusion we can say that so far the advancements in
dental adhesives are tremendous, but further research is required to optimize the
performance in clinical application fully.
References
Amin, S., Shetty, H.K., Varma, R.K., Amin, V., Nair, P.M., 2014. Comparative evaluation of
antibacterial activity of total-etch and self-etch adhesive systems: an ex vitro study. J.
Conserv. Dent. 17, 266 270.
Andre, C.B., Gomes, B.P., Duque, T.M., Stipp, R.N., Chan, D.C., Ambrosano, G.M., et al.,
2015. Dentine bond strength and antimicrobial activity evaluation of adhesive systems.
J. Dent. 43, 466 475.
Asmussen, E., Uno, S., 1992. Adhesion of restorative resins to dentin: chemical and physicochemical aspects. Oper. Dent. (Suppl. 5), 68 74.
Baier, R.E., 1992. Principles of adhesion. Oper. Dent. (Suppl. 5), 1 9.
Barbour, M., Rees, J., 2004. The laboratory assessment of enamel erosion: a review. J. Dent.
32, 591 602.
Barkmeier, W.W., Cooley, R.L., 1992. Laboratory evaluation of adhesive systems. Oper.
Dent. (Suppl. 5), 50 61.
Bowen, R., 1980. Adhesive bonding of various materials to hard tooth tissues. XXII. The
effects of a cleanser, mordant, and polySAC on adhesion between a composite resin and
dentin. J. Dent. Res. 59, 809 814.
Bowen, R.L., Marjenhoff, W.A., 1992. Development of an adhesive bonding system. Oper.
Dent. (Suppl. 5), 75 80.
Bozalis, W., Marshall, J.G., Cooley, R., 1979. Mechanical pretreatments and etching of
primary-tooth enamel. ASDC J. Dent. Child. 46, 43 49.
Brenna, F., 2012. Restorative Dentistry: Treatment Procedures and Future Prospects.
Elsevier/Mosby, St. Louis, MO.
Breschi, L., Gobbi, P., Mazzotti, G., Falconi, M., Ellis, T.H., Stangel, I., 2002. High resolution SEM evaluation of dentin etched with maleic and citric acid. Dent. Mater. 18,
26 35.
Brown, M.L., Davis, H.B., Tufekci, E., Crowe, J.J., Covell, D.A., Mitchell, J.C., 2011. Ion
release from a novel orthodontic resin bonding agent for the reduction and/or prevention
of white spot lesions. An in vitro study. Angle Orthod. 81, 1014 1020.
Buonocore, M., Matsui, A., Gwinnett, A., 1968. Penetration of resin dental materials into
enamel surfaces with reference to bonding. Arch. Oral Biol. 13, 61 70.
Cal-Neto, J.P., Miguel, J.A.M., 2006. Scanning electron microscopy evaluation of the bonding mechanism of a self-etching primer on enamel. Angle Orthod. 76, 132 136.
Enamel etching and dental adhesives
249
Carneiro, K.K., Araujo, T.P., Carvalho, E.M., Meier, M.M., Tanaka, A., Carvalho, C.N.,
et al., 2018. Bioactivity and properties of an adhesive system functionalized with an
experimental niobium-based glass. J. Mech. Behav. Biomed. Mater. 78, 188 195.
Chen, C., Weir, M.D., Cheng, L., Lin, N.J., Lin-Gibson, S., Chow, L.C., et al., 2014.
Antibacterial activity and ion release of bonding agent containing amorphous calcium
phosphate nanoparticles. Dent. Mater. 30, 891 901.
Cheng, L., Zhang, K., Weir, M.D., Melo, M.A., Zhou, X., Xu, H.H., 2015. Nanotechnology
strategies for antibacterial and remineralizing composites and adhesives to tackle dental
caries. Nanomedicine 10, 627 641.
Cocco, A.R., Rosa, W.L., Silva, A.F., Lund, R.G., Piva, E., 2015. A systematic review about
antibacterial monomers used in dental adhesive systems: current status and further prospects. Dent. Mater. 31, 1345 1362.
De Morais, R.C., Silveira, R.E., Chinelatti, M., Geraldeli, S., De Carvalho Panzeri Pires-DeSouza, F., 2018. Bond strength of adhesive systems to sound and demineralized dentin
treated with bioactive glass ceramic suspension. Clin. Oral Investig. 22, 1923 1931.
Degrazia, F.W., Leitune, V.C.B., Samuel, S.M.W., Collares, F.M., 2017. Boron nitride nanotubes as novel fillers for improving the properties of dental adhesives. J. Dent. 62,
85 90.
Devarasa, G., Subba Reddy, V., Chaitra, N., Swarna, Y., 2012. Self-etching adhesive on
intact enamel, with and without pre-etching. Microsc. Res. Tech. 75, 650 654.
Di Lenarda, R., Cadenaro, M., Sbaizero, O., 2000. Effectiveness of 1 mol L21 citric acid and
15% EDTA irrigation on smear layer removal. Int. Endod. J. 33, 46 52.
Eliaz, N., Metoki, N., 2017. Calcium phosphate bioceramics: a review of their history, structure, properties, coating technologies and biomedical applications. Materials 10.
Erickson, R.L., 1992. Surface interactions of dentin adhesive materials. Oper. Dent. (Suppl.
5), 81 94.
Fatemeh, K., Mohammad Javad, M., Samaneh, K., 2017. The effect of silver nanoparticles
on composite shear bond strength to dentin with different adhesion protocols. J. Appl.
Oral. Sci. 25, 367 373.
Garcia, I.M., Leitune, V.C.B., Visioli, F., Samuel, S.M.W., Collares, F.M., 2018. Influence
of zinc oxide quantum dots in the antibacterial activity and cytotoxicity of an experimental adhesive resin. J. Dent. 73, 57 60.
Garcia-Godoy, F., Gwinnett, A., 1991. Effect of etching times and mechanical pretreatment
on the enamel of primary teeth: an SEM study. Am. J. Dent. 4, 115 118.
Genari, B., Leitune, V.C.B., Jornada, D.S., Aldrigui, B.R., Pohlmann, A.R., Guterres, S.S.,
et al., 2018. Effect on adhesion of a nanocapsules-loaded adhesive system. Braz. Oral
Res. 32, e008.
Geraldeli, S., Soares, E.F., Alvarez, A.J., Farivar, T., Shields, R.C., Sinhoreti, M.A.C., et al.,
2017. A new arginine-based dental adhesive system: formulation, mechanical and anticaries properties. J. Dent. 63, 72 80.
Ghaffari, H., Mirhashemi, A., Baherimoghadam, T., Azmi, A., Rasooli, R., 2017. Effect of
surface treatment on enamel cracks after orthodontic bracket debonding: Er,Cr:YSGG
laser-etching versus acid-etching. J. Dent. 14, 259.
Gwinnett, A.J., 1994. Chemically conditioned dentin: a comparison of conventional and environmental scanning electron microscopy findings. Dent. Mater. 10, 149 155.
Han, Q., Li, B., Zhou, X., Ge, Y., Wang, S., Li, M., et al., 2017. Anti-caries effects of dental
adhesives containing quaternary ammonium methacrylates with different chain lengths.
Materials 10, 643.
250
Advanced Dental Biomaterials
Haznedaroğlu, F., 2003. Efficacy of various concentrations of citric acid at different pH
values for smear layer removal. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod.
96, 340 344.
Henn, S., Nedel, F., De carvalho, R.V., Lund, R.G., Cenci, M.S., Pereira-Cenci, T., et al.,
2011. Characterization of an antimicrobial dental resin adhesive containing zinc methacrylate. J. Mater. Sci. Mater. Med. 22, 1797 1802.
Hennequin, M., Douillard, Y., 1995. Effects of citric acid treatment on the Ca, P and Mg contents of human dental roots. J. Clin. Periodontol. 22, 550 557.
Heymann, H., Swift, E.J., Ritter, A.V., Sturdevant, C.M., 2013. Sturdevant’s Art and Science
of Operative Dentistry. Elsevier/Mosby, St. Louis, MO.
Imazato, S., Ma, S., Chen, J.H., Xu, H.H., 2014. Therapeutic polymers for dental adhesives:
loading resins with bio-active components. Dent. Mater. 30, 97 104.
Jedrychowski, J.R., Caputo, A.A., Kerper, S., 1983. Antibacterial and mechanical properties
of restorative materials combined with chlorhexidines. J. Oral Rehabil. 10, 373 381.
Kanca 3rd, J., 1992. Resin bonding to wet substrate. 1. Bonding to dentin. Quintessence Int.
23, 39 41.
Kasraei, S., Atai, M., Khamverdi, Z., Nejad, S.K., 2009. The effect of nanofiller addition to
an experimental dentin adhesive on microtensile bond strength to human dentin. J. Dent.
Tehran Univ. Med. Sci. 6, 36 41.
Khan, A.S., Ahmed, Z., Edirisinghe, M.J., Wong, F.S., Rehman, I.U., 2008. Preparation and
characterization of a novel bioactive restorative composite based on covalently coupled
polyurethane-nanohydroxyapatite fibres. Acta Biomater. 4, 1275 1287.
Kim, S.R., Shin, D.H., 2014. Antibacterial effect of self-etching adhesive systems on
Streptococcus mutans. Restor. Dent. Endod. 39, 32 38.
Kugel, G., Ferrari, M., 2000. The science of bonding: from first to sixth generation. J. Am.
Dent. Assoc. 131, 20S 25S.
Lee, B.-S., Hsieh, T.-T., Lee, Y.-L., Lan, W.-H., Hsu, Y.-J., Wen, P.-H., et al., 2003. Bond
strengths of orthodontic bracket after acid-etched, Er: YAG laser-irradiated and combined treatment on enamel surface. Angle Orthod. 73, 565 570.
Li, F., Chen, J., Chai, Z., Zhang, L., Xiao, Y., Fang, M., et al., 2009. Effects of a dental adhesive incorporating antibacterial monomer on the growth, adherence and membrane integrity of Streptococcus mutans. J. Dent. 37, 289 296.
Lopes, G.C., Vieira, L.C., Araujo, E., Bruggmann, T., Zucco, J., Oliveira, G., 2011. Effect of
dentin age and acid etching time on dentin bonding. J. Adhes. Dent. 13, 139 145.
Lutz, F., Krejci, I., Oddera, M., 1996. Advanced adhesive restorations: the post-amalgam
age. Pract. Periodontics Aesthet. Dent. 8, 385 394. quiz 398.
Manfred, L., Covell, D.A., Crowe, J.J., Tufekci, E., Mitchell, J.C., 2013. A novel biomimetic
orthodontic bonding agent helps prevent white spot lesions adjacent to brackets. Angle
Orthod. 83, 97 103.
Mccomb, D., Smith, D.C., 1975. A preliminary scanning electron microscopic study of root
canals after endodontic procedures. J. Endod. 1, 238 242.
Melo, M.A., Cheng, L., Weir, M.D., Hsia, R.C., Rodrigues, L.K., Xu, H.H., 2013. Novel dental adhesive containing antibacterial agents and calcium phosphate nanoparticles. J.
Biomed. Mater. Res. B Appl. Biomater. 101, 620 629.
Mirzaei, H., Darroudi, M., 2017. Zinc oxide nanoparticles: biological synthesis and biomedical applications. Ceram. Int. 43, 907 914.
Mitchell, L., 1992. Decalcification during orthodontic treatment with fixed appliances—an
overview. Br. J. Orthod. 19, 199 205.
Enamel etching and dental adhesives
251
Mizunuma, T., 1986. Relationship between bond strength of resin to dentin and structural
change of dentin collagen during etching. Influence of ferric chloride on structure of the
collagen. J. Jpn. Dent. Mater. 5, 54 64.
Mortazavi, V., Fathi, M., Ataei, E., Khodaeian, N., Askari, N., 2012. Shear bond strengths
and morphological evaluation of filled and unfilled adhesive interfaces to enamel and
dentine. Int. J. Dent. 2012, 858459.
Moszner, N., Salz, U., Zimmermann, J., 2005. Chemical aspects of self-etching enamel dentin adhesives: a systematic review. Dent. Mater. 21, 895 910.
Nakabayashi, N., Kojima, K., Masuhara, E., 1982. The promotion of adhesion by the infiltration of monomers into tooth substrates. J. Biomed. Mater. Res. Part A 16, 265 273.
Ozer, F., Sengun, A., Ozturk, B., Say, E.C., Tagami, J., 2005. Effect of tooth age on microtensile bond strength of two fluoride-releasing bonding agents. J. Adhes. Dent. 7, 289 295.
Pashley, D.H., Carvalho, R.M., 1997. Dentine permeability and dentine adhesion. J. Dent.
25, 355 372.
Pashley, D.H., Tay, F.R., Breschi, L., Tjäderhane, L., Carvalho, R.M., Carrilho, M., et al.,
2011. State of the art etch-and-rinse adhesives. Dent. Mater. 27, 1 16.
Passariello, C., Sannino, G., Petti, S., Gigola, P., 2014. Intensity and duration of in-vitro antibacterial activity of different adhesives used in orthodontics. Eur. J. Oral Sci. 122,
154 160.
Pei, D.D., Liu, S.Y., Yang, H.Y., Gan, J., Huang, C., 2017. Effect of a nano hydroxyapatite
desensitizing paste application on dentin bond strength of three self-etch adhesive systems. Zhonghua Kou Qiang Yi Xue Za Zhi 52, 278 282.
Perdigao, J., 2002. Dentin bonding as a function of dentin structure. Dent. Clin. North Am.
46, 277 301. vi.
Perdigão, J., 2010. Dentin bonding—variables related to the clinical situation and the substrate treatment. Dent. Mater. 26, e24 e37.
Perdigão, J., Sezinando, A., 2013. Enamel and dentin bonding for adhesive restorations. NonMetallic Biomaterials for Tooth Repair and Replacement. Elsevier.
Peumans, M., Kanumilli, P., De munck, J., Van landuyt, K., Lambrechts, P., Van meerbeek,
B., 2005. Clinical effectiveness of contemporary adhesives: a systematic review of current clinical trials. Dent. Mater. 21, 864 881.
Prado, M., Gusman, H., Gomes, B.P., Simão, R.A., 2011. Scanning electron microscopic
investigation of the effectiveness of phosphoric acid in smear layer removal when compared with EDTA and citric acid. J. Endod. 37, 255 258.
Raghupathi, K.R., Koodali, R.T., Manna, A.C., 2011. Size-dependent bacterial growth inhibition and mechanism of antibacterial activity of zinc oxide nanoparticles. Langmuir 27,
4020 4028.
Saeki, K., Marshall, S., Gansky, S., Marshall, G., 2001. Etching characteristics of dentin:
effect of ferric chloride in citric acid. J. Oral Rehabil. 28, 301 308.
Sarwar, S., Ali, A., Pal, M., Chakrabarti, P., 2017. Zinc oxide nanoparticles provide anticholera activity by disrupting the interaction of cholera toxin with the human GM1
receptor. J. Biol. Chem. 292, 18303 18311.
Sauro, S., Osorio, R., Watson, T.F., Toledano, M., 2012. Therapeutic effects of novel resin
bonding systems containing bioactive glasses on mineral-depleted areas within the
bonded-dentine interface. J. Mater. Sci. Mater. Med. 23, 1521 1532.
Say, E.C., Nakajima, M., Senawongse, P., Soyman, M., Ozer, F., Tagami, J., 2005. Bonding
to sound vs caries-affected dentin using photo- and dual-cure adhesives. Oper. Dent. 30,
90 98.
252
Advanced Dental Biomaterials
Sfalcin, R.A., Correr, A.B., Morbidelli, L.R., Araujo, T.G.F., Feitosa, V.P., Correr-Sobrinho,
L., et al., 2017. Influence of bioactive particles on the chemical-mechanical properties
of experimental enamel resin infiltrants. Clin. Oral Investig. 21, 2143 2151.
Silverstone, L.M., 1974. Fissure sealants. Caries Res. 8, 2 26.
Smutka, S., Jedrychowski, J., Caputo, A., 1978. An evaluation of primary enamel pretreatments and their effects on resin retention. J. Dent. Res. 57, 796 799.
Sofan, E., Sofan, A., Palaia, G., Tenore, G., Romeo, U., Migliau, G., 2017a. Classification
review of dental adhesive systems: from the IV generation to the universal type. Ann.
Stomatol. (Roma) 8, 1.
Sofan, E., Sofan, A., Palaia, G., Tenore, G., Romeo, U., Migliau, G., 2017b. Classification
review of dental adhesive systems: from the IV generation to the universal type. Ann.
Stomatol. (Roma) 8, 1 17.
Su, M., Yao, S., Gu, L., Huang, Z., Mai, S., 2018. Antibacterial effect and bond strength of a
modified dental adhesive containing the peptide nisin. Peptides 99, 189 194.
Swift, E.J., Perdigao, J., Heymann, H.O., 1995. Bonding to enamel and dentin: a brief history
and state of the art, 1995. Quintessence Int. 26, 95 110.
Tao, L., Pashley, D.H., Boyd, L., 1988. Effect of different types of smear layers on dentin
and enamel shear bond strengths. Dent. Mater. 4, 208 216.
Taubock, T.T., Zehnder, M., Schweizer, T., Stark, W.J., Attin, T., Mohn, D., 2014.
Functionalizing a dentin bonding resin to become bioactive. Dent. Mater. 30, 868 875.
Tay, F.R., Pashley, D.H., 2009. Biomimetic remineralization of resin-bonded acid-etched
dentin. J. Dent. Res. 88, 719 724.
Tezvergil-Mutluay, A., Agee, K.A., Uchiyama, T., Imazato, S., Mutluay, M.M., Cadenaro,
M., et al., 2011. The inhibitory effects of quaternary ammonium methacrylates on soluble and matrix-bound MMPs. J. Dent. Res. 90, 535 540.
Tezvergil-Mutluay, A., Agee, K.A., Mazzoni, A., Carvalho, R.M., Carrilho, M., Tersariol, I.
L., et al., 2015. Can quaternary ammonium methacrylates inhibit matrix MMPs and
cathepsins? Dent. Mater. 31, e25 e32.
Tezvergil-Mutluay, A., Seseogullari-Dirihan, R., Feitosa, V.P., Cama, G., Brauer, D.S.,
Sauro, S., 2017. Effects of composites containing bioactive glasses on demineralized
dentin. J. Dent. Res. 96, 999 1005.
Thanatvarakorn, O., Nakajima, M., Prasansuttiporn, T., Ichinose, S., Foxton, R.M., Tagami,
J., 2014. Effect of smear layer deproteinizing on resin-dentine interface with self-etch
adhesive. J. Dent. 42, 298 304.
Toledano, M., Yamauti, M., Ruiz-Requena, M.E., Osorio, R., 2012. A ZnO-doped adhesive
reduced collagen degradation favouring dentine remineralization. J. Dent. 40, 756 765.
Tseng, W.Y., Chen, M.H., Lu, H.H., Lin, C.W., Hsieh, T.T., Chen, C.H., et al., 2007. Tensile
bond strength of Er, Cr:YSGG laser-irradiated human dentin to composite inlays with
two resin cements. Dent. Mater. J. 26, 746 755.
Uysal, T., Amasyali, M., Koyuturk, A.E., Ozcan, S., Sagdic, D., 2010. Amorphous calcium
phosphate-containing orthodontic composites. Do they prevent demineralisation around
orthodontic brackets?. Aust. Orthod. J. 26, 10 15.
Van Meerbeek, B., Lambrechts, P., Inokoshi, S., Braem, M., Vanherle, G., 1992. Factors
affecting adhesion to mineralized tissues. Oper. Dent. (Suppl. 5), 111 124.
Van Meerbeek, B., De munck, J., Yoshida, Y., Inoue, S., Vargas, M., Vijay, P., et al., 2003a.
Adhesion to enamel and dentin: current status and future challenges. Oper. Dent. 28,
215 235.
Van Meerbeek, B., De munck, J., Yoshida, Y., Inoue, S., Vargas, M., Vijay, P., et al., 2003b.
Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future
challenges. Oper. Dent. 28, 215 235.
Enamel etching and dental adhesives
253
Vinagre, A., Ramos, J., 2016. Adhesion in restorative dentistry. Adhesives-Applications and
Properties. InTech.
Wang, L., Xie, X., Weir, M.D., Fouad, A.F., Zhao, L., Xu, H.H., 2016. Effect of bioactive
dental adhesive on periodontal and endodontic pathogens. J. Mater. Sci. Mater. Med. 27,
168.
Wei, S., Sadr, A., Shimada, Y., Tagami, J., 2008. Effect of caries-affected dentin hardness on
the shear bond strength of current adhesives. J. Adhes. Dent. 10, 431 440.
Weir, M.D., Chow, L.C., Xu, H.H.K., 2012. Remineralization of demineralized enamel via
calcium phosphate nanocomposite. J. Dent. Res. 91, 979 984.
Wiegand, A., Buchalla, W., Attin, T., 2007. Review on fluoride-releasing restorative materials—fluoride release and uptake characteristics, antibacterial activity and influence on
caries formation. Dent. Mater. 23, 343 362.
Wu, Y.Z., Sun, J., Yang, H., Zhao, X., He, D., Pu, M., et al., 2018. Biosynthetic mechanism
of luminescent ZnO nanocrystals in the mammalian blood circulation and their functionalization for tumor therapy. ACS Appl. Mater. Interfaces 10, 105 113.
Xie, D., Zhao, J., Weng, Y., Park, J.G., Jiang, H., Platt, J.A., 2008. Bioactive glass-ionomer
cement with potential therapeutic function to dentin capping mineralization. Eur. J. Oral
Sci. 116, 479 487.
Xie, X., Wang, L., Xing, D., Zhang, K., Weir, M.D., Liu, H., et al., 2017. Novel dental adhesive with triple benefits of calcium phosphate recharge, protein-repellent and antibacterial functions. Dent. Mater. 33, 553 563.
Yamaguchi, M., Yoshida, K., Suzuki, R., Nakamura, H., 1996. Root canal irrigation with
citric acid solution. J. Endod. 22, 27 29.
Yang, S.Y., Piao, Y.Z., Kim, S.M., Lee, Y.K., Kim, K.N., Kim, K.M., 2013. Acid neutralizing, mechanical and physical properties of pit and fissure sealants containing meltderived 45S5 bioactive glass. Dent. Mater. 29, 1228 1235.
Yang, S.-Y., Kim, S.-H., Choi, S.-Y., Kim, K.-M., 2016. Acid neutralizing ability and shear
bond strength using orthodontic adhesives containing three different types of bioactive
glass. Materials 9, 125.
Yokota, Y., Fujita, K.N., Uchida, R., Aida, E., Aoki, N.T., Aida, M., et al., 2016.
Quantitative evaluation of MDP-Ca salt and DCPD after application of an MDP-based
one-step self-etching adhesive on enamel and dentin. J. Adhes. Dent. 18, 205 213.
Yoshihara, K., Nagaoka, N., Maruo, Y., Sano, H., Yoshida, Y., Van meerbeek, B., 2017.
Bacterial adhesion not inhibited by ion-releasing bioactive glass filler. Dent. Mater. 33,
723 734.
Zehnder, M., Soderling, E., Salonen, J., Waltimo, T., 2004. Preliminary evaluation of bioactive glass S53P4 as an endodontic medication in vitro. J. Endod. 30, 220 224.
Zhang, K., Li, F., Imazato, S., Cheng, L., Liu, H., Arola, D.D., et al., 2013. Dual antibacterial
agents of nano-silver and 12-methacryloyloxydodecylpyridinium bromide in dental
adhesive to inhibit caries. J. Biomed. Mater. Res. B Appl. Biomater. 101, 929 938.
Zhang, L., Weir, M.D., Hack, G., Fouad, A.F., Xu, H.H.K., 2015a. Rechargeable dental adhesive with calcium phosphate nanoparticles for long-term ion release. J. Dent. 43,
1587 1595.
Zhang, N., Melo, M.A., Chen, C., Liu, J., Weir, M.D., Bai, Y., et al., 2015b. Development of
a multifunctional adhesive system for prevention of root caries and secondary caries.
Dent. Mater. 31, 1119 1131.
Endodontic materials: from old
materials to recent advances
12
Mai Saleh Ali1,2 and Bassel Kano3
1
Faculty of Dentistry, University of Toronto, Toronto, ON, Canada, 2Private Practice,
Amman, Jordan, 3Division of Endodontics, Faculty of Dentistry, McGill University,
Montreal, QC, Canada
Chapter Outline
12.1 Introduction 256
12.2 Materials used in vital pulp therapy
12.2.1
12.2.2
12.2.3
12.2.4
12.2.5
12.3 Materials used as root canal irrigants
12.3.1
12.3.2
12.3.3
12.3.4
12.3.5
12.3.6
12.3.7
12.3.8
12.3.9
12.3.10
Sodium hypochlorite 263
Ethylenediamine tetra-acetic acid 265
Chlorhexidine 266
Citric acid 267
MTAD 267
Tetraclean 269
Hydrogen peroxide 269
Iodine potassium iodide 269
1-Hydroxyethylidene-1,1-bisphosphonate
QMiX 270
12.4 Intracanal medicaments
12.4.1
12.4.2
12.4.3
12.4.4
12.4.5
256
Mineral trioxide aggregates 257
Biodentine (Septodont, Saint-Maur-des-Fosses, France) 262
Bioaggregate (Innovative Bioceramix, Vancouver, BC, Canada) 262
Mineral Trioxide Aggregate Angelus (Londrina, PR, Brazil) 262
Endosequence (Brasseler USA, Savanah, Georgia, United States) 262
263
269
271
Calcium hydroxide 271
Chlorhexidine 272
Ledermix 273
Triple antibiotics pastes 273
Bioactive glass 274
12.5 Root canal obturation materials
274
12.5.1 Core obturation materials 274
12.5.2 Root canal sealers (cementing medium) 277
12.6 Root-end filling materials
12.6.1
12.6.2
12.6.3
12.6.4
12.6.5
290
Amalgam 290
Zinc oxide eugenol cements 290
Composite resins (Retroplast) 290
Glass ionomer cements 292
Diaket (3M/ESPE, Seefeld, Germany) 292
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00012-8
Copyright © 2019 Elsevier Ltd. All rights reserved.
256
Advanced Dental Biomaterials
12.6.6 Resin ionomer suspension and compomer 292
12.6.7 Other types of cement 292
12.7 Perforation repair materials
12.8 Summary 293
References 293
Further reading 299
12.1
292
Introduction
The aim of endodontics is the diagnosis, prevention, and treatment of diseases and
injuries of the dental pulp along with the associated periradicular structures. Vital
pulp therapy, nonsurgical treatment of the root canal system, periradicular surgery
for persistent infections, and repair of iatrogenic perforations are a few of the endodontic procedures that require the use of materials to reach a favorable result.
Fortunately, the field of endodontics has greatly benefited from the recent advances
and technologies in material sciences and equipment, thus providing the clinician
with options that can facilitate treatment with high success rates. This chapter will
cover materials used in vital pulp therapy, irrigants, intracanal medicaments, obturation materials, root-end fillings, and repair materials.
12.2
Materials used in vital pulp therapy
In the cases of teeth with reversible pulpitis or partially inflamed pulps caused by
chemical, mechanical, or traumatic injury, where the healthy remaining pulpal tissue can be conserved, vital pulp therapy is recommended to generate a hard tissue
barrier to preserve, seal, and protect the pulp from microbial insult (Fig. 12.1). This
can prolong tooth survival and delay or avoid root canal treatment. Indirect pulp
capping, direct pulp capping, and pulpotomy are all different vital pulp therapy procedures. Caries extension and pulp exposure are factors affecting the decision of
which procedure is to be approached. Properties of an ideal material for vital pulp
therapy are summarized in Box 12.1; nevertheless, none of those available satisfy
them all (Qureshi et al., 2014).
Table 12.1 summarizes some of the materials that have been used for vital pulp
therapy through the years. However, recently bioceramic materials, such as calcium
silicate materials, calcium aluminate cements, and calcium phosphate cements, are
among the most widely studied materials due to their bioactivity (Jitaru et al.,
2016), regenerative abilities, and their promising results not only as materials for
vital pulp therapy, but also as root repair materials and as root-end fillings. Among
the increasing number of bioceramic materials, calcium silicate cements are the
most studied. Therefore the following section will focus on a few materials that
belong to this family of cements.
Endodontic materials: from old materials to recent advances
257
Figure 12.1 Vital pulp therapy: (A) indirect pulp capping can be defined as “a procedure
performed in a tooth with a deep carious lesion approximating the pulp but without signs or
symptoms of pulp degeneration” and “indicated in a permanent tooth diagnosed with no
signs or symptoms of pulpitis or with a diagnosis of reversible pulpitis”; (B) direct pulp
capping is defined by the American Association of Endodontists (2012) as “placing a
material directly on a mechanical or traumatic vital pulp exposure to induce reparative dentin
formation”; and (C) pulpotomy, defined by the AAE as “the removal of the coronal portion
of the vital pulp as a means of preserving the vitality of the remaining radicular portion.”
AAE, American Association of Endodontists.
Box 12.1 Properties of an ideal vital pulp therapy material
G
G
G
G
G
G
G
G
G
G
G
G
G
G
Stimulates reparative dentin formation
Maintains pulpal vitality
Releases fluoride to prevent secondary caries
Bactericidal or bacteriostatic
Adheres to dentin
Adheres to restorative material
Resists forces during restoration placement and during the life of restoration
Sterile
Radiopaque
Provides a seal against bacteria and the oral environment
Insoluble in biological fluids
Dimensionally stable
Nonresorbable, nontoxic, noncarcinogenic, nongenotoxic
Biocompatible and bioactive
12.2.1 Mineral trioxide aggregates
Mineral trioxide aggregate (MTA) was introduced in the mid-1990s by Dr.
Mahmoud Torabinejad and associates as a promising pulp capping material (Ford
et al., 1996). ProRoot MTA Gray (Dentsply Tulsa Dental Specialties, Johnson City,
Tennessee, United States) was the first material to be marketed and it is composed
of 75% Type I Portland cement, 20% bismuth oxide, and 5% calcium sulfate
Table 12.1 Some of the materials used for vital pulp therapy.
Material
Description
Polycarboxylate cement
Corticosteroids and
antibiotics
It is not used anymore due to its lack of calcific bridge formation and antibacterial effect (McWalter et al., 1976)
The rationale is that those materials will reduce pulpal inflammation. However, there is lack of research to their viability as a
vital pulp therapy material
CH: Dycal (Dentsply,
United States), Life
(Kerr, United States)
It has been considered as the
universal standard for vital pulp
therapy materials; however, its
drawbacks can no longer make it
the preferred one
RMGI
G
G
Adhesive systems
Clearfil SE Bond
(Kuraray Medical,
Japan)
Optibond S (Kerr,
United States)
Prime & Bond 2.1
(Dentsply, United
States)
Composition
G
G
G
G
Base paste: titanium dioxide, calcium
tungstate 1,3-butylene glycol
disalicylate
Catalyst paste: CH, zinc oxide, zinc
stearate, ethyl toluene sulfonamide
1. Reparative hard tissue bridge
formation subjacent to CH has tunnel
defects (Andelin et al., 2003)
2. It has been shown CH can induce
pulp cell apoptosis
3. Dimensionally unstable with weak
marginal adaptation to dentin
4. CH degrades and dissolutes with time
allowing microleakage and further
pulpal injury
5. CH can cause primary tooth
resorption
If used as a direct pulp capping material,
there is lack of dentin bridge
formation and the pulp exhibits
chronic inflammation (Tarim et al.,
1998)
Primer: MDP, dimethacrylate
monomer, HEMA, silica, N,Ndiethanol-p-toluidine,
camphorquinone
Bond: HEMA, dimethacrylate
monomer, bis-GMA, N,N-diethanolp-toluidine silica, camphorquinone
Cytotoxic to pulp cells
(Silva et al., 2013)
Best used as an indirect pulp
capping material with no direct
contact with the pulp
Conventional glass ionomer is less
toxic than the resin-modified
formulations
G
G
G
Disadvantages
(Continued)
Table 12.1 (Continued)
Material
Zinc oxide eugenol
IRM (Dentsply,
United States)
Temp Bond (Kerr,
United States)
Relix Tempo (3M
ESPE, United States)
Formocresol
Buckley’s
Formocresol (Sultan
Healthcare,
United States)
Description
Composition
G
G
G
Powder: zinc oxide, PMMA pigment
Liquid: eugenol, acetic acid
G
G
G
G
G
Ferric sulfate: ViscoStat
(Ultradent, United
States),
Astringedent
(Ultradent, United
States)
Collagen
Hydroxyapatite
G
G
G
GF
BMP which belongs
to super family TGF-β
Recombinant insulin
like GF-I
G
G
G
It is mostly used in pulpotomies in
primary teeth
It is applied on the radicular
stump for 1 5 min
Formaldehyde, ortho-cresol, glycerin,
ethyl alcohol
It is mostly used in pulpotomies in
primary teeth as an alternative to
formocresol
It is applied on the radicular stump
for 10 15 s (Loh et al., 2004)
Ferric sulfate, silica, aqueous vehicle
There is lack of research regarding
hydroxyapatite but a study showed.
It can be used as scaffolding for
the newly formed mineralized
tissue (Hayashi et al., 1999)
Disadvantages
1. Direct contact with pulp tissue causes
chronic
inflammation and ultimately necrosis
2. It lacks the formation of a calcific
barrier
(Glass and Zander, 1949)
G
G
It is a caustic material and causes
severe burns in contact
The use of formaldehyde is
controversial due to its toxicity and
corrosiveness (Lewis and Chestner,
1981)
It does not form a thick dentin bridge
(Dick and Carmichael, 1980)
More research is needed
More research is needed (Lianjia et al.,
1993; Lovschall et al., 2001)
(Continued)
Table 12.1 (Continued)
Material
Description
Propolis (Russian
penicillin)
EMD
It is an enamel matrix derivative.
It has an important role during
periodontal tissue formation and
stimulates PDL regeneration
It comes as an injectable gel
solution (Al-Hezaimi et al., 2011;
Kaida et al., 2008)
COB cement is a natural polyol
containing three hydroxyl radicals
Used for vital pulp therapy, root and
perforation repair, and as a rootend filling. Introduced by Asgary
et al. (2006)
G
G
COB cement
Calcium phosphate
cement
CEM cement
(BioniqueDent, Iran)
G
Composition
Disadvantages
Contains flavonoids, phenolics, iron,
zinc, and other various aromatic
compounds (Parolia et al., 2010)
It consists of enamel matrix proteins
(amelogenin), water and a carrier
(propylene glycol alginate). It also
contains BMP-like molecules and
BMP-expressing cells
More research is needed
81% 96% Triglyceride of ricinoleic
acid
Powder: calcium compounds such as
calcium oxide, calcium phosphate,
calcium carbonate, calcium silicate,
calcium sulfate, CH, calcium chloride
Liquid: distilled water
Powder: aluminum oxide, calcium
oxide, silicon dioxide, magnesium
oxide, iron oxide, bismuth oxide
Liquid: distilled water
More research is needed (Camargo et al.,
2009)
More research is needed (Ambard and
Mueninghoff, 2006; Asgary et al.,
2015)
G
Some clinical trials failed to prove that
EMD improves tertiary dentin
formation when used as direct pulp
capping material in primary teeth and
pulpotomy in permanent teeth
(Kiatwateeratana et al., 2009)
G
Calcium aluminate
cement
EndoBinder
(Binderware, Brazil)
Capasio (Primus
Consulting,
Bradenton, FL)
Quick-Set (Primus
Consulting,
Bradenton, FL)
G
Used for vital pulp therapy, root and
perforation repair, and as a rootend filling
G
More research is needed
G
G
Bis-GMA, Bisphenol A glycidyl methacrylate; BMP, bone morphogenetic protein; CEM, calcium enriched mixture; CH, calcium hydroxide; COB, castor oil bean; EMD, Emdogain; GF, growth factors;
HEMA, hydroxyethyl methacrylate; IRM, intermediate restorative material; MDP, 10-methacryloyloxydecyl dihydrogen phosphate; PDL, periodontal ligament; PMMA, polymethyl methacrylate; RMGI,
resin-modified glass ionomer cements; TGF-β, transforming growth factor beta.
Endodontic materials: from old materials to recent advances
261
dehydrate (gypsum). Portland cement is composed of tricalcium silicate, dicalcium
silicate, tricalcium aluminate tetracalcium aluminoferrite, magnesium oxide, calcium sulfate, and calcium oxide. Bismuth oxide is added as a radiopacifier, while
calcium sulfate acts as a setting modifier (Camilleri et al., 2005). In 2002 white
MTA was introduced to prevent the tooth discoloration caused by gray MTA, by
reducing the amount of iron and magnesium. Moreover, white MTA has smaller,
finer, and more homogenous powder particles and thus allows easier handling properties than gray MTA (Parirokh and Torabinejad, 2010a).
One of the positive characteristics of MTA is that it is a hydraulic material
which means it sets in the presence of moisture (i.e., moisture affects its setting
favorably). Nevertheless, excessive moisture may cause a detrimental effect
(Fridland and Rosado, 2003). The reaction of MTA and water is considered as an
exothermic hydration reaction. The main ingredients that are hydrated during this
reaction are tricalcium silicate and dicalcium silicate which forms calcium silicate
hydrates and calcium hydroxide. Both reaction products play a role in the bioactivity of MTA. The calcium silicate hydrates form a colloidal gel that solidifies into a
hard structure with calcium hydroxide nucleated in an amorphous matrix (Parirokh
and Torabinejad, 2010a). MTA has a working time of 5 minutes and sets over a
period of 4 hours.
When used as a capping material, it is recommended to place a rigid restorative
material such as adhesive fillings over MTA in the subsequent clinical appointment
after a few days. This restorative material will provide adequate strength to withstand occlusal forces and allow MTA to complete its hydration reaction and gain
adequate strength. Table 12.2 lists the advantages and disadvantages of MTA.
Table 12.2 Advantages and disadvantages of mineral trioxide aggregates (MTA).
Advantages
Disadvantages
1. Its ability to stimulate reparative
dentinogenesis and hard tissue formation
by inducing the release of dentin matrix
components that are essential for hard
tissue repair (Yasuda et al., 2008)
2. MTA has a superior marginal adaptation
to dentin since it forms an interfacial layer
at the surface of dentin that is similar to
hydroxyapatite (Min et al., 2008)
3. Excellent biocompatibility (Yavari et al.,
2009)
4. Excellent sealing ability (Estrela et al.,
2011)
5. Antibacterial due to its high pH
(Torabinejad et al., 1995)
6. Radiopaque (Borges et al., 2011)
1. Discoloration of tooth structure
especially with gray MTA
2. Expensive
3. Difficult handling characteristics
4. Prolonged setting time (Parirokh and
Torabinejad, 2010b; Kratchman,
2004; Camilleri et al., 2005)
MTA, Mineral trioxide aggregate.
262
Advanced Dental Biomaterials
12.2.2 Biodentine (Septodont, Saint-Maur-des-Fosses, France)
Biodentine was manufactured as a “dentin replacement” material. It is a powder/
liquid material mixed by trituration. It consists of tricalcium silicate, dicalcium silicate, calcium carbonate, iron oxide, and zirconium oxide (radiopacifier), whereas the
liquid contains calcium chloride as an accelerator and a hydrosoluble polymer that
serves as a water reducing agent. Like other calcium silicate materials, it has a hydration setting reaction with calcium hydroxide as one of the reaction products, it is bioactive with alkaline pH, biocompatible and has excellent sealability (Grech et al.,
2013). Unlike MTA, biodentine is characterized by a short setting time (9 12 minutes) and color stability (Keskin et al., 2015).
12.2.3 Bioaggregate (Innovative Bioceramix, Vancouver, BC,
Canada)
Bioaggregate, also known as DiaRoot, consists of tricalcium silicate, dicalcium silicate, calcium phosphate monobasic, amorphous silicon dioxide, and tantalum pentoxide (as a radiopacifier) (Camilleri et al., 2015). Bioaggregate has a fine
nanoparticle aluminum-free powder that is mixed with deionized water. It is bioinductive, highly biocompatible, and antibacterial. Compared to MTA, bioaggregate
demonstrates higher fracture resistance and a greater resistance to dislodgement in
an acidic environment (Hashem and Wanees Amin, 2012).
12.2.4 Mineral Trioxide Aggregate Angelus (Londrina, PR, Brazil)
It is composed of 80% Portland cement and 20% bismuth oxide (Duarte et al.,
2003). It has a lower radiopacity compared to gray MTA and its lack of calcium
sulfate provides a short setting time (10 minutes).
12.2.5 Endosequence (Brasseler USA, Savanah, Georgia, United
States)
Endosequence comes in two forms: the first is endosequence root repair material
(ERRM) in a preloaded paste consistency in a syringe, and the second is endosequence root repair putty (ERRP)—a premixed moldable putty (Lovato and Sedgley,
2011). Like other bioceramics and calcium silicates, it is bioactive, biocompatible
with antibacterial activity, and it can be used as a pulp capping material in addition
to root repair. Both ERRM and ERRP are bioceramic materials that come as bright
white nanosphere particles that are composed of a combination of calcium silicate,
calcium phosphate monobasic, zirconium oxide, tantalum oxide, filler, and thickening agents. They are also premixed and ready to use.
There are several calcium silicate and bioceramic materials that are regularly
being introduced to the market—to name a few, Ortho MTA (BioMTA, Seoul,
Korea), MTA Bio (Angelus, Londrina, PR, Brazil), Fluoride-Doped MTA
Cement, Cimento Endodontico Rapido, Endocem, Ceramicrete-D (Tulsa Dental
Endodontic materials: from old materials to recent advances
263
Specialties/Argonne National Laboratory, Argonne, Illinois, United States),
Generex A (Dentsply Tulsa Dental Specialties, Tulsa, Oklahoma, United States),
Tech Biosealer capping (Isasan Srl, Rovello Porro, Co, Italy), TheraCal (Bisco
Inc, Schaumburg, Illinois, United States), and many others. All the abovementioned materials demonstrate promising bioactive potential and possess somewhat
similar properties with various modifications to their composition in hopes of
overcoming the shortcomings of MTA.
12.3
Materials used as root canal irrigants
The next step after a straight-line access cavity is the removal of pulpal tissue,
microbes, and dentine shavings from the canal. This is achieved via mechanical
preparation and chemical irrigation. Root canal irrigation plays an important role in
the disinfection of the root canal system and is critical for the treatment’s success.
According to Zehnder (2006), an ideal irrigant should possess all the properties
mentioned in Box 12.2, yet none of the available ones combine all those characteristics. Accordingly, clinicians often use the irrigant that has many of the most
important properties or a combination of different irrigants that complement each
other’s action. Table 12.3 summarizes the properties and effects of different irrigants used during root canal treatment.
12.3.1 Sodium hypochlorite
Sodium hypochlorite (NaOCl) is the most commonly used irrigant worldwide since
it satisfies most of the properties stated in Box 12.2 (Mohammadi, 2008). It is an
alkaline, hypertonic solution with a pH . 11. In water, NaOCl ionizes to produce
Box 12.2 Ideal properties of a root canal irrigant
G
G
G
G
G
G
G
G
G
G
G
G
Broad antimicrobial spectrum
High efficacy against anaerobic and facultative microorganisms organized in
biofilms
Able to dissolve necrotic pulp tissue remnants
Able to inactivate endotoxins
Able to prevent the formation of a smear layer during instrumentation or to dissolve
it once formed
Systemically, nontoxic, nonantigenic, and noncarcinogenic if it comes in contact
with vital tissues
Noncaustic to periodontal tissues
Little potential to cause an anaphylactic reaction
Has low surface tension
Does not stain tooth structures
Has no adverse effects on the sealing ability of filling material
Relatively inexpensive
Table 12.3 Summary of the properties and effects of different irrigants.
Irrigant
Antibacterial effect
Dissolution of tissues
Smear layer removal
Concentration
(%)
NaOCl
Effective antibacterial agent by
breaking down proteins into amino
acids
Dissolves necrotic tissue at
low concentration
At high concentration, it
dissolves both vital and
necrotic tissues
No dissolution capacity
Removes the organic part of
smear layer (Goldman
et al., 1976)
0.5 6.25
Removes the inorganic part of
smear layer
No smear layer removal
17
EDTA
Limited antibacterial effect
CHX
Effective antibacterial agent against
Gram negative, Gram, Gram
positive, and yeasts
Antibacterial effect due to
doxycycline
No antibacterial effect
Antibacterial effect
Antibacterial effect
Very minimal antibacterial effect
Antibacterial effect
MTAD
Citric acid
H2O2
IKI
HEBP
QMiX
G
G
No dissolution capacity
No dissolution capacity
No dissolution capacity
No dissolution capacity
No dissolution capacity
No dissolution capacity
No dissolution capacity
Removes smear layer through
doxycycline and citric acid
Removes smear layer
None
None
Weak decalcifying property
Removes smear layer
2
10 50
3 5
2 5
CHX, Chlorhexidine; EDTA, ethylenediamine tetra-acetic acid; HEBP, 1-hydroxyethylidene-1,1-bisphosphonate; IKI, iodine potassium iodide; MTAD, a mixture of doxycycline, citric
acid, and a detergent; NaOCl, sodium hypochlorite.
Endodontic materials: from old materials to recent advances
265
sodium ion (Na1) and hypochlorite ion (OCl2) which establishes equilibrium with
hypochlorous acid HOCL according to the following equation:
NaOCl1H2 O2NaOH 1 HOCl2Na1 1OH2 1H 1 1OCl2
Once NaOCl comes in contact with tissue protein, nitrogen, formaldehyde, and
acetaldehyde are formed. This protein disintegration enables the replacement of
hydrogen in the amino groups ( NH ) by chlorine, and thus forming chloramines
( NCl ). Chloramination contributes to the antimicrobial properties effect of
NaOCl and makes this irrigant distinguished by its ability to dissolve both vital and
necrotic pulp tissues. However, NaOCl is more efficient at dissolving necrotic tissue.
Moreover, breaking down proteins into amino acids is essential in dissolving the
organic part of the smear layer and biofilms, which, in turn, allows the irrigant to
reach inaccessible areas in the root canal system. In addition to chloramination,
NaOCl degrades fatty acids which transform into fatty acid salts (soap) and glycerol
(alcohol). This saponification reaction reduces the surface tension of the solution
allowing better penetration of dentinal tubules (Estrela et al., 2002). NaOCl also acts
as a lubricant and flushes away all the debris packed inside the canal. Probably, two
of its most important characteristics are that it is readily available and inexpensive.
On the other hand, NaOCl also has some disadvantages. Prolonged irrigation
using NaOCl affects the flexural strength of dentin (Grigoratos et al., 2001).
Moreover, NaOCl accident is one of the complications that may encounter the clinician. To avoid this complication, it is recommended to use specially designed irrigation needles which should be inserted loosely instead of being wedged inside the
root canal (Bettina and Markus, 2012). Allergic reactions to NaOCl are rare, but if
present then the irrigant of choice is iodine potassium iodide (IKI) assuming the
patient does not have an allergy to it as well.
NaOCl is available in different concentrations varying from 0.5% to 6.25%. With
lower concentrations, it can dissolve necrotic tissues only, while in higher concentrations, it dissolves both vital and necrotic tissue but it is more toxic (Hand et al.,
1978; Spangberg et al., 1973). To avoid the negative impact of NaOCl toxicity, we
can increase the effectiveness of a low concentration through different ways:
G
G
G
G
Increase the volume of low-concentration NaOCl (Siqueira et al., 2000).
Increase the temperature of low-concentration NaOCl (Zehnder, 2006). However, the efficacy of this method remains questionable since there are no clinical studies showing that
heating NaOCl is effective (Bettina and Markus, 2012).
Ultrasonic activation of NaOCl to create cavitational effects, preferably after the canal
preparation (Macedo et al., 2014).
Adding a detergent to the NaOCl solution to decrease surface tension which will enhance
the penetration of NaOCl into the dentinal tubules and hence have a broader effect on
eliminating bacteria (Stojicic et al., 2010).
12.3.2 Ethylenediamine tetra-acetic acid
Ethylenediamine tetra-acetic acid (EDTA) is a polyaminocarboxylic acid
(Fig. 12.2), colorless, and water soluble. EDTA activity lasts for extended periods
266
Advanced Dental Biomaterials
Figure 12.2 Chemical structure of polyaminocarboxylic acid.
Figure 12.3 Chemical structure of polybiquanide family.
of time after direct exposure by extracting bacterial surface proteins and combining
with metal ions present in the bacterial cell envelope which can eventually lead to
cell death (Hulsmann et al., 2003). It also sequesters di- and tri-cationic metal ions
such as Ca21 and Fe31.
Furthermore, EDTA is a well-known chelator that reacts with the calcium ions
in dentine and forms soluble calcium chelates. One of its major uses is to open
occluded, very fine canals since it is capable of decalcifying dentin to a depth of
20 30 μm in 5 minutes. EDTA is commonly used in a concentration of 17%, which
demonstrates limited antiseptic activity. However, since it removes the inorganic
part of smear layers and biofilms within less than 1 minute after being in contact
with root canal wall, it is often used synergistically with NaOCl (Goldman et al.,
1976). Even though EDTA has a self-limited action (Hulsmann et al., 2003), it
should be used with care following the manufacturer’s instructions as it can erode
dentin if used for long periods of time.
EDTA retains its ability to form calcium complexes when mixed with NaOCl.
On the other hand, EDTA diminishes the tissue-dissolving capacity of NaOCl
(Grawehr et al., 2003). Therefore it is suggested to use EDTA and NaOCl separately and copious amounts of NaOCl should be administered to wash out remnants
of the EDTA. Overall, EDTA is preferably used at the end of a procedure to
remove the smear layer.
12.3.3 Chlorhexidine
Chlorhexidine (CHX) is a broad-spectrum antimicrobial agent and has been widely
used as a disinfectant for a long time. It belongs to the polybiguanide antibacterial
family, consisting of two symmetric four chlorophenyl rings and two biguanide
groups connected by a central hexamethylene chain (Fig. 12.3). CHX is a positively
charged hydrophobic and lipophilic molecule that interacts with phospholipids and
lipopolysaccharides (LPS) on the negatively charged bacterial cell membrane and
Endodontic materials: from old materials to recent advances
267
penetrates the cell through a certain type of active or passive transport mechanism
(Davies, 1973). This process will disrupt the microorganism’s permeability altering
its equilibrium and making CHX antimicrobial.
Unlike NaOCl, CHX overcomes some of the drawbacks of NaOCl including the
bad odor, periapical reactions when extruded beyond the root apex, and bleaching
spots on patient’s clothes. However, CHX does not possess the tissue-dissolving
capacity of NaOCl. Hence, although NaOCl and CHX have comparable antibacterial effects, NaOCl dissolving capacity renders it more superior.
CHX is effective against both Gram-positive and Gram-negative bacteria as well
as yeasts (Block, 2001), although its activity against Gram-negative bacteria is not
as strong as against Gram-positive bacteria. CHX is available as gel, liquid, or
controlled-release devices. Some studies reported that CHX gel is more efficient
than liquid. Nevertheless, the mode of application is not considered an important
factor in the effectiveness of CHX; its concentration is the pivotal one (Basrani
et al., 2003) and 2% CHX has better antibacterial efficacy than 0.12%. High concentrations are bactericidal since it damages the cell membrane which causes precipitation of the cytoplasm. While low concentrations are bacteriostatic, low
molecular weight substances such as potassium and phosphorus will leak out without the cell being irreversibly damaged (Basrani and Lemonie, 2005).
Substantivity is considered a unique characteristic for CHX (Basrani et al.,
2002). Due to its cationic nature, it can be absorbed by anionic substrates present in
the oral cavity, such as the apatite molecules present in teeth. Substantivity prolongs
the antimicrobial effect of CHX, which contributes to delaying the coronal recontamination. Furthermore, CHX improves the resin dentin bond stability due to its
broad-spectrum matrix metalloproteinase inhibitory effect (Carrilho et al., 2007).
When CHX and NaOCl interact, they form para-chloroaniline (PCA) which is a
neutral toxic insoluble precipitate that may interfere with the seal of obturation,
causing color change (brownish-reddish) and cyanosis due to methemoglobin formation (Basrani et al., 2007). Table 12.4 presents some possible interactions
between the different irrigants.
12.3.4 Citric acid
Citric acid is an organic acid and a chelator used in concentrations between 10%
and 50%. It is more potent as a chelator than EDTA at similar concentrations and is
highly efficient in removing the smear layer and detaching bacterial biofilms
(Smith and Wayman, 1986). Although EDTA is a weak antibacterial agent, it is
stronger than citric acid in inhibiting bacterial growth (Siqueira et al., 1998).
12.3.5 MTAD
MTAD is a mixture of 3% doxycycline hyclate, 4.25% citric acid, and 0.5%
polysorbate-80 detergent (Tween 80) (Table 12.5). It is mixed as a liquid and powder and recommended as a final rinse for 5 minutes. MTAD is the first product that
can both remove the smear layer and disinfect the root canal system. The whole
Table 12.4 Summary of the possible interactions between different irrigants.
Interactions
NaOCl
EDTA
NaOCl
G
G
EDTA
NaOCl loses its
tissue-dissolving
capacity, with
virtually no free
chlorine detected
in combinations
A bubbling effect
reflects the
chemical reaction
but has no effect
on cleansing
PCA a precipitate
that causes color
change (brownishreddish) and may
interfere with the
seal of obturation
Chlorhexidine
EDTA retains its
calciumcomplexing ability
when mixed with
NaOCl
A bubbling effect
reflects the
chemical reaction
but has no effect on
cleansing
White precipitate
that involves the
formation of salt
rather than
undergoing a
chemical
reaction
G
G
Chlorhexidine
PCA a precipitate
that causes color
change
(brownishreddish) and may
interfere with the
seal of obturation
White precipitate that
involves the
formation of salt
rather than
undergoing a
chemical reaction
EDTA, Ethylenediamine tetra-acetic acid; NaOCl, sodium hypochlorite; PCA, para-chloroaniline.
Table 12.5 Composition of MTAD.
Doxycycline
G
G
G
G
G
Isomer of
tetracycline
Broad-spectrum
antibiotic
Bacteriostatic by
inhibition of
protein synthesis
In high
concentrations it
is bactericidal
Has an effect in
smear layer
removal
Citric acid
G
G
Smear layer removal
Addition of NaOCl is
important to remove
organic part of smear
layer
Tween 80
1. Main action is lowering surface
tension
2. May increase antibacterial effect
a. directly by affecting the
bacterial cell membrane and
b. indirectly through facilitating
the penetration of MTAD into
dentin
3. It may decrease antibacterial
effect
a. by being a nutrient to some
bacteria
b. by inactivating CHX and
iodine effect if CHX and IKI
were used as irrigants
CHX, Chlorhexidine; IKI, iodine potassium iodide; MTAD, a mixture of doxycycline, citric acid, and a detergent;
NaOCl, sodium hypochlorite.
Endodontic materials: from old materials to recent advances
269
mixture may have a synergistic effect on the disruption of the bacterial cell wall
and on the cytoplasmic membrane (Torabinejad et al., 2003). MTAD components
impart its mode of action which includes:
G
G
G
lowering the surface tension through Tween 80 which allows the irrigant to penetrate the
dentinal tubules and inaccessible areas;
smear layer removal with doxycycline and citric acid; and
antibacterial efficacy due to doxycycline.
12.3.6 Tetraclean
Tetraclean is similar to MTAD, but they differ in the concentration of antibiotics
and the kind of detergent used. In MTAD, doxycycline has the concentration of
150 mg/5 mL, while the concentration of doxycycline in Tetraclean is 50 mg/5 mL.
The detergent of MTAD detergent is Tween 80, while polypropylene glycol is used
in Tetraclean (Giardino et al., 2005).
12.3.7 Hydrogen peroxide
H2O2 is a clear and colorless liquid that is used widely as a disinfectant; however,
it has a poor popularity among endodontists and it is not recommended to be used
as a routine irrigant. H2O2 is available in concentrations ranging from 3% to 5%
and produces hydroxyl-free radicals (HO2) that attack microbial components such
as proteins and DNA. Moreover, it is active against bacteria, viruses, and yeasts but
some bacteria produce catalase or superoxide dismutase which can provide them
with partial protection against H2O2 (Bettina and Markus, 2012).
12.3.8 Iodine potassium iodide
It is a halogen releasing agent consisting of 2% iodine in 4% potassium iodide
(Siren et al., 2004). IKI is used as an irrigant due to its excellent antibacterial effect
and low cytotoxicity (Spangberg et al., 1973). In addition, it is an oxidizing agent
that cleaves the disulfide bonds present in the free sulfhydryl groups of bacterial
enzymes. In the rare cases of hypersensitivity to NaOCl and CHX, IKI is considered
the ideal irrigant due to its low cytotoxicity. Nevertheless, there are more allergy
concerns linked to IKI compared to NaOCl and CHX. IKI also stains dentin which
is one of its major shortcomings.
12.3.9 1-Hydroxyethylidene-1,1-bisphosphonate
1-Hydroxyethylidene-1,1-bisphosphonate (HEBP) is also called etidronic acid. It is
used systematically in patients suffering from osteoporosis and Paget’s disease. As
an irrigant, it is a chelator like EDTA and citric acid; however, it is considered a
weak decalcifying agent and thus cannot be an effective final rinse. It is preferred
to use HEBP in combination with (NaOCl), particularly since HEBP does not affect
its proteolytic or antimicrobial properties (Zehnder, 2006).
270
Advanced Dental Biomaterials
12.3.10 QMiX
QMiX was first introduced in 2011 as a new combination irrigation solution
(Stojicic et al., 2012). It is recommended to be used as a final rinse after NaOCl
irrigation and complete instrumentation. QMiX is available as a ready-to-use solution and contains a CHX-analog, triclosan (N-cetyl-N,N,N-trimethylammonium bromide), and EDTA. Since it contains CHX, it is recommended to rinse out the
NaOCl from the canal with saline before using QMiX to prevent PCA formation.
Moreover, it was shown that QMiX has comparable antibacterial properties and
ability to remove the smear layer when compared to EDTA (Dai et al., 2011).
Nevertheless, most studies on QMiX are ex vivo and in vivo, and further clinical
studies are needed to ascertain the efficacy of QMiX. Table 12.6 describes some of
the latest available irrigants.
Table 12.6 Some of the newer available irrigants.
Irrigant
Smear Clear
(SybronEndo)
Description
G
G
G
G
Chlor-XTRA
(Vista Dental)
CHX-Plus
(Vista Dental)
Hypoclean A and
Hypoclean B
HEBP
G
G
G
G
G
G
G
G
G
G
G
QMiX
G
G
G
G
Clear and odorless
Water soluble solution
Water 1 17% EDTA 1 salts 1 a cationic surfactant
(cetrimide) 1 anionic surfactant
Adding detergents or surface-active agents is to increase the
wettability of the solution and reduce the surface tension
6% NaOCl with surface modifiers
Adding detergents or surface-active agents is to increase the
wettability of the solution and reduce the surface tension
2% CHX with surface modifiers
Adding detergents or surface-active agents is to increase the
wettability of the solution and reduce the surface tension
5.25% NaOCl solutions modified with surfactants
Adding detergents or surface-active agents is to increase the
wettability of the solution and reduce the surface tension
Used in combination with NaOCl with little interference with
NaOCl activity
Alternative to citric acid and EDTA
Prevents bone resorption
Used systematically in patients suffering osteoporosis and
Paget’s disease
Needs to be studied with further investigations
Contains a CHX-analog, Triclosan
(N-cetyl-N,N,N-trimethylammonium bromide), and EDTA
Ready to use
Used as a final rinse after NaOCl
It lowers surface tension, removes smear layer, and has an
antibacterial effect
CHX, Chlorhexidine; EDTA, ethylenediamine tetra-acetic acid; HEBP, 1-hydroxyethylidene-1,1-bisphosphonate;
NaOCl, sodium hypochlorite.
Endodontic materials: from old materials to recent advances
12.4
271
Intracanal medicaments
It has been a trend among clinicians to use intracanal medicaments in cases where
root canal treatment could not be completed in one visit. According to Athanassiadis
et al. (2007) (Box 12.3), intracanal medicaments are necessary adjuncts to inhibit
bacterial regrowth between appointments due to surviving bacteria and leaky temporary restorations. There are various materials that can be used as intracanal medicaments to enhance the antimicrobial effect of our cleaning procedures. Table 12.7
summarizes old intracanal medicaments that are not commonly used now.
12.4.1 Calcium hydroxide
Calcium hydroxide has a particular importance in dentistry. It has been extensively
used as an intracanal medicament since Hermann introduced it in 1920. It is a slurry
of Ca(OH)2 in a water base but can be mixed with either water or saline and should
have a thick consistency in order to carry as many Ca(OH)2 particles as possible.
Chemically, calcium hydroxide is classified as a strong base with a high pH
(approximately 12.5 12.8) that kills bacteria by direct contact (Safavi et al., 1990);
hence, it should fill the entire length of the canal homogenously in order to exert its
maximum biological effect.
Fig. 12.4 summarizes the physical and chemical effects of Ca(OH)2. In general,
the biological properties of calcium hydroxide are exerted through the ionic dissociation of Ca21 and OH2 ions, this contributes to a high pH which makes Ca(OH)2
antimicrobial (Bystrom and Sundqvist, 1985). It also can inactivate and hydrolyze
bacterial LPS especially in necrotic cases (Safavi and Nichols, 1993). Promoting
hard tissue formation is yet another significant action exerted by Ca(OH)2 (Frank,
1966). However, Ca(OH)2 has some limitations, for example, the rate of diffusion
of hydroxyl ions is slowed due to the inherent buffering capacity of the dentine
(Mohammadi and Dummer, 2011).
There is controversy regarding the use of calcium hydroxide since it was shown
that it does not reduce the number of bacteria significantly when used as an interappointment medicament. Moreover, 20% 45% residue is left on the canal walls even
after irrigating with NaOCl or EDTA (Lambrianidis et al., 1999); this residue affects
the sealing ability of zinc oxide eugenol (ZOE) sealers (Margelos et al., 1997).
Box 12.3 Rationale of intracanal medicaments use
G
G
G
G
G
To eliminate or destroy any remaining viable bacteria in the root canal system that
have not been destroyed by the chemomechanical preparation process (i.e., instrumentation and irrigation)
To reduce periradicular inflammation and hence reduce pain
To help eliminate apical exudate if it is present
To prevent or arrest inflammatory root resorption if it is present
To prevent reinfection of the root canal system by acting as both a chemical and a
physical barrier if the temporary or interim restoration breaks down
272
Advanced Dental Biomaterials
Table 12.7 Intracanal medicaments that are not recommended anymore.
Phenol
compounds
Formaldehyde
Examples
Mode of action
Disadvantages
Several phenolic
preparations have been
used for disinfecting
root canals such as
phenol, camphorated
phenol,
paramonochlorophenol,
thymol, cresol,
camphorated
parachlorophenol
Applying those
compounds
through cotton
pellets or paper
points allows
their
vaporization.
Those vapors
come in direct
contact with
microorganisms
once they
penetrate the
root canal
system
Formaldehyde is a
volatile material
that produces
antimicrobial
vapors when
applied via a
cotton pellet
The antimicrobial
effect
accompanied
with those
compounds
does not
balance the
cytotoxicity
caused by them.
For that reason,
their use has
been decreased
significantly
(Spangberg
et al., 1973)
It is cytotoxic and
has a mutagenic
effect. Its use as
an antimicrobial
medicament is
not justified due
to its toxicity
(Spangberg
et al., 1973;
Lewis and
Chestner, 1981)
It can stain dentin
and is
considered a
severe allergen
G
G
Halogens
G
G
G
Formocresol:
formaldehyde (ranges
between 19% and
37%)
Tricresol formalin:
formaldehyde
component is 90% and
contains 10% tricresol
Chloramine-T
N-Chloro tosylamide
sodium salts
IKI can be used as
both an irrigant and
intracanal medicament
It releases
antimicrobial
vapors which
can disinfect
dentin in 5 min
and has low
toxicity (Safavi
et al., 1990)
IKI, Iodine potassium iodide.
In addition to being used as an intracanal medicament, Ca(OH)2 is used in apexification procedures for immature teeth before obturating the canal with gutta-percha
(GP). Moreover, it has been recently used as a substitute for triple antibiotic pastes
in revascularization procedures of immature teeth (Law, 2013).
12.4.2 Chlorhexidine
Please refer to CHX in section 12.3.3 for more details. CHX has a substantive antimicrobial activity that prevents bacterial colonization for prolonged periods of time,
Endodontic materials: from old materials to recent advances
273
Figure 12.4 The physical and chemical effects of Ca(OH)2.
and this property is behind the rationale for using CHX as an intracanal medicament
in a concentration of 2%.
12.4.3 Ledermix
Schroeder first developed this material as a combination of antibiotic/corticosteroids
paste. Ledermix paste is a nonsetting, water-soluble paste material with a combination of a tetracycline antibiotic, demeclocycline HCl (at a concentration of 3.2%),
and a corticosteroid, triamcinolone acetonide (concentration 1%), in a polyethylene
glycol base. In patients experiencing severe endodontic pain, Ledermix (Riemser
Arzneimittel AG, Insel Riems, Germany) can sometimes be used as an initial medicament in order to alleviate the symptoms (Schroeder, 1975). Furthermore, some
studies have shown that Ledermix can inhibit root resorption and promotes favorable
root healing (Chen et al., 2008). However, there is still controversy regarding products containing corticosteroids due to concern related to their release to the blood
circulation (Abbott, 1992).
12.4.4 Triple antibiotics pastes
As the name indicates, this medicament is composed of three antibiotics in one
paste (metronidazole, ciprofloxacin, and minocycline). This paste can be effective
in eradicating bacteria and has also been used in regenerative endodontics (Windley
et al., 2005). Indeed, it was shown clinically that it promoted root formation in
young permanent teeth with an open apex despite the presence of a periapical radiolucency and a draining buccal sinus tract (She et al., 2016). It should be noted that
there are still concerns related to its use, such as tooth discoloration from minocycline and bacterial resistance.
274
Advanced Dental Biomaterials
12.4.5 Bioactive glass
Bioactive glass consists of a SiO2 Na2O CaO P2O5 system (Zehnder et al.,
2004). It is considered a promising material due its antimicrobial effect and osteoinductive ability. Its antibacterial mechanism of action is achieved through its high
pH, its ability to increase the osmotic pressure above 1% which can inhibit many
bacteria, and through inducing mineralization on bacterial surfaces.
12.5
Root canal obturation materials
Throughout the history of endodontics, several materials were used as root filling
materials ranging from tin foil, cotton pellets, plaster of Paris, to leaving the root
canal unfilled. Grossman outlined in 1987 the properties of an ideal obturation
material and provided criteria that can help identify the optimal obturation material
(Box 12.4).
After proper chemomechanical debridement, the disinfected root canal should be
sealed in order to prevent reinfection. Accordingly, obturation materials should seal
the root canal:
G
G
G
apically to block the exit of surviving microorganisms to the periradicular tissue;
coronally to prevent reinfection of the pulp space from the oral cavity; and
throughout the canal to seal the openings of accessory and lateral canals.
The obturation step involves the use of two types of materials (Fig. 12.5): one is
the core obturation material in the solid form (e.g., GP and resilon) and another
semisolid cementing medium (i.e., sealers).
12.5.1 Core obturation materials
12.5.1.1 Silver points (or cones)
Jasper introduced silver points in 1933 claiming that they are as successful as GP.
Silver points are rigid and have the same diameter and taper as the instruments
Box 12.4 Properties of an ideal obturation material
G
G
G
G
G
G
G
G
G
G
G
Easily manipulated and provides ample working time
Dimensionally stable with no shrinkage once inserted
Seals the canal laterally and apically, conforming to its complex internal anatomy
Nonirritating to the periapical tissues
Impervious to moisture and nonporous
Unaffected by tissue fluids—no corrosion or oxidization
Inhibits bacterial growth
Radiopaque and easily discernible on radiographs
Does not discolor tooth structure
Sterile
Easily removed from the canal if necessary
Endodontic materials: from old materials to recent advances
275
Figure 12.5 Diagrammatic illustration of the root canal fillings.
Table 12.8 Advantages and disadvantages of silver points.
Advantages of silver points
G
G
G
G
Rigid
Have the same taper and diameter as
the files used to shape the canal
Easily placed inside the canal
More predictable length control
Disadvantages of silver points
G
G
G
G
Nonadaptable and unable to fill canal
irregularities and this permits leakage
It corrodes when in contact with tissue
fluids or saliva
The cytotoxic corrosion by-products
impair periapical healing
Difficult to remove if retreatment is
indicated
used to shape the canal, this property facilitated their placement and allowed a
more predictable length control. Silver points possess most of the properties
Grossman identified, yet their rigidity precludes proper adaptation to the root canal,
and thus inability to form a proper seal apically and laterally. Table 12.8 lists the
main advantages and disadvantages of silver points. Furthermore, the leakage of the
sealers caused the corrosion of silver points and formation of cytotoxic silver salts
(Brady and del Rio, 1975). With those major disadvantages of silver points their
use nowadays is considered as below the standard of care.
12.5.1.2 Gutta-percha
GP is considered the most widely used obturation material. It is derived from various species of rubber trees from Malaysia, Borneo, Indonesia, and South America,
mainly from Brazil. It is the trans-isomer of 1,4-polyisoprene (rubber) and it exists
in two crystalline forms (α and β) (Goodman et al., 1974) (Fig. 12.6). The β phase
is the unheated solid form that can be compacted. When heated, it transforms into
the α phase which exhibits superior thermoplastic properties since it becomes
pliable and can flow when pressure is applied. This characteristic is utilized in
heat-softened GP obturation techniques (e.g., Thermafil and Obtura) and is now
considered the gold standard.
276
Advanced Dental Biomaterials
Figure 12.6 cis and trans isomers of 1,4-polyisoprene (natural rubber and gutta-percha).
Box 12.5 Ideal properties of a root canal irrigant
G
G
G
G
59% 76% Zinc oxide
18% 22% Gutta-percha
1% 18% Heavy metals salts
1% 4% Wax or resin
Table 12.9 Advantage and disadvantages of gutta-percha points.
Advantages
G
G
G
G
G
G
Plasticity
Ease of manipulation
Minimal toxicity (inert)
Radiopaque
Can be removed with heat or solvents
Adapts with compaction to canal
irregularities
Disadvantages
G
G
G
G
Lack of adhesion to dentin
Shrinkage on cooling (1% 2%)
Elasticity (rebounds, pulls away)
Oxidizes to air and light and becomes
more brittle
According to Friedman et al. (1975), GP is not the main constituent of these
obturation points and contains zinc oxide as a filler, wax, and resins as plasticizers
and radiopacifier heavy metals such as barium sulfate (Box 12.5). It satisfies most
of the properties identified by Grossman; however, its main disadvantage is that it
lacks adequate rigidity. Another disadvantage is its inability to seal without a sealer.
Table 12.9 summarizes the advantages and disadvantages of GP.
GP is available in standardized International Standards Organization (ISO) sizes
and nonstandardized sizes such as extrafine, fine fine, fine, medium fine, fine
medium, medium, large, and extralarge. Initially, it was fabricated in the standard
0.02 taper, but with the introduction of newer shaping instruments with larger
tapers, GP points are manufactured to match those instruments. For instance, a fine
medium cone means that the cone has a fine tip with a medium body.
Endodontic materials: from old materials to recent advances
277
GP can be sterilized by 5.25% NaOCl for 1 minute, then rinsed with ethyl alcohol to remove crystallized NaOCl, which, if not removed, would impair the obturation seal. It is important to note that it cannot be heat-sterilized. GP oxidizes to air
and light and becomes brittle; consequently, storage in a cool dry place such as
refrigerators is imperative. Moreover, it can be softened by chloroform, halothane,
and to a lesser degree by turpentine and xylene.
12.5.1.3 Resilon
Resilon is a polyurethane thermoplastic root canal filling material. It is used with
certain sealers such as Epiphany, RealSeal, and Resinate. The introduction of this
material aimed to achieve what is known as “monoblock” where the resilon sealer
(epiphany) bonds to both the etched canal wall and the resilon cone, but whether
this can be truly achieved is still controversial (Tay and Pashley, 2007; Raina et al.,
2007). Moreover, the use of this bonding resin does not strengthen the tooth.
Resilon consists of the following (Shipper et al., 2004):
G
G
G
Methacrylate resin (difunctional) bisphenol A glycidyl methacrylate (bis-GMA).
Bioactive glass.
Radiopaque fillers (bismuth oxychloride and barium sulfate) make up 65% of its content.
Similar to GP, Resilon is manufactured in the same ISO sizes and shapes; it can
also be softened using heat or chloroform and can be used with any obturation technique (lateral condensation, thermoplasticized, carrier based). Furthermore, the sealing ability of Resilon is comparable to GP (Baumgartner et al., 2007). In addition,
Resilon is nontoxic, nonmutagenic, and biocompatible (Emre et al., 2008). It is also
compatible to be used with cores and posts that are resin placed.
The Resilon system consists of a primer, a sealer, and synthetic polymer points
or pellets. Preparatory steps are needed to use this material, such as using a SelfEtch Primer. This primer consists of sulfonic acid-terminated functional monomer,
2-hydroxyethyl methacrylate, water, and polymerization initiator. The primer is
applied (two to three drops) with a pipette or syringe or paper point. It is essential
to know that NaOCl affects the bond of the primer so it is mandatory to use EDTA
as a final rinse before rinsing the canal with sterile water, saline, or CHX.
Afterward, the excess primer is removed, and the resin sealer is mixed and applied
to a paper point, lentulo spiral, or Resilon point. Eventually, the canal is filled with
any obturation technique.
12.5.2 Root canal sealers (cementing medium)
Since root filling materials do not bond to the dentinal wall of the root canal, sealers are crucial for sealing the space between the two surfaces and fill the voids and
irregularities in the root canal anatomy during obturation. In 1982 Grossman outlined the properties of an ideal sealer (Box 12.6). However, currently, no sealer
satisfies all these characteristics. Different kinds of sealers are present, each with
their advantages and disadvantages.
278
Advanced Dental Biomaterials
Box 12.6 Properties of an ideal root canal sealer
G
G
G
G
G
G
G
G
G
G
G
Exhibits tackiness when mixed to provide good adhesion between it and the canal
wall when set
Can establish a hermetic seal
Radiopaque
Made of a very fine powder, so that it can mix easily with liquid
Exhibits a slow set
Does not undergo shrinkage on setting
Does not stain the tooth structure
Bacteriostatic, or at least does not encourage bacterial growth
Insoluble in tissue fluids
Tissue tolerant, that is, nonirritating to periradicular tissue
Soluble in a common solvent if it is necessary to remove the root canal filling
12.5.2.1 Zinc oxide eugenol sealers
It is the most commonly used sealer so far. There are various product brands that
contain ZOE as the main ingredient and only differ in the other components added
to the sealer. The advantages of ZOE sealers are its antimicrobial activity (Heling
and Chandler, 1996), slow setting time (Allan et al., 2001), and it undergoes resorption when extruded into the periradicular tissues (Augsburger and Peters, 1990).
Nevertheless, some formulas of ZOE sealers can stain the tooth structure and shrink
on the setting (Krastl et al., 2013; Kazemi et al., 1993). Table 12.10 summarizes
different ZOE sealers.
One characteristic of ZOE sealers is the ability of the constituents of the material
to enhance its properties. For instance, paraformaldehyde was added for antimicrobial and mummifying effects; however, it is not acceptable due to its severe adverse
effects. When corticosteroids are added to the sealer, they can suppress inflammatory reactions. Canada Balsam can also be added for a more sticky and tacky properties that would improve the sealer’s adhesion to dentin. Rosins (colophony),
which are derived from conifers, were initially added for better adhesive properties
(Grossman, 1982), but it was later found that resins acids which form 90% of rosins
might be cytotoxic, yet the addition of resin acids to zinc oxide may be beneficial.
Recent research is trying to add nanoparticles such as chitosan and quaternary
ammonium polyethylenimine to enhance the antibacterial effectiveness of the sealer
(Shrestha and Kishen, 2016). Chitosan [poly(1,4-b-D-glucopyranosamine)] is a long
polymer chain which gains its effectiveness from its chemical structure. By adding
chitosan nanoparticles, the antibacterial effect of the sealer is increased without
deteriorating its flow characteristics. However, more research is required for the
incorporation of nanoparticles into dental materials.
12.5.2.2 Calcium hydroxide sealers
This sealer was introduced to exploit the antibacterial and hard tissue formation
properties of calcium hydroxide. Nevertheless, those properties could not be
Endodontic materials: from old materials to recent advances
279
Table 12.10 Zinc oxide eugenol (ZOE) sealers.
Rickert’s formula
Pulp Canal Sealer
(SybronEndo)
Pulp Canal Sealer EWT
Proscol (Procosol, Inc.,
Philadelphia, PA)
Roth’s Sealer (Roth’s
Pharmacy, Chicago, IL)
Wach’s sealer (Balas Dental,
Chicago, IL)
Tubliseal
1. The earliest formula of ZOE
2. It satisfied most of Grossman’s properties except that
it caused staining to tooth tissues due to silver
particles
1. It followed Rickert’s formula
2. It exhibited very rapid setting time
3. This sealer used extensively by clinicians in
thermoplastic warm vertical obturation
1. It is a modification of Pulp Canal Sealer
2. It was marketed as having a 6 h working time
3. This sealer is used extensively by clinicians in
thermoplastic warm vertical obturation
1. It is a modification of Rickert’s formula by removing
the silver particles to make a nonstaining sealer
2. It contains zinc oxide, hydrogenated staybelite resin,
bismuth subcarbonate, and barium sulfate
1. It is a modification of Rickert’s formula by removing
the silver particles to make a nonstaining sealer
2. It contains zinc oxide, hydrogenated staybelite resin,
bismuth subnitrate, and barium sulfate
1. Its powder contains zinc oxide, bismuth subnitrate,
bismuth subiodide, magnesium oxide, and calcium
phosphate, while the liquid consists of oil of cloves,
eucalyptol, Canada balsam, and beechwood creosote
2. Canada balsam is what makes this sealer different than
other sealers when used in lateral compaction due to
its tacky property that softens the gutta-percha into a
more homogeneous mass
1. Unlike the previous powder/liquid formulas, it is a
catalyst/base sealer
2. It is known to be easily mixed with a two-paste
system in two separate tubes. The paste contains zinc
oxide-base, barium sulfate for radiopacity, and mineral
oil, cornstarch, and lecithin. The catalyst tube has
polypale resin, eugenol, and thymol iodide
3. Tubliseal has the disadvantage of having a rapid
setting time and that it is modified in Tubliseal EWT
EWT, Extended working time.
demonstrated (Desai and Chandler, 2009). Furthermore, in order to release significant amounts of calcium hydroxide, the sealer should exhibit high solubility properties, which is inconsistent with the optimum properties of sealers. SealApex,
Calciobiotic Root Canal Sealer, and Apexit have calcium hydroxide as one of their
main ingredients. Table 12.11 describes the composition of the different calcium
hydroxide sealers.
280
Advanced Dental Biomaterials
Table 12.11 Composition of different calcium hydroxide Ca(OH)2 sealers.
Type of Ca(OH)2
sealer
SealApex
Ingredients
G
G
CRCS
G
G
Apexit
G
G
Base: Zinc oxide, calcium hydroxide, butyl benzene,
sulfonamide, and zinc stearate
Catalyst: Barium sulfate and titanium dioxide for radiopacity, a
proprietary resin, isobutyl salicylate, and aerosil R792
Powder: Calcium hydroxide, zinc oxide, bismuth dioxide, and
barium sulfate
Liquid: Eugenol and eucalyptol
Base: Calcium hydroxide, zinc oxide, calcium oxide, silicon
dioxide, zinc stearate, hydrogenized colophony, tricalcium
phosphate, and polydimethylsiloxane
Activator: Trimethyl hexanediol diasalicylate, bismuth carbonate
basic, bismuth oxide, silicon dioxide, 1,3-butanedioldisalicylate,
hydrogenized colophony, tricalcium phosphate, and zinc stearate
CRCS, Calciobiotic Root Canal Sealer.
12.5.2.3 Glass ionomer sealers
Glass ionomers are capable of binding to dentin, and thus, they were incorporated
in certain endodontic sealers, such as Ketac-Endo (3M, Minneapolis, MN)
(Friedman et al., 1995). However, the disadvantage of this sealer is its limited antimicrobial effect (Heling and Chandler, 1996), the difficulty in conditioning the middle and apical parts of the root canal to receive the glass ionomer sealer, and the
difficulty of removing the sealer in cases of retreatment. Glass ionomer sealers are
usually used with Activ GP (Brasseler USA, Savannah, Georgia) which is composed of GP impregnated with glass ionomer.
12.5.2.4 Resin sealers
Resin sealers are popular for their favorable adhesive properties and lack of eugenol.
These sealers are either epoxy-resin sealers (e.g., AH-26 and AH-plus) or urethane
methacrylate resin sealers (e.g., EndoREZ and Epiphany). AH-26 (Dentsply
International Maillefer) is a bisphenol epoxy resin sealer that uses hexamethylenetetramine (methenamine) for polymerization. In addition to its adhesive properties,
AH-26 demonstrates increased radiopacity, low solubility, low polymerization shrinkage, and tissue compatibility. However, the methenamine releases some formaldehyde as it sets, which is the major disadvantage of using this sealer (Spangberg et al.,
1993). Moreover, tooth staining and extended working time are other disadvantages.
AH-plus (Dentsply International) is a modification of AH-26 with comparable sealing
properties without the release of formaldehyde (De Moor and De Bruyne, 2004).
Compared to AH-26, the AH-plus sealer exhibits lower solubility, higher radiopacity,
and shorter working time (B4 hours) and setting time compared to AH-26.
As for methacrylate resin sealers, four generations of endodontic sealers have
been marketed so far summarized in Table 12.12 (Kim et al., 2010).
Table 12.12 Methacrylate resin sealers.
Methacrylate resin
sealer generation
Major components
Main characteristics
First generationHydron
(Hydron
Technologies, Inc.,
Boca Raton, FL)
Poly(2-HEMA)
G
G
Hydrophilic
Injectable without the
use of root filling core
material
Advantages
G
G
G
G
G
Second
generationEndoREZ
(Ultradent Products
Inc, South Jordan,
UT)
G
G
Nonacidic
diurethane
dimethacrylate
In addition to
triethylene glycol
dimethacrylate
G
G
G
G
G
G
G
Nonetching
Radiopaque
Dual cured
Hydrophilic in nature
Can be used with
conventional gutta-percha
or specific EndoREZ
points which are resin
coated gutta-percha cones
Seals best when applied to
moist intraradicular dentin
No adjunctive use of a
dentin adhesive.
However, an accelerator
has been introduced for
rapid cure
G
G
Injectable which makes
it easy to use
Nonirritating
Highly adaptable to the
canal walls
Nonsupportive of
bacterial growth
Calcification ability in
the event of
inadvertent extrusion
of the sealer into the
periapical regions
Retentive due to the
formation of resin tags
when it flows into the
accessory canals and
dentinal tubules
especially after the
removal of the smear
layer with NaOCl and
EDTA
It might be used in the
wet environment of the
root canal system
Disadvantages
G
G
G
G
G
G
Smear layer
removal
Severe
inflammatory
reaction
Absorption of
the material
Severe leakage
Water sorption
and swelling
Low bond
strength to the
dentinal wall
when used
with
conventional
uncoated
gutta-percha
Studies that
show its
superiority
lacked the use
of additional
sealers for
comparison
Smear layer removal
by a final rinse of
NaOCl and EDTA
is very important
for the formation of
resin tags
(Continued)
Table 12.12 (Continued)
Methacrylate resin
sealer generation
Major components
Main characteristics
Third generation: selfetching sealers
FibreFill R.C.S. root
canal sealant
(Pentron Clinical
Technologies,
Wallingford, CT)
Epiphany (Pentron
Clinical
Technologies)
RealSeal
(SybronEndo,
Orange, CA),
Resinate (Obtura
Spartan Corp,
Fenton, MO)
Smart (Discus
Dental, Culver City,
CA)
Contains a selfetching primer and
a dual-cured resin
composite root
canal sealer
Using an acidic self-etching
primer brought back the
concept of incorporating
the smear layer formed
by hand/rotary
instrumentation along the
sealer dentin interface.
The primer is applied to
the surface of dentin to
penetrate the smear layer
and demineralize the
superficial dentin and
then it is air-dried to
remove any volatile
carrier
1. The dual cure flowable
resin sealer is applied
after the primer and
polymerized
G
G
G
G
Advantages
G
G
Bonding procedure is
simplified
The self-etching
primers in some sealers
are even reduced from
a two-bottle system to
a single-bottle system.
These self-etching
primers contain AMPS
as the functional
acidic. This shorten the
time needed before
bonding
Disadvantages
Smear layer
removal
Bonding apically
may be
compromised if
the primer was
not aggressive
enough to
penetrate the
smear layer in
the apical third
The primer is applied
to the surface of
dentin and able to
penetrate through
the smear layer
and to
demineralize the
superficial dentin
Fourth generation:
MetaSEAL, Parkell
Inc; RealSeal SE,
SybronEndo or
Hybrid Bond SEAL
(Sun Medical Co Ltd,
Shiga, Japan)
MetaSEAL or
Hybrid Bond
SEAL are
composed of
acidic resin
monomers that are
usually found in
dentin adhesive
primers are
integrated into the
resin-based sealer
which makes them
self-adhesive
1. 4-META which
makes the sealer
self-etching,
hydrophilic and
promotes
monomer
diffusion into the
underlying intact
dentin to produce
a hybrid layer
after
polymerization
G
G
Eliminated the separate
etching/bonding step
Those sealer creates a
hybrid layer in both the
thermoplastic root filling
and the radicular dentin
which promotes their
bonding
G
G
G
G
G
The fact that the
etchant, primer, and
sealer form an all-inone self-etching, selfadhesive sealer reduces
the application time
and the errors that
usually occur during
the bonding stage
Self-adhesive
Dual-cured sealer
Hydrophilic
Self-etching
G
G
Studies have
shown similar
or slightly
inferior sealing
properties as
conventional
nonbonding
epoxy resinbased sealers
Limited
aggressiveness
of hybridizing
radicular
dentin
especially
apically and
inaccessible
areas of the
root call like
isthmi
It is recommended by
the manufacturers
to use EDTA as a
final rinse when
using methacrylate
resin-based sealers
in order to remove
the smear layer,
reduce the leakage
and improve the
seal of filled
canals
4-META, 4-Methacryloyloxyethyl trimellitate anhydride; AMPS, 2-acrylamido-2-methyl-propanesulfonic acid; EDTA, ethylenediamine tetra-acetic acid; HEMA, hydroxyethyl methacrylate; NaOCl, sodium
hypochlorite.
284
Advanced Dental Biomaterials
12.5.2.5 Bioceramic-based sealers
These sealers are currently gaining a wide popularity due to their outgrowth from
MTA and the extensive research and technology directed toward enhancing the use
of bioceramics in endodontics. MTA and MTA-like materials are made of tricalcium silicate and their importance rises from their hydrophilic properties, excellent
sealing ability, and their bioactivity (Al-Haddad and Che Ab Aziz, 2016).
Table 12.13 summarizes the available bioceramic-based sealers and a few newer
ones that are still in the experimental phase.
12.5.2.6 Other sealers
Other types of sealers include noneugenol sealers, silicone sealers, chloropercha,
and sealers containing formaldehyde. For more details about these sealers refer to
Table 12.14 which summarizes the main sealers used in endodontics.
Table 12.13 Bioceramic-based sealers.
Bioceramic-based sealer
MTA Fillapex (Angelus
Industria de Produtos
Odontologicos Ltda;
Londrina, Parana, Brazil)
iRoot SP (Innovative
BioCeramix Inc.,
Vancouver, BC, Canada)
aka Endosequence BC
sealer (Brasseler USA,
Savannah, GA)
Endo CPM Sealer (EGEO
SRL, Buenos Aires,
Argentina)
MTA Plus (Avalon Biomed,
Bradenton, FL) and (Prevest
Denpro, Jammu City, India)
Description
G
G
G
G
G
G
G
G
A resin MTAbased root canal
sealer
Available as a
dual paste that
are combined in
a mixing tip
A bioactive
alkaline calcium
silicate sealer
Premixed readyto-use single
paste
An MTA-based
root canal sealer
Powder/gel
A calcium
silicate sealer
Powder/gel
Composition
Natural resin, salicylate resin,
diluting resin, bismuth
trioxide, nanoparticulated
silica, MTA, and pigments
G
G
Zirconium oxide, calcium
silicates, calcium phosphate
monobasic
CH and filling and
thickening agents
MTA in addition to calcium
chloride, calcium carbonate,
sodium citrate, propylene
glycol alginate, and
propylene glycol
MTA powder with a finer
particle size
Two formulations are
available either mixed with
water or a hydrosoluble gel
for decreasing washout
property
G
G
(Continued)
Endodontic materials: from old materials to recent advances
285
Table 12.13 (Continued)
Bioceramic-based sealer
Generex B ProRoot Endo
Sealer (Dentsply Tulsa
Dental Specialties, Tulsa,
OK, United States)
Description
G
G
A calcium
silicate sealer
Mixed with a
liquid-to-powder
ratio of 1:2
Composition
The powder is composed of
tricalcium silicate,
dicalcium silicate, calcium
sulfate (as a setting
retardant), bismuth oxide
(as a radiopacifier), and a
small amount of tricalcium
aluminate
The liquid is composed of
water and a viscous watersoluble polymer
Two formulas are available:
The first one was
introduced by Camilleri
and associates consist of a
mixture of 80% white
Portland cement and 20%
bismuth oxide
The second one was
introduced from Brazil and
is composed of Portland
cement, zirconium oxide
(radiopacifier), calcium
chloride, and a resinous
vehicle
Powder: α-tricalcium
phosphate and hydroxySankin apatite in type I,
iodoform added to powder
in type II (30%) and type
III (5%)
Liquid: polyacrylic acid
and water
Powder: TTCP and DCPA,
Portland cement (gray
cement in type I and white
cement in type II),
zirconium oxide, and others
Liquid: hydroxypropyl
methyl cellulose in sodium
phosphate solution
G
G
Mineral Trioxide Aggregate
Sealer (MTAS)
Powder-to-liquid
ratio of 5:3 by
weight
G
G
Sankin apatite root canal
sealer (I III), Sankin
Kogyo, Tokyo, Japan
Calcium
phosphate based
root canal sealer
G
G
G
G
Capseal (I and II)
Experimental
Calcium
phosphate based
root canal sealer
G
G
CH, Calcium hydroxide; DCPA, dicalcium phosphate anhydrous; MTA, mineral trioxide aggregate; TTCP,
tetracalcium phosphate.
Table 12.14 Root canal sealers.
Description
Zinc oxide
eugenol
cement sealer
G
G
G
G
G
G
Calcium
hydroxide
sealers
Most commonly used sealer
Modification of the regular ZnOE
The mixing vehicle is mostly
eugenol
Powder contains ZnO that has been
finely sifted to enhance the flow
Setting process is a chemical
reaction with physical embedding
of ZnO in a matrix of zinc
eugenolate
Free eugenol always remains in the
mass as an irritant
Advantages
G
G
Absorbed if extruded into
periradicular tissue
Antimicrobial effect through
ZnO or additives such as
rosin and Canada Balsam or
corticosteroids
Disadvantages
G
G
G
Developed from periodontal
dressing
It is a catalyst/base sealer with a
base of zinc oxide, barium sulfate,
bismuth oxychloride, and
vegetable oil, and the catalyst
containing hydrogenated rosin,
methyl abietate, lauric acid,
chlorothymol, and salicylic acid
G
G
G
G
G
G
G
Noneugenol
sealers
G
G
It was developed for two main
reasons:
1. Antimicrobial effect
2. Osteogenic cementogenic potential
However, these two effects were not
demonstrated
G
Shrinks on setting
Stains the tooth (Roth’s Sealer
was developed to be as a
nonstaining ZnOE sealer)
Examples
No irritating effect of eugenol
Needs to be soluble in order
to leach out the hydroxyl
group responsible for its
activity but sealers shouldn’t
exhibit solubility
Poor cohesive strength
Poor dentin adhesion
G
G
G
Pulp Canal Sealer
(SybronEndo)
Pulp Canal Sealer
EWT
Proscol (Procosol, Inc.,
Philadelphia, PA)
Roth (Roth’s
Pharmacy, Chicago,
IL)
Tubliseal (SybronEndo/
Kerr)
Wach’s Sealer (Balas
Dental, Chicago, IL)
CRCS (Coltène/
Whaledent)
Sealapex (SybronEndo)
Apexit (Ivoclar
Vivadent)
Nogenol (GC America,
Alsip, IL)
Glass ionomer
sealers
Developed to take advantage of their
bond to dentin, fluoride release,
antimicrobial activity, and
biocompatibility
G
G
G
Dentin binding
Minimal tissue irritation
Low toxicity
G
G
G
G
Resin sealers
G
G
G
Introduced because it provides
good adhesion
AH-26 and AH-plus are epoxy
resins
Methacrylate resin sealers were
introduced in four generations
G
G
Good adhesion ability
Does not contain eugenol
G
G
Solubility concern
Inadequate bonding with guttapercha due to difficult
conditioning of the middle and
apical thirds of the root canal
Minimal antibacterial effect
Difficulty in case of
retreatment
AH-26 contains formaldehyde
which is toxic when freshly
mixed but this toxicity
declines rapidly after 24 h.
This was modified by the
introduction of AH-plus that
does not release formaldehyde
Some of the disadvantages of
methacrylate resin sealers are
polymerization shrinkage,
failure of bonding at the
dentin sealer interface,
presence of residual monomers,
cytotoxicity in case extrusion
outside the canal, difficulty of
removal in cases of retreatment
and its low cohesive, tensile,
compressive strengths in
comparison with dentin which
indicates their inability to
enhance the mechanical
properties of root canal dentin
G
G
G
G
G
G
G
G
G
G
G
Ketac-Endo (3M ESPE,
Minneapolis, MN)
Activ GP (Brasseler
USA, Savannah, GA)
which is a gutta-percha
cone impregnated with
GI coating
AH-26 (Dentsply
International Maillefer)
AH-Plus (Dentsply
International)
EndoREZ (Ultradent
Products Inc, South
Jordan, UT)
FibreFill R.C.S. root
canal sealant (Pentron
Clinical Technologies,
Wallingford, CT)
Epiphany (Pentron
Clinical Technologies)
RealSeal (SybronEndo,
Orange, CA)
Resinate (Obtura
Spartan Corp, Fenton,
MO)
Smart (Discus Dental,
Culver City, CA)
MetaSEAL (Parkell
Inc; RealSeal SE,
SybronEndo); Hybrid
Bond SEAL (Sun
Medical Co Ltd, Shiga,
Japan)
(Continued)
Table 12.14 (Continued)
Description
Advantages
Disadvantages
Examples
Silicone-based
sealers
Two materials are available:
1. RoekoSeal (Coltène/Whaledent): which is a polyvinylsiloxane or polydimethylsiloxane root canal sealer and which exhibits slight
expansion on setting (Orstavik et al., 2001)
2. GuttaFlow (Coltène/Whaledent)
a. Cold, flowable, self-curing obturation material for root canals that combines gutta-percha and polydimethylsiloxane sealer (RoekoSeal)
into one injectable system
b. Fills canal irregularities (Zielinski et al., 2008)
c. Inject the material in the canal and then place a single master cone
d. Working time is 15 min and cures in 25 30 min
e. Available in capsules to be triturated
f. Delay of setting time with final irrigation of NaOCl (Bouillaguet et al., 2006)
g. Biocompatible (Bouillaguet et al., 2006)
Chloropercha
White gutta-percha (Alba) mixed
with chloroform
Not used anymore
Composed of zirconium oxide and
calcium silicates. And some have
calcium phosphate as well
G
G
Bioceramicbased sealers
The addition of chloroform
allows the gutta-percha cone
to fit better in the canal
Hydrophilic
Sets by utilizing moisture, the
reaction of calcium silicates
in the presence of the dentin’s
moisture, will form
hydroxyapatite and this will
enhance the sealing ability of
the sealer
No shrinkage on setting
Antimicrobial effect during
setting
Biocompatible
G
G
No adhesive ability
Toxicity of chloroform
(Zakariasen et al., 1990)
Hardens on setting so retreatment
might be difficult to perform if
required
G
G
G
G
G
G
G
G
MTA Fillapex
(Angelus Industria de
Produtos
Odontologicos Ltda;
Londrina, Parana,
Brazil)
Generex B ProRoot
Endo Sealer (Dentsply
Tulsa Dental
Specialties, Tulsa, OK,
United States)
iRoot SP (Innovative
BioCeramix Inc.,
Vancouver, BC,
Canada) aka
G
G
G
G
G
Sealers
containing
formaldehyde
Absolutely contraindicated
G
G
Toxic
Overextension causes
irreversible neurotoxicity
dysesthesia (Kleier and
Averbach, 1988)
G
G
G
G
CRCS, Calciobiotic Root Canal Sealer; EWT, extended working time; GI, glass ionomer; GP, gutta-percha; MTA, mineral trioxide aggregate; NaOCl, sodium hypochlorite.
Endosequence BC
sealer (Brasseler USA)
Endo CPM Sealer
(EGEO SRL, Buenos
Aires, Argentina)
MTA Plus (Avalon
Biomed, Bradenton,
FL) and (Prevest
Denpro, Jammu City,
India)
MTAS
Sankin apatite root
canal sealer (I, II, and
III) Sankin Kogyo,
Tokyo, Japan
Capseal I and II
Endomethasone
(Septodont, Paris,
France)
Rieber’s paste
(Amubarut; Wera Karl,
Biesingen, Germany)
N2 (Indrag-Agsa,
Losone, Switzerland)
SPAD
290
Advanced Dental Biomaterials
12.6
Root-end filling materials
Periradicular surgery is an indispensable part of endodontics. When orthograde
retreatment does not eradicate the periradicular pathosis, root-end resection is
required followed by applying a biocompatible root-end filling material for proper
seal. Many root-end filling materials are available in the market, but none of them
verify all the requirements of an ideal root-end filling as summarized by Chong and
Pitt Ford (2005) (Box 12.7).
12.6.1 Amalgam
Amalgam is a radiopaque material and can be manipulated easily. Nevertheless,
there are many disadvantages that are associated with its use as a root-end filling,
such as tissue biocompatibility, ineffective seal, amalgam tattoo appearance, corrosion, and dimensional changes (Dorn and Gartner, 1990). Hence, the use of amalgam as a root-end filling is decreasing significantly.
12.6.2 Zinc oxide eugenol cements
These cements are made of the basic ZOE mixture with the addition of other materials that can counteract its shortcomings such as solubility and reduced strength
(refer Table 12.15).
12.6.3 Composite resins (Retroplast)
Retroplast is a radiopaque dentin-bonding composite resin. It is provided in a twopaste system that is mixed in equal parts to form a dual cure composite resin with a
working time of 1.5 2 minutes. Paste A is composed of bis-GMA/TEGDMA 1:1,
benzoyl peroxide N,N-di-(hydroxyethyl)-p-toluidine, and butylated hydroxytoluene
Box 12.7 Requirements of an ideal root-end filling material
G
G
G
G
G
G
G
G
G
G
G
Should adheres or bond to tooth tissue and “seal” the root-end three dimensionally
Should not promote, and preferably inhibit, the growth of pathogenic
microorganisms
Dimensionally stable and unaffected by moisture in either the set or unset state
Well tolerated by periradicular tissues with no inflammatory reactions
Stimulates the regeneration of normal periodontium
Nontoxic both locally and systemically
Should not corrode or be electrochemically active
Should not stain the tooth or the periradicular tissues
Easily distinguishable on radiographs
Has a long shelf life
Easy to handle
Endodontic materials: from old materials to recent advances
291
Table 12.15 Root-end filling materials—zinc oxide eugenol (ZOE) cements (Dorn and
Gartner, 1990; Walivaara et al., 2009).
Root-end
filling
material
Chemical composition
Description
IRM (Caulk/
Dentsply,
Milford,
DE)
Powder/liquid mixed in equal
parts. However, a higher
powder-to-liquid ratio of IRM
is recommended, forming a
consistency with easier
placement, shorter setting
time, decreased toxicity and
solubility
Powder: 75% zinc oxide and
20% 25% polymethacrylate
Liquid: 99% eugenol and less
than 1% acetic acid
It is a reinforced ZOE cement with
polymethacrylate added to it.
Since eugenol is the major
cytotoxic component in ZOE
cement, polymethyl
methacrylate will limit its
release because of eugenol’s
high affinity to it. It has better
sealing ability than amalgam
and it is well tolerated by the
periapical tissue but without
hard tissue regenerative
capabilities (Crooks et al., 1994)
Super EBA is another reinforced
ZOE cement. It comes in two
forms, regular set and fast set.
Super EBA is well tolerated by
the periradicular tissues yet with
no capacity to regenerate
cementum. It has much better
physical properties than ZOE
such as high compressive
strength and better tensile
strength. A good healing
response was observed with
super EBA with minimal
chronic inflammation at the root
apex and less apical leakage
G
G
Super EBA
(Bosworth,
Skokie, IL)
Powder/liquid mixed in equal
parts
Powder: 60% zinc oxide, 34%
aluminum oxide, and 6%
natural resin
Liquid: 37.5% eugenol and
62.5% o-methoxybenzoic acid
G
G
IRM, Intermediate restorative material; super EBA, super ethoxybenzoic acid.
(BHT); whereas paste B is made of resin ytterbium trifluoride aerosil ferric oxide.
To enable the adhesion of Retroplast to the root-end surface, a specifically designed
dentin-bonding agent known as GLUMA is used to condition the root-end surface.
Interestingly, it was shown that Retroplast-GLUMA system demonstrates better
sealing properties than the other filling materials including amalgam, intermediate
restorative material (IRM), super ethoxybenzoic acid (super EBA), and glass ionomer cements (GIC). Moreover, some studies showed that it promotes a favorable
periradicular healing response and can promote periodontal regeneration with
some evidence of cementum layer formation over the root-end filling (Yazdi et al.,
2007; Rud et al., 1991a,b). However, similar to all composites, Retroplast is
292
Advanced Dental Biomaterials
technique-sensitive and any blood contamination during bonding process will
reduce its strength and increase leakage.
12.6.4 Glass ionomer cements
GIC is made of aqueous polymeric acids such as polyacrylic acid plus basic glass
powders such as calcium aluminosilicate. It can be either chemically cured or lightcured; however, the seal of light-cured GIC is superior to the chemically cured
counterparts. GIC has similar sealability and tissue response to IRM and super
EBA, and like Retroplast, contamination with blood and moisture affects its properties (Scherer and Dragoo, 1995; Zetterqvist et al., 1991).
12.6.5 Diaket (3M/ESPE, Seefeld, Germany)
Diaket is a polyvinyl resin with an excellent sealing ability. When mixed at thicker
consistencies, it demonstrated good biocompatibility with osseous tissues with a
regenerative potential (Williams and Gutmann, 1996). This material is not available
in the United States.
12.6.6 Resin ionomer suspension and compomer
These materials combine the advantages of both composites and glass ionomers.
Two common examples are Geristore and Dyract (Dentsply, Tulsa, Oklahoma).
Both these materials are light-cured, require dentin-bonding agents, and exhibit less
leakage than IRM, super EBA, and amalgam (Greer et al., 2001). Maintaining a dry
environment during application results in a strong bond, though these materials are
less sensitive to moisture than conventional GIC (Cho et al., 1995). Geristore has a
paste/paste formula made of hydrophilic bis-GMA with long-term fluoride release.
Geristore also demonstrates a potential to regenerate periradicular tissue which promoted its use as a root-end filling material and a restoration material (Scherer and
Dragoo, 1995).
12.6.7 Other types of cement
Other types of cements are also used as root filling materials including MTA, calcium aluminate, calcium phosphate, and calcium silicate cements. Refer to those
materials where mentioned in this chapter.
12.7
Perforation repair materials
Many materials have been used for repairing root perforations and Box 12.8
describes the ideal properties of those materials (Hartwell and England, 1993;
Kakani et al., 2015). Examples of materials used include Indium foil, amalgam,
Endodontic materials: from old materials to recent advances
293
Box 12.8 Ideal properties of perforation repair materials
G
G
G
G
G
G
G
It should provide adequate seal
It should be biocompatible
It should have ability to produce osteogenesis and cementogenesis
It should be bacteriostatic and radiopaque
It should also be beneficial to use a resorbable matrix in which a sealing material
can be condensed
It should be relatively inexpensive
It should be nontoxic, noncariogenic, and easy to place
ZnO eugenol, IRM, super EBA, GIC, adhesives, calcium hydroxide, calcium phosphate cements, MTA, calcium silicate cements, etc. Refer to those materials where
mentioned in this chapter.
12.8
Summary
The principles of endodontic instrumentation and therapy are well established.
Thorough cleaning of the canal system to render it as free as possible of pulpal tissue, bacterial presence, and by-products, followed by complete obturation to prevent apical or coronal leakage creates an environment that promotes periradicular
healing. The philosophy of achieving a hermetic seal of the root apex has been
abandoned in favor of development of a fluid-tight antibacterial seal as a requirement for modern root canal sealers. The continuum of research and development of
materials and instruments will drive the continued development of new materials
for endodontic therapy.
References
Abbott, P.V., 1992. Systemic release of corticosteroids following intra-dental use. Int. Endod.
J. 25, 189 191.
Al-Haddad, A., Che Ab Aziz, Z.A., 2016. Bioceramic-based root canal sealers: a review. Int.
J. Biomater. 2016, 10.
Al-Hezaimi, K., Al-Tayar, B.A., Bajuaifer, Y.S., Salameh, Z., Al-Fouzan, K., Tay, F.R.,
2011. A hybrid approach to direct pulp capping by using emdogain with a capping material. J. Endod. 37, 667 672.
Allan, N.A., Walton, R.C., Schaeffer, M.A., 2001. Setting times for endodontic sealers under
clinical usage and in vitro conditions. J. Endod. 27, 421 423.
Ambard, A.J., Mueninghoff, L., 2006. Calcium phosphate cement: review of mechanical and
biological properties. J. Prosthodont. 15, 321 328.
American Association of Endodontists, 2012. Glossary of Endodontic Terms. American
Association of Endodontists, Chicago, IL.
294
Advanced Dental Biomaterials
Andelin, W.E., Shabahang, S., Wright, K., Torabinejad, M., 2003. Identification of hard tissue after experimental pulp capping using dentin sialoprotein (DSP) as a marker. J.
Endod. 29, 646 650.
Asgary, S., Eghbal, M.J., Fazlyab, M., Baghban, A.A., Ghoddusi, J., 2015. Five-year results
of vital pulp therapy in permanent molars with irreversible pulpitis: a non-inferiority
multicenter randomized clinical trial. Clin. Oral Investig. 19, 335 341.
Asgary, S., Eghbal, M.J., Parirokh, M., Torabzadeh, H., 2006. Sealing ability of three commercial mineral trioxide aggregates and an experimental root-end filling material. Iran
Endod J 1, 101 105.
Athanassiadis, B., Abbott, P.V., Walsh, L.J., 2007. The use of calcium hydroxide, antibiotics
and biocides as antimicrobial medicaments in endodontics. Aust. Dent. J. 52, S64 S82.
Augsburger, R.A., Peters, D.D., 1990. Radiographic evaluation of extruded obturation materials. J. Endod. 16, 492 497.
Basrani, B., Lemonie, C., 2005. Chlorhexidine gluconate. Aust. Endod. J. 31, 48 52.
Basrani, B., Santos, J.M., Tjaderhane, L., Grad, H., Gorduysus, O., Huang, J., et al., 2002.
Substantive antimicrobial activity in chlorhexidine-treated human root dentin. Oral Surg.
Oral Med. Oral Pathol. Oral Radiol. Endod. 94, 240 245.
Basrani, B., Tjaderhane, L., Santos, J.M., Pascon, E., Grad, H., Lawrence, H.P., et al., 2003.
Efficacy of chlorhexidine- and calcium hydroxide-containing medicaments against
Enterococcus faecalis in vitro. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod.
96, 618 624.
Basrani, B.R., Manek, S., Sodhi, R.N., Fillery, E., Manzur, A., 2007. Interaction between
sodium hypochlorite and chlorhexidine gluconate. J. Endod. 33, 966 969.
Baumgartner, G., Zehnder, M., Paque, F., 2007. Enterococcus faecalis type strain leakage
through root canals filled with gutta-percha/AH plus or Resilon/Epiphany. J. Endod. 33,
45 47.
Bettina, B., Markus, H., 2012. Update on endodontic irrigating solutions. Endod. Top. 27,
74 102.
Block, S.S., 2001. Disinfection, Sterilization, and Preservation. Lippincott Williams &
Wilkins.
Borges, A.H., Pedro, F.L., Semanoff-Segundo, A., Miranda, C.E., Pecora, J.D., Cruz Filho,
A.M., 2011. Radiopacity evaluation of Portland and MTA-based cements by digital
radiographic system. J. Appl. Oral. Sci. 19, 228 232.
Bouillaguet, S., Wataha, J.C., Tay, F.R., Brackett, M.G., Lockwood, P.E., 2006. Initial
in vitro biological response to contemporary endodontic sealers. J. Endod. 32, 989 992.
Brady, J.M., del Rio, C.E., 1975. Corrosion of endodontic silver cones in humans: a scanning
electron microscope and X-ray microprobe study. J. Endod. 1, 205 210.
Bystrom, A., Sundqvist, G., 1985. The antibacterial action of sodium hypochlorite and
EDTA in 60 cases of endodontic therapy. Int. Endod. J. 18, 35 40.
Camargo, S.E., Camargo, C.H., Hiller, K.A., Rode, S.M., Schweikl, H., Schmalz, G., 2009.
Cytotoxicity and genotoxicity of pulp capping materials in two cell lines. Int. Endod. J.
42, 227 237.
Camilleri, J., Montesin, F.E., Brady, K., Sweeney, R., Curtis, R.V., Ford, T.R., 2005. The
constitution of mineral trioxide aggregate. Dent. Mater. 21, 297 303.
Camilleri, J., Sorrentino, F., Damidot, D., 2015. Characterization of un-hydrated and hydrated
BioAggregate and MTA Angelus. Clin. Oral Investig. 19, 689 698.
Carrilho, M.R.O., Carvalho, R.M., de Goes, M.F., Di Hipólito, V., Geraldeli, S., Tay, F.R.,
et al., 2007. Chlorhexidine preserves dentin bond in vitro. J. Dent. Res. 86, 90 94.
Endodontic materials: from old materials to recent advances
295
Chen, H., Teixeira, F.B., Ritter, A.L., Levin, L., Trope, M., 2008. The effect of intracanal
anti-inflammatory medicaments on external root resorption of replanted dog teeth after
extended extra-oral dry time. Dent. Traumatol. 24, 74 78.
Cho, E., Kopel, H., White, S.N., 1995. Moisture susceptibility of resin-modified glass-ionomer materials. Quintessence Int. 26, 351 358.
Chong, B.S., Pitt Ford, T.R., 2005. Root-end filling materials: rationale and tissue response.
Endod. Top. 11, 114 130.
Crooks, W.G., Anderson, R.W., Powell, B.J., Kimbrough, W.F., 1994. Longitudinal evaluation of the seal of IRM root end fillings. J. Endod. 20, 250 252.
Dai, L., Khechen, K., Khan, S., Gillen, B., Loushine, B.A., Wimmer, C.E., et al., 2011. The
effect of QMix, an experimental antibacterial root canal irrigant, on removal of canal
wall smear layer and debris. J. Endod. 37, 80 84.
Davies, A., 1973. The mode of action of chlorhexidine. J. Periodontal Res. Suppl. 12,
68 75.
De Moor, R.J., De Bruyne, M.A., 2004. The long-term sealing ability of AH 26 and AH plus
used with three gutta-percha obturation techniques. Quintessence Int. 35, 326 331.
Desai, S., Chandler, N., 2009. Calcium hydroxide-based root canal sealers: a review. J.
Endod. 35, 475 480.
Dick, H.M., Carmichael, D.J., 1980. Reconstituted antigen-poor collagen preparations as
potential pulp-capping agents. J. Endod. 6, 641 644.
Dorn, S.O., Gartner, A.H., 1990. Retrograde filling materials: a retrospective success-failure
study of amalgam, EBA, and IRM. J. Endod. 16, 391 393.
Duarte, M.A., Demarchi, A.C., Yamashita, J.C., Kuga, M.C., Fraga Sde, C., 2003. pH and
calcium ion release of 2 root-end filling materials. Oral Surg. Oral Med. Oral Pathol.
Oral Radiol. Endod. 95, 345 347.
Emre, B., Mehtap, M., Mahmut, S., Tolga, G., 2008. The response of subcutaneous connective tissue to a new endodontic filling material. J. Biomed. Mater. Res. Part B Appl.
Biomater. 84B, 463 467.
Estrela, C., Estrela, C.R., Barbin, E.L., Spano, J.C., Marchesan, M.A., Pecora, J.D., 2002.
Mechanism of action of sodium hypochlorite. Braz. Dent. J. 13, 113 117.
Estrela, C., Estrada-Bernabe, P.F., Daniel de Almeida-Decurcio, D., Almeida-Silva, J.,
Rodrigues-Araujo-Estrela, C., Poli-Figueiredo, J.A., 2011. Microbial leakage of MTA,
Portland cement, Sealapex and zinc oxide-eugenol as root-end filling materials. Med.
Oral Patol. Oral Cir. Bucal. 16, e418 e424.
Ford, T.R., Torabinejad, M., Abedi, H.R., Bakland, L.K., Kariyawasam, S.P., 1996. Using mineral trioxide aggregate as a pulp-capping material. J. Am. Dent. Assoc. 127, 1491 1494.
Frank, A.L., 1966. Therapy for the divergent pulpless tooth by continued apical formation. J.
Am. Dent. Assoc. 72, 87 93.
Fridland, M., Rosado, R., 2003. Mineral trioxide aggregate (MTA) solubility and porosity
with different water-to-powder ratios. J. Endod. 29, 814 817.
Friedman, C.M., Sandrik, J.L., Heuer, M.A., Rapp, G.W., 1975. Composition and mechanical
properties of gutta-percha endodontic points. J. Dent. Res. 54, 921 925.
Friedman, S., Lost, C., Zarrabian, M., Trope, M., 1995. Evaluation of success and failure
after endodontic therapy using a glass ionomer cement sealer. J. Endod. 21, 384 390.
Giardino, L., Pecora, G., Ambu, E., Savoldi, E., 2005. A new irrigant in the treatment of apical periodontitis: from research to clinic. In: 12th Biennial Congress European Society
of Endodontology, Dublin. pp. 15 17.
Glass, R.L., Zander, H.A., 1949. Pulp healing. J. Dent. Res. 28, 97 107.
296
Advanced Dental Biomaterials
Goldman, M., Kronman, J.H., Goldman, L.B., Clausen, H., Grady, J., 1976. New method of
irrigation during endodontic treatment. J. Endod. 2, 257 260.
Goodman, A., Schilder, H., Aldrich, W., 1974. The thermomechanical properties of guttapercha: II. The history and molecular chemistry of gutta-percha. Oral Surg. Oral Med.
Oral Pathol. 37, 954 961.
Grawehr, M., Sener, B., Waltimo, T., Zehnder, M., 2003. Interactions of ethylenediamine tetraacetic acid with sodium hypochlorite in aqueous solutions. Int. Endod. J. 36,
411 417.
Grech, L., Mallia, B., Camilleri, J., 2013. Investigation of the physical properties of tricalcium silicate cement-based root-end filling materials. Dent. Mater. 29, e20 e28.
Greer, B.D., West, L.A., Liewehr, F.R., Pashley, D.H., 2001. Sealing ability of Dyract,
Geristore, IRM, and super-EBA as root-end filling materials. J. Endod. 27, 441 443.
Grigoratos, D., Knowles, J., Ng, Y.L., Gulabivala, K., 2001. Effect of exposing dentine to
sodium hypochlorite and calcium hydroxide on its flexural strength and elastic modulus.
Int. Endod. J. 34, 113 119.
Grossman, L.I., 1982. The effect of pH of rosin on setting time of root canal cements. J.
Endod. 8, 326 327.
Hand, R.E., Smith, M.L., Harrison, J.W., 1978. Analysis of the effect of dilution on the
necrotic tissue dissolution property of sodium hypochlorite. J. Endod. 4, 60 64.
Hartwell, G.R., England, M.C., 1993. Healing of furcation perforations in primate teeth after
repair with decalcified freeze-dried bone: a longitudinal study. J. Endod. 19, 357 361.
Hashem, A.A., Wanees Amin, S.A., 2012. The effect of acidity on dislodgment resistance of
mineral trioxide aggregate and bioaggregate in furcation perforations: an in vitro comparative study. J. Endod. 38, 245 249.
Hayashi, Y., Imai, M., Yanagiguchi, K., Viloria, I.L., Ikeda, T., 1999. Hydroxyapatite applied
as direct pulp capping medicine substitutes for osteodentin. J. Endod. 25, 225 229.
Heling, I., Chandler, N.P., 1996. The antimicrobial effect within dentinal tubules of four root
canal sealers. J. Endod. 22, 257 259.
Hulsmann, M., Heckendorff, M., Lennon, A., 2003. Chelating agents in root canal treatment:
mode of action and indications for their use. Int. Endod. J. 36, 810 830.
Jitaru, S., Hodisan, I., Timis, L., Lucian, A., Bud, M., 2016. The use of bioceramics in endodontics—literature review. Clujul Med. 89, 470 473.
Kaida, H., Hamachi, T., Anan, H., Maeda, K., 2008. Wound healing process of injured pulp
tissues with emdogain gel. J. Endod. 34, 26 30.
Kakani, A.K., Veeramachaneni, C., Majeti, C., Tummala, M., Khiyani, L., 2015. A review
on perforation repair materials. J. Clin. Diagn. Res. 9, ZE09 ZE13.
Kazemi, R.B., Safavi, K.E., Spangberg, L.S., 1993. Dimensional changes of endodontic sealers. Oral Surg. Oral Med. Oral Pathol. 76, 766 771.
Keskin, C., Demiryurek, E.O., Ozyurek, T., 2015. Color stabilities of calcium silicate-based
materials in contact with different irrigation solutions. J. Endod. 41, 409 411.
Kiatwateeratana, T., Kintarak, S., Piwat, S., Chankanka, O., Kamaolmatyakul, S., Thearmontree,
A., 2009. Partial pulpotomy on caries-free teeth using enamel matrix derivative or calcium
hydroxide: a randomized controlled trial. Int. Endod. J. 42, 584 592.
Kim, Y.K., Grandini, S., Ames, J.M., Gu, L.S., Kim, S.K., Pashley, D.H., et al., 2010.
Critical review on methacrylate resin-based root canal sealers. J. Endod. 36, 383 399.
Kleier, D.J., Averbach, R.E., 1988. Painful dysesthesia of the inferior alveolar nerve following use of a paraformaldehyde-containing root canal sealer. Dent. Traumatol. 4, 46 48.
Krastl, G., Allgayer, N., Lenherr, P., Filippi, A., Taneja, P., Weiger, R., 2013. Tooth discoloration induced by endodontic materials: a literature review. Dent. Traumatol. 29, 2 7.
Endodontic materials: from old materials to recent advances
297
Kratchman, S.I., 2004. Perforation repair and one-step apexification procedures. Dent. Clin.
North Am. 48, 291 307.
Lambrianidis, T., Margelos, J., Beltes, P., 1999. Removal efficiency of calcium hydroxide
dressing from the root canal. J. Endod. 25, 85 88.
Law, A.S., 2013. Considerations for regeneration procedures. J. Endod. 39, S44 S56.
Lewis, B.B., Chestner, S.B., 1981. Formaldehyde in dentistry: a review of mutagenic and carcinogenic potential. J. Am. Dent. Assoc. 103, 429 434.
Lianjia, Y., Yuhao, G., White, F.H., 1993. Bovine bone morphogenetic protein-induced dentinogenesis. Clin. Orthop. Relat. Res. 305 312.
Loh, A., O’Hoy, P., Tran, X., Charles, R., Hughes, A., Kubo, K., et al., 2004. Evidencebased assessment: evaluation of the formocresol versus ferric sulfate primary molar pulpotomy. Pediatr. Dent. 26, 401 409.
Lovato, K.F., Sedgley, C.M., 2011. Antibacterial activity of Endosequence Root Repair
Material and proroot MTA against clinical isolates of Enterococcus faecalis. J. Endod.
37, 1542 1546.
Lovschall, H., Fejerskov, O., Flyvbjerg, A., 2001. Pulp-capping with recombinant human
insulin-like growth factor I (rhIGF-I) in rat molars. Adv. Dent. Res. 15, 108 112.
Macedo, R., Verhaagen, B., Rivas, D.F., Versluis, M., Wesselink, P., van der Sluis, L., 2014.
Cavitation measurement during sonic and ultrasonic activated irrigation. J. Endod. 40,
580 583.
Margelos, J., Eliades, G., Verdelis, C., Palaghias, G., 1997. Interaction of calcium hydroxide with zinc oxide-eugenol type sealers: a potential clinical problem. J. Endod. 23,
43 48.
McWalter, G.M., El-Kafrawy, A.H., Mitchell, D.F., 1976. Long-term study of pulp capping
in monkeys with three agents. J. Am. Dent. Assoc. 93, 105 110.
Min, K.S., Park, H.J., Lee, S.K., Park, S.H., Hong, C.U., Kim, H.W., et al., 2008. Effect of
mineral trioxide aggregate on dentin bridge formation and expression of dentin sialoprotein and heme oxygenase-1 in human dental pulp. J. Endod. 34, 666 670.
Mohammadi, Z., 2008. Sodium hypochlorite in endodontics: an update review. Int. Dent. J.
58, 329 341.
Mohammadi, Z., Dummer, P.M., 2011. Properties and applications of calcium hydroxide in
endodontics and dental traumatology. Int. Endod. J. 44, 697 730.
Orstavik, D., Nordahl, I., Tibballs, J.E., 2001. Dimensional change following setting of root
canal sealer materials. Dent. Mater. 17, 512 519.
Parirokh, M., Torabinejad, M., 2010a. Mineral trioxide aggregate: a comprehensive literature
review—Part I: Chemical, physical, and antibacterial properties. J. Endod. 36, 16 27.
Parirokh, M., Torabinejad, M., 2010b. Mineral trioxide aggregate: a comprehensive literature
review—Part III: Clinical applications, drawbacks, and mechanism of action. J. Endod.
36, 400 413.
Parolia, A., Kundabala, M., Rao, N.N., Acharya, S.R., Agrawal, P., Mohan, M., et al., 2010.
A comparative histological analysis of human pulp following direct pulp capping with
propolis, mineral trioxide aggregate and Dycal. Aust. Dent. J. 55, 59 64.
Qureshi, A., Soujanya, E., Nandakumar, Pratapkumar, Sambashivarao, 2014. Recent
advances in pulp capping materials: an overview. J. Clin. Diagn. Res. 8, 316 321.
Raina, R., Loushine, R.J., Weller, R.N., Tay, F.R., Pashley, D.H., 2007. Evaluation of the
quality of the apical seal in Resilon/Epiphany and gutta-percha/AH Plus-filled root
canals by using a fluid filtration approach. J. Endod. 33, 944 947.
Rud, J., Munksgaard, E.C., Andreasen, J.O., Rud, V., 1991a. Retrograde root filling with
composite and a dentin-bonding agent. 2. Endod. Dent. Traumatol. 7, 126 131.
298
Advanced Dental Biomaterials
Rud, J., Munksgaard, E.C., Andreasen, J.O., Rud, V., Asmussen, E., 1991b. Retrograde root
filling with composite and a dentin-bonding agent. 1. Endod. Dent. Traumatol. 7,
118 125.
Safavi, K.E., Nichols, F.C., 1993. Effect of calcium hydroxide on bacterial lipopolysaccharide. J. Endod. 19, 76 78.
Safavi, K.E., Spangberg, L.S., Langeland, K., 1990. Root canal dentinal tubule disinfection.
J. Endod. 16, 207 210.
Scherer, W., Dragoo, M.R., 1995. New subgingival restorative procedures with Geristore
resin ionomer. Pract. Periodontics Aesthet. Dent. 7, 1 4.
Schroeder, A., 1975. Ledermix 1962—Ledermix today. Evaluation after 13 years of experience. Zahnarztl Prax 26, 195 196.
She, C.M., Cheung, G.S., Zhang, C.F., 2016. Long-term follow-up of a revascularized immature necrotic tooth evaluated by CBCT. Case Rep. Dent. 2016, 4982458.
Shipper, G., Orstavik, D., Teixeira, F.B., Trope, M., 2004. An evaluation of microbial leakage in roots filled with a thermoplastic synthetic polymer-based root canal filling material (Resilon). J. Endod. 30, 342 347.
Shrestha, A., Kishen, A., 2016. Antibacterial nanoparticles in endodontics: a review. J.
Endod. 42, 1417 1426.
Silva, G.A., Gava, E., Lanza, L.D., Estrela, C., Alves, J.B., 2013. Subclinical failures of
direct pulp capping of human teeth by using a dentin bonding system. J. Endod. 39,
182 189.
Siqueira JR., J.F., Batista, M.M., Fraga, R.C., de Uzeda, M., 1998. Antibacterial effects of
endodontic irrigants on black-pigmented Gram-negative anaerobes and facultative bacteria. J. Endod. 24, 414 416.
Siqueira Jr., J.F., Rocas, I.N., Favieri, A., Lima, K.C., 2000. Chemomechanical reduction of
the bacterial population in the root canal after instrumentation and irrigation with 1%,
2.5%, and 5.25% sodium hypochlorite. J. Endod. 26, 331 334.
Siren, E.K., Haapasalo, M.P., Waltimo, T.M., Orstavik, D., 2004. In vitro antibacterial effect
of calcium hydroxide combined with chlorhexidine or iodine potassium iodide on
Enterococcus faecalis. Eur. J. Oral Sci. 112, 326 331.
Smith, J.J., Wayman, B.E., 1986. An evaluation of the antimicrobial effectiveness of citric
acid as a root canal irrigant. J. Endod. 12, 54 58.
Spangberg, L., Engstrom, B., Langeland, K., 1973. Biologic effects of dental materials. 3.
Toxicity and antimicrobial effect of endodontic antiseptics in vitro. Oral Surg. Oral
Med. Oral Pathol. 36, 856 871.
Spangberg, L.S., Barbosa, S.V., Lavigne, G.D., 1993. AH 26 releases formaldehyde. J.
Endod. 19, 596 598.
Stojicic, S., Zivkovic, S., Qian, W., Zhang, H., Haapasalo, M., 2010. Tissue dissolution by
sodium hypochlorite: effect of concentration, temperature, agitation, and surfactant. J.
Endod. 36, 1558 1562.
Stojicic, S., Shen, Y., Qian, W., Johnson, B., Haapasalo, M., 2012. Antibacterial and smear
layer removal ability of a novel irrigant, QMiX. Int. Endod. J. 45, 363 371.
Tarim, B., Hafez, A.A., Cox, C.F., 1998. Pulpal response to a resin-modified glass-ionomer
material on nonexposed and exposed monkey pulps. Quintessence Int. 29, 535 542.
Tay, F.R., Pashley, D.H., 2007. Monoblocks in root canals—a hypothetical or a tangible
goal. J. Endod. 33, 391 398.
Torabinejad, M., Hong, C.U., Mcdonald, F., Pitt Ford, T.R., 1995. Physical and chemical
properties of a new root-end filling material. J. Endod. 21, 349 353.
Endodontic materials: from old materials to recent advances
299
Torabinejad, M., Khademi, A.A., Babagoli, J., Cho, Y., Johnson, W.B., Bozhilov, K., et al.,
2003. A new solution for the removal of the smear layer. J. Endod. 29, 170 175.
Walivaara, D.A., Abrahamsson, P., Samfors, K.A., Isaksson, S., 2009. Periapical surgery
using ultrasonic preparation and thermoplasticized gutta-percha with AH Plus sealer or
IRM as retrograde root-end fillings in 160 consecutive teeth: a prospective randomized
clinical study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108, 784 789.
Williams, S.S., Gutmann, J.L., 1996. Periradicular healing in response to Diaket root-end filling material with and without tricalcium phosphate. Int. Endod. J. 29, 84 92.
Windley III, W., Teixeira, F., Levin, L., Sigurdsson, A., Trope, M., 2005. Disinfection of
immature teeth with a triple antibiotic paste. J. Endod. 31, 439 443.
Yasuda, Y., Ogawa, M., Arakawa, T., Kadowaki, T., Saito, T., 2008. The effect of mineral
trioxide aggregate on the mineralization ability of rat dental pulp cells: an in vitro study.
J. Endod. 34, 1057 1060.
Yavari, H.R., Shahi, S., Rahimi, S., Shakouie, S., Roshangar, L., Mesgari Abassi, M., et al.,
2009. Connective tissue reaction to white and gray MTA mixed with distilled water or
chlorhexidine in rats. Iran. Endod. J. 4, 25 30.
Yazdi, P.M., Schou, S., Jensen, S.S., Stoltze, K., Kenrad, B., Sewerin, I., 2007. Dentinebonded resin composite (Retroplast) for root-end filling: a prospective clinical and
radiographic study with a mean follow-up period of 8 years. Int. Endod. J. 40, 493 503.
Zakariasen, K.L., Brayton, S.M., Collinson, D.M., 1990. Efficient and effective root canal
retreatment without chloroform. J. Can. Dent. Assoc. 56, 509 512.
Zehnder, M., 2006. Root canal irrigants. J. Endod. 32, 389 398.
Zehnder, M., Soderling, E., Salonen, J., Waltimo, T., 2004. Preliminary evaluation of bioactive glass S53P4 as an endodontic medication in vitro. J. Endod. 30, 220 224.
Zetterqvist, L., Hall, G., Holmlund, A., 1991. Apicectomy: a comparative clinical study of
amalgam and glass ionomer cement as apical sealants. Oral Surg. Oral Med. Oral
Pathol. 71, 489 491.
Zielinski, T.M., Baumgartner, J.C., Marshall, J.G., 2008. An evaluation of Guttaflow and
gutta-percha in the filling of lateral grooves and depressions. J. Endod. 34, 295 298.
Further reading
Guideline Pulp Therapy, 2016. Guideline on pulp therapy for primary and immature permanent teeth. Pediatr. Dent. 38, 280 288.
Chong, B.S., Pitt Ford, T.R., Watson, T.F., Wilson, R.F., 1995. Sealing ability of potential
retrograde root filling materials. Dent. Traumatol. 11, 264 269.
13
Fiber-reinforced composites
Daniel Varley1, Safiyya Yousaf1, Mansour Youseffi1,
Masoud Mozafari2,3, Zohaib Khurshid4 and Farshid Sefat5,6
1
Medical Engineering Department, Faculty of Engineering and Informatics, University of
Bradford, Bradford, United Kingdom, 2Bioengineering Research Group, Nanotechnology
and Advanced Materials Department, Materials and Energy Research Centre (MERC),
Tehran, Iran, 3Department of Tissue Engineering & Regenerative Medicine, Faculty of
Advanced Technologies in Medicine, Iran University of Medical Sciences (IUMS), Tehran,
Iran, 4Department of Prosthodontics and Dental Implantology, College of Dentistry, King
Faisal University, Al-Ahsa, Saudi Arabia, 5Interdisciplinary Research Centre in Polymer
Science & Technology (IRC Polymer), University of Bradford, Bradford, United Kingdom,
6
Biomedical and Electrical Engineering Department, School of Engineering, University of
Bradford, Bradford, United Kingdom
Chapter Outline
13.1 Introduction 302
13.2 Anatomy and physiology of teeth
13.2.1
13.2.2
13.2.3
13.2.4
13.2.5
302
Enamel 303
Dentin 303
Dental pulp 304
Cementum 304
Tooth development 304
13.3 Mechanical properties of teeth 305
13.4 Biomaterials used in dentistry 305
13.4.1 Metals 305
13.4.2 Ceramics 306
13.4.3 Composites 306
13.5 Fiber-reinforced composites
306
13.5.1 Fiber-reinforced composite composition 306
13.5.2 Influencing factors on mechanical properties 308
13.6 Clinical applications of fiber-reinforced composites
13.6.1
13.6.2
13.6.3
13.6.4
13.6.5
13.6.6
Tooth restoration 311
Implants 311
Endodontics 312
Prosthodontics 312
Orthodontic 312
Periodontal 312
13.7 Conclusion
313
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00013-X
Copyright © 2019 Elsevier Ltd. All rights reserved.
311
302
Advanced Dental Biomaterials
References 313
Further reading 315
13.1
Introduction
Dental application is constantly evolving as a result of innovative treatment solutions based on the development of new biomaterials, advancement in technologies,
and more successful treatment techniques, with fiber-reinforced composites (FRCs)
being a superb example of this. The use of fibers within composite materials has
greatly enhanced their uses in the field of dentistry, giving dentists more options
due to the many applications of this exciting group of materials.
A FRC is a combination of conventional dental composite and most commonly
glass fibers; this combination gives the same level of strength and flexibility that is
also found in boats, light aircraft, and F1 racing cars. FRCs consist of three components: (1) the matrix, this is usually made of resin and becomes a polymer after curing or polymerization. Additionally, it provides a place for the fibers to reside. (2)
The reinforcing constituent, which is fibers of high strength and modulus; these are
usually glass, carbon, or polyethylene fibers. (3) The fine interphase region, also
known as the interface; this is the key element of the composite as it transfers the
load from the matrix to the fibers (Zhandarov and Mäder, 2005). For many decades,
engineers have been using fibers as high aspect ratio fillers to construct materials/
devices with high levels of strength and fracture toughness. Hence, this is why these
materials are desirable in the field of dentistry (He et al., 2017).
FRCs have been the center of attention in dentistry for the last two decades
because of their excellent adhesion and esthetic appearance. They have provided
many clinical applications, such as fixed prosthodontics, restorative dentistry, periodontology orthodontics, and in repairs of prosthetic devices (Nagata et al., 2016).
13.2
Anatomy and physiology of teeth
Human tooth can be broken down into two anatomical parts. The root is the part
embedded within the jaw, as seen in Fig. 13.1. The purpose of the root is to anchor the
tooth within the bony socket of the jaw. The root of the tooth is not normally visible as
it is found below the cementoenamel junction and extends deep into the gingivae.
Additionally, the majority of the root is composed of dentin and contains pulp canals.
Figure 13.1 A diagram to show the structure of a fiber-reinforced composite.
Fiber-reinforced composites
303
Figure 13.2 An image showing the cross section of the tooth, including the various layers.
Also depicted in Fig. 13.2 is the second anatomical part, which is known as the
crown; this part of the tooth is above the cementoenamel junction and is visible
within the mouth. The crown is completely covered with enamel, which is
extremely hard and protects the tooth from the many stresses and strains faced on a
daily basis (Berkovitz et al., 2009).
A human tooth is very complex as it consists of various layers, each with different purposes and properties.
13.2.1 Enamel
As depicted in Fig. 13.2, enamel is the outermost layer of the human tooth.
Furthermore it is the hardest and most highly mineralized substance within the
human body, which allows it to cope with impact forces and shearing very well. One
very important property of enamel is that it has very high abrasion resistance; this
constitutes to wear being very slow. Unfortunately, if enamel is destroyed, the body
cannot repair or reproduce any more, and the reason behind this is that the enamel
does not contain any living cells, so it cannot regenerate (Berkovitz et al., 2009).
13.2.2 Dentin
Dentin, pale yellow in color, forms the bulk of the tooth and is a mineralized tissue;
it is usually covered by enamel on the crown, cementum on the root, and surrounds
the entire pulp. Dentin consists of a large quantity of small parallel tubules that lay
within a collagen matrix, which is highly mineralized. This structure provides
304
Advanced Dental Biomaterials
dentin with greater compressive, tensile, and flexural strength than enamel.
However, dentin is not as hard as enamel but is harder than bone and cementum.
Odontoblasts are responsible for forming the tissue, and the cell bodies of these
odontoblasts play a key role in lining the deep surface of dentin. The combination
of enamel and dentin provides a very hard and rigid structure that is perfect for tearing and masticating.
13.2.3 Dental pulp
Dental pulp is a specialized, unmineralized oral tissue, which is composed of soft
connective tissue, nervous, and vascular elements (Berkovitz et al., 2009). Pulp has
a soft gelatinous consistency and occupies the central pulp cavity of each tooth; the
main role is to form dentin of the tooth. In newly erupted teeth, the dental pulp is
large, but as teeth age the pulp cavity becomes more constricted, meaning the pulp
becomes progressively smaller (Nelson, 2014).
The mesenchymal tissue is characterized by the presence of odontoblasts, which
are the primary cells of dental pulp. Odontoblasts are extremely important as they
continuously lay down secondary dentin throughout life. Furthermore, these are
responsible for the production of tertiary reactionary dentin when the tooth comes
under minor insult or experiences dental caries (Nor, 2006).
13.2.4 Cementum
Cementum is the specialized thin layer of calcified tissue covering the dentin of the
root; its role is to help support the tooth within the jaw by attaching to collagen
fibers of the periodontal ligament. Unlike bone, cementum is not vascular and exhibits little turnover; it grows slowly by surface apposition, throughout life (Berkovitz
et al., 2009). Cementum, such as dentin, is also pale yellow in color with a dull surface. However, when compared, cementum is a lot softer and far more permeable
than dentin. Due to the softness and thinness of the tissue, it can be quite easily
removed by abrasion, hence for this reason, it is well protected.
13.2.5 Tooth development
There are three phases that sum up tooth development: initiation, morphogenesis,
and histogenesis. During initiation, there is an appearance of tooth germs along
the oral epithelium, and the sites of future teeth are established. It is during the
morphogenesis phase a that combination of cell movement and proliferation determines the shape of the tooth. Finally, during the histogenesis phase, the differentiation of cells proceed into fully formed dental tissues, both mineralized and
unmineralized. Additionally, tooth germs are categorized into three stages before
actual tooth eruption, these are the bud stage, cap stage, and bell stage and are
shown in Fig. 13.3.
Fiber-reinforced composites
305
Figure 13.3 An image showing the various stages of tooth development. (A) Thickening,
(B) bud, (C) cap, (D) bell and (E) erupted tooth.
13.3
Mechanical properties of teeth
The mechanical properties of teeth include hardness, elasticity, viscoelasticity, and
fracture behavior. Hardness is a measure of the hardness or softness of a material
and represents the ability of a solid material to resist plastic deformation, elastic
deformation, and destruction.
Elasticity is a term used to characterize how a material changes under an applied
external force and resumes after the force is removed. The elastic property parameters of human teeth include the shear modulus, elastic modulus, and Poisson’s
ratio. Viscoelasticity is the property of materials that exhibit both viscous and elastic characteristics when undergoing deformation.
13.4
Biomaterials used in dentistry
The field of dentistry is blessed with an ever-expanding number of biomaterials that
can be used for many different treatments and procedures. These biomaterials have
a diverse range of physical and mechanical properties and can be categorized into
three different sections:
13.4.1 Metals
G
G
G
G
Amalgam—Also commonly named filling, amalgam is a sealant made of small particles
of tin, copper, and silver allied with mercury. The mechanical properties and longevity of
this material made it the first choice for many years. On the other hand, this material does
have its flaws, it is not esthetically pleasing, and it contains mercury, which is poisonous
to humans.
Gold—In dentistry gold is found in the form of alloys. This material is ideal for posterior
prosthetic realizations due to its harmlessness, rigidity, and precision.
Titanium—This material is used most commonly in implantology due to its antiallergic
qualities.
Steel (chrome-cobalt)—Due to its high tensile strength, this material is used most commonly in removable prosthetics for frameworks and clasps.
306
Advanced Dental Biomaterials
13.4.2 Ceramics
Dental ceramics are materials that are part of systems designed with the purpose of
producing dental prostheses, which are used to replace damaged or missing dental
structures. Ceramics have a high compressive strength but low tensile strength,
meaning they are brittle and are likely to fracture under low strains (Shenoy and
Shenoy, 2010).
The different types of ceramics used in dentistry:
G
G
G
G
Glass-ceramics—A glass ceramic is a multiphase solid containing a residual glass phase
with a finely dispersed crystalline phase. Their size and growth rate are regulated by the
time and temperature of heat treatment.
Metal ceramics—A hybrid construction type where a porcelain covering encases a metal
substructure. These crowns can provide both good esthetics and strength. However, many
problems can occur due to the release of metallic ions into the gingival tissue.
Infiltrated ceramics—Infiltrated ceramics are formed through a process called slipcasting. This process gives the material greater strength and toughness and allows fewer
defects from processing. The three different infiltrated ceramics are spinel, alumina, and
zirconia.
Polycrystalline ceramics—Polycrystalline ceramics are formed from powders that can be
packed only to 70% of their theoretical density. An example of a polycrystalline ceramic
would be transformation-toughened zirconium oxide; this oxide can take three different
crystalline structures depending on temperature (Shenoy and Shenoy, 2010).
13.4.3 Composites
G
G
Composite resin—These are a type of synthetic material that consist of a resin matrix and
quartz or silica particles known as fillers. The most common matrixes used in dental composites are: bisphenol A-glycidyl methacrylate, urethane dimethacrylate, and triethylene
glycol dimethacrylate. The size of the filler determines the surface roughness of the composite, while the amount of filler increases the mechanical properties of the composite.
Glass ionomer cements—Glass ionomer cements are tooth-colored materials that bond
chemically to dental hard tissues and release fluoride for a relatively long period. These
tend to be the material of choice when restoring primary teeth.
13.5
Fiber-reinforced composites
13.5.1 Fiber-reinforced composite composition
13.5.1.1 Fiber types
The properties of a composite material are determined by the properties of the fiber
used to reinforce it. There are three types of fibers mainly used to reinforce composites in dentistry, these are glass, carbon, and polyethylene, and each of these reinforcing fibers give very diverse physical and mechanical properties to the finished
materials.
Fiber-reinforced composites
307
13.5.1.2 Glass
Glass fibers are the most common of all reinforcing fibers used commercially for
polymeric matrix composites (Ravindra et al., 1997). When toughness and tensile
strength must be maximized, glass fibers are the reinforcement of choice. The
recent innovations in glass fiber formulation allow strengths similar to that of carbon fibers (Stickel and Nagarajan, 2012).
The main advantages of glass fibers are low cost, high tensile strength, good
insulating properties, and high chemical resistance. While on the other hand, the
disadvantages associated with glass fibers are their low tensile modulus, low fatigue
resistance, as well as their high density and higher sensitivity to wear (Migliaresi
and Alexander, 2004; Ravindra et al., 1997).
Depending on the chemical composition of glass they are commercially available
in different grades.
1. Glass A—or Alkali glass was a common basic material for glass fiber production. This
glass is cheap and can be used as filler for plastics; however, with low chemical resistance
to water and low strength, this type of glass is not as desirable in the field of dentistry.
2. Glass C—or Chemical-resistant glass, these fibers have good corrosion resistance and are
used in the manufacturing of surfacing layers to provide additional chemical resistance
over E glass.
3. Glass E—or Electric glass is the most common type of glass fiber used in dentistry due to
its excellent electrical and mechanical properties. These fibers are characterized by their
ability to strongly resist attack by water. The main disadvantage of this grade is
unpredictable constituents such as fluorine.
4. Glass R—A reinforcement glass made with calcium aluminosilicates used where higher
strength and acid corrosion resistance is needed.
5. Glass S—This glass has high elasticity and strength. However, it is very expensive due to
its manufacturing processes. Glass S has very limited applications and is used mostly in
the aerospace industry.
13.5.1.3 Carbon
Carbon fibers were one of the early developments in composite reinforcement. In
1969, the first paper on the fabrication and characterization of an experimental
composite with a pure silica matrix reinforced with carbon fibers was published
(Boccaccini, 2005).
Carbon fiber is a material consisting of fibers around 5 10 µm in diameter and
composed mostly of carbon atoms. Carbon atoms are bonded together in crystals
that are aligned parallel to the long axis of the fiber. It is this crystal alignment that
gives the fiber high strength-to-volume ratio. Carbon fiber reinforced materials are
lightweight, very high in strength, and have good impact resistance. However, on
the other hand carbon fibers possess poor shear strength and when the material fractures fibers disintegrate making the results unpredictable.
Carbon fibers did not produce the best results for in vivo tests; in fact, many
patients that had been treated with carbon fiber reinforced biomaterial presented
308
Advanced Dental Biomaterials
with osteolysis (Migliaresi and Alexander, 2004), resulting in a number of products
being withdrawn from the market.
13.5.1.4 Polyethlene
Polyethylene is a very versatile material and has many applications in the field of
dentistry. The main use is to reinforce composites in a fiber form. Polyethylene
fibers are used due to them being highly esthetic when compared with cast metal or
metal mesh. Additionally, polyethylene fibers have high flexibility as well as being
thin and strong making them suitable to strengthen composites in large restorations.
Polyethylene fibers are recognized for having good biocompatibility and can be
surface treated to enhance resin bonding. However, most clinical cases using polyethylene fibers were short term. To enhance credibility, further clinical trials with
long-term results are required (Agrawal, 2014).
13.5.2 Influencing factors on mechanical properties
13.5.2.1 Fiber quantity
The number of fibers used to reinforce a material can have a significant effect on
the mechanical properties of that material. In general GFRCs have a high volume
fraction of fiber at around 60 vol.%, meanwhile in dentistry the fiber fraction is
kept relatively low, as the glass fiber should be covered with a layer of unfilled
polymer (Abdulmajeed et al., 2011).
Wear behavior of GFRC was investigated by Callaghan et al., what they found
was the specimen with 7.6 wt.% glass fibers had very little matrix and a cluster of
fibers due to possible overloading. High concentration of glass fibers can lead to
premature fiber fracture. To achieve the best wear resistance, bonding, and
decreased risk of fracture the amount of fibers should be between 2.0 and 7.6 wt.%
for the matrix (Callaghan et al., 2006).
13.5.2.2 Fiber distribution
The way fibers are distributed within a composite greatly influences the properties
of that material (Khan et al., 2015). Fibers that are evenly distributed tend to have a
positive effect on fatigue resistance, meaning it can withstand more cyclic stresses.
However, on the other hand, if the fibers are situated in one place then they can
cause the strength and Young’s modulus to increase (Narva, 2002). Fonseca et al.
(2014) found that fracture toughness, flexural strength, and compressive strength
were all higher when using randomly distributed short glass fibers.
13.5.2.3 Fiber orientation
As shown in Fig. 13.4, fibers can orientate perpendicular to each other, parallel to
each other, or randomly distributed. Unidirectional fibers are anisotropic, meaning
reinforcement is in one direction only, while bidirectional fibers are orthotropic and
Fiber-reinforced composites
309
Figure 13.4 A diagram to show the various orientations of fibers within a matrix; the arrows
represent the direction of force.
offer support in two directions. Randomly orientated short fibers provide an isotropic reinforcement in all directions. Unidirectional longitudinal FRCs are a lot stronger when the force is applied along the direction of the fiber; when a stress is
applied at an angle to the direction of the fibers, their strength reduces (Garoushi
et al., 2006).
Fiber orientation also plays a key role in adhesion to dentin and enamel.
Tezvergil et al. showed that randomly orientated fibers gave the highest shear bond
strength with enamel. However, on the other hand, it is bidirectional fibers that give
the highest shear bond strength to dentin (Tezvergil-Mutluay, 2017).
13.5.2.4 Fiber length
It is essential that stress transfers from the polymer matrix to the fibers, a key factor
for this to happen is to determine the length of the reinforcing fibers (Petersen,
2005). To ensure the stress is transferred between the fibers, the reinforcing fibers
length must be equal to or greater than the critical fiber length (Lc). When the
length of the fiber is much higher than Lc, it is known as continuous, and shorter
fibers are termed discontinuous. Fibers that are significantly shorter than Lc cause
the matrix to deform around the fibers, producing very little transference of stress
and virtually no reinforcement (Garoushi et al., 2007).
310
Advanced Dental Biomaterials
13.5.2.5 Adhesion of fibers to polymer matrix
Adhesion is defined as a molecular or atomic attraction between two contacting surfaces promoted by the interfacial force or attraction between the molecules or
atoms. Adhesion between matrix and fiber is of great importance as it affects the
strength of the material. If the adhesion was inadequate, the fibers would act as an
inclusion in the matrix, therefore weakening the composite (Khan et al., 2015).
Typically all glass fibers contain hydroxyl groups ( OH) on their surface, meaning that they potentially have good adhesion to resinous materials (Vallittu, 2017).
To help the adhesion process, fibers are chemically treated on their surface, this is
known as sizing. The process of sizing consists of fibers being coated with antistatic
compounds; there is a diverse blend of ingredients used in sizing, such as polymeric
components, a coupling agent, and a range of additives (Vallittu, 2017). Silane coupling agents are synthetic compounds and are mainly for surface modification
between two different materials. These bonds are created artificially and so not
occur naturally (Vallittu, 2017).
13.5.2.6 Impregnation of fibers with polymer matrix
Good contact of reinforcing fibers to the resin matrix is an essential requirement for
adhesion of fibers with the resin; therefore wetting of the surface of the fiber is
required (Vallittu, 1998). Resin impregnation relates to the surface wetting properties and viscosity of resin material. Poor impregnation creates voids between the
matrix and fiber resulting in decreased load-bearing capacity (Abdulmajeed et al.,
2011). Another additional problem with poor impregnation is it can lead to water
sorption, this is where water is allowed to enter through cracks and voids reducing
bond strength between matrix and fiber, leading to hydrolytic degradation (Khan
et al., 2015).
13.5.2.7 Water sorption
The effect of sorption and solubility may lead to adverse consequences in a dental
FRC. Over time, the absorption of water can lead to the decrease in mechanical
properties. The reason for this is a hydrolytic breakdown of the bond between fibers
and matrix or hydrolytic degradation of the fibers (Soderholm et al., 1984). It has
been found that the mechanical properties, such as wear resistance, flexural
strength, tensile strength, and modulus of elasticity, are all deleteriously affected by
water absorption (Soderholm and Roberts, 1990; Sideridou et al., 2003). The negative effect that water sorption has on mechanical properties of FRCs has raised concern about the shortened service life of these materials (Ferracane, 2006). Although
water sorption has many negative effects on the properties of FRC materials, it also
can have some positive effects. McCabe and Rusby (2004) found expansion caused
by water sorption can help to overcome stresses from polymerization shrinkage on
the restoration interphase.
Fiber-reinforced composites
311
13.5.2.8 Polymerization shrinkage
When polymerized, dental FRCs shrink due to a decrease in the distance between
the atoms as the monomers react to establish a covalent bond (Rueggeberg, 2002;
Schneider et al., 2010). This polymerization shrinkage creates contraction and internal stresses resulting in deformation in the surrounding tooth structure and, furthermore, a still poor marginal seal (Kleverlaan and Feilzer, 2005).
The curing reaction of dental resin composites often involves visible-light initiation of dimethacrylate monomers to form a highly cross-linked polymer. Higher
fiber volume fraction leads to a decrease in polymerization shrinkage (Puckett
et al., 2007). The problem of polymerization shrinkage and shrinkage stress is still
yet to be solved; however, alternative curing methods may be the answer.
13.6
Clinical applications of fiber-reinforced composites
FRCs are a group of relatively new materials, and due to this factor, their clinical
experience is limited. However, with fibers and matrix systems that are biocompatible, they have become biomaterials within dentistry. Additionally, these materials
possess great esthetics, corrosion resistance, no metal allergy response, and the ability to be handled chair-side (Khan et al., 2015).
The various clinical (dental) applications of FRCs are listed and explained here.
13.6.1 Tooth restoration
Someday it will likely be possible to culture cells from a patient and use them to
grow a new tooth to replace one they have lost. However, until then dentists are
required to use a number of artificial replacements for lost and missing teeth. FRCs
provide an amazing blend of strength, esthetics, and the least amount of drilling to
sound tooth tissue, making these materials an excellent candidate for tooth restoration. FRCs can be adapted by hand to connect teeth together, reinforce cracked
teeth, support crowns or bridges, and can be used as a direct filling (Butterworth
et al., 2003).
13.6.2 Implants
Implants are routinely restored with overdentures, fixed partial dentures, or hybrid
prostheses (Tayab and Shetty, 2015). However, standard metallic abutment has
proven unacceptable for hybrid prostheses due to limitations in bonding; hence,
FRC has become the common material of choice, as they can be bonded and
retained successfully due to excellent bonding properties (Bergendal et al., 1995).
312
Advanced Dental Biomaterials
13.6.3 Endodontics
FRC endodontic posts have been introduced to replace ceramics and metal alloys,
due to them having high tensile strength and similar rigidity and elasticity to that of
root dentin. This minimizes the risk of root fractures caused by tension peaks
induced by loading forces (Khan et al., 2015). Catastrophic collapse, which leads to
a fracture in the tooth root, is less likely in contrast to posts made from metal
(Mannocci et al., 1999).
13.6.4 Prosthodontics
Metal ceramic fixed partial dentures are a standard restoration for single-tooth
replacement in dental practice. For many years metal ceramic prostheses have provided an excellent record due to their strong and durable substructure; however, a
number of problems continue to arise regarding esthetics (Freilich et al., 1998).
FRCs have combatted the problems with esthetics, as the substructure is translucent
and requires no opaque masking. Various types of fibers may be used to strengthen
provisional partial dentures; however, a number of studies have shown glass fibers
are the most effective (Khan et al., 2015).
13.6.5 Orthodontic
As FRC’s success grows in other areas of dentistry, they are also gaining popularity
in the orthodontic area due to their use a space-maintaining device. Both glass and
polyethylene fibers have been used to produce unilateral fixed space maintainers
(Tayab and Shetty, 2015).
In this application, bonding and fracture characteristics are of great importance.
Subramaniam et al. found that FRC space maintainers demonstrated superior retention when compared with stainless steel band and loop maintainers after a 1-year
follow-up period of children aged 6 8 years (Tayab and Shetty, 2015;
Subramaniam et al., 2008).
13.6.6 Periodontal
A splint is defined as a rigid or flexible device that maintains a displaced or movable part in a position. Splints are used in the cases of periodontal disease; where
periodontal fibers are disorganized, resorption of bone and destruction of epithelial
cell attachment occur (Davies et al., 2001), resulting in teeth drift, and gingival
margins start to recede.
Due to excellent bonding properties, FRC materials are extremely common for
splinting periodontally mobile teeth. FRCs provide stabilization with no need for
extra tooth preparation as retention is accomplished by resin adhesion to etched
enamel (Freilich et al., 2002).
Fiber-reinforced composites
13.7
313
Conclusion
This chapter demonstrates the wide range of clinical applications that FRCs have in
the field of dentistry. As more research is carried out on FRCs, there will be a greater
understanding of these fascinating materials. I can be sure that the clinical applications in dentistry will expand further. In a generation where esthetics is paramount,
FRCs are becoming extremely popular and sought-after by patients. However, there
are still many questions to be answered about FRCs as well as barriers to overcome.
The literature has shown that FRCs have good mechanical properties; the problem is
that many factors can influence these properties, making it difficult for dental technicians to carry out high-quality treatments with long-term positive outcomes. It is
agreed by many that more long-term clinical trials are a necessity to answer the questions about the longevity of dental FRCs. These long-term trials would increase the
credibility of these new materials massively, as the literature has very few longitudinal cases that monitor the performance of FRC restorations.
References
Abdulmajeed, A.A., Narhi, T.O., Vallitu, P.K., Lassila, L.V., 2011. The effect of high fiber
fraction on some mechanical properties of unidirectional glass fibre-reinforced composite. Dent. Mater. 27, 313 321.
Agrawal, M., 2014. Applications of ultrahigh molecular weight polyethylene fibres in dentistry: a review article. J. Adv. Med. Dent. Sci. 2 (2), 95 99.
Bergendal, T., Ekstrand, K., Karlsson, U., 1995. Evaluation of implant supported carbon/
graphite fiber-reinforced poly(methyl methacrylate) prostheses. A longitudinal multicentre study. Clin. Oral Implants Res. 6, 246 253.
Berkovitz, B.K.B., Holland, G.R., Moxham, B.J., 2009. Oral Anatomy, Histology and
Embryology, fourth ed. Mosby Elsevier, London.
Boccaccini, A.R., 2005. Continuous fibre reinforced glass and glass-ceramic matrix composites. Handbook of Ceramic Composites. Springer US, pp. 461 484.
Butterworth, C., Ellakwa, A.E., Shortall, A., 2003. Fibre-reinforced composites in restorative
dentistry. Dent. Update 30 (2), 300 306.
Callaghan, J.D., Vaziri, A., Nayeb-Hashemi, H., 2006. Effect of fiber volume fraction and
length on the wear characteristics of glass fiber-reinforced dental composites. Dent.
Mater. 22, 84 93.
Davies, S.J., Gray, R.J., Linden, G.J., James, J.A., 2001. Occlusal considerations in periodontics. Br. Dent. J. 191, 597 604.
Ferracane, J.L., 2006. Hygroscopic and hydrolytic effects in dental polymer networks. Dent.
Mater. 22, 211 222.
Fonseca, R.B., de Paula, M.S., Favarao, I.N., Kasuya, A.V.B., de Almeida, L.N., Mendes, G.
A.M., et al., 2014. Reinforcement of dental methacrylate with glass fibre after heated
silane application. Biomed. Res. Int. 2014, 364398.
Freilich, M.A., Karmaker, A.C., Burstone, C.J., Goldberg, A.J., 1998. Development and clinical applications of a light-polymerized fibre-reinforced composite. J. Prosthet. Dent. 80
(3), 311 318.
314
Advanced Dental Biomaterials
Freilich, M.A., Meiers, J.C., Duncan, J.P., 2002. Clinical evaluation of fibre-reinforced fixed
bridges. J. Am. Dent. Assoc. 133, 1524 1534.
Garoushi, S.K., Lassila, L.V., Vallittu, P.K., 2006. Short fibre reinforced composite: the
effect of fibre length and volume fraction. J. Contemp. Dent. Pract. 7, 10 17.
He, J., Vallittu, P., Lassila, L.V., 2017. Preparation and characterization of high radio-opaque
E-glass fibre-reinforced composite with iodine containing methacrylate monomer. Dent.
Mater. 33 (2), 218 225.
Khan, A.S., Azam, M.T., Khan, M., Mia, S.A., Rheman, I.U., 2015. An update on glass fibre
dental restorative composites: a systematic review. Mater. Sci. Eng. C. 47 (1), 26 39.
Kleverlaan, C.J., Feilzer, A.J., 2005. Polymerization shrinkage and contraction stress of dental resin composites. Dent. Mater. 21 (12), 1150 1157.
Mannocci, F., Ferrari, M., Watson, T.F., 1999. Intermittent loading of teeth restored using
quartz fibre, carbon quartz fibre and zirconium dioxide ceramic root canal posts. J.
Adhes. Dent. 1, 153 158.
McCabe, J.F., Rusby, S., 2004. Water absorption, dimensional change and radial pressure in
resin matrix dental restorative materials. Biomaterials 25, 4001 4007.
Migliaresi, C., Alexander, H., 2004. Biomaterials Science, second ed. Academic Press, San
Diego, CA, pp. 181 197.
Nagata, K., Garoushi, S.K., Vallittu, P.K., Wakabayashi, N., Takahashi, H., Lassila, L.V.J.,
2016. Fracture behaviour of single-structure fibre-reinforced composite restorations.
Acta Biomater. Odontol. Scand. 2 (1), 118 124.
Narva, K., 2002. Clinical and laboratory findings reinforcing denture base acrylic. In: The
Third International Symposium on Fibre-Reinforced Plastics in Dentistry. pp. 113 124.
Nelson DDS, MS, S.J., 2014. Wheeler’s Dental Anatomy, Physiology, & Occlusion, 10th ed.
Elsevier, 31, 203.
Nor, J.E., 2006. Tooth regeneration in operative dentistry. Oper. Dent. 31, 633 642.
Petersen, R.C., 2005. Discontinuous fibre-reinforced composites above critical length. J.
Dent. Restor. 84, 365 370.
Ravindra, R., Mcilroy, P.J., Patel, S.A., 1997. Drugs that influence tubulin polymerization
modulate thyrotropin-releasing hormone receptor number in at T-20 cells. Pharmacol.
Toxicol. 80, 24 29.
Rueggeberg, F.A., 2002. From vulcanite to vinyl, a history of resins in restorative dentistry.
J. Prosthet. Dent. 87, 364 379.
Schneider, L.F., Cavalcante, L.M., Silikas, N., 2010. Shrinkage stresses generated during
resin-composite applications: a review. J. Dent. Biomech. 2010, 1 14.
Shenoy, A., Shenoy, N., 2010. Dental ceramics: an update. J. Conserv. Dent. 13 (4),
195 203.
Sideridou, I., Tserki, V., Papanastasiou, G., 2003. Study of water sorption, solubility and
modulus of elasticity of light-cured dimethacrylate-based dental resins. Biomaterials 23,
655 665.
Soderholm, K.J., Roberts, M.J., 1990. Influence of water exposure on the tensile strength of
composites. J. Dent. Res. 69, 1812 1816.
Soderholm, K.J., Zigan, M., Ragan, M., Fischlsweiger, W., Bergman, M., 1984. Hydrolytic
degradation of dental composites. J. Dent. Res. 63, 1248 1254.
Stickel, J.M., Nagarajan, M., 2012. Glass fiber-reinforced composites: from formulation to
application. Int. J. Appl. Glass Sci. 3 (2), 122 136.
Subramaniam, P., Babu, G.K., Sunny, R., 2008. Glass fibre reinforced composite resin as a
space maintainer. A clinical study. J. Indian Soc. Pedod. Prevent. Dent. 26 (Suppl 3),
S98 S103.
Fiber-reinforced composites
315
Tayab, T., Shetty, A., 2015. The clinical applications of fibber reinforced composites in all
specialties of dentistry an overview. Int. J. Compos. Mater. 5 (1), 18 24.
Tezvergil-Mutluay, A., 2017. Tooth as an adhesive substrate for fibre reinforced composites.
In: Clinical Guide to Principles of Fibre-Reinforced Composites in Dentistry, vol. 1.
Woodhead Publishing Series in Biomaterials, pp. 79 96.
Vallittu, P., 2017. Types of FRCs used in dentistry. In: Vallittu, P., Özcan, M. (Eds.),
Clinical Guide to Principles of Fiber-Reinforced Composites in Dentistry. Elsevier
Science & Technology, Cambridge, pp. 11 32.
Zhandarov, S., Mäder, E., 2005. Characterization of fibre/matrix interface strength: applicability of different tests, approaches and parameters. Compos. Sci. Technol. 65 (1),
149 160.
Further reading
Altair Enlighten, 2016. Fibre reinforced composites. ,https://altairenlighten.com/in-depth/
fiber-reinforced-composites/. (accessed 20.02.18.).
Dyer, S.R., Lassila, L.V., Jokinen, M., Vallittu, P.K., 2004. Effect of fibre position and orientation on fracture load of fibre-reinforced composite. Dent. Mater. 20, 947 955.
Tucker, A., Sharpe, P., 2004. The cutting-edge of mammalian development; how the embryo
makes teeth. Nat. Rev. Genet. 5 (7), 499 508.
Zhang, Y.R., Du, W., Zhou, X.D., Yu, H.Y., 2014. Review of research on the mechanical
properties of the human tooth. Int. J. Oral Sci. 6 (2), 61 69.
Zirconium in dentistry
14
Rafael Pino Vitti1,2, Anderson Catelan3, Marina Amaral1
and Rafael Rocha Pacheco4
1
Department of Dentistry, University of Taubaté, Taubaté, Brazil, 2Department of
Dentistry, Araras Dental School (FHO|UNIARARAS), Araras, Brazil, 3Faculty of Health
Sciences, University of Western São Paulo, Presidente Prudente, Brazil,
4
School of Dentistry, University of Detroit Mercy, Detroit, MI, United States
Chapter Outline
14.1 Introduction 317
14.2 Classification 321
14.2.1
14.2.2
14.2.3
14.2.4
14.2.5
Feldspathic ceramics 323
Leucite-based ceramics 323
Lithium disilicate based ceramics 323
Alumina-based ceramics 323
Zirconia-based ceramics 324
14.3
14.4
14.5
14.6
Zirconia in dentistry 324
Yttrium-stabilized tetragonal zirconia 326
Zirconia-toughened alumina 328
Surface topography, clinical treatments of zirconia surface, and adhesion
to zirconia in dental restorations 329
14.7 Failure and fractographic analysis of zirconia restorations 333
14.8 Mechanical testing of zirconia ceramics 335
14.9 Limitations and challenges 337
Further reading 338
14.1
Introduction
Restorative dentistry has always been an essential area in the dental field and has
grown recently due to higher esthetic demands from society. The term “restorative”
implies the act of performing a “restoration,” which can be defined by the action of
returning something to a former owner, place, or condition. In the dental field, a
“restoration” can be defined as a structure provided to replace or repair dental tissue
to restore its form and function. Each tooth is one individual organ formed by different tissues, with different properties. Hard tissues present in the dental structure,
such as enamel and dentin, also differ regarding properties such as mechanical,
physical. Clinicians have used many restorative materials as an attempt at “restoring” these original tooth properties, with extensive research and development.
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00014-1
Copyright © 2019 Elsevier Ltd. All rights reserved.
318
Advanced Dental Biomaterials
Restorative dental materials are usually classified as ceramics, polymers, composites, or metals. Ceramics are inorganic, nonmetallic materials widely used in different applications. Glass is a subset of ceramics, known by its elevated hardness
and translucency, properties that are similar to dental enamel. Due to these desired
properties, one of the first ceramics used in dentistry was the feldspathic ceramic, a
glass obtained from feldspar, one of the most common minerals present on earth.
These ceramics can be processed through traditional laboratorial condensation
methods followed by sintering. The sintering process is used to produce densitycontrolled materials by applying thermal energy, resulting, in this particular case, in
a glassy matrix containing leucite crystals. The amount and distribution of these
crystals can modify the mechanical and physical properties of the ceramic. An
increased content of leucite crystals can lead to increased flexural strength,
increased hardness, and increased thermal expansion. However, it also reduces
translucency. Due to its low flexural strength, the use of feldspathic ceramic is limited to areas with lower stress incidences. Furthermore, these materials can be processed through pressing or milling methods. Due to the low flexural strength
(approximately 65 MPa) observed for feldspathic ceramics, the indications for these
materials are limited to laminates, and veneering of infrastructure/frameworks.
Contrarily to the feldspathic ceramic, metals are known to present increased ductility/malleability, resulting in increased plastic strain and, consequently, increased
toughness. The association of feldspathic ceramics to different alloys results in fullcoverage restorations with increased flexural strength and indications for higher
load bearing regions. The porcelain fused to metal (PFM) restorations represented
an important moment in dentistry since the range of procedures where ceramics
could be used were significantly increased. A metallic core (made with specific
alloys) is created by using the well-established lost-wax technique with room for
the feldspathic ceramic to be applied later. The compatibility of physical properties
between alloy and ceramic is essential for a successful restoration. The fusion temperature for the ceramic cannot be higher than the melting temperature of the alloy.
In addition, differences in the coefficient of thermal expansion could lead to stress
concentrations and future failure of the restoration. The crystalline portion of the
ceramic determines the coefficient of thermal expansion and mechanical properties,
allowing the properties to be manipulated in such a way that these materials are
compatible with the selected alloy. The feldspathic ceramic is applied to the pretreated surface of the alloy and, after sintering, both materials are intimately bonded
by the mechanical retention caused by the interpenetration of the ceramic in the
micromechanical retentions of the alloy surface, chemical bonds between ceramic
and metallic oxides on the surface of the alloy, and stresses caused by the shrinkage
of the ceramic during cooling. This intimate contact allows increased stress distribution from the ceramic to the metallic core. PFMs can be indicated for full crown
procedures, fixed dental prosthesis (FPD), and are still extensively used in dentistry,
especially for the restoration of implants.
However, the metallic core of PFMs can lead to reduced esthetic properties
due to the reduced translucency of the alloy (when compared to the ceramic and
dental structure) and limitations caused by the metallic appearance of the core.
Zirconium in dentistry
319
Furthermore, with time, there is the possibility of exposure of cementing line and
corrosion of the alloy which could result in increased concerns regarding esthetics.
Due to the previously mentioned constant growing esthetic demand, there was the
need for restorations that would match the shade of the dental element regarding all
color parameters (hue, chroma, and value). Value is significantly affected by the
translucency of the restorative material; thus the metallic core can negatively affect
the final restoration aspect. As an attempt to remove the metallic core without
impacting the mechanical properties, dental ceramics were reinforced by an
increased crystalline content, resulting in metal-free restorations.
An increased leucite content leads to higher flexural strength (160 MPa) increasing the range of indications when compared to feldspathic ceramic: veneers, laminates, full anterior crowns, anterior full crown infrastructure, inlays, and onlays.
Leucite-reinforced ceramics are considered glass-ceramics and can be processed by
conventional condensation methods (also used for PFMs), pressed, or milled. There
are limitations for the incorporation of leucite crystals, which impacts the strength
and esthetics of the ceramic. For a ceramic to be considered as leucite reinforced, it
needs to contain leucite at a volume of at least 35%. The incorporation of different
crystals, such as lithium disilicate, allowed a new perspective on the research and
development of dental ceramics. This crystal, in particular, resulted in a type of
reinforced glass-ceramic with increased flexural strength (350 MPa), when compared to other glass-ceramics, with excellent esthetic properties and adhesive potential. These properties increased the number of indications for this material
including, but not limited to veneers, laminates, full anterior crowns, anterior full
crown infrastructure, posterior full crowns, posterior full crown infrastructure,
crowns over implants, abutments, inlays, onlays, and up to three-element FPD.
Lithium disilicate reinforced ceramics contain, approximately, 70% of lithium
disilicate crystals in their composition and can be processed through pressing methods and are also available as CAD/CAM (computer-assisted design/computerassisted manufacturing) blocks. These blocks can be found presintered or fully sintered. A great advantage for glass-ceramics over other restorative materials is the
possibility of being subjected to surface treatments, allowing the modification of
the surface regarding surface area and energy, and the possibility of silanization.
Silane is a bifunctional molecule (silanol and methacrylate groups) that creates a
link between silica and the polymeric matrix of resin-based materials, such as adhesive systems and resin cements.
The modern practice of dentistry is based on a conservative approach, usually
referred to as minimally invasive dentistry, which tends to preserve as much sound
dental structure as possible. The introduction of adhesive dentistry allowed clinicians to perform minimally invasive procedures by bonding these glass-ceramics to
the dental tissues. However, due to the brittle nature of glass-ceramics (lack of
deformation before fracture), preparations for these restorations can result in
increased amount of reduction of the dental structure, in order to provide adequate
thickness for the restorative material and, consequently, increased mechanical strength.
The selection of a glass-ceramic as the restorative material for a full-coverage
crown would require a minimal thickness for the restoration of, approximately,
320
Advanced Dental Biomaterials
1.5 mm, whereas for metallic restorations the minimal thickness is of 0.5 mm. The
option for a metallic crown could result in minimal reduction of the dental structure, however, without the esthetics required for anterior procedures and the disadvantage of not bonding these materials to the tooth structure.
Polycrystalline ceramics have been used as an attempt to replace the metallic
structures without drastically reducing the flexural strength. White metallic oxides
such as alumina (aluminum oxide) and zirconia (zirconium oxide) have been used
as crystals in ceramics that are fabricated through processing methods of slipcasting and/or milling. These materials present a reduced (to none) volume of glass,
resulting in elevated flexural strength. However, due to its nature and morphology,
these materials demonstrate reduced translucency and increased hardness, when
compared to any glass-ceramic. Alumina (aluminum oxide) is commonly used in
dentistry as an abrasive due to its high elastic modulus (300 GPa). Alumina-based
ceramics contain approximately 99.5% of alumina crystals. The reduced volume of
glass (or the absence of) leads to a high elastic modulus and reduced translucency.
Due to that fact, these ceramics require veneering and are not acid sensitive, which
represents a limitation regarding adhesion. The indication of this material is limited
to infrastructures for the crown and three elements anterior bridge (requires veneering). The traditional processing method used for this ceramic is through slipcasting, which is a time-consuming and technique-sensitive procedure, yet some
blocks are available for CAD/CAM. The development of new materials and technologies, added to the limitations of alumina-based materials, has reduced the use
of these materials.
One particular polycrystalline ceramic has drawn interest due to the potential of
combining the minimal reduction with acceptable esthetic properties. Due to its
composition and morphological structure, which will be discussed further in this
chapter, zirconia tends to demonstrate increased mechanical properties when compared to any other ceramic. The increased flexural strength and, consequently, fracture toughness allow the restorations to be fabricated with reduced thickness. Thus
preparations do not require as much reduction as the ones for glass-ceramics.
Higher flexural strength also allows this material to replace the metallic core of
PFM crowns, creating a new type of restoration named as porcelain fused to zirconia (PFZ). The mechanical properties of zirconia lead to a wide range of indications
including, but not limited to PFZ core, monolithic crown, FPD frameworks,
implants, implant abutments, and dentures. However, the properties observed for
zirconia are not necessarily similar to the ones of dental tissues (flexural strength,
translucency, and hardness). The absence of glass on the composition also makes
bonding to these materials a challenge. Modifications have been made to obtain
optimal properties, such as the association of zirconia to other types of ceramics,
such as alumina-toughened zirconia (ATZ) or zirconia-toughened alumina (ZTA).
One example of ATZ ceramic ( . 50% of zirconia crystals) is the combination of
67.9% of ZrO2, 21.5% Al2O3, 19.6% CeO2, 0.06% MgO, and 0.03% TiO.
Recently, promising new types of glass-ceramics have been released to the dental market as an attempt at overcoming the limitations of lithium disilicate based
ceramics and reducing milling/processing time. Both classes of materials include
Zirconium in dentistry
321
Figure 14.1 Fully crystallized glass-ceramic milling block.
Table 14.1 Classification of dental ceramics according to fusion temperature and
indications.
Classification
Fusion
temperature ( C)
Indications
High fusing
.1300
Medium
fusing
Low fusing
Ultralow
fusing
1101 1300
Denture teeth, and fully sintered alumina and
zirconia core ceramics
Denture teeth and presintered zirconia
850 1100
,850
Crown and bridge veneering
Crown and bridge veneering
addition zirconia or alumina to the crystalline portion of lithium silicate-based ceramics (Fig. 14.1). The constant development and advancements in CAD/CAM technology and its applications in dentistry have increased the need for new restorative
materials. Resin-based CAD/CAM blocks with increased inorganic content have
been introduced in the dental field as an alternative to the ceramic blocks, named as
resin-matrix ceramics (nanoceramics).
14.2
Classification
Dental ceramics can be classified according to the volume and composition of crystalline content, and fabrication methods, including fusion temperature (Table 14.1).
In terms of crystalline content (Fig. 14.2), there are, essentially, predominantly
glass or polycrystalline ceramics. The third type of ceramic in that classification
would be the so-called glass-infiltrated ceramics which are processed through the
slip-casting technique. As the name already describes, these ceramics (usually
322
Advanced Dental Biomaterials
Figure 14.2 Classification of dental ceramics according to crystalline content.
Figure 14.3 Classification of dental ceramics according to the composition.
alumina-based) are, basically, a porous crystalline structure interpenetrated by the
glass. Predominantly glass-ceramics are considered acid-sensitive since its surface
can be modified by etching procedures using hydrofluoric acid, while polycrystalline ceramics are considered acid resistant. The acid interacts with the silica on the
surface of the ceramic, promoting an increase in the surface area and, consequently,
surface energy. Furthermore, the silanol group present on the silane molecule bonds
chemically to the silica present on the ceramic surface, while the methacrylate
group is free to bond to other dental polymeric materials, creating a link between
the ceramic and adhesive system/resin cement.
Dental ceramics vary in terms of composition (Fig. 14.3), especially regarding
their crystalline content. Feldspathic ceramic is a predominantly glass-ceramic
(K2O Al2O3 6SiO2) used mostly for restoring enamel tissue, due to its optical
properties, and veneering of infrastructures and frameworks. For processing metalfree restorations, these ceramics needed to be reinforced by an increased crystalline
content, resulting in higher flexural strength. The reinforced ceramics can be
divided by the type of crystal used in their composition which can be, mainly,
leucite (K2O Al2O3 4SiO2), lithium disilicate (Li2O 2SiO2), alumina (Al2O3), or
zirconia (ZrO2).
Zirconium in dentistry
323
14.2.1 Feldspathic ceramics
14.2.1.1 Commercial examples
G
G
G
Condensation: VITAVM 7 (Vita Zahnfabrik); VITAVM 9 (Vita Zahnfabrik); VITAVM
11 (Vita Zahnfabrik); VITAVM 13 (Vita Zahnfabrik); VITAVM 15 (Vita Zahnfabrik);
VITA VMK Master (Vita Zahnfabrik); IPS e.max Ceram (Ivoclar Vivadent); Ceramco
(Dentsply); CERABIEN ZR (Noritake); Super Porcelain EX-3 (Noritake); Cercon Ceram
Kiss (Dentsply); Lava Ceram (3M ESPE)
Pressing: IPS e.max ZirPress (Ivoclar Vivadent); VITAPM 9 (Vita Zahnfabrik);
CERABIEN ZR PRESS (Noritake); Super Porcelain EX-3 PRESS (Noritake); Cercon
Ceram Press (Dentsply)
Milling: VITABLOCS TriLuxe forte (Vita Zahnfabrik); VITABLOCS RealLife (Vita
Zahnfabrik); VITABLOCS Mark II (Vita Zahnfabrik); VITABLOCS Esthetic Line
(Vita Zahnfabrik); CEREC Blocs C (Dentsply Sirona)
14.2.2 Leucite-based ceramics
14.2.2.1 Commercial examples
G
G
G
Condensation: IPS Empress Esthetic Veneer (Ivoclar Vivadent); IPS Empress In-Line
(Ivoclar Vivadent); Fortress (Mirage Dental Systems); IPS d.SIGN (Ivoclar Vivadent),
Avanté Micro Crystal (Pentron)
Pressing: IPS Empress Esthetic (Ivoclar Vivadent); Cergo Kiss (DeguDent); Ceramco iC
(Dentsply)
Milling: IPS Empress CAD (Ivoclar Vivadent); Paradigm C (3M ESPE); Kavo Everest
G-Blank (KaVo); Rosetta BM (HASS)
14.2.3 Lithium disilicate based ceramics
14.2.3.1 Commercial examples
G
G
Pressing: IPS e.max PRESS (Ivoclar Vivadent); Suprême.press (Axsys); Amber Press
(HASS); Rosetta SP (HASS); Amber Li-Si-POZ (HASS)
Milling: IPS e.max CAD (Ivoclar Vivadent); Suprême.cad (Axsys); Amber Mill (HASS);
Rosetta SM (HASS).
Lithium aluminosilicate reinforced with lithium disilicate: n!ce (Straumann)
Zirconia-reinforced lithium silicate: Suprinity (VITA Zahnfabrik); Celtra Duo
(Dentsply Sirona)
G
G
14.2.4 Alumina-based ceramics
14.2.4.1 Commercial examples
G
G
Slip-cast technique: VITA In-Ceram ALUMINA (Vita Zahnfabrik); VITA In-Ceram
SPINELL (Vita Zahnfabrik)
Milling: VITA In-Ceram ALUMINA for inLab (Vita Zahnfabrik); Procera AllCeram
(Nobel Biocare)
324
Advanced Dental Biomaterials
14.2.5 Zirconia-based ceramics
14.2.5.1 Commercial examples
G
Milling: VITA YZ XT (Vita Zahnfabrik); VITA YZ ST (Vita Zahnfabrik); VITA YZ HT
(Vita Zahnfabrik); VITA YZ T (Vita Zahnfabrik); AxZir HT Zr (Axsys); AxZir ST Zr
(Axsys); AxZir TT Zr (Axsys); Zirtooth (HASS); NobelProcera (Nobel Biocare); Cercon
(Dentsply Sirona); Celtra Duo (Dentsply Sirona); Zerion (Straumann); Zolid (Straumann);
IPS e.max ZirCAD (Ivoclar Vivadent)
14.3
Zirconia in dentistry
The zirconia is a biomaterial used in biomedical applications since the 1960s.
Among the dental ceramics, zirconia or zirconium dioxide (ZrO2) has approximately 96% 99% crystalline content with no glassy phase, presenting high physicochemical properties, such as flexural strength, fracture toughness, and hardness,
increased mechanical properties, excellent biocompatibility, and satisfactory
esthetic, thus expanding its application considerably in dentistry.
Due to the increasing interest in esthetics and concerns about cytotoxicity and
allergic reactions to certain metals, patients and dentists have been looking for
metal-free restorations. Although there are many types of zirconia-based ceramic
systems available, currently only two types are commonly used in dentistry:
yttrium-stabilized tetragonal zirconia (Y-TZP) and ZTA.
Zirconia structures used in dentistry treatments are fabricated using CAD/CAM
in two different methods. In one method, the fully sintered block of zirconia is
milled, and no distortion (shrinkage) occurred in the final structure. The main disadvantage is the wear promoted by burrs and, consequently, flaws produced during
the machining that can compromise the mechanical property of the zirconia structure. The other method consists of milling the zirconia structure from a presintered
block. In this method, the final mechanical property is reached after the sintering
process, and the structural shrinkage can be partly compensated at the drawing
phase improving the fit of the zirconia restoration.
The zirconia can be used as base material for feldspathic ceramic (porcelain)
restorations where the zirconia core structure is layered with porcelain and is
mainly used for anterior teeth. Full zirconia restorations are used in posterior teeth
where no esthetic porcelain layered on top is necessary. The bond strength of layered PFZ is critical. Thus crowns and bridges may be entirely constructed of the
zirconia ceramic in situations where esthetic demands are not extremely high.
Zirconium (Zr) is a solid metal with similar physicochemical properties to titanium. Thus zirconia also can be used in dental implants as abutments attached to
the implants, and it provides some advantages over alumina in order to solve the
problem of brittleness and the potential failure of implants. It is important to point
out that the fatigue performance of zirconia abutments is dependent on its abutment
diameter.
Zirconium in dentistry
325
However, the clinical success of zirconia implants is also dependent of the feldspathic ceramic survival. The long-term stability of the zirconia implant is questionable because the implant failures are related with zirconia fractures, which can
occur through laboratory technical complications, and/or feldspathic veneering ceramics fractures. Recently, a single body implant in zirconia (monotype zirconia
implant) was also developed. In this way, an entire implant reconstruction will be
metal free. Titanium implants are widely used in implants treatment, but their disadvantages (unwanted chemical biological interactions with the surrounding soft
and hard tissues and discoloration) can promote unsatisfying esthetical results,
mainly in patients with thinner mucosal biotype, gingival recession, or high smile
line. However, there are limited studies about zirconia in dental implants. Thus the
clinical success rate of these devices is not entirely known. Table 14.2 shows all
dental applications where the zirconia can be utilized.
For restorations of endodontically treated anterior teeth, metallic posts may result
in unfavorable esthetic results, such as a gray discoloration of ceramic crowns and
the surrounding gingival margin. Further, corrosive reactions with prefabricated
posts may cause complications involving the surrounding tissues. These concerns
promoted the development of esthetic posts made of zirconia and other ceramic
materials. Besides esthetic properties, some studies demonstrated that the zirconia
posts have higher mechanical strength than those reported for other types of
ceramic posts. In addition, zirconia posts also possess some advantages with respect
to biocompatibility but present some limitations, such as stiffness and low ductility.
Thus dentists found difficulties in roots with small sizes and in root canal retreatment procedures.
The esthetic orthodontic brackets can be manufactured using zirconia. As mentioned above, zirconia brackets are also another option to alumina ceramic brackets,
because they have the greatest toughness among all polycrystalline ceramics.
Moreover, in general zirconia brackets are cheaper than alumina ceramic brackets.
However, zirconia has high opacity making the orthodontic brackets less esthetically
pleasing. Studies show no differences regarding frictional properties between zirconia
and alumina brackets, but higher sliding properties have been reported for zirconia
brackets over both stainless steel and nickel titanium archwires with reduced plaque
adhesion, besides of the clinically acceptable bracket-tooth bond strength.
Table 14.2 Zirconia in dentistry.
Materials/procedures
Abutments
Composite resins
Cores
Crows (full and partial)
Implants
Orthodontic brackets
Posts
Veneers
326
14.4
Advanced Dental Biomaterials
Yttrium-stabilized tetragonal zirconia
Zirconia is obtained by minerals such as baddeleyite and zircon (ZrSIO4), and it has
both basic and acidic chemical properties. Unalloyed zirconia is a polymorph that
assumes three crystallographic forms depending on the temperature: monoclinic
(warped prism with parallelepiped borders), tetragonal (straight prism with rectangular borders), and cubic (straight prism with squares borders). The zirconia has a
monoclinic crystalline structure at room temperature and is stable up to 1170 C. In
this form, the zirconia shows reduced mechanical properties as well as cohesive
strength (low density). Between 1170 C and 2370 C the zirconia has a tetragonal
structure and allows a ceramic with improved mechanical properties. Above 2370 C,
the zirconia crystals have a cubic shape with intermediate mechanical properties.
The zirconium oxide can be stabilized with the addition of approximately
2 3 mol.% of yttrium oxide (Y2O3). After its processing, during the cooling, the
tetragonal phase again becomes monoclinic, and this transformation results in a substantial volume expansion of approximately 3% 4.5%. Zirconia exposure to water
and humidity also triggers spontaneous phase transformation, creating residual compression stress even without mechanical surface change or load application. However,
the tetragonal phase at room temperature may be stabilized by oxides such as calcium, magnesium, cerium, and yttrium, controlling crystal phase transformation. Thus
yttrium oxide is added to zirconia in order to maintain a metastable phase at temperatures below the tetragonal-to-monoclinic transformation temperature, creating a fully
tetragonal zirconia ceramic made of small metastable tetragonal grains (Y-TZP).
This procedure depends on the processing temperature, the yttrium oxide content, and the grain size, and it improves the mechanical strength of the zirconia,
because when the Y-TZP is induced by tensions that initiate the propagation of a
crack, the tetragonal crystals close to the crack become the stable monoclinic phase
(Fig. 14.4). The metastable phase exhibits good crack propagation resistance since
it is associated with a volume expansion of 3% 5% of the particles that cause
stresses of compression that oppose the growth and propagation of the crack. Thus
extra energy is required in order to propagate the crack. Biomedical applications
are focused in Y-TZP characterized by the addition of approximately 2 3 mol.% of
yttrium oxide tetragonal fine-grained microstructures. For this reason, Y-TZP has
physicochemical properties of great interest to dentistry, such as high strength, fracture toughness, hardness, high frictional behavior, wear and corrosion resistance,
and low thermal conductivity (Table 14.3).
Besides the physicochemical properties, Y-TZP is a chemically inert material
and no negative reactions (cytotoxic, oncogenic, or mutagenic effects) in biological
tissue have been reported. Several studies demonstrated the high biocompatibility
of Y-TZP with cytotoxicity results similar to alumina and lower than titanium dioxide. The improved biocompatibility of Y-TZP implants is due to strong bone
response and low bacterial colonization. Furthermore, the Y-TZP implants present
long-term osseointegration stability without biomechanical problems as well as titanium ones.
Zirconium in dentistry
327
Figure 14.4 Tetragonal monoclinic transformation phase during crack propagation.
Table 14.3 Physicochemical, electrical, and thermal properties of yttrium-stabilized
tetragonal zirconia.
Properties
Mean values
Properties
Mean values
Compressive strength
Density
Dielectric constant
Elastic modulus
Flexural strength
Fracture toughness
Latent heat of fusion
Melting point
4900 MPa
6.05 g/cm3
16.5
200 GPa
900 1600 MPa
9.5 MPa/m
760 kJ/kg
2625 C
0.27
3.16 3 1027 Ω m
600 MPa
2.1 2.2
70 GPa
413 MPa
2 W/m K
11 3 1026
Porosity
,0.05%
Poisson’s ratio
Resistivity
Rupture modulus
Refractive index
Shear strength
Tensile strength
Thermal conductivity
Thermal expansion
coefficient
Vickers hardness
1200 kgf/mm2
The optical property is another important factor to be considered in dental restoration manufacturing. Y-TZP has a high refractive index, high opacity, and low
absorption coefficient (Table 14.3). The Y-TZP transmission coefficient
(400 700 nm wavelengths) is higher than alumina and ZTA ceramics, but lower
than densely sintered alumina and lithium disilicate ceramics. Y-TZP contains a
highly crystalline phase; this fact confers opacity of the indirect restoration; since
being a white material it needs to be veneered most often with porcelain-based
esthetic ceramics, serving as prosthesis infrastructure. The high opacity is useful in
328
Advanced Dental Biomaterials
some clinical situations, such as masking abutment teeth or metallic posts/cores.
The Y-TZP opaque effect is predicated on dispersed particles slightly greater in
size than the wavelength of light. Thus the size of the crystalline grain is the microstructural characteristic more closely related to the adjustment of opacity of Y-TZP
ceramics. Lager grains lead to a smaller number of grain borders, decreasing light
scattering, but larger grains are harmful to mechanical properties and the stability
of the tetragonal phase of Y-TZP. Therefore the adjustment of the Y-TZP opacity
could not be obtained by increasing its grain size. Moreover, the Y-TZP tetragonal
phase has different refractive indexes according to its crystallographic orientation in
the microstructure. This anisotropic behavior is related to different refractive
indexes and causes significant light scattering (birefringence phenomenon).
Increased esthetic properties of zirconia by sintering temperature change and
fabricating processes were previously reported, mainly its translucency. In this
same way, monolithic zirconia appears as a good alternative for clinical use, showing excellent mechanical properties, even at minimum thicknesses, and adequate
translucency, and avoiding delamination and chipping failures of the porcelain layer
due to poor bonding between the zirconia framework and the veneering porcelain.
Some manufacturers introduce different zirconia colors to better esthetic outcomes of the white shade zirconia frameworks, which can be further esthetically
customized by veneering with feldspathic ceramic using layering or pressing techniques. Both methods require some sort of feldspathic ceramic for zirconia bonding.
Several studies show some chemical elements which may contribute to this bonding. Recently, among polycrystalline ceramics, Y-TZP for monolithic restorations
has been developed to overcome problems related to chipping of feldspathic
ceramic layers applied over zirconia. The Y-TZP high density and low residual
porosity (Table 14.3) provide a satisfactory level of opacity, which can mask underlying discolored abutments and allow a controlled depth of translucency after
veneering even with restricted core thickness (0.5 mm). Moreover, Y-TZP restorations do not affect visible color changes with clinical situations with 2 3 mm thick
mucosa, with or without the application of veneering ceramic.
The Y-TZP is exposed to several surface flaws as a result of the pressing or milling methods and other laboratory procedures. Besides its microstructure, the
mechanical properties of Y-TZP ceramic also depend on the defects produced during the manufacturing methods. Impurities in zirconium dioxide (ZrO2) particles, as
well as differences in Y-TZP processing, can affect the stability of the tetragonal
phase. There is a correlation between flexural strength and any surface damage as
shown by surface roughness. Thus the mechanical properties and long-term stability
of Y-TZP restorations can be quite different than those of starting ceramic.
14.5
Zirconia-toughened alumina
The introduction of zirconia up to 10 vol.% into an alumina matrix results in a class
of ceramic material named as ZTA. The ZTA ceramics are used in several fields
and especially in dentistry (dental restorations) because it exhibits transformation
Zirconium in dentistry
329
toughening at high temperature, which improves the fracture toughness, mechanical
strength, and stability. Alumina is one of the hardest ceramics and, thus, has low
surface wear. However, with a high hardness, the chance of brittle fracture is
increased. The addition of Y-TZP to the alumina matrix to form ZTA improves the
mechanical properties of fracture toughness (6 12 MPa/m) and flexural strength of
alumina, decreasing the risk of brittle fracture and improving the efficiency and
reliability of the ceramic restoration. Thus the combination of alumina and zirconia
allows compensating for the moderate toughness of alumina and the aging effect of
zirconia. ZTA ceramic exhibits not only a high toughness value but also, more
importantly, a greater threshold for the stress coefficient, decreasing the crack propagation. Furthermore, alumina has a lower susceptibility to assisted corrosion by
water or body fluid. Then, ZTA has higher hydrothermal stability than Y-TZP ceramic.
The Y-TZP particles are associated with tetragonal monoclinic transformation,
increasing the fracture toughness of the ceramic. For alumina, toughening is due to
grain bridging in the direction of the propagating crack, which shields the ceramic
from the applied load. Moreover, there is the difference in elastic modulus between
the alumina matrix and the zirconia particles, so the cracks will tend to move across
the zirconia grains, inducing their tetragonal-to-monoclinic transformation and dissipating the crack energy. Thus ZTA ceramics can be used as infrastructure materials for crowns and fixed-partial dentures, improving the lifetime and reliability of
ceramic prostheses.
14.6
Surface topography, clinical treatments of zirconia
surface, and adhesion to zirconia in dental
restorations
The glass-free dense polycrystalline microstructure of zirconia ceramic makes the
material chemically inert, and due to the absence of silica in its composition, conventional adhesive luting procedures using hydrofluoric acid etching and silanization are not recommended for this material. Therefore high bond strength and
bonding durability to zirconia in the long term is still a challenge. Although conventional cements, such as zinc phosphate and glass ionomer, had been initially
recommended for zirconia restoration luting, resin-based luting agents provide higher retention with better physicochemical properties than conventional ones, with
increased fracture resistance, fatigue resistance, and long-term durability of ceramic
restorations. Thus several mechanical and chemical treatments on zirconia surface
are proposed.
In addition, after clinical evaluation of ceramic restoration for occlusion adjustment and contact with adjacent teeth, saliva, blood, try-in paste, silicone indicators,
and other contaminants may be present on the internal surface of indirect restoration
and lead to a reduction in the bond strength. Water-spray rinsing alone is not sufficient to remove saliva contaminants; so chemical cleaning using solvent, emulsion,
acidic, alkaline, and neutral products has been recommended for adequate cleaning.
330
Advanced Dental Biomaterials
Among the main cleaning agents, alcohol, acetone, sodium hypochlorite, suspension of zirconium dioxide particles, and phosphoric acid gel are the most used for
zirconia decontamination. However, alcohol was not effective in removing salivary
organic contaminants. Already acetone was effective in removing silicone contamination but was not effective in removing salivary contaminants. Although sodium
hypochlorite is a nonspecific proteolytic solution capable of removing organic
material, resin polymerization may be impaired due to oxygen generation. A commercial alkaline paste of zirconium dioxide suspension removes salivary phosphates
by adsorption, but residual agglomerated zirconium dioxide particles on the zirconia
surface may be associated with slight bond strength reduction or bonding effectiveness of uncontaminated zirconia.
Commonly 30% 40% phosphoric acid gel is recommended to remove contaminants of the bonding surface of prosthetic restoration. Phosphoric acid was an effective method to remove salivary contamination, but it reduces surface free energy
and residual phosphate groups could compete with the binding sites of 10methacryloyloxydecyl dihydrogen phosphate (MDP) monomer on the hydroxyl
groups of zirconia surface, reducing the bond strength. Therefore additional
airborne-particle abrasion after try-in procedures removes contaminants successfully
and improves bond strength durability in the long term.
Previous studies showed that aluminum oxide airborne-particle abrasion caused
an increase in the surface roughness, and surface free energy, increasing the bonding area available for mechanical interlocking and surface wettability of zirconia
ceramic. Air abrasion removes mechanically the superficial ceramic and exposes a
fresh bonding area, improving the bond between rougher zirconia and resin-based
materials and between zirconia and veneering porcelain by micromechanical retention. Alumina grain size used in the air-abrasion particles method varies from 25 to
250 μm applied under 0.05 0.45 MPa for 5 30 seconds at a distance of 5 20 mm
between the nozzle of the sandblaster and ceramic restoration.
Unfortunately, it has been reported that alumina airborne-particle abrasion
could cause surface microcracks and activate the transformation of zirconia crystals from tetragonal-to-monoclinic phase at the surface and subsurface of zirconia
and should be used with caution since that excessive abrasion may weaken and
decrease the mechanical properties of zirconia material. For this reason, manufacturers suggest the use of alumina abrasion before final sintering and/or the heat
treatment after this procedure to reverse the tetragonal-to-monoclinic phase. In
addition, air-abrasion particles of 50 μm, air-abrasion using the regular pressure of
0.25 MPa, or the combination of low pressure of 0.05 MPa and priming with
MDP-containing primers, at 10 mm of distance from the bonding surface, seem to
be useful to achieve durable bond strength, which could reduce the chance of
phase transformation.
Surface grinding methods using disks and diamond rotatory instruments were
tested in order to increase roughness and optimize bond strength. However, due to
the high hardness of zirconia coarse diamond burrs are necessary to produce a
rougher surface and adequate bonding of luting cements to zirconium dioxide ceramics, but this procedure may induce microcracks, decrease mechanical properties,
Zirconium in dentistry
331
increase crystalline phase transformation, and cause damage to zirconia surface. So
proximal and occlusal adjustments should be performed with caution and under
constant water spray to avoid heating.
Tribochemical silica coating consists of airborne-particle abrasion of aluminum
oxide particles modified by silica, promoting a roughened surface that is coated
with silica and receptive to silanization treatment. It is reported that this technique
is better compared to conventional air-abrasion particle. Silica coating improves
bond strength due to micromechanical interlocking by the increased bonding area
and surface free energy, but ultrasonic cleaning destroys this effect. Moreover, silicatized alumina followed by application of silane coupling agent promotes chemical
adhesion by the formation of silanol groups, which react with the silica layer on the
inner surface of the zirconia restoration. Silica coating and silanization improved
long-term resin bonding to zirconia ceramics and water resistance.
In dentistry, lasers are used to cut dental hard tissues, in the same way, the laser
may modify the material surface, including zirconia ceramic. Laser irradiation
represents an effective technique for conditioning zirconia surfaces, enhancing
micromechanical retention, and improving the bond strength of resin cement on zirconia ceramic and porcelain zirconia bonding, due to the increase in the surface
roughness and optimizing wettability. Carbon dioxide (CO2) laser treatment is
reported to be capable of increased bond strength for irradiated zirconia. Erbiumdoped yttrium aluminum garnet and neodymium-doped yttrium aluminum garnet
etching also improved the bond strength. However, the use of these lasers may
induce microcracks formation, cause silver spot at application point, and increase
the amount of monoclinic phase. The titanium/sapphire-based laser with ultrashort
femtosecond pulses seems to be a promising technique to provide necessary surface
roughness, increase adhesive efficiency of zirconia resin interface, remove contaminants with minimum thermal and mechanical damage, and without phase
transformation.
Another nondestructive method to improve zirconia bonding is the use of
plasma technology by cleaning, etching, surface functionalization, and deposition
of thin functional films. For dental purposes, the application of nonthermal atmospheric pressure plasma has been commonly used for surface modification of
biomaterials by the emission of plasma-containing ions, electrons, and molecules
in an unbalanced nature. Silica vapor nanofilm is deposited on zirconia surface by
reactive magnetron sputtering, making it more chemically reactive. Film deposition of silica precursors, such as hexamethyldisiloxane and tetramethylsilane, is
also responsible for improving adhesive bonding. Plasmatized elements and
hydrophilic properties of zirconia are enhanced after decomposition and vaporization processes, resulting in the reduction of contact angle and improvement of
wettability of argon and methane plasma. Also, plasma application increases the
surface energy and removes contaminants, once C C and C H bonds can be
broken; as well as enhancing chemical bonding by van der Waals secondary
bonds. After atmospheric pressure plasma treatment, the polycrystalline structure
of zirconia ceramic remains unchanged, with the adhesive interface having waterresistant behavior.
332
Advanced Dental Biomaterials
Selective infiltration etching on the structural integrity of the zirconia ceramic
consists of heating-induced maturation and grain boundary diffusion, which in
contact with a thin layer of low temperature melting glass, transforms the zirconia
surface from a relatively nonretentive into a highly retentive surface, establishing a
strong and durable bonding to zirconia. Application of a thin layer of vitreous
porcelain glaze, composed basically of high silica content, amorphous matrix, or
silicon dioxide, results in the vitrification of the ceramic surface that promotes adequate bond strength. Glazed zirconia makes this surface etchable by hydrofluoric
acid and subject to silanization, a condition similar to silica-based ceramics.
Therefore low-fusing porcelain glaze application on zirconia surface seems to be a
promising method for improving the bond strength to the resin cement and optimizes zirconia porcelain adhesion and fracture resistance. However, coated zirconia surfaces with porcelain glaze should not be treated with hydrofluoric acid for
too long, because the etching may completely remove the glassy film from the surface, to approximately 12 μm of thickness. Moreover, glass coating in the inner surface of a metal-free prosthesis forms a layer thick enough to interfere in the seating
of the zirconia restorations, but within clinically acceptable marginal discrepancies.
Hydrofluoric acid is considered an efficient agent capable of dissolving the
glassy matrix, but zirconium dioxide ceramics are acid resistant to typically etching
using low concentration (4% 10%) hydrofluoric acid. Therefore it is unable to create microretention on the crystalline surface of zirconia, without glass content. In
this way, several studies have evaluated different concentrations, application times,
ultrasonic and hot etching. Highly concentrated (above 40%) hydrofluoric acid
applied on zirconia surface under medium-to-long time at room temperature has
shown increased wettability, surface roughness, morphologic irregularities, and
bond strength to the resin-luting materials. Hot hydrofluoric acid etching enhances
surface roughening to improve resin zirconia bonding; even at low concentration
(9.5%) for a short duration time (60 seconds), it may create roughness, making the
etching safer due to the hazardous nature of hydrofluoric acid. Unfortunately, zirconia surfaces etched with hydrofluoric acid induce tetragonal-to-monoclinic phase
transformation due to low-temperature degradation (LTD), but this was lower compared to the airborne-particle abrasion. Other solutions include hot hydrochloric
acid, hydrochloric acid and ferric selenide solution, sulfuric acid in solution with
hydrogen peroxide, a mixture of nitric acid and hydrofluoric acid, hot sulfuric acid,
and hot sulfuric acid mixed with hydrofluoric acid that also improved bond strength
and promoted a roughened surface.
The use of coupling agents, such as zirconia primers, metal primers, and silanes,
have been recommended to provide chemical bonding to zirconia and improve
bond strength, preferentially after surface treatment. After tribochemical silica coating, glass-ceramic coating, and deposition of silica by plasma technique on the zirconia surface, application of bifunctional silane coupling agent promotes bonding
to both inorganic and organic surfaces, increasing the adhesion between resin
cement and zirconia, because zirconium dioxide ceramic is not readily reactive to
conventional silane agents. The silane-coupling agent contains 1% 2% of prehydrolyzed γ-methacryloxypropyltrimethoxy-silane in ethanol water solution, under
Zirconium in dentistry
333
a pH of 4 5 adjusted using acetic acid. Silanes chemically bond to the silicacoated zirconia through silanol functional groups and may react to zirconia forming
Si O Zr bonds, sufficient to stabilize tetragonal-phase and copolymerize with the
resin cement matrix, increasing surface energy and wettability of substrate.
An important component of primers is the adhesive functional monomer phosphate MDP, which improves the bond strength, due to the formation of P O Zr
covalent chemical bonds between MDP and zirconia, and is resistant to water
storage. Some universal primers also include phosphoric acid and sulfide acrylate
monomers that enhance chemical bonding to oxide ceramics and other prosthetic
materials. These adhesive monomers have the ability to form secondary bonds as
van der Waals forces and hydrogen bonds with metal oxides, interfacial forces that
improve the surface wettability of zirconia. Heat treatment of metal/zirconia primer
improved the initial bond strength. In addition, resin cements containing phosphoric
acid group monomers are recommended to improve the bonding to zirconium
dioxide ceramic, but these cements alone are not sufficient for creating a
stable adhesion and primer should be applied previously. Some universal adhesives
contain both silane and phosphoric monomers and seem to be a good alternative
strategy for bonding to zirconia, by simplifying the practical handling. Therefore
the combination of a surface treatment followed by the application of phosphatebased primer and resin-luting agents containing phosphate monomers shows promising results.
14.7
Failure and fractographic analysis of zirconia
restorations
Clinical studies report the higher failure of PFZ restorations than PFM restorations,
mainly related to chipping or delamination of veneering porcelain and deboning of
the restoration. Core fractures of zirconia-based restorations may also be found in
literature but are not usually reported due to the high strength of zirconia. For multiunit FPDs, clinical failures have their origin located at the gingival area of connectors; the origin is reported to be at the cervical margin of the crowns, where the
anatomical shape of tooth crown presents a curvature toward the occlusal surface
and where stress concentrates during chewing. Chipping or delamination of porcelain are usually reported as material dependent, resulting from thermal incompatibilities between porcelain and zirconia, adhesion/wet problems or pores at this
interface, inappropriate support provided by zirconia infrastructure for the veneering porcelain, contamination during veneering, or irregular porcelain thickness. The
fracture origin may be located at the interface between the framework and porcelain
or related to occlusal contact wear.
For implant supported crowns, zirconia presented seven times more complications, most related to screw loosening, loss of retention, and porcelain fracture. The
areas of contact between the zirconia abutment and the implant platform and/or
the titanium screw are also sites of fracture origin. The difference between elastic
334
Advanced Dental Biomaterials
modulus of involved materials (zirconia: 269 GPa; titanium: 110 GPa) promotes
unequal stress distribution at the system, favoring fractures at the interfaces.
The criteria established for clinical survival or failure varies between the clinical
trials. Cohesive fractures of veneering ceramic usually do not impair function, they
may be polished/repaired and restoration is not removed. For this reason, chipping
may be classified as “survival.” The variation in classifying survival/failure criteria
explain studies that show clinical success rates of PFZ crowns similar to PFM
crowns, both tooth or implant supported, or no difference in esthetic or function of
metal-ceramic or all-ceramic three-unit FPD, according to patients and dentist evaluation after 3 years. The adequate approach by the thought of the authors would be
to consider failure “the restorations that require replacement”—those which failed
in reestablishing esthetics and function.
It is also difficult to reproduce the clinical failure of crowns in in vitro experiments. The occlusal loading is complex to simulate in laboratory experiments, usually leading to damage at the load application site, with the origin of fractures
related to contact damage but not from the cervical area, as in the clinical scenario.
The use of soft pistons for load application and abutments with elastic properties
similar to dentin may be useful for simulating clinical failures of all-ceramic
restorations. The load used in laboratory experiments is usually greater than the
clinical chewing loads, also a reason for fracture origins at the load application site.
Higher loads are used for accelerating the experiments since clinically failures take
place after 3 5 years of service, which is not a feasible laboratory time.
The study of fractured restorations started around the 1990s. It aims to identify
signs of crack propagation at the fractured surface, for determination of the fracture
origin. Furthermore, quantitative analysis may be performed after in vitro tests for
calculation of fracture toughness. The fracture origin may help researchers to identify the causes of failure, and where the efforts of improvement must be focused on
increasing clinical survival of restorations. The fractographic analysis of ceramics
and glasses has a guide recommended by the National Institute for Standards and
Technology, written by George Quinn, where researchers and clinicians may find
information on how to proceed with the analysis of both laboratory samples and
clinically fractured restorations and also the equipment that are useful/necessary for
the analysis. It is available online and free of charge.
All materials have an inherent population of defects. Defects in zirconia may be
originated during manufacturing, machining (presintering), or during laboratory and
clinical adjustments (after sintering). A defect with a critical size will determine the
strength and fatigue life of the prosthetic piece, and the material will fail when the
nominal strength overcome the stress field created around this defect.
Laboratory failed specimens may be directly observed under the microscope for
determination of the fracture origin. In the case of evaluating fractured clinical
pieces, the restoration may be removed. In cases where replacement is required, or
when the restoration may be repaired and keep performing esthetic and function, it
is possible to make an impression of the fractured restoration/surfaces with
ultralight-bodied impression material followed by an epoxy-poured replica, which
can be observed under the microscope.
Zirconium in dentistry
335
The first evaluation under a stereomicroscope with lateral illumination will guide
the observer to the fracture origin site. Afterward, scanning electron microscopy
images will allow more detailed observation of the critical defect which led the restoration to fracture. The identification of the critical defect, together with information, such as the stress field, the load applied/tooth arc position, the history of
fracture reported by the patient, cementation procedures adopted, number of cycles/
time in service, will help the identification of the most likely cause of fracture. In
the case of zirconia, the image of round-shaped grains at the failure origin indicates
a defect introduced in the presintering stage, while angulated grains may indicate a
defect introduced after sintering, as grinding cracks for example. The observation
with transillumination of frameworks prior to veneer application will help to identify failures occurred in the manufacturing or machining stages. These rough failures, and also failures introduced during veneer application, are responsible for
premature clinical failures.
The reproduction of clinical failures in the laboratorial environment is of high
relevance since in vitro data have relevance when simulating the oral situation. The
fractography is the tool that allows the clinician and the researcher to investigate
the possible reason for the failure of the restoration and to verify if the laboratorial
pieces failed for the same reasons.
14.8
Mechanical testing of zirconia ceramics
Every new technique, composition or structural design, proposed for a material/restoration must be tested before large appliance. In the field of dental materials, not
all materials launched or the alterations proposed may be tested clinically due to
the long time expended in clinical researches. Thus mechanical tests are applied.
These tests should be performed with a focus on investigating factors responsible
for the clinical failures, such as chipping, delamination, and fractures caused by
introduced defects in different stages of material production and the restoration’s
manufacturing. Besides that, fatigue tests are of high relevance in clinical experimentation of ceramics, since restorations will fail after being subjected to a period
of clinical service, at loads below the fracture strength of the material or prosthetic
piece. Fracture occurs after the rupture of the bonds in a material, and in ceramics
is determined by the largest defect present in the loaded piece.
Usually bending and/or flexural tests (three- and four-point bending and biaxial
flexural strength tests) are used to measure the mechanical performance, structural
integrity, strength, and fatigue of zirconia ceramics, by employing bar or disk specimens. The biaxial flexural strength test is advocated to present a more clinical relevant stress scenario and failure mode than uniaxial tests, presenting delamination
failures in layered zirconia.
Several standards are applied for testing the properties of dental materials. The
ISO 6872 describes the tests to be applied for dental ceramic materials indicated
for fixed all-ceramic and metal-ceramic restorations and prostheses. Zirconia is
336
Advanced Dental Biomaterials
classified as type II ceramics, which are provided in other forms than powders,
pastes, or aerosols. The dimensions of samples and test devices, such as the calculation of strengths, are provided in detail by the standard. Other standards are available for specific tests, such as American Society for Testing and Materials
standards, Deutsches Institut für Normung, and others.
The martensitic phase transformation of zirconia grains when the surface is subjected to stimuli, such as air abrasion or grinding, increases strength and fatigue of
zirconia. The mechanical stimuli trigger the transformation on the zirconia surface,
and the volume expansion creates a compression layer of about 0.5 7 μm, which
acts against the tensile forces generated during strength tests. This characteristic,
together with the high initial mechanical strength of zirconia, will require test
equipment with high strength capacity.
One of the main clinical failures of zirconia is the chipping or delamination of
the veneering porcelain. For testing of layered structures, the variation in elastic
properties of the different materials and the thickness of the layers must be considered. The use of nonplanar specimens, such as curved disks or dome structures,
may also lead to relevant failure modes like fractures with the origin located at the
margin of the structures. However, the clinical geometries are far more complex,
mainly in occlusal and cervical proximal tooth faces. Even though, load-to-failure
tests of cemented crowns lead to very high load results and do not present a significant clinical outcome.
In the clinical situation, failures occur under the application of a load below that
registered in strength tests. However, for zirconia, the fatigue limit of monolithic
zirconia bridges was reported to be around 1600 N even after 106 mechanical
cycles in water, a load much higher than the occlusal loads registered for the posterior region (around 300 400 N). The high loads and high cyclic frequencies are
applied with the aim of decreasing the time expended in laboratory tests. Fatigue is
defined as the degradation of the material under mechanical, chemical, and biological stress. Defects in the bulk or surface of the ceramic present a slow growth under
fatigue, until reaching a critical size, which will lead to fracture. Fatigue tests may
represent the clinical failure mode, based on time in service. The sliding-contact
fatigue test presented failures as porcelain chipping similar to the clinical pattern.
The aim is to reproduce the clinical failure mechanics in laboratory fatigue tests,
with similar origins, flaw type, and damage caused over time. A complete description of characteristics and indications of fatigue tests for ceramics can be found in
ADM guidance, published in 2017.
Zirconia ceramics present a specific degradation caused by water, extensively
evaluated and exposed by Chevalier et al. (1999), called LTD. It is represented by
the phase transformation of zirconia crystals, from tetragonal to monoclinic when
in the presence of water at low temperatures. The transformation initiates in isolated
surface grains and spreads through the entire surface of the material. This transformation is accompanied by a volume expansion of around 4%, which leads to nucleation of grains and enhanced surface roughness. Also, cracks are created between
gains and allow the penetration of water, which brings the degradation process to
the bulk of the material. Properties such as strength, toughness, and density are
Zirconium in dentistry
337
affected. Besides that, the transformation of the crystals that also occurs during
heating and cooling may lead to the development of residual stresses at grain
boundaries, which can lead to nucleation of microcracking under external stresses.
The distribution of flaws has a great effect on the strength of ceramics: ceramics
with large flaws have low strength and high scatter in the experimental data. For
this reason, the Weibull statistical analysis is recommended for analysis of data
generated during strength and fatigue tests.
14.9
Limitations and challenges
The zirconia-based ceramics have been the target of many studies, in vitro, in vivo,
or in silico (numerical method with computer simulation). Like any other material,
it has many advantages, as discussed already in this chapter, but also presents some
disadvantages and aspects to be improved. The initial obstacle to be overcome is to
develop a material which can replace dental tissues—one single material is not
able, at the moment, to replace both enamel and dentin, due to the mechanical and
structural discrepancies between both tissues.
In the clinical situation, zirconia presents other limitations, like the chipping/
delamination of veneering porcelain, and the difficulty in adhesion, which requires
mechanically retentive abutments. The LTD was already reported in a clinical situation, but for hip prosthesis, and demonstrated in vitro. In laboratory tests, the origin
of failures, the high loads, and time required for fracture hamper the simulation of
the clinical situation.
The high incidence of chipping and delamination of veneering porcelain of zirconia restorations in clinical studies has led the manufacturers to develop zirconia
for monolithic restorations, which may be stained for a better esthetic match.
Polychromatic CAD/CAM blocks are also available in the market, which imitate
the color variations from cervical to incisal thirds of teeth. Translucency has also
been increased in zirconia blocks, aiming to mimic the esthetic effect of glass containing ceramics. However, clinically, they are more suitable for the posterior
region.
The absence of the glassy phase or silica content in zirconia ceramics leads to a
material with improved mechanical characteristics, but also a chemically inert
material. The noninteraction of the ceramic surface hinders the adhesive procedures.
Sandblasting may help adhesion, but the damage caused to the material is something to consider in the long-term clinical service of restorations. The application of
very complex surface treatments, like plasma deposition, does not help in overcoming this limitation either. At the moment, zirconia restorations are somehow dependent on mechanical retention, limiting the indications of the material.
The development of glass-infiltrated zirconia is a promising solution for adhesion. When the glass is added to the cementation surface, the adhesive procedures
are facilitated, and the esthetic appearance and the veneer bonding benefit. Even
strength was reported to be the highest in glass-infiltrated zirconia. Different
338
Advanced Dental Biomaterials
techniques for glass infiltration into zirconia grains were already presented in literature, but no version is available on the market.
Regarding adhesion tests, the gold standard microtensile bond strength test is
hard to perform due to the very high strength and hardness of sintered zirconia,
which impairs the cutting of extremely small samples. To evaluate bonding to zirconia surface, the most employed tests are the shear and microshear bond strength
tests. The limitations offered by this methodology, such as unequal stress distribution, the emergence of compression and tensile stresses at the bonded interface, and
cohesive failures of the substrate, may influence the result of the researches but are
well accepted in literature.
The simulation of fatigue of zirconia pieces in laboratory conditions is the most
important approach for the prediction of the clinical performance of the material.
Due to the excellent good performance of the material, very high loads and very
long time are necessary to obtain a failure by fatigue. Time-consuming laboratorial
tests are usually the first option to be discarded. Thus very high loads are used, a
fact that may underestimate the lifetime/survival of zirconia samples. Very high frequencies (above 10 Hz) for load application may also distance the laboratory test
from the clinical situation. Moreover, when high loads and/or frequencies of load
application are employed, they require specific and more sophisticated equipment.
Thus obtaining fatigue failures of zirconia samples is not a simple task.
The high loads applied, for fatigue or even for load-to-fracture tests, to zirconia
pieces may cause fractures with the origin located at the load application site, which
is not found clinically. Since laboratorial tests aim to generate clinically relevant
data, the origin located in a different site decreases the significance of the research.
Despite the presented limitations, zirconia is still the highest strength ceramic
available for dental application, allowing restorations that were only possible in
metal, to be fabricated in an all-ceramic setup. The adhesive cementation does not
have an established protocol and must be further investigated. The limitations
regarding veneering are supposed to be solved with the use of monolithic zirconia.
The laboratorial simulation of clinical services must also be improved. However,
following the indications, zirconia is a beneficial and predictable material, with
high clinical success rates.
Further reading
Abbas, S., Maleksaeedi, S., Kolos, E., Ruys, A.J., 2015. Processing and properties of
zirconia-toughened alumina prepared by gel casting. Materials (Basel) 8 (7),
4344 4362.
Aboushelib, M.N., Kleverlaan, C.J., Feilzer, A.J., 2007. Selective infiltration-etching technique for a strong and durable bond of resin cements to zirconia-based materials.
J. Prosthet. Dent. 98 (5), 379 388.
Aboushelib, M.N., Feilzer, A.J., Kleverlaan, C.J., 2010. Bonding to zirconia using a new
surface treatment. J. Prosthodont. 19 (5), 340 346.
Zirconium in dentistry
339
Akın, H., Ozkurt, Z., Kırmalı, O., Kazazoglu, E., Ozdemir, A.K., 2011. The shear bond
strength of resin cement to zirconia ceramic after aluminum oxide sandblasting and various laser treatments. Photomed. Laser. Surg. 29 (12), 797 802.
Akpinar, Y.Z., Kepceoglu, A., Yavuz, T., Aslan, M.A., Demirtag, Z., Kılıc, H.S., et al., 2015.
Effect of femtosecond laser beam angle on bond strength of zirconia-resin cement.
Lasers Med. Sci. 30 (8), 2123 2128.
Al Jeaidi, Z.A., Alqahtani, M.A., Awad, M.M., Rodrigues, F.P., Alrahlah, A.A., 2017. Bond
strength of universal adhesives to air-abraded zirconia ceramics. J. Oral Sci. 59 (4),
565 570.
Amaral, M., Valandro, L.F., Bottino, M.A., Souza, R.O., 2013. Low-temperature degradation
of a Y-TZP ceramic after surface treatments. J. Biomed. Mater. Res. B Appl. Biomater.
101 (8), 1387 1392.
Amaral, M., Belli, R., Cesar, P.F., Valandro, L.F., Petschelt, A., Lohbauer, U., 2014. The
potential of novel primers and universal adhesives to bond to zirconia. J. Dent. 42 (1),
90 98.
Amaral, M., Villefort, R.F., Melo, R.M., Pereira, G.K.R., Zhang, Y., Valandro, L.F., et al., 2017.
Fatigue limit of monolithic Y-TZP three-unit-fixed dental prostheses: effect of grinding at
the gingival zone of the connector. J. Mech. Behav. Biomed. Mater. 72, 159 162.
Amaral, M., Weitzel, I.S.S.L., Silvestri, T., Guilardi, L.F., Pereira, G.K.R., Valandro, L.F.,
2018. Effect of grinding and aging on subcritical crack growth of a Y-TZP ceramic.
Braz. Oral Res. 32, e32.
Antunes, M.C.F., Miranda, J.S., Carvalho, R.L.A., Carvalho, R.F., Kimpara, E.T., Assunção,
E., et al., 2018. Can low-fusing glass application affect the marginal misfit and bond
strength of Y-TZP crowns?. Braz. Oral Res. 32, e34.
Anusavice, K.J., Shen, C., Rawls, H.R., 2013. Phillips’ Science of Dental Materials. Elsevier
Health Sciences.
Att, W., Grigoriadou, M., Strub, J.R., 2007. ZrO2 three-unit fixed partial dentures: comparison of failure load before and after exposure to a mastication simulator. J. Oral Rehabil.
34 (4), 282 390.
Attia, A., Kern, M., 2011. Long-term resin bonding to zirconia ceramic with a new universal
primer. J. Prosthet. Dent. 106 (5), 319 327.
Bacchi, A., Consani, R.L.X., Mesquita, M.F., dos Santos, M.B., 2013. Stress distribution in
fixed-partial prosthesis and peri-implant bone tissue with different framework materials
and vertical misfit levels: a three-dimensional finite element analysis. J. Oral Sci. 55 (3),
239 244.
Borba, M., de Araújo, M.D., de Lima, E., Yoshimura, H.N., Cesar, P.F., Griggs, J.A., et al.,
2011. Flexural strength and failure modes of layered ceramic structures. Dent. Mater. 27
(12), 1259 1266.
Bottino, M.A., Bergoli, C., Lima, E.G., Marocho, S.M., Souza, R.O., Valandro, L.F., 2014.
Bonding of Y-TZP to dentin: effects of Y-TZP surface conditioning, resin cement type,
and aging. Oper. Dent. 39 (3), 291 300.
Campos, T.M., Ramos, N.C., Machado, J.P., Bottino, M.A., Souza, R.O., Melo, R.M., 2016.
A new silica-infiltrated Y-TZP obtained by the sol-gel method. J. Dent. 48, 55 61.
Cavalcanti, A.N., Foxton, R.M., Watson, T.F., Oliveira, M.T., Giannini, M., Marchi, G.M.,
2009. Bond strength of resin cements to a zirconia ceramic with different surface treatments. Oper. Dent. 34 (3), 280 287.
Cesar, P.F., Della Bona, A., Scherrer, S.S., Tholey, M., van Noort, R., Vichi, A., et al., 2017.
ADM guidance-ceramics: fracture toughness testing and method selection. Dent. Mater.
33 (6), 575 584.
340
Advanced Dental Biomaterials
Chen, L., Suh, B.I., Brown, D., Chen, X., 2012. Bonding of primed zirconia ceramics: evidence of chemical bonding and improved bond strengths. Am. J. Dent. 25 (2), 103 108.
Cheng, C.W., Chien, C.H., Chen, C.J., Papaspyridakos, P., 2018. Randomized controlled
clinical trial to compare posterior implant-supported modified monolithic zirconia and
metal-ceramic single crowns: one-year results. J. Prosthodont. 28, 15 21.
Chevalier, J., Cales, B., Drouin, J.M., 1999. Low-temperature aging of Y-TZP ceramics. J.
Am. Ceram. Soc. 82 (8), 2150 2154.
Chevalier, J., Deville, S., Münch, E., Jullian, R., Lair, F., 2004. Critical effect of cubic phase
on aging in 3mol% yttria-stabilized zirconia ceramics for hip replacement prosthesis.
Biomaterials 25 (24), 5539 5545.
Cho, J.H., Kim, S.J., Shim, J.S., Lee, K.W., 2017. Effect of zirconia surface treatment using
nitric acid-hydrofluoric acid on the shear bond strengths of resin cements. J. Adv.
Prosthodont. 9 (2), 77 84.
Coelho, P.G., Silva, N.R., Bonfante, E.A., Guess, P.C., Rekow, E.D., Thompson, V.P., 2009.
Fatigue testing of two porcelain-zirconia all-ceramic crown systems. Dent. Mater. 25
(9), 1122 1127.
Conrad, H.J., Seong, W.J., Pesun, I.J., 2007. Current ceramic materials and systems with clinical recommendations: a systematic review. J. Prosthet. Dent. 98 (5), 389 404.
Curtis, A.R., Wright, A.J., Fleming, G.J., 2006. The influence of surface modification techniques on the performance of a Y-TZP dental ceramic. J. Dent. 34 (3), 195 206.
Dal Piva, A., Contreras, L., Ribeiro, F.C., Anami, L.C., Camargo, S., Jorge, A., et al., 2018.
Monolithic ceramics: effect of finishing techniques on surface properties, bacterial adhesion and cell viability. Oper. Dent. 43 (3), 315 325.
Delgado-Ruı́z, R.A., Calvo-Guirado, J.L., Moreno, P., Guardia, J., Gomez-Moreno, G., MateSánchez, J.E., et al., 2011. Femtosecond laser microstructuring of zirconia dental
implants. J. Biomed. Mater. Res. B Appl. Biomater. 96 (1), 91 100.
Della Bona, A., Kelly, J.R., 2008. The clinical success of all-ceramic restorations. J. Am.
Dent. Assoc. 139 (Suppl.), 8S 13S.
Della Bona, A., Donassollo, T.A., Demarco, F.F., Barrett, A.A., Mecholsky Jr., J.J., 2007.
Characterization and surface treatment effects on topography of a glass-infiltrated alumina/zirconia-reinforced ceramic. Dent. Mater. 23 (6), 769 775.
Denry, I., 1996. Recent advances in ceramics for dentistry. Crit. Rev. Oral. Biol. Med. 7 (2),
134 143.
Denry, I., Kelly, J.R., 2008. State of the art of zirconia for dental applications. Dent. Mater.
24 (3), 299 307.
Denry, I., Kelly, J.R., 2014. Emerging ceramic-based materials for dentistry. J. Dent. Res. 93
(12), 1235 1242.
Dérand, P., Dérand, T., 2000. Bond strength of luting cements to zirconium oxide ceramics.
Int. J. Prosthodont. 13 (2), 131 135.
Druck, C.C., Pozzobon, J.L., Callegari, G.L., Dorneles, L.S., Valandro, L.F., 2015. Adhesion
to Y-TZP ceramic: study of silica nanofilm coating on the surface of Y-TZP. J. Biomed.
Mater. Res. B Appl. Biomater. 103 (1), 143 150.
Ernst, C.P., Cohnen, U., Stender, E., Willershausen, B., 2005. In vitro retentive strength of zirconium oxide ceramic crowns using different luting agents. J. Prosthet. Dent. 93 (6), 551 558.
Everson, P., Addison, O., Palin, W.M., Burke, F.J., 2012. Improved bonding of zirconia substructures to resin using a “glaze-on” technique. J. Dent. 40 (4), 347 351.
Feitosa, S.A., Patel, D., Borges, A.L., Alshehri, E.Z., Bottino, M.A., Özcan, M., et al., 2015.
Effect of cleansing methods on saliva-contaminated zirconia—an evaluation of resin
bond durability. Oper. Dent. 40 (2), 163 171.
Zirconium in dentistry
341
Goyatá, F., Galvão, Y., Simões, T.R., Goyatá, L.F., Arruda, J.A., Moreno, A., 2018. Effect of
surface treatments with acid solutions on the surface roughness of an yttrium-tetragonal
zirconia polycrystal. J. Clin. Exp. Dent. 10 (4), e367 e370.
Gracis, S., Thompson, V.P., Ferencz, J.L., Silva, N.R., Bonfante, E.A., 2015. A new classification system for all-ceramic and ceramic-like restorative materials. Int. J. Prosthodont.
28 (3), 227 235.
Grasel, R., Santos, M.J., Rêgo, H.C., Rippe, M.P., Valandro, L.F., 2018. Effect of resin luting
systems and alumina particle air abrasion on bond strength to zirconia. Oper. Dent. 43
(3), 282 290.
Griffith, A.A., 1921. The phenomena of rupture and flow in solids. Phil. Trans. R. Soc.
Lond. A 221, 163 198.
Han, G.J., Kim, J.H., Kim, C.K., Chung, S.N., Chun, B.H., Cho, B.H., 2013. Sequential deposition of hexamethyldisiloxane and benzene in non-thermal plasma adhesion to dental
ceramic. Macromol. Res. 21 (10), 1118 1126.
Helmer, J.O., Driskell, R.D., 1969. Research on bioceramics. Symposium on Use of
Ceramics as Surgical Implants. Clemson University, Clemson, SC.
Henriques, B., Fabris, D., Souza, J.C.M., Silva, F.S., Carvalho, Ó., Fredel, M.C., et al., 2018.
Bond strength enhancement of zirconia-porcelain interfaces via Nd:YAG laser surface
structuring. J. Mech. Behav. Biomed. Mater. 81, 161 167.
Hirano, M., 1992. Inhibition of low-temperature degradation of tetragonal zirconia ceramics—a
review. Br. Ceram. Trans. J. 91, 139 147.
Inokoshi, M., De Munck, J., Minakuchi, S., Van Meerbeek, B., 2014. Meta-analysis of bonding effectiveness to zirconia ceramics. J. Dent. Res. 93 (4), 329 334.
Ishii, R., Tsujimoto, A., Takamizawa, T., Tsubota, K., Suzuki, T., Shimamura, Y., et al.,
2015. Influence of surface treatment of contaminated zirconia on surface free energy
and resin cement bonding. Dent. Mater. J. 34 (1), 91 97.
Ito, Y., Okawa, T., Fukumoto, T., Tsurumi, A., Tatsuta, M., Fujii, T., et al., 2016. Influence
of atmospheric pressure low-temperature plasma treatment on the shear bond strength
between zirconia and resin cement. J. Prosthodont. Res. 60 (4), 289 293.
Kaimal, A., Ramdev, P., Shruthi, C.S., 2017. Evaluation of effect of zirconia surface treatment, using plasma of argon and silane, on the shear bond strength of two composite
resin cements. J. Clin. Diagn. Res. 11 (8), ZC39 ZC43.
Karakoca, S., Yilmaz, H., 2009. Influence of surface treatments on surface roughness, phase
transformation, and biaxial flexural strength of Y-TZP ceramics. J. Biomed. Mater. Res.
B Appl. Biomater. 91 (2), 930 937.
Kelly, J.R., 2004. Dental ceramics: current thinking and trends. Dent. Clin. North Am. 48
(2), 513 530.
Kelly, J.R., Cesar, P.F., Scherrer, S.S., Della Bona, A., van Noort, R., Tholey, M., et al.,
2017. ADM guidance-ceramics: fatigue principles and testing. Dent. Mater. 33 (11),
1192 1204.
Kim, J.W., Covel, N.S., Guess, P.C., Rekow, E.D., Zhang, Y., 2010. Concerns of hydrothermal degradation in CAD/CAM zirconia. J. Dent. Res. 89 (1), 91 95.
Larsson, C., Wennerberg, A., 2014. The clinical success of zirconia-based crowns: a systematic review. Int. J. Prosthodont. 27 (1), 33 43.
Lee, J.H., Lee, C.H., 2017. Effect of the surface treatment method using airborne-particle
abrasion and hydrofluoric acid on the shear bond strength of resin cement to zirconia.
Dent. J. (Basel) 5 (3), E23.
Lee, M.H., Son, J.S., Kim, K.H., Kwon, T.Y., 2015. Improved resin-zirconia bonding by
room temperature hydrofluoric acid etching. Materials (Basel) 8 (3), 850 866.
342
Advanced Dental Biomaterials
Lekesiz, H., 2014. Reliability estimation for single-unit ceramic crown restorations. J. Dent.
Res. 93 (9), 923 928.
Liu, D., Tsoi, J.K., Matinlinna, J.P., Wong, H.M., 2015. Effects of some chemical surface
modifications on resin zirconia adhesion. J. Mech. Behav. Biomed. Mater. 46, 23 30.
Lohbauer, U., Amberger, G., Quinn, G.D., Scherrer, S.S., 2010. Fractographic analysis of a
dental zirconia framework: a case study on design issues. J. Mech. Behav. Biomed.
Mater. 3 (8), 623 629.
Lohbauer, U., Scherrer, S.S., Della Bona, A., Tholey, M., van Noort, R., Vichi, A., et al.,
2017. ADM guidance-ceramics: all-ceramic multilayer interfaces in dentistry. Dent.
Mater. 33 (6), 585 598.
Malkondu, O., Tinastepe, N., Kazazoglu, E., 2016. Influence of type of cement on the color
and translucency of monolithic zirconia. J. Prosthet. Dent. 116 (6), 902 908.
McLean, J.W., Hughes, T.H., 1965. The reinforcement of dental porcelain with ceramic oxides. Br. Dent. J. 119 (6), 251 267.
Menani, L.R., Farhat, I.A., Tiossi, R., Ribeiro, R.F., Guastaldi, A.C., 2014. Effect of surface
treatment on the bond strength between yttria partially stabilized zirconia ceramics and
resin cement. J. Prosthet. Dent. 112 (2), 357 364.
Negreiros, W.M., Ambrosano, G.M.B., Giannini, M., 2017. Effect of cleaning agent, primer
application and their combination on the bond strength of a resin cement to two yttriumtetragonal zirconia polycrystal zirconia ceramics. Eur. J. Dent. 11 (1), 6 11.
Nevarez-Rascon, A., Aguilar-Elguezabal, A., Orrantia, E., Bocanegra-Bernal, M.H., 2009.
On the wide range of mechanical properties of ZTA and ATZ based dental ceramic
composites by varying the Al2O3 and ZrO2 content. Int. J. Refract. Met. Hard Mater. 27,
962 970.
Nicolaisen, M.H., Bahrami, G., Schropp, L., Isidor, F., 2016. Functional and esthetic comparison of metal-ceramic and all-ceramic posterior three-unit fixed dental prostheses. Int. J.
Prosthodont. 29 (5), 473 481.
Øilo, M., Arola, D., 2018. Fractographic analyses of failed one-piece zirconia implant
restorations. Dent. Mater. 34, 922 931.
Øilo, M., Kvam, K., Tibballs, J.E., Gjerdet, N.R., 2013. Clinically relevant fracture testing of
all-ceramic crowns. Dent. Mater. 29 (8), 815 823.
Øilo, M., Hardang, A.D., Ulsund, A.H., Gjerdet, N.R., 2014. Fractographic features of glassceramic and zirconia-based dental restorations fractured during clinical function. Eur. J.
Oral Sci. 122 (3), 238 244.
Özcan, M., Bernasconi, M., 2015. Adhesion to zirconia used for dental restorations: a systematic review and meta-analysis. J. Adhes. Dent. 17 (1), 7 26.
Özcan, M., Cura, C., Valandro, L.F., 2011. Early bond strength of two resin cements to YTZP ceramic using MPS or MPS/4-META silanes. Odontology 99 (1), 62 67.
Paes, P.N.G., Bastian, F.L., Jardim, P.M., 2017. The influence of Y-TZP surface treatment
on topography and ceramic/resin cement interfacial fracture toughness. Dent. Mater. 33
(9), 976 989.
Pandoleon, P., Kontonasaki, E., Kantiranis, N., Pliatsikas, N., Patsalas, P., Papadopoulou, L.,
et al., 2017. Aging of 3Y-TZP dental zirconia and yttrium depletion. Dent. Mater. 33
(11), e385 e392.
Park, C., Yoo, S.H., Park, S.W., Yun, K.D., Ji, M.K., Shin, J.H., et al., 2017. The effect of
plasma on shear bond strength between resin cement and colored zirconia. J. Adv.
Prosthodont. 9 (2), 118 123.
Peampring, C., Aksornmuang, J., Sanohkan, S., 2017. In vitro fracture resistance of
composite-resin-veneered zirconia crowns. J. Conserv. Dent. 20 (4), 225 229.
Zirconium in dentistry
343
Pereira, G.K., Silvestri, T., Camargo, R., Rippe, M.P., Amaral, M., Kleverlaan, C.J.,
et al., 2016. Mechanical behavior of a Y-TZP ceramic for monolithic restorations:
effect of grinding and low-temperature aging. Mater. Sci. Eng. C Mater. Biol. Appl.
63, 70 77.
Piconi, C., Maccauro, G., 1999. Zirconia as a ceramic biomaterial. Biomaterials 20 (1),
1 25.
Pitta, J., Branco, T.C., Portugal, J., 2018. Effect of saliva contamination and artificial aging
on different primer/cement systems bonded to zirconia. J. Prosthet. Dent. 119 (5),
833 839.
Qasim, T., Ford, C., Bush, M.B., Hu, X.Z., Malament, K.A., Lawn, B.R., 2007. Margin failures in brittle dome structures: relevance to failure of dental crowns. J. Biomed. Mater.
Res. B Appl. Biomater. 80 (1), 78 85.
Qualtrough, A.J., Piddock, V., 1997. Ceramics update. J. Dent. 25 (2), 91 95.
Quinn, G.D., 2016. NIST recommended practice guide: fractography of ceramics and glasses.
Special Publication 960-16e2. National Institute of Standards and Technology,
Washington, DC.
Ramos-Tonello, C.M., Trevizo, B.F., Rodrigues, R.F., Magalhães, A.P.R., Furuse, A.Y.,
Lisboa-Filho, P.N., et al., 2017. Pre-sintered Y-TZP sandblasting: effect on surface
roughness, phase transformation, and Y-TZP/veneer bond strength. J. Appl. Oral Sci. 25
(6), 666 673.
Ritter, A.V., 2017. Sturdevant’s Art & Science of Operative Dentistry. Elsevier Health Sciences.
Sailer, I., Balmer, M., Hüsler, J., Hämmerle, C.H.F., Känel, S., Thoma, D.S., 2017.
Comparison of fixed dental prostheses with zirconia and metal frameworks: five-year
results of a randomized controlled clinical trial. Int. J. Prosthodont. 30 (5), 426 428.
Scherrer, S.S., Cattani-Lorente, M., Vittecoq, E., de Mestral, F., Griggs, J.A., Wiskott, H.W.,
2011. Fatigue behavior in water of Y-TZP zirconia ceramics after abrasion with 30 μm
silica-coated alumina particles. Dent. Mater. 27 (2), e28 e42.
Scherrer, S.S., Lohbauer, U., Della Bona, A., Vichi, A., Tholey, M.J., Kelly, J.R., et al.,
2017. ADM guidance-ceramics: guidance to the use of fractography in failure analysis
of brittle materials. Dent. Mater. 33 (6), 599 620.
Silva, L.H., Costa, A.K., Queiroz, J.R., Bottino, M.A., Valandro, L.F., 2012. Ceramic primer
heat-treatment effect on resin cement/Y-TZP bond strength. Oper. Dent. 37 (6),
634 640.
Silva, L.H.D., Miranda, R.B.D.P., Favero, S.S., Lohbauer, U., Cesar, P.F., 2017. Dental ceramics:
a review of new materials and processing methods. Braz. Oral Res. 31 (Suppl.), e58.
Skovgaard, M., Almdal, K., van Lelieveld, A., 2011. Stabilization of metastable tetragonal
zirconia nanocrystallites by surface modification. J. Mater. Sci. 46 (6), 1824 1829.
Available from: https://doi.org/10.1007/s10853-010-5007-1.
Smielak, B., Klimek, L., 2015. Effect of hydrofluoric acid concentration and etching duration
on select surface roughness parameters for zirconia. J. Prosthet. Dent. 113 (6),
596 602.
Sriamporn, T., Thamrongananskul, N., Busabok, C., Poolthong, S., Uo, M., Tagami, J., 2014.
Dental zirconia can be etched by hydrofluoric acid. Dent. Mater. J. 33 (1), 79 85.
Tabatabaian, F., 2018. Color in zirconia-based restorations and related factors: a literature
review. J. Prosthodont. 27 (2), 201 211.
Tholey, M.J., Swain, M.V., Thiel, N., 2011. Thermal gradients and residual stresses in
veneered Y-TZP frameworks. Dent. Mater. 27 (11), 1102 1110.
Thompson, J.Y., Stoner, B.R., Piascik, J.R., Smith, R., 2011. Adhesion/cementation to zirconia and other non-silicate ceramics: where are we now?. Dent. Mater. 27 (1), 71 82.
344
Advanced Dental Biomaterials
Tsuo, Y., Yoshida, K., Atsuta, M., 2006. Effects of alumina-blasting and adhesive primers on
bonding between resin luting agent and zirconia ceramics. Dent. Mater. J. 25 (4),
669 674.
Tzanakakis, E.G., Tzoutzas, I.G., Koidis, P.T., 2016. Is there a potential for durable adhesion
to zirconia restorations? A systematic review. J. Prosthet. Dent. 115 (1), 9 19.
Ural, Ç., Külünk, T., Külünk, Ş., Kurt, M., 2010. The effect of laser treatment on bonding
between zirconia ceramic surface and resin cement. Acta Odontol. Scand. 68 (6),
354 359.
Vagkopoulou, T., Koutayas, S.O., Koidis, P., Strub, J.R., 2009. Zirconia in dentistry: Part 1.
Discovering the nature of an upcoming bioceramic. Eur. J. Esthet. Dent. 4 (2),
130 151.
Vanderlei, A., Bottino, M.A., Valandro, L.F., 2014. Evaluation of resin bond strength to
yttria-stabilized tetragonal zirconia and framework marginal fit: comparison of different
surface conditionings. Oper. Dent. 39 (1), 50 63.
Vechiato-Filho, A.J., Matos, A.O., Landers, R., Goiato, M.C., Rangel, E.C., De Souza, G.M.,
et al., 2017. Surface analysis and shear bond strength of zirconia on resin cements after
non-thermal plasma treatment and/or primer application for metallic alloys. Mater. Sci.
Eng. C Mater. Biol. Appl. 72, 284 292.
Vicente, M., Gomes, A.L., Montero, J., Rosel, E., Seoane, V., Albaladejo, A., 2016.
Influence of cyclic loading on the adhesive effectiveness of resin-zirconia interface after
femtosecond laser irradiation and conventional surface treatments. Lasers Surg. Med. 48
(1), 36 44.
Wandscher, V.F., Prochnow, C., Rippe, M.P., Dorneles, L.S., Callegari, G.L., Baldissara, P.,
et al., 2017. Retentive strength of Y-TZP crowns: comparison of different silica coating
methods on the intaglio surfaces. Oper. Dent. 42 (5), E121 E133.
Weber, K.K., 2018. Biomaterials, Zirconia. NCBI Bookshelf.
Wendler, M., Belli, R., Petschelt, A., Mevec, D., Harrer, W., Lube, T., et al., 2017. Chairside
CAD/CAM materials. Part 2: Flexural strength testing. Dent. Mater. 33 (1), 99 109.
Xie, H., Chen, C., Dai, W., Chen, G., Zhang, F., 2013. In vitro short-term bonding performance of zirconia treated with hot acid etching and primer conditioning etching and
primer conditioning. Dent. Mater. J. 32 (6), 928 938.
Xie, H., Li, Q., Zhang, F., Lu, Y., Tay, F.R., Qian, M., et al., 2016. Comparison of resin
bonding improvements to zirconia between one-bottle universal adhesives and tribochemical silica coating, which is better?. Dent. Mater. 32 (3), 403 411.
Xie, H., Cheng, Y., Chen, Y., Qian, M., Xia, Y., Chen, C., 2017. Improvement in the bonding
of Y-TZP by room-temperature ultrasonic HF etching. J. Adhes. Dent. 19 (5), 425 433.
Yamamoto, L.T., Rodrigues, V.A., Dornelles, L.S., Bottino, M.A., Valandro, L.F., Melo, R.
M., 2016. Low-fusing porcelain glaze application on 3Y-TZP surfaces can enhance
zirconia-porcelain adhesion. Braz. Dent. J. 27 (5), 543 547.
Yang, B., Wolfart, S., Scharnberg, M., Ludwig, K., Adelung, R., Kern, M., 2007. Influence
of contamination on zirconia ceramic bonding. J. Dent. Res. 86 (8), 749 753.
Yang, B., Lange-Jansen, H.C., Scharnberg, M., Wolfart, S., Ludwig, K., Adelung, R., et al.,
2008. Influence of saliva contamination on zirconia ceramic bonding. Dent. Mater. 24
(4), 508 513.
Yang, B., Barloi, A., Kern, M., 2010. Influence of air-abrasion on zirconia ceramic bonding
using an adhesive composite resin. Dent. Mater. 26 (1), 44 50.
Yoshida, K., 2018. Influence of cleaning methods on resin bonding to saliva-contaminated
zirconia. J. Esthet. Restor. Dent. 30, 259 264.
Zirconium in dentistry
345
Zhang, Y., Kim, J.W., 2010. Graded zirconia glass for resistance to veneer fracture. J. Dent.
Res. 89 (10), 1057 1062.
Zhang, Y., Pajares, A., Lawn, B.R., 2004. Fatigue and damage tolerance of Y-TZP ceramics
in layered biomechanical systems. J. Biomed. Mater. Res. B Appl. Biomater. 71 (1),
166 171.
Zhao, L., Jian, Y.T., Wang, X.D., Zhao, K., 2016. Bond strength of primer/cement systems
to zirconia subjected to artificial aging. J. Prosthet. Dent. 116 (5), 790 796.
Natural and synthetic bone
replacement graft materials for
dental and maxillofacial
applications
15
Zeeshan Sheikh1,2,3, Nader Hamdan4, Mohamed-Nur Abdallah1,
Michael Glogauer1,5 and Marc Grynpas2,3,6
1
Faculty of Dentistry, University of Toronto, Toronto, ON, Canada, 2Lunenfeld-Tanenbaum
Research Institute, Mount Sinai Hospital, Toronto, ON, Canada, 3Department of
Laboratory Medicine and Pathobiology, University of Toronto, Toronto, ON, Canada,
4
Department of Dental Clinical Sciences, Faculty of Dentistry, Dalhousie University,
Halifax, NS, Canada, 5Institute of Biomaterials and Biomedical Engineering, University of
Toronto, Toronto, ON, Canada, 6Princess Margaret Cancer Centre, Department of Dental
Oncology and Maxillofacial Prosthetics, Toronto, ON, Canada
Chapter Outline
15.1 Introduction 347
15.2 Rationale behind use of bone replacement graft materials 348
15.3 Natural tissues and synthetic biomaterials used for bone grafting
15.3.1
15.3.2
15.3.3
15.3.4
Autografts
Allografts
Xenografts
Alloplasts
350
352
353
354
355
15.4 Biocompatibility of bone replacement graft materials and their degradation
products 363
15.5 Biodegradation of implanted graft materials and bone formation 363
15.6 Future of bone tissue graft materials 365
References 366
15.1
Introduction
Bone replacement is a complex phenomenon and a challenging task to accomplish. Bone grafts are the second most common transplanted tissue after blood
and more than 2.2 million grafting procedures take place annually worldwide in
order to repair bone defects in orthopedics, dentistry, and neurosurgery
(Lewandrowski et al., 2000). The treatments of posttraumatic skeletal
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00015-3
Copyright © 2019 Elsevier Ltd. All rights reserved.
348
Advanced Dental Biomaterials
complications, such as delayed unions, nonunions, malunions along with spinal
fusions, filling defects following removal of bone tumors, and several congenital
diseases, are challenges that can be met successfully by grafting procedures
(Aludden et al., 2017). An understanding of bone biology and its constitutional
elements is imperative in comprehending the challenges that must be overcome
when successful bone grafting is the desired goal. Bone formation starts with the
secretion of collagen molecules and ground substance by osteoblasts. The collagen
molecules polymerize in order to create collagen fibers. Calcium salts then precipitate in the ground substance to form osteoid along the collagen fibers. The osteoblasts become trapped in the osteoid, which are referred to as osteocytes (Hall,
2015). Mature compact bone is composed of approximately 30% organic matrix
and 70% calcium salts. Of note, 90% 95% of the organic matrix is collagen
fibers, and the remainder is the gelatinous medium named as ground substance,
which comprises chondroitin sulfate and hyaluronic acid (Hall, 2015). The collagen fibers are oriented along the lines of tensional force. The main crystalline
salt, composed of calcium and phosphate, is hydroxyapatite (HA). Compact bone
has HA crystals that are adjacent to and bound to the collagen fibers. The collagen fibers provide tensile strength, and the HA crystals are responsible for imparting compressional strength (Hall, 2015). Hence this natural composite we
commonly refer to as bone comes into existence, comprised organic and inorganic
components. Bone formation is an elaborate process and it is beyond the scope of
this chapter to cover all aspects in detail.
15.2
Rationale behind use of bone replacement graft
materials
Bone replacement grafts serve as a structural framework for clot development, maturation, and remodeling that ultimately leads to bone formation in osseous defects
(Sheikh, 2013). After implantation of the graft material, the hard and soft tissue
host bed surrounding the graft must be viable and have adequate blood supply. It is
rare for grafts to survive when placed within nonvital host bone. In the weeks following the implantation, new blood vessels, interstitial cells and materials, and
woven bone (by new osteoblasts) are produced by the host bed. All of these embed
the graft material to create the graft-woven bone complex. The graft material and
the woven bone are fused together by cement lines to achieve the desired mechanical strength. Bone formation in grafting procedures involves one or more of the following biologic mechanisms:
1. Osteogenesis: The formation of new bone by osteoblasts derived from the graft material
itself.
2. Osteoinduction: The ability of a material to induce the formation of osteoblasts from the
surrounding tissue at the graft host site, resulting in bone growth.
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
349
3. Osteoconduction: The ability of a material to support the growth of bone over a
surface.
Osteogenesis is achieved with autogenous grafts and the presence of cellular elements or progenitor cells of the autogenous grafts is thought to be responsible for
this to occur (Schallhorn et al., 1970). As explained later in this chapter, other types
of bone replacement grafts do not provide any cellular elements. The best case scenario for these nonautogenous grafts would be osteoinduction, which would stimulate phenotypic conversion of progenitor cells within the healing wound to those
that can form osseous tissue. Osteoconductive materials provide a scaffold to allow
bone ingrowth and deposition. Most bone replacement grafts are osteoconductive,
relatively inert filling materials, and integrate with new bone without providing
much histological evidence of extensive regeneration (Sheikh et al., 2017a).
Although osteointegration, the ability to chemically bind to surrounding bone is not
directly responsible for bone formation, is a desirable property as it aids in the
incorporation of the graft at the host site. The most important aspect for the success
of a bone graft is that it can be completely resorbed and remodeled. This allows the
graft to not interfere with physiologic bone adaptation.
The presence and recruitment of osteoblast precursors and growth factors at sites
of augmentation are essential for bone regeneration to occur. Some graft materials
(cancellous autogenous grafts) and the recipient bed can provide the osteoblast precursors required (Finkemeier, 2002), whereas the growth factors come from the vasculature and recipient bed. Active bone resorption and formation throughout the
graft dominates the early phase of bone regeneration at grafted sites (Sheikh et al.,
2015a,b). The latter phase is mainly known to be characterized by the osteoconductive processes (Urist, 1980). Osteoconduction is a function of a bone graft substrate
providing a three-dimensional (3D) scaffold area promoting ingrowth of host
capillaries and osteoprogenitor cells (Cornell and Lane, 1998). Biomaterials that
imitate natural bone chemistry and structure closely are considered ideal for cellular
osteogenic differentiation. Graft macroporosity and pore interconnection have a
major impact on osteoinduction potential as higher levels of porosity, appropriate
pore-shape, and sufficient interconnectivity are essential for ingrowth of blood vessels and bone matrix deposition (Mastrogiacomo et al., 2006).
During the initial first few weeks, new bone is synthesized by mature osteoblasts
that are differentiated from osteoblast precursors under the influence of osteoinductors. The growth factors involved in formation of new bone act directly on osteoblast and fibroblast proliferation, mesenchymal cell differentiation, extracellular
matrix deposition, and vascular proliferation (Boyne, 1988). Early stages of induction are influenced by the fibroblast growth factor and platelet-derived growth factor (PDGF) by stimulating fibroblast and osteoblast proliferation. On the other
hand, bone morphogenetic proteins (BMPs) affect later stages of osteoinduction
such as vascular proliferation and mesenchymal cell differentiation. Whereas transforming growth factor-beta does not affect mesenchymal cell differentiation but
acts on cellular proliferation, matrix deposition, and vascularization (Sheikh et al.,
2015e).
350
15.3
Advanced Dental Biomaterials
Natural tissues and synthetic biomaterials used for
bone grafting
There are various graft options available and used for alveolar bone grafting and
divided into natural transplants (autografts, allografts, and xenografts) and synthetic
materials (alloplasts) (Tables 15.1 and 15.2) (Sheikh et al., 2015e). These graft
materials are used because they possess either osteogenic, osteoinductive, and/or
osteoconductive properties (Sheikh, 2013). These grafts should ideally be biocompatible, easily molded and/or carved, integrate well with the native bone, and have
adequate mechanical properties with an ideal replacement rate, and be
predictable with a good level of patient acceptance (Sheikh et al., 2015d). Hard
tissue substitute graft materials that have the ability to be resorbed undergo a
replacement process during which they are partially or completely resorbed
by macrophages/osteoclasts before native bone is deposited by osteoblasts
Table 15.1 Available tissue and biomaterial bone replacement graft
options.
Bone replacement graft materials
Human bone graft tissues
1. Autografts (cancellous and/or cortical)
a. Extraoral
b. Intraoral
2. Allografts (cancellous and/or cortical)
c. Fresh or frozen bone
d. FDBA
e. DFDBA
Nonhuman source materials
1. Xenografts
a. Bovine hydroxyapatite
b. Porcine bone
c. Equine bone
d. Coralline calcium carbonate
Synthetic materials (alloplasts)
1. Bioactive glasses
2. Calcium phosphates
a. Hydroxyapatite
b. Tricalcium phosphate
c. Other calcium phosphates (brushite, monetite, CPP)
3. Calcium sulfate
CPP, Calcium polyphosphates; DFDBA, demineralized freeze-dried bone allograft;
FDBA, freeze-dried bone allograft.
Table 15.2 Examples of common commercially available bone grafts for dental and maxillofacial
applications.
Category
Brand name
Company
Generic name/composition
Source
Allograft
Accell
DBX Putty
DynaBlast
Citagenix
DENTSPLY
Keystone Dental
Human bone
Human bone
Human bone
Grafton
MTF—
DFDBA
Puros
Raptos
BioHorizons
Musculoskeletal
Transplant
Foundation
Musculoskeletal
Transplant
Foundation
Bacterin
International
Bacterin
International
Zimmer Biomet
Citagenix
Demineralized bone matrix
Demineralized bone matrix
Demineralized and mineralized
bone matrix
Demineralized bone matrix
Demineralized freeze-dried
bone
Biocoral
Bio-Oss
Inoteb
Geistlich
Cerabone
Botiss Dental
Endobon
Zimmer Biomet
Gen-Os
Interpore-200
Tecnoss Dental
Interpore
International
Osteomed
Dentsply
Dentsply
MTF—
FDBA
OsteoSelect
OsteoSponge
Xenograft
Xenograft/
synthetic
Alloplast
Osseograft
Osteograf/N
PepGen P-15
Ceros
Cerasorb
IngeniOs
β-TCP
Macrobone
Vitoss
Guidor easygraft
Biogran
PerioGlass
Capset
Osteoset
Calciresorb
35
Ceraform
Eurobone
Cerapatite
IngeniOs HA
TransOssatite
Thommen Medical
Curasan
Zimmer Dental
Euroteknika Groupe
Stryker
Sunstar
Atek Medical Group
NovaBone
Lifecore Biomedicals
Wright Medical
Ceraver
Teknimed
Kasios
Ceraver
Zimmer Dental
Transysteme JMT
implant
Human bone
Human bone
Freeze-dried bone
Human bone
Demineralized bone matrix
Human bone
Demineralized bone matrix
Human bone
Mineralized bone
Mineralized/demineralized
bone allograft
Corraline calcium carbonate
Deproteinized bovine bone
mineral
Decalcified freeze-dried bovine
bone
Deproteinized bovine bone
mineral
Anorganic porcine bone mineral
Porous HA
Human bone
Human bone
Demineralized bone matrix
Anorganic bovine bone mineral
Anorganic bovine bone mineral
with a synthetic biomimetic
of the 15 amino acid
sequence of Type-I collagen
β-TCP
β-TCP
β-TCP
Bovine bone
Bovine bone
Bovine bone/
tissue
engineering
β-TCP
β-TCP
In situ hardening β-TCP
granules coated with PLGA
Bioactive glass
Bioactive glass
CS
CS
DCP (65% HA/35% β-TCP)
Synthetic
Synthetic
Synthetic
DCP (65% HA/35% β-TCP)
DCP/dihydrate (Brushite)—
DCPD
HA
HA
HA
Synthetic
Synthetic
marine corals
Bovine bone
Bovine bone
Bovine bone
Porcine bone
Marine corals
Synthetic
Synthetic
Synthetic
Synthetic
Synthetic
Synthetic
Synthetic
Synthetic
Synthetic
Synthetic
Synthetic
β-TCP, Beta-tricalcium phosphate; CS, calcium sulfate; DCP, dicalcium phosphate; DFDBA, demineralized freeze-dried bone allograft;
FDBA, freeze-dried bone allograft; HA, hydroxyapatite; PLGA, poly(lactic-co-glycolic acid).
352
Advanced Dental Biomaterials
(Sheikh et al., 2015a,b). This section discusses the various graft tissues and biomaterial alternatives used for alveolar bone grafting and periodontal defect fill
applications.
15.3.1 Autografts
Autografts are harvested from a donor site in the same individual and transplanted
to another site. Autografts are a source of most osteogenic organic material for
grafting, however, donor site morbidity and limited graft volume that can be
obtained are disadvantages (Table 15.3) (McAllister and Haghighat, 2007; Younger
and Chapman, 1989). Autografts used for dental grafting applications may be of
extraoral or intraoral origin. Intraoral autograft harvest sites are the spina nasalis,
the tuberosity and crista zygomatico-alveolaris from the maxilla, the ramus, retromolar region and the symphysis region in the mandible, as well as bony exostoses
and bone harvested from different sites utilizing bone scrapers (Draenert et al.,
2014). Mandibular autografts are commonly used as bone chips, blocks, and milled
particles (Misch, 1997; Simion et al., 2001). Autografts obtained from extraoral
sites such as the iliac crest provide osteoinductive, osteoconductive, and osteogenic
potential (Cypher and Grossman, 1996). The calvaria is another extraoral site that
can be used to potentially obtain bone tissue for surgical applications (Simion and
Fontana, 2004; Jackson et al., 1986). However, there is less morbidity associated
with intraoral donor sites and that is the reason they are preferred (Misch, 1997).
The common extraoral harvest site that provides large amounts of autologous
cortical-cancellous bone is the iliac crest (Nkenke et al., 2004). Cortical autografts
have high initial strength that after about 6 months of implantation is about 50%
weaker than the physiologically normal bone tissue (Wilk, 2004). Conversely, cancellous bone autografts are initially weaker because of their porous structure and
gain strength over time (Sheikh, 2013). The cancellous autografts revascularize earlier than the cortical grafts around the fifth day after implantation due to their
Table 15.3 Advantages and disadvantages of using autologous (autografts) bone graft.
Advantages
Disadvantages
Biocompatible
Additional surgical phase to obtain
the autograft
Increased operative time and cost
Donor site morbidity, increased
postsurgical pain
Increased risk fracture
Dead bone is at a potential for
infection
Variability in quality of harvested
bone tissue
Limitation of the amount of bone
tissue that can be harvested
Osteoinductive
Osteoinductive
High osteogenic potential
Sufficient mechanical properties to provide
adequate structural support
Good and easier integration into the transplant
host site (no immune response)
Availability in both cortical and cancellous
forms for use
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
353
spongy architecture (Sheikh, 2013). Vertical and horizontal alveolar ridge augmentation using particulate autografts with GBR has been shown to be successful for
placing dental implants (Rocchietta et al., 2015; Merli et al., 2010). However, block
grafts outperform particulate grafts with regards to revascularization, bone-toimplant contact, and bone remodeling (Rocchietta et al., 2015).
15.3.2 Allografts
Graft tissues obtained from genetically nonidentical members of the same species
are known as allografts. These grafts are available in larger quantities for use and
do not have the usual drawbacks of autografts (Table 15.3). Allografts (cortical and
cancellous) of various particle size ranges are used routinely for bone augmentation
procedures with minimal risk of disease transmission (Table 15.4) (Block and
Degen, 2004; Araujo et al., 2013; Sterio et al., 2013). Allografts are available for
periodontal applications as cortical wedges, cortical chips, cortical granules, and
cancellous powders prepared as frozen, freeze-dried, mineralized, and demineralized bone (Al Ruhaimi, 2001).
15.3.2.1 Fresh or frozen allografts
Fresh and/or frozen cancellous bone and marrow tissues demonstrate the highest
osteoconductive and osteoinductive potential among all allografts (Dias et al., 2014;
Macedo et al., 2012). Atrophic maxillary ridges when grafted with human block
grafts of tibia and fresh-frozen chips show features representative of mature and
compact osseous tissue surrounded by marrow spaces (Contar et al., 2009, 2011).
However, due to the risk of disease transmission, use of fresh or frozen iliac allografts is now obsolete.
Table 15.4 Comparison between autografts and allografts.
Bone graft
Strength
Osteogenesis
Osteoconduction
Osteoinduction
3
0
2
3
2
3
2
3
3
1
1
1
0
0
0
0
0
0
2
2
1
1
0
0
Autografts
Cortical
Cancellous
Allografts
Cortical
Frozen
Freeze-dried
Cancellous
Frozen
Freeze-dried
Scores: 0 (none), 1 (moderate), 2 (good), and 3 (excellent).
354
Advanced Dental Biomaterials
15.3.2.2 Mineralized freeze-dried bone allografts
The freeze-drying to process these grafts for use distorts the 3D presentation of the
human leukocyte antigens on the surface of graft particles that affects the immune
recognition (Quattlebaum et al., 1988; Friedlaender et al., 1976). Freeze-dried bone
allograft (FDBA) is known to be osteoconductive and can be combined with autografts to enhance the osteogenic potential (Committee on Research, 2001;
Mellonig, 2000). These graft tissues are mineralized and used for the treatment of
periodontal defects (Mellonig, 1991; Kukreja et al., 2014; Blaggana et al., 2014;
Markou et al., 2009). Cortical FDBA demonstrate greater osteoinductive potential
due to the growth factors stored in the matrix (Sunitha Raja and Naidu, 2008).
FDBA used in combination with resorbable barrier membranes have been used as a
replacement for autograft blocks for ridge augmentation (Lyford et al., 2003). The
use of FDBA blocks for alveolar ridge grafting has shown the presence of vital
bone with a lamellar organization (Jacotti et al., 2012; Wallace and Gellin, 2010).
15.3.2.3 Demineralized freeze-dried bone allogeneic grafts
These allografts that have been demineralized are used alone or in combination
with FDBA and autografts. Demineralized freeze-dried bone allograft (DFDBA)
undergoes resorption at a quick rate (Russell et al., 1997; Hopp et al., 1989) and
often have osteoinductive potential due to the BMPs and growth factors present in
the graft matrix (Mellonig et al., 1981). DFDBA has been shown to produce a lesser
amount of vital new bone in comparison to autografts (Scarano et al., 2006).
DFDBA acquired from younger cadavers has higher osteogenic potential in comparison with grafts from older individuals, resulting in variation in BMP levels in
different batches of DFDBA (Dodson et al., 1996; Jergesen et al., 1991).
15.3.3 Xenografts
Xenografts are graft tissues obtained from nonhuman species, that is, animals, and
are usually osteoconductive with limited resorptive potential (Thaller et al., 1993;
McAllister et al., 1999). The xenograft most commonly used in periodontal regeneration procedures is the deproteinized bovine bone mineral, commercially known as
Bio-Oss, which is a commercially available bone of bovine origin processed to
yield natural bone mineral without the organic elements (Liu et al., 2016). After
heat and chemical treatments, the inorganic phase of bovine bone consists mainly
of HA that retains the porous architecture (Jarcho, 1981). Bovine-derived bone graft
particles and blocks have been used for alveolar ridge augmentation procedures and
intrabony defect filling (Zitzmann et al., 1997; Yildirim et al., 2000).
Bio-Oss remains the most researched xenogeneic bone grafting material. Several
research papers were published on the use of Bio-Oss in different surgical scenarios
(Proussaefs et al., 2003; Valentini and Abensur, 1997; Wallace et al., 2005;
Proussaefs et al., 2002; Berglundh and Lindhe, 1997). Of particular interest was the
use of Bio-Oss as a graft material during direct subantral augmentation (sinus lift)
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
355
procedures where dental implants placed in Bio-Oss grafts had survival rates at
least similar if not better than autogenous grafts (Wallace and Froum, 2003).
However, although bovine-derived bone block grafts have high osteoconductive
potential, these grafts are inherently brittle and lack toughness. This makes them
prone to failure during the screw fixation procedures and/or after implantation
(Yildirim et al., 2000; Felice et al., 2009).
In addition to bovine-derived bone mineral, bone mineral can be obtained from
other animal sources, such as equine or porcine sources. Porcine bone graft tissue is
a porous inorganic bone graft material consisting predominantly of calcium phosphate. These are supplied in granular form with a particle size of 0.25 1 and
1 2 mm (Gen-Os) and are produced by removal of the organic components from
porcine bone (Nannmark and Sennerby, 2008; Pearce et al., 2007). The anorganic
bone mineral matrix is biocompatible, having an interconnecting macro- and microscopic porous structure that supports the formation and ingrowth of new bone at the
implantation site (Nannmark and Sennerby, 2008). A clinical study in humans in
which porcine-derived graft was investigated for implant site development showed
it reduced the hard tissue resorption after tooth extraction (Festa et al., 2013).
The porous microstructure of marine coral has also been used as a template to
fabricate porous coralline HA materials such as interpore-200 (White and Shors,
1986). These materials are fabricated by coral being subjected to high temperature
under pressurized treatment in the presence of aqueous phosphate solutions (Roy
and Linnehan, 1974). This converts the coral to calcium HA, while conserving the
highly organized, permeable, and interconnecting pore structure (Roy and
Linnehan, 1974; White and Shors, 1986). These graft materials have an average
pore diameter of 200 μm, and consist of about 60% porosity/void spaces (Weber
and White, 1973; Weber et al., 1971).
Some other xenograft materials that are being researched include chitosan, red
algae, and gusuibu (Wong and Rabie, 2006; Cho et al., 2005). Chitosan is a product
of the exoskeleton of crustaceans, and has shown the ability to stimulate mesenchymal stem cell differentiation into osteoblasts. When chitosan is combined with HA,
the osteoconductivity is markedly increased (Cho et al., 2005). Red algae are one of
the oldest groups of eukaryotic algae, and also one of the largest, with about
5000 6000 species of mostly multicellular, marine algae, including many
notable seaweeds. Red algae can be chemically converted to HA, which then is utilized for grafting bone defects (Ewers, 2005). Gusuibu is a rhizome of perennial
pteridophyte Drynaria fortunei. This herb has been shown to have good osteoconductive properties and an increase in alkaline phosphatase expression that has a positive effect of promoting calcification (Wong and Rabie, 2006) (Fig. 15.1).
15.3.4 Alloplasts
Alloplastic synthetic biomaterials were developed to overcome the disadvantages of
autografts and are fabricated in various forms with varying physicochemical properties and can be both degradable and nondegradable (Sheikh et al., 2015a,c,d,e,
2017a; AlGhamdi et al., 2010; Shetty and Han, 1991). Alloplasts are usually
356
Advanced Dental Biomaterials
Figure 15.1 Examples of different bone grafting materials used in different clinical
scenarios as per their indication. (A) Block autograft cut from chin. (B) Block autograft
being stabilized using fixation screws in posterior mandible. (C) Allograft (FDBA) being
placed for socket preservation covered with absorbable collagen membrane for placing dental
implant in future. (D) Xenograft (Bio-Oss) used to augment bone around dental implants. (E
and H) Allograft (FDBA) and xenograft (Bio-Oss) used together for sandwich technique to
augment bone in the mandibular anterior region for placing dental implants. (F) An allograft
(FDBA) used to augment anterior maxilla after ridge splitting for future implant placement.
(G) Xenograft (Bio-Oss) used for performing sinus lifting. (I) Allograft (FDBA) covered
with absorbable collagen membrane used for site preparation of partially edentulous
maxillary ridge. (J) Xenograft used for ridge augmentation as part of pontic site development
for three-unit fixed partial denture. (K) Alloplast (FDBA and Enamel Matrix Derivative/
EMD) for GTR procedure. FDBA, Freeze-dried bone allograft; GTR, guided tissue
regeneration.
osteoconductive without any osteoinductive or osteogenic potential on their own
and have been used extensively for periodontal regeneration (Shetty and Han,
1991). The most routinely used alloplastic materials are HA, tricalcium phosphates
(TCP), and bioactive glasses. Calcium phosphate biomaterials are of great interest
to be used as bone replacement graft materials in periodontal regeneration as they
have a similar composition to bone mineral, are osteoconductive, form bone
apatite-like material or carbonated HA, and form a very strong bone calcium phosphate biomaterial interface (Sheikh et al., 2015a,d).
Alloplastic bone grafting materials are sought after because they provide an
abundant amount without the problems associated with autografts (Hench, 1998).
These are fabricated in various forms and with varying physicochemical properties
and can be both resorbable and nonresorbable (Sheikh et al., 2015c,d,e; AlGhamdi
et al., 2010; Shetty and Han, 1991). Alloplastic materials are usually osteoconductive without having any osteogenic and osteoinductive potential and have been used
successfully in periodontal reconstructive applications (Shetty and Han, 1991).
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
357
15.3.4.1 Polymers
Polymers can be classified based on origin: natural and synthetic. Natural polymers
that have been utilized in the fabrication of bone grafts include polysaccharides
(e.g., alginate, argose, chitosan, and hyaluronic acid) and polypeptides (e.g., gelatin
and collagen). Natural polymers possess weak mechanical properties and variable
or negligible rates of degradation, hence their use is limited as bone grafting materials (Asghari et al., 2017). However, natural polymers play an important role in
composite grafts by serving as polymeric shell capsules, which incorporate particles
of allografts. Synthetic polymers (e.g., polyglycolic acid, polylactic acid, polyorthoester, and polyanhydride) provide a platform for regulating and controlling the
biomechanical properties of scaffolds and they also serve as drug delivery carriers
in tissue engineering applications (Sokolsky-Papkov et al., 2007).
HTR Synthetic Bone (Bioplant, Norwalk, CT) is a biocompatible microporous
composite made up of polymethylmethacrylate (PMMA), polyhydroxylethylmethacrylate, and calcium hydroxide. The acronym HTR stands for “Hard Tissue
Replacement” and acceptable clinical results have been achieved in treatment of
intrabony and furcation defects with its use (Yukna, 1990, 1994). Histologically
new bone growth has been observed on the particles of this material (Froum, 1996;
Yukna and Greer, 1992; Stahl et al., 1990). This material has hydrophilicity that
enhances clotting, and the negative particle charges on the surface allows adherence
to bone. Clinically acceptable defect fill and resolution can be achieved and support
the use of HTR as a biocompatible alloplastic bone substitute (Buck et al., 1989;
Murray, 1988). Furthermore, polymers have also traditionally been used as barrier
membranes in the periodontal guided tissue regeneration procedures (Murphy and
Gunsolley, 2003).
15.3.4.2 Calcium phosphates
Calcium phosphate biomaterials have outstanding properties: a similar composition
to bone mineral, bioactivity, ability to promote cellular function and expression
leading to formation of a uniquely strong bone biomaterial interface and osteoconductivity. In addition, calcium phosphates with appropriate 3D geometry are able to
bind and concentrate endogenous BMPs in circulation, may become osteoinductive,
and can be effective carriers of bone cells. Therefore calcium phosphates are potentially useful in bone tissue engineering.
Hydroxyapatite
This is a commonly used calcium phosphate biomaterial for bone regeneration
applications due to having a composition and structure similar to natural bone mineral (Table 15.5) (Wang et al., 2007). HA-based grafts form a chemical bond
directly to bone once implanted (Bagambisa et al., 1993). Synthetic HA is available
and used in various forms: (1) porous nonresorbable, (2) solid nonresorbable, and
(3) resorbable (nonceramic, porous) (Tevlin et al., 2014). HA is nonosteogenic and
mainly functions as an osteoconductive graft material. HA grafts show slow and
limited resorptive potential and generally are dependent on passive dissolution in
Table 15.5 List of existing calcium phosphate compounds (Fernandez et al., 1999; Dorozhkin, 2009; Dorozhkin and Epple, 2002).
Ca/P
ionic
ratio
Density
(g/cm3)
Solubility at 37 C,
2 log(ksp)
MCPM
0.5
2.23
Not available
Ca(H2PO4)2
MCPA
0.5
2.58
Not available
CaHPO4.2H2O
DCPD
Brushite
1.0
2.38
6.63
CaHPO4
DCPA
Monetite
1.0
2.89
7.02
Ca8(HPO4)2(PO4)4 5H2O
α-Ca3(PO4)2
β-Ca3(PO4)2
CaxHy(PO4)z nH2O,
n 5 3 4.5; 15% 20% H2O
Ca82x(HPO4)x(PO4)62x(OH)22x
OCP
α-TCP
B-TCP
ACP
1.33
1.5
1.5
1.2 2.2
2.61
2.86
3.07
3.01
95.9
25.5
29.5
25 32
PHA
1.33 1.67
3.16
Not available
Ca102x(HPO4)x(PO4)62x
(OH)22x (0 , x , 1)
Ca10(PO4)6(OH)2
Ca10(PO4)6O
Ca10(PO4)6F2
Ca2(PO4)2O
CDHA
1.5 1.67
3.16
85.1
1.67
1.67
1.67
2.0
3.16
3.20
3.18
3.05
117.2
Not available
Not available
37 42
Compound name
Chemical formula
Symbol
Monocalcium
phosphate
monohydrate
Monocalcium
phosphate anhydrous
Dicalcium phosphate
dehydrate
Dicalcium phosphate
anhydrous
Octacalcium phosphate
α-Tricalcium phosphate
β-Tricalcium phosphate
Amorphous calcium
phosphate
Precipitated
hydroxyapatite
Calcium-deficient
hydroxyapatite
Hydroxyapatite
Oxyapatite
Fluorapatite
Tetracalcium phosphate
Ca(H2PO4)2 H2O
HA
OXA
FA
TTCP
Mineral
Hydroxyapatite
Hilgenstockite
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
359
tissue fluid and cell-mediated processes such as phagocytosis of particles for resorption (Jarcho, 1981; De Groot, 1980). The degradation rate of HA depends on the
method of ceramic formation, the calcium to phosphate ratio, crystallographic structure, and porosity (Osborn and Newesely, 1980; Jarcho, 1981). The ability of HA to
resorb is also heavily dependent upon the processing temperature. HA grafts synthesized at high temperatures are very dense with very limited biodegradability (Klein
et al., 1983). These dense grafts are usually used as inert biocompatible fillers
(Rabalais et al., 1981; Meffert et al., 1985). At lower temperatures, the particulate
HA is porous and undergoes slow resorption (Ricci et al., 1992). Early implant
loading studies in alveolar ridges augmented with nanostructured HA have shown
promise (Canullo et al., 2006; Sugar et al., 1995). Also, ridge augmentation with
HA granules alone (Sugar et al., 1995) or in combination with autografts has been
investigated (Small et al., 1993).
Tricalcium phosphate
Over the last few years, TCP has been used and extensively investigated as a bone
substitute. TCP has two crystallographic forms; α-TCP and β-TCP (Tamimi et al.,
2012b). β-TCP exhibits good biocompatibility and osteoconductivity and is used
commonly as a partially resorbable filler allowing replacement with newly formed
bone (Shetty and Han, 1991). Resorption of TCP grafts is thought to be dependent
on dissolution by biological fluids in the absence of osteoclasts around the materials
(Lu et al., 1998) and by presence of osteoclast-mediated resorption based on the
osteoclast-like giant cells in defect areas in many studies (Renooij et al., 1985). In
terms of bone regenerative potential, β-TCP grafts have been shown to be similar to
autogenous bone, FDBA, DFDBA, and collagen sponge (Nakajima et al., 2007).
TCP biomaterials have been used in human clinical studies to repair periapical and
marginal periodontal defects, as well as alveolar bony defects (Stavropoulos et al.,
2010; Metsger et al., 1982). In addition, there are studies using β-TCP that report
alveolar ridge augmentation in vertical and horizontal dimensions with variable
results (Shalash et al., 2013; Nyan et al., 2014).
Dicalcium phosphates
These are acidic calcium phosphates that have a high solubility at physiological pH.
Dicalcium phosphate dihydrate (DCPD or Brushite) has been investigated for both
bone defect repair and vertical bone augmentation applications as
injectable cements or as preset cement granules (Tamimi et al., 2009, 2010; Sheikh
et al., 2016). It has been demonstrated that injectable brushite cements are capable
of regenerating bone in atrophic alveolar ridges, buccal dehiscence defects, and
maxillary sinus floor elevation procedures (Gehrke and Famà, 2010). Bone growth
in the vertical direction obtained with brushite cement granules has been seen to be
higher than that obtained with commercially available bovine HA materials
(Tamimi et al., 2006). However, brushite grafts after implantation undergo phase
conversion to insoluble HA that ultimately limits their resorption rate and extent
(Sheikh et al., 2015f; Tamimi et al., 2012b). Brushite can be used as precursor to
the anhydrous form of DCP, dicalcium phosphate anhydrous, also known as DCPA
360
Advanced Dental Biomaterials
Figure 15.2 Scanning electron microscopic micrographs of (A) hydroxyapatite; (B)
β-tricalcium phosphate; (C) octacalcium phosphate; (D) dicalcium phosphate dihydrate
(brushite); (E) calcium polyphosphate; and (F) dicalcium phosphate anhydrous (monetite).
or monetite. Monetite can be precipitated by dehydration of brushite or by modifying the precipitation conditions of brushite cements in order to favor DCP crystallization into monetite instead of brushite (Tamimi et al., 2012b). Monetite does not
convert to HA after implantation (Sheikh et al., 2015f, 2016, 2017c; Tamimi et al.,
2006, 2008) and resorbs at faster rates compared to brushite cement grafts (Gbureck
et al., 2007; Tamimi et al., 2012a; Idowu et al., 2014; Sheikh et al., 2017c).
Monetite granules have been compared with commercially available bovine HA
(Bio-Oss), and have shown greater resorption and bone formation in the extraction
sockets (Tamimi et al., 2010) (Fig. 15.2).
15.3.4.3 Bioactive glasses
These graft materials are composed of silicon dioxide, calcium oxide, sodium
oxide, and phosphorus pentoxide (Schepers et al., 1991; Shue et al., 2012). The particle sizes of bioactive glasses (Bio-Glass) range from 90 710 to 300 355 μm
(Schepers et al., 1991; Schepers and Ducheyne, 1997). After implantation of bioactive glass, a silicon-rich gel is formed on the bioactive ceramic surface with the
outer layer serving as a bonding surface for osteogenic cells and collagen fibers
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
361
(Hall et al., 1999; Xynos et al., 2001). Bioactive glass nanoparticles have been
shown to induce cementoblasts to proliferate in an in vivo study (Carvalho et al.,
2012). Clinical reports of alveolar ridge grafting performed with bioactive glass
reveal bone formation in close contact to the particles (Schepers et al., 1991).
However, limited true periodontal regenerative outcomes based on human histological analysis have been demonstrated with the use of bioactive glass (Nevins et al.,
2000; Knapp et al., 2003).
15.3.4.4 Calcium polyphosphate
Inorganic polyphosphates (polyP) are polymers of orthophosphate, linked by
energy-rich phosphoanhydride bonds to form polymeric chains. These phosphate
polymers exhibit varied biological roles and modulate many biological processes.
Calcium polyphosphate (CPP) was first developed as a bone substitute to address
some of the shortcomings of traditional materials in use for bone healing, such as
HA, TCP, and bioactive glasses. CPP is a good bone substitute as it can be made
with mechanical properties similar to trabecular bone, controlled degradability, and
shows very good integration to host bone when implanted in vivo (Grynpas et al.,
2002). CPP has been used in different forms, such as sintered porous blocks (Pilliar
et al., 2001), particulates (Pilliar et al., 2016), or nanoparticles (Chen et al., 2015).
This flexibility in fabrication has made CPP a good material for use in bone regeneration. Nelson et al. were the first to investigate CPP for bone regeneration as they
explored its ability to repair canine mandibular alveolar defects. The bone defect
was either filled with CPP or autologous bone. Assessment at 4 months showed
increased bone and greater rates of union in the CPP group than in the bone graft
control (Nelson et al., 1993). There have been multiple studies examining tissue
engineering of oral or dental tissues with CPP. El Sayegh et al. (2002) demonstrated
that the degradation rate of CPP did not substantially affect the interactions of
human gingival fibroblasts with CPP materials but that compared with titanium
alloy substrates, cell spreading and attachment were inhibited. These studies suggest
that CPP has promise as a biomaterial for biological and periodontal regenerative
therapy (Wang et al., 2006).
15.3.4.5 Glass ionomers
Glass-ionomer cements were first used in dentistry as calcium/aluminum/fluorosilicate glass powder mixed with polycarboxylic acid to produce a cement paste that
hardens in approximately 5 minutes after which it is rendered water insoluble. Bone
replacement grafts based on glass-ionomer cements are porous, which leads to bone
ingrowth via their osteoconductive nature. After 24 hours of setting they have a
compressive strength and modulus of elasticity (stiffness) that is comparable with
cortical bone. Glass ionomers have been considered as a replacement for PMMAbased bone fillers, which have an exothermic setting reaction (polymerization)
(Jonck et al., 1989). A possible advantage of using this material could be their fluoride release mechanism that may be adapted for controlled (slow release profile)
362
Advanced Dental Biomaterials
drug delivery (antibiotics) in the local periodontal defect environment. A major disadvantage is the lack of resorbability (Denissen et al., 1997), limiting its clinical
use as a scaffold for bone regeneration application.
15.3.4.6 Calcium sulfate
These compounds have a compressive strength greater than that of cancellous bone
(Moore et al., 2001). Calcium sulfate is usually applied as a barrier material to
improve the clinical outcomes of periodontal regeneration therapy (Pecora et al.,
1997). When used as a barrier, calcium sulfate materials work as an adjunct with
other graft materials. A combination of β-TCP and calcium phosphate has been
investigated, which does not require a membrane, lowers cost, reduces surgical
time, and has the potential to treat periodontal intrabony defects (Paolantonio et al.,
2008; Sukumar et al., 2011). A randomized controlled clinical trial over 12 months
has shown that the use of calcium sulfate is useful in minimizing postsurgical recession when compared with the use of collagen membrane (Paolantonio et al., 2008;
Sheikh et al., 2017b; Sheikh, 2014). The clinical outcome of class II mandibular
molar furcation defects has also been shown to be enhanced with the use of a mixture of calcium sulfate and DFDBA (Maragos et al., 2002).
15.3.4.7 Magnesium-based biodegradable materials
Elemental magnesium (Mg) was discovered in 1808 and Mg and its alloys have
generated significant interest for use in biomedical applications as implants, osteosynthesis devices, ligatures, wires for aneurysm treatment, and connectors for vessel
anastomosis (Seal et al., 2009; Staiger et al., 2006). Mg21 is a cation that is mostly
stored in bone tissues and is the fourth most abundant ion in the human body. Mgbased metals corrode in aqueous environments via electrochemical reactions that
result in the production of Mg hydroxide and hydrogen gas (Staiger et al., 2006).
The corrosion product of Mg (Mg21) is easily excreted in urine resulting in the
good biological behavior observed when Mg and its alloys are used for medical
applications (Staiger et al., 2006). Mg-based biomaterials have better mechanical
properties when compared with other conventional biodegradable materials such as
polymers and ceramics (Tan et al., 2013).
Based on the distinct advantages of Mg-based metals, they have been extensively
investigated both in vitro and in vivo for osteologic repair and regeneration applications. Mostly the focus has been on fabricating screws and plates for fracture fixation and porous scaffold (Staiger et al., 2006). However, since these have inferior
mechanical properties than the conventional metallic nondegradable devices, Mgbased devices are not being used for load bearing application (Witte et al., 2008;
Brar et al., 2009; Tan et al., 2013). After implantation of Mg-Ca alloy pins in rabbit
femoral shafts, no cytotoxicity was observed and elevated activity of osteocytes and
osteoblasts was shown around the implants indicating good biocompatibility and
bioactivity (Li et al., 2008).
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
15.4
363
Biocompatibility of bone replacement graft
materials and their degradation products
To perform successfully, biomaterial grafts must not cause abnormal responses in local
tissues and should not produce toxic or carcinogenic effects. Biodegradable materials
in particular should serve their intended function while releasing products of degradation that are biocompatible and do not interfere with tissue healing (Ratner, 2004). A
major concern associated with using biodegradable materials especially polymers is
the possibility of local inflammation due to themselves or via their degradation products (Gooptu and Lomas, 2008). Once implanted, the biodegradation and resorption
processes begin and are accompanied by a release of acidic by-products, which can
result in inflammatory reactions (Van Der Giessen et al., 1996). If the capacity of the
surrounding tissue to eliminate the by-products is low, due to the poor vascularization
or low metabolic activity, the chemical composition of the by-products may lead to
local and systemic disturbances (Anderson, 1988). The inflammatory response to polymer degradation can be controlled somewhat by the incorporation of basic salts such
as sodium bicarbonate, calcium bicarbonate, and calcium HA (Hollinger and
Chaudhari, 1992). Also, the incorporation of TCP (Hutmacher et al., 2001), HA
(Shikinami and Okuno, 1999), and basic salts (Agrawal and Athanasiou, 1997) into
the polymeric matrix results in the production of a hybrid/composite material.
Calcium phosphate based bioceramics are also widely used for bone regeneration applications. Biodegradable dicalcium phosphates are generally well tolerated
by bone and soft tissues and do not cause inflammations in the long term (Apelt
et al., 2004; Lu et al., 1999). Following implantation these grafts are enclosed in
loose connective tissue (Frayssinet et al., 1998), although they can also be surrounded by fibrous connective tissue if the cement composition is acidic (Tamimi
et al., 2009). In vivo studies have shown that early resorption of calcium phosphate
cements is regulated by macrophages rather than osteoclasts (Constantz et al., 1998;
Kuemmerle et al., 2005; Sheikh et al., 2015a,b). Similar to in vitro studies,
implanted cement grafts can resorb via disintegration/fragmentation and rather passive dissolution based upon the solubility constant product of the material (Grover
et al., 2003). This is critical, since it is known that particles released from calcium
phosphate grafts can affect osteoblast function, viability, and proliferation and production of extracellular matrix adversely (Tamimi et al., 2012b). The maximum
number of particles that a single osteoblast can support is B50, and the smaller the
disintegration products are, the stronger the negative effect is observed (Pioletti
et al., 2000). These released particles can also potentially result in peri-implant
osteolysis and failure if the microenvironment around the implanted biomaterial is
not cleared by extracellular media refreshment (Meijer et al., 2008).
15.5
Biodegradation of implanted graft materials and
bone formation
The resorptive capability of implanted bone replacement graft materials allows for
space to be produced for newly forming bone tissue to not only grow along the
364
Advanced Dental Biomaterials
implant surface (creeping substitution via osteoconduction) but also to infiltrate
within the resorbing matrix along with new blood vessels (Sheikh et al., 2015e).
This infiltration of biomaterial scaffold matrix with blood vessels allows for the
bone formation front to progress and be provided with oxygen that is mandatory for
the survival of the regenerating tissues (Klein-Nulend et al., 2005). It is crucial for
the biodegradable scaffold to retain its strength during the healing period so as to
provide fixation at the fracture site but degrade after the healing as completed.
Initial resorption of calcium phosphate cement grafts is affected by the inherent
cement properties such as porosity, as well as the site of implantation, which affects
the rate of fluid exchange and the properties of the surrounding medium (Grover
et al., 2003; Sheikh et al., 2015c,f). The amount of new bone formed is also highly
dependent on implantation site and vascular supply, as an adequate blood supply
increases the speed of cement resorption and replacement by new woven bone
(Constantz et al., 1998). It is known for serum proteins to be adsorbed onto the
cement surface, altering the interfacial properties of the calcium phosphate crystals
(Giocondi et al., 2010), and favoring in vivo resorption (Grover et al., 2003).
Research shows that unlike HA cements that undergo negligible resorption over
time, dicalcium phosphate cements resorb to a much greater extent in vivo (Oberle
et al., 2005; Apelt et al., 2004).
The effect of particle size of the implanted graft materials affects the rate and
effectiveness of cellular resorption activity (Hannink and Arts, 2011). The cells that
take part in cell-mediated calcium phosphate resorption may be osteoclasts, multinucleated giant cells, monocytes, and macrophages directly available in the bone marrow tissue. Phagocytic mechanisms regulated by the monocytes/macrophages or
acidic mechanisms via osteoclasts (by reduction of pH in the microenvironment)
result in bioresorption of calcium phosphate cements in vivo (Heymann et al., 1999).
Macrophages respond to small fragments and particles (,10 μm in diameter) by
internalization via phagocytosis and intracellular digestion (Fig. 15.3). If the particle
size is larger than 10 μm and smaller than 100 μm, the macrophages fuse together
forming giant cells which in turn engulf the particles and digest them (Fig. 15.3)
(Sheikh et al., 2015b). If the particles are larger, the bulk resorption is carried out via
osteoclast-mediated resorption (Sheikh et al., 2015b; Xia and Triffitt, 2006).
As mentioned earlier, the resorption of cement matrix is an important feature
with respect to bone formation at the implanted sites, since it frees up the space
needed for new bone formation ideally without compromising mechanical stability.
The surfaces of dicalcium phosphates have been shown to stimulate osteoblasts
activity (Klammert et al., 2009). The release of growth factors incorporated into
cement matrices has also been used to stimulate the bone formation. Vascular endothelial growth factor (VEGF), PDGF, and receptor activator of nuclear factor jB
ligand (RANKL) are some of the growth factors that have been assessed to enhance
bone regenerative capacity in vivo (Le Nihouannen et al., 2008; Tamimi et al.,
2012b). Bone formation has been observed to be considerably greater with PDGFloaded brushite chitosan scaffolds, as well as with the combination PDGF/VEGF
(De la Riva et al., 2010). RANKL is a growth factor that promotes osteoclast differentiation and is important toward the biodegradation of calcium phosphate grafts
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
365
Figure 15.3 (A) Macrophages respond to small fragments and particles (,10 μm in
diameter) by internalization via phagocytosis and intracellular digestion. (B) If the particle
size is larger than 10 μm and smaller than 100 μm, the macrophages fuse together forming
giant cells which in turn engulf the particles and digest them. (C) If the particles are larger,
the bulk digestion is carried out via extracellular degradation by macrophages and
macrophage fused giant cells through release of enzymes and/or pH lowering mechanisms.
(Silva and Branco, 2010). Results from studies suggest that the application of
growth factors using biodegradable materials could improve the tissue response and
promote bone formation in bone regeneration applications (Le Nihouannen et al.,
2008).
15.6
Future of bone tissue graft materials
There is an increasing demand to replace or restore the function of lost, damaged
human bone. Autologous bone grafts remain the gold standard for bone reconstruction, particularly in large bone defects; however, due to their limited supply and
other drawbacks, alternative strategies are essentially required to regenerate and/or
restore bone. In the past several decades, there has been tremendous research activity in the field of bone engineering and increased understanding of bone biology
that has translated into the development of new possible approaches to regenerate
bone. Despite all these vast advancements in the field of bone tissue engineering,
the development of synthetic bone graft materials for maxillofacial and periodontal
applications remains a challenge from a biological, engineering, and surgical
perspective.
Possibly one of the biggest challenges facing bone tissue engineering is fabricating a mechanically strong porous interconnected scaffold that promotes favorable
host integration and proper vascularization. Currently, most of the synthetic grafts
366
Advanced Dental Biomaterials
experience bone tissue regeneration that is limited to the outer surface layers of the
biomaterial upon implantation, as a result of insufficient vascularization of the scaffold. Therefore there is a need to investigate the complex biological parameters to
be considered when designing the synthetic materials for proper bone regeneration
and vascularization (e.g., pore size, porosity, resorption rate). Moreover, the interplay between inflammatory response, cells and the biomaterial surface, and other
molecules involved in the bone formation/bone resorption pathways is far from
being fully understood. One approach to tackle this problem would be the incorporation of immunomodulatory strategies to modulate the host’s foreign-body
response (i.e., fibrous tissue encapsulation). In addition, further investigation is
needed to understand how endogenously or exogenously supplied growth factors
with the grafting material can promote favorable cellular differentiation and reproduction as well as inhibit unfavorable inflammatory reactions. The challenges in the
field are further compounded by the high cost of some of the synthetic alternatives
and the lack of strong evidence (i.e., lack of randomized controlled human studies),
thus being scarcely recommendable for clinical use. Accordingly, the future of bone
tissue engineering primarily depends on the ability of clinicians, researchers, and
engineers to communicate together to overcome the previous hurdles and fabricate
an optimal clinically relevant graft with the best possible clinical outcomes, and the
lowest possible morbidity and cost.
References
Agrawal, C.M., Athanasiou, K.A., 1997. Technique to control pH in vicinity of biodegrading
PLA-PGA implants. J. Biomed. Mater. Res. 38, 105 114.
Alghamdi, A.S., Shibly, O., Ciancio, S.G., 2010. Osseous grafting part II: xenografts and
alloplasts for periodontal regeneration—a literature review. J. Int. Acad. Periodontol. 12,
39 44.
Al Ruhaimi, K.A., 2001. Bone graft substitutes: a comparative qualitative histologic review
of current osteoconductive grafting materials. Int. J. Oral Maxillofac. Implants 16,
105 114.
Aludden, H., Mordenfeld, A., Hallman, M., Dahlin, C., Jensen, T., 2017. Lateral ridge augmentation with Bio-Oss alone or Bio-Oss mixed with particulate autogenous bone graft:
a systematic review. Int. J. Oral Maxillofac. Surg. 46, 1030 1038.
Anderson, J.M., 1988. Inflammatory response to implants. ASAIO J. 34, 101 107.
Apelt, D., Theiss, F., El-Warrak, A.O., Zlinszky, K., Bettschart-Wolfisberger, R., Bohner,
M., et al., 2004. In vivo behavior of three different injectable hydraulic calcium phosphate cements. Biomaterials 25, 1439 1451.
Araujo, P.P., Oliveira, K.P., Montenegro, S.C., Carreiro, A.F., Silva, J.S., Germano, A.R.,
2013. Block allograft for reconstruction of alveolar bone ridge in implantology: a systematic review. Implant. Dent. 22, 304 308.
Asghari, F., Samiei, M., Adibkia, K., Akbarzadeh, A., Davaran, S., 2017. Biodegradable and
biocompatible polymers for tissue engineering application: a review. Artif. Cells
Nanomed. Biotechnol. 45, 185 192.
Bagambisa, F.B., Joos, U., Schilli, W., 1993. Mechanisms and structure of the bond between
bone and hydroxyapatite ceramics. J. Biomed. Mater. Res. A 27, 1047 1055.
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
367
Berglundh, T., Lindhe, J., 1997. Healing around implants placed in bone defects treated
with Bio-Osss. An experimental study in the dog. Clin. Oral. Implants. Res. 8,
117 124.
Blaggana, V., Gill, A.S., Blaggana, A., 2014. A clinical and radiological evaluation of the
relative efficacy of demineralized freeze-dried bone allograft versus anorganic bovine
bone xenograft in the treatment of human infrabony periodontal defects: a 6 months
follow-up study. J. Indian Soc. Periodontol. 18, 601 607.
Block, M.S., Degen, M., 2004. Horizontal ridge augmentation using human mineralized particulate bone: preliminary results. J. Oral Maxillofac. Surg. 62, 67 72.
Boyne, P.J., 1988. Bone induction and the use of HTR polymer as a vehicle for osseous
inductor materials. Compend. Suppl. S337 S341.
Brar, H.S., Platt, M.O., Sarntinoranont, M., Martin, P.I., Manuel, M.V., 2009. Magnesium as
a biodegradable and bioabsorbable material for medical implants. JOM 61, 31 34.
Buck, B., Malinin, T.I., Brown, M.D., 1989. Bone transplantation and human immunodeficiency virus: an estimate of risk of acquired immunodeficiency syndrome (AIDS). Clin.
Orthop. Relat. Res. 240, 129 136.
Canullo, L., Trisi, P., Simion, M., 2006. Vertical ridge augmentation around implants using
e-PTFE titanium-reinforced membrane and deproteinized bovine bone mineral (bio-oss):
a case report. Int. J. Periodontics. Restorative. Dent. 26, 355 361.
Carvalho, S.M., Oliveira, A.A., Jardim, C.A., Melo, C., Gomes, D.A., Leite, M., et al., 2012.
Characterization and induction of cementoblast cell proliferation by bioactive glass
nanoparticles. J. Tissue Eng. Regen. Med. 6, 813 821.
Chen, X.R., Bai, J., Yuan, S.J., Yu, C.X., Huang, J., Zhang, T.L., et al., 2015. Calcium phosphate nanoparticles are associated with inorganic phosphate-induced osteogenic differentiation of rat bone marrow stromal cells. Chem. Biol. Interact. 238, 111 117.
Cho, B.C., Chung, H.Y., Lee, D.G., Yang, J.D., Park, J.W., Roh, K.H., et al., 2005. The
effect of chitosan bead encapsulating calcium sulfate as an injectable bone substitute on
consolidation in the mandibular distraction osteogenesis of a dog model. J. Oral
Maxillofac. Surg. 63, 1753 1764.
Committee On Research, S, 2001. Tissue banking of bone allografts used in periodontal
regeneration. J. Periodontol. 72, 834.
Constantz, B.R., Barr, B.M., Ison, I.C., Fulmer, M.T., Baker, J., Mckinney, L., et al., 1998.
Histological, chemical, and crystallographic analysis of four calcium phosphate cements
in different rabbit osseous sites. J. Biomed. Mater. Res. 43, 451 461.
Contar, C.M., Sarot, J.R., Bordini JR., J., Galvao, G.H., Nicolau, G.V., Machado, M.A.,
2009. Maxillary ridge augmentation with fresh-frozen bone allografts. J. Oral
Maxillofac. Surg. 67, 1280 1285.
Contar, C.M., Sarot, J.R., Da Costa, M.B., Bordini, J., De Lima, A.A., et al., 2011. Freshfrozen bone allografts in maxillary ridge augmentation: histologic analysis. J. Oral
Implantol. 37, 223 231.
Cornell, C.N., Lane, J.M., 1998. Current understanding of osteoconduction in bone regeneration. Clin. Orthop. Relat. Res. 355, S267 S273.
Cypher, T.J., Grossman, J.P., 1996. Biological principles of bone graft healing. J. Foot Ankle
Surg. 35, 413 417.
De Groot, K., 1980. Bioceramics consisting of calcium phosphate salts. Biomaterials 1,
47 50.
De La Riva, B., Sanchez, E., Hernandez, A., Reyes, R., Tamimi, F., Lopez-Cabarcos, E.,
et al., 2010. Local controlled release of VEGF and PDGF from a combined brushitechitosan system enhances bone regeneration. J. Control Release 143, 45 52.
368
Advanced Dental Biomaterials
Denissen, H., Van Beek, E., Martinetti, R., Klein, C., Van Der Zee, E., Ravaglioli, A., 1997.
Net-shaped hydroxyapatite implants for release of agents modulating periodontal-like
tissues. J. Periodontal Res. 32, 40 46.
Dias, R.R., Sehn, F.P., De Santana Santos, T., Silva, E.R., Chaushu, G., Xavier, S.P., 2014.
Corticocancellous fresh-frozen allograft bone blocks for augmenting atrophied posterior
mandibles in humans. Clin. Oral Implants Res. 27 (1), 39 46.
Dodson, S.A., Bernard, G.W., Kenney, E.B., Carranza, F.A., 1996. In vitro comparison of
aged and young osteogenic and hemopoietic bone marrow stem cells and their derivative
colonies. J. Periodontol. 67, 184 196.
Dorozhkin, S.V., 2009. Calcium orthophosphates in nature, biology and medicine. Materials
2, 399 498.
Dorozhkin, S.V., Epple, M., 2002. Biological and medical significance of calcium phosphates. Angew. Chem. Int. Ed. 41, 3130 3146.
Draenert, F.G., Huetzen, D., Neff, A., Mueller, W.E., 2014. Vertical bone augmentation procedures: basics and techniques in dental implantology. J. Biomed. Mater. Res. A 102,
1605 1613.
El Sayegh, T.Y., Pilliar, R.M., Mcculloch, C.A., 2002. Attachment, spreading, and matrix
formation by human gingival fibroblasts on porous-structured titanium alloy and calcium polyphosphate substrates. J. Biomed. Mater. Res. 61, 482 492.
Ewers, R., 2005. Maxilla sinus grafting with marine algae derived bone forming material: a
clinical report of long-term results. J. Oral Maxillofac. Surg. 63, 1712 1723.
Felice, P., Marchetti, C., Iezzi, G., Piattelli, A., Worthington, H., Pellegrino, G., et al., 2009.
Vertical ridge augmentation of the atrophic posterior mandible with interpositional bloc
grafts: bone from the iliac crest vs. bovine anorganic bone. Clinical and histological
results up to one year after loading from a randomized-controlled clinical trial. Clin.
Oral Implants Res. 20, 1386 1393.
Fernández, E., Gil, F., Ginebra, M., Driessens, F., Planell, J., Best, S., 1999. Production and
characterization of new calcium phosphate bone cements in the CaHPOv 4 α-Ca 3 (PO
4) 2 system: pH, workability and setting times. J. Mater. Sci.: Mater. Med. 10,
223 230.
Festa, V.M., Addabbo, F., Laino, L., Femiano, F., Rullo, R., 2013. Porcine-derived xenograft
combined with a soft cortical membrane versus extraction alone for implant site development: a clinical study in humans. Clin. Implant Dent Relat. Res. 15, 707 713.
Finkemeier, C.G., 2002. Bone-grafting and bone-graft substitutes. J. Bone Joint Surg. 84,
454 464.
Frayssinet, P., Gineste, L., Rouquet, N., 1998. Osteointegration of different kinds of calcium
phosphate biomaterials: ceramics and hydraulic cements. Morphologie 82, 3 7.
Friedlaender, G.E., Strong, D.M., Sell, K.W., 1976. Studies on the antigenicity of bone. I.
Freeze-dried and deep-frozen bone allografts in rabbits. J. Bone Joint Surg. Am. 58,
854 858.
Froum, S.J., 1996. Human histologic evaluation of HTR polymer and freeze-dried bone allograft. A case report. J. Clin. Periodontol. 23, 615 620.
Gbureck, U., Hölzel, T., Klammert, U., Würzler, K., Müller, F.A., Barralet, J.E., 2007.
Resorbable dicalcium phosphate bone substitutes prepared by 3D powder printing. Adv.
Funct. Mater. 17, 3940 3945.
Gehrke, S., Famà, G., 2010. Buccal dehiscence and sinus lift cases predictable bone augmentation with synthetic bone material. Implants 11, 4.
Giocondi, J.L., El-Dasher, B.S., Nancollas, G.H., Orme, C.A., 2010. Molecular mechanisms
of crystallization impacting calcium phosphate cements. Philos. Trans. R. Soc. Lond. A:
Math. Phys. Eng. Sci. 368, 1937 1961.
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
369
Gooptu, B., Lomas, D.A., 2008. Polymers and inflammation: disease mechanisms of the serpinopathies. J. Exp. Med. 205, 1529 1534.
Grover, L.M., Knowles, J.C., Fleming, G.J.P., Barralet, J.E., 2003. In vitro ageing of brushite
calcium phosphate cement. Biomaterials. 24, 4133 4141.
Grynpas, M.D., Pilliar, R.M., Kandel, R.A., Renlund, R., Filiaggi, M., Dumitriu, M., 2002.
Porous calcium polyphosphate scaffolds for bone substitute applications in vivo studies.
Biomaterials 23, 2063 2070.
Hall, J.E., 2015. Guyton and Hall Textbook of Medical Physiology e-Book. Elsevier Health
Sciences.
Hall, E.E., Meffert, R.M., Hermann, J.S., Mellonig, J.T., Cochran, D.L., 1999. Comparison
of bioactive glass to demineralized freeze-dried bone allograft in the treatment of intrabony defects around implants in the canine mandible. J. Periodontol. 70, 526 535.
Hannink, G., Arts, J.C., 2011. Bioresorbability, porosity and mechanical strength of bone
substitutes: what is optimal for bone regeneration? Injury 42, S22 S25.
Hench, L.L., 1998. Bioactive materials: the potential for tissue regeneration. J. Biomed.
Mater. Res. 41, 511 518.
Heymann, D., Pradal, G., Benahmed, M., 1999. Cellular mechanisms of calcium phosphate
ceramic degradation. Histol. Histopathol. 14, 871 877.
Hollinger, J., Chaudhari, A., 1992. Bone regeneration materials for the mandibular and craniofacial complex. Cells Mater. 2, 143 151.
Hopp, S.G., Dahners, L.E., Gilbert, J.A., 1989. A study of the mechanical strength of long
bone defects treated with various bone autograft substitutes: an experimental investigation in the rabbit. J. Orthop. Res. 7, 579 584.
Hutmacher, D.W., Kirsch, A., Ackermann, K.L., Hürzeler, M.B., 2001. A tissue engineered
cell-occlusive device for hard tissue regeneration—a preliminary report. Int. J.
Periodontics Restorative Dent. 21, 49 59.
Idowu, B., Cama, G., Deb, S., Di Silvio, L., 2014. In vitro osteoinductive potential of porous
monetite for bone tissue engineering. J. Tissue Eng. 5, 1 8. 2041731414536572.
Jackson, I.T., Helden, G., Marx, R., 1986. Skull bone grafts in maxillofacial and craniofacial
surgery. J. Oral Maxillofac. Surg. 44, 949 955.
Jacotti, M., Wang, H.L., Fu, J.H., Zamboni, G., Bernardello, F., 2012. Ridge augmentation
with mineralized block allografts: clinical and histological evaluation of 8 cases treated
with the 3-dimensional block technique. Implant. Dent. 21, 444 448.
Jarcho, M., 1981. Calcium phosphate ceramics as hard tissue prosthetics. Clin. Orthop. Relat.
Res. 157, 259 278.
Jergesen, H.E., Chua, J., Kao, R.T., Kaban, L.B., 1991. Age effects on bone induction by
demineralized bone powder. Clin. Orthop. Relat. Res. 253 259.
Jonck, L., Grobbelaar, C., Strating, H., 1989. Biological evaluation of glass-ionomer cement
(Ketac-0) as an interface material in total joint replacement. A screening test. Clin.
Mater. 4, 201 224.
Klammert, U., Reuther, T., Jahn, C., Kraski, B., Kubler, A.C., Gbureck, U., 2009.
Cytocompatibility of brushite and monetite cell culture scaffolds made by threedimensional powder printing. Acta Biomater. 5, 727 734.
Klein, C.P., Driessen, A.A., De Groot, K., Van Den Hooff, A., 1983. Biodegradation behavior of
various calcium phosphate materials in bone tissue. J. Biomed. Mater. Res. 17, 769 784.
Klein-Nulend, J., Bacabac, R., Mullender, M., 2005. Mechanobiology of bone tissue. Pathol.
Biol. 53, 576 580.
Knapp, C.I., Feuille, F., Cochran, D.L., Mellonig, J.T., 2003. Clinical and histologic evaluation of bone-replacement grafts in the treatment of localized alveolar ridge defects. Part
2: Bioactive glass particulate. Int. J. Periodontics Restorative Dent. 23, 1 12.
370
Advanced Dental Biomaterials
Kuemmerle, J.M., Oberle, A., Oechslin, C., Bohner, M., Frei, C., Boecken, I., et al., 2005.
Assessment of the suitability of a new brushite calcium phosphate cement for cranioplasty an experimental study in sheep. J. Cranio-Maxillofac. Surg. 33, 37 44.
Kukreja, B.J., Dodwad, V., Kukreja, P., Ahuja, S., Mehra, P., 2014. A comparative evaluation of platelet-rich plasma in combination with demineralized freeze-dried bone allograft and DFDBA alone in the treatment of periodontal intrabony defects: a
clinicoradiographic study. J. Indian Soc. Periodontol. 18, 618 623.
Le Nihouannen, D., Hacking, S.A., Gbureck, U., Komarova, S.V., Barralet, J.E., 2008. The
use of RANKL-coated brushite cement to stimulate bone remodelling. Biomaterials 29,
3253 3259.
Lewandrowski, K.U., Gresser, J.D., Wise, D.L., Trantolo, D.J., 2000. Bioresorbable bone
graft substitutes of different osteoconductivities: a histologic evaluation of osteointegration of poly(propylene glycol-co-fumaric acid)-based cement implants in rats.
Biomaterials 21, 757 764.
Li, Z., Gu, X., Lou, S., Zheng, Y., 2008. The development of binary Mg-Ca alloys for use as
biodegradable materials within bone. Biomaterials 29, 1329 1344.
Liu, X., Li, Q., Wang, F., Wang, Z., 2016. Maxillary sinus floor augmentation and dental
implant placement using dentin matrix protein-1 gene-modified bone marrow stromal
cells mixed with deproteinized boving bone: a comparative study in beagles. Arch. Oral.
Biol. 64, 102 108.
Lu, J., Gallur, A., Flautre, B., Anselme, K., Descamps, M., Thierry, B., et al., 1998.
Comparative study of tissue reactions to calcium phosphate ceramics among cancellous,
cortical, and medullar bone sites in rabbits. J. Biomed. Mater. Res. 42, 357 367.
Lu, J.X., About, I., Stephan, G., Van Landuyt, P., Dejou, J., Fiocchi, M., et al., 1999.
Histological and biomechanical studies of two bone colonizable cements in rabbits.
Bone 25, 41S 45S.
Lyford, R.H., Mills, M.P., Knapp, C.I., Scheyer, E.T., Mellonig, J.T., 2003. Clinical evaluation of freeze-dried block allografts for alveolar ridge augmentation: a case series. Int. J.
Periodontics Restorative Dent. 23, 417 425.
Macedo, L.G., Mazzucchelli-Cosmo, L.A., Macedo, N.L., Monteiro, A.S., Sendyk, W.R.,
2012. Fresh-frozen human bone allograft in vertical ridge augmentation: clinical and
tomographic evaluation of bone formation and resorption. Cell. Tissue Bank 13,
577 586.
Maragos, P., Bissada, N.F., Wang, R., Cole, B.P., 2002. Comparison of three methods using
calcium sulfate as a graft/barrier material for the treatment of Class II mandibular molar
furcation defects. Int. J. Periodontics Restorative Dent. 22, 493 501.
Markou, N., Pepelassi, E., Vavouraki, H., Stamatakis, H.C., Nikolopoulos, G., Vrotsos, I.,
et al., 2009. Treatment of periodontal endosseous defects with platelet-rich plasma alone
or in combination with demineralized freeze-dried bone allograft: a comparative clinical
trial. J. Periodontol. 80, 1911 1919.
Mastrogiacomo, M., Scaglione, S., Martinetti, R., Dolcini, L., Beltrame, F., Cancedda, R.,
et al., 2006. Role of scaffold internal structure on in vivo bone formation in macroporous calcium phosphate bioceramics. Biomaterials 27, 3230 3237.
Mcallister, B.S., Haghighat, K., 2007. Bone augmentation techniques. J. Periodontol. 78,
377 396.
Mcallister, B.S., Margolin, M.D., Cogan, A.G., Buck, D., Hollinger, J.O., Lynch, S.E., 1999.
Eighteen-month radiographic and histologic evaluation of sinus grafting with anorganic
bovine bone in the chimpanzee. Int. J. Oral Maxillofac. Implants 14, 361 368.
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
371
Meffert, R.M., Thomas, J.R., Hamilton, K.M., Brownstein, C.N., 1985. Hydroxylapatite as an
alloplastic graft in the treatment of human periodontal osseous defects. J. Periodontol.
56, 63 73.
Meijer, G.J., De Bruijn, J.D., Koole, R., Van Blitterswijk, C.A., 2008. Cell based bone tissue
engineering in jaw defects. Biomaterials 29, 3053 3061.
Mellonig, J.T., 1991. Freeze-dried bone allografts in periodontal reconstructive surgery.
Dent. Clin. North Am. 35, 505 520.
Mellonig, J.T., 2000. Human histologic evaluation of a bovine-derived bone xenograft in the
treatment of periodontal osseous defects. Int. J. Periodontics Restorative Dent. 20,
19 29.
Mellonig, J.T., Bowers, G.M., Bailey, R.C., 1981. Comparison of bone graft materials. Part I.
New bone formation with autografts and allografts determined by Strontium-85. J.
Periodontol. 52, 291 296.
Merli, M., Lombardini, F., Esposito, M., 2010. Vertical ridge augmentation with autogenous
bone grafts 3 years after loading: resorbable barriers versus titanium-reinforced barriers.
A randomized controlled clinical trial. Int. J. Oral Maxillofac. Implants 25, 801 807.
Metsger, D.S., Driskell, T., Paulsrud, J., 1982. Tricalcium phosphate ceramic—a resorbable
bone implant: review and current status. J. Am. Dent. Assoc. 105, 1035 1038.
Misch, C.M., 1997. Comparison of intraoral donor sites for onlay grafting prior to implant
placement. Int. J. Oral Maxillofac. Implants 12, 767 776.
Moore, W.R., Graves, S.E., Bain, G.I., 2001. Synthetic bone graft substitutes. ANZ. J. Surg.
71, 354 361.
Murphy, K.G., Gunsolley, J.C., 2003. Guided tissue regeneration for the treatment of periodontal intrabony and furcation defects. A systematic review. Ann. Periodontol. 8,
266 302.
Murray, V.K., 1988. Clinical applications of HTR polymer in periodontal surgery. Compend.
Suppl. 10, S342 S347.
Nakajima, Y., Fiorellini, J.P., Kim, D.M., Weber, H.P., Dent, M., 2007. Regeneration of standardized mandibular bone defects using expanded polytetrafluoroethylene membrane
and various bone fillers. Int. J. Periodontics Restorative Dent. 27, 151.
Nannmark, U., Sennerby, L., 2008. The bone tissue responses to prehydrated and collagenated cortico-cancellous porcine bone grafts: a study in rabbit maxillary defects. Clin.
Implant. Dent. Relat. Res. 10, 264 270.
Nelson, S.R., Wolford, L.M., Lagow, R.J., Capano, P.J., Davis, W.L., 1993. Evaluation of
new high-performance calcium polyphosphate bioceramics as bone graft materials. J.
Oral Maxillofac. Surg. 51, 1363 1371.
Nevins, M.L., Camelo, M., Nevins, M., King, C.J., Oringer, R.J., Schenk, R.K., et al., 2000.
Human histologic evaluation of bioactive ceramic in the treatment of periodontal osseous defects. Int. J. Periodontics Restorative Dent. 20, 458 467.
Nkenke, E., Weisbach, V., Winckler, E., Kessler, P., Schultze-Mosgau, S., Wiltfang, J., et al.,
2004. Morbidity of harvesting of bone grafts from the iliac crest for preprosthetic augmentation procedures: a prospective study. Int. J. Oral Maxillofac. Surg. 33, 157 163.
Nyan, M., Miyahara, T., Noritake, K., Hao, J., Rodriguez, R., Kasugai, S., 2014. Feasibility
of alpha tricalcium phosphate for vertical bone augmentation. J. Investig. Clin. Dent. 5,
109 116.
Oberle, A., Theiss, F., Bohner, M., Muller, J., Kastner, S.B., Frei, C., et al., 2005.
Investigation about the clinical use of brushite-and hydroxylapatite-cement in sheep.
Schweiz. Arch. Tierheilkd. 147, 482 490.
372
Advanced Dental Biomaterials
Osborn, J., Newesely, H., 1980. The material science of calcium phosphate ceramics.
Biomaterials 1, 108 111.
Paolantonio, M., Perinetti, G., Dolci, M., Perfetti, G., Tetè, S., Sammartino, G., et al., 2008.
Surgical treatment of periodontal intrabony defects with calcium sulfate implant and
barrier versus collagen barrier or open flap debridement alone: a 12-month randomized
controlled clinical trial. J. Periodontol. 79, 1886 1893.
Pearce, A., Richards, R., Milz, S., Schneider, E., Pearce, S., 2007. Animal models for implant
biomaterial research in bone: a review. Eur. Cell. Mater. 13, 1 10.
Pecora, G., Andreana, S., Margarone, J.E., Covani, U., Sottosanti, J.S., 1997. Bone regeneration with a calcium sulfate barrier. Oral Surg. Oral Med. Oral Pathol. Oral Radiol.
Endodontol. 84, 424 429.
Pilliar, R.M., Filiaggi, M.J., Wells, J.D., Grynpas, M.D., Kandel, R.A., 2001. Porous calcium
polyphosphate scaffolds for bone substitute applications—in vitro characterization.
Biomaterials 22, 963 972.
Pilliar, R.M., Kandel, R.A., Grynpas, M.D., Theodoropoulos, J., Hu, Y., Allo, B., et al.,
2016. Calcium polyphosphate particulates for bone void filler applications. J. Biomed.
Mater. Res. B. Appl. Biomater. 105 (4), 874 884.
Pioletti, D.P., Takei, H., Lin, T., Van Landuyt, P., Ma, Q.J., Kwon, S.Y., et al., 2000. The
effects of calcium phosphate cement particles on osteoblast functions. Biomaterials 21,
1103 1114.
Proussaefs, P., Lozada, J., Rohrer, M.D., 2002. A clinical and histologic evaluation of a block
onlay graft in conjunction with autogenous particulate and inorganic bovine mineral
(Bio-Oss): a case report. Int. J. Periodontics Restorative Dent. 22, 567 574.
Proussaefs, P., Lozada, J., Kleinman, A., Rohrer, M.D., Mcmillan, P.J., 2003. The use of titanium mesh in conjunction with autogenous bone graft and inorganic bovine bone mineral (Bio-Oss) for localized alveolar ridge augmentation: a human study. Int. J.
Periodontics Restorative Dent. 23, 185 195.
Quattlebaum, J.B., Mellonig, J.T., Hensel, N.F., 1988. Antigenicity of freeze-dried cortical
bone allograft in human periodontal osseous defects. J. Periodontol. 59, 394 397.
Rabalais J.R., M.L., Yukna, R.A., Mayer, E.T., 1981. Evaluation of durapatite ceramic as an
alloplastic implant in periodontal osseous defects. I. Initial six-month results. J.
Periodontol. 52, 680 689.
Ratner, B.D., 2004. Biomaterials Science: An Introduction to Materials in Medicine.
Academic Press.
Renooij, W., Hoogendoorn, H.A., Visser, W.J., Lentferink, R.H., Schmitz, M.G., Van
Ieperen, H., et al., 1985. Bioresorption of ceramic strontium-85-labeled calcium phosphate implants in dog femora: a pilot study to quantitate bioresorption of ceramic
implants of hydroxyapatite and tricalcium orthophosphate in vivo. Clin. Orthop. Relat.
Res. 197, 272 285.
Ricci, J.L., Blumenthal, N.C., Spivak, J.M., Alexander, H., 1992. Evaluation of a lowtemperature calcium phosphate particulate implant material: physical-chemical properties and in vivo bone response. J. Oral Maxillofac. Surg. 50, 969 978.
Rocchietta, I., Simion, M., Hoffmann, M., Trisciuoglio, D., Benigni, M., Dahlin, C., 2015.
Vertical bone augmentation with an autogenous block or particles in combination with
guided bone regeneration: a clinical and histological preliminary study in humans. Clin.
Implant. Dent. Relat. Res. 18 (1), 19 29.
Roy, D.M., Linnehan, S.K., 1974. Hydroxyapatite Formed From Coral Skeletal Carbonate by
Hydrothermal Exchange. 247 (5438), p. 220.
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
373
Russell, J., Scarborough, N., Chesmel, K., 1997. Ability of commercial demineralized freezedried bone allograft to induce new bone formation. J. Periodontol. 68, 804 806.
Scarano, A., Degidi, M., Iezzi, G., Pecora, G., Piattelli, M., Orsini, G., et al., 2006. Maxillary
sinus augmentation with different biomaterials: a comparative histologic and histomorphometric study in man. Implant. Dent. 15, 197 207.
Schallhorn, R.G., Hiatt, W.H., Boyce, W., 1970. Iliac transplants in periodontal therapy. J.
Periodontol. 41, 566 580.
Schepers, E.J., Ducheyne, P., 1997. Bioactive glass particles of narrow size range for the
treatment of oral bone defects: a 1-24 month experiment with several materials and particle sizes and size ranges. J. Oral Rehabil. 24, 171 181.
Schepers, E., De Clercq, M., Ducheyne, P., Kempeneers, R., 1991. Bioactive glass particulate
material as a filler for bone lesions. J. Oral Rehabil. 18, 439 452.
Seal, C., Vince, K., Hodgson, M., 2009. Biodegradable surgical implants based on magnesium alloys—a review of current research. IOP Conference Series: Materials Science
and Engineering. IOP Publishing, 012011.
Shalash, M.A., Rahman, H.A., Azim, A.A., Neemat, A.H., Hawary, H.E., Nasry, S.A., 2013.
Evaluation of horizontal ridge augmentation using beta tricalcium phosphate and demineralized bone matrix: a comparative study. J. Clin. Exp. Dent. 5, e253 e259.
Sheikh, Z., Javaid, M.A., Abdallah, M.N., 2013. Bone replacement graft materials in dentistry. In: Khurshid, Z.S.Z. (Ed.), Dental Biomaterials (Principle and Its Application),
second ed. Paramount Publishing Enterprise.
Sheikh, Z., Abdallah, M.N., Hamdan, N., Javaid, M.A., Khurshid, Z., 2014. Barrier membranes
for tissue regeneration and bone augmentation techniques in dentistry. In: Matilinna, K.P.
(Ed.), Handbook of Oral Biomaterials. Pan Stanford Publishing, Singapore.
Sheikh, Z., Abdallah, M.-N., Hanafi, A.A., Misbahuddin, S., Rashid, H., Glogauer, M.,
2015a. Mechanisms of in vivo degradation and resorption of calcium phosphate based
biomaterials. Materials 8, 7913 7925.
Sheikh, Z., Brooks, P.J., Barzilay, O., Fine, N., Glogauer, M., 2015b. Macrophages, foreign
body giant cells and their response to implantable biomaterials. Materials 8, 5671 5701.
Sheikh, Z., Geffers, M., Christel, T., Barralet, J.E., Gbureck, U., 2015c. Chelate setting of
alkali ion substituted calcium phosphates. Ceram. Int. 41 (8), 10010 10017.
Sheikh, Z., Najeeb, S., Khurshid, Z., Verma, V., Rashid, H., Glogauer, M., 2015d.
Biodegradable materials for bone repair and tissue engineering applications. Materials 8,
5744 5794.
Sheikh, Z., Sima, C., Glogauer, M., 2015e. Bone replacement materials and techniques used
for achieving vertical alveolar bone augmentation. Materials 8, 2953 2993.
Sheikh, Z., Zhang, Y.L., Grover, L., Merle, G.E., Tamimi, F., Barralet, J., 2015f. In vitro
degradation and in vivo resorption of dicalcium phosphate cement based grafts. Acta
Biomater. 26, 338 346.
Sheikh, Z., Drager, J., Zhang, Y.L., Abdallah, M.N., Tamimi, F., Barralet, J., 2016.
Controlling bone graft substitute microstructure to improve bone augmentation. Adv.
Healthc. Mater. 5 (13), 1646 1655.
Sheikh, Z., Hamdan, N., Ikeda, Y., Grynpas, M., Ganss, B., Glogauer, M., 2017a. Natural
graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive
applications: a review. Biomater. Res. 21, 9.
Sheikh, Z., Qureshi, J., Alshahrani, A.M., Nassar, H., Ikeda, Y., Glogauer, M., et al., 2017b.
Collagen based barrier membranes for periodontal guided bone regeneration applications. Odontology 105, 1 12.
374
Advanced Dental Biomaterials
Sheikh, Z., Zhang, Y.L., Tamimi, F., Barralet, J., 2017c. Effect of processing conditions of
dicalcium phosphate cements on graft resorption and bone formation. Acta Biomater.
53, 526 535.
Shetty, V., Han, T.J., 1991. Alloplastic materials in reconstructive periodontal surgery. Dent.
Clin. North Am. 35, 521 530.
Shikinami, Y., Okuno, M., 1999. Bioresorbable devices made of forged composites of
hydroxyapatite (HA) particles and poly-L-lactide (PLLA): Part I. Basic characteristics.
Biomaterials 20, 859 877.
Shue, L., Yufeng, Z., Mony, U., 2012. Biomaterials for periodontal regeneration: a review of
ceramics and polymers. Biomatter 2, 271 277.
Silva, I., Branco, J., 2010. Rank/Rankl/opg: literature review. Acta Reumatol. Port. 36,
209 218.
Simion, M., Fontana, F., 2004. Autogenous and xenogeneic bone grafts for the bone regeneration. A literature review. Minerva Stomatol. 53, 191 206.
Simion, M., Jovanovic, S.A., Tinti, C., Benfenati, S.P., 2001. Long-term evaluation of
osseointegrated implants inserted at the time or after vertical ridge augmentation. A retrospective study on 123 implants with 1-5 year follow-up. Clin. Oral Implants Res. 12,
35 45.
Small, S.A., Zinner, I.D., Panno, F.V., Shapiro, H.J., Stein, J.I., 1993. Augmenting the maxillary sinus for implants: report of 27 patients. Int. J. Oral Maxillofac. Implants 8,
523 528.
Sokolsky-Papkov, M., Agashi, K., Olaye, A., Shakesheff, K., Domb, A.J., 2007. Polymer carriers for drug delivery in tissue engineering. Adv. Drug Deliv. Rev. 59, 187 206.
Stahl, S.S., Froum, S.J., Tarnow, D., 1990. Human clinical and histologic responses to the
placement of HTR polymer particles in 11 intrabony lesions. J. Periodontol. 61,
269 274.
Staiger, M.P., Pietak, A.M., Huadmai, J., Dias, G., 2006. Magnesium and its alloys as orthopedic biomaterials: a review. Biomaterials 27, 1728 1734.
Stavropoulos, A., Windisch, P., Szendröi-Kiss, D., Peter, R., Gera, I., Sculean, A., 2010.
Clinical and histologic evaluation of granular beta-tricalcium phosphate for the treatment of human intrabony periodontal defects: a report on five cases. J. Periodontol. 81,
325 334.
Sterio, T.W., Katancik, J.A., Blanchard, S.B., Xenoudi, P., Mealey, B.L., 2013. A prospective, multicenter study of bovine pericardium membrane with cancellous particulate
allograft for localized alveolar ridge augmentation. Int. J. Periodontics Restorative Dent.
33, 499 507.
Sugar, A.W., Thielens, P., Stafford, G.D., Willins, M.J., 1995. Augmentation of the atrophic
maxillary alveolar ridge with hydroxyapatite granules in a Vicryl (polyglactin 910) knitted tube and simultaneous open vestibuloplasty. Br. J. Oral Maxillofac. Surg. 33,
93 97.
Sukumar, S., Drizhal, I., Paulusová, V., Bukac, J., 2011. Surgical treatment of periodontal
intrabony defects with calcium sulphate in combination with beta-tricalcium phosphate:
clinical observations two years post-surgery. Acta Medica (Hradec Kralove) 54, 13 20.
Sunitha Raja, V., Naidu, M., 2008. Platelet-rich fibrin: evolution of a second-generation
platelet concentrate. Indian J. Dent. Res. 19, 42.
Tamimi, F.M., Torres, J., Tresguerres, I., Clemente, C., Lopez-Cabarcos, E., Blanco, L.J.,
2006. Bone augmentation in rabbit calvariae: comparative study between Bio-Oss (R)
and a novel beta-TCP/DCPD granulate. J. Clin. Periodontol. 33, 922 928.
Natural and synthetic bone replacement graft materials for dental and maxillofacial applications
375
Tamimi, F., Torres, J., Kathan, C., Baca, R., Clemente, C., Blanco, L., et al., 2008. Bone
regeneration in rabbit calvaria with novel monetite granules. J. Biomed. Mater. Res. A
87A, 980 985.
Tamimi, F., Torres, J., Lopez-Cabarcos, E., Bassett, D.C., Habibovic, P., Luceron, E., et al.,
2009. Minimally invasive maxillofacial vertical bone augmentation using brushite based
cements. Biomaterials 30, 208 216.
Tamimi, F., Torres, J., Bassett, D., Barralet, J., Cabarcos, E.L., 2010. Resorption of monetite
granules in alveolar bone defects in human patients. Biomaterials 31, 2762 2769.
Tamimi, F., Le Nihouannen, D., Eimar, H., Sheikh, Z., Komarova, S., Barralet, J., 2012a.
The effect of autoclaving on the physical and biological properties of dicalcium phosphate dihydrate bioceramics: brushite vs. monetite. Acta Biomater. 8, 3161 3169.
Tamimi, F., Sheikh, Z., Barralet, J., 2012b. Dicalcium phosphate cements: brushite and monetite. Acta Biomater. 8, 474 487.
Tan, L., Yu, X., Wan, P., Yang, K., 2013. Biodegradable materials for bone repairs: a review.
J. Mater. Sci. Technol. 29, 503 513.
Tevlin, R., Mcardle, A., Atashroo, D., Walmsley, G.G., Senarath-Yapa, K., Zielins, E.R.,
et al., 2014. Biomaterials for craniofacial bone engineering. J. Dent. Res. 93,
1187 1195.
Thaller, S.R., Hoyt, J., Borjeson, K., Dart, A., Tesluk, H., 1993. Reconstruction of calvarial
defects with anorganic bovine bone mineral (Bio-Oss) in a rabbit model. J. Craniofac.
Surg. 4, 79 84.
Urist, M.R., 1980. Bone transplants and implants. In: Mr, U. (Ed.), Fundamental and Clinical
Bone Physiology. JB Lippincott, Philadelphia, PA.
Valentini, P., Abensur, D., 1997. Maxillary sinus floor elevation for implant placement with
demineralized freeze-dried bone and bovine bone (Bio-Oss): a clinical study of 20
patients. Int. J. Periodontics Restorative Dent. 17, 32 45.
Van Der Giessen, W.J., Lincoff, A.M., Schwartz, R.S., Van Beusekom, H.M., Serruys, P.W.,
Holmes, D.R., et al., 1996. Marked inflammatory sequelae to implantation of biodegradable and nonbiodegradable polymers in porcine coronary arteries. Circulation 94,
1690 1697.
Wallace, S.S., Froum, S.J., 2003. Effect of maxillary sinus augmentation on the survival of
endosseous dental implants. A systematic review. Ann. Periodontol. 8, 328 343.
Wallace, S., Gellin, R., 2010. Clinical evaluation of freeze-dried cancellous block allografts for
ridge augmentation and implant placement in the maxilla. Implant. Dent. 19, 272 279.
Wallace, S.S., Froum, S.J., Cho, S.-C., Elian, N., Monteiro, D., Kim, B.S., et al., 2005. Sinus
augmentation utilizing anorganic bovine bone (Bio-Oss) with absorbable and nonabsorbable membranes placed over the lateral window: histomorphometric and clinical analyses. Int. J. Periodontics Restorative Dent. 25, 450 465.
Wang, F.M., Qiu, K., Hu, T., Wan, C.X., Zhou, X.D., Gutmann, J.L., 2006. Biodegradable
porous calcium polyphosphate scaffolds for the three-dimensional culture of dental pulp
cells. Int. Endod. J. 39, 477 483.
Wang, H., Li, Y., Zuo, Y., Li, J., Ma, S., Cheng, L., 2007. Biocompatibility and osteogenesis
of biomimetic nano-hydroxyapatite/polyamide composite scaffolds for bone tissue engineering. Biomaterials 28, 3338 3348.
Weber, J., White, E.W., 1973. Carbonate materials as precursors of new ceramic, metal, and
polymer materials for biomedical applications. Miner. Sci. Eng. 5, 151 165.
Weber, J.N., White, E.W., Lebiedzik, J., 1971. New porous biomaterials by replication of
echinoderm skeletal microstructures. Nature 233, 337 339.
376
Advanced Dental Biomaterials
White, E., Shors, E., 1986. Biomaterial aspects of Interpore-200 porous hydroxyapatite.
Dent. Clin. North Am. 30, 49 67.
Wilk, R., 2004. Bony reconstruction of the jaws. In: Michael, M. (Ed.), Peterson’s Principles
of Oral and Maxillofacial Surgery, second ed. B C Decker, Hamilton (London).
Witte, F., Hort, N., Vogt, C., Cohen, S., Kainer, K.U., Willumeit, R., et al., 2008. Degradable
biomaterials based on magnesium corrosion. Curr. Opin. Solid State Mater. Sci. 12,
63 72.
Wong, R.W., Rabie, A.B., 2006. Effect of Gusuibu graft on bone formation. J. Oral
Maxillofac. Surg. 64, 770 777.
Xia, Z., Triffitt, J.T., 2006. A review on macrophage responses to biomaterials. Biomed.
Mater. 1, R1.
Xynos, I.D., Edgar, A.J., Buttery, L.D., Hench, L.L., Polak, J.M., 2001. Gene-expression profiling of human osteoblasts following treatment with the ionic products of Bioglasss
45S5 dissolution. J. Biomed. Mater. Res. A 55, 151 157.
Yildirim, M., Spiekermann, H., Biesterfeld, S., Edelhoff, D., 2000. Maxillary sinus augmentation using xenogenic bone substitute material Bio-Oss in combination with venous
blood. A histologic and histomorphometric study in humans. Clin. Oral Implants Res.
11, 217 229.
Younger, E.M., Chapman, M.W., 1989. Morbidity at bone graft donor sites. J. Orthop.
Trauma 3, 192 195.
Yukna, R.A., 1990. HTR polymer grafts in human periodontal osseous defects. I. 6-month
clinical results. J. Periodontol. 61, 633 642.
Yukna, R.A., 1994. Clinical evaluation of HTR polymer bone replacement grafts in human
mandibular Class II molar furcations. J. Periodontol. 65, 342 349.
Yukna, R.A., Greer JR., R.O., 1992. Human gingival tissue response to HTR polymer. J.
Biomed. Mater. Res. 26, 517 527.
Zitzmann, N.U., Naef, R., Scharer, P., 1997. Resorbable versus nonresorbable membranes in
combination with Bio-Oss for guided bone regeneration. Int. J. Oral Maxillofac.
Implants 12, 844 852.
16
Calcium orthophosphates as a
dental regenerative material
Sergey V. Dorozhkin
Moscow, Russia
Chapter Outline
16.1
16.2
16.3
16.4
Introduction 377
General definitions and knowledge 383
Brief information on current biomedical applications of CaPO4
CaPO4 for dental caries prevention and in dentifrices 385
16.4.1
16.4.2
16.4.3
16.4.4
385
Toothpastes 386
Chewing gums 389
Teeth remineralization 390
Dentin hypersensitivity treatments 392
16.5 Clinical applications of CaPO4 in dentistry
394
16.5.1 Classification according to the existing CaPO4 395
16.5.2 Classification according to the dental specialties 404
16.6 Tissue engineering approaches
16.7 Conclusion 416
References 416
Further reading 452
16.1
414
Introduction
Dental caries, also known as tooth decay or a cavity, is an infectious disease
(usually of bacterial origin), which causes demineralization and destruction of teeth.
If left untreated, the disease can lead to pain, tooth loss, and infection. Historically,
this disease is very old and it is not exclusive to the human species. Namely, evidence of dental lesions compatible with caries has been observed in creatures as old
as Paleozoic fishes (570250 million years ago), Mesozoic herbivores dinosaurs
(24565 million years ago), prehominines of the Eocene (6025 million years
ago), as well as in the Miocene (255 million years ago), Pliocene (51.6 million
years ago), and Pleistocene animals (1.6 million10,000 years ago). Nowadays
caries is also detected in bears and other wild animals, as well as being common in
domestic animals (Lanfranco and Eggers, 2012). Back to humans, dental caries has
been detected in various epochs and societies throughout the world (Wang et al.,
2008; Bellagarda, 1965; Fujita, 2009; Corbett and Moore, 1971, 1973, 1975, 1976;
Kerr, 1990). Even though in most of the developed countries the prevalence of the
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00016-5
Copyright © 2019 Elsevier Ltd. All rights reserved.
378
Advanced Dental Biomaterials
disease has decreased since the introduction of fluoride for dental care, dental caries
remains a major public health problem.
Very schematically, dental caries occurs as follows. As the most highly mineralized structure in vertebrate bodies, dental enamel is composed of numerous nanodimensional needle-like crystals of ion-substituted calcium orthophosphates (CaPO4)
with the apatitic structure (the so-called biological apatite), which are bundled in
parallel ordered prisms or rods to ensure their unique mechanical strength, remarkable hardness, and biological protection. Nevertheless, all types of teeth possess
some porosity allowing fluids beneath their surface. Organic (mainly, lactic and
acetic) acids, produced by dental plaque cariogenic bacteria (such as Streptococcus
mutans and Lactobacillus) from fermentable carbohydrates of sugar or from the
remaining food debris, initiate the disease. When the sufficient quantity of acids is
produced, so that the solution pH drops below B5.5 (a critical pH), saliva and
plaque fluids cease to be saturated with calcium and orthophosphate ions. Thus
dental enamel begins to be demineralized (dissolved) and the aforementioned pores
become larger (Fig. 16.1A). The demineralization process can be described with a
simplified chemical reaction:
Ca10 ðPO4 Þ6 ðOHÞ2 1 H1 ! Ca21 1 HPO22
4 1 H2 O
As seen from this reaction, enamel dissolution increases concentrations of both
the major ions (calcium and acid orthophosphate) and the minor ones [magnesium,
bicarbonate (not shown)] in the local microenvironment of the caries lesions,
leading to the formation of various types of acidic CaPO4 (LeGeros, 1999;
González-Cabezas, 2010; West and Joiner, 2014). Simultaneously, H1 ions are
consumed which results in the pH increasing. Due to both the accumulation of the
aforementioned ions in saliva and the increasing pH, the demineralization processes
of teeth slow down. Several models were developed to simulate dental caries (Ilie
et al., 2012; Fabregas and Rubinstein, 2014a,b; Yu et al., 2017).
Figure 16.1 Schematic drawings of (A) demineralization and (B) remineralization processes
of dental enamel.
Calcium orthophosphates as a dental regenerative material
379
Luckily, saliva has some restorative functions, acting not only as a buffer, to
reduce the acidity caused by plaque bacteria, but also as the constant source of soluble ions of calcium and orthophosphate (González-Cabezas, 2010; Dowd, 1999).
Therefore upon neutralization of the plaque acids, CaPO4 complexes from saliva
diffuse back into the channels between the depleted enamel rods, replenishing the
supply of the dissolved ions (Fig. 16.1B). Consequently, the surface of dental
tissues is remineralized. Additional application of toothpastes, mouthwashes, mouth
rinses, tooth mousses, etc. assists the remineralization. Thus under normal circumstances, enamel demineralization is compensated for its remineralization. This
dynamic process takes place more or less continually and equally in a favorable
oral environment. However, when the demineralization exceeds the combined
abilities of saliva, toothpastes, mouthwashes, mouth rinses, tooth mousses, etc. to
remineralize, the dental tissues are progressively dissolved and finally break down,
producing dental caries, which look like cavities and/or holes in the teeth
(Fejerskov and Kidd, 2008). An example of cariogenic teeth is shown in Fig. 16.2.
In addition to dental caries, there is dental erosion, which is a chemical wear of
the dental hard tissues without the involvement of bacteria resulting in bulk mineral
loss with a partly demineralized surface of reduced microhardness. Clinical features
are a loss of surface structures with shallow lesions on smooth surfaces and cupping
and flattening of cusps; already in early stages, coronal dentine often is exposed.
Frequently, it is caused by acid-containing drinks and/or food. The acids that cause
erosion are rather strong with an average pH of B2 for the colas, B22.5 for citrus fruits, and B1 for gastric contents. A repeated exposure leads to surface demineralization and, therefore, softening, while the softened surface is susceptible to
loss by abrasion from food or a toothbrush. Repeated cycles of acid exposure lead
to smooth, cupped out cavities. Palatal surfaces of maxillary anterior teeth appear
to be the most susceptible erosion places, although other teeth are also affected.
Currently, dental erosion is considered as one of the main tooth pathologies,
Figure 16.2 Dental caries (teeth decay).
380
Advanced Dental Biomaterials
which is able to cause patient discomfort after periodontal diseases and caries
(West and Joiner, 2014; Eccles, 1979; Lussi, 2006). Filling with artificial materials
is a conventional treatment to repair damaged places. However, secondary caries
frequently arise at the interfaces between the tooth and foreign materials, which
always require restoration replacement (Mjör and Toffenetti, 2000).
Furthermore, there are other reasons why people need restorative dental biomaterials, such as inlays, onlays, crowns, veneers, or bridges. The causes may be of a
medical (decay or periodontal disease), age (population aging), traumatic (accident),
or genetic (disorders) nature. All these causes adversely affect masticator efficiency,
language function, facial esthetics, and even the psychological health. Still other
patients simply wish to change their smile to improve an appearance of their own.
Since no one wants to cover up one’s mouth when smiling, the demand for esthetic,
tooth-colored (invisible) restorations permanently increases (Höland et al., 2008).
Finally, there are dental abrasion and dental attrition processes. The former is
defined as a mechanical removal of hard tissues by the repeated introduction of foreign bodies into the oral cavity that are in contact with the teeth, while the latter is
a physiological wearing out of dental hard tissues though tooth-to-tooth contact,
without an intervention of foreign substances (West and Joiner, 2014).
Therefore due to their visibility, the restorative dental biomaterials are fundamentally different from artificial implants for bone replacements (reviewed in
Dorozhkin, 2015, 2016a). The greatest driving force to develop biomaterials for
dental restoration is to fulfill the customers’ (patients, dentists, and dental technicians) needs. In addition to the esthetic requirements, pressures from the environmental regulations and public apprehension are on the verge of eliminating dental
amalgam as a practical and inexpensive restorative filling material (Widström et al.,
1992). Thus by the late 1990s, amalgam use in several European countries was
phased out. Consequently, development of metal-free restorations with properties
close to natural teeth (with respect to translucency, color, and abrasive behavior) or
even better mechanical properties and better durability than natural teeth has been a
great challenge for many years (Höland et al., 2008).
Briefly, all restorative dental biomaterials must meet the following basic requirements (Höland et al., 2008):
G
G
G
G
They must be durable and biocompatible.
Their optical characteristics (gloss, translucency, and color, in particular) must be comparable to those of natural teeth.
Their mechanical properties (strength and toughness) must meet the requirements of the
indication range (namely, the required strength of an inlay is lower than that of a dental
bridge).
Their wear behavior must be similar to that of natural teeth.
In addition, they should be easily implantable or injectable, which is a critical
requirement for any medical application.
Hence, a selecting problem of the appropriate biomaterials arises. When all material characteristics and clinical factors are considered, bioceramics offer, perhaps, the
best choice for a metal-free dentistry. Namely, bioceramics possess excellent chemical
Calcium orthophosphates as a dental regenerative material
381
durability, wear resistance, biocompatibility, environmental friendliness, and esthetics.
The bioceramic restorations can be used in situations such as treatments of primary caries where inlays can be applied without a more excessive removal of
tooth structure that is associated with amalgam. Besides, bioceramic onlays or
crowns can also be used in place of large amalgam restorations. However, the
widespread use of all-ceramic restorations has been hindered by concerns related
to marginal fracture resistance and clinical longevity. Therefore the goal of dental
bioceramics research is to produce all-ceramic dental restorative systems that
utilize the known advantages of ceramic materials and minimize the existing
disadvantages (Thompson et al., 2007).
Due to the chemical composition, CaPO4 belong to bioceramics but they have
some specific advantages due to a chemical similarity to the inorganic part of both
human and mammalian bones and teeth. This makes CaPO4 the only bioceramics
potentially applicable for remineralization of dental surfaces (Reynolds, 2008).
Owing to these known similarities, dentists have been using CaPO4 in clinical
practice for over a century. Namely, Dr. Junius E. Cravens (18441920) from the
United States proffered creative concepts in pulp capping in the 1870s. He had
the opinion that dentin-like material would be the best to keep the pulp vital.
Therefore Cravens used a CaPO4 powder, which was mixed with lactic acid to low
viscosity. The result was a soluble calcium lactic orthophosphate, which was applied
to the exposed pulp tissue (Cravens, 1876). This pulp capping agent was brought to
the market by the S.S. White Company with the trade name “Lacto-Phosphate of
Lime” (Fig. 16.3) (Pendleton, 1873).
The available CaPO4, their standard abbreviations, and solubility values are
listed in Table 16.1 (Dorozhkin, 2012a,b). Additional details on CaPO4, their properties, and applications are available in the special monographs on the subject
(LeGeros, 1991; Elliott, 1994; Dorozhkin, 2016c). The objective of this overview is
to provide the current state-of-the-art on CaPO4 applications in dentistry and
dentistry-relevant fields.
Figure 16.3 An advertisement of the S.S. White company for “Lacto-Phosphate of Lime”
1873.
Source: Reprinted from Dent. Cosmos 1873, 15, 683.
Table 16.1 Existing calcium orthophosphates (CaPO4) and their major properties (Dorozhkin, 2012, 2016).
Ca/P molar
ratio
Compounds and their
typical abbreviations
Chemical formula
Solubility at
25 C, 2 log (Ks)
Solubility at
25 C, g/L
0.5
0.5
1.0
1.0
Ca(H2PO4)2 H2O
Ca(H2PO4)2
CaHPO4 2H2O
CaHPO4
1.14
1.14
6.59
6.90
B18
B17
B0.088
B0.048
1.33
1.5
1.5
1.22.2
MCPM
MCPA or MCP
DCPD, mineral brushite
DCPA or DCP, mineral
monetite
OCP
α-TCP
β-TCP
ACP
96.6
25.5
28.9
5.57.0
c
B0.0081
B0.0025
B0.0005
c
B512d
1.51.67
CDHA or Ca-def HAe
B85
B0.0094
6.59.5
1.67
1.67
1.67
HA, Hap, or OHAp
FA or FAp
OA, OAp, or OXAf, mineral
voelckerite
TTCP or TetCP, mineral
hilgenstockite
Ca8(HPO4)2(PO4)4 5H2O
α-Ca3(PO4)2
β-Ca3(PO4)2
CaxHy(PO4)z nH2O, n 5 34.5;
1520% H2O
Ca102x(HPO4)x(PO4)62x(OH)22x
(0 , x , 1)
Ca10(PO4)6(OH)2
Ca10(PO4)6F2
Ca10(PO4)6O
116.8
120.0
B69
B0.0003
B0.0002
B0.087
9.512
712
Ca4(PO4)2O
3844
B0.0007
b
2.0
pH stability range in
aqueous solutions at 25 C
0.02.0
a
2.06.0
a
b
b
b
ACP, Amorphous calcium phosphates; CDHA or Ca-def HA, calcium-deficient hydroxyapatite; DCPA or DCP, dicalcium phosphate anhydrous; DCPD, dicalcium phosphate dehydrate; FA or
FAp, fluorapatite; HA, Hap, or OHAp, hydroxyapatite; MCPA or MCP, monocalcium phosphate anhydrous; MCPM, monocalcium phosphate monohydrate; OA, OAp or OXA, oxyapatite; OCP,
octacalcium phosphate; PHA, precipitated HA; TTCP or TetCP, tetracalcium phosphate; α-TCP, α-tricalcium phosphate; β-TCP, β-tricalcium phosphate.
a
Stable at temperatures above 100 C.
b
These compounds cannot be precipitated from aqueous solutions.
c
Cannot be measured precisely. However, the following values were found: 25.7 6 0.1 (pH 5 7.40), 29.9 6 0.1 (pH 5 6.00), 32.7 6 0.1 (pH 5 5.28). The comparative extent of dissolution in
acidic buffer is ACPcα-TCPcβ-TCP . CDHAcHA . FA.
d
Always metastable.
e
Occasionally, it is called “PHA.”
f
Existence of OA remains questionable.
Calcium orthophosphates as a dental regenerative material
16.2
383
General definitions and knowledge
According to Wikipedia, the free encyclopedia:
Dentistry is the branch of medicine that is involved in the study, diagnosis,
prevention, and treatment of diseases, disorders and conditions of the oral cavity,
maxillofacial area and the adjacent and associated structures and their impact on
the human body. The American Dental Association recognizes nine dental
specialties: public health dentistry, endodontics, oral and maxillofacial pathology,
oral and maxillofacial radiology, oral and maxillofacial surgery, orthodontics,
pediatric dentistry, periodontics, prosthodontics, and general dentistry. There are
other dental niches such as oral medicine, dental aesthetics, dental implantation,
and orofacial pain and temporomandibular disorders, some of them are recognized
as dental specialties in other countries. In the European Union, all member states
must recognize the specialties of orthodontics and oral and maxillofacial surgery
(Dentistry).
Now it is necessary to describe briefly all dental specialties and determine in
which of them CaPO4 is used. According to Wikipedia, “Dental public health is
involved in the assessment of dental health needs and improving the dental health
of populations rather than individuals. One of the controversial subjects relating to
dental public health is fluoridation of drinking water” (Dental Public Health). A
search in Scopus database has been performed for papers containing in the title a
combination of terms (keywords) “public health dentistry” 1 “apatite” and “public
health dentistry” 1 “calcium phosphate.” Zero publications have been found for
either case (Table 16.2). Thus this direction has nothing in common with CaPO4.
(odous) “tooth”] deals
Endodontics [from the Greek ε νδo (endo) “inside” and o δoυς
with the tooth pulp and tissues surrounding roots of teeth. If the pulp (this is the
only vascularized connective tissue of teeth, which contains nerves, arterioles,
venules, lymphatic tissue, and fibrous tissue) becomes diseased or injured, endodontic treatment is required to save the tooth (Endodontics). The results of a similar
search (Table 16.2) revealed that CaPO4 is used rarely in endodontics. Oral and
maxillofacial pathology, radiology, and surgery represent “the study, diagnosis,
and sometimes the treatment of oral and maxillofacial related diseases,” “the study
and radiologic interpretation of oral and maxillofacial diseases,” and “extractions,
implants, and facial surgery,” respectively (Specialty dentistry). Only surgery
appears to deal with CaPO4 very rarely (Table 16.2). Furthermore, within these
three dental specialties, one needs to differentiate between “oral” and “maxillofacial” terms. The former term is relevant to the subject of this review, while the latter is undoubtedly irrelevant, since it deals with the treatment of the surrounding
bones. Various CaPO4-based formulations have been proposed for the reconstruction of the contour and discontinuity defects in maxillofacial surgery (Friedman
et al., 1991, 2000; Reddi et al., 1999; Smartt et al., 2005; Kuemmerle et al., 2005;
Luaces-Rey et al., 2009; Tamimi et al., 2009; Abe et al., 2009; Benson and
Djalilian, 2009; Lee et al., 2010a; Singh et al., 2010; Bambakidis et al., 2010;
384
Advanced Dental Biomaterials
Table 16.2 The amount of publications containing the selected keywords in their titles,
found in Scopus database.
Number of publications
Dental specialty
Apatite
Calcium phosphate
Cumulative
Public health dentistry
Endodontics
Oral and maxillofacial pathology
Oral and maxillofacial radiology
Oral and maxillofacial surgery
Orthodontics
Pediatric dentistry
Periodontics
Prosthodontics
0
23
0
0
5
14
0
219
9
0
14
0
0
2
36
0
118
0
0
37
0
0
7
50
0
337
9
427
25
80
5
39
846
249
19
95
2
96
631
676
44
175
7
135
1477
Additional keywords
Dental
Dentistry
Oral
Stomatology
Caries
Totala
a
Duplications are possible.
Huang et al., 2010a; Sanada et al., 2011); however, this subject was contained
within the field of bone grafts (Dorozhkin, 2015, 2016a). Orthodontics, formerly
orthodontia [from Greek o ρθoς (orthos) “straight, or proper, or perfect” and o δoυς
(odous) “tooth”], is the first specialty of dentistry that is concerned with the study
and treatment of malocclusions (improper bites), which may be a result of tooth
irregularity, disproportionate jaw relationships, or both (Orthodontics). CaPO4 is
used rarely in orthodontics (Table 16.2). Pediatric dentistry [formerly pedodontics
(American English) or paedodontics (Commonwealth English)] is the branch of
dentistry dealing with children from birth through adolescence. It places special
importance in preventing tooth decay. In addition, pediatric dentists work toward
the maintenance of primary teeth (baby teeth) until they are naturally lost. It is irrelevant to the CaPO4 subject (Table 16.2). Periodontics [also periodontology, from
(odous) “tooth”] is the specialty of dentistry
Greek περι (peri) “around” and o δoυς
that studies supporting structures of teeth, as well as diseases of periodontium (these
are specialized tissues investing and supporting teeth, including cementum, periodontal ligament, alveolar bone, and gingiva, characterized by the loss of support
around teeth) and conditions that affect them. Although CaPO4 is frequently used in
periodontics (Table 16.2); in fact, they are applied to treat alveolar bones, which,
again, is another story (Dorozhkin, 2015, 2016a). Prosthodontics [from Greek
(odous) “tooth”], also known as dental
πρoσθεση (prosthesis) “addition” and o δoυς
Calcium orthophosphates as a dental regenerative material
385
prosthetics or prosthetic dentistry, is a dental specialty pertaining to the diagnosis,
treatment planning, rehabilitation, and maintenance of the oral function, comfort,
appearance, and health of patients with clinical conditions associated with missing
or deficient teeth and/or oral and maxillofacial tissues using biocompatible substitutes (Prosthodontics). CaPO4 is used very rarely in prosthodontics (Table 16.2). In
addition, similar searches in Scopus database using keywords “dental,” “dentistry,”
“oral,” “stomatology,” and “caries” combined with “apatite” or “calcium phosphate” have been performed (Table 16.2, the bottom lines).
16.3
Brief information on current biomedical
applications of CaPO4
Due to a chemical similarity to the inorganic part of normal calcified tissues (bones,
teeth, and deer antlers) of mammals, artificially prepared CaPO4 possess good
biocompatibility, bioactivity, and osteoconductivity (Dorozhkin, 2012a, 2016b,c;
LeGeros, 1991; Elliott, 1994). These properties of CaPO4 are extensively used in
medicine for repair or replacement of injured or damaged bones and teeth. Since
the diverse biomedical applications require different formulations, configurations,
and/or shapes, the biomedically relevant CaPO4 is produced in various physical
forms, such as powders, particles, granules, dense blocks, porous scaffolds, selfsetting formulations, suspensions, nonhardening pastes, implant coatings, as well as
composite components of different origin (natural, biological, or synthetic) often
with the specific shapes, such as implants, prostheses, or prosthetic devices
(Dorozhkin, 2012a, 2015, 2016a,b,c; LeGeros, 1991; Elliott, 1994; Xie et al., 2012;
Fernández et al., 2017). In view of the fact that several dental specialties deal with
an invasion into and/or treatment of the surrounding bones (such as bone drilling to
insert an implant), in principle, all the aforementioned forms, formulations, configurations, and shapes of CaPO4 might be applicable to the dentistry field as well.
16.4
CaPO4 for dental caries prevention and in
dentifrices
Traditionally, caries prevention strategies have focused on reducing bacterial
growth, neutralizing oral acids, and teeth remineralization. Among them, only the
third strategy appears to deal with the CaPO4 subject. Briefly, the teeth remineralization is a process in which dissolved CaPO4 minerals are returned to the molecular
structure of the teeth themselves (Fig. 16.1B). To reduce dental caries by performing remineralization, systemic and/or topical fluoridation of water is commonly
used (Reynolds, 2008). In addition, various ion-delivering agents are used in the
form of dentifrices, toothpastes, mouthwashes, mouth rinses, chewing gums, etc.
Many of these remineralizing agents contain CaPO4 (Roveri et al., 2009a). This is
because the focus in caries research has shifted to the development of methodologies for detection of the early stages of caries lesions and noninvasive treatment
386
Advanced Dental Biomaterials
of these lesions. For example, in the presence of calcium and orthophosphate ions,
topical fluoride ions promote the formation of fluorapatite (FA) (which is the least
soluble compound among all known types of CaPO4, Table 16.1) in dental enamel.
This property of fluorides has been known since, at least, 1956 (Fischer et al.,
1956). However, to form one unit cell of FA, 10 calcium and 6 orthophosphate ions
are required for every 2 fluoride ions. Hence, on topical application of fluoride
ions, the availability of calcium and orthophosphate ions can be the limiting factor
for net enamel remineralization to occur, and this is highly exacerbated under the
xerostomic (i.e., a dry mouth) conditions (Reynolds, 2008).
Now, let me describe the applications of CaPO4 in dentifrices. According to
Wikipedia, “Dentifrice are agents used along with toothbrush to clean and polish
natural teeth. They are supplied as paste, powder, gel, or liquid form” (Dentifrice).
To the best of my findings, the earliest study dealing with an application of CaPO4
as a dentifrice was presented at the 23rd general meeting of the International
Association for Dental Research (held in Chicago, Illinois, May 27, 1945) and the
abstract of that presentation was published shortly afterward (McClendon and
Carpousis, 1945). Since then, numerous studies devoted to various applications of
CaPO4 in dentifrices have been published (Shern et al., 1979, 1984; Wefel and
Harless, 1987; Schreiber et al., 1988; Kani et al., 1988, 1989; Okashi et al., 1991;
Gaffar et al., 1993; Zhang et al., 1995; Sullivan et al., 1997, 2001; Kodaka et al.,
1999; Hicks and Flaitz, 2000; Boneta et al., 2001; Silva et al., 2001; Niwa
et al., 2001; Sintes et al., 2002; Kim et al., 2006, 2009; Jeong et al., 2006, 2007;
Lv et al., 2007; Roveri et al., 2009b; Tschoppe et al., 2011; Najibfard et al., 2011;
Wang et al., 2011a; Kovtun et al., 2012; Vanichvatana and Auychai, 2013; Sun
et al., 2014; Browning et al., 2012; Comar et al., 2013; Hannig et al., 2013;
Kensche et al., 2017; de Carvalho et al., 2014; Mielczarek and Michalik, 2014;
Vyavhare et al., 2015; Souza et al., 2015; Hill et al., 2015; Gomes et al., 2017;
Nakata et al., 2018; Hiller et al., 2018). A number of such formulations also contain
fluorides (Shern et al., 1979, 1984; Gaffar et al., 1993; Zhang et al., 1995; Hicks
and Flaitz, 2000; Sullivan et al., 2001; Boneta et al., 2001; Silva et al., 2001; Sintes
et al., 2002; Roveri et al., 2009b; Wang et al., 2011a; Vyavhare et al., 2015;
Souza et al., 2015; Hill et al., 2015; Gomes et al., 2017; Nakata et al., 2018;
Hiller et al., 2018).
16.4.1 Toothpastes
CaPO4-containing toothpastes were found to promote a partial remineralization of
the demineralized enamel (Jeong et al., 2006; Lv et al., 2007; Roveri et al., 2009b;
Kim et al., 2009; Tschoppe et al., 2011; Wang et al., 2011a; Kovtun et al., 2012;
Vanichvatana and Auychai, 2013; Sun et al., 2014; de Carvalho et al., 2014;
Mielczarek and Michalik, 2014; Vyavhare et al., 2015; Souza et al., 2015); as well
as depending on the addition of other constituents, they also can possess some whitening effect (Niwa et al., 2001; Kim et al., 2006; Hill et al., 2015) and reduce tooth
sensitivity (Kim et al., 2009; Browning et al., 2012; Hiller et al., 2018). For example, the polishing and whitening properties of hydroxyapatite (HA)-containing
Calcium orthophosphates as a dental regenerative material
387
toothpastes were investigated in a combined study (Niwa et al., 2001). The polishing properties were evaluated by means of artificial teeth by polishing with different
toothpastes, while the brightening and whitening properties were examined in
volunteers using two colorimeters with two specially made fiberscopes. The results
revealed that the addition of HA to the toothpaste did not alter its polishing properties, while it did result in a marked increase in tooth whitening. It was also found
that the brightening and whitening properties increased as the amount of HA in the
toothpaste increased. Thus HA-containing toothpaste appeared to be effective at
whitening teeth and whitening was not due to their polishing effect on the tooth surface (Niwa et al., 2001). The whitening properties of HA-containing toothpastes
were also found by other researchers (Kim et al., 2006; Hill et al., 2015).
Further, a randomized study with 181 children (92 boys, 89 girls) from different
Japanese schools over a period of 3 years is worth mentioning (Kani et al., 1989).
After lunch, the children brushed their teeth under supervision either with a toothpaste containing 5% HA or a control group with a paste without HA. Yearly controls of the DMFT (number of decayed, missing, and filled teeth due to caries)
index were diagnosed as well as the caries incidence on newly erupted teeth. The
DMFT index appeared to be significantly deeper in the HA-containing toothpaste
group, while the incidence for caries in newly erupted teeth was significantly lower
if compared to the control (Kani et al., 1989).
Besides, dentifrices containing a combination of monofluorophosphate (MFP) with
a dicalcium phosphate dehydrate (DCPD) abrasive were evaluated in a variety of
in vivo tests (Gaffar et al., 1993). MFP with silicon dioxide abrasive at the equivalent
fluoride concentration was used for comparison. The data indicated that DCPD was
more effective than silica in preventing pH drop of plaque. A toothpaste containing
MFP 1 DCPD was significantly more effective than an MFP 1 silica toothpaste. In
addition, a toothpaste containing 45Ca radiolabeled DCPD was applied topically in
rats’ teeth. The results showed that 45Ca was incorporated into the enamel with a concomitant reduction in enamel solubility. In a rat caries study using MFP 1 DCPD,
matching placebo, and MFP 1 silica, the MFP 1 DCPD dentifrice showed a significantly greater reduction in smooth surface caries. These dentifrices were also tested
in an in situ human model for fluoride uptake in artificial root caries lesions where
MFP 1 DCPD provided a significantly higher fluoride uptake than MFP 1 silica. A
second in situ study in humans evaluated the same dentifrices, MFP 1 DCPD
increased salivary plaque calcium and fluoride. These results of laboratory, animal,
and in situ studies taken together indicated that the MFP 1 DCPD combination was
the unique one in providing extra supersaturation in saliva and plaque with concomitant enhanced anticaries efficacy (Gaffar et al., 1993).
Thus due to the aforementioned successful cases of CaPO4 addition to toothpastes, such toothpastes are commercially produced worldwide (Table 16.3). As
seen from Table 16.3, toothpastes for both human and animals are available. One
should note that HA and amorphous calcium phosphates (ACPs) are added to
toothpastes to provide remineralization properties, while DCPD and dicalcium
phosphate anhydrous (DCPA) are added to toothpastes as abrasives to provide a
gentle polishing action.
Table 16.3 Trademarks of CaPO4-containing commercial toothpastes.
Type of
CaPO4
Human or
animals
Trade name and producer
(when available)
HA
Human
Aclaim (Group Pharmaceuticals Limited, India)
Active Remineralization Toothpaste (A.R.T.)
(Pearlie White, Corlison, Singapore)
ApaCare (Cumdente, Germany)
Apadent (Sangi Co., Japan)
Apagard Premio (Sangi Co., Japan)
Arcticum (SPLAT-COSMETICA, Russia)
Biorepair (Coswell, Italy)
Biorepair (Dr. Wolff, Bielefeld, Germany)
Coolin Bubble (Canavena Co., Korea)
DIO (DIO Co., Korea)
Desensibilize Nano P (FGM Produtos Odontológicos, Brazil)
Desensin repair (Dentaid)
Hakusanshiko (Japan)
Janina (Janina Ultra White, United Kingdom)
Kalident—calcium hydroxyapatite (Kalichem, Italia)
MAXDENT (STS Cosmetics, Bulgaria)
Megasonex (Goldspire Group, Hong Kong)
nanoXIM CarePaste (FLUIDINOVA, Portugal)
Parodontol Active (Svoboda Ltd., Russia)
PrevDent (PrevDent International, The Netherlands)
Renamel AfterBleach (Sangi Co., Japan)
Remin (X-PUR, Oral Science, QC, Canada)
R.O.C.S. SENSITIVE (DRC Group, Russia)
Sensitive Reminx (Pharma Jenistec Co., Korea)
Triple Denta (TripleLife Co., Ltd., Korea)
Ultracomplex (SPLAT-COSMETICA, Russia)
UltraDEX Recalcifying and Whitening
(Periproducts Ltd., United Kingdom)
VITIS anticaries toothpaste (Dentaid)
YP Dental (You Co., Ltd. Japan)
Clinpro Tooth Crème (3M ESPE, United States)
Age Defying (Arm & Hammer, Church & Dwight Co.
New Jersey, United States)
Complete Care (Arm & Hammer,
Church & Dwight Co. New Jersey, United States)
EnaFix (Group Pharmaceuticals Limited, India)
Enamel Care (Arm & Hammer, Church &
Dwight Co. New Jersey, United States)
Enamel Pro (Premier Dental Products Company,
United States)
Enamelon (Premier Dental Products Company,
United States)
GC Tooth Mousse (GC Corporation, Japan)
INNOVA (SPLAT-COSMETICA, Russia)
MI paste (GC America, Illinois, United States)
MI paste plus (GC America, Illinois, United States)
G
TCP
ACP
Human
Human
(Continued)
Calcium orthophosphates as a dental regenerative material
389
Table 16.3 (Continued)
Type of
CaPO4
Human or
animals
Trade name and producer
(when available)
DCPD
or DCPA
Human
All White (Dr. Collins, United States)
Colgate Cavity Protection (Colgate-Palmolive,
New York, United States)
Dentu-Creme Denture (Polident, GlaxoSmithKline,
United Kingdom)
Plus White (CCA Industries Inc., New Jersey, United States)
Pureen (Singapore)
R.O.C.S. PRO Baby (DRC Group, Russia)
Snappy Jaws (Australia)
Supersmile (United States)
Triple Action Whitening (Pearl Drops, Church & Dwight,
New Jersey, United States)
Triple Power Whitening (Pearl Drops, Church & Dwight,
New Jersey, United States)
VITA-MYR (Nevada, United States)
Advanced Oral Care (Nylabone, New Jersey, United States)
C.E.T. Enzymatic (Virbac, Texas, United States)
Dental Care Kit (Sentry Petrodex, Sergeant’s Pet Care
Products, Nebraska, United States)
Dentifresh (Hatchwell, United Kingdom)
Enzymatic toothpaste (Sentry Petrodex, Sergeant’s
Pet Care Products, Nebraska, United States)
Four Paws Pet Dental (Four Paws Products,
New York, United States)
VetOne (VetOne, Idaho, United States)
TriMedica Pure MSM (TriMedica, Northern Ireland,
United Kingdom)
Animals
Undisclosed
CaPO4
Human
ACP, Amorphous calcium phosphates; DCPA, dicalcium phosphate anhydrous; DCPD, dicalcium phosphate
dehydrate; HA, hydroxyapatite; TCP, tricalcium phosphate.
To finalize this section, one should mention one of the studies in which the addition of CaPO4 to toothpastes did not show any positive influence on enamel and/or
dentin demineralization/remineralization properties (Esteves-Oliveira et al., 2017).
16.4.2 Chewing gums
Apart from toothpastes, CaPO4 is added to chewing gums to reduce dental caries
(Pickel and Bilotti, 1965; Finn and Jamison, 1967; Finn, 1967; Richardson et al.,
1972; Wilson, 1975; Chow et al., 1994; Vogel et al., 1998, 2000; Shen et al., 2001;
Iijima et al., 2004; Itthagarun et al., 2005; Cai et al., 2007; Morgan et al., 2008;
Thaweboon et al., 2009; Dodds et al., 2012; Shammukha et al., 2012; Porciani
et al., 2014; Emamieh et al., 2015; Sultan et al., 2016; Hasnamudhia et al., 2017).
390
Advanced Dental Biomaterials
In the vast majority of cases, a positive effect was noticed. Namely, to evaluate
chewing gums as a vehicle to increase salivary mineral saturation levels and
enhance salivation, both monocalcium phosphate monohydrate (MCPM) and the
equimolar mixture of tetracalcium phosphate (TTCP) with DCPA were chosen as
experimental chewing gum additives (Chow et al., 1994). Each subject chewed a
commercial sugar-free bubble gum (control) for 16 minutes or the same gum to
which 5 wt.% of MCPM or TTCP 1 DCPA mixture had been added. Both experimental gums were found to increase significantly the concentrations of calcium and
orthophosphate ions in saliva during the 16-minute period even more than with a
previously evaluated gum that contained DCPD. The degree of saturation of tooth
mineral was significantly increased by both experimental gums, with a greater
increase being produced by the TTCP 1 DCPA gum. The MCPM gum produced a
significantly greater saliva flow and a lower salivary pH than did the control and
TTCP 1 DCPA gums. The results suggested that the experimental gums could be
useful for promoting remineralization in general and for inducing salivation in xerostomic patients (Chow et al., 1994).
In other studies, both sugar-free gums (control) and casein phosphopeptideACP
(CPPACP) containing gums were chewed for either 20-minute periods, four times a
day or 5-minute periods, seven times a day. Microradiography and computer-assisted
densitometric image analysis demonstrated that regardless the gum type and chewing
duration (e.g., 20 or 5 minutes), the nanodimensional CPPACP complexes produced
a dose-related remineralization of enamel subsurface lesions in situ. The gums containing 18.8 and 56.4 mg of the nanodimensional CPPACP complexes, chewed for
20 minutes, four times per day for 14 days, increased enamel subsurface remineralization by 101% and 151%, respectively, relative to the control sugar-free gums.
Microradiographs of the enamel lesions before and after remineralization showed that
the nanodimensional CPPACP complexes promoted remineralization throughout
the body of the lesion. Electron microprobe wavelength dispersive spectrometric
analyses of sections of the remineralized enamel indicated that the mineral deposited
was apatite with a higher Ca/P ratio than that in the stoichiometric HA. Acid challenge of the enamel remineralized by the nanodimensional CPPACP complexes in
situ showed that the remineralized apatite was more resistant to acid challenge than
the normal calcium-deficient carbonated tooth enamel. Thus the clinical trials of
CPPACP-containing sugar-free chewing gums demonstrated that these gums significantly slowed progression of caries and enhanced regression of caries compared with
the control sugar-free gums (Shen et al., 2001; Iijima et al., 2004; Itthagarun et al.,
2005; Cai et al., 2007; Morgan et al., 2008).
16.4.3 Teeth remineralization
In general, remineralization of teeth can be defined as the process in which calcium
and orthophosphate ions are supplied from a source external to teeth to promote
their deposition into crystal voids in demineralized enamel, to produce net mineral
gain (Cochrane et al., 2010). The earliest found paper on a possibility of a remineralization phenomenon occurring in caries was published in 1912 (Head, 1912),
while that using CaPO4 for rehardening was performed in 1961 with solutions
Calcium orthophosphates as a dental regenerative material
391
containing dissolved ions of calcium and orthophosphate (Koulourides et al., 1961),
followed by the set of the studies performed by Silverstone (Silverstone and
Johnson, 1971; Silverstone, 1972), as well as by 10 Cate and Arends (ten Cate and
Arends, 1977, 1978, 1980; ten Cate et al., 1981).
The early attempts to use CaPO4 for remineralization of dental surface were
unsuccessful due to their low solubility, particularly in the presence of fluoride
ions. Namely, the insoluble CaPO4 cannot be applied easily; they do not localize
effectively on the tooth surface and require an acidic environment for solubility
levels sufficient to produce ions capable of diffusing into enamel subsurface lesions.
Furthermore, due to the intrinsic insolubility of CaPO4 at the physiological pH
values, soluble calcium and orthophosphate ions can only be used at very low concentrations. Besides, the soluble ions of calcium and orthophosphate are neither
substantially incorporated into the dental plaque nor localized at the tooth surface
to produce the effective concentration gradients to drive diffusion into the subsurface enamel (Reynolds, 2008).
Nevertheless, studies on teeth remineralization keep going. For example, a remineralization potential of HA itself for caries lesion treatment was investigated
(Okashi et al., 1991). Previously demineralized enamel blocks were immersed
into an aqueous solution of sludgy HA at 37 C for 55 hours, followed by 24 hours
washing with synthetic saliva and another group was washed only with synthetic
saliva. Artificial caries lesions were remineralized slightly by immersion into artificial saliva but a significant acceleration of remineralization was observed in the
sludgy HA group (Okashi et al., 1991). Positive results were also obtained in
other studies (Kani et al., 1988; Yamagishi et al., 2005; Kim et al., 2007; Lu et al.,
2007; Zhen et al., 2007; Rimondini et al., 2007; Roveri et al., 2008; Huang
et al., 2009, 2011; Yin et al., 2009; Lv et al., 2010; Wu et al., 2013; Haghgoo et al.,
2014; Besinis et al., 2014; Kensche et al., 2016). In 2005 a study on the potential of
HA in repairing enamel lesions was published in which an HA-containing paste
demonstrated an enamel-repairing effect that was confirmed by transmission electron microscopy and atomic force microscopy (Yamagishi et al., 2005). The results
of an in situ study showed a potential accumulation of HA from a mouthwash in
the dental pellicle; however, no significant erosion protection was found from this
accumulation (Kensche et al., 2016). Furthermore, remineralization of caries lesions
could be performed by supersaturated solutions (Chow and Takagi, 1995; Reynolds,
1997; Wen et al., 2016) and/or gels (Wang et al., 2011b; Ning et al., 2012; Tian
et al., 2012; Gu et al., 2013; Chen et al., 2013b; Cao et al., 2014; Wu et al., 2015;
Wang et al., 2015a; Zaharia et al., 2017) containing dissolved ions of calcium and
orthophosphate. In addition, supersaturated CaPO4 mouth rinses were found to
experience a significant increase in reversals of caries in high risk for caries patients
due to xerostomia (salivary hypofunction) (Singh and Papas, 2009). A remineralization potential of sports drinks, containing nano-sized HA particles, was also studied
(Lee et al., 2007; Min et al., 2011).
More complicated formulations, such as CaPO4-loaded liposomes combined
with amelogenin-inspired oligopeptides (Luo et al., 2012), as well as biocomposites
of nanodimensional ACP with various polymeric compounds (Liang et al., 2017a,b;
Weir et al., 2017; Xiao et al., 2017) have been also developed to promote
392
Advanced Dental Biomaterials
remineralization of dental enamel. Thus CaPO4 appear to be the chemicals able to
reduce dental caries at the early stages. However, studies performed by using
atomic force microscopy nanoindentation technique revealed that previously demineralized samples of dental enamel further exposed to remineralizing solutions did
show a crystalline layer of CaPO4 formed on their surface. Unfortunately, the reprecipitated deposits of CaPO4 always consisted of loosely packed crystals and did not
protect the underlying enamel from a subsequent acid attack. Furthermore, these
surface deposits were completely removed by either a toothbrush or a short exposure to an erosive acidic solution (Jandt, 2006; Lippert et al., 2004a,b,c). In this
context, it should be emphasized that the term “remineralization,” which is often
misused in the literature, should imply the process of mineral growth that goes
hand in hand with a strengthening effect of the weakened enamel surface. Since no
strengthening of an exposure to remineralizing solutions was observed, it might be
considered that no “passive mineralization” was found (in spite of the real evidence of
the reprecipitated surface deposits of CaPO4) (Jandt, 2006; Lippert et al., 2004b,c).
Further details on the remineralization attempts of teeth are available in the topical
reviews (Li et al., 2014a; Niu et al., 2014; Cao et al., 2015).
To finalize this section, one should mention a new technology called “electrically assisted enhanced remineralization” developed by Reminova Ltd. (Scotland,
United Kingdom), which relies on the use of a tiny electrical current of a few
micro-Amps to reverse tooth decay by boosting remineralization. Although the
details are not disclosed, the science behind this process is described as follows: “It
is a two-step process. First, a lesion in the enamel is identified by a dentist and conditioned with a quick and simple set of washes to remove decay and exogenous
materials that may have built up within the decayed lesion. Some natural minerals
are applied locally to the lesion and then a tiny electric field is used to help drive
the minerals into the deepest parts of the now cleaned-out lesion. The minerals
pack closely together and start precipitating (hardening) onto the existing enamel
structure. Very quickly, the lesion will fill and the enamel is strong and healthy
again. Because it is based on a natural process, it is understood how minerals (calcium and phosphate molecules) go back into tooth enamel, and how they join and
form part of the enamel.” Obviously, either CaPO4 compounds or Ca- and PO4-containing constituents are used as “some natural minerals” in this technology.
16.4.4 Dentin hypersensitivity treatments
As written in Wikipedia, the free encyclopedia
Dentin hypersensitivity (abbreviated to DH or DHS and also termed sensitive
dentin, dentin sensitivity, cervical sensitivity and/or cervical hypersensitivity) is
dental pain which is sharp in character and of short duration, arising from exposed
dentin surfaces in response to stimuli, typically thermal, evaporative, tactile,
osmotic, chemical or electrical and which cannot be ascribed to any other dental
disease (Dentin hypersensitivity).
Calcium orthophosphates as a dental regenerative material
393
Dentin hypersensitivity is a frequently reported oral pain condition, which is
mostly diagnosed at the buccal surfaces of teeth, where enamel is missing due to
erosion, abrasion, and/or attrition. Contrary to enamel, which is dense and contains
a small amount of pores, dentine has a great number of tiny tubes (tubules) that
lead to the nerve and are filled with fluids. However, until about the third or fourth
decade of life in healthy individuals, the surface of dentin is not exposed and the
tubules are sealed. When a tooth loses its protection from gum recession and/or
tooth enamel wear, these tubules are exposed to the outside, allowing external stimuli to reach the nerve endings. Therefore even mild external stimuli such as hot or
cold foods and beverages can cause a change in fluid movement, which causes the
nerve endings to react in response, triggering a short but sharp pain.
There are several strategies to prevent dentin hypersensitivity in oral care,
including occlusion of dentin tubules with different particulate materials (arginine/
calcium carbonate, calcium sodium phosphosilicate, strontium fluoride, etc.) or
nerve desensitization with agents such as potassium salts (Enax and Epple, 2018).
However, all these cases are beyond the scope of this review. Back on the topic,
some types of CaPO4 were found to be able to treat this disease as well (Kim et al.,
2009; Browning et al., 2012; Porciani et al., 2014; Hüttemann and Dönges, 1987;
Sugawara et al., 1989; Yates et al., 1998; Suge et al., 2002; Geiger et al., 2003;
Shetty et al., 2010; Low et al., 2015; Vano et al., 2018; Mehta et al., 2015; Zhou
et al., 2016). For example, already in 1987, the results of a clinical study of 140
patients with hypersensitive teeth, in which HA-containing pastes with different
particle sizes of HA were used for treatment, were published. A paste containing
2-μm-sized HA particles appeared to be more effective than that containing
6-μm-sized HA particles and 90% of all patients experienced relief from tooth
hypersensitivity after 35 days (Hüttemann and Dönges, 1987). In another study,
an HA-containing toothpaste was compared with positive control toothpastes, in
which the HA-containing toothpaste was similarly effective in reducing dentine
hypersensitivity with preexisting benchmark toothpastes (Kim et al., 2009). Positive
results were also obtained with both HA-containing Renamel AfterBleach toothpaste (Browning et al., 2012) and an undisclosed nano-HA, potassium nitrate,
sodium MFP, and antioxidants-containing toothpaste (Low et al., 2015). In another
study, HA-treated teeth showed statistically significant reduction in hypersensitive
symptoms compared to the control groups and the authors concluded that HA
showed “definite potential as an effective and permanent desensitizer when used as
an in-office procedure” (Shetty et al., 2010). Furthermore, a CaPO4 precipitation
method was once tried as a treatment for dentin hypersensitivity using the vital
teeth of beagle dogs. The results revealed that dentin tubules were occluded
homogeneously and completely with an apatitic mineral after application of the CaPO4
precipitation in vital teeth (Suge et al., 2002). A commercial self-setting formulation
TEETHMATE DESENSITIZER (Kuraray Noritake Dental Inc., Japan), consisting of a
mixture of DCPA 1 TTCP 1 some fluoride-free additives, which formed calciumdeficient HA (CDHA) precipitates upon exposure to saliva, appeared to able to occlude
open dentinal tubules, and, by this way, acted as an effective desensitizer compound
(Mehta et al., 2015; Zhou et al., 2016; Moogi et al., 2017; Shetty et al., 2017).
394
Advanced Dental Biomaterials
Nevertheless, there are similar formulations with fluorides (Medvecky et al., 2018). In
addition, there is commercially produced dental gel Relief ACP (Discus dental, United
States), containing 0.375% ACP and 1100 ppm fluoride (Arafa, 2017), as well as MI
varnish (3M ESPE, United States), containing ACP stabilized by a CPP and NaF
(Sharma et al., 2017). Both of them are used to treat dentin hypersensitivity. Additional
details on this topic are available in a recent review (Enax and Epple, 2018).
16.5
Clinical applications of CaPO4 in dentistry
As said in Section 16.1, dentists have been using CaPO4 for over a century.
However, to the best of my findings, the first available publication on decalcification of teeth as the reason for various dental pathologies was published in 1925
(Miloslavich, 1925). Furthermore, the clinical applications of CaPO4 in dentistry
started only in the 1970s (Monroe et al., 1971). Namely, the first application of a
CaPO4 [erroneously described as “tricalcium phosphate (TCP) of HA structure”]
bioceramics in surgically created periodontal defects was reported in 1975 (Nery
et al., 1975), followed by a publication on alveolar ridge augmentation in 1978
(Nery et al., 1978), while the use of dense HA cylinders for immediate tooth root
replacement was reported in 1979 (Denissen and de Groot, 1979). A summary on
early (before 1987) studies can be found in Table 16.3 of. LeGeros (1988), while
Table 16.4 of this publication represents the various types of dental applications of
CaPO4 in the mid-1980s (LeGeros, 1988, 1991).
Overall, the reasons for the clinical application of CaPO4 in dentistry are similar
to those for their applications in bone grafting. A chemical similarity to the inorganic phases of teeth and bones appears to be the major reason. Consequently,
CaPO4 possess an excellent biocompatibility, biotolerance, an ability to be resorbed
by both tooth- and bone-related cells, osteoconductivity, etc. In addition, CaPO4 is
less expensive than the majority of inorganic fillers used today. In the following
subsections, the clinical applications of CaPO4 in dentistry have been classified into
two ways: according to the existing CaPO4, as listed in Table 16.1, and according
to the modern dental specialties, as listed in Table 16.2.
Table 16.4 Dental applications of CaPO4 in the mid-1980s (LeGeros, 1991; LeGeros,
1988).
1
2
3
4
5
6
7
Restore (augment) alveolar ridge for better denture fit
Immediate tooth root replacement to prevent resorption of alveolar ridge
Fillers for periodontal defects or bone loss
Coatings for metal implants to improve boneimplant adhesion and prevent loosening
of the metal implants
Repair of cleft palate
Repair of maxillofacial defects
Pulp capping materials
Calcium orthophosphates as a dental regenerative material
395
16.5.1 Classification according to the existing CaPO4
16.5.1.1 Monocalcium phosphate monohydrate and
monocalcium phosphate anhydrous
Just a few studies on dental applications of MCPM and monocalcium phosphate
anhydrous (MCPA) were found in databases of scientific literature (Table 16.1).
According to the available publications, both compounds are used in dentistry as
components of self-setting formulations (Kouassi et al., 2003; Mehdawi et al.,
2009), including sealers (Koch et al., 2010). For example, a commercial product
EndoSequence BC Sealer (Brasseler USA, Savannah, Georgia) is a premixed readyto-use injectable cement paste developed for permanent root canal filling and sealing applications. It contains zirconium oxide, calcium silicates, MCPA, calcium
hydroxide, filler, and thickening agents. When this sealer is placed in the root canal,
it absorbs water from the dentin tubules causing hydration reactions of calcium silicates. Simultaneously, MCPA reacts with calcium hydroxide to precipitate CDHA.
This leads to the formation of a composite network of gel-like calcium silicate
hydrates, which intimately mixes with CDHA crystals and forms a hermetic seal
inside the root canal (Koch et al., 2010). In addition, MCPM and/or MCPA were
tried as components of caries-inhibiting dental biocomposites, releasing ions of calcium and orthophosphate (Mehdawi et al., 2009; Xu et al., 2007a). Once a MCPMcontaining chewing gum was tested, it produced a significantly greater saliva flow
and a lower salivary pH than the control gum did (Chow et al., 1994).
16.5.1.2 Dicalcium phosphate dehydrate and dicalcium
phosphate anhydrous
As seen in Table 16.3, DCPD and/or DCPA are often added to toothpastes as gentle
polishing agents. In addition, DCPD and/or DCPA (unfortunately, the authors of
the publications on the subject rarely specified which of them was used) are added
to chewing gums (Pickel and Bilotti, 1965; Finn and Jamison, 1967; Finn, 1967;
Richardson et al., 1972; Chow et al., 1994; Thaweboon et al., 2009) and other types
of dentifrices (Shern et al., 1984; Wefel and Harless, 1987; Schreiber et al., 1988;
Gaffar et al., 1993; Zhang et al., 1995; Sullivan et al., 1997, 2001; Kodaka et al.,
1999; Hicks and Flaitz, 2000; Boneta et al., 2001; Silva et al., 2001; Sintes et al.,
2002). Furthermore, they are used as either components or end products of various
CaPO4-based self-setting formulations (Kuemmerle et al., 2005; Luaces-Rey et al.,
2009; Sugawara et al., 1989, 2008; Mehta et al., 2015; Zhou et al., 2016; Moogi
et al., 2017; Shetty et al., 2017; Medvecky et al., 2018; Dickens-Venz et al., 1994;
Lee et al., 2003; Briak et al., 2002; Dickens et al., 2003; Michaı̈lesco et al., 2005;
Xu et al., 2006a; Wei et al., 2011a,b; Thein-Han et al., 2012; Panahi et al., 2017)
and root canal sealers (Yoshikawa et al., 1997). In addition, both compounds are
added to biocomposites (Xu et al., 2006b, 2007b,c; Chen, 2010). For example, a
decrease of DCPA particle dimensions was found to increase the Ca- and PO4-ions
releases from DCPA-based biocomposites. Therefore such biocomposites possess
both high strength and good release of Ca and PO4 ions, which may provide the
396
Advanced Dental Biomaterials
needed and unique combination of stress-bearing and caries-inhibiting capabilities
suitable for dental applications (Xu et al., 2007c). In addition, DCPD was tried in
pulpectomy (Jean et al., 1993).
16.5.1.3 Octacalcium phosphate
Just a few publications on applications of octacalcium phosphate (OCP) in dentistry
and dentistry-related fields were found. Namely, OCP might be used as a coating
(Stefanic et al., 2012; Bao et al., 2014), a component of biocomposites (Bao et al.,
2014; Miura et al., 2012; Kawai et al., 2018), and in self-setting formulations (Sena
et al., 2004; Imamura et al., 2010). In addition, OCP was tried in pulpectomy (Jean
et al., 1993), as a direct pulp capping material (Sena et al., 2004), and for alveolar
ridge augmentation (Miura et al., 2012; Kamakura et al., 1996). Furthermore, investigations with rats revealed that implanted OCP could serve as a core for initiating
bone formation and cause osteoinduction and osteoconduction in experimentally
created cranial defects (Sena et al., 2004) and enhanced reparative dentine formation via induction of odontoblast differentiation (Wang et al., 2015b).
16.5.1.4 Amorphous calcium phosphates
Unlike OCP, ACPs appear to be very popular compounds for dental applications
(Reynolds, 1998, 2008; Shammukha et al., 2012; Emamieh et al., 2015; Sultan
et al., 2016; Hasnamudhia et al., 2017; Yates et al., 1998; Geiger et al., 2003;
Ambrosio et al., 2001; Skrtic et al., 1996a,b, 2001, 2003, 2004; Skrtic and
Antonucci, 2005, 2007, 2011; Oshiro et al., 2007; O’Donnell et al., 2009;
Antonucci et al., 2009; Walker et al., 2010; Xu et al., 2011; Uysal et al., 2009a,b,c,
2010a,b,c, 2011; Tung and Eichmiller, 1999; Dunn, 2007; Keçik et al., 2008; Foster
et al., 2008; Sun et al., 2008; Bröchner et al., 2011; Antonucci and Skrtic, 2010;
Beerens et al., 2010; Zhao et al., 2011, 2012; Gupta and Prakash, 2011; Zhang
et al., 2011; Moreau et al., 2011; Fletcher et al., 2011; Tabrizi and Cakirer, 2011;
Hamba et al., 2011; Chow et al., 2011; Hegde and Moany, 2012; Bar-Hillel et al.,
2012; Çehreli et al., 2012; Hammad et al., 2013; Park et al., 2013; Gurunathan and
Somasundaram, 2015; Baysal and Uysal, 2012; Liu et al., 2018a; Prabhakar et al.,
2012; Weir et al., 2012; Kato et al., 2013, 2015; Reema et al., 2014). For example,
two ACP-based remineralization systems have been developed and are now commercially available: a CPP-stabilized ACP with a trade name Recaldent (Cadbury
Enterprises Pte Ltd., Singapore) and an unstabilized ACP with a trade name
Enamelon (Enamelon Inc., Cranbury, New Jersey, United States). CPP is produced
from milk protein casein and has a remarkable ability to stabilize CaPO4 in solutions and substantially increase the level of CaPO4 in dental plaque. Therefore in
Recaldent technology, it is claimed that CPP stabilizes high concentrations of calcium and orthophosphate ions, together with fluoride ions, at the tooth surface by
binding to pellicle and plaque. Through the cluster sequence, CPP binds to forming
nanodimensional clusters of ACP preventing their growth to the critical size
required for nucleation and phase transformation. CPPACP nanodimensional
Calcium orthophosphates as a dental regenerative material
397
complexes with a hydrodynamic radius of 1.526 6 0.044 nm at pH 5 6.0, which
increases to 1.923 6 0.082 nm at pH 5 9.0, are formed as a result (Cross et al.,
2016). It is believed that these CPPACP nanodimensional complexes enter the
porosities of an enamel subsurface lesion and diffuse down concentration gradients
into the body of the subsurface lesion. Once present there, the nanodimensional
complexes release the weakly bound calcium and orthophosphate ions, which would
then deposit into crystal voids (Cochrane et al., 2010). Due to ACPs’ bioactivity,
local Ca- and PO4-enriched environments are created with supersaturation conditions favorable for the regeneration of tooth mineral lost to decay or wear.
Although all the available ions are stabilized by CPP from promoting dental calculus, they are freely available to diffuse down concentration gradients into enamel
subsurface lesions thereby effectively promoting remineralization in vivo. The
Enamelon technology applies calcium ions (e.g., calcium sulfate) and orthophosphate ions (e.g., ammonium orthophosphate, sometimes in the presence of fluoride
ions) separately (e.g., from a dual chamber device). Therefore as the salts mix
with saliva, they dissolve releasing calcium and orthophosphate ions and ACP (or
F-containing ACP) forms intraorally. In the intraoral environment, both ACP
and F-containing ACP are very unstable and rapidly transform to a more thermodynamically stable, insoluble crystalline phases, such as CDHA and a blend of
CDHA 1 FA, respectively. It is believed that this helps rebuild tooth enamel
through remineralization (Hicks and Flaitz, 2000; Schemehorn et al., 1999; Mayne
et al., 2011); however, this approach may also promote dental calculus (Reynolds,
2008). Thus both previously prepared ACP (Recaldent) and in situ precipitated
ACP (Enamelon, Relief ACP) are used in dentistry to remineralize tooth surface.
This property of ACPs is used in toothpastes (Table 16.3). In addition, there is a
commercially produced MI varnish (3M ESPE, United States), containing
CPPACP Recaldent, which was found to be effective in dentinal hypersensitivity
reducing (Sharma et al., 2017).
As seen from the available references, in dentistry ACPs are generally used as
components of various biocomposites. In an acidic oral environment, such biocomposites take advantages of the ability of ACPs to release calcium and orthophosphate ions, which potentially can take part in enamel remineralization (Vyavhare
et al., 2015; Shen et al., 2001; Iijima et al., 2004; Cai et al., 2003, 2007; Morgan
et al., 2008; Shammukha et al., 2012; Emamieh et al., 2015; Sultan et al., 2016;
Hasnamudhia et al., 2017; Liang et al., 2017a,b, 2018; Weir et al., 2012, 2017;
Xiao et al., 2017; Ambrosio et al., 2001; Skrtic et al., 1996a,b, 2001, 2003, 2004;
Skrtic and Antonucci, 2005, 2007, 2016; Oshiro et al., 2007; O’Donnell et al.,
2009; Antonucci et al., 2009; Reynolds, 1998; Tung and Eichmiller, 1999; Gupta
and Prakash, 2011; Zhang et al., 2011, 2014, 2016a,b,c; Liu et al., 2018a,b;
Prabhakar et al., 2012; Reema et al., 2014; Llena et al., 2009; Langhorst et al.,
2009; Kumar et al., 2008; Ranjitkar et al., 2009a,b; Wegehaupt and Attin,
2010; Al-Mullahi and Toumba, 2010; Giniger et al., 2005a,b; Reynolds et al., 2008;
Ramalingam et al., 2005; Panich and Poolthong, 2009; Silva et al., 2010; Bayrak
et al., 2009; Yengopal and Mickenautsch, 2009; Walker et al., 2006, 2009;
Willershausen et al., 2009; Mei et al., 2009; Melo et al., 2013a,b; Aykut-Yetkiner
398
Advanced Dental Biomaterials
et al., 2014; Zhou et al., 2014; Li et al., 2014b; Xie et al., 2018; Mendes et al.,
2018). The ACP-containing biocomposites and hybrid biomaterials can be prepared
in various forms, such as crèmes (Zhang et al., 2011), nanodimensional fibers
(Fletcher et al., 2011), or cements (Zhang et al., 2016b). Such formulations are used
mainly as anticariogenic and/or remineralizing agents (Shen et al., 2001; Iijima
et al., 2004; Cai et al., 2003, 2007; Morgan et al., 2008; Liang et al., 2017a,b,
2018; Weir et al., 2012, 2017; Xiao et al., 2017; Gupta and Prakash, 2011; Zhang
et al., 2011, 2014, 2016a,b,c; Liu et al., 2018a,b; Prabhakar et al., 2012; Reema
et al., 2014; Llena et al., 2009; Langhorst et al., 2009; Kumar et al., 2008; Ranjitkar
et al., 2009a,b; Wegehaupt and Attin, 2010; Al-Mullahi and Toumba, 2010;
Giniger et al., 2005a,b; Reynolds et al., 2008; Ramalingam et al., 2005; Panich
and Poolthong, 2009; Silva et al., 2010; Bayrak et al., 2009; Yengopal and
Mickenautsch, 2009; Walker et al., 2006, 2009; Willershausen et al., 2009; Mei
et al., 2009; Melo et al., 2013a,b; Aykut-Yetkiner et al., 2014; Zhou et al., 2014;
Li et al., 2014b; Xie et al., 2018; Skrtic and Antonucci, 2016; Mendes et al., 2018),
for example, in chewing gums (Shen et al., 2001; Iijima et al., 2004; Cai et al.,
2007; Morgan et al., 2008; Shammukha et al., 2012; Emamieh et al., 2015; Sultan
et al., 2016; Hasnamudhia et al., 2017), sugar confections (Walker et al., 2010),
lozenges (Cai et al., 2003), various tooth mousses (Kumar et al., 2008; Ranjitkar
et al., 2009a,b), bleaching gels (Giniger et al., 2005a,b), mouth rinses (Reynolds
et al., 2008), various drinks (Ramalingam et al., 2005; Panich and Poolthong,
2009), or even in milk (Walker et al., 2006, 2009). In 2016 rechargeable
ACP-containing formulations with sustained ion release and rerelease were introduced (Zhang et al., 2016a,b; Xie et al., 2018; Liang et al., 2018). To improve cell
adhesion, coatings composed of ACP and hyaluronic acid were used (Sun et al.,
2008). Finally, ultrathin freestanding ACP sheets were manufactured and tested
(Kato et al., 2013, 2015). Additional details of dental applications of ACPcontaining biocomposites are available elsewhere (Skrtic and Antonucci, 2016;
Shyam et al., 2017).
16.5.1.5 α-Tricalcium phosphate and β-tricalcium phosphate
According to the available literature, α-TCP and/or β-TCP (unfortunately, the
authors of the publications on the subject do not always specify which of them
was used) are widely used in dentistry and dentistry-related fields. For example,
they are used for augmentation of the surrounding bones (Nery et al., 1978;
Pepelassi et al., 1991; Wiltfang et al., 2003; Zerbo et al., 2004; Zijderveld et al.,
2005; Shayesteh et al., 2008; Marukawa et al., 2011; Klijn et al., 2012; Yoshino
et al., 2013), in maxillofacial surgery (Fischer-Brandies and Dielert, 1985;
Ignatius et al., 2001; Horch et al., 2006; Saito et al., 2012), as a component of
root canal sealers (Bilginer et al., 1997) and self-setting formulations to fill dental
cavities (Dou et al., 2017), as implant coatings (Niwa et al., 2009; Yamamoto
et al., 2015), as remineralization (Karlinsey et al., 2010a,b; Karlinsey and Pfarrer,
2012) and pulpotomy (Shayegan et al., 2008) agents, for dental pulp capping
(Heller et al., 1975; Koenigs et al., 1975; Boone and Kafrawy, 1979; Himel et al.,
Calcium orthophosphates as a dental regenerative material
399
1985; Yoshiba et al., 1994; Higashi, 1996), to treat perforations (Sinai et al.,
1989; Balla et al., 1991), as endodontic plugs (Harbert, 1991), and to fill various
types of bone defects and lesions (Gaberthüel and Strub, 1977; Strub and
Gaberthüel, 1978; Baldock et al., 1985; Saffar et al., 1990; Stavropoulos et al.,
2010; Asvanund and Chunhabundit, 2012; Okubo et al., 2013; Saito et al., 2014;
Matsuura et al., 2015; Matsuse et al., 2018). Microspheres of Mg-doped TCP
were tested as delivery vehicles for tooth-bleaching agents (Mellgren et al.,
2018). In addition, the investigations to assess the effect of nanodimensional
β-TCP on enamel repair revealed that the use of β-TCP had a significant effect on
improving enamel mineralization and penetrating into intercrystalline spaces
(Rezvani et al., 2015). Furthermore, α-TCP-containing chewing gums were prepared and tested (Vogel et al., 1998, 2000).
To extend a variety of applications, β-TCP can be functionalized by various
organic compounds, such as sodium lauryl sulfate (Karlinsey et al., 2010a), fumaric
acid (Karlinsey et al., 2010b), and some other compounds (Karlinsey and Pfarrer,
2012; Ogawa et al., 2016; Cãlin and Pãtraşcu, 2016). Functionalization of β-TCP
served two major purposes: first, it provided a barrier that prevented premature
β-TCPfluoride interactions, and second, it provided a targeted delivery of β-TCP
when applied to the teeth. Placebo-controlled clinical studies demonstrated that
if compared to fluoride alone, the combination of fluoride plus functionalized
β-TCP improved remineralization by building stronger, more acid-resistant mineral
in both white spot lesions as well as eroded enamel (Karlinsey et al., 2010a,b;
Karlinsey and Pfarrer, 2012). A therapy of 36 teeth with deep caries by both HA
and undisclosed TCP was carried out. Repeated examinations of patients 1 and 6
months after treatment showed that both HA and TCP normalized the function of
the pulp and caused remineralization of dentin in the bottom of carious cavity
(Maksimovskii and Zemskova, 1994).
To finalize this topic, one should mention a commercially produced Clinpro
white varnish (3M ESPE, United States), containing functionalized undisclosed
TCP and 22,600 ppm of fluorides, as well as a toothpaste with a similar composition from the same producer (Table 16.3).
16.5.1.6 Apatites (hydroxyapatite, calcium-deficient
hydroxyapatite, and fluorapatite)
As in Table 16.2, apatites (HA, CDHA, and FA) appear to be the most popular type
of CaPO4 used for dental applications. Since nanodimensional and nanocrystalline
apatites are often considered as the model compounds of dental enamel due to both
the chemical and phase similarities (LeGeros, 1991; Elliott, 1994), their use in
restorative dentistry offers several promising advantages, including intrinsic radiopaque response, enhanced polishability, and improved wear performance. In addition, they have hardness similar to that of natural teeth (Wang and Wang, 2010).
For example, nanodimensional HA particles were found to have an ability to infiltrate a demineralized collagen matrix of dentin. Afterward, the infiltrated collagen
matrix of dentin might provide a suitable scaffold for dentin remineralization,
400
Advanced Dental Biomaterials
whereby the infiltrated HA particles could act as seeds within the collagen matrix
and, given the appropriate remineralizing environment, dentin remineralization
might occur (Besinis et al., 2012). In addition, it was demonstrated that nano-sized
HA particles could be self-assembled to form enamel-like structures (Chen et al.,
2005). Therefore a localized biomimetic repair of the enamel surface could be
achieved by nano-sized (B20 nm) HA, which were analogs to the basic building
blocks of the enamel rods. This similarity resulted in a good fixation of artificial
biomaterials to natural tissues. Moreover, the enamel structure became reinforced
by nano-sized HA since a secondary caries was suppressed and the hardness was
retained (Onuma et al., 2005; Meng et al., 2007; Li et al., 2007). Furthermore,
nano-sized HA could be adsorbed onto the enamel surface strongly and even be
integrated into the natural enamel structure (Li et al., 2008). Generally, these studies also suggest that analogs of nanodimensional building blocks of biominerals
should be highlighted in the entire subject of biomineralization. This strategy may
have prospective applications in dentistry as it offers an easy but effective method
to reconstruct tooth enamel that is suffering from mineral losses.
Normally, apatites for dental applications are prepared from the pure chemicals;
however, they could also be prepared from biological sources, such as teeth (Lim
et al., 2011). Due to the versatile applications in dentistry, apatites could be used in
various formulations, configurations, and/or shapes. First, apatites are added to
toothpastes (Table 16.3). Second, apatites are used as coatings to enhance the
osteoinductivity of various dental implants (Block et al., 1987, 1994, 2000; Jones
et al., 1997, 1999; Gineste et al., 1999; Ong and Chan, 1999; Yoshinari et al., 2002;
Schliephake et al., 2006; Kim et al., 2011a; Jung et al., 2012; Kano et al., 2012;
van Oirschot et al., 2016a; Yu and Choe, 2018). For example, degradation rates of
dental implants covered by 50- and 100-μm-thick coatings of HA, FA, and fluorohydroxylapatite (FHA) were studied (Gineste et al., 1999). The implants were
inserted in dog jaws and retrieved for histological analysis after 3, 6, and 12
months. The HA and FA coatings (even 100 μm thick) were almost totally degraded
within the implantation period. In contrast, the FHA coatings did not show significant degradation during the same period (Gineste et al., 1999). The apatite coatings
on titanium implants followed by bisphosphonate-immobilization appeared to be
effective in the promotion of osteogenesis on surfaces of dental implants (Yoshinari
et al., 2002). Such coatings are commercially produced. For example, there is a
commercial “μ-ONE HA implant” (Yamahachi Dental, Japan) in which an HA film
of 12 μm thick is sputtered by an undisclosed technique to the surface of fixing
device (embedded in maxilla during surgery) of titanium implanted teeth.
Regarding their durability, the HA-coated dental implants were found to work well
in the short to medium terms [during 46 years (Tinsley et al., 2001), 810 years
(Binahmed et al., 2007), and 14 years (Iezzi et al., 2007)]; nevertheless, even longer
term clinical results are awaited with a great interest (van Oirschot et al., 2016a).
Third, apatites are added as components to intermediate restorative materials
(Owadally and Ford, 1994; Owadally et al., 1994), glass-ionomer cements (which
are dental restorative materials used for filling teeth) (Nicholson et al., 1993; Yap
et al., 2002; Lucas et al., 2003; Moshaverinia et al., 2008a; Moshaverinia et al.,
Calcium orthophosphates as a dental regenerative material
401
2008b; Arita et al., 2011; Lin et al., 2011), enamel resin infiltrants (Neto et al.,
2016), various dental biocomposites (Domingo et al., 2001; Brostow et al., 2008;
Oduncu et al., 2010; Huang et al., 2010b; Zhang and Wang, 2012; Vargas et al.,
2013; Schlafer et al., 2016; Ai et al., 2017), dentifrices (Kani et al., 1988, 1989;
Kodaka et al., 1999; Jeong et al., 2007; Najibfard et al., 2011), mouth rinses
(Hannig et al., 2013; Kensche et al., 2017), and toothpastes (Comar et al., 2013; de
Carvalho et al., 2014; Mielczarek and Michalik, 2014; Vyavhare et al., 2015; Souza
et al., 2015; Hill et al., 2015). An artificial dental bite was produced by stereolithography from HA-containing biocomposite (Makvandi et al., 2018). Furthermore, the
application of HA powder was found to be effective in apexogenesis of young
permanent teeth of dogs (Marković et al., 2007). In addition, an interesting
approach to control dental caries by CDHA-osteopontin biocomposites was introduced (Schlafer et al., 2016). Since dental caries is caused by acid production by
bacteria in biofilms located on dental surfaces, its prevention involves a control of
microorganisms producing the acids. Interestingly that HA-containing mouth rinses
were found to be able to reduce the initial bacterial colonization (Kensche et al.,
2017). In another study, CDHA-osteopontin biocomposite particles were prepared
to bind to bacteria in the biofilms, impede biofilms building-up without killing the
microflora, and release orthophosphate ions to buffer bacterial acid production if
pH decreased below 6. Analysis of the results revealed that the treatment by either
CDHA-osteopontin or pure osteopontin led to less biofilm formation compared to
untreated controls. Thus the antibiofilm effect of the CDHA-osteopontin particles
was ascribed to osteopontin, while CDHA was responsible for the buffering effect,
which kept pH always above 5.5 (Schlafer et al., 2016).
Fourth, there are various types of self-setting apatite-forming and/or apatitecontaining formulations (Friedman et al., 1991, 2000; Reddi et al., 1999; Abe et al.,
2009; Benson and Djalilian, 2009; Lee et al., 2010a,b; Singh et al., 2010;
Bambakidis et al., 2010; Krell and Wefel, 1984; Krell and Madison, 1985;
Chohayeb et al., 1987; Sugawara et al., 1990, 2002; Chaung et al., 1996;
Dupoirieux and Gard, 2000; Cherng et al., 2001; Fujikawa et al., 2002; Comuzzi
et al., 2002; Shirakata et al., 2002; Kim et al., 2004; Noetzel et al., 2006;
Witjaksono et al., 2007; Ascherman et al., 2008; Arisan et al., 2010; Barros et al.,
2012; Xiao et al., 2015). For example, a cement was injected as a bone filler for
gaps around oral implants placed on the medial femoral condyles of six goats and
excellent bone formation around the graft material was found. Unfortunately, the
degradation rate of the cement appeared to be very slow and no resorption was
observed (Comuzzi et al., 2002). In another study, a cement was placed on artificially created periodontal defects but no significant difference was found between
the cement and control. Nevertheless, the cement acted as a scaffold for bone formation and provided histocompatible healing of periodontal tissues (Shirakata
et al., 2002). Other investigators used cements for direct pulp capping (Chaung
et al., 1996; Dupoirieux and Gard, 2000) and compared them to calcium hydroxide.
Both materials were found to be equally capable of producing a secondary dentin at
B24 weeks (Chaung et al., 1996). Still other investigators extracted all mandibular
premolar teeth from beagles (Sugawara et al., 2002). After 1 month of healing,
402
Advanced Dental Biomaterials
alveolar bones were reduced to make space for previously fabricated CaPO4 cement
blocks. One more month later, 8 mm HA implants were placed in such a manner
that the apical half was embedded into alveolar bones and the coronal half in the
cement blocks. The investigators observed that the cement blocks were gradually
replaced by bone and the histopathologic features of the cement area were similar
to that of natural bone. Moreover, the coronal half of the implants, previously surrounded by the cement, was firmly attached by natural bone (Sugawara et al.,
2002). In another study, the same researchers used fluorescent labeling analysis and
electron microanalysis to measure the extent of new bone formation and elemental
(Ca, P, Mg) distribution (Fujikawa et al., 2002). Besides, several apatite-forming
and/or apatite-containing self-setting formulations were tested as root canal fillers
(Michaı̈lesco et al., 2005; Sugawara et al., 1990; Noetzel et al., 2006) and sealers
(Krell and Wefel, 1984; Krell and Madison, 1985; Chohayeb et al., 1987; Cherng
et al., 2001; Kim et al., 2004; Witjaksono et al., 2007). Since HA alone does not
possess the self-setting abilities, to create a self-setting formulation it could be
mixed with an epoxy resin (Witjaksono et al., 2007). To impart an antibacterial
effect, an apatite-forming MCPM 1 CaO self-setting formulation with an excess of
CaO (which after contact with water was transformed to Ca(OH)2) was elaborated
(Koch et al., 2010). Finally, injectable forms of such cements can be used as
adjunctive supportive agents for dental implants (Arisan et al., 2010).
An interesting approach was performed in an attempt to regenerate tooth enamel
in vitro using thin and flexible HA sheets (Hontsu et al., 2012). First, a thin HA
film was deposited onto a soluble substrate by pulsed laser deposition technique.
Next, the HA film was collected as a freestanding sheet by dissolving the substrate
using a solvent. HA sheets of one to several microns thick and up to 50 mm in
diameter could be produced by this technique. Then, the HA sheet was adhered to
the extracted human teeth using a CaPO4-containing solution with a pH of 5.5. The
authors found that the HA sheet was fused with tooth enamel within approximately
1 week and that the HA sheet was effective for the restoration and conservation of
the tooth in dental applications (Hontsu et al., 2012). This approach was further
developed in later studies by introducing a bit thicker (8 μm thick) HA sheets with
an additionally deposited thin layer of undisclosed TCP of 500 nm thick
(Yamamoto et al., 2013a,b). One should mention that due to a small thickness, the
HA sheets are transparent (therefore invisible) and their coloration is possible.
Therefore they could be applied in cosmetic dentistry. In addition, the HA sheets
have a number of minute holes that allow liquid and air to escape from underneath
to prevent their forming bubbles when it is applied onto a tooth. One problem is
that it takes almost a whole day for an HA sheet to adhere firmly to the tooth’s
surface. Similar sheets from ACP were developed and tested as well (Kato et al.,
2013, 2015).
More to the point, dental applications of apatites include direct pulp capping
(Higashi, 1996; Jaber et al., 1991, 1992; Li et al., 1998; Hayashi et al., 1999; Zhang
et al., 2008), dentin hypersensitivity treatments (Shetty et al., 2010; Low et al.,
2015; Vano et al., 2018), using in endodontics (Nakagawa, 1983; Maeda et al.,
1984; Roane and Benenati, 1987; Yamaguchi, 1989; Tomizuka, 1990; White and
Calcium orthophosphates as a dental regenerative material
403
Goodis, 1991; MacDonald et al., 1994; Gambarini and Tagger, 1996; Mangin et al.,
2003; Yu et al., 2003; Marković et al., 2004; Teodorović and Martinović, 2005;
Fathi et al., 2006; Masudi et al., 2010; Vaishnavi et al., 2011; Collares et al., 2012;
Wang and Geogi, 2014; Alhashimi et al., 2016), orthodontics (Hara et al., 1989;
Müller, 1989; Schneider and Diedrich, 1989; Giordano et al., 1996; Liang et al.,
1998; Akhavan et al., 2013; Enan and Hammad, 2013; Seifi et al., 2015; Ajami
et al., 2016), oral and maxillofacial surgery (Fischer-Brandies and Dielert, 1985;
Block et al., 2000; Frame et al., 1981; Boyne, 1982; Mangano et al., 1984; Cranin
et al., 1987a,b; Frame and Brady, 1987; Frame, 1987; Asanami et al., 1988;
Shirakawa et al., 1988; Salyer and Hall, 1989; Hemmerle et al., 1995; Kent et al.,
1983; Holmes and Hagler, 1987; Wittkampf, 1988; Friedman et al., 1998; Ylinen
et al., 2002; Hallman et al., 2002; Wiltfang et al., 2004; Zecha et al., 2011; Scarano
et al., 2012; Mercier, 1995; Redondo et al., 1995; Mercier et al., 1996; Lew et al.,
1997; Mishra et al., 2010; Zhang et al., 2010; Sverzut et al., 2015), orthognathic
surgery (Wolford et al., 1987; Moenning and Wolford, 1989; Rosen and Ackerman,
1991; Cottrell and Wolford, 1998; Wolford and Freitas, 1999), prosthodontics
(Larsen et al., 1983, 1984; Balshi, 1987; Nelson and von Gonten, 1988; Tanaka
et al., 1988, 1989; Zeltser et al., 1989; Denissen et al., 1989; Ogiso et al., 1994;
Ngoc et al., 1997; Sung et al., 2007), and periodontics (Meffert et al., 1985; Stahl
and Froum, 1987; Bowen et al., 1989; Mora and Ouhayoun, 1995; Brown et al.,
1998; Yukna et al., 1998; Morris et al., 2000; Okuda et al., 2005, 2009; Kawase
et al., 2010; Trombelli et al., 2010; Heinz et al., 2010; Jung et al., 2011; Horváth
et al., 2013; Yoshinuma et al., 2012; Shirai et al., 2012; Machot et al., 2014;
Madhumathi and Kumar, 2014; Pradeep et al., 2017; Vaca-Cornejo et al., 2017;
Madhumathi et al., 2018). Several apatite-containing biocomposites are commercially produced. The examples comprise Cavalite (Kerr Italia S.r.l., Italia), which is
a light-cured cavity liner containing HA and glass-ionomer powder, as well as
NovaPro Fill and NovaPro Flow (Nanova Biomaterials Inc., Missouri, United
States), which are nanofiber-reinforced biocomposites containing nanodimensional
powder of HA.
To conclude this section, one should mention that due to close chemical and
phase similarities between apatites and dental enamel, dissolution of apatites in
acids is considered a good model of dental caries (Dorozhkin, 2012b).
16.5.1.7 Tetracalcium phosphate
According to the available literature, TTCP alone is rarely used in dentistry (Xu
and Moreau, 2010; Shen et al., 2010). In the vast majority of the cases, TTCP is
combined with either other types of CaPO4 (mainly DCPD or DCPA) or other chemicals to form various self-setting formulations (Sugawara et al., 1989, 2008;
Mehta et al., 2015; Zhou et al., 2016; Moogi et al., 2017; Shetty et al., 2017;
Medvecky et al., 2018; Dickens-Venz et al., 1994; Lee et al., 2003; Dickens et al.,
2003; Xu et al., 2006a; Wei et al., 2011a,b; Thein-Han et al., 2012), biocomposites
(Dickens-Venz et al., 1994; Lee et al., 2003; Dickens et al., 2003; Xu et al., 2009),
as well as root canal sealers (Yoshikawa et al., 1997) and fillings (Chen et al.,
404
Advanced Dental Biomaterials
2013a). For example, a FA forming self-setting formulation consisting of solid
TTCP, solid NaF, and liquid H3PO4 was prepared and used for in vitro filling of
big enamel carious cavities. The results revealed that the hardened formulation was
tightly combined with the enamel surface due to the chemical interaction between
the formulation and enamel apatite (Wei et al., 2011b). A TTCP-containing chewing
gum was prepared and tested (Chow et al., 1994).
16.5.1.8 Biphasic and multiphasic CaPO4 formulations
According to the definition, biphasic and multiphasic CaPO4 formulations represent
various blends of two or more individual types of CaPO4, respectively, and, among
them, a biphasic calcium phosphate (abbreviated as BCP) formulation, consisting of
HA and β-TCP, appears to be the most popular one (Dorozhkin, 2016a). An
injectable bone and dental substitute constituted of BCP and a hydrosoluble cellulose polymer as a carrier was developed (Daculsi et al., 1999). This formulation
was used for filling bone defects after tooth extractions in 11 patients. Three years
after surgery, small biopsies of the implanted areas were harvested and analyzed by
using microcomputed tomography, nondecalcified histology, and histomorphometry. The BCP granules appeared in direct contact with mineralized bone tissue,
thereby supporting bone growth. A gradual substitution of the filler by bone tissue
was observed thus preserving the height of the alveolar bone crest (Weiss et al.,
2007). Similar results were obtained in another study (Struillou et al., 2011). In
addition, BCP was found to be effective for healing of dental bones, osseous, and/
or intrabony defects (Huang et al., 2010a; Ellinger et al., 1986; Nery et al., 1990a,b,
1992; Sculean et al., 2008; Shi et al., 2008; Su et al., 2008; Pandit et al., 2010;
Kaushick et al., 2011; Kim et al., 2011b; Wagner et al., 2012; Pietruska et al.,
2012a; Wang et al., 2012; Seong et al., 2014). For example, micro- and macroporous BCP combined with a fibrin sealant was found to be safe and effective in sinus
floor elevation for dental implant placement, supporting bone regeneration (Wagner
et al., 2012). Furthermore, BCP was used to fill dental root canals (Bosco et al.,
2006) and as a hypersensitivity treatment agent (Ngoc et al., 2018), while a triphasic CaPO4 (α-TCP 1 HA 1 TTCP) was applied as a direct pulp capping material
(Kiba et al., 2010).
16.5.2 Classification according to the dental specialties
16.5.2.1 Endodontics
Generally, root canal filling materials are divided into core materials and root canal
sealers (Table 16.2). Root canal obturation consists of placing an inert filling material in the space previously occupied by pulp tissue. To achieve successful endodontic therapy, it is important to obturate the root canal system completely. Thus the
effective endodontic obturation must provide a dimensionally stable, inert fluidtight apical seal that will eliminate any portal of communication between the canal
space and the surrounding periapical tissues through the apical foramen. According
Calcium orthophosphates as a dental regenerative material
405
to the databases, the earliest publication on the use of CaPO4 in endodontics was
published in Japanese in 1983 (Nakagawa, 1983), followed by a publication in
English in 1984 (Maeda et al., 1984). Several examples of endodontic applications
of CaPO4 are given below.
A case of combined endodonticperiodontic lesions on a mandibular first molar
was treated by intentional replantation and application of HA. Four months after
the surgery, a porcelain-mental full crown restoration was completed. The
15-month follow-up examination showed that the tooth was clinically and radiographically healthy and functioned well (Yu et al., 2003). Several types of CaPO4
[DCPD, OCP, β-TCP, BCP (HA 1 β-TCP), and HA] in particle sizes of ,5 or
,150 μm were used for pulp capping teeth of pigs, rats, and dogs. All types of
CaPO4 showed biocompatibility. Based on these results, it was suggested that these
types of CaPO4 might be useful for specific clinical applications in endodontics,
such as pulp capping (microparticles of HA, β-TCP, BCP) and pulpectomy
(HA, OCP, DCPD) (Jean et al., 1993). Applicability of CaPO4 in pulpotomy and
pulpectomy was confirmed in other studies (Shayegan et al., 2008; Nevins et al.,
1980; Shayegan et al., 2010).
Bone regeneration in endodontically induced periapical lesions using HA,
platelet-rich plasma, and a combination of HA with platelet-rich plasma was evaluated for a period of 1 year with 20 systemically healthy patients (Vaishnavi et al.,
2011). To qualify, the patient had to have a tooth where nonsurgical root canal therapy had failed, periapical radiolucency was present, and periapical root end surgery
was required. The bony defect had to be confined to the apical area, with the bone
covering the entire root surface coronally, with an intact lingual cortical plate. The
patients were randomly divided into four groups, with five patients in each, as follows: replacement with HA; replacement with platelet-rich plasma; replacement
with HA with platelet-rich plasma; and a control group with no substitutes. The
radiographic evaluation revealed that the HA patients showed complete bone regeneration with evidence of a trabecular pattern at the end of 1 year, the platelet-rich
plasma patients showed complete bone regeneration at the end of 9 months, the HA
with platelet-rich plasma patients showed complete bone regeneration at the end of
6 months, while the control patients showed unsatisfactory bone regeneration even
after 1 year. Thus HA addition to platelet-rich plasma was proven to facilitate bone
regeneration (Vaishnavi et al., 2011).
An injectable bone substitute made of a suspension of BCP (HA 1 β-TCP) bioceramics was used to fill dental root canals after removal of canal pulp (Bosco
et al., 2006). The aim of that study was to verify the ability of a CaPO4 ceramic
suspension to fill the apical zone of teeth both ex vivo and in vivo in a sheep
model. The results showed that injection was possible with a good level of BCP
granules at the end of the root dental canal with extracted tooth. The results of scanning electron microscopy investigations revealed mineral formation at the apex
level with mineral tissue conduction between the BCP granules; however, only one
tooth showed a good apical filling with a good sealing. The authors concluded that
the sealing of the apex seemed to depend on the amount of BCP granules (Bosco
et al., 2006).
406
Advanced Dental Biomaterials
Furthermore, there are CaPO4-containing endodontic and/or root canal sealers
(Yoshikawa et al., 1997; Bilginer et al., 1997; Krell and Wefel, 1984; Krell and
Madison, 1985; Chohayeb et al., 1987; Cherng et al., 2001; Kim et al.,
2004; Witjaksono et al., 2007; White and Goodis, 1991; MacDonald et al., 1994;
Marković et al., 2004; Teodorović and Martinović, 2005; Masudi et al., 2010;
Collares et al., 2012; Wang and Geogi, 2014; Alhashimi et al., 2016; Yang et al.,
2007; Khashaba et al., 2009, 2011; Bae et al., 2010, 2011; Shon et al., 2012; Tiwari
and Nandlal, 2012; Chang et al., 2014, 2015; Al-Haddad et al., 2015; Portella et al.,
2015; Wang et al., 2017; Cahyanto et al., 2017; Shieh et al., 2017). The composition of two examples of such sealers (Sankin apatite root canal sealer and Capseal)
are presented in Table 16.5 (Shon et al., 2012). Of them, Capseal was found to
result in both higher alkalinity and higher calcium ion releases than Sankin apatite
root canal sealers (Bae et al., 2011). The results of their application revealed that
the sealers mentioned in Table 16.5 facilitated the periapical dentoalveolar and
alveolar healing by controlling cellular mediators from periodontal ligament cells
and osteoblast differentiation of precursor cells (Shon et al., 2012).
More to the point, endodontic perforations were treated by CaPO4 (Sinai et al.,
1989; Balla et al., 1991; Roane and Benenati, 1987; Chau et al., 1997), but once a
lack of complete healing was noticed (Balla et al., 1991). Additional examples of
the endodontic applications of CaPO4 comprise the following cases. They can be
used as components of endodontic cements (Dou et al., 2017; Yamaguchi, 1989;
Cahyanto et al., 2017; Shieh et al., 2017; Chau et al., 1997; Cherng et al., 2010) or
coatings for endodontic dental implants (Fathi et al., 2006), as well as serve as a
root endfilling material (MacDonald et al., 1994; Mangin et al., 2003) and as endodontic endosseous implants (Tomizuka, 1990). Since CaPO4 does not cause
inflammation (Sinai et al., 1989), it could be used as a hard plug deep inside teeth
(Harbert, 1991). Finally yet importantly, CaPO4 crowns were manufactured (Ishida
et al., 1992).
Table 16.5 Composition of the available CaPO4-containing sealer materials
(Shon et al., 2012).
Brand name
Manufacturer
Components
Sankin apatite root
canal sealer
(I, II, and III)
Sankin Kogyo,
Tokyo, Japan
Capseal (I and II)
Experimental
Powder: α-TCP and Sankin HA in type I,
iodoform is added to powder in type II (30%)
and type III (5%). Liquid: polyacrylic acid and
water
Powder: TTCP and DCPA, Portland cement
(gray cement in type I and white cement in
type II), zirconium oxide, and others.
Liquid: hydroxypropyl methyl cellulose in
sodium phosphate solution
DCPA, Dicalcium phosphate anhydrous; TTCP, tetracalcium phosphate; α-TCP, α-tricalcium phosphate.
Calcium orthophosphates as a dental regenerative material
407
16.5.2.2 Oral and maxillofacial surgery
An insufficient bone volume and a poor bone density are common problems in
edentulous patients with resorbed maxilla. One method that makes implant placement possible in such difficult situations is the augmentation of maxillary sinus
using various bone grafts (Tiwari and Nandlal, 2012). In addition, there are other
cases in which bone grafts appear to be necessary for dentistry-related fields.
Due to these cases, CaPO4 has been used in oral and maxillofacial surgery since
the 1980s (Fischer-Brandies and Dielert, 1985; Frame et al., 1981; Boyne, 1982;
Mangano et al., 1984; Cranin et al., 1987a,b; Frame and Brady, 1987; Frame, 1987;
Asanami et al., 1988; Shirakawa et al., 1988; Salyer and Hall, 1989) and up to now
many scientific articles have been published on the subject (Friedman et al., 1991,
2000; Reddi et al., 1999; Smartt et al., 2005; Kuemmerle et al., 2005; Luaces-Rey
et al., 2009; Tamimi et al., 2009; Abe et al., 2009; Benson and Djalilian, 2009; Lee
et al., 2010a; Singh et al., 2010; Bambakidis et al., 2010; Huang et al., 2010a;
Sanada et al., 2011; Ignatius et al., 2001; Hemmerle et al., 1995). However, as discussed in Section 16.2, the vast majority of the publications on this subject deal
with a treatment of the surrounding bones and, thus, they fall into a category of
bone substitutes, which is another story. Nevertheless, the following directions
of CaPO4 application in oral and maxillofacial surgery can be outlined: coatings on
various types of dental implants (Block et al., 1987, 1994, 2000; Jones et al., 1997,
1999; Gineste et al., 1999; Ong and Chan, 1999; Yoshinari et al., 2002;
Schliephake et al., 2006; Kim et al., 2011a; Jung et al., 2012; Kano et al., 2012;
van Oirschot et al., 2016a,b; Yu and Choe, 2018; Tinsley et al., 2001; Binahmed
et al., 2007; Iezzi et al., 2007; Fathi et al., 2006; Hulshoff and Jansen, 1997;
Alexander et al., 2009; Junker et al., 2011; Palarie et al., 2012; Alghamdi et al.,
2013), augmentation of the surrounding bones (Tamimi et al., 2009; Miura et al.,
2012; Kamakura et al., 1996; Wiltfang et al., 2003, 2004; Zerbo et al., 2004;
Zijderveld et al., 2005; Shayesteh et al., 2008; Marukawa et al., 2011; Klijn et al.,
2012; Yoshino et al., 2013; Block et al., 2000; Sugawara et al., 2002; Schneider
and Diedrich, 1989; Giordano et al., 1996; Liang et al., 1998; Akhavan et al., 2013;
Enan and Hammad, 2013; Seifi et al., 2015; Ajami et al., 2016; Frame et al.,
1981; Boyne, 1982; Mangano et al., 1984; Cranin et al., 1987a,b; Frame and Brady,
1987; Frame, 1987; Asanami et al., 1988; Shirakawa et al., 1988; Salyer and Hall,
1989; Hemmerle et al., 1995; Kent et al., 1983; Holmes and Hagler, 1987;
Wittkampf, 1988; Friedman et al., 1998; Ylinen et al., 2002; Hallman et al., 2002;
Zecha et al., 2011; Scarano et al., 2012; Sato et al., 2009), and use as fillers of osseous mandible and/or jaw defects (Horch et al., 2006; Dupoirieux and Gard, 2000;
Ascherman et al., 2008; Mercier, 1995; Redondo et al., 1995; Mercier et al., 1996;
Lew et al., 1997; Mishra et al., 2010; Zhang et al., 2010; Sverzut et al., 2015).
16.5.2.3 Orthodontics
According to the databases, the earliest publications on the use of CaPO4 in orthodontics appeared in 1989 (Hara et al., 1989; Müller, 1989; Schneider and Diedrich,
408
Advanced Dental Biomaterials
Figure 16.4 Appearances of CaPO4 ceramic brackets (A) Hyaline and (B) Hyaline II.
Source: Reprinted with permission from Meguro, D., Hayakawa, T., Kasai, K., 2006b.
Efficacy of using orthodontic adhesive resin in bonding and debonding characteristics of a
calcium phosphate ceramic bracket. Orthod. Waves 65, 148154.
1989). Coatings of CaPO4 [both HA (Liang et al., 1998) and α-TCP (Niwa et al.,
2009)] were successfully applied to titanium implants and the coated implants were
found to be applicable as anchorage for short-term orthodontic treatment (Liang
et al., 1998) and both types of coatings appeared to be effective stimulators of new
bone formation (Niwa et al., 2009). In another study, HA addition to an orthodontic
cement was found to have a protective action on the dental enamel near the orthodontic bands or brackets (Giordano et al., 1996). Furthermore, there are CaPO4 bioceramic brackets Hyaline (Tomy International Inc., Tokyo, Japan) (Fig. 16.4). In
addition to excellent biocompatibility, these brackets have a hardness equivalent to
that of tooth enamel, which eliminates fears of dental abrasion due to the occluding
tooth even when the patient has a deep-bite (Meguro et al., 2006a,b; Joo and Park,
2007). Besides, there is a study, in which researchers improved antibacterial properties of commercially produced light cure adhesive Transbond XT (3M Oral
Care, Minnesota, United States) by addition of nanodimensional composite particles
of HA with silver. The Transbond XT composite disks containing 5% and 10% of
Ag/HA were found to produce bacterial growth inhibition zones and showed antibacterial properties against biofilms (Sodagar et al., 2016).
However, among all the available types of CaPO4 (Table 16.1), ACP-containing
formulations are most often used in orthodontics (Uysal et al., 2009a,b,c, 2010a,b,c,
2011; Dunn, 2007; Keçik et al., 2008; Foster et al., 2008; Bröchner et al., 2011;
Beerens et al., 2010; Tabrizi and Cakirer, 2011; Chow et al., 2011; Hegde and
Moany, 2012; Bar-Hillel et al., 2012; Çehreli et al., 2012; Hammad et al., 2013;
Park et al., 2013; Gurunathan and Somasundaram, 2015; Baysal and Uysal, 2012;
Liu et al., 2018a). For example, an efficacy of an ACP-containing orthodontic biocomposite and a resin-modified glass-ionomer cement on enamel demineralization
adjacent to orthodontic brackets was evaluated by a new laser fluorescence device.
The authors concluded that both formulations should be recommended for any atrisk orthodontic patient to provide preventive actions and potentially remineralize
subclinical enamel demineralization (Uysal et al., 2009a). Similarly, ACPcontaining orthodontic biocomposites were found to reduce both enamel decalcification around orthodontic brackets (Uysal et al., 2010b,c; Chow et al., 2011) and
Calcium orthophosphates as a dental regenerative material
409
bacterial adherence (Chow et al., 2011). Furthermore, ACP-containing orthodontic
biocomposites were found to possess a lower but still satisfactory bond strength
needed to function as orthodontic adhesives (Uysal et al., 2009b, 2010a; Dunn,
2007; Foster et al., 2008; Sun et al., 2008). Therefore CPPACP biocomposite,
either alone or combined with fluoride, may safely be used as a prophylactic agent
before bracket bonding (Tabrizi and Cakirer, 2011; Çehreli et al., 2012). In addition, a pretreatment by CPPACP, enamel microabrasion, and the combination of
these two methods were found to improve the bonding of orthodontic brackets to
demineralized enamel (Çehreli et al., 2012). Rechargeable orthodontic self-setting
formulations containing ACP with sustained ion release and rerelease were developed, as well (Zhang et al., 2016b; Xie et al., 2018; Liang et al., 2018).
Adiaphorous results were obtained as well. For example, a topical treatment of
white spot lesions after debonding of orthodontic appliances with a CPP-stabilized
ACP agent resulted in significantly reduced fluorescence and reduced areas of the
lesions after 4 weeks; however, the improvement was not superior to the natural
regression following daily use of fluoride toothpaste (Bröchner et al., 2011). In
addition, no clinical advantages for use of a CPP-fluoridated ACP paste supplementary to normal oral hygiene over the time span of 12 weeks were found in another
study (Beerens et al., 2010).
16.5.2.4 Prosthodontics
Humans have long used both natural and synthetic materials as replacements for
lost teeth. For example, the earliest known dental implant was made of iron and
found in a Roman male, who lived around the 1st or 2nd century CE (Crubezy
et al., 1998). The first known tooth made from a natural material was found in a
Mayan woman, estimated around 600 CE, and was made of nacre from seashells
(Bobbio, 1972). Nevertheless, despite a long history of tooth grafts, just a few publications on prosthodontic applications of CaPO4 are available (Table 16.2).
According to the databases, the earliest publication on the subject was published in
1983 (Larsen et al., 1983), followed by another publication by the same authors
(Larsen et al., 1984). A 4-year study and evaluation of nonresorbable HA to augment different alveolar ridges was performed. The technique used resulted in
improved contour, height, and width of the alveolar ridge. The state and health of
the tissues were found to be improved with the use of HA or HA combined with
bone marrow (Larsen et al., 1983). However, the study dealt with a treatment of
bones but not teeth, which is another story. Similar can be said about other publications on the subject (Balshi, 1987; Nelson and von Gonten, 1988; Tanaka et al.,
1988, 1989; Zeltser et al., 1989; Denissen et al., 1989; Ogiso et al., 1994; Ngoc
et al., 1997). Furthermore, as seen from the publication dates, all these papers were
published in the last century and only one recent paper (Sung et al., 2007) has been
found. Nevertheless, even this recent paper is devoted to the subject of preparation,
with just a possibility of using the material as dental prosthesis. Thus one can mention the past attempts to use CaPO4 in prosthetic dentistry and, since no promising
results were obtained, currently CaPO4 is not used in prosthodontics.
410
Advanced Dental Biomaterials
To finalize this topic, it is important to mention that one of the challenges in
dental implantology is to achieve and maintain a good osseointegration, as well as
an epithelial junction of gingival tissues with the implants. An intimate junction
among them may prevent bacteria colonization leading to peri-implantitis, while
the direct bonding may ensure a biomechanical anchoring of the artificial dental
roots (Fig. 16.5) (Lavenus et al., 2010). To achieve this, the presence of sufficient
bone volume is an important prerequisite for dental implant placement. However,
this is not always the case. Namely, atrophic maxilla and mandible bones are less
tolerant to the placement of dental implants due to their reduced height and
width; hence, supplementary bone augmentation by CaPO4 might be necessary
Figure 16.5 Tissue integration of a dental implant. Note the intimate contact with gingival
tissue in the upper part and the desired contact osteogenesis in the tapered lower part rather
than distance osteogenesis.
Source: Reprinted with permission from Lavenus, S., Louarn, G., Layrolle, P., 2010.
Nanotechnology and dental implants. Int. J. Biomater. 2010, 915327.
Calcium orthophosphates as a dental regenerative material
411
(Khoury et al., 2007; Chiapasco et al., 2009). In addition, I would like to point
the readers’ attention to a review on dental implants for patients with osteoporosis. According to the authors, osteoporosis is not a contraindication for the
implant surgery if the accurate analysis of bone quality has been performed
(Gaetti-Jardim et al., 2011).
16.5.2.5 Periodontics (periodontology)
In general, the regeneration of tissues affected by periodontal disease is a complex
process; it encompasses the formation of bones, cementum, and periodontal ligaments (Reis et al., 2011). According to the databases, the earliest publication on the
use of CaPO4 in periodontics was published in 1974 (Levin et al., 1974), followed
by research papers of 1975 (Nery et al., 1975) and 1977 (Gaberthüel and Strub,
1977), and a review of 1978 (Strub and Gaberthüel, 1978). A schematic diagram of
the management of periodontal defects by a bone graft technique is shown in
Fig. 16.6 (Chen et al., 2010). However, as discussed in Section 16.2, the vast majority of the publications on periodontics deal with the treatment of the surrounding
bones and, thus, they fall into a category of bone substitutes (Xu et al., 2006a;
Pepelassi et al., 1991; Baldock et al., 1985; Saffar et al., 1990; Stavropoulos et al.,
2010; Asvanund and Chunhabundit, 2012; Okubo et al., 2013; Saito et al., 2014;
Matsuura et al., 2015; Matsuse et al., 2018; Mellgren et al., 2018; Rezvani et al.,
2015; Ogawa et al., 2016; Cãlin and Pãtraşcu, 2016; Xiao et al., 2015; Meffert
et al., 1985; Stahl and Froum, 1987; Bowen et al., 1989; Mora and Ouhayoun,
1995; Brown et al., 1998; Yukna et al., 1998; Morris et al., 2000; Okuda et al.,
2005, 2009; Kawase et al., 2010; Trombelli et al., 2010; Heinz et al., 2010; Jung
et al., 2011; Horváth et al., 2013; Yoshinuma et al., 2012; Shirai et al., 2012;
Machot et al., 2014; Madhumathi and Kumar, 2014; Pradeep et al., 2017; VacaCornejo et al., 2017; Madhumathi et al., 2018; Nery et al., 1992; Shi et al., 2008;
Figure 16.6 A schematic diagram of the management of periodontal defects by a bone graft
technique. The CaPO4 grafts stimulate bone growth and a new bone fills the defect, which
provides a better support for a tooth (A) open, (B) add, (C) close and fix.
Source: Reprinted with permission from Chen, F.M., Zhang, J., Zhang, M., An, Y., Chen, F.,
Wu, Z.F., 2010. A review on endogenous regenerative technology in periodontal regenerative
medicine. Biomaterials 31, 78927927.
412
Advanced Dental Biomaterials
Kaushick et al., 2011; Pietruska et al., 2012a; Wang et al., 2012; Seong et al., 2014;
Hayashi et al., 2006; Shirakata et al., 2008, 2012; Chitsazi et al., 2011; D’Lima
et al., 2014; Bansal et al., 2014; Dan et al., 2014; Nevins and Cymerman, 2015;
Elgendy and Shady, 2015). Nevertheless, a few examples are given next.
Postextraction bone resorption is an increasing problem in modem dentistry.
Namely, after extraction of a tooth, the bony socket heals naturally. First, it is
immediately filled with coagulated blood. In a few days afterward, the granular and
fibrous tissues are organized to gradually form a new bone tissue. However, due to
the tooth absence, maxilla and/or mandibular alveolar atrophies occur simultaneously. These resorptive and remodeling phenomena of the surrounding bone negatively affect the support for the adjacent teeth; the shallow ridge makes it difficult
for future prosthesis retention and less bony support remains for any dental implant
placement in the future. To promote healing, the socket of an extracted tooth might
be filled by CaPO4 bioceramics. For example, an efficacy of commercial HA granules APAFILL-G as a filler to prevent the resorption of alveolar bone after tooth
extraction was studied (Garcı́a et al., 2001). After 7 days, the result revealed that
only one of all treated patients experienced an adverse response that was observed
under the clinical evaluation and that promptly disappeared after analgesic treatment. The remaining 32 had no adverse clinical response. Radiographically, a continuous radiopacity between bone and the implant resorption was detected after 1
year and the surrounding alveolar bone maintained its contour without symptoms of
resorption for 100% of the patients (Garcı́a et al., 2001). In another study, two different types of HA grafting materials, biomimetic and nanocrystalline, were placed
into fresh extraction sockets aiming to limit bone resorption. The surgical sites
were histologically, clinically, and radiographically evaluated for 6 months after
tooth extraction. The percentages of bone, osteoid areas, and residual material in
the two groups were not statistically different (Checchi et al., 2011).
Furthermore, repositioning maxillary and mandibular bone segments in orthognathic surgery frequently creates bone gaps or continuity defects. These often
require grafting to provide positional stability and bony continuity and CaPO4 is
used for this purpose. For example, as early as 1987 there was a study to evaluate
the use of coralline porous HA as a bone graft substitute in orthognathic surgery
(Wolford et al., 1987), followed by another study in 1989 (Moenning and Wolford,
1989). Ninety-two individual patients received a total of 355 block implants to the
maxilla (294), mandible (41), and midface (20). There were 202 implants positioned directly adjacent to the maxillary sinus. Complications were minimal, the
most common being exposure of the implant to the oral or nasal cavity.
Histological evaluation of implants that were biopsied in nine patients, 416
months’ postsurgery, revealed connective tissue ingrowth throughout the implants
with approximately one-third being bone of variable maturity and two-thirds being
soft tissue (Wolford et al., 1987). Similar results were obtained in another study
(Moenning and Wolford, 1989). Periodontal ligaments around extracted sockets
were found to have an ability to regenerate bone on HA-coated tooth-shaped
implants (Kano et al., 2012). Positive results were also observed in another study,
in which bone formation around BCP (HA 1 β-TCP) particles in periodontal defects
Calcium orthophosphates as a dental regenerative material
413
of dogs were found to be more discernible if compared to healing in the control
(Struillou et al., 2011). In addition, the porosity of the implanted CaPO4 was found
to influence the periodontal healing of furcation defects in dogs (Saito et al., 2012).
To increase a treatment efficiency of the periodontal defects, CaPO4 might be
combined with the biologically active molecules, such as hormones, growth factors,
morphogenetic proteins (Sculean et al., 2008; Lee et al., 2010c; Emerton et al.,
2011; Ridgway et al., 2008; Jayakumar et al., 2011; Sorensen et al., 2004; Pietruska
et al., 2012b; Elangovan et al., 2013). For example, an application of recombinant
human growth and differentiation factor-5 (rhGDF-5) lyophilized onto β-TCP granules demonstrated an effective regeneration of the artificially created periodontal
defects (Lee et al., 2010c; Emerton et al., 2011). Positive results were also obtained
for a combination of a recombinant human platelet-derived growth factor BB
(rhPDGF-BB) with β-TCP for the treatment of human intraosseous periodontal
defects (Ridgway et al., 2008; Jayakumar et al., 2011). However, a combination of
an enamel matrix derivative with BCP (HA 1 β-TCP) resulted in none to minimal
new bone formation (Sculean et al., 2008). Furthermore, a combination of human
bone morphogenetic protein-2 (rhBMP-2) with a bioresorbable CaPO4 cement
Ceredex (ETEX Corporation, Massachusetts, United States) was not suggested for
periodontal indications (Sorensen et al., 2004). Besides, there are results indicating
that the use of CaPO4 after open flap procedure does not improve the clinical and
radiological treatment outcomes of periodontal intrabony defects (Pietruska et al.,
2012b). Thus applications of CaPO4 in periodontology were not always positive.
Additional details on this topic are available in special reviews (Bayani et al.,
2017; Sepantafar et al., 2018).
16.5.2.6 Other types of oral applications
Mucositis is the painful inflammation and ulceration of the mucous membranes lining the digestive tract, usually as an adverse effect of chemotherapy and radiotherapy treatment for cancer. Mucositis can occur anywhere along the gastrointestinal
tract, but oral mucositis refers to the particular inflammation and ulceration that
occurs in the mouth (Mucositis). It can delay discharge, interrupt treatment, and
threaten life. To help the patients, rinses, supersaturated by undisclosed types of
CaPO4, were prepared and evaluated (Papas, 2008; Markiewicz et al., 2012;
Miyamoto et al., 2012; Quinn, 2013; Svanberg et al., 2015; Bhatt et al., 2017). For
example, a review paper is available, in which the author looked at data from all
known adult and pediatric studies investigating the use of a supersaturated by
CaPO4 mouth rinse Caphosol (EUSA Pharma, United Kingdom) in patients receiving
high-dose cancer therapy in order to evaluate its efficacy for both the prevention
and treatment of oral mucositis. Thirty studies were identified. The majority of
these studies (n 5 24) found Caphosol to be efficacious at reducing the grade and/or
duration, as well as pain associated with this disease (Quinn, 2013). However, the
most recent data claim that supersaturated CaPO4 rinses were found to be ineffective in treating mucositis (Svanberg et al., 2015; Bhatt et al., 2017).
414
16.6
Advanced Dental Biomaterials
Tissue engineering approaches
As seen from the aforementioned, CaPO4 is widely used in dentistry to restore and/
or repair various types of oral defects and diseases. However, all the previously
mentioned approaches have encountered shortcomings if compared to the normal
and healthy teeth and surrounding bones. Therefore various tissue engineering
approaches to develop new strategies for tooth regeneration have been attempted.
The history of tissue engineering in dentistry started in 1982, when the first regeneration technology of periodontium was introduced (Nyman et al., 1982). The modern
tissue engineering approaches in dentistry include combinations of cells, engineering materials, and suitable biochemical and physicochemical factors to improve or
replace biological functions. Finally, it will cause in vivo formation and growth of
new functional tissues instead of reparation and/or replacement of damaged and/or
missing ones by artificial materials and/or implants (Chai and Slavkin, 2003; Hu
et al., 2006; Duailibi et al., 2008; Ikeda et al., 2009; Horst et al., 2012). From the
material point of view, there are two main approaches toward making a bioengineered tooth: scaffold-free and scaffold-based regenerations. The scaffold-free
approaches, such as tissue recombination, cell pellet engineering, and chimerical
tooth engineering, are being developed and the correct tooth-like structures could
be generated after transplantation in the subrenal capsule (Yelick and Vacanti,
2006; Nakao et al., 2007; Yu et al., 2007). However, with an exception of using soluble calcium- and orthophosphate-containing solutions to promote proliferation,
osteogenic differentiation, and mineralization of various types of dental cells (An
et al., 2012), the scaffold-free approaches do not utilize CaPO4. Therefore in this
review, only scaffold-based tooth regeneration approaches are considered. A schematic drawing of this process is shown in Fig. 16.7 (Kitamura et al., 2012).
For example, it was hypothesized that dental follicle cells combined with β-TCP
might become a novel therapeutic strategy to restore periodontal defects. The
Figure 16.7 A schematic diagram of entire tooth regeneration from the proper combination
of growth factors and cells (stem cells or progenitor cells) seeded on a CaPO4 scaffold.
Source: Adapted with permission from Kitamura, C., Nishihara, T., Terashita, M., Tabata,
Y., Washio, A., 2012. Local regeneration of dentin-pulp complex using controlled release of
FGF-2 and naturally derived sponge-like scaffolds. Int. J. Dent. 2012, 190561 (8 pp.).
Calcium orthophosphates as a dental regenerative material
415
authors suggested isolation of dental follicle cells from a beagle dog. The isolated
cells should be induced by bone morphogenetic protein-2, basic-fibroblast growth
factors, and dexamethasone and, then, seeded onto β-TCP bioceramics. Afterward,
the complex should be autoimplanted into the periodontal defects in the same dog
to observe regeneration of periodontal tissue in vivo (Zuolin et al., 2010). However,
this was just a hypothesis. Let me describe the real investigations.
The biocompatibility of four different types of 3D scaffolds for the regeneration of tooth tissues was tested (Zheng et al., 2011). The scaffolds consisted of
pure poly(lactic-co-glycolic) acid (PLGA) or 50/50 w/w biocomposites of PLGA
with HA, β-TCP, or carbonate-containing HA. Afterward, human dental pulp stem
cells were seeded onto the scaffolds, followed by implantation into the mesentery
or subrenal capsule of mice or rats for 45 weeks. The results showed that while
all CaPO4-containing formulations were able to support effective regeneration of
the tooth tissues, the PLGA/β-TCP scaffolds appeared to be superior to the other
three scaffolds for tooth tissues regeneration, especially for dentin formation
(Zheng et al., 2011). Very promising results were also obtained by other researchers for β-TCP/chitosan biocomposites (Liao et al., 2010), recombinant human
transforming growth factor-beta 1 (rhTGF-β1) combined with two different bone
grafts: calcified freeze-dried bone allograft and porous BCP (Markopoulou et al.,
2011) and a complex of recombinant human bone morphogenetic protein-2
(rhBMP-2)mediated dental pulp stem cells and nano-sized HA/collagen/poly(Llactide) for clinical reconstruction of periodontal bone defects (Liu et al., 2011).
Positive results were also obtained for polycaprolactone-TCP scaffolds (Goh
et al., 2014).
In still other studies, polyglycolic acid (PGA) scaffolds were compared with
β-TCP, fibrin, and collagen scaffolds for their capacity to grow dental structures
when seeded with tooth germs from 6-month-old minipigs. On fibrin and collagen
gels, the porcine third molar tooth bud maintained its epithelial structure, resembling tooth buds, whereas on PGA and β-TCP the implanted tooth buds produced
more dentin-like material (Ohara et al., 2010). Porous BCP (HA 1 β-TCP),
powdered BCP, and PGA fiber mesh were used as scaffolds and transplanted with
cultured porcine dental pulp-derived cells into the backs of nude mice for 6 weeks.
Although newly formed hard tissues were observed in all implants, a dentin-like
hard tissue was observed when porous BCP was used (Tonomura et al., 2010).
Besides, incorporation of nano-sized HA into electrospun poly(ε-caprolactone)/gelatin
scaffolds was found to enhance dental pulp stem cells differentiation toward an
odontoblast-like phenotype both in vitro and in vivo (Yang et al., 2010). The osteoblast marker bone sialoprotein was highly expressed on β-TCP scaffolds seeded by
dental follicle cells but almost absent in differentiated dental follicle cells without
β-TCP (Viale-Bouroncle et al., 2011). The latter means that dental progenitor cells
have to be combined with CaPO4 bioceramics.
To conclude this topic, the tissue engineering approaches of dental regeneration,
obviously, appear to be the most promising healing technologies and many interesting studies on a combination of CaPO4 scaffolds with cells and/or growth factors
are expected to appear in the near future.
416
16.7
Advanced Dental Biomaterials
Conclusion
The biologically relevant types of CaPO4 are the emerging bioceramics, which are
widely used in various biomedical applications, including dentistry. They have excellent biomedical properties and biological behavior because their composition and
structure are similar to those of human bones and teeth. Therefore CaPO4 possess
exceptional biocompatibility and unique bioactivity, which are widely used in dentistry and dentistry-related fields. For example, incorporation of CaPO4 into various
restorative biomaterials was found to improve the mechanical properties of the biomaterials without impeding their inherent biological properties. Other examples have
been described earlier. Nevertheless, the versatile employing strategies of CaPO4 in
dentistry aim to ultimately reach the same goal, namely, to enhance osseointegration
process of dental implants in the context of immediate loading and to augment formation of surrounding bones to guarantee a long-term success. However, still the complete understanding related to use of CaPO4 in clinical dentistry is lacking and further
research is needed to improve their efficacy in clinical dentistry.
References
Abe, T., Anan, M., Kamida, T., Fujiki, M., 2009. Surgical technique for anterior skull base
reconstruction using hydroxyapatite cement and titanium mesh. Acta Neurochirur. 151,
13371338.
Ai, M., Du, Z., Zhu, S., Geng, H., Zhang, X., Cai, Q., et al., 2017. Composite resin reinforced
with silver nanoparticlesladen hydroxyapatite nanowires for dental application. Dent.
Mater. 33, 1222.
Ajami, S., Pakshir, H.R., Babanouri, N., 2016. Impact of nanohydroxyapatite on enamel surface
roughness and color change after orthodontic debonding. Prog. Orthod. 17, 11 (8 pp.).
Akhavan, A., Sodagar, A., Mojtahedzadeh, F., Sodagar, K., 2013. Investigating the effect of
incorporating nanosilver/nanohydroxyapatite particles on the shear bond strength of
orthodontic adhesives. Acta Odontol. Scand. 71, 10381042.
Alexander, F., Christian, U., Stefan, T., Christoph, V., Reinhard, G., Georg, W., 2009. Longterm effects of magnetron-sputtered calcium phosphate coating on osseointegration of
dental implants in non-human primates. Clin. Oral Implant. Res. 20, 183188.
Alghamdi, H.S., van Oirschot, B.A.J.A., Bosco, R., van den Beucken, J.J., Aldosari, A.A.F.,
Anil, S., et al., 2013. Biological response to titanium implants coated with nanocrystals calcium phosphate or type 1 collagen in a dog model. Clin. Oral Implant. Res. 24, 475483.
Al-Haddad, A., Abu Kasim, N.H., Che Ab Aziz, Z.A., 2015. Interfacial adaptation and thickness of bioceramic-based root canal sealers. Dent. Mater. J. 34, 516521.
Alhashimi, R.A., Mannocci, F., Sauro, S., 2016. Experimental polyethylene-hydroxyapatite
carrier-based endodontic system: an in vitro study on dynamic thermomechanical properties, sealing ability, and measurements of micro-computed tomography voids. Eur. J.
Oral Sci. 24, 279286.
Al-Mullahi, A.M., Toumba, K.J., 2010. Effect of slow-release fluoride devices and casein
phosphopeptide/amorphous calcium phosphate nanocomplexes on enamel remineralization in vitro. Caries Res. 44, 364371.
Calcium orthophosphates as a dental regenerative material
417
Ambrosio, A.M.A., Sahota, J.S., Khan, Y., Laurencin, C.T., 2001. A novel amorphous calcium phosphate polymer ceramic for bone repair: I. Synthesis and characterization. J.
Biomed. Mater. Res. 58, 295301.
An, S., Ling, J., Gao, Y., Xiao, Y., 2012. Effects of varied ionic calcium and phosphate on
the proliferation, osteogenic differentiation and mineralization of human periodontal
ligament cells in vitro. J. Periodontol. Res. 47, 374382.
Antonucci, J.M., Skrtic, D., 2010. Fine-tuning of polymeric resins and their interfaces with
amorphous calcium phosphate. A strategy for designing effective remineralizing dental
composites. Polymers 2, 378392.
Antonucci, J.M., O’Donnell, J.N.R., Schumacher, G.E., Skrtic, D., 2009. Amorphous calcium
phosphate composites and their effect on compositeadhesivedentin bonding.
J. Adhes. Sci. Technol. 23, 11331147.
Arafa, A., 2017. Synergetic remineralization effectiveness of calcium, phosphate and fluoride
based systems in primary teeth. Pediatric Dent. J. 27, 6571.
Arisan, V., Anil, A., Wolke, J.G., Özer, K., 2010. The effect of injectable calcium phosphate
cement on bone anchorage of titanium implants: an experimental feasibility study in
dogs. Int. J. Oral Maxillofac. Surg. 39, 463468.
Arita, K., Yamamoto, A., Shinonaga, Y., Harada, K., Abe, Y., Nakagawa, K., et al., 2011.
Hydroxyapatite particle characteristics influence the enhancement of the mechanical
and chemical properties of conventional restorative glass ionomer cement. Dent. Mater.
J. 30, 672683.
Asanami, S., Koike, O., Chikata, M., Shiba, H., Ikeuchi, S., Okada, Y., et al., 1988. Studies
of the clinical usefulness of porous hydroxylapatite in the field of dental and oral surgery. Keio J. Med. 37, 265281.
Ascherman, J.A., Foo, R., Nanda, D., Parisien, M., 2008. Reconstruction of cranial bone
defects using a quick-setting hydroxyapatite cement and absorbable plates. J. Craniofac.
Surg. 19, 11311135.
Asvanund, P., Chunhabundit, P., 2012. Alveolar bone regeneration by implantation of nacre
and B-tricalcium phosphate in guinea pig. Implant Dent. 21, 248253.
Aykut-Yetkiner, A., Kara, N., Ateş, M., Ersin, N., Ertuğrul, F., 2014. Does casein phosphopeptid amorphous calcium phosphate provide remineralization on white spot lesions and
inhibition of Streptococcus mutans? J. Clin. Pediatr. Dent. 38, 302306.
Bae, W.J., Chang, S.W., Lee, S.I., Kum, K.Y., Bae, K.S., Kim, E.C., 2010. Human periodontal ligament cell response to a newly developed calcium phosphate-based root canal
sealer. J. Endod. 36, 16581663.
Bae, K.H., Chang, S.W., Bae, K.S., Park, D.S., 2011. Evaluation of pH and calcium ion
release in capseal I and II and in two other root canal sealers. Oral Surg. Oral Med. Oral
Pathol. Oral Radiol. Endod. 112, e23e28.
Baldock, W.T., Hutchens Jr., L.H., McFall Jr., W.T., Simpson, D.M., 1985. An evaluation of
tricalcium phosphate implants in human periodontal osseous defects of two patients. J.
Periodontol. 56, 17.
Balla, R., LoMonaco, C.J., Skribner, J., Lin, L.M., 1991. Histological study of furcation
perforations treated with tricalcium phosphate, hydroxylapatite, amalgam, and life.
J. Endod. 17, 234238.
Balshi, T.J., 1987. Preventive durapatite ridge augmentation for esthetic fixed prosthodontics.
J. Prost. Dent. 58, 266270.
Bambakidis, N.C., Munyon, C., Ko, A., Selman, W.R., Megerian, C.A., 2010. A novel
method of translabyrinthine cranioplasty using hydroxyapatite cement and titanium
mesh: a technical report. Skull Base 20, 157161.
418
Advanced Dental Biomaterials
Bansal, R., Patil, S., Chaubey, K., Thakur, R., Goyel, P., 2014. Clinical evaluation of hydroxyapatite and β-tricalcium phosphate composite graft in the treatment of intrabony periodontal defect: a clinico-radiographic study. J. Indian Soc. Periodontol. 18, 610617.
Bao, L., Liu, J., Shi, F., Jiang, Y., Liu, G., 2014. Preparation and characterization of TiO2
and Si-doped octacalcium phosphate composite coatings on zirconia ceramics (Y-TZP)
for dental implant applications. Appl. Surf. Sci. 290, 4852.
Bar-Hillel, R., Feuerstein, O., Tickotsky, N., Shapira, J., Moskovitz, M., 2012. Effects of
amorphous calcium phosphate stabilized by casein phosphopeptides on enamel de- and
remineralization in primary teeth: an in vitro study. J. Dent. Child. (Chic.) 79, 914.
Barros, C.M.B., de Oliveira, S.V., Marques, J.B., Viana, K.M.S., Costa, A.C.F.M., 2012.
Analysis of the hydroxyapatite incorporate MTA dental application. Mater. Sci. Forum
727728, 13811386.
Bayani, M., Torabi, S., Shahnaz, A., Pourali, M., 2017. Main properties of nanocrystalline
hydroxyapatite as a bone graft material in treatment of periodontal defects. A review of
literature. Biotechnol. Biotechnol. Equip. 31, 215220.
Bayrak, S., Tunc, E.S., Sonmez, I.S., Egilmez, T., Ozmen, B., 2009. Effects of casein
phosphopeptide-amorphous calcium phosphate (CPP-ACP) application on enamel
microhardness after bleaching. Am. J. Dent. 22, 393396.
Baysal, A., Uysal, T., 2012. Do enamel microabrasion and casein phosphopeptide-amorphous
calcium phosphate affect shear bond strength of orthodontic brackets bonded to a demineralized enamel surface? Angle Orthod. 82, 3641.
Beerens, M.W., van der Veen, M.H., van Beek, H., Ten Cate, J.M., 2010. Effects of casein
phosphopeptide amorphous calcium fluoride phosphate paste on white spot lesions and
dental plaque after orthodontic treatment: a 3-month follow-up. Eur. J. Oral Sci. 118,
610617.
Bellagarda, G., 1965. La carie dentaria e le sue cure negli scritti degli antichi. [Dental caries and
their treatment in the writings of the ancients]. Minerva Med. 56, 892903 (in Italian).
Benson, A.G., Djalilian, H.R., 2009. Complications of hydroxyapatite bone cement reconstruction of retrosigmoid craniotomy: two cases. Ear Nose Throat J. 88, E1E4.
Besinis, A., van Noort, R., Martin, N., 2012. Infiltration of demineralized dentin with silica
and hydroxyapatite nanoparticles. Dent. Mater. 28, 10121023.
Besinis, A., van Noort, R., Martin, N., 2014. Remineralization potential of fully demineralized dentin infiltrated with silica and hydroxyapatite nanoparticles. Dent. Mater. 30,
249262.
Bhatt, N., Naithani, R., Gupta, S.K., 2017. Supersaturated calcium phosphate rinse in prevention and treatment of mucositis in patients undergoing hematopoietic stem cell transplant. Exp. Clin. Transplant. 15, 567570.
Bilginer, S., Esener, T., Söylemezoglu, F., Tiftik, A.M., 1997. The investigation of biocompatibility and apical microleakage of tricalcium phosphate based root canal sealers.
J. Endod. 23, 105109.
Binahmed, A., Stoykewych, A., Hussain, A., Love, B., Pruthi, V., 2007. Long-term follow-up
of hydroxyapatite-coated dental implants a clinical trial. Int. J. Oral Maxillofac.
Implants 22, 963968.
Block, M.S., Kent, J.N., Kay, J.F., 1987. Evaluation of hydroxylapatite-coated titanium
dental implants in dogs. J. Oral Maxillofac. Surg. 45, 601607.
Block, M.S., Kent, J.N., Beirne, O.R., 1994. Long-term follow-up on hydroxylapatite-coated
cylindrical dental implants: a comparison between developmental and recent periods.
J. Oral Maxillofac. Surg. 52, 937944.
Calcium orthophosphates as a dental regenerative material
419
Block, M.S., Gardiner, D., Almerico, B., Neal, C., 2000. Loaded hydroxylapatite-coated
implants and uncoated titanium-threaded implants in distracted dog alveolar ridges. Oral
Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 89, 676685.
Bobbio, A., 1972. The first endosseous alloplastic implant in the history of man. Bull. Hist.
Dent. 20, 16.
Boneta, A.E., Neesmith, A., Mankodi, S., Berkowitz, H.J., Sánchez, L., Mostler, K., et al.,
2001. The enhanced anticaries efficacy of a sodium fluoride and dicalcium phosphate
dihydrate dentifrice in a dual-chambered tube. A 2-year caries clinical study on children
in the United States of America. Am. J. Dent. 14 (Spec. Iss. 5), 13A17A.
Boone, M.E., Kafrawy, H., 1979. Pulp reaction to a tricalcium phosphate ceramic capping
agent. Oral Surg. Oral Med. Oral Pathol. 47, 369371.
Bosco, J., Enkel, B., Armengol, V., Daculsi, G., Jean, A., Weiss, P., 2006. Bioactive calcium
phosphate material for dental endodontic treatment. Root apical deposition. Key Eng.
Mater. 309311, 11571160.
Bowen, J.A., Mellonig, J.T., Gray, J.L., Towle, H.T., 1989. Comparison of decalcified
freeze-dried bone allograft and porous particulate hydroxyapatite in human periodontal
osseous defects. J. Periodontol. 60, 647654.
Boyne, P., 1982. Impact of durapatite as a bone grafting material in oral and maxillofacial
surgery. Compend. Contin. Educ. Dent. (Suppl. 2), S83S86.
Briak, H.E., Durand, D., Nurit, J., Munier, S., Pauvert, B., Boudeville, P., 2002. Study of a
hydraulic dicalcium phosphate dihydrate/calcium oxide-based cement for dental applications. J. Biomed. Mater. Res. 63, 447453.
Bröchner, A., Christensen, C., Kristensen, B., Tranæus, S., Karlsson, L., Sonnesen, L., et al.,
2011. Treatment of post-orthodontic white spot lesions with casein phosphopeptidestabilised amorphous calcium phosphate. Clin. Oral Investig. 15, 369373.
Brostow, W., Estevez, M., Lobland, H.E.H., Hoang, L., Rodriguez, J.R., Vargar, S., 2008.
Porous hydroxyapatite-based obturation materials for dentistry. J. Mater. Res. 23,
15871596.
Brown, G.D., Mealey, B.L., Nummikoski, P.V., Bifano, S.L., Waldrop, T.C., 1998.
Hydroxyapatite cement implant for regeneration of periodontal osseous defects in
humans. J. Periodontol. 69, 146157.
Browning, W.D., Cho, S.D., Deschepper, E.J., 2012. Effect of a nano-hydroxyapatite paste
on bleaching-related tooth sensitivity. J. Esthet. Restor. Dent. 24, 268276.
Cahyanto, A., Megasari, E., Zakaria, M.N., Djustiana, N., Sunarso, Usri, K., Aripin, D.,
et al., 2017. Fabrication of carbonate apatite cement as endodontic sealer. Key Eng.
Mater. 758, 6165.
Cai, F., Shen, P., Morgan, M.V., Reynolds, E.C., 2003. Remineralization of enamel subsurface lesions in situ by sugar-free lozenges containing casein phosphopeptide-amorphous
calcium phosphate. Aust. Dent. J. 48, 240243.
Cai, F., Manton, D.J., Shen, P., Walker, G.D., Cross, K.J., Yuan, Y., et al., 2007. Effect of
addition of citric acid and casein phosphopeptide-amorphous calcium phosphate to a
sugar-free chewing gum on enamel remineralization in situ. Caries Res. 41, 377383.
Cãlin, C., Pãtraşcu, I., 2016. Growth factors and beta-tricalcium phosphate in the treatment
of periodontal intraosseous defects: a systematic review and meta-analysis of randomised controlled trials. Arch. Oral Biol. 66, 4454.
Cao, C.Y., Mei, M.L., Li, Q.L., Lo, E.C., Chu, C.H., 2014. Agarose hydrogel biomimetic
mineralization model for the regeneration of enamel prism-like tissue. ACS Appl.
Mater. Interfaces 6, 410420.
420
Advanced Dental Biomaterials
Cao, C.Y., Mei, M.L., Li, Q.L., Lo, E.C.M., Chu, C.H., 2015. Methods for biomimetic mineralisation of human enamel: a systematic review. Materials 8, 28732886.
Çehreli, S.B., Şar, C., Polat-Özsoy, O., Ünver, B., Özsoy, S., 2012. Effects of a fluoridecontaining casein phosphopeptide-amorphous calcium phosphate complex on the shear
bond strength of orthodontic brackets. Eur. J. Orthod. 34, 193197.
Chai, Y., Slavkin, H.C., 2003. Prospects for tooth regeneration in the 21st century: a perspective. Microsc. Res. Tech. 60, 469479.
Chang, S.W., Lee, S.Y., Kang, S.K., Kum, K.Y., Kim, E.C., 2014. In vitro biocompatibility,
inflammatory response, and osteogenic potential of 4 root canal sealers: Sealapex,
Sankin apatite root sealer, MTA Fillapex, and iRoot SP root canal sealer. J. Endod. 40,
16421648.
Chang, S.W., Lee, Y.K., Zhu, Q., Shon, W.J., Lee, W.C., Kum, K.Y., et al., 2015.
Comparison of the rheological properties of four root canal sealers. Int. J. Oral Sci. 7,
5661.
Chau, J.Y.M., Hutter, J.W., Mork, T.O., Nicoll, B.K., 1997. An in vitro study of furcation
perforation repair using calcium phosphate cement. J. Endod. 23, 588592.
Chaung, H.M., Hong, C.H., Chiang, C.P., Lin, S.K., Kuo, Y.S., Lan, W.H., et al., 1996.
Comparison of calcium phosphate cement mixture and pure calcium hydroxide as direct
pulp-capping agents. J. Formos. Med. Assoc. 95, 545550.
Checchi, V., Savarino, L., Montevecchi, M., Felice, P., Checchi, L., 2011. Clinicalradiographic and histological evaluation of two hydroxyapatites in human extraction
sockets: a pilot study. Int. J. Oral Maxillofac. Surg. 40, 526532.
Chen, M.H., 2010. Update on dental nanocomposites. J. Dent. Res. 89, 549560.
Chen, H., Clarkson, B.H., Sun, K., Mansfield, J.F., 2005. Self-assembly of synthetic hydroxyapatite nanorods into an enamel prism-like structure. J. Colloid Interface. Sci. 288,
97103.
Chen, F.M., Zhang, J., Zhang, M., An, Y., Chen, F., Wu, Z.F., 2010. A review on endogenous regenerative technology in periodontal regenerative medicine. Biomaterials 31,
78927927.
Chen, Y.Z., Lü, X.Y., Liu, G.D., 2013a. A novel root-end filling material based on hydroxyapatite, tetracalcium phosphate and polyacrylic acid. Int. Endod. J. 46, 556564.
Chen, L., Liang, K., Li, J., Wu, D., Zhou, X., Li, J., 2013b. Regeneration of biomimetic
hydroxyapatite on etched human enamel by anionic PAMAM template in vitro. Arch.
Oral Biol. 58, 975980.
Cherng, A.M., Chow, L.C., Takagi, S., 2001. In vitro evaluation of a calcium phosphate
cement root canal filler/sealer. J. Endod. 27, 613615.
Cherng, A.M., Takagi, S., Chow, L.C., 2010. Acid neutralization capacity of a tricalcium
silicate-containing calcium phosphate cement as an endodontic material. J. Res. Natl.
Inst. Stand. Technol. 115, 471476.
Chiapasco, M., Casentini, P., Zaniboni, M., 2009. Bone augmentation procedures in implant
dentistry. Int. J. Oral Maxillofac. Implants 24 (Suppl. 2), 3759.
Chitsazi, M.T., Shirmohammadi, A., Faramarzie, M., Pourabbas, R., Rostamzadeh, A.N.,
2011. A clinical comparison of nano-crystalline hydroxyapatite (Ostim) and autogenous
bone graft in the treatment of periodontal intrabony defects. Med. Oral Patol. Oral Cir.
Bucal 16, 448453.
Chohayeb, A.A., Chow, L.C., Tsaknis, P., 1987. Evaluation of calcium phosphate as a root
canal sealer-filler material. J. Endod. 13, 384387.
Chow, L.C., Takagi, S., 1995. Remineralization of root lesions with concentrated calcium
and phosphate solutions. Dent. Mater. J. 14, 3136.
Calcium orthophosphates as a dental regenerative material
421
Chow, L.C., Takagi, S., Shern, R.J., Chow, T.H., Takagi, K.K., Sieck, B.A., 1994. Effects on
whole saliva of chewing gums containing calcium phosphates. J. Dent. Res. 73, 2632.
Chow, C.K.W., Wu, C.D., Evans, C.A., 2011. In vitro properties of orthodontic adhesives
with fluoride or amorphous calcium phosphate. Int. J. Dent. 2011, 583521 (8 pp.).
Cochrane, N.J., Cai, F., Huq, N.L., Burrow, M.F., Reynolds, E.C., 2010. New approaches to
enhanced remineralization of tooth enamel. J. Dent. Res. 89, 11871197.
Collares, F.M., Leitune, V.C.B., Rostirolla, F.V., Trommer, R.M., Bergmann, C.P., Samuel,
S.M.W., 2012. Nanostructured hydroxyapatite as filler for methacrylate-based root canal
sealers. Int. Endod. J. 45, 6367.
Comar, L.P., Souza, B.M., Gracindo, L.F., Buzalaf, M.A.R., Magalhães, A.C., 2013. Impact
of experimental nano-HAP pastes on bovine enamel and dentin submitted to a pH
cycling model. Braz. Dent. J. 24, 273278.
Comuzzi, L., Ooms, E., Jansen, J.A., 2002. Injectable calcium phosphate cement as a filler
for bone defects around oral implants, an experimental study in goats. Clin. Oral
Implants Res. 13, 304311.
Corbett, M.E., Moore, W.J., 1971. Distribution of dental caries in ancient British populations. 1.
Anglo-Saxon period. Caries Res. 5, 151168.
Corbett, M.E., Moore, W.J., 1973. Distribution of dental caries in ancient British populations.
II. Iron age, Romano-British and Mediaeval periods. Caries Res. 7, 139153.
Corbett, M.E., Moore, W.J., 1975. Distribution of dental caries in ancient British populations. III.
The 17th century. Caries Res. 9, 163175.
Corbett, M.E., Moore, W.J., 1976. Distribution of dental caries in ancient British populations.
IV. The 19th century. Caries Res. 10, 401414.
Cottrell, D.A., Wolford, L.M., 1998. Long-term evaluation of the use of coralline hydroxyapatite in orthognathic surgery. J. Oral Maxillofac. Surg. 56, 935941. discussion
941942.
Cranin, A.N., Tobin, G.P., Glebman, J., 1987a. Applications of hydroxylapatite in oral and
maxillofacial surgery. Part I: Periodontal and endosteal-implant repairs. Compendium
(Newtown, PA) 8, 254256. 258, 261.
Cranin, A.N., Tobin, G.P., Gelbman, J., 1987b. Applications of hydroxylapatite in oral and
maxillofacial surgery. Part II: Ridge augmentation and repair of major oral defects.
Compendium (Newtown, PA) 8, 334335. 337.
Cravens, J.E., 1876. Lacto-phosphate of lime; pathology and treatment of exposed dental
pulps and sensitive dentine. Dent. Cosmos 18, 463469. discussion 469476.
Cross, K.J., Huq, N.L., Reynolds, E.C., 2016. Casein phosphopeptideamorphous calcium
phosphate nanocomplexes: a structural model. Biochemistry 55, 43164325.
Crubezy, E., Murail, P., Girard, L., Bernadou, J.P., 1998. False teeth of the Roman world.
Nature 391, 29.
Daculsi, G., Weiss, P., Bouler, J.M., Gauthier, O., Millot, F., Aguado, E., 1999. Biphasic calcium phosphate/hydrosoluble polymer composites: a new concept for bone and dental
substitution biomaterials. Bone 25 (Suppl. 1), 59S61S.
Dan, H., Vaquette, C., Fisher, A.G., Hamlet, S.M., Xiao, Y., Hutmacher, D.W., et al., 2014.
The influence of cellular source on periodontal regeneration using calcium phosphate
coated polycaprolactone scaffold supported cell sheets. Biomaterials 35, 113122.
de Carvalho, F.G., Vieira, B.R., Santos, R.L., Carlo, H.L., Lopes, P.Q., de Lima, B.A., 2014.
In vitro effects of nano-hydroxyapatite paste on initial enamel carious lesions. Pediatr.
Dent. 36, 8589.
Denissen, H.W., de Groot, K., 1979. Immediate dental root implants from synthetic dense
calcium hydroxylapatite. J. Prost. Dent. 42, 551556.
422
Advanced Dental Biomaterials
Denissen, H.W., Kalk, W., Veldhuis, A.A.H., van den Hooff, A., 1989. Eleven-year study of
hydroxyapatite implants. J. Prost. Dent. 61, 706712.
Dickens, S.H., Flaim, G.M., Takagi, S., 2003. Mechanical properties and biochemical activity
of remineralizing resin-based CaPO4 cements. Dent. Mater. 19, 558566.
Dickens-Venz, S.H., Takagi, S., Chow, L.C., Bowen, R.L., Johnston, A.D., Dickens, B.,
1994. Physical and chemical properties of resin-reinforced calcium phosphate cements.
Dent. Mater. 10, 100106.
D’Lima, J.P., Paul, J., Palathingal, P., Varma, B.R.R., Bhat, M., Mohanty, M., 2014.
Histological and histometrical evaluation of two synthetic hydroxyapatite based biomaterials in the experimental periodontal defects in dogs. J. Clin. Diagn. Res. 8,
ZC52ZC55.
Dodds, M.W., Chidichimo, D., Haas, M.S., 2012. Delivery of active agents from chewing
gum for improved remineralization. Adv. Dent. Res. 24, 5862.
Domingo, C., Arcı́s, R.W., López-Macipe, A., Osorio, R., Rodrı́guez-Clemente, R., Murtra,
J., et al., 2001. Dental composites reinforced with hydroxyapatite: mechanical behavior
and absorption/elution characteristics. J. Biomed. Mater. Res. 56, 297305.
Dorozhkin, S.V., 2012a. Calcium Orthophosphates: Applications in Nature, Biology, and
Medicine. Pan Stanford, Singapore, 854 pp.
Dorozhkin, S.V., 2012b. Dissolution mechanism of calcium apatites in acids: a review of literature. World J. Methodol. 2, 117.
Dorozhkin, S.V., 2015. Calcium orthophosphates bioceramics. Ceram. Int. 41, 1391313966.
Dorozhkin, S.V., 2016a. Multiphasic calcium orthophosphate (CaPO4) bioceramics and their
biomedical applications. Ceram. Int. 42, 65296554.
Dorozhkin, S.V., 2016b. Calcium orthophosphates (CaPO4): occurrence and properties. Prog.
Biomater. 5, 970.
Dorozhkin, S.V., 2016c. Calcium Orthophosphate-Based Bioceramics and Biocomposites.
Wiley-VCH, Weinheim, Germany, 405 pp.
Dou, W., Mastrogiacomo, S., Veltien, A., Alghamdi, H.S., Walboomers, X.F., Heerschap, A.,
2017. Visualization of calcium phosphate cement in teeth by zero echo time 1H MRI at
high field. NMR Biomed. 31, e3859 (12 pp.).
Dowd, F.J., 1999. Saliva and dental caries. Dent. Clin. North Am. 43, 579597.
Duailibi, S.E., Duailibi, M.T., Zhang, W., Asrican, R., Vacanti, J.P., Yelick, P.C., 2008.
Bioengineered dental tissues grown in the rat jaw. J. Dent. Res. 87, 745750.
Dunn, W.J., 2007. Shear bond strength of an amorphous calcium-phosphate-containing orthodontic resin cement. Am. J. Orthod. Dentofac. Orthoped. 131, 243247.
Dupoirieux, L., Gard, C., 2000. Hydroxyapatite cement for calvarial reconstruction. Oral
Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 89, 140142.
Eccles, J.D., 1979. Dental erosion of nonindustrial origin. A clinical survey and classification. J. Prosthet. Dent. 42, 649653.
Elangovan, S., Jain, S., Tsai, P.C., Margolis, H.C., Amiji, M., 2013. Nano-sized calcium
phosphate particles for periodontal gene therapy. J. Periodontol. 84, 117125.
Elgendy, E.A., Shady, T.E.A., 2015. Clinical and radiographic evaluation of nanocrystalline
hydroxyapatite with or without platelet-rich fibrin membrane in the treatment of periodontal intrabony defects. J. Indian Soc. Periodontol. 19, 6165.
Ellinger, R.F., Nery, E.B., Lynch, K.L., 1986. Histological assessment of periodontal osseous
defects following implantation of hydroxyapatite and biphasic calcium phosphate ceramics: a case report. Int. J. Periodontics Restorative Dent. 6, 2233.
Elliott, J.C., 1994. Structure and chemistry of the apatites and other calcium orthophosphates,
Studies in Inorganic Chemistry, Vol. 18. Elsevier, Amsterdam, The Netherlands, 389 pp.
Calcium orthophosphates as a dental regenerative material
423
Emamieh, S., Khaterizadeh, Y., Goudarzi, H., Ghasemi, A., Baghban, A.A., Torabzadeh, H.,
2015. The effect of two types chewing gum containing casein phosphopeptideamorphous calcium phosphate and xylitol on salivary Streptococcus mutans. J. Conserv.
Dent. 18, 192195.
Emerton, K.B., Drapeau, S.J., Prasad, H., Rohrer, M., Roffe, P., Hopper, K., et al., 2011.
Regeneration of periodontal tissues in non-human primates with rhGDF-5 and betatricalcium phosphate. J. Dent. Res. 90, 14161421.
Enan, E.T., Hammad, S.M., 2013. Microleakage under orthodontic bands cemented with
nano-hydroxyapatite-modified glass ionomer: an in vivo study. Angle Orthod. 83,
981986.
Enax, J., Epple, M., 2018. Synthetic hydroxyapatite as a biomimetic oral care agent. Oral
Health Prev. Dent. 16, 719.
Esteves-Oliveira, M., Santos, N.M., Meyer-Lueckel, H., Wierichs, R.J., Rodrigues, J.A.,
2017. Caries-preventive effect of anti-erosive and nano-hydroxyapatite-containing toothpastes in vitro. Clin. Oral. Investig. 21, 291300.
Fabregas, R., Rubinstein, J., 2014a. On the initial propagation of dental caries. J. R. Soc.
Interface 11, 20140809.
Fabregas, R., Rubinstein, J., 2014b. A mathematical model for the progression of dental caries. Math. Med. Biol. 31, 319337.
Fathi, M.H., Salehi, M., Mortazavi, V., Mousavi, S.B., Parsapour, A., 2006. Novel hydroxyapatite/niobium surface coating for endodontic dental implant. Surf. Eng. 22, 353358.
Fejerskov, O., Kidd, E. (Eds.), 2008. Dental Caries: The Disease and Its Clinical
Management. second ed. Wiley-Blackwell, 640 pp.
Fernández, M.P.R., Gehrke, S.A., Mazón, P., Calvo-Guirado, J.L., de Aza, P.N., 2017.
Implant stability of biological hydroxyapatites used in dentistry. Materials 10, 644.
Finn, S.B., 1967. The role of a dicalcium phosphate chewing gum in the control of human
dental caries. Int. Dent. J. 17, 339352.
Finn, S.B., Jamison, H.C., 1967. The effect of a dicalcium phosphate chewing gum on caries
incidence in children: 30-month results. J. Am. Dent. Assoc. 74, 987995.
Fischer, R.B., Muhler, J.C., Ring, C.E., 1956. X-ray study of fluorapatite formation during
the fluoride treatment of powdered dental enamel. J. Dent. Res. 35, 773777.
Fischer-Brandies, E., Dielert, E., 1985. Clinical use of tricalciumphosphate and hydroxyapatite in maxillofacial surgery. J. Oral Implant. 12, 4044.
Fletcher, J., Walsh, D., Fowler, C.E., Mann, S., 2011. Electrospun mats of PVP/ACP nanofibres for remineralization of enamel tooth surfaces. CrystEngComm 13, 36923697.
Foster, J.A., Berzins, D.W., Bradley, T.G., 2008. Bond strength of an amorphous calcium
phosphate-containing orthodontic adhesive. Angle Orthod. 78, 339344.
Frame, J.W., 1987. Hydroxyapatite as a biomaterial for alveolar ridge augmentation. Int. J.
Oral Maxillofac. Surg. 16, 642655.
Frame, J.W., Brady, C.L., 1987. The versatility of hydroxyapatite blocks in maxillofacial surgery. Br. J. Oral Maxillofac. Surg. 25, 452464.
Frame, J.W., Brady, C.L., Browne, R.M., 1981. Augmentation of the edentulous mandible
using bone and hydroxyapatite: a comparative study in dogs. Int. J. Oral Surg. 10, 8892.
Friedman, C.D., Costantino, P.D., Jones, K., Chow, L.C., Pelzer, H., Sisson, G., 1991.
Hydroxyapatite cement. II. Obliteration and reconstruction of the cat frontal sinus. Arch.
Otolaryngol. Head Neck Surg. 117, 385389.
Friedman, C.D., Costantino, P.D., Takagi, S., Chow, L.C., 1998. BoneSourcet hydroxyapatite cement, a novel biomaterial for craniofacial skeletal tissue engineering and reconstruction. J. Biomed. Mater. Res. 43, 428432.
424
Advanced Dental Biomaterials
Friedman, C.D., Costantino, P.D., Synderman, C.H., Chow, L.C., Takagi, S., 2000.
Reconstruction of the frontal sinus and frontofacial skeleton with hydroxyapatite
cement. Arch. Facial Plast. Surg. 2, 124129.
Fujikawa, K., Sugawara, A., Kusama, K., Nishiyama, M., Murai, S., Takagi, S., et al., 2002.
Fluorescent labeling analysis and electron probe microanalysis for alveolar ridge
augmentation using calcium phosphate cement. Dent. Mater. J. 21, 296305.
Fujita, H., 2009. Dental caries in Japanese human skeletal remains. J. Oral Biosci 51,
105114.
Gaberthüel, T.W., Strub, J.R., 1977. Treatment of periodontal pockets with tricalcium phosphate in man. A preliminary report. SSO Schweiz Monatsschr. Zahnheilkd. 87,
809814.
Gaetti-Jardim, E.C., Santiago-Junior, J.F., Goiato, M.C., Pellizer, E.P., Magro-Filho, O.,
Jardim Jr., E.G., 2011. Dental implants in patients with osteoporosis: a clinical reality?
J. Craniofac. Surg. 22, 11111113.
Gaffar, A., Blake-Haskins, J., Mellberg, J., 1993. In vivo studies with a dicalcium phosphate
dihydrate/MFP system for caries prevention. Int. Dent. J 43 (Suppl. 1), 8188.
Gambarini, G., Tagger, M., 1996. Sealing ability of a new hydroxyapatite-containing endodontic sealer using lateral condensation and thermatic compaction of gutta-percha,
in vitro. J. Endod. 22, 165167.
Garcı́a, D., Garcı́a, L., Pérez, M.P., Suarez, M., Delgado, J.A., Garcı́a, R., et al., 2001. Filling
of post-extraction dental socket with hydroxyapatite granules APAFILL-Gt. Key Eng.
Mater. 192195, 925928.
Geiger, S., Matalon, S., Blasbalg, J., Tung, M.S., Eichmiller, F.C., 2003. The clinical effect
of amorphous calcium phosphate (ACP) on root surface hypersensitivity. Oper. Dent.
28, 496500.
Gineste, L., Gineste, M., Ranz, X., Ellefterion, A., Guilhem, A., Rouquet, N., et al., 1999.
Degradation of hydroxylapatite, fluorapatite, and fluorhydroxyapatite coatings of dental
implants in dogs. J. Biomed. Mater. Res. 48, 224234.
Giniger, M., MacDonald, J., Spaid, M., Felix, H., 2005a. A 180-day clinical investigation of
the tooth whitening efficacy of a bleaching gel with added amorphous calcium phosphate. J. Clin. Dent. 16, 1116.
Giniger, M., MacDonald, J., Ziemba, S., Felix, H., 2005b. The clinical performance of professionally dispensed bleaching gel with added amorphous calcium phosphate. J. Am.
Dent. Assoc. 136, 383392.
Giordano, M., Macchi, A., Ostinelli, E., Tagliabue, A., 1996. Effetto protettivo sullo smalto
della idrossilapatite ultramicronizzata addizionata ad un cemento composito ortodontico.
Studio in vivo. [Protective effect on enamel of ultra-micronized hydroxyapatite in combination with orthodontic composite cement. In vivo study]. Minerva Stomatol. 45,
2935.
Goh, B.T., Chanchareonsook, N., Tideman, H., Teoh, S.H., Chow, J.K., Jansen, J.A., 2014.
The use of a polycaprolactone-tricalcium phosphate scaffold for bone regeneration of
tooth socket facial wall defects and simultaneous immediate dental implant placement in
Macaca fascicularis. J. Biomed. Mater. Res. A 102A, 13791388.
Gomes, Y.S.L., Alexandrino, L.D., Alencar, C.M., Alves, E.B., Faial, K.C., Silva, C.M.,
2017. In situ effect of nanohydroxyapatite paste in enamel teeth bleaching. J. Contemp.
Dent. Pract. 18, 9961003.
González-Cabezas, C., 2010. The chemistry of caries: remineralization and demineralization
events with direct clinical relevance. Dent. Clin. North. Am. 54, 469478.
Calcium orthophosphates as a dental regenerative material
425
Gu, H., Mijares, D., Zhao, Z., Boylan, R., Ling, J., LeGeros, R.Z., 2013. Experimental antibacterial and mineralizing calcium phosphate-based treatment for dentin surfaces. J.
Biomater. Appl. 27, 783790.
Gupta, R., Prakash, V., 2011. CPP-ACP complex as a new adjunctive agent for remineralisation: a review. Oral Health Prev. Dent. 9, 151165.
Gurunathan, D., Somasundaram, S., 2015. Prevention of white spot lesion in orthodontic
patients using casein phosphopeptide-stabilized amorphous calcium phosphate a systematic review. Int. J. Pharma Bio Sci. 6, B702B706.
Haghgoo, R., Rezvani, M.B., Zeinabadi, M.S., 2014. Comparison of nano-hydroxyapatite and
sodium fluoride mouthrinse for remineralization of incipient carious lesions. J. Dent.
(Tehran) 11, 406410.
Hallman, M., Hedin, M., Sennerby, L., Lundgren, S., 2002. A prospective 1-year clinical and
radiographic study of implants placed after maxillary sinus floor augmentation with
bovine hydroxyapatite and autogenous bone. J. Oral Maxillofac. Surg. 60, 277284.
Hamba, H., Nikaido, T., Inoue, G., Sadr, A., Tagami, J., 2011. Effects of CPP-ACP with
sodium fluoride on inhibition of bovine enamel demineralization: a quantitative assessment using micro-computed tomography. J. Dent. 39, 405413.
Hammad, S.M., El Banna, M.S., Elsaka, S.E., 2013. Twelve-month bracket failure rate with
amorphous calcium phosphate bonding system. Eur. J. Orthod. 35, 622627.
Hannig, C., Basche, S., Burghardt, T., Al-Ahmad, A., Hannig, M., 2013. Influence of a
mouthwash containing hydroxyapatite microclusters on bacterial adherence in situ. Clin.
Oral Investig. 17, 805814.
Hara, Y., Murakami, T., Kajiyama, K., Maeda, K., Akamine, A., Nagamine, N., et al., 1989.
Application of calcium phosphate ceramics to periodontal therapy. 8. Effects of orthodontic force on repaired bone with hydroxyapatite. Nihon Shishubyo Gakkai Kaishi 31,
224234.
Harbert, H., 1991. Generic tricalcium phosphate plugs: an adjunct in endodontics. J. Endod.
17, 131134.
Hasnamudhia, F., Bachtiar, E.W., Sahlan, M., Soekanto, S.A., 2017. The effect of CPP-ACPpropolis chewing gum on calcium and phosphate ion release on caries-active subjects’ saliva
and the formation of Streptococcus mutans biofilm. J. Phys. Conf. Ser. 884, 012137.
Hayashi, Y., Imai, M., Yanagiguchi, K., Viloria, I.L., Ikeda, T., 1999. Hydroxyapatite applied
as direct pulp capping medicine substituted for osteodentin. J. Endod. 25, 225229.
Hayashi, C., Kinoshita, A., Oda, S., Mizutani, K., Shirakata, Y., Ishikawa, I., 2006.
Injectable calcium phosphate bone cement provides favorable space and a scaffold for
periodontal regeneration in dogs. J. Periodontol. 77, 940946.
Head, J.A., 1912. A study of saliva and its action on tooth enamel in reference to its hardening and softening. J. Am. Med. Assoc. 59, 21182122.
Hegde, M., Moany, A., 2012. Remineralization of enamel subsurface lesions with casein
phosphopeptide-amorphous calcium phosphate: a quantitative energy dispersive X-ray
analysis using scanning electron microscopy: an in vitro study. J. Conserv. Dent. 15,
6167.
Heinz, B., Kasaj, A., Teich, M., Jepsen, S., 2010. Clinical effects of nanocrystalline hydroxyapatite paste in the treatment of intrabony periodontal defects: a randomized controlled
clinical study. Clin. Oral Investig. 14, 525531.
Heller, A.I., Koenigs, J.F., Brilliant, J.D., Melfi, R.C., Driskell, T.D., 1975. Direct pulp capping of permanent teeth in primates using a resorbable form of tricalcium phosphate
ceramic. J. Endod. 1, 95101.
426
Advanced Dental Biomaterials
Hemmerle, J., Leize, M., Voegel, J.C., 1995. Long-term behaviour of a hydroxyapatite/collagen-glycosaminoglycan biomaterial used for oral surgery: a case report. J. Mater. Sci.
Mater. Med. 6, 360366.
Hicks, M.J., Flaitz, C.M., 2000. Enamel caries formation and lesion progression with a fluoride dentifrice and a calcium-phosphate containing fluoride dentifrice: a polarized light
microscopic study. ASDC J. Dent. Child. 67, 2128.
Higashi, T., 1996. Influence of particle size of calcium phosphate ceramics as a capping
agent on the formation of a hard tissue barrier in amputated dental pulp. J. Endod. 22,
281283.
Hill, R.G., Gillam, D.G., Chen, X., 2015. The ability of a nano hydroxyapatite toothpaste and
oral rinse containing fluoride to protect enamel during an acid challenge using 19F solid
state NMR spectroscopy. Mater. Lett. 156, 6971.
Hiller, K.A., Buchalla, W., Grillmeier, I., Neubauer, C., Schmalz, G., 2018. In vitro effects
of hydroxyapatite containing toothpastes on dentin permeability after multiple applications and ageing. Sci. Rep. 8, 4888.
Himel, V., Brady, J., Weir, J., 1985. Evaluation of repair of mechanical perforations of the
pulp chamber floor using biodegradable tricalcium phosphate or calcium hydroxide. J.
Endod. 11, 161165.
Höland, W., Schweiger, M., Watzke, R., Peschke, A., Kappert, H., 2008. Ceramics as biomaterials for dental restoration. Expert Rev. Med. Dev 5, 729745.
Holmes, R.E., Hagler, H.K., 1987. Porous hydroxylapatite as a bone graft substitute in mandibular contour augmentation: a histometric study. J. Oral Maxillofac. Surg. 45,
421429.
Hontsu, S., Kato, N., Yamamoto, E., Nishikawa, H., Kusunoki, M., Hayami, T., et al., 2012.
Regeneration of tooth enamel by flexible hydroxyapatite sheet. Key Eng. Mater.
493494, 615619.
Horch, H.H., Sader, R., Pautke, C., Neff, A., Deppe, H., Kolk, A., 2006. Synthetic, purephase beta-tricalcium phosphate ceramic granules (Cerasorbs) for bone regeneration in
the reconstructive surgery of the jaws. Int. J. Oral Maxillofac. Surg. 35, 708713.
Horst, O.V., Chavez, M.G., Jheon, A.H., Desai, T., Klein, O.D., 2012. Stem cell and biomaterials research in dental tissue engineering and regeneration. Dent. Clin. North Am. 56,
495520.
Horváth, A., Stavropoulos, A., Windisch, P., Lukács, L., Gera, I., Sculean, A., 2013.
Histological evaluation of human intrabony periodontal defects treated with an unsintered nanocrystalline hydroxyapatite paste. Clin. Oral Investig. 17, 423430.
Hu, B., Nadiri, A., Kuchler-Bopp, S., Perrin-Schmitt, F., Peters, H., Lesot, H., 2006. Tissue
engineering of tooth crown, root, and periodontium. Tissue Eng. 12, 20692075.
Huang, S.B., Gao, S.S., Yu, H.Y., 2009. Effect of nano-hydroxyapatite concentration on
remineralization of initial enamel lesion in vitro. Biomed. Mater. 4, 034104.
Huang, M.S., Wu, H.D., Teng, N.C., Peng, B.Y., Wu, J.Y., Chang, W.J., et al., 2010a. In
vivo evaluation of poorly crystalline hydroxyapatite-based biphasic calcium phosphate
bone substitutes for treating dental bony defects. J. Dent. Sci. 5, 100108.
Huang, S., Gao, S., Cheng, L., Yu, H., 2010b. Combined effects of nano-hydroxyapatite and
Galla chinensis on remineralisation of initial enamel lesion in vitro. J. Dent. 38, 811819.
Huang, S., Gao, S., Cheng, L., Yu, H., 2011. Remineralization potential of nanohydroxyapatite on initial enamel lesions: an in vitro study. Caries Res. 45, 460468.
Hulshoff, J.E.G., Jansen, J.A., 1997. Initial interfacial healing events around calcium phosphate (Ca-P) coated oral implants. Clin. Oral Implant. Res. 8, 393400.
Calcium orthophosphates as a dental regenerative material
427
Hüttemann, R.W., Dönges, H., 1987. Untersuchungen zur Therapie überempfindlicher
Zahnhälse mit Hydroxylapatit. Dtsch. Zahnärztl. Z 42, 486488.
Iezzi, G., Scarano, A., Petrone, G., Piattelli, A., 2007. Two human hydroxyapatite-coated
dental implants retrieved after a 14-year loading period: a histologic and histomorphometric case report. J. Periodontol. 78, 940947.
Ignatius, A.A., Ohnmacht, M., Claes, L.E., Kreidler, J., Palm, F., 2001. A composite polymer/tricalcium phosphate membrane for guided bone regeneration in maxillofacial surgery. J. Biomed. Mater. Res. 58, 564569.
Iijima, Y., Cai, F., Shen, P., Walker, G., Reynolds, C., Reynolds, E.C., 2004. Acid resistance
of enamel subsurface lesions remineralized by a sugar-free chewing gum containing
casein phosphopeptide-amorphous calcium phosphate. Caries Res. 38, 551556.
Ikeda, E., Morita, R., Nakao, K., Ishida, K., Nakamura, T., Takano-Yamamoto, T., et al.,
2009. Fully functional bioengineered tooth replacement as an organ replacement therapy. Proc. Natl. Acad. Sci. U.S.A. 106, 1347513480.
Ilie, O., van Loosdrecht, M.C.M., Picioreanu, C., 2012. Mathematical modelling of tooth
demineralisation and pH profiles in dental plaque. J. Theor. Biol. 309, 159175.
Imamura, Y., Tanaka, Y., Nagai, A., Yamashita, K., Takagi, Y., 2010. Self-sealing ability of OCPmediated cement as a deciduous root canal filling material. Dent. Mater. J. 29, 582588.
Ishida, H., Nahara, Y., Hamada, T., 1992. Dimensional accuracy of castable apatite ceramic
crowns: the influence of heat treatment on dimensional changes and distortion of
crowns. J. Prost. Dent. 68, 279283.
Itthagarun, A., King, N.M., Yiu, C., Dawes, C., 2005. The effect of chewing gums containing
calcium phosphates on the remineralization of artificial caries-like lesions in situ. Caries
Res. 39, 251254.
Jaber, L., Mascres, C., Donohue, W.B., 1991. Electron microscope characteristics of dentin
repair after hydroxyapatite direct pulp capping in rats. J. Oral. Pathol. Med. 20,
502508.
Jaber, L., Mascrès, C., Donohue, W.B., 1992. Reaction of the dental pulp to hydroxyapatite.
Oral Surg. Oral Med. Oral Pathol. 73, 9298.
Jandt, K.D., 2006. Probing the future in functional soft drinks on the nanometre scale
towards tooth friendly soft drinks. Trends Food Sci. Technol. 17, 263271.
Jayakumar, A., Rajababu, P., Rohini, S., Butchibabu, K., Naveen, A., Reddy, P.K., et al.,
2011. Multi-centre, randomized clinical trial on the efficacy and safety of recombinant
human platelet-derived growth factor with β-tricalcium phosphate in human intraosseous periodontal defects. J. Clin. Periodontol. 38, 163172.
Jean, A.H., Pouezat, J.A., Daculsi, G., 1993. Pulpal response to calcium phosphate materials.
In vivo study of calcium phosphate materials in endodontics. Cell. Mater. 3, 193200.
Jones, J.D., Saigusa, M., van Sickels, J.E., Tiner, B.D., Gardner, W.A., 1997. Clinical evaluation
of hydroxyapatite-coated titanium plasma-sprayed and titanium plasma-sprayed cylinder
dental implants. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 84, 137141.
Jones, J.D., Lupori, J., van Sickels, J.E., Gardner, W., 1999. A 5-year comparison of
hydroxyapatite-coated titanium plasma-sprayed and titanium plasma-sprayed cylinder
dental implants. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 87, 649652.
Jeong, S.H., Jang, S.O., Kim, K.N., Kwon, H.K., Park, Y.D., Kim, B.I., 2006.
Remineralization potential of new toothpaste containing nano-hydroxyapatite. Key Eng.
Mater. 309311, 537540.
Jeong, S.H., Hong, S.J., Choi, C.H., Kim, B.I., 2007. Effect of new dentifrice containing nanosized carbonated apatite on enamel remineralization. Key Eng. Mater. 330332, 291294.
428
Advanced Dental Biomaterials
Joo, H.J., Park, Y.G., 2007. Friction of calcium phosphate brackets to stainless steel wire.
Korean J. Orthod. 37, 376385.
Jung, U.W., Lee, J.S., Park, W.Y., Cha, J.K., Hwang, J.W., Park, J.C., et al., 2011. Periodontal
regenerative effect of a bovine hydroxyapatite/collagen block in one-wall intrabony
defects in dogs: a histometric analysis. J. Periodont. Implant Sci. 41, 285292.
Jung, U.W., Hwang, J.W., Choi, D.Y., Hu, K.S., Kwon, M.K., Choi, S.H., et al., 2012.
Surface characteristics of a novel hydroxyapatite-coated dental implant. J. Periodont.
Implant Sci 42, 5963.
Junker, R., Manders, P.J.D., Wolke, J., Borisov, Y., Braceras, I., Jansen, J.A., 2011. Bone
reaction adjacent to microplasma-sprayed calcium phosphate-coated oral implants subjected to an occlusal load, an experimental study in the dog. Clin. Oral Implant. Res. 22,
135142.
Kamakura, S., Sasano, Y., Nakamura, M., Suzuki, O., Ohki, H., Kagayama, M., et al., 1996.
Initiation of alveolar ridge augmentation in the rat mandible by subperiosteal implantation of octacalcium phosphate. Arch. Oral Biol. 41, 10291038.
Kani, T., Kani, M., Isozaki, A., Kato, H., Fukuoka, Y., Ohashi, T., et al., 1988. The effect to
apatite-containing dentifrices on artificial caries lesions. J. Dent. Health 38, 364365.
Kani, T., Kani, M., Isozaki, A., Shimatani, H., Ohashi, T., Tokumoto, T., 1989. Effect of
apatite-containing dentifrices on dental caries in school children. J. Dent. Health 39,
104109.
Kano, T., Yamamoto, R., Miyashita, A., Komatsu, K., Hayakawa, T., Sato, M., et al., 2012.
Regeneration of periodontal ligament for apatite-coated tooth-shaped titanium implants
with and without occlusion using rat molar model. J. Hard Tissue Biol. 21, 189202.
Karlinsey, R.L., Pfarrer, A.M., 2012. Fluoride plus functionalized β-TCP: a promising combination for robust remineralization. Adv. Dent. Res. 24, 4852.
Karlinsey, R.L., Mackey, A.C., Walker, E.R., Frederick, K.E., 2010a. Surfactant-modified
β-TCP: structure, properties, and in vitro remineralization of subsurface enamel lesions.
J. Mater. Sci. Mater. Med. 21, 20092020.
Karlinsey, R.L., Mackey, A.C., Walker, E.R., Frederick, K.E., 2010b. Preparation, characterization and in vitro efficacy of an acid-modified β-TCP material for dental hard-tissue
remineralization. Acta Biomater. 6, 969978.
Kato, N., Yamamoto, E., Isai, A., Nishikawa, H., Kusunoki, M., Yoshikawa, K., et al., 2013.
Ultrathin amorphous calcium phosphate freestanding sheet for dentin tubule sealing.
Bioceram. Dev. Appl. S1, 007.
Kato, N., Isai, A., Yamamoto, E., Nishikawa, H., Kusunoki, M., Yoshikawa, K., et al., 2015.
Evaluation of dentin tubule sealing rate improved by attaching ultrathin amorphous calcium phosphate sheet. Key Eng. Mater. 631, 258261.
Kaushick, B.T., Jayakumar, N.D., Padmalatha, O., Varghese, S., 2011. Treatment of human
periodontal infrabony defects with hydroxyapatite 1 β tricalcium phosphate bone graft
alone and in combination with platelet rich plasma: a randomized clinical trial. Indian J.
Dent. Res. 22, 505510.
Kawai, T., Matsui, K., Ezoe, Y., Kajii, F., Suzuki, O., Takahashi, T., et al., 2018. Efficacy of
octacalcium phosphate collagen composite for titanium dental implants in dogs.
Materials 11, 229.
Kawase, T., Okuda, K., Kogami, H., Nakayama, H., Nagata, M., Sato, T., et al., 2010.
Human periosteum-derived cells combined with superporous hydroxyapatite blocks used
as an osteogenic bone substitute for periodontal regenerative therapy: an animal implantation study using nude mice. J. Periodontol. 81, 420427.
Calcium orthophosphates as a dental regenerative material
429
Keçik, D., Çehreli, S.B., Şar, Ç., Ünver, B., 2008. Effect of acidulated phosphate fluoride
and casein phosphopeptide-amorphous calcium phosphate application on shear bond
strength of orthodontic brackets. Angle Orthod. 78, 129133.
Kensche, A., Pötschke, S., Hannig, C., Richter, G., Hoth-Hannig, W., Hannig, M., 2016.
Influence of calcium phosphate and apatite containing products on enamel erosion. Sci.
World. J. 2016, 7959273 (12 pp.).
Kensche, A., Holder, C., Basche, S., Tahan, N., Hannig, C., Hannig, M., 2017. Efficacy of a
mouthrinse based on hydroxyapatite to reduce initial bacterial colonisation in situ. Arch.
Oral. Biol. 80, 1826.
Kent, J.N., Quinn, J.H., Zide, M.F., 1983. Alveolar ridge augmentation using nonresorbable
hydroxylapatite with or without autogenous cancellous bone. J. Oral Maxillofac. Surg.
41, 629642.
Kerr, N.W., 1990. The prevalence and pattern of distribution of root caries in a Scottish
medieval population. J. Dent. Res. 69, 857860.
Khashaba, R.M., Chutkan, N.B., Borke, J.L., 2009. Comparative study of biocompatibility of
newly developed calcium phosphate-based root canal sealers on fibroblasts derived from
primary human gingiva and a mouse L929 cell line. Int. Endod. J. 42, 711718.
Khashaba, R.M., Moussa, M.M., Chutkan, N.B., Borke, J.L., 2011. The response of subcutaneous connective tissue to newly developed calcium phosphate-based root canal sealers.
Int. Endod. J. 44, 342352.
Khoury, F., Antoun, H., Missika, P., 2007. Bone Augmentation in Oral Implantology.
Quintessence Publishing, Hanover Park, IL, 435 pp.
Kiba, W., Imazato, S., Takahashi, Y., Yoshioka, S., Ebisu, S., Nakano, T., 2010. Efficacy of
polyphasic calcium phosphates as a direct pulp capping material. J. Dent. 38, 828837.
Kim, J.S., Baek, S.H., Bae, K.S., 2004. In vitro study of the biocompatibility of newly developed calcium phosphate-based root canal sealers. J. Endod. 30, 708711.
Kim, B.I., Jeong, S.H., Jang, S.O., Kim, K.N., Kwon, H.K., Park, Y.D., 2006. Tooth whitening
effect of toothpastes containing nano-hydroxyapatite. Key Eng. Mater. 309311, 541544.
Kim, M.Y., Kwon, H.K., Choi, C.H., Kim, B.I., 2007. Combined effects of nanohydroxyapatite and NaF on remineralization of early caries lesion. Key Eng. Mater.
330332, 13471350.
Kim, S.H., Park, J.B., Lee, C.W., Koo, K.T., Kim, T.I., Seol, Y.J., et al., 2009. The clinical
effects of a hydroxyapatite containing toothpaste for dentine hypersensitivity. J. Korean
Acad. Periodontol. 39, 8794.
Kim, S.G., Hahn, B.D., Park, D.S., Lee, Y.C., Choi, E.J., Chae, W.S., et al., 2011a. Aerosol
deposition of hydroxyapatite and 4-hexylresorcinol coatings on titanium alloys for dental implants. J. Oral Maxillofac. Surg. 69, e354e363.
Kim, S., Jung, U.W., Lee, Y.K., Choi, S.H., 2011b. Effects of biphasic calcium phosphate
bone substitute on circumferential bone defects around dental implants in dogs. Int. J.
Oral Maxillofac. Implants 26, 265273.
Kitamura, C., Nishihara, T., Terashita, M., Tabata, Y., Washio, A., 2012. Local regeneration
of dentin-pulp complex using controlled release of FGF-2 and naturally derived spongelike scaffolds. Int. J. Dent. 2012, 190561 (8 pp.).
Klijn, R.J., Hoekstra, J.W.M., van den Beucken, J.J.J.P., Meijer, G.J., Jansen, J.A., 2012.
Maxillary sinus augmentation with microstructured tricalcium phosphate ceramic in
sheep. Clin. Oral Implant. Res. 23, 274280.
Koch, K.A., Brave, D.G., Nasseh, A.A., 2010. Bioceramic technology: closing the endorestorative circle, Part I. Dent. Today 29, 100105.
430
Advanced Dental Biomaterials
Kodaka, T., Kobori, M., Hirayama, A., Masayuki, A., 1999. Abrasion of human enamel by
brushing with a commercial dentifrice containing hydroxyapatite crystals in vitro. J.
Electron Microsc. 48, 167172.
Koenigs, J.F., Heller, A.L., Brilliant, J.D., Melfi, R.C., Driskell, T.D., 1975. Induced apical
closure of permanent teeth in adult primates using a resorbable form of tricalcium phosphate ceramic. J. Endod. 1, 102106.
Kouassi, M., Michaı̈lesco, P., Lacoste-Armynot, A., Boudeville, P., 2003. Antibacterial effect
of a hydraulic calcium phosphate cement for dental applications. J. Endod. 29, 100103.
Koulourides, T., Cueto, H., Pigman, W., 1961. Rehardening of softened enamel surfaces of
human teeth by solutions of calcium phosphates. Nature 189, 226227.
Kovtun, A., Kozlova, D., Ganesan, K., Biewald, C., Seipold, N., Gaengler, P., et al., 2012.
Chlorhexidine-loaded calcium phosphate nanoparticles for dental maintenance treatment: combination of mineralising and antibacterial effects. RSC Adv. 2, 870875.
Krell, K.V., Madison, S., 1985. Comparison of apical leakage in teeth obturated with a calcium phosphate cement or Grossman’s cement using lateral condensation. J. Endod. 11,
336339.
Krell, K.V., Wefel, J.S., 1984. A calcium phosphate cement root canal sealer scanning
electron microscopic analysis. J. Endod. 10, 571576.
Kuemmerle, J.M., Oberle, A., Oechslin, C., Bohner, M., Frei, C., Boecken, I., et al., 2005.
Assessment of the suitability of a new brushite calcium phosphate cement for cranioplasty an experimental study in sheep. J. Cran. Maxillofac. Surg. 33, 3744.
Kumar, V.L.N., Itthagarun, A., King, N.M., 2008. The effect of casein phosphopeptideamorphous calcium phosphate on remineralization of artificial caries-like lesions: an
in vitro study. Aust. Dent. J. 53, 3440.
Lanfranco, L.P., Eggers, S., 2012. Caries through time: an anthropological overview. In: Li,
M.Y. (Ed.), Contemporary Approach to Dental Caries. InTech, Rijeka, Croatia,
pp. 334.
Langhorst, S.E., O’Donnell, J.N.R., Skrtic, D., 2009. In vitro remineralization of enamel by
polymeric amorphous calcium phosphate composite: quantitative microradiographic
study. Dent. Mater. 25, 884891.
Larsen, H.D., Finger, I.M., Guerra, L.R., Kent, J.N., 1983. Prosthodontic management of the
hydroxylapatite denture patient: a preliminary report. J. Prost. Dent. 49, 461470.
Larsen, H.D., Guerra, L.R., Finger, I.M., 1984. Hydroxylapatite: prosthodontic clinical considerations. Compend. Contin. Educ. Dent. 5, 786790.
Lavenus, S., Louarn, G., Layrolle, P., 2010. Nanotechnology and dental implants. Int. J.
Biomater. 2010, 915327 (9 pp.).
Lee, Y.K., Lim, B.S., Kim, C.W., 2003. Mechanical properties of calcium phosphate based
dental filling and regeneration materials. J. Oral Rehabil. 30, 418425.
Lee, H.J., Min, J.H., Choi, C.H., Kwon, H.G., Kim, B.I., 2007. Remineralization potential
of sports drink containing nano-sized hydroxyapatite. Key Eng. Mater. 330-332,
275278.
Lee, D.W., Kim, J.Y., Lew, D.H., 2010a. Use of rapidly hardening hydroxyapatite cement
for facial contouring surgery. J. Craniofac. Surg. 21, 10841088.
Lee, S.K., Lee, S.K., Lee, S.I., Park, J.H., Jang, J.H., Kim, H.W., et al., 2010b. Effect of calcium phosphate cements on growth and odontoblastic differentiation in human dental
pulp cells. J. Endod. 36, 15371542.
Lee, J.S., Wikesjö, U.M.E., Jung, U.W., Choi, S.H., Pippig, S., Siedler, M., et al., 2010c.
Periodontal wound healing/regeneration following implantation of recombinant human
Calcium orthophosphates as a dental regenerative material
431
growth/differentiation factor-5 in a β-tricalcium phosphate carrier into one-wall intrabony defects in dogs. J. Clin. Periodontol. 37, 382389.
LeGeros, R.Z., 1988. Calcium phosphate materials in restorative dentistry: a review. Adv.
Dent. Res. 2, 164180.
LeGeros, R.Z., 1991. Calcium Phosphates in Oral Biology and Medicine. Karger, Basel,
Switzerland, 210 pp.
LeGeros, R.Z., 1999. Calcium phosphates in demineralization/remineralization processes. J.
Clin. Dent. 10, 6573.
Levin, M.P., Getter, L., Cutright, D.E., Bhaskar, S.N., 1974. Biodegradable ceramic in periodontal defects. Oral Surg. Oral Med. Oral Pathol. 38, 344351.
Lew, D., Farrell, B., Bardach, J., Keller, J., 1997. Repair of craniofacial defects with hydroxyapatite cement. J. Oral Maxillofac. Surg. 55, 14411449. discussion 14491451.
Li, T., Akao, M., Takagi, M., 1998. Tissue reaction of hydroxyapatite sol to rat molar pulp.
J. Mater. Sci. Mater. Med. 9, 631642.
Li, B.G., Wang, J.P., Zhao, Z.Y., Sui, Y.F., Zhang, Y.X., 2007. Mineralizing of nanohydroxyapatite powders on artificial caries. Rare Metal. Mat. Eng. 36, 128130.
Li, L., Pan, H.H., Tao, J.H., Xu, X.R., Mao, C.Y., Gu, X.H., et al., 2008. Repair of enamel
by using hydroxyapatite nanoparticles as the building blocks. J. Mater. Chem. 18,
40794084.
Li, X., Wang, J., Joiner, A., Chang, J., 2014a. The remineralisation of enamel: a review of
the literature. J. Dent 42 (Suppl. 1), S12S20.
Li, J., Xie, X., Wang, Y., Yin, W., Antoun, J.S., Farella, M., et al., 2014b. Long-term remineralizing effect of casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) on
early caries lesions in vivo: a systematic review. J. Dent. 42, 769777.
Liang, X., Tang, S.Q., Lu, D., Zhao, Z.H., Chao, Y.L., Wang, H., 1998. Study on
hydroxyapatite-coated titanium implants used as orthodontic anchorage an experimental investigation of implant stability and peri-implant neck tissue in dogs. Chin. J. Dent.
Res. 1, 5761.
Liang, K., Zhou, H., Weir, M.D., Bao, C., Reynolds, M.A., Zhou, X., et al., 2017a. Poly
(amido amine) and calcium phosphate nanocomposite remineralization of dentin in
acidic solution without calcium phosphate ions. Dent. Mater. 33, 818829.
Liang, K., Weir, M.D., Reynolds, M.A., Zhou, X., Li, J., Xu, H.H.K., 2017b. Poly (amido
amine) and nano-calcium phosphate bonding agent to remineralize tooth dentin in cyclic
artificial saliva/lactic acid. Mater. Sci. Eng. C 72, 717.
Liang, K., Xiao, S., Wu, J., Li, J., Weir, M.D., Cheng, L., et al., 2018. Long-term dentin
remineralization by poly(amido amine) and rechargeable calcium phosphate nanocomposite after fluid challenges. Dent. Mater. 34, 607618.
Liao, F., Chen, Y., Li, Z., Wang, Y., Shi, B., Gong, Z., et al., 2010. A novel bioactive threedimensional β-tricalcium phosphate/chitosan scaffold for periodontal tissue engineering.
J. Mater. Sci. Mater. Med. 21, 489496.
Lim, K.T., Suh, J.D., Kim, J., Choung, P.H., Chung, J.H., 2011. Calcium phosphate bioceramics fabricated from extracted human teeth for tooth tissue engineering. J. Biomed.
Mater. Res. B: Appl. Biomater. 99B, 399411.
Lin, J., Zhu, J., Gu, X., Wen, W., Li, Q., Fischer-Brandies, H., et al., 2011. Effects of incorporation of nano-fluorapatite or nano-fluorohydroxyapatite on a resin-modified glass
ionomer cement. Acta Biomater. 7, 13461353.
Lippert, F., Parker, D.M., Jandt, K.D., 2004a. In situ remineralisation of surface softened
human enamel studied with AFM nanoindentation. Surf. Sci. 553, 105114.
432
Advanced Dental Biomaterials
Lippert, F., Parker, D.M., Jandt, K.D., 2004b. In vitro demineralization / remineralization
cycles at human tooth enamel surfaces investigated by AFM and nanoindentation. J.
Colloid Interface Sci. 280, 442448.
Lippert, F., Parker, D.M., Jandt, K.D., 2004c. Toothbrush abrasion of surface softened enamel
studied with tapping mode AFM and AFM nanoindentation. Caries Res. 38, 464472.
Liu, H.C., E, L.L., Wang, D.S., Su, F., Wu, X., Shi, Z.P., et al., 2011. Reconstruction of alveolar
bone defects using bone morphogenetic protein 2 mediated rabbit dental pulp stem cells
seeded on nano-hydroxyapatite/collagen/poly(L-lactide). Tissue Eng. A 17, 24172433.
Liu, Y., Zhang, L., Niu, L.N., Yu, T., Xu, H.H.K., Weir, M.D., et al., 2018a. Antibacterial
and remineralizing orthodontic adhesive containing quaternary ammonium resin monomer and amorphous calcium phosphate nanoparticles. J. Dent. 72, 5363.
Liu, Y., Zhang, L., Niu, L.N., Yu, T., Xu, H.H.K., Weir, M.D., et al., 2018b. Antibacterial
and remineralizing orthodontic adhesive containing quaternary ammonium resin monomer and amorphous calcium phosphate nanoparticles. J. Dent. 72, 5363.
Llena, C., Forner, L., Baca, P., 2009. Anticariogenicity of casein phosphopeptide-amorphous
calcium phosphate: a review of the literature. J. Contemp. Dent. Pract. 10, 19.
Low, S.B., Allen, E.P., Kontogiorgos, E.D., 2015. Reduction in dental hypersensitivity with
nano-hydroxyapatite, potassium nitrate, sodium monoflurophosphate and antioxidants.
Open Dent. J 9, 9297.
Lu, K., Meng, X., Zhang, J., Li, X., Zhou, M., 2007. Inhibitory effect of synthetic nanohydroxyapatite on dental caries. Key Eng. Mater. 336338, 15381541.
Luaces-Rey, R., Garcı́a-Rozado, A., Crespo-Escudero, J.L., Seijas, B.P., Arenaz-Búa, J.,
López-Cedrún, J.L., 2009. Use of carbonated calcium phosphate bone cement and
resorbable plates for the treatment of frontal sinus fractures: two case reports. J. Plast.
Reconstr. Aesthet. Surg. 62, 272273.
Lucas, M.E., Arita, K., Nishino, M., 2003. Toughness, bonding and fluoride release properties of hydroxyapatite-added glass ionomer cement. Biomaterials 24, 37873794.
Luo, J., Ning, T., Cao, Y., Zhu, X., Xu, X., Tang, X., et al., 2012. Biomimic enamel remineralization by hybridization calcium- and phosphate-loaded liposomes with amelogenininspired peptide. Key Eng. Mater. 512-515, 17271730.
Lussi, A. (Ed.), 2006. Dental Erosion: From Diagnosis to Therapy. Karger, Basel, Switzerland, 219 pp.
Lv, K., Zhang, J., Meng, X., Li, X., 2007. Remineralization effect of the nano-HA toothpaste
on artificial caries. Key Eng. Mater. 330332, 267270.
Lv, K.L., Yuan, H.W., Meng, X.C., Li, X.Y., 2010. Remineralized evaluation of nanohydroxyapatite to artificial caries. Adv. Mater. Res. 105106, 576579.
MacDonald, A., Moore, B.K., Newton, C.W., Brown Jr., C.E., 1994. Evaluation of an apatite
cement as a root end filling material. J. Endod. 20, 598604.
Machot, E.A., Hoffmann, T., Lorenz, K., Khalili, I., Noack, B., 2014. Clinical outcomes after
treatment of periodontal intrabony defects with nanocrystalline hydroxyapatite (Ostim)
or enamel matrix derivatives (Emdogain): a randomized controlled clinical trial.
BioMed Res. Int. 2014, 786353 (9 pp.).
Madhumathi, K., Kumar, T.S.S., 2014. Regenerative potential and anti-bacterial activity of
tetracycline loaded apatitic nanocarriers for the treatment of periodontitis. Biomed.
Mater. (Bristol) 9, Article number 035002.
Madhumathi, K., Rekha, L.J., Kumar, T.S.S., 2018. Tailoring antibiotic release for the treatment of periodontal infrabony defects using bioactive gelatin-alginate/apatite nanocomposite films. J. Drug Deliv. Sci. Technol. 43, 5764.
Maeda, Y., Okada, M., Okuno, Y., Soga, K., Yamamoto, H., Okazaki, M., 1984. Clinical
application of implant stabilizers: combined use of single-crystal sapphire endodontic
implants with hydroxyapatite particles. J. Osaka Univ. Dent. Sch. 24, 131144.
Calcium orthophosphates as a dental regenerative material
433
Maksimovskii, I.M., Zemskova, M.I., 1994. Primenenie kal’tsii-fosfatnoi keramiki pri lechenii glubokogo kariesa. [The use of a calcium phosphate ceramic in treating deep caries.].
Stomatologiia 73, 1417.
Makvandi, P., Corcione, C.E., Paladini, F., Gallo, A.L., Montagna, F., Jamaledin, R., et al.,
2018. Antimicrobial modified hydroxyapatite composite dental bite by stereolithography. Polym. Adv. Technol. 29, 364371.
Mangano, C., Venini, E., Venini, G., 1984. Il DAC blu come sostituto dell’osso in chirurgia
orale. [Dense apatite ceramic (DAC) as a bone substitute in oral surgery]. Dent. Cadmos
52, 97. 100101, 104105.
Mangin, C., Yesilsoy, C., Nissan, R., Stevens, R., 2003. The comparative sealing ability of
hydroxyapatite cement, mineral trioxide aggregate, and super ethoxybenzoic acid as
root-end filling materials. J. Endod. 29, 261264.
Markiewicz, M., Dzierzak-Mietla, M., Frankiewicz, A., Zielinska, P., Koclega, A.,
Kruszelnicka, M., et al., 2012. Treating oral mucositis with a supersaturated calcium
phosphate rinse: comparison with control in patients undergoing allogeneic hematopoietic stem cell transplantation. Support. Care Cancer 20, 22232229.
Markopoulou, C.E., Dereka, X.E., Vavouraki, H.N., Pepelassi, E.E., Mamalis, A.A.,
Karoussis, I.K., et al., 2011. Effect of rhTGF-β1 combined with bone grafts on human
periodontal cell differentiation. Growth Factors 29, 1420.
Marković, D., Živojinović, V., Koković, V., Jokanović, V., 2004. Hydroxyapatite as a root
canal system filling material: cytotoxicity testing. Mater. Sci. Forum 453454, 555560.
Marković, D., Petrović, V., Krstić, N., Lazarević-Macanović, M., Nikolić, Z., 2007.
Radiological assessment of apex formation following use of hydroxyapatite. Acta Veter.
(Beograd) 57, 275287.
Marukawa, K., Ueki, K., Okabe, K., Nakagawa, K., Yamamoto, E., 2011. Use of self-setting
α-tricalcium phosphate for maxillary sinus augmentation in rabbit. Clin. Oral Implant.
Res. 22, 606612.
Masudi, S.M., Luddin, N., Mohamad, D., Alkashakhshir, J.J., Adnan, R., Ramli, R.A., 2010.
In vitro study on apical sealing ability of nano-hydroxyapatite-filled epoxy resin based
endodontic sealer. AIP Conf. Proceed. 1217, 467471.
Matsuse, K., Hashimoto, Y., Kakinoki, S., Yamaoka, T., Morita, S., 2018. Periodontal regeneration induced by porous alpha-tricalcium phosphate with immobilized basic fibroblast
growth factor in a canine model of 2-wall periodontal defects. Med. Mol. Morphol. 51,
4856.
Matsuura, T., Akizuki, T., Hoshi, S., Ikawa, T., Kinoshita, A., Sunaga, M., et al., 2015.
Effect of a tunnel-structured β-tricalcium phosphate graft material on periodontal regeneration: a pilot study in a canine one-wall intrabony defect model. J. Periodont. Res. 50,
347355.
Mayne, R.J., Cochrane, N.J., Cai, F., Woods, M.G., Reynolds, E.C., 2011. In-vitro study of
the effect of casein phosphopeptide amorphous calcium fluoride phosphate on iatrogenic
damage to enamel during orthodontic adhesive removal. Am. J. Orthod. Dentofac.
Orthoped. 139, e543e551.
McClendon, J.F., Carpousis, A., 1945. Prevention of dental caries by brushing the teeth with
powdered fluorapatite. J. Dent. Res. 24, 199.
Medvecky, L., Stulajterova, R., Giretova, M., Mincik, J., Vojtko, M., Balko, J., et al., 2018.
Effect of tetracalcium phosphate/monetite toothpaste on dentin remineralization and
tubule occlusion in vitro. Dent. Mater. 34, 442451.
Meffert, R.M., Thomas, J.R., Hamilton, K.M., Brownstein, C.N., 1985. Hydroxylapatite as an
alloplastic graft in the treatment of human periodontal osseous defects. J. Periodontol.
56, 6373.
434
Advanced Dental Biomaterials
Meguro, D., Hayakawa, T., Kawasaki, M., Kasai, K., 2006a. Shear bond strength of calcium
phosphate ceramic brackets to human enamel. Angle Orthod. 76, 301305.
Meguro, D., Hayakawa, T., Kasai, K., 2006b. Efficacy of using orthodontic adhesive resin in
bonding and debonding characteristics of a calcium phosphate ceramic bracket. Orthod.
Waves 65, 148154.
Mehdawi, I., Neel, E.A., Valappil, S.P., Palmer, G., Salih, V., Pratten, J., et al., 2009.
Development of remineralizing, antibacterial dental materials. Acta Biomater. 5,
25252539.
Mehta, D., Gowda, V., Finger, W.J., Sasaki, K., 2015. Randomized, placebo-controlled study
of the efficacy of a calcium phosphate containing paste on dentin hypersensitivity. Dent.
Mater. 31, 12981303.
Mei, H.L., Chen, L.Y., Zhang, D., Zhang, P.L., Liu, B., Zhao, W., et al., 2009. Effects of
casein phosphopeptide-stabilized amorphous calcium phosphate solution on enamel
remineralization. J. Clin. Rehabil. Tissue Eng. Res. 13, 48254828.
Mellgren, T., Qin, T., Öhman-Mägi, C., Zhang, Y., Wu, B., Xia, W., et al., 2018. Calcium
phosphate microspheres as a delivery vehicle for tooth-bleaching agents. J. Dent. Res.
97, 283288.
Melo, M.A., Cheng, L., Weir, M.D., Hsia, R.C., Rodrigues, L.K., Xu, H.H.K., 2013a. Novel
dental adhesive containing antibacterial agents and calcium phosphate nanoparticles. J.
Biomed. Mater. Res. B: Appl. Biomater. 101B, 620629.
Melo, M.A., Cheng, L., Zhang, K., Weir, M.D., Rodrigues, L.K., Xu, H.H.K., 2013b. Novel
dental adhesives containing nanoparticles of silver and amorphous calcium phosphate.
Dent. Mater. 9, 199210.
Mendes, A.C., Restrepo, M., Bussaneli, D., Zuanon, A.C., 2018. Use of casein amorphous
calcium phosphate (CPP-ACP) on white-spot lesions: randomised clinical trial. Oral
Health Prev. Dent. 16, 2731.
Meng, X., Lv, K., Zhang, J., Qu, D., 2007. Caries inhibitory activity of the nano-HA in vitro.
Key Eng. Mater. 330332, 251254.
Mercier, P., 1995. Failures in ridge reconstruction with hydroxyapatite. Analysis of cases and
methods for surgical revision. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod.
80, 389393.
Mercier, P., Bellavance, F., Cholewa, J., Djokovic, S., 1996. Long-term stability of atrophic
ridges reconstructed with hydroxylapatite: a prospective study. J. Oral Maxillofac. Surg.
54, 960969.
Michaı̈lesco, P., Kouassi, M., Briak, H.E., Armynot, A., Boudeville, P., 2005. Antimicrobial
activity and tightness of a DCPD CaO-based hydraulic calcium phosphate cement for
root canal filling. J. Biomed. Mater. Res. B: Appl. Biomater. 74B, 760-767.
Mielczarek, A., Michalik, J., 2014. The effect of nano-hydroxyapatite toothpaste on enamel
surface remineralization. An in vitro study. Am. J. Dent. 27, 287290.
Miloslavich, E.L., 1925. Calcium metabolism in its relation to dental pathology calciprival
odontopathia. Int. J. Orthodontia Oral Surg. Radiography 11, 111123.
Min, J.H., Kwon, H.K., Kim, B.I., 2011. The addition of nano-sized hydroxyapatite to a sports
drink to inhibit dental erosion in vitro study using bovine enamel. J. Dent. 39, 629635.
Mishra, S., Singh, R.K., Mohammad, S., Pradhan, R., Pal, U.S., 2010. A comparative evaluation of decalcified freeze dried bone allograft, hydroxyapatite and their combination in
osseous defects of the jaws. J. Maxillofac. Oral Surg. 9, 236240.
Miura, K., Matsui, K., Kawai, T., Kato, Y., Matsui, A., Suzuki, O., et al., 2012. Octacalcium
phosphate collagen composites with titanium mesh facilitate alveolar augmentation in
canine mandibular bone defects. Int. J. Oral Maxillofac. Surg. 41, 11611169.
Calcium orthophosphates as a dental regenerative material
435
Miyamoto, C.T., Wobb, J., Micaily, B., Li, S., Achary, M.P., 2012. A retrospective match
controlled study of supersaturated calcium phosphate oral rinse vs. supportive care for
radiation induced oral mucositis. J. Cancer Ther. 3, 630636.
Mjör, I.A., Toffenetti, F., 2000. Secondary caries: a literature review with case reports.
Quintessence Int. 31, 165179.
Moenning, J.E., Wolford, L.M., 1989. Coralline porous hydroxyapatite as a bone graft substitute in orthognathic surgery: 24-month follow-up results. Int. J. Adult Orthod.
Orthognathic Surg. 4, 105117.
Monroe, E.A., Votava, W., Bass, D.B., Mcmullen, J., 1971. New calcium phosphate ceramic
material for bone and tooth implants. J. Dent. Res. 50, 860862.
Moogi, P., Rupesh, M.C., Mehta, D., Finger, W.J., Sasaki, K., 2017. A novel desensitizer
paste containing calcium phosphate: randomized, placebo-controlled, double-blinded
and 6 months trial. World J. Dent. 8, 440444.
Mora, F., Ouhayoun, J.P., 1995. Clinical evaluation of natural coral and porous hydroxyapatite implants in periodontal bone lesions: results of a 1-year follow-up. J. Clin.
Periodontol. 22, 877884.
Moreau, J.L., Sun, L., Chow, L.C., Xu, H.H.K., 2011. Mechanical and acid neutralizing properties and bacteria inhibition of amorphous calcium phosphate dental nanocomposite. J.
Biomed. Mater. Res. B: Appl. Biomater. 98B, 8088.
Morgan, M.V., Adams, G.G., Bailey, D.L., Tsao, C.E., Fischman, S.L., Reynolds, E.C., 2008.
The anticariogenic effect of sugar-free gum containing CPP-ACP nanocomplexes on
approximal caries determined using digital bitewing radiography. Caries Res. 42, 171184.
Morris, H.F., Ochi, S., Spray, J.R., Olson, J.W., 2000. Periodontal-type measurements associated with hydroxyapatite-coated and non-HA-coated implants: uncovering to 36 months.
Ann. Periodontol. 5, 5667.
Moshaverinia, A., Ansari, S., Moshaverinia, M., Roohpour, N., Darr, J.A., Rehman, I.,
2008a. Effects of incorporation of hydroxyapatite and fluoroapatite nanobioceramics
into conventional glass ionomer cements (GIC). Acta Biomater. 4, 432440.
Moshaverinia, A., Ansari, S., Movasaghi, Z., Billington, R.W., Darr, J.A., Rehman, I.U.,
2008b. Modification of conventional glass-ionomer cements with N-vinylpyrrolidone
containing polyacids, nano-hydroxy and fluoroapatite to improve mechanical properties.
Dent. Mater. 24, 13811390.
Müller, N., 1989. Alveolarfortsatzerhohung mit Hydroxylapatit. Klinische Erfahrungen aus
prothetischer Sicht. [Augmentation of alveolar process with hydroxylapatite. Clinical
orthodontic experience]. Dtsch. Zahnarztl. Z 44, 596599.
Najibfard, K., Chedjieu, I., Ramalingam, K., Amaechi, B.T., 2011. Remineralization of early
caries by a nano-hydroxyapatite dentifrice. J. Clin. Dent. 22, 139143.
Nakagawa, K.I., 1983. Clinico-pathological studies of dental biomaterials in endodontic therapy, with special reference to the biocompatibility of the hydroxyapatite on exposed
vital human pulp. Shikwa Gakuho 83, 501527.
Nakao, K., Morita, R., Saji, Y., Ishida, K., Tomita, Y., Ogawa, M., et al., 2007. The development of a bioengineered organ germ method. Nat. Methods 4, 227230.
Nakata, T., Kitasako, Y., Sadr, A., Nakashima, S., Tagami, J., 2018. Effect of a calcium
phosphate and fluoride paste on prevention of enamel demineralization. Dent. Mater. J.
37, 6570.
Nelson, D.R., von Gonten, A.S., 1988. Prosthodontic management of the hydroxylapatiteaugmented ridge. Gen. Dent. 36, 315319.
Nery, E.B., Lynch, K.L., Hirthe, W.M., Mueller, K.H., 1975. Bioceramic implants in surgically produced infrabony defects. J. Periodontol. 46, 328347.
436
Advanced Dental Biomaterials
Nery, E.B., Lynch, K.L., Rooney, G.E., 1978. Alveolar ridge augmentation with tricalcium
phosphate ceramic. J. Prost. Dent. 40, 668675.
Nery, E.B., Eslami, A., van Swol, R.L., 1990a. Biphasic calcium phosphate ceramic combined with fibrillar collagen with and without citric acid conditioning in the treatment of
periodontal osseous defects. J. Periodontol. 61, 166172.
Nery, E.B., Lee, K.K., Czajkowski, S., Dooner, J.J., Duggan, M., Ellinger, R.F., et al., 1990b.
A Veterans Administration Cooperative Study of biphasic calcium phosphate ceramic in
periodontal osseous defects. J. Periodontol. 61, 737744.
Nery, E.B., LeGeros, R.Z., Lynch, K.L., Lee, K., 1992. Tissue response to biphasic calcium
phosphate ceramic with different ratios of HA/βTCP in periodontal osseous defects. J.
Periodontol. 63, 729735.
Neto, D.M.A., Carvalho, E.V., Rodrigues, E.A., Feitosa, V.P., Sauro, S., Mele, G., et al.,
2016. Novel hydroxyapatite nanorods improve anti-caries efficacy of enamel infiltrants.
Dent. Mater. 32, 784793.
Nevins, A.J., Cymerman, J.J., 2015. Revitalization of open apex teeth with apical periodontitis using a collagen-hydroxyapatite scaffold. J. Endod. 41, 966973.
Nevins, A.J., LaPorta, R.F., Borden, B.G., Spangberg, L.S., 1980. Pulpotomy and partial pulpectomy procedures in monkey teeth using cross-linked collagen-calcium phosphate gel.
Oral Surg. Oral Med. Oral Pathol. 49, 360365.
Ngoc, N.T.B., Mukohyama, H., Hlaing, S., Kondo, H., Inoue, T., Taniguchi, H., et al., 1997.
Prosthodontic treatment for patients with large mandibular defects; porous hydroxyapatite grafts. J. Med. Dent. Sci. 44, 9398.
Ngoc, T.N.D., Tra, T.N., Nguyen, T.H., Huynh, C.K., Van, T.V., 2018. Preparation and characterization of nano-sized biphasic calcium phosphate (BCP) for demineralized dentin
infiltration in hypersensitivity treatment. IFMBE Proc. 63, 677680.
Nicholson, J.W., Hawkins, S.J., Smith, J.E., 1993. The incorporation of hydroxyapatite into
glass-polyalkenoate (“glass-ionomer”) cements: a preliminary study. J. Mater. Sci.
Mater. Med. 4, 418421.
Ning, T.Y., Xu, X.H., Zhu, L.F., Zhu, X.P., Chu, C.H., Liu, L.K., et al., 2012. Biomimetic
mineralization of dentin induced by agarose gel loaded with calcium phosphate. J.
Biomed. Mater. Res. B: Appl. Biomater. 100, 138144.
Niu, L.N., Zhang, W., Pashley, D.H., Breschi, L., Mao, J., Chen, J.H., et al., 2014.
Biomimetic remineralization of dentin. Dent. Mater. 30, 7796.
Niwa, M., Sato, T., Li, W., Aoki, H., Aoki, H., Daisaku, T., 2001. Polishing and whitening
properties of toothpaste containing hydroxyapatite. J. Mater. Sci. Mater. Med. 12,
277281.
Niwa, K., Ogawa, K., Miyazawa, K., Aoki, T., Kawai, T., Goto, S., 2009. Application of
α-tricalcium phosphate coatings on titanium subperiosteal orthodontic implants reduces
the time for absolute anchorage: a study using rabbit femora. Dent. Mater. J. 28,
477486.
Noetzel, J., Özer, K., Reisshauer, B.H., Anil, A., Rössler, R., Neumann, K., et al., 2006.
Tissue responses to an experimental calcium phosphate cement and mineral trioxide
aggregate as materials for furcation perforation repair, a histological study in dogs. Clin.
Oral Investig. 10, 7783.
Nyman, S., Lindhe, J., Karring, T., Rylander, H., 1982. New attachment following surgical
treatment of human periodontal disease. J. Clin. Periodontol. 9, 290296.
O’Donnell, J.N.R., Schumacher, G.E., Antonucci, J.M., Skrtic, D., 2009. Adhesion of amorphous calcium phosphate composites bonded to dentin: a study in failure modality. J.
Biomed. Mater. Res. B: Appl. Biomater. 90B, 238249.
Calcium orthophosphates as a dental regenerative material
437
Oduncu, B.S., Yucel, S., Aydin, I., Sener, I.D., Yamaner, G., 2010. Polymerisation shrinkage
of light-cured hydroxyapatite (HA) reinforced dental composites. World Acad. Sci.
Eng. Technol. 40, 286291.
Ogawa, K., Miyaji, H., Kato, A., Kosen, Y., Momose, T., Yoshida, T., et al., 2016.
Periodontal tissue engineering by nano beta-tricalcium phosphate scaffold and fibroblast
growth factor-2 in one-wall infrabony defects of dogs. J. Periodont. Res. 51, 758767.
Ogiso, M., Tabata, T., Kuo, P.T., Borgese, D., 1994. A histologic comparison of the functional loading capacity of an occluded dense apatite implant and the natural dentition. J.
Prost. Dent. 71, 581588.
Ohara, T., Itaya, T., Usami, K., Ando, Y., Sakurai, H., Honda, M.J., et al., 2010. Evaluation
of scaffold materials for tooth tissue engineering. J. Biomed. Mater. Res. A 94A,
800805.
Okashi, T., Kani, T., Isozaki, A., Nishida, A., Shintani, H., Tokumoto, T., et al., 1991.
Remineralization of artificial caries lesions by hydroxyapatite. J. Dent. Health 41,
214223.
Okubo, N., Fujita, T., Ishii, Y., Ota, M., Shibukawa, Y., Yamada, S., 2013. Coverage of gingival recession defects using acellular dermal matrix allograft with or without betatricalcium phosphate. J. Biomater. Appl. 27, 627637.
Okuda, K., Tai, H., Tanabe, K., Suzuki, H., Sato, T., Kawase, T., et al., 2005. Platelet-rich
plasma combined with a porous hydroxyapatite graft for the treatment of intrabony periodontal defects in humans: a comparative controlled clinical study. J. Periodontol. 76,
890898.
Okuda, K., Yamamiya, K., Kawase, T., Mizuno, H., Ueda, M., Yoshie, H., 2009. Treatment
of human infrabony periodontal defects by grafting human cultured periosteum sheets
combined with platelet-rich plasma and porous hydroxyapatite granules: case series. J.
Int. Acad. Periodontol. 11, 206213.
Ong, J.L., Chan, D.C.N., 1999. Hydroxyapatite and their use as coatings in dental implants: a
review. Crit. Rev. Biomed. Eng. 28, 667707.
Onuma, K., Yamagishi, K., Oyane, A., 2005. Nucleation and growth of hydroxyapatite
nanocrystals for nondestructive repair of early caries lesions. J. Cryst. Growth 282,
199207.
Oshiro, M., Yamaguchi, K., Takamizawa, T., Inage, H., Watanabe, T., Irokawa, A., et al.,
2007. Effect of CPP-ACP paste on tooth mineralization: an FE-SEM study. J. Oral Sci.
49, 115120.
Owadally, I.D., Ford, T.R.P., 1994. Effect of addition of hydroxyapatite on the physical properties of IRM. Int. Endod. J. 27, 227232.
Owadally, I.D., Chong, B.S., Ford, T.R.P., Wilson, R.F., 1994. Biological properties of IRM
with the addition of hydroxyapatite as a retrograde root filling material. Endod. Dent.
Traumatol. 10, 228232.
Palarie, V., Bicer, C., Lehmann, K.M., Zahalka, M., Draenert, F.G., Kämmerer, P.W., 2012.
Early outcome of an implant system with a resorbable adhesive calcium-phosphate coating—a prospective clinical study in partially dentate patients. Clin. Oral Investig. 16,
10391048.
Panahi, F., Rabiee, S.M., Shidpour, R., 2017. Synergic effect of chitosan and dicalcium phosphate on tricalcium silicate-based nanocomposite for root-end dental application. Mater.
Sci. Eng. C 80, 631-641.
Pandit, N., Gupta, R., Gupta, S., 2010. A comparative evaluation of biphasic calcium phosphate material and bioglass in the treatment of periodontal osseous defects: a clinical
and radiological study. J. Contemp. Dent. Pract. 11, 2532.
438
Advanced Dental Biomaterials
Panich, M., Poolthong, S., 2009. The effect of casein phosphopeptide-amorphous calcium
phosphate and a cola soft drink on in vitro enamel hardness. J. Am. Dent. Assoc. 140,
455460.
Papas, A., 2008. Calcium phosphate mouth rinse for preventing oral mucositis. Community
Oncol. 5, 171172.
Park, S.Y., Cha, J.Y., Kim, K.N., Hwang, C.J., 2013. The effect of casein phosphopeptide
amorphous calcium phosphate on the in vitro shear bond strength of orthodontic brackets. Korean J. Orthod. 43, 2328.
Pendleton, L.W., 1873. The lacto-phosphate of lime. Trans. Maine Med. Assoc. 4, 313318.
Pepelassi, E.M., Bissada, N.F., Greenwell, H., Farah, C.F., 1991. Doxycycline-tricalcium
phosphate composite graft facilitates osseous healing in advanced periodontal furcation
defects. J. Periodontol. 62, 106115.
Pickel, F.D., Bilotti, A., 1965. The effects of a chewing gum containing dicalcium phosphate
on salivary calcium and phosphate. Alabama J. Med. Sci. 2, 286287.
Pietruska, M., Pietruski, J., Nagy, K., Brecx, M., Arweiler, N.B., Sculean, A., 2012a. Fouryear results following treatment of intrabony periodontal defects with an enamel matrix
derivative alone or combined with a biphasic calcium phosphate. Clin. Oral Investig. 16,
11911197.
Pietruska, M., Skurska, A., Pietruski, J., Dolińska, E., Arweiler, N., Milewski, R., et al.,
2012b. Clinical and radiographic evaluation of intrabony periodontal defect treatment by
open flap debridement alone or in combination with nanocrystalline hydroxyapatite
bone substitute. Ann. Anat. 194, 533537.
Porciani, P.F., Chazine, M., Grandini, S., 2014. A clinical study of the efficacy of a new
chewing gum containing calcium hydroxyapatite in reducing dentin hypersensitivity. J.
Clin. Dent. 25, 3236.
Portella, F.F., Collares, F.M., dos Santos, L.A., dos Santos, B.P., Camassola, M., Leitune,
V.C.B., et al., 2015. Glycerol salicylate-based containing α-tricalcium phosphate as a
bioactive root canal sealer. J. Biomed. Mater. Res. B: Appl. Biomater. 103B,
16631669.
Prabhakar, A.R., Sharma, D., Sugandhan, S., 2012. Comparative evaluation of the remineralising effects and surface microhardness of glass ionomer cement containing grape seed
extract and casein phosphopeptide amorphous calcium phosphate: an in vitro study.
Eur. Arch. Paediatr. Dent. 13, 138143.
Pradeep, A.R., Bajaj, P., Rao, N.S., Agarwal, E., Naik, S.B., 2017. Platelet-rich fibrin combined with a porous hydroxyapatite graft for the treatment of 3-wall intrabony defects in
chronic periodontitis: a randomized controlled clinical trial. J. Periodontol. 88,
12881296.
Quinn, B., 2013. Efficacy of a supersaturated calcium phosphate oral rinse for the prevention
and treatment of oral mucositis in patients receiving high-dose cancer therapy: a review
of current data. Eur. J. Cancer Care 22, 564579.
Ramalingam, L., Messer, L.B., Reynolds, E.C., 2005. Adding casein phosphopeptideamorphous calcium phosphate to sports drinks to eliminate in vitro erosion. Pediatr.
Dent. 27, 6167.
Ranjitkar, S., Rodriguez, J.M., Kaidonis, J.A., Richards, L.C., Townsend, G.C., Bartlett, D.
W., 2009a. The effect of casein phosphopeptide-amorphous calcium phosphate on erosive enamel and dentine wear by toothbrush abrasion. J. Dent. 37, 250254.
Ranjitkar, S., Narayana, T., Kaidonis, J.A., Hughes, T.E., Richards, L.C., Townsend, G.C.,
2009b. The effect of casein phosphopeptide-amorphous calcium phosphate on erosive
dentine wear. Aust. Dent. J. 54, 101107.
Calcium orthophosphates as a dental regenerative material
439
Reddi, S.P., Stevens, M.R., Kline, S.N., Villanueva, P., 1999. Hydroxyapatite cement in craniofacial trauma surgery, indications and early experience. J. Cran. Maxillofac. Trauma
5, 712.
Redondo, L.M., Garcı́a Cantera, J.M., Hernández, A.V., Puerta, C.V., 1995. Effect of particulate porous hydroxyapatite on osteoinduction of demineralized bone autografts in experimental reconstruction of the rat mandible. Int. J. Oral Maxillofac. Surg. 24, 445448.
Reema, S.D., Lahiri, P.K., Roy, S.S., 2014. Review of casein phosphopeptides-amorphous
calcium phosphate. Chin. J. Dent. Res. 17, 714.
Reis, E.C.C., Borges, A.P.B., Araújo, M.V.F., Mendes, V.C., Guan, L., Davies, J.E., 2011.
Periodontal regeneration using a bilayered PLGA/calcium phosphate construct.
Biomaterials 32, 92449253.
Reynolds, E.C., 1997. Remineralization of enamel subsurface lesions by casein
phosphopeptide-stabilized calcium phosphate solutions. J. Dent. Res. 76, 15871595.
Reynolds, E.C., 1998. Anticariogenic complexes of amorphous calcium phosphate stabilized
by casein phosphopeptides: a review. Spec. Care Dent. 18, 816.
Reynolds, E.C., 2008. Calcium phosphate-based remineralization systems: scientific evidence? Aust. Dent. J. 53, 268273.
Reynolds, E.C., Cai, F., Cochrane, N.J., Shen, P., Walker, G.D., Morgan, M.V., et al., 2008.
Fluoride and casein phosphopeptide-amorphous calcium phosphate. J. Dent. Res. 87,
344348.
Rezvani, M., Atai, M., Rouhollahi, H., Malekhoseini, K., Rezai, H., Hamze, F., 2015. Effect
of nano-tricalcium phosphate and nanohydroxyapatite on staining susceptibility of
bleached enamel. Int. Sch. Res. Notices 2015, 935264 (7 pp.).
Richardson, A.S., Hole, L.W., McCombie, F., Kolthammer, J., 1972. Anticariogenic effect of
dicalcium phosphate dihydrate chewing gum: results after two years. J. Can. Dent.
Assoc. 38, 213218.
Ridgway, H.K., Mellonig, J.T., Cochran, D.L., 2008. Human histologic and clinical evaluation of recombinant human platelet-derived growth factor and beta-tricalcium phosphate
for the treatment of periodontal intraosseous defects. Int. J. Periodontics Restorative
Dent. 28, 171179.
Rimondini, L., Palazzo, B., Iafisco, M., Canegallo, L., Demarosi, F., Merlo, M., et al., 2007.
The remineralizing effect of carbonate-hydroxyapatite nanocrystals on dentine. Mater.
Sci. Forum 539543, 602605.
Roane, J.B., Benenati, F.W., 1987. Successful management of a perforated mandibular molar
using amalgam and hydroxyapatite. J. Endod. 13, 400404.
Rosen, H.M., Ackerman, J.L., 1991. Porous block hydroxyapatite in orthognathic surgery.
Angle Orthod. 61, 185191. discussion 192.
Roveri, N., Battistella, E., Foltran, I., Foresti, E., Iafisco, M., Lelli, M., et al., 2008. Synthetic
biomimetic carbonate-hydroxyapatite nanocrystals for enamel remineralization. Adv.
Mater. Res. 4750, 821824.
Roveri, N., Foresti, E., Lelli, M., Lesci, I.G., 2009a. Recent advancements in preventing teeth
health hazard: the daily use of hydroxyapatite instead of fluoride. Rec. Pat. Biomed.
Eng. 2, 197215.
Roveri, N., Battistella, E., Bianchi, C.L., Foltran, I., Foresti, E., Iafisco, M., et al., 2009b.
Surface enamel remineralization: biomimetic apatite nanocrystals and fluoride ions different effects. J. Nanomater. 2009, 746383 (9 pp.).
Saffar, J.L., Colombier, M.L., Detienville, R., 1990. Bone formation in tricalcium phosphatefilled periodontal intrabony lesions. Histological observations in humans. J. Periodontol.
61, 209216.
440
Advanced Dental Biomaterials
Saito, E., Saito, A., Kuboki, Y., Kimura, M., Honma, Y., Takahashi, T., et al., 2012.
Periodontal repair following implantation of beta-tricalcium phosphate with different
pore structures in class III furcation defects in dogs. Dent. Mater. J. 31, 681688.
Saito, A., Saito, E., Ueda, Y., Shibukawa, Y., Honma, Y., Takahashi, T., et al., 2014. Effect
of tunnel structure of β-TCP on periodontal repair in class III furcation defects in dogs.
Bioceram. Dev. Appl 4, 073.
Salyer, K.E., Hall, C.D., 1989. Porous hydroxyapatite as an onlay bone-graft substitute for
maxillofacial surgery. Plast. Reconstr. Surg. 84, 236244.
Sanada, Y., Fujinaka, T., Yoshimine, T., Kato, A., 2011. Optimal reconstruction of the bony
defect after frontotemporal craniotomy with hydroxyapatite cement. J. Clin. Neurosci.
18, 280282.
Sato, I., Akizuki, T., Oda, S., Tsuchioka, H., Hayashi, C., Takasaki, A.A., et al., 2009.
Histological evaluation of alveolar ridge augmentation using injectable calcium phosphate bone cement in dogs. J. Oral Rehabil 36, 762769.
Scarano, A., Degidi, M., Perrotti, V., Piattelli, A., Iezzi, G., 2012. Sinus augmentation with
phycogene hydroxyapatite: histological and histomorphometrical results after 6 months
in humans. A case series. Oral Maxillofac. Surg. 16, 4145.
Schemehorn, B.R., Orban, J.C., Wood, G.D., Fischer, G.M., Winston, A.E., 1999.
Remineralization by fluoride enhanced with calcium and phosphate ingredients. J. Clin.
Dent. 10, 1316.
Schlafer, S., Birkedal, H., Olsen, J., Skovgaard, J., Sutherland, D.S., Wejse, P.L., et al.,
2016. Calcium-phosphate-osteopontin particles for caries control. Biofouling 32,
349357.
Schliephake, H., Scharnweber, D., Roesseler, S., Dard, M., Sewing, A., Aref, A., 2006.
Biomimetic calcium phosphate composite coating of dental implants. Int. J. Oral
Maxillofac. Implants 21, 738746.
Schneider, B., Diedrich, P., 1989. Interaktion von kieferorthopadischer Zahnbewegung und
Hydroxylapatit-Keramik. [Interaction between orthodontic tooth movement and
hydroxyapatite ceramics]. Dtsch. Zahnarztl. Z 44, 282285.
Schreiber, C.T., Shern, R.J., Chow, L.C., Kingman, A., 1988. Effects of rinses with an acidic
calcium phosphate solution on fluoride uptake, caries, and in situ plaque pH in rats. J.
Dent. Res. 67, 959963.
Sculean, A., Windisch, P., Szendröi-Kiss, D., Horváth, A., Rosta, P., Becker, J., et al., 2008.
Clinical and histologic evaluation of an enamel matrix derivative combined with a
biphasic calcium phosphate for the treatment of human intrabony periodontal defects. J.
Periodontol. 79, 19911999.
Seifi, M., Arayesh, A., Shamloo, N., Hamedi, R., 2015. Effect of nanocrystalline hydroxyapatite socket preservation on orthodontically induced inflammatory root resorption. Cell J.
16, 514527.
Sena, M., Yamashita, Y., Nakano, Y., Ohgaki, M., Nakamura, S., Yamashita, K., et al., 2004.
Octacalcium phosphate-based cement as a pulp-capping agent in rats. Oral Surg. Oral
Med. Oral Pathol. Oral Radiol. Endod. 97, 749-755.
Seong, K.C., Cho, K.S., Daculsi, C., Seris, E., Daculsi, G., 2014. Eight-year clinical followup of sinus grafts with micro-macroporous biphasic calcium phosphate granules. Key
Eng. Mater. 587, 321324.
Sepantafar, M., Mohammadi, H., Maheronnaghsh, R., Tayebi, L., Baharvand, H., 2018.
Single phased silicate-containing calcium phosphate bioceramics: promising biomaterials for periodontal repair. Ceram. Int. (early view).
Calcium orthophosphates as a dental regenerative material
441
Shammukha, G., Santhosh, B.P., Preeti, J., Naveen, B., Inderjith, G., Santhosh, B., et al.,
2012. Evaluation of changes in salivary concentration of calcium by CPP-ACP containing chewing gum a clinical trial. Int. J. Adv. Res. Oral Sci. 1, 17.
Sharma, H., Gupta, C., Thakur, S., Srivastava, S., 2017. Comparative evaluation of calcium
phosphate-based varnish and resin-modified glass ionomer-based varnish in reducing dentinal hypersensitivity: a randomized controlled clinical trial. Eur. J. Dent. 11, 491495.
Shayegan, A., Petein, M., Abbeele, A.V., 2008. Beta-tricalcium phosphate, white mineral trioxide aggregate, white Portland cement, ferric sulfate, and formocresol used as pulpotomy agents in primary pig teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod.
105, 536542.
Shayegan, A., Atash, R., Petein, M., Abbeele, A.V., 2010. Nanohydroxyapatite used as a pulpotomy and direct pulp capping agent in primary pig teeth. J. Dent. Child. (Chic.) 77,
7783.
Shayesteh, Y.S., Khojasteh, A., Soleimani, M., Alikhasi, M., Khoshzaban, A., Ahmadbeigi,
N., 2008. Sinus augmentation using human mesenchymal stem cells loaded into a
β-tricalcium phosphate/hydroxyapatite scaffold. Oral Surg. Oral Med. Oral Pathol. Oral
Radiol. Endod. 106, 203209.
Shen, P., Cai, F., Nowicki, A., Vincent, J., Reynolds, E.C., 2001. Remineralization of enamel
subsurface lesions by sugar-free chewing gum containing casein phosphopeptideamorphous calcium phosphate. J. Dent. Res. 80, 20662070.
Shen, Q., Sun, J., Wu, J., Liu, C., Chen, F., 2010. An in vitro investigation of the
mechanical-chemical and biological properties of calcium phosphate/calcium silicate/
bismutite cement for dental pulp capping. J. Biomed. Mater. Res. B: Appl. Biomater.
94B, 141148.
Shern, R.J., Couet, K.M., Chow, L.C., Brown, W.E., 1979. Effects of sequential calcium
phosphate-fluoride rinses on fluoride uptake in rats. J. Dent. Res. 58 (Spec. Iss. B),
1023.
Shern, R.J., Chow, L.C., Couet, K.M., Kingman, A., Brown, W.E., 1984. Effects of sequential calcium phosphate-fluoride rinses on dental plaque, staining, fluoride uptake, and
caries in rats. J. Dent. Res. 63, 13551359.
Shetty, S., Kohad, R., Yeltiwar, R., 2010. Hydroxyapatite as an in-office agent for tooth
hypersensitivity: a clinical and scanning electron microscopic study. J. Periodontol. 81,
17811789.
Shetty, R., Bhat, A.N., Mehta, D., Finger, W.J., 2017. Effect of a calcium phosphate desensitizer on pre- and postcementation sensitivity of teeth prepared for full-coverage restorations: a randomized, placebo-controlled clinical study. Int. J. Prosthodont. 30, 3842.
Shi, H., Ma, J., Zhao, N., Chen, Y., Liao, Y., 2008. Periodontal regeneration in
experimentally-induced alveolar bone dehiscence by an improved porous biphasic calcium phosphate ceramic in beagle dogs. J. Mater. Sci. Mater. Med. 19, 35153524.
Shieh, T.M., Hsu, S.M., Chang, K.C., Chen, W.C., Lin, D.J., 2017. Calcium phosphate
cement with antimicrobial properties and radiopacity as an endodontic material.
Materials 10, 1256.
Shirai, Y., Okuda, K., Kubota, T., Wolff, L.F., Yoshie, H., 2012. The comparative effectiveness of granules or blocks of superporous hydroxyapatite for the treatment of intrabony
periodontal defects. Open J. Stomatol. 2, 8187.
Shirakata, Y., Oda, S., Kinoshita, A., Kikuchi, S., Tsuchioka, H., Ishikawa, I., 2002.
Histocompatible healing of periodontal defects after application of injectable calcium
phosphate bone cement. A preliminary study in dogs. J. Periodontol. 73, 10431053.
442
Advanced Dental Biomaterials
Shirakata, Y., Setoguchi, T., Machigashira, M., Matsuyama, T., Furuichi, Y., Hasegawa, K.,
et al., 2008. Comparison of injectable calcium phosphate bone cement grafting and open
flap debridement in periodontal intrabony defects: a randomized clinical trial. J.
Periodontol. 79, 2532.
Shirakata, Y., Taniyama, K., Yoshimoto, T., Takeuchi, N., Noguchi, K., 2012. Effect of bone
swaging with calcium phosphate bone cement on periodontal regeneration in dogs. Oral
Surg. Oral Med. Oral Pathol. Oral Radiol. 114, 3542.
Shirakawa, M., Nomura, T., Itoh, T., Sakai, N., Shizume, M., 1988. Clinical application of
hydroxyapatite ceramics APS-7 in the field of oral surgery. Shigaku 76, 782815.
Shon, W.J., Bae, K.S., Baek, S.H., Kum, K.Y., Han, A.R., Lee, W.C., 2012. Effects of calcium phosphate endodontic sealers on the behavior of human periodontal ligament fibroblasts and MG63 osteoblast-like cells. J. Biomed. Mater. Res. B: Appl. Biomater. 100B,
21412147.
Shyam, R., Manjunath, B.C., Kumar, A., Narang, R., Ghanghas, M., Rani, G., 2017. Role of
casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) in prevention of dental caries: a review. Int. J. Adv. Res. 5, 9991004.
Silva, M.F.D.A., Melo, E.V.D.S., Stewart, B., de Vizio, W., Sintes, J.L., Petrone, M.E., et al.,
2001. The enhanced anticaries efficacy of a sodium fluoride and dicalcium phosphate
dihydrate dentifrice in a dual-chambered tube. A 2-year caries clinical study on children
in Brazil. Am. J. Dent. 14 (Spec. Iss. 5), 19A23A.
Silva, K.G., Pedrini, D., Delbem, A.C.B., Ferreira, L., Cannon, M., 2010. In situ evaluation
of the remineralizing capacity of pit and fissure sealants containing amorphous calcium
phosphate and/or fluoride. Acta Odontol. Scand. 68, 1118.
Silverstone, L.M., 1972. Remineralization of human enamel in vitro. Proc. R. Soc. Med. 65,
906908.
Silverstone, L.M., Johnson, N.W., 1971. The effect on sound human enamel of exposure to
calcifying fluids in vitro. Caries Res. 5, 323342.
Sinai, I.H., Romea, D.J., Glassman, G., Morse, D.R., Fantasia, J., Furst, M.L., 1989. An evaluation of tricalcium phosphate as a treatment for endodontic perforations. J. Endod. 15,
399403.
Singh, M.L., Papas, A.S., 2009. Long-term clinical observation of dental caries in salivary
hypofunction patients using a supersaturated calcium-phosphate remmeralizing rinse. J.
Clin. Dent. 20, 8792.
Singh, K.A., Burstein, F.D., Williams, J.K., 2010. Use of hydroxyapatite cement in pediatric
craniofacial reconstructive surgery: strategies for avoiding complications. J. Craniofac.
Surg. 21, 11301135.
Sintes, J.L., Elı́as-Boneta, A., Stewart, B., Volpe, A.R., Lovett, J., 2002. Anticaries efficacy
of a sodium monofluorophosphate dentifrice containing xylitol in a dicalcium phosphate
dihydrate base. A 30-month caries clinical study in Costa Rica. Am. J. Dent. 15,
215219.
Skrtic, D., Antonucci, J.M., 2005. Matrix resin effects on selected physicochemical properties
of amorphous calcium phosphate composites. J. Bioact. Compat. Polym. 20, 2949.
Skrtic, D., Antonucci, J.M., 2007. Dental composites based on amorphous calcium
phosphate resin composition/physicochemical properties study. J. Biomater. Appl.
21, 375393.
Skrtic, D., Antonucci, J.M., 2011. Bioactive polymeric composites for tooth mineral regeneration: physicochemical and cellular aspects. J. Funct. Biomater. 2, 271307.
Skrtic, D., Antonucci, J.M., 2016. Polymeric dental composites based on remineralizing
amorphous calcium phosphate fillers. Curr. Trends Polym. Sci. 17, 131.
Calcium orthophosphates as a dental regenerative material
443
Skrtic, D., Antonucci, J.M., Eanes, E.D., 1996a. Improved properties of amorphous calcium
phosphate fillers in remineralizing resin composites. Dent. Mater. 12, 295301.
Skrtic, D., Hailer, A.W., Takagi, S., Antonucci, J.M., Eanes, E.D., 1996b. Quantitative
assessment of the efficacy of amorphous calcium phosphate/methacrylate composites in
remineralizing caries-like lesions artificially produced in bovine enamel. J. Dent. Res.
75, 16791686.
Skrtic, D., Antonucci, J.M., Eanes, E.D., 2001. Effect of the monomer and filler system on
the remineralizing potential of bioactive dental composites based on amorphous calcium
phosphate. Polym. Adv. Technol. 12, 369379.
Skrtic, D., Antonucci, J.M., Eanes, E.D., 2003. Amorphous calcium phosphate-based bioactive polymeric composites for mineralized tissue regeneration. J. Res. Natl. Inst. Stand.
Technol. 108, 167182.
Skrtic, D., Antonucci, J.M., Eanes, E.D., Eidelman, N., 2004. Dental composites based on
hybrid and surface-modified amorphous calcium phosphates. Biomaterials 25,
11411150.
Smartt, J.M., Karmacharya, J., Gannon, F.H., Ong, G., Jackson, O., Bartlett, S.P., et al.,
2005. Repair of the immature and mature craniofacial skeleton with a carbonated calcium phosphate cement: assessment of biocompatibility, osteoconductivity and remodeling capacity. Plast. Reconstr. Surg. 115, 16421650.
Sodagar, A., Akhavan, A., Hashemi, E., Arab, S., Pourhajibagher, M., Sodagar, K., et al.,
2016. Evaluation of the antibacterial activity of a conventional orthodontic composite
containing silver/hydroxyapatite nanoparticles. Prog. Orthod. 17, 40.
Sorensen, R.G., Wikesjö, U.M.E., Kinoshita, A., Wozney, J.M., 2004. Periodontal repair in
dogs: Evaluation of a bioresorbable calcium phosphate cement (Ceredext) as a carrier
for rhBMP-2. J. Clin. Periodontol. 31, 796804.
Souza, B.M., Comar, L.P., Vertuan, M., Neto, C.F., Buzalaf, M.A., Magalhães, A.C., 2015.
Effect of an experimental paste with hydroxyapatite nanoparticles and fluoride on dental
demineralisation and remineralisation in situ. Caries Res. 49, 499507.
Stahl, S.S., Froum, S.J., 1987. Histologic and clinical responses to porous hydroxylapatite
implants in human periodontal defects. Three to twelve months postimplantation. J.
Periodontol. 58, 689695.
Stavropoulos, A., Windisch, P., Szendröi-Kiss, D., Peter, R., Gera, I., Sculean, A., 2010. Clinical
and histologic evaluation of granular beta-tricalcium phosphate for the treatment of human
intrabony periodontal defects: a report on five cases. J. Periodontol. 81, 325334.
Stefanic, M., Krnel, K., Pribosic, I., Kosmac, T., 2012. Rapid biomimetic deposition of octacalcium phosphate coatings on zirconia ceramics (Y-TZP) for dental implant applications. Appl. Surf. Sci. 258, 46494656.
Strub, J.R., Gaberthüel, T.W., 1978. Trikalziumphosphat und dessen biologisch abbaubare
Keramik in der parodontalen Knochenchirurgie Eine Literaturubersicht. [Tricalcium
phosphate and its biodegradable ceramics in periodontal bone surgery. A review of the
literature]. SSO Schweiz Monatsschr. Zahnheilkd. 88, 798803.
Struillou, X., Boutigny, H., Badran, Z., Fellah, B.H., Gauthier, O., Sourice, S., et al., 2011.
Treatment of periodontal defects in dogs using an injectable composite hydrogel/
biphasic calcium phosphate. J. Mater. Sci. Mater. Med. 22, 17071717.
Su, B., Su, J., Ran, J., Su, B., 2008. Biological performance of dental biphasic calcium phosphate ceramics modified by cold plasma. Key Eng. Mater. 368372, 12641267.
Sugawara, A., Chow, L.C., Takagi, S., Nishiyama, M., Ohashi, M., 1989. An in vitro study
of dentin hypersensitivity using calcium phosphate cement. Shika Zairyo Kikai 8,
282294.
444
Advanced Dental Biomaterials
Sugawara, A., Chow, L.C., Takagi, S., Chohayeb, H., 1990. In vitro evaluation of the sealing
ability of a calcium phosphate cement when used as a root canal sealer-filler. J. Endod.
16, 162165.
Sugawara, A., Fujikawa, K., Kusama, K., Nishiyama, M., Murai, S., Takagi, S., et al., 2002.
Histopathologic reaction of calcium phosphate cement for alveolar ridge augmentation.
J. Biomed. Mater. Res. 61, 4752.
Sugawara, A., Fujikawa, K., Takagi, S., Chow, L.C., 2008. Histological analysis of calcium
phosphate bone grafts for surgically created periodontal bone defects in dogs. Dent.
Mater. J. 27, 787-794.
Suge, T., Ishikawa, K., Kawasaki, A., Suzuki, K., Matsuo, T., Noiri, Y., et al., 2002. Calcium
phosphate precipitation method for the treatment of dentin hypersensitivity. Am. J.
Dent. 15, 220226.
Sullivan, R.J., Charig, A., Blake-Haskins, J., Zhang, Y.P., Miller, S.M., Strannick, M., et al.,
1997. In vivo detection of calcium from dicalcium phosphate dihydrate dentifrices in
demineralized human enamel and plaque. Adv. Dent. Res. 11, 380387.
Sullivan, R.J., Masters, J., Cantore, R., Roberson, A., Petrou, I., Stranick, M., et al., 2001.
Development of an enhanced anticaries efficacy dual component dentifrice containing sodium
fluoride and dicalcium phosphate dihydrate. Am. J. Dent. 14 (Spec. Iss. 5), 3A11A.
Sultan, S., Chaitra, T.R., Chaudhary, S., Manuja, N., Kaur, H., Amit, S.A., et al., 2016.
Effect of ACP-CPP chewing gum and natural chewable products on plaque pH: calcium
and phosphate concentration. J. Clin. Diagn. Res. 10, ZC13ZC17.
Sun, W., Zhang, F., Guo, J., Wu, J., Wu, W., 2008. Effects of amorphous calcium phosphate
on periodontal ligament cell adhesion and proliferation in vitro. J. Med. Biol. Eng. 28,
107112.
Sun, Y., Li, X., Deng, Y., Sun, J.N., Tao, D., Chen, H., et al., 2014. Mode of action studies
on the formation of enamel minerals from a novel toothpaste containing calcium silicate
and sodium phosphate salts. J. Dent. 42 (Suppl. 1), S30S38.
Sung, Y.M., Shin, Y.K., Ryu, J.J., 2007. Preparation of hydroxyapatite/zirconia bioceramic
nanocomposites for orthopaedic and dental prosthesis applications. Nanotechnology 18,
065602.
Svanberg, A., Ohrn, K., Birgegard, G., 2015. Caphosols mouthwash gives no additional protection against oral mucositis compared to cryotherapy alone in stem cell transplantation. A pilot study. Eur. J. Oncol. Nurs. 19, 5053.
Sverzut, A.T., Rodrigues, D.C., Lauria, A., Armando, R.S., de Oliveira, P.T., Moreira, R.W.F.,
2015. Clinical, radiographic, and histological analyses of calcium phosphate cement as
filling material in maxillary sinus lift surgery. Clin. Oral Implant. Res. 26, 633638.
Tabrizi, A., Cakirer, B., 2011. A comparative evaluation of casein phosphopeptideamorphous calcium phosphate and fluoride on the shear bond strength of orthodontic
brackets. Eur. J. Orthod. 33, 282287.
Tamimi, F., Torres, J., Cabarcos, E.L., Bassett, D.C., Habibovic, P., Luceron, E., et al., 2009.
Minimally invasive maxillofacial vertical bone augmentation using brushite based
cements. Biomaterials 30, 208216.
Tanaka, O., Hirai, T., Murase, H., 1988. Prosthodontic analysis in mandibular ridge augmentation with hydroxyapatite particle. Part I. Evaluation of alveolar ridge form. Nippon
Hotetsu Shika Gakkai Zasshi 32, 13451357.
Tanaka, O., Hirai, T., Murase, H., 1989. Prosthodontic analysis in mandibular ridge augmentation with hydroxyapatite particle. 2. Evaluation of masticatory function and overall
assessment. Nippon Hotetsu Shika Gakkai Zasshi 33, 14661476.
Calcium orthophosphates as a dental regenerative material
445
ten Cate, J.M., Arends, J., 1977. Remineralization of artificial enamel lesions in vitro. Caries
Res 11, 277286.
ten Cate, J.M., Arends, J., 1978. Remineralization of artificial enamel lesions in vitro. II.
Determination of activation energy and reaction order. Caries Res. 12, 213222.
ten Cate, J.M., Arends, J., 1980. Remineralization of artificial enamel lesions in vitro. III. A
study of the deposition mechanism. Caries Res. 14, 351358.
ten Cate, J.M., Jongebloed, W.L., Arends, J., 1981. Remineralization of artificial enamel
lesions in vitro. IV. Influence of fluorides and diphosphonates on short- and long-term
remineralization. Caries Res. 15, 6069.
Teodorović, N., Martinović, Ž., 2005. Significance of crown-down root canal preparation
technique in endodontic therapy by using the hydroxylapatite sealer. Vojnosanit. Pregl.
62, 447452.
Thaweboon, S., Nakornchai, S., Miyake, Y., Yanagisawa, T., Thaweboon, B., Sooampon, S.,
et al., 2009. Remineralization of enamel subsurface lesions by xylitol chewing gum containing funoran and calcium hydrogenphosphate. Southeast Asian J. Trop. Med. Public
Health 40, 345353.
Thein-Han, W., Liu, J., Xu, H.H.K., 2012. Calcium phosphate cement with biofunctional
agents and stem cell seeding for dental and craniofacial bone repair. Dent. Mater. 28,
10591070.
Thompson, J.Y., Stoner, B.R., Piascik, J.R., 2007. Ceramics for restorative dentistry: critical
aspects for fracture and fatigue resistance. Mater. Sci. Eng. C 27, 565569.
Tian, K., Peng, M., Wu, P., Liao, C.H., Huang, F.Y., 2012. Biomineralization of the hydroxyapatite with 3D-structure for enamel reconstruction. Adv. Mater. Res. 391392,
633637.
Tinsley, D., Watson, C.J., Russell, J.L., 2001. A comparison of hydroxylapatite coated
implant retained fixed and removable mandibular prostheses over 4 to 6 years. Clin.
Oral Implant. Res. 12, 159166.
Tiwari, S., Nandlal, B., 2012. Role of Synthetic Hydroxyapatite in Dentistry. Lap Lambert
Academic Publishing, Saarbrucken, Deutschland, 90 pp.
Tomizuka, K., 1990. Experimental study on apatite ceramics used as endodontic endosseous
implant. Kokubyo Gakkai Zasshi 57, 201226.
Tonomura, A., Mizuno, D., Hisada, A., Kuno, N., Ando, Y., Sumita, Y., et al., 2010.
Differential effect of scaffold shape on dentin regeneration. Ann. Biomed. Eng. 38,
16641671.
Trombelli, L., Simonelli, A., Pramstraller, M., Wikesjö, U.M.E., Farina, R., 2010. Single
flap approach with and without guided tissue regeneration and a hydroxyapatite biomaterial in the management of intraosseous periodontal defects. J. Periodontol. 81,
12561263.
Tschoppe, P., Zandim, D.L., Martus, P., Kielbassa, A.M., 2011. Enamel and dentine remineralization by nano-hydroxyapatite toothpastes. J. Dent. 39, 430437.
Tung, M.S., Eichmiller, F.C., 1999. Dental applications of amorphous calcium phosphates. J.
Clin. Dent. 10, 16.
Uysal, T., Amasyali, M., Koyuturk, A.E., Sagdic, D., 2009a. Efficiency of amorphous calcium phosphate-containing orthodontic composite and resin modified glass ionomer on
demineralization evaluated by a new laser fluorescence device. Eur. J. Dent. 3,
127134.
Uysal, T., Ulker, M., Baysal, A., Usumez, S., 2009b. Microleakage between composite-wire
and composite-enamel interfaces of flexible spiral wire retainers. Part 2: Comparison of
446
Advanced Dental Biomaterials
amorphous calcium phosphate-containing adhesive with conventional lingual retainer
composite. Eur. J. Orthod. 31, 652657.
Uysal, T., Ulker, M., Akdogan, G., Ramoglu, S.I., Yilmaz, E., 2009c. Bond strength of amorphous calcium phosphate-containing orthodontic composite used as a lingual retainer
adhesive. Angle Orthod. 79, 117121.
Uysal, T., Ustdal, A., Nur, M., Catalbas, B., 2010a. Bond strength of ceramic brackets
bonded to enamel with amorphous calcium phosphate-containing orthodontic composite.
Eur. J. Orthod. 32, 281284.
Uysal, T., Amasyali, M., Ozcan, S., Koyuturk, A.E., Akyol, M., Sagdic, D., 2010b. In vivo
effects of amorphous calcium phosphate-containing orthodontic composite on enamel
demineralization around orthodontic brackets. Aust. Dent. J. 55, 285291.
Uysal, T., Amasyali, M., Koyuturk, A.E., Ozcan, S., Sagdic, D., 2010c. Amorphous calcium
phosphate-containing orthodontic composites. Do they prevent demineralisation around
orthodontic brackets? Aust. Orthod. J 26, 1015.
Uysal, T., Baysal, A., Uysal, B., Aydinbelge, M., Al-Qunaian, T., 2011. Do fluoride and
casein phosphopeptide-amorphous calcium phosphate affect shear bond strength of
orthodontic brackets bonded to a demineralized enamel surface? Angle Orthod. 81,
490495.
Vaca-Cornejo, F., Reyes, H.M., Jiménez, S.H.D., Velázquez, R.A.L., Jiménez, J.M.D., 2017.
Pilot study using a chitosan-hydroxyapatite implant for guided alveolar bone growth in
patients with chronic periodontitis. J. Funct. Biomater. 8, 29.
Vaishnavi, C., Mohan, B., Narayanan, L.L., 2011. Treatment of endodontically induced periapical lesions using hydroxyapatite, platelet-rich plasma, and a combination of both: an
in vivo study. J. Conserv. Dent. 14, 140146.
Vanichvatana, S., Auychai, P., 2013. Efficacy of two calcium phosphate pastes on the remineralization of artificial caries: a randomized controlled double-blind in situ study. Int.
J. Oral Sci. 5, 224228.
Vano, M., Derchi, G., Barone, A., Pinna, R., Usai, P., Covani, U., 2018. Reducing dentine
hypersensitivity with nano-hydroxyapatite toothpaste: a double-blind randomized controlled trial. Clin. Oral. Investig. 22, 313320.
van Oirschot, B.A.J.A., Bronkhorst, E.M., van den Beucken, J.J.J.P., Meijer, G.J., Jansen, J.
A., Junker, R., 2016a. A systematic review on the long-term success of calcium phosphate plasma-spray-coated dental implants. Odontology 104, 347356.
van Oirschot, B.A.J.A., Bronkhorst, E.M., van den Beucken, J.J.J.P., Meijer, G.J., Jansen, J.
A., Junker, R., 2016b. A systematic review on the long-term success of calcium phosphate plasma-spray-coated dental implants. Odontology 104, 347356.
Vargas, S., Estevez, M., Hernandez, A., Laiz, J.C., Brostow, W., Lobland, H.E.H., et al.,
2013. Hydroxyapatite based hybrid dental materials with controlled porosity and
improved tribological and mechanical properties. Mater. Res. Innov. 17, 154160.
Viale-Bouroncle, S., Bey, B., Reichert, T.E., Schmalz, G., Morsczeck, C., 2011.
β-Tricalcium-phosphate stimulates the differentiation of dental follicle cells. J. Mater.
Sci. Mater. Med. 22, 17191724.
Vogel, G.L., Zhang, Z., Carey, C.M., Ly, A., Chow, L.C., Proskin, H.M., 1998. Composition
of plaque and saliva following a sucrose challenge and use of an α-tricalcium-phosphate-containing chewing gum. J. Dent. Res. 77, 518524. erratum: p. 1575.
Vogel, G.L., Zhang, Z., Carey, C.M., Ly, A., Chow, L.C., Proskin, H.M., 2000. Composition
of plaque and saliva following use of an α-tricalcium-phosphate-containing chewing
gum and a subsequent sucrose challenge. J. Dent. Res. 79, 5862.
Calcium orthophosphates as a dental regenerative material
447
Vyavhare, S., Sharma, D.S., Kulkarni, V.K., 2015. Effect of three different pastes on remineralization of initial enamel lesion: an in vitro study. J. Clin. Pediatr. Dent. 39,
149160.
Wagner, W., Wiltfang, J., Pistner, H., Yildirim, M., Ploder, B., Chapman, M., et al., 2012. Bone
formation with a biphasic calcium phosphate combined with fibrin sealant in maxillary sinus
floor elevation for delayed dental implant. Clin. Oral Implants Res. 23, 11121117.
Walker, G.D., Cai, F., Shen, P., Reynolds, C., Ward, B., Fone, C., et al., 2006. Increased
remineralization of tooth enamel by milk containing added casein phosphopeptideamorphous calcium phosphate. J. Dairy Res. 73, 7478.
Walker, G.D., Cai, F., Shen, P., Bailey, D.L., Yuan, Y., Cochrane, N.J., et al., 2009.
Consumption of milk with added casein phosphopeptide-amorphous calcium phosphate
remineralizes enamel subsurface lesions in situ. Aust. Dent. J. 54, 245249.
Walker, G.D., Cai, F., Shen, P., Adams, G.G., Reynolds, C., Reynolds, E.C., 2010. Casein
phosphopeptide-amorphous calcium phosphate incorporated into sugar confections inhibits the progression of enamel subsurface lesions in situ. Caries Res. 44, 3340.
Wang, Y., Wang, Q.S., 2010. Application of nano-hydroxyapatite and its composite biomaterials in stomatology. J. Clin. Rehabil. Tissue Eng. Res. 14, 14261428.
Wang, J.P., Geogi, G., 2014. Antimicrobial and sealant properties of nanohydroxyapatite as
endodontic sealer. Chin. J. Tissue Eng. Res. 18, 33503354.
Wang, W., Zeng, X.L., Liu, W., 2008. Dental caries in ancient Chinese in Xia dynasty.
Zhonghua Kou Qiang Yi Xue Za Zhi 43, 308310 (in Chinese).
Wang, C.J., Zhang, Y.F., Wei, J., Wei, S.C., 2011a. Repair of artificial enamel lesions by
nano fluorapatite paste containing fluorin. J. Clin. Rehabil. Tissue Eng. Res. 15,
63466350.
Wang, H.Y., Sun, K.N., Shan, T., Yang, X.Q., Zhao, Y., Liang, Y.J., 2011b. Biomimetic synthesis of fluorapatite coating. Adv. Mater. Res. 306307, 6371.
Wang, L., Li, J., Xie, Y., Yang, P., Liao, Y., Guo, G., 2012. Effect of nano biphasic calcium
phosphate bioceramics on periodontal regeneration in the treatment of alveolar defects.
Adv. Mater. Res. 486, 422425.
Wang, Q., Liu, S., Gao, X., Wei, Y., Deng, X., Chen, H., et al., 2015a. Remineralizing efficacy of fluorohydroxyapatite gel on artificial dentinal caries lesion. J. Nanomater. 2015,
Article number 380326.
Wang, X., Suzawa, T., Miyauchi, T., Zhao, B., Yasuhara, R., Anada, T., et al., 2015b.
Synthetic octacalcium phosphate-enhanced reparative dentine formation via induction of
odontoblast differentiation. J. Tissue Eng. Regen. Med. 9, 13101320.
Wang, L., Xie, X., Li, C., Liu, H., Zhang, K., Zhou, Y., et al., 2017. Novel bioactive root
canal sealer to inhibit endodontic multispecies biofilms with remineralizing calcium
phosphate ions. J. Dent. 60, 2535.
Wefel, J.S., Harless, J.D., 1987. The use of saturated DCPD in remineralization of artificial
caries lesions in vitro. J. Dent. Res. 66, 16401643.
Wegehaupt, F.J., Attin, T., 2010. The role of fluoride and casein phosphopeptide/amorphous
calcium phosphate in the prevention of erosive/abrasive wear in an in vitro model using
hydrochloric acid. Caries Res. 44, 358363.
Wei, J., Wang, J., Shan, W., Liu, X., Ma, J., Liu, C., et al., 2011a. Development of fluorapatite
cement for dental enamel defects repair. J. Mater. Sci. Mater. Med. 22, 1607-1614.
Wei, J., Wang, J., Liu, X., Ma, J., Liu, C., Fang, J., et al., 2011b. Preparation of fluoride
substituted apatite cements as the building blocks for tooth enamel restoration. Appl.
Surf. Sci. 257, 78877892.
448
Advanced Dental Biomaterials
Weir, M.D., Chow, L.C., Xu, H.H.K., 2012. Remineralization of demineralized enamel via
calcium phosphate nanocomposite. J. Dent. Res. 91, 979984.
Weir, M.D., Ruan, J., Zhang, N., Chow, L.C., Zhang, K., Chang, X., et al., 2017. Effect of
calcium phosphate nanocomposite on in vitro remineralization of human dentin lesions.
Dent. Mater. 33, 10331044.
Weiss, P., Layrolle, P., Clergeau, L.P., Enckel, B., Pilet, P., Amouriq, Y., et al., 2007. The
safety and efficacy of an injectable bone substitute in dental sockets demonstrated in a
human clinical trial. Biomaterials 28, 32953305.
Wen, Z., Chen, J., Wang, H., Zhong, S., Hu, Y., Wang, Z., et al., 2016. Abalone watersoluble matrix for self-healing biomineralization of tooth defects. Mater. Sci. Eng. C 67,
182187.
West, N.X., Joiner, A., 2014. Enamel mineral loss. J. Dent 42 (Suppl. 1), S2S11.
White, J.M., Goodis, H., 1991. In vitro evaluation of an hydroxyapatite root canal system filling material. J. Endod. 17, 561566.
Widström, E., Birn, H., Haugejorden, O., Sundberg, H., 1992. Fear of amalgam: dentists’
experiences in the Nordic countries. Int. Dent. J. 42, 6570.
Willershausen, B., Schulz-Dobrick, B., Gleissner, C., 2009. In vitro evaluation of enamel
remineralisation by a casein phosphopeptide-amorphous calcium phosphate paste. Oral
Health Prev. Dent. 7, 1321.
Wilson, C.J., 1975. The effect of calcium sucrose phosphates chewing gum on caries incidence in children. J. Wis. Dent. Assoc. 51, 521525.
Wiltfang, J., Schlegel, K.A., Schultze-Mosgau, S., Nkenke, E., Zimmermann, R., Kessler, P.,
2003. Sinus floor augmentation with β-tricalciumphosphate (β-TCP): does platelet-rich
plasma promote its osseous integration and degradation? Clin. Oral Implant. Res. 14,
213218.
Wiltfang, J., Kessler, P., Buchfelder, M., Merten, H.A., Neukam, F.W., Rupprecht, S., 2004.
Reconstruction of skull bone defects using the hydroxyapatite cement with calvarial split
transplants. J. Oral Maxillofac. Surg. 62, 2935.
Witjaksono, W., Naing, L., Mulyawati, E., Samsudin, A.R., Oo, M.M.T., 2007. Sealing ability of hydroxyapatite as a root canal sealer: in vitro study. Dent. J 40, 101105.
Wittkampf, A.R.M., 1988. Augmentation of the maxillary alveolar ridge with hydroxylapatite
and fibrin glue. J. Oral Maxillofac. Surg. 46, 10191021.
Wolford, L.M., Freitas, R.Z., 1999. Porous block hydroxyapatite as a bone graft substitute in
the correction of jaw and craniofacial deformities. BUMC Proc. 12, 243246.
Wolford, L.M., Wardrop, R.W., Hartog, J.M., 1987. Coralline porous hydroxylapatite as
a bone graft substitute in orthognathic surgery. J. Oral Maxillofac. Surg. 45,
10341042.
Wu, D., Yang, J., Li, J., Chen, L., Tang, B., Chen, X., et al., 2013. Hydroxyapatite-anchored
dendrimer for in situ remineralization of human tooth enamel. Biomaterials 34,
50365047.
Wu, X.T., Mei, M.L., Li, Q.L., Cao, C.Y., Chen, J.L., Xia, R., et al., 2015. A direct electric
field-aided biomimetic mineralization system for inducing the remineralization of dentin
collagen matrix. Materials 8, 78897899.
Xiao, Y., Yin, Q., Wang, L., Bao, C., 2015. Macro-porous calcium phosphate scaffold with
collagen and growth factors for periodontal bone regeneration in dogs. Ceram. Int. 41,
9951003.
Xiao, Z., Que, K., Wang, H., An, R., Chen, Z., Qiu, Z., et al., 2017. Rapid biomimetic remineralization of the demineralized enamel surface using nano-particles of amorphous
calcium phosphate guided by chimaeric peptides. Dent. Mater. 33, 12171228.
Calcium orthophosphates as a dental regenerative material
449
Xie, C., Lu, H., Li, W., Chen, F.M., Zhao, Y.M., 2012. The use of calcium phosphate-based
biomaterials in implant dentistry. J. Mater. Sci. Mater. Med. 23, 853862.
Xie, X.J., Xing, D., Wang, L., Zhou, H., Weir, M.D., Bai, Y.X., et al., 2018. Novel rechargeable calcium phosphate nanoparticle-containing orthodontic cement. Int. J. Oral Sci. 9,
2432.
Xu, H.H.K., Moreau, J.L., 2010. Dental glass-reinforced composite for caries inhibition:
calcium phosphate ion release and mechanical properties. J. Biomed. Mater. Res. B:
Appl. Biomater. 92B, 332340.
Xu, H.H.K., Takagi, S., Sun, L., Hussain, L., Chow, L.C., Guthrie, W.F., et al., 2006a.
Development of a nonrigid, durable calcium phosphate cement for use in periodontal
bone repair. J. Am. Dent. Assoc. 137, 11311138.
Xu, H.H.K., Sun, L., Weir, M.D., Antonucci, J.M., Yakagi, S., Chow, L.C., et al., 2006b.
Nano DCPA-whisker composites with high strength and Ca and PO4 release. J. Dent.
Res. 85, 722727.
Xu, H.H.K., Sun, L., Weir, M.D., Takagi, S., Chow, L.C., Hockey, B., 2007a. Effects of
incorporating nanosized calcium phosphate particles on of properties of whiskerreinforced dental composites. J. Biomed. Mater. Res. B: Appl. Biomater. 81B,
116125.
Xu, H.H.K., Weir, M.D., Sun, L., Takagi, S., Chow, L.C., 2007b. Effects of calcium phosphate nanoparticles on Ca-PO4 composite. J. Dent. Res. 86, 378383.
Xu, H.H.K., Weir, M.D., Sun, L., 2007c. Nanocomposites with Ca and PO4 release: effects
of reinforcement, dicalcium phosphate particle size and silanization. Dent. Mater. 23,
14821491.
Xu, H.H.K., Weir, M.D., Sun, L., 2009. Calcium and phosphate ion releasing composite:
effect of pH on release and mechanical properties. Dent. Mater. 25, 535542.
Xu, H.H.K., Moreau, J.L., Sun, L., Chow, L.C., 2011. Nanocomposite containing amorphous
calcium phosphate nanoparticles for caries inhibition. Dent. Mater. 27, 762769.
Yamagishi, K., Onuma, K., Suzuki, T., Okada, F., Tagami, J., Otsuki, M., et al., 2005.
Materials chemistry: a synthetic enamel for rapid tooth repair. Nature 433, 819.
Yamaguchi, K., 1989. Biological evaluation of new hydroxyapatite endodontic cement
in vivo. Histopathological and clinico-pathological observation. Dent. Sci. Rep. 89,
761792.
Yamamoto, E., Kato, N., Nishikawa, H., Kusunoki, M., Hayami, T., Yoshikawa, K., et al.,
2013a. Adhesive strength between flexible hydroxyapatite sheet and tooth enamel. Key
Eng. Mater. 529530, 522525.
Yamamoto, E., Kato, N., Isai, A., Nishikawa, H., Kusunoki, M., Yoshikawa, K., et al.,
2013b. Restoration of tooth enamel using a flexible hydroxyapatite sheet coated with tricalcium phosphate. Bioceram. Dev. Appl S1, 006.
Yamamoto, E., Kato, N., Isai, A., Nishikawa, H., Hashimoto, Y., Yoshikawa, K., et al., 2015.
A novel treatment for dentine cavities with intraoral laser ablation method using an Er:
YAG laser. Key Eng. Mater. 631, 262266.
Yang, S.E., Baek, S.H., Lee, W., Kum, K.Y., Bae, K.S., 2007. In vitro evaluation of the sealing ability of newly developed calcium phosphate-based root canal sealer. J. Endod. 33,
978981.
Yang, X., Yang, F., Walboomers, X.F., Bian, Z., Fan, M., Jansen, J.A., 2010. The performance of dental pulp stem cells on nanofibrous PCL/gelatin/nHA scaffolds. J. Biomed.
Mater. Res. A 93A, 247257.
Yap, A.U., Pek, Y.S., Kumar, R.A., Cheang, P., Khor, K.A., 2002. Experimental studies on a
new bioactive material: HAIonomer cements. Biomaterials 23, 955962.
450
Advanced Dental Biomaterials
Yates, R., Owens, J., Jackson, R., Newcombe, R.G., Addy, M., 1998. A split-mouth placebocontrolled study to determine the effect of amorphous calcium phosphate in the treatment of dentine hypersensitivity. J. Clin. Periodontol. 25, 687692.
Yelick, P.C., Vacanti, J.P., 2006. Bioengineered teeth from tooth bud cells. Dent. Clin. North
Am. 50, 191203.
Yengopal, V., Mickenautsch, S., 2009. Caries preventive effect of casein phosphopeptideamorphous calcium phosphate (CPP-ACP): a meta-analysis. Acta Odontol. Scand. 67,
321332.
Yin, Y., Yun, S., Fang, J., Chen, H., 2009. Chemical regeneration of human tooth enamel
under near-physiological conditions. Chem. Commun. 58925894.
Ylinen, P., Suuronen, R., Taurio, R., Törmälä, P., Rokkanen, P., 2002. Use of hydroxylapatite/polymer-composite in facial bone augmentation. An experimental study. Int. J. Oral
Maxillofac. Surg. 31, 405409.
Yoshiba, K., Yoshiba, N., Iwaku, M., 1994. Histological observations of hard tissue barrier
formation in amputated dental pulp capped with alpha-tricalcium phosphate containing
calcium hydroxide. Endod. Dent. Traumatol. 10, 113120.
Yoshikawa, M., Hayami, S., Tsuji, I., Toda, T., 1997. Histopathological study of a newly
developed root canal sealer containing tetracalcium-dicalcium phosphates and 1.0%
chondroitin sulfate. J. Endod. 23, 162166.
Yoshinari, M., Oda, Y., Inoue, T., Matsuzaka, K., Shimono, M., 2002. Bone response to calcium phosphate-coated and bisphosphonate-immobilized titanium implants. Biomaterials
23, 28792885.
Yoshino, K., Taniguchi, Y., Yoda, Y., Matsukubo, T., 2013. Autotransplantation of tooth by
osteotome sinus floor elevation technique with beta-tricalcium phosphate (β-TCP). J.
Oral Maxillofac. Surg. Med. Pathol. 25, 351354.
Yoshinuma, N., Sato, S., Fukuyama, T., Murai, M., Ito, K., 2012. Ankylosis of nonresorbable
hydroxyapatite graft material as a contributing factor in recurrent periodontitis. Int. J.
Periodontics Restorative Dent. 32, 331336.
Yu, J.M., Choe, H.C., 2018. Mg-containing hydroxyapatite coatings on Ti-6Al-4V alloy for
dental materials. Appl. Surf. Sci. 432, 294299.
Yu, L., Xu, B., Wu, B., 2003. Treatment of combined endodontic-periodontic lesions by
intentional replantation and application of hydroxyapatites. Dent. Traumatol. 19,
6063.
Yu, J.H., Wang, Y.J., Deng, Z.H., Tang, L., Li, Y.F., Shi, J.N., et al., 2007. Odontogenic
capability: bone marrow stromal stem cells versus dental pulp stem cells. Biol. Cell 99,
465674.
Yu, O.Y., Zhao, I.S., Mei, M.L., Lo, E.C.M., Chu, C.H., 2017. A review of the common
models used in mechanistic studies on demineralization-remineralization for cariology
research. Dent. J 5, 20.
Yukna, R.A., Callan, D.P., Krauser, J.T., Evans, G.H., Aichelmann-Reidy, M.E., Moore, K.,
et al., 1998. Multi-center clinical evaluation of combination anorganic bovine-derived
hydroxyapatite matrix (ABM)/cell binding peptide (P-15) as a bone replacement graft
material in human periodontal osseous defects. 6-month results. J. Periodontol. 69,
655663.
Zaharia, A., Muşat, V., Anghel, E.M., Atkinson, I., Mocioiu, O.C., Buşilă, M., et al., 2017.
Biomimetic chitosan-hydroxyapatite hybrid biocoatings for enamel remineralization.
Ceram. Int. 43, 1139011402.
Zecha, P.J., Schortinghuis, J., van der Wal, J.E., Nagursky, H., van den Broek, K.C.,
Sauerbier, S., et al., 2011. Applicability of equine hydroxyapatite collagen (eHAC) bone
Calcium orthophosphates as a dental regenerative material
451
blocks for lateral augmentation of the alveolar crest. A histological and histomorphometric analysis in rats. Int. J. Oral Maxillofac. Surg. 40, 533542.
Zeltser, C., Masella, R., Cholewa, J., Mercier, P., 1989. Surgical and prosthodontic residual
ridge reconstruction with hydroxyapatite. J. Prost. Dent. 62, 441448.
Zerbo, I.R., Zijderveld, S.A., de Boer, A., Bronckers, A.L.J.J., de Lange, G., ten Bruggenkate,
C.M., et al., 2004. Histomorphometry of human sinus floor augmentation using a porous
β-tricalcium phosphate: a prospective study. Clin. Oral Implant. Res. 15, 724732.
Zhang, Y., Wang, Y., 2012. Hydroxyapatite effect on photopolymerization of self-etching
adhesives with different aggressiveness. J. Dent. 40, 564570.
Zhang, Y.P., Din, C.S., Miller, S., Nathoo, S.A., Gaffar, A., 1995. Intra-oral remineralization
of enamel with a MFP/DCPD and MFP/silica dentifrice using surface microhardness. J.
Clin. Dent. 6, 148153.
Zhang, W., Walboomers, X.F., Jansen, J.A., 2008. The formation of tertiary dentin after pulp
capping with a calcium phosphate cement, loaded with PLGA microparticles containing
TGF-β1. J. Biomed. Mater. Res. A 85A, 439444.
Zhang, J.C., Lu, H.Y., Lv, G.Y., Mo, A.C., Yan, Y.G., Huang, C., 2010. The repair of
critical-size defects with porous hydroxyapatite/polyamide nanocomposite: an experimental study in rabbit mandibles. Int. J. Oral Maxillofac. Surg. 39, 469477.
Zhang, Q., Zou, J., Yang, R., Zhou, X., 2011. Remineralization effects of casein
phosphopeptide-amorphous calcium phosphate crème on artificial early enamel lesions
of primary teeth. Int. J. Paediatr. Dent 21, 374381.
Zhang, X., Li, Y., Sun, X., Kisheen, A., Deng, X., Yang, X., et al., 2014. Biomimetic remineralization of demineralized enamel with nano-complexes of phosphorylated chitosan
and amorphous calcium phosphate. J. Mater. Sci. Mater. Med. 25, 26192628.
Zhang, L., Weir, M.D., Chow, L.C., Antonucci, J.M., Chen, J., Xu, H.H.K., 2016a. Novel
rechargeable calcium phosphate dental nanocomposite. Dent. Mater. 32, 285293.
Zhang, L., Weir, M.D., Chow, L.C., Reynolds, M.A., Xu, H.H.K., 2016b. Rechargeable calcium phosphate orthodontic cement with sustained ion release and re-release. Sci. Rep.
6, 36476 (11 pp.).
Zhang, K., Cheng, L., Weir, M.D., Bai, Y.X., Xu, H.H.K., 2016c. Effects of quaternary
ammonium chain length on the antibacterial and remineralizing effects of a calcium
phosphate nanocomposite. Int. J. Oral Sci. 8, 4553.
Zhao, J., Liu, Y., Sun, W.B., Zhang, H., 2011. Amorphous calcium phosphate and its application in dentistry. Chem. Cent. J. 8, 40 (7 pp.).
Zhao, J., Liu, Y., Sun, W.B., Yang, X., 2012. First detection, characterization, and application of amorphous calcium phosphate in dentistry. J. Dent. Sci. 7, 316323.
Zhen, T., Hongkun, W., Anchun, M., Zhiqin, C., Yubao, L., 2007. Effect of apatite nanoparticles on remineralization of the demineralized human dentin. Key Eng. Mater. 330332,
13811384.
Zheng, L., Yang, F., Shen, H., Hu, X., Mochizuki, C., Sato, M., et al., 2011. The effect of
composition of calcium phosphate composite scaffolds on the formation of tooth tissue
from human dental pulp stem cells. Biomaterials 32, 70537059.
Zhou, C., Zhang, D., Bai, Y., Li, S., 2014. Casein phosphopeptide-amorphous calcium phosphate remineralization of primary teeth early enamel lesions. J. Dent. 42, 2129.
Zhou, J., Chiba, A., Scheffel, D.L., Hebling, J., Agee, K., Niu, L.N., et al., 2016. Effects of a
dicalcium and tetracalcium phosphate-based desensitizer on in vitro dentin permeability.
PLoS One 11, e0158400.
Zijderveld, S.A., Zerbo, I.R., van den Bergh, J.P.A., Schulten, E.A.J.M., ten Bruggenkate, C.
M., 2005. Maxillary sinus floor augmentation using a β-tricalcium phosphate
452
Advanced Dental Biomaterials
(Cerasorbs) alone compared to autogenous bone grafts. Int. J. Oral Maxillofac.
Implants 20, 432440.
Zuolin, J., Hong, Q., Jiali, T., 2010. Dental follicle cells combined with beta-tricalcium phosphate ceramic: a novel available therapeutic strategy to restore periodontal defects. Med.
Hypotheses 75, 669670.
https://en.wikipedia.org/wiki/Dental_public_health (accessed May 2018.).
https://en.wikipedia.org/wiki/Dentifrice (accessed May 2018.).
https://en.wikipedia.org/wiki/Dentin_hypersensitivity (accessed May 2018.).
https://en.wikipedia.org/wiki/Dentistry (accessed May 2018.).
https://en.wikipedia.org/wiki/Endodontics (accessed May 2018.).
https://en.wikipedia.org/wiki/Mucositis (accessed May 2018.).
https://en.wikipedia.org/wiki/Orthodontics (accessed May 2018.).
https://en.wikipedia.org/wiki/Prosthodontics (accessed May 2018.).
https://en.wikipedia.org/wiki/Specialty_dentistry (accessed May 2018.).
Further reading
Kamakura, S., Sasano, Y., Homma, H., Suzuki, O., Kagayama, M., Motegi, K., 2001.
Experimental oral pathology: implantation of octacalcium phosphate nucleates isolated
bone formation in rat skull defects. Oral Dis. 7, 259265.
McDonagh, M.S., Kleijnen, J., Whiting, P.F., Wilson, P.M., Sutton, A.J., Chestnutt, I., et al.,
2000. Systematic review of water fluoridation. Br. Med. J. 321, 855859.
Bioactive glasses—structure and
applications
17
Imran Farooq1, Saqib Ali1, Shehriar Husain2, Erum Khan3,4 and
Robert G. Hill5
1
Department of Biomedical Dental Sciences, College of Dentistry, Imam Abdulrahman Bin
Faisal University, Dammam, Saudi Arabia, 2Department of Dental Materials Science,
Jinnah Sindh Medical University, Karachi, Pakistan, 3Bhitai Dental and Medical College,
Liaquat University of Medical and Health Sciences, Jamshoro, Pakistan, 4Faculty of
Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia, 5Dental Physical Sciences,
Institute of Dentistry, Barts and The London School of Medicine and Dentistry, Queen
Mary University of London, London, United Kingdom
Chapter Outline
17.1 Introduction 454
17.2 Bioactivity of glasses
454
17.2.1 Mechanism of action 455
17.2.2 Solubility 455
17.3 Factors affecting apatite formation 456
17.4 Composition of different bioactive glasses
456
17.4.1 Silicate-based bioactive glasses 457
17.4.2 Borate-based bioactive glasses 458
17.5 Methods of synthesis 460
17.6 Clinical applications of bioactive glasses
17.6.1
17.6.2
17.6.3
17.6.4
17.6.5
17.6.6
17.6.7
17.6.8
17.6.9
460
Bone graft substitute 461
Bone regeneration 461
Drug delivery system 462
Coating of implants 463
Use in toothpastes 463
Antibacterial activity 465
Role in minimal invasive dentistry 465
Bioactive glass scaffolds 465
Particle size of bioactive glasses and its effect on various clinical applications 468
17.7 Future of bioactive glasses
17.8 Conclusion 470
References 470
Further reading 476
469
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00017-7
Copyright © 2019 Elsevier Ltd. All rights reserved.
454
17.1
Advanced Dental Biomaterials
Introduction
“A material is said to be bioactive, if it gives an appropriate biological response
and results in the formation of a bond between material and the tissue” (Farooq
et al., 2012). Bioactive glass (BG) is a biomaterial that was introduced by Prof.
Larry Hench in 1969 (Hench, 2006), with the intent of developing a biocompatible
material that forms an intimate bond with the bone. The first glass discovered is
known as 45S5 (Bioglass), having a glass composition of 46.1 mol.% SiO2,
24.4 mol.% Na2O, 26.9 mol.% CaO, and 2.6 mol.% P2O5 (Kobayashi et al., 2010).
BG has the capability to interact with the body tissues to form a resilient bond, and
its controlled degradation over time is useful in releasing therapeutic ions, which
can help the bone regeneration (Fuchs et al., 2015; Ali et al., 2014). Safety of these
glasses was a concern, so various studies were performed, and these glasses were
graded safe to be used by US Food and Drug Administration (FDA) (Paolinelis
et al., 2008). BGs are synthetic and osteoconductive materials that form a hydroxycarbonate apatite (HCA) layer at the site, after the dissolution of the glass (Jones,
2013). This HCA is comparable to the bone mineral, and it interacts with collagen
fibers of the bone to form an adherent interface between the material and the tissue
(Jones, 2013; Nejatain et al., 2017). Recently, BGs have been used for different
dental applications such as in toothpaste to enhance enamel remineralization and
occlude open dentinal tubules (Farooq et al., 2012).
Recent modifications in the structure of BG have resulted in various formulations being available, such as high phosphate-based glasses, borate-based glasses,
and fluoride-containing BGs (Khalid et al., 2017), and these glasses are different
from the conventional 45S5 glass. Borate and phosphate glasses have rapid solubility (which can be altered from several hours to several months based on the end
application) (Fu et al., 2010a), whereas fluoride-containing glasses can form fluorapatite (FAP) layer, on the surface, which promotes remineralization and is more
durable in the mouth (Farooq et al., 2013).
This chapter focuses on the structure of different BGs and their clinical applications. Apart from these objectives, this chapter also reviews the methods of their
synthesis and gives an overview of bioactivity of these glasses.
17.2
Bioactivity of glasses
The BGs are highly bioactive and a previous in vitro study has demonstrated the
formation of apatite by the new composition of glasses in Tris-buffer solution, in as
little as 6 hours (Farooq et al., 2013). These glasses stimulate cell cycling in vitro,
which results in stimulation of osteoblasts, as a result of which more mineralized
tissue is formed in a shorter time (Xynos et al., 2000). Due to ion exchange, BGs
can raise the pH of the solution in which they are present, thus exhibiting antibacterial effects (Gubler et al., 2008). Some groups of these glasses, such as silvercontaining BGs (Newby et al., 2011), release important ions, such as silver, which
Bioactive glasses—structure and applications
455
can augment these antibacterial effects (Kwakye-Awuah et al., 2008). In vivo studies are important as they help in predicting the clinical performance of a material.
An in vivo survey carried out in rabbits showed better performance of 45S5 as compared to the synthetic hydroxyapatite (HAP) regarding bone regeneration (Oonishi
et al., 2000).
17.2.1 Mechanism of action
The bioactivity of these glasses is dependent on their mechanism and speed of
action. Briefly, the reactions to form HAP involve ion exchange of Ca21 and Na1
ions for H1 ions from the solution, a consequent increase in the pH of the solution,
the formation of silanol (Si-OH) bonds on the surface of the glass, and the resulting
formation of a silica-rich layer, degradation of silica (due to increased pH), and
then then the development of a layer of amorphous CaO P2O5 on the silica-rich
layer, which then crystallizes as HAP due to the absorption of hydroxyl and carbonate ions (Jones, 2013).
17.2.2 Solubility
The glass composition plays a vital role in determining the solubility and bioactivity of BGs. At this point, understanding some other terms such as glass transition
temperature (Tg) and network connectivity (NC) becomes essential.
The Tg is defined as a range of transformation when an amorphous solid is converted into a supercooled liquid on heating (Dudowicz et al., 2005). The degradation rate of the glass and its strength can be assessed through Tg (O’Donnell, 2011).
There is a presence of a significant processing window between the Tg and peak
crystallization temperature of glass warrants that the glass will not crystallize during
quenching (Dimarzio and Gibbs, 1959). The presence of crystalline phases reduces
the exchange of ions, and thus bioactivity is reduced (Ali et al., 2014).
The NC can be defined as the mean number of bridging oxygen bonds per silicon
atom (Hill and Brauer, 2011). It can be used to analyze the solubility and bioactivity of a glass, as a low NC implies that the glass has lower Tg, but a high solubility
and bioactivity (Hill, 1996).
The silica in the glass is considered a network former, which can hold the glass
structure together (Srivastava et al., 2012). Therefore a lower content of silica can
ensure faster dissolution and more rapid bioactivity (Jones, 2013). Fluoride is an
essential ion when it comes to dentistry as it remineralizes tooth structure and prevents demineralization (Featherstone, 2000). The inclusion of fluoride in the BG
composition decreases its Tg, which means that the glass will have a reduced hardness, but it will be more bioactive (Farooq et al., 2012). Sodium oxide (Na2O) can
also affect the properties of BGs. The Na2O is regarded as a network disrupter as
its addition expands the glass network; therefore it reduces Tg and the glass
becomes more bioactive (Wallace et al., 1999). In the fluoride-containing BG compositions, when phosphate content is increased, it results in maintenance of the NC
and formation of FAP (Brauer et al., 2010). In an in vitro study, it was reported that
456
Advanced Dental Biomaterials
high phosphate-containing BGs were able to form apatite more rapidly in Trisbuffer solution and within 6 hours, as compared with low phosphate-containing
BGs (which formed apatite after 3 days) (Mneimne et al., 2011). This means that
by controlling the amount of phosphate in the BG composition, reactivity, and
apatite-forming ability of the BGs can be controlled (Mneimne et al., 2011).
17.3
Factors affecting apatite formation
Many factors, such as different ions, can accelerate or hinder apatite formation ability of BGs. As described in the previous section, phosphate content can significantly increase apatite formation capabilities of BGs (when NC is maintained)
(O’Donnell et al., 2009). Similarly, controlled addition of fluoride (Brauer et al.,
2010) and substitution of calcium by strontium can positively favor the apatite formation process (Brauer, 2015). On the other hand, magnesium ions have been
shown to delay or inhibit apatite formation (Diba et al., 2012), probably due to the
obstruction of active growth sites on the apatite crystal surfaces (Kanzaki et al.,
2000).
Generally, for dental applications, faster apatite formation is required, whereas
for some other medical applications, such as cartilage repair, a slower apatite formation is desirable (Brauer, 2015). Therefore the addition of different ions into BG
composition can be carefully planned according to the desired outcome.
17.4
Composition of different bioactive glasses
The affinity of a biomaterial to bond to mineralized biological tissue is dependent
upon its composition. A range of such glass systems has been developed over the
years, which include compositional modifications with certain elemental additives
and variations in synthesis techniques. The compositions of 45S5 and a few essential variants are shown in Table 17.1.
Table 17.1 Composition of different bioactive glasses (Khalid et al., 2017).
45S5
13 93
6P53B
58S
70S30C
13 93B1
13 93B1
P50C35N15
Na2O
K2O
MgO
CaO
SiO2
P2O5
B2O3
24.5
6.0
10.3
0
0
5.8
5.5
9.3
0
12.0
2.8
0
0
11.7
11.1
0
0
5.0
10.2
0
0
4.9
4.6
0
24.5
20.0
18.0
32.6
28.6
19.5
18.5
19.7
45.0
53.0
52.7
58.2
71.4
34.4
0
0
6.0
4.0
6.0
9.2
0
3.8
3.7
71.0
0
0
0
0
0
19.9
56.6
0
Bioactive glasses—structure and applications
457
17.4.1 Silicate-based bioactive glasses
Silicate glasses are considered as a reliable material when considering the design of
novel medical devices boasting specific properties. A large surface area, a high
degree of purity index, and porosity within the bulk of the material contribute significantly toward the high level of reactivity exhibited when employing this material for research purposes and as a component of a biomaterial (Aguiar et al., 2009).
The open-ended structure of these BGs enables the manifestation of free space
within the bulk of the material. This allows for the addition of Na1, K1, Ca21, and
Mg21 cations into the glass matrix. These cationic species are termed as network
modifiers. Network modifiers are known to induce network disruption—a crucial
preliminary step if realization of nonbridging oxygen (NBO) groups is to occur
within the glass structure (González et al., 2003; Sen and Youngman, 2003). The
presence of NBOs has a strong influence on the connectivity of the material as a
whole.
The commercial variant 45S5 (based on silicate glass) has been the focus of multiple studies pertaining to biomedical applications (Hench, 2006). The inherent
properties of this version of 45S5 allow for it to bond to mineralized bone tissue—a
phenomenon which has been the subject of numerous investigations for the better
part of four decades and counting. The silicate glass 45S5 structure can be best
visualized as a three-dimensional (3D) SiO2 network with a central silicon ion surrounded by four coordinating oxygen ions arranged in a tetrahedron configuration.
The SiO2 content in silicate BG compositions is in direct relation to their chemical
stability. Moreover, glass network modifiers in variable ratios are the primary structural and compositional determinants of the bioactive nature of this material.
Common glass network modifiers include Na2O and CaO, whereas magnesium
(Mg21) and zinc (Zn21) fall on the border of modifiers and intermediate ions
(which increase the processing window to avoid crystallization) (Dietzel, 1941).
The role of these modifiers is to break some part of the Si O bonds, thereby creating NBOs and disturbing the tetrahedral silicate network (Benoit et al., 2001). In
other words, these network modifiers are responsible for considerably lowering the
connectivity value of the SiO2 network attributed to the formation of nonbridging
silicon oxygen bonds. The resulting enhanced dissolution index translates into an
increased probability of ionic exchange events at the surface of the material that
would eventually contribute to the formation of a biomimetic HAP layer on the surface of the implanted material (Vichery and Nedelec, 2016; Hench, 1991).
Phosphate ions can increase the bioactivity of the glass (Mercier et al., 2011), and a
linear relationship in terms of increased bioactivity can be observed with the addition of phosphate in BG, owing to the inherent ability of phosphate to influence the
formation of apatite in living mineralized tissues (Hill and Brauer, 2011). Some
studies have aimed to decipher the bonding configurations and the presence of
NBO groups by utilizing spectroscopic techniques such as infrared (IR) spectroscopy and X-ray photoelectron spectroscopy (Serra et al., 2003). The results from
these analyses were found to be in agreement with one another. The inclusion of
network modifiers to the silica network has a direct effect on electron density of the
458
Advanced Dental Biomaterials
bonding states of the silicon and oxygen atomic structure (Serra et al., 2003).
Moreover, by carrying out these analyses, the investigators were able to demonstrate a rise in the proportion of alkali-earth elements in the silica network, which
leads to a concurrent cleavage of Si O Si (bridging oxygen) by Si O NBO
groups (nonbridging silicon oxygen groups). This has far-reaching implications in
terms of eliciting a reproducible and robust biological response at the material interface when submerged in body fluids (Peitl et al., 2001). The role of NBO groups
during the initial stages of bioactivity of BGs is of much importance. IR spectroscopy has emerged as a powerful tool that yields useful information in terms of
developing a quantifiable database pertaining to the concentration of Si O NBO
groups and ultimately their bond strength, which may be ascertained from the relative intensity of the respective IR absorption bands. The ideal ratio between the
Si O NBO and the Si O groups, estimated to be at $ 1 as derived from IR
absorption band intensity, is critical for realization of an effective ion exchange and
subsequent dissolution of the silica—ultimately contributing to the formation of an
SiO2-rich layer on the material surface (Serra et al., 2002). Therefore a definite correlation exists between the nature and type of NBO functional groups and the formation of calcium phosphate rich layers. Hence spectroscopic techniques have
established themselves as reliable techniques for gaining a deeper understanding of
the pivotal role of network modifiers through alteration of the BG structure and
subsequently their bioactive behavior.
When the 45S5 BG is implanted, a chemical degradation reaction process releasing cationic species such as Na1 and Ca21 ensues. This paves the way for the formation of a carbonate-substituted HAP-like material. This leads to a subsequent
release of silicon in the guise of silicic acid (Si(OH)4) (Lai et al., 2002). The low
SiO2 and high Na2O and CaO content are important compositional features determining the bioactivity of 45S5 (Huang et al., 2006a).
Many investigators still consider the original 45S5 version as the gold standard
in the realm of BG for hard mineralized tissue regeneration. However, issues pertaining to the impact of time-dependent release of degradation products especially
during the initial stages, when there is an uptake in the alkaline earth metal sourced
cationic species concentrations of Na1 and Ca21 from the bulk of the material with
accompanying pH changes (Tahriri et al., 2017), have yet to be fully elucidated in
light of their biological niche, toxicity, and subsequent dispersion from the site of
implantation. Another limitation of 45S5 glass is its incredible performance in high
load-bearing applications such as bone scaffolds (Hench and Jones, 2015). Research
is still going on to achieve tougher scaffolds that can serve as an appropriate scaffolding material.
17.4.2 Borate-based bioactive glasses
The trace element boron is essential for maintaining bone health. The first borosilicate glass formulation to be considered for biomedical applications was conceived in 1990 (Brink, 1997). These glasses are considered as a reactive species,
which accounts for their low chemical stability index. This translates to a more
Bioactive glasses—structure and applications
459
rapid conversion rate into HAP for this group of BG as compared to their silicabased counterparts (Yao et al., 2007). The substitution of SiO2 with B2O3 allowed
a significant escalation in the conversion rate of borate glass to HAP postimmersion in aqueous phosphate solutions (Huang et al., 2006b). Although the mechanism by which borate-based BG undergoes conversion to a layer of apatite is
similar to its silica-based equivalent, in that a borate-rich layer ensues in place of
a silicate-rich layer, borate-based BGs are more amenable to precise tinkering
with the degradation profile and sintering behavior, which can be achieved over a
range of time lines in contrast to silicate-based BGs (Yang et al., 2012). Spanning
the course of a few decades, a significant amount of research has been conducted,
and consequently, key data have been generated from studies pertaining to the
behavior and properties of the original formulation of 45S5 BG. On the other
hand, probing research questions exploring borate-based compositions are only
just beginning to surface in the literature (Rahaman et al., 2011; Kaur et al., 2014)
An innovative take on developing BG powders was the development of sphericalshaped borate-based BG powders for replacement of bone tissue using spray
pyrolysis (Cho and Kang, 2009). Evidence for the resulting crystalline structure of
the powders prepared in this way was gathered using X-ray diffraction (XRD)
analysis. The preparation technique had a profound influence on the phase transitions observed in the glass powder. Powders synthesized (using pyrolysis) below
a temperature range of 1400 C predominantly exhibited a crystalline phase that
dominated the composition. A low rate of turnover to the glass phase was attributed, in this instance, to a shorter “stay” time within the confines of the alumina
reactor. The opposite is true in the case of increased preparation temperatures of
1500 C, in that the amorphous phase enjoyed a majority throughout the glass substructure summed up by a reduction in sharpness of the XRD peaks. In this way
ideal temperature parameters for preparing spherical bioactive borate-based glass
powders with a dense inner core were identified to stand at 1200 C. A standing
criticism leveled against silicate-based BG stems from an incomplete conversion
process for yielding a calcium phosphate material postimplantation in vivo.
Indeed corresponding XRD patterns between different glass samples have in fact
revealed the strongest intensity hydroxyapatite (HA) peaks, an indication of
enhanced bioactive potential, in glass samples with increasing B2O3:SiO2 molar
ratio postimmersion in a phosphate solution (Fu et al., 2007). These findings were
in agreement with pH and weight loss studies—solutions containing glass samples
having increased B2O3 content consistently showing increased pH values and
more significant weight loss with immersion time compared to neat borate- and
silicate-based glass samples (Huang et al., 2006b). The significant disparity in the
reactivity, pH, and observable weight change rate between silicate and boratebased glass is primarily attributed to their overall network structure. The BO3
trihedron chains possess a threefold coordination number that hinders the formation of a 3D network structure when compared to their silicon-based counterpart
(Cheng et al., 2009). This has a profound impact in lowering the chemical
durability of the borate glass network structure translating to an accelerated dissolution rate.
460
Advanced Dental Biomaterials
Moreover, in line with the suggestion put forth by prominently featured works,
formation of a layer of HA on the surface of a biomaterial under certain parameters
in vitro can be extrapolated as its bioactive potential in vivo (Hench, 1998;
Zadpoor, 2014). The formation of a dense microstructured HAP as evidenced by
scanning electron microscopy (SEM)-based surface morphological analysis on
borate-based BG samples as reported previously (Yao et al., 2007) can be evaluated
as evidence for bioactive potential in the same light. It is important to mention at
this point the deviations in the mechanism that allows for the conversion of boratebased BG and silicate-based BG to carbonate-substituted HAP. Even though a large
part of the dissolution precipitation reaction process for both glasses is similar for
the most part, pure borate-based BG conversion to carbonate-substituted HAP differs considerably in that it does not involve the formation of the SiO2-rich layer at
any point of the conversion and dissolution sequence when assessed postimmersion
in a phosphate-rich solution (Huang et al., 2006b). Rather a complete ionic dissolution of the borate-based glass into the solution ensues due to a simultaneous infiltration and breakdown of the B O glass network structure by the phosphate solution.
The process continues until the full conversion of the borate glass to carbonatesubstituted HAP postleaching and reaction of the Ca21 ions with the PO432 in
solution. The rate at which borate-based BG undergoes conversion to carbonatedsubstituted HAP, a reliable scale for a measure of its degree of bioactivity, is
heavily predicated on the B2O3:SiO2 ratio of the glass, with a higher B2O3 level
translating to a higher borate glass conversion rate to HAP in this case.
17.5
Methods of synthesis
The BGs require a high standard of raw material purity prior to their preparation.
This is mainly because the quality of the materials heavily influences the quality of
the end product at the starting point. Pure silica sand (quartz), reactive grade carbonates of sodium and/or potassium, etc. are some of the common ingredients
required in weighted amounts. BGs are usually of a soft nature. This usually allows
for their easy shaping and sizing. Two common methods of preparing BGs include
melt quenching (at temperatures exceeding 1200 C) and sol gel method (converting the system from a liquid “sol” into a solid “gel”) (O’Donnell, 2012). However,
going into the details of these methods is beyond the scope of this chapter.
17.6
Clinical applications of bioactive glasses
The BGs are different from conventional glasses as they possess numerous features
which ensure their wide-ranging clinical applications. These glasses are biocompatible, osteoconductive, and can bond firmly to the tissue (Toosi and Behravan, 2017).
The conventional silicate-based glasses are composed of phosphate and calcium in
somewhat similar proportion to that of the bone HAP. Due to these abilities, they
Bioactive glasses—structure and applications
461
can be utilized in a broad range of medical and dental applications. The BGs can be
divided into different families having different compositions, which can be used for
a specific function or to achieve a desired clinical outcome (Rao and Ravindranadh,
2016). These glasses can be effectively used for replacement, repair, or reconstruction of different body parts such as bone and teeth (Baino et al., 2014). Some of the
most important applications of BGs are discussed in the following subsections.
17.6.1 Bone graft substitute
When bone is lost due to an infection, disease process, or trauma, the bone can be
replaced with a bone graft. Clinically, BG has been in use for more than a decade
as a synthetic bone graft. In orthopedics, it is as a product called Novabone
(Elshahat, 2006) and in maxillofacial surgeries as PerioGlas (Fetner et al., 1994).
A very common BG which has been used as a bone graft is 45S5 (Rao and
Ravindranadh, 2016). The FDA in 2005 permitted the use of 45S5 for osteostimulation (Hench, 1998). In another study it was reported that BGs have an osteostimulatory effect along with an osteoconductive function (Boccaccini et al., 2010), which
other osteoconductive bioceramics usually lack (Gerhardt and Boccaccini, 2010).
Also, their ability to bond to osseous tissues is much superior as compared with
other alloplastic materials (Wilson et al., 1993).
It is a reality that BGs do not have ideal mechanical properties, but the addition
of Na2O into SiO2 CaO BG composition improves its biological absorbability and
mechanical capability (Chen et al., 2010). A previous study reported that BG scaffolds can totally resorb in 6 months with little inflammatory response (Moimas
et al., 2006), demonstrating their superiority over other bone graft materials which
can cause adverse reactions as well (Wang and Yeung, 2017).
An earlier study that was conducted on animal models where properties of BG
and HAP were compared concluded that it is very easy to manipulate the composition of BG for specific uses, and BG takes less time in response generation as compared to HAP (Oonishi et al., 1997). The BGs when used as a bone graft have also
shown admirable bone healing properties in numerous follow-ups of long-term studies (Khalid et al., 2017; Van-Gestel et al., 2015).
17.6.2 Bone regeneration
Bone regeneration is another important clinical application, and BGs have a greater
filler effect than that of an autogenous bone (Heikkilä et al., 1995). In a previous
study by Macedo et al. (2004) two different compositions of BGs were used to
study bone formation in tibiae of rats, and it was reported that both compositions of
BGs promoted bone formation. It has been reported earlier that significant bone
regeneration can be promoted by BGs in vitro as they have osteostimulatory effects
(Hench, 2013). The presence of BGs in the treatment of large bony defects can
result in infection-free bone regeneration (Stoor et al., 2017). In an animal study,
periodontal defects were treated with particles of BG, which triggered bone mineralization (Felipe et al., 2009).
462
Advanced Dental Biomaterials
One of the advancements in BG research is control of its degradation rate with
the manipulation of its composition. Borate-based BGs are very useful in bone
regeneration because of the variation of controlled degradations rates along with the
ease of their fabrication. The compositional flexibility and easy manipulation of the
glass composition can make it a source of different elements such as copper, fluoride, or boron which can encourage growth of the bone (Toosi and Behravan,
2017).
17.6.3 Drug delivery system
Researchers have always been looking for an innovative drug delivery system to
have superior medication control with a prolonged action. Assuming that a certain
medication or molecule will reach a specific site without any secondary reactions
and will perform the desired reaction, the drug delivery system becomes supremely
important to the researchers.
These glasses show larger flexibility in terms of compositional manipulation,
making them independent of any specific stoichiometry. Thus ions of various concentrations having different therapeutic properties can be incorporated in conventional compositions. These ions can be released during the process of dissolution,
and they can execute their desired therapeutic function in the human body (Hoppe
et al., 2011). In a study on pulp capping agents containing BG, there was a greater
occurrence of development of a properly positioned dentin bridge (Stanley et al.,
2001).
As discussed earlier, borate-based BGs are used in bone regeneration and can
also be used in the treatment of infection of bone, where they act as a drugreleasing substrate (Liu et al., 2010; Jia et al., 2010). An earlier in vitro study comparing borate-based BGs with 45S5 reported that higher content of B2O3 improved
the conversion rate to HAP, as compared to 45S5 particles, which stopped after
only partial conversion of particles to HAP (Brown et al., 2009). Another study has
also revealed that teicoplanin-loaded borate BG implants could be helpful in treating chronic osteomyelitis in animals (Zhang et al., 2010), so it can be predicted that
they will be equally useful in humans as well.
In a previous study conducted on animal models, BG porous blocks were used
for delivering antibiotics in treating osteomyelitis (Kundu et al., 2011). After 2 years
of treatment of infected arthroplasty, some outstanding results were witnessed, and
osteogenesis was triggered by the implant material, which was evident on radiography where complete radiological replacement of the osseous defects was seen
(Kawanabe et al., 1998).
Excellent bone integration and biocompatibility were seen in BG implants
infused with gentamicin sulfate, which released gentamicin into local osseous tissues, and during the resorption process, these implants also promoted the growth of
the bone (Meseguer-Olmo et al., 2006; Arcos et al., 2001). In another study BG
combined with tetracycline and BG combined with tetracycline:beta-cyclodextrin
were able to demonstrate considerable bacteriostatic activity with little effect on the
bioactivity of the glass itself (Domingues et al., 2004).
Bioactive glasses—structure and applications
463
17.6.4 Coating of implants
The success of dental implants is dependent on several factors, of which the implant
material is of utmost importance (Najeeb et al., 2015). Over time, the use of metallic materials has grown significantly due to their ideal mechanical properties
(Roessler et al., 2002). Metals such as titanium, cobalt, and stainless steel (SS)
grade 316L are used in the preparation of implants (Garcia et al., 2004). SS has
been the choice in orthopedic implants as it is quite economical (Fathi et al., 2003).
But this material, in long-term use, is very much prone to unwanted biological reactions, thus leading to failure of the implant mechanically. Titanium (Ti) and
Ti-alloys have good mechanical and physical properties which makes them the
material of choice for implant applications, and currently, they are the most widely
used implant material (Najeeb et al., 2017). It is a challenge to get a perfect interface between the dental/orthopedic implant and the bone, because the development
and preservation of viable bone opposing the biomaterial surfaces are very essential
for the success and the stability of noncemented dental/orthopedic implants
(Moimas et al., 2006).
There has been the initiation of extensive research into coatings of metallic
implants with BGs as BGs offer worthy bone bonding ability with controlled surface reactivity (Greenspan, 1999; Hench and Andersson, 1993; Ferraris et al.,
1996). It was reported earlier that a bond is formed between implanted bioceramics
and natural tissues as a result of an active biological layer that is formed on the surface of the implant by bioactive materials (Rahaman et al., 2011). In another study
performed on the human jaw bone, there was a comparison of Ti-alloy dental
implants coated with BG and HAP, and it was concluded that both materials were
nontoxic and biocompatible, and BG demonstrated good osseointegration properties, comparable to that of HAP (Mistry et al., 2011).
It is a common practice nowadays to use implants coated with BGs for achieving
good osseointegration with the alveolar bone. Using BG in dental implants as coating material shows superior bone regeneration along with better adherence to the
metal surface of the implant (Koller et al., 2007).
17.6.5 Use in toothpastes
The use of BGs in toothpaste has been increased in the last two decades. They have
been incorporated in various toothpastes because of their potential to treat dentin
hypersensitivity and to remineralize tooth structure (Abbasi et al., 2015). BGs’ first
commercial use in oral health was to treat dentin hypersensitivity, keeping in mind
that they have the capability to occlude by a HAP layer the uncovered dentinal
tubules that are the main cause of the pain and sensitivity (Burwell et al., 2009;
Dababneh et al., 1999). The BG-based dentifrice has showed superior tubule occlusion properties on dentin discs of extracted human teeth when compared with a
standard fluoride-based dentifrice, before and after a citric acid challenge, in an
in vitro SEM study (Fig. 17.1) (Farooq et al., 2015).
464
Advanced Dental Biomaterials
Figure 17.1 Scanning electron microscopy micrograph of a dentin disc that was brushed
with bioactive glass containing toothpaste, post citric acid challenge at 6000 3 , scale bar:
20 mm.
Source: Adapted from Farooq, I., Moheet, I.A., AlShwaimi, E., 2015. In vitro dentin tubule
occlusion and remineralization competence of various toothpastes. Arch. Oral. Biol. 60 (9),
1246 1253.
Lynch et al. (2012) also reported admirable capability of fluoride-containing
BGs in occluding open dentinal tubules in an in vitro study.
In recent times it has also been established that BGs can act as a remineralizing
agent (Mehta et al., 2014; Reynolds, 2008). The role of fluoride in prevention and
its application is of interest in dentistry. The addition of fluoride to BGs not only
enhances remineralization, but it also prevents demineralization of enamel and dentin (O’Donnell, 2011). Farooq et al. (2018) performed a study to analyze remineralization potential of a novel dentifrice consisting of fluoride-containing BG
(BiominF) with that of a dentifrice containing only BG (Novamin). Enamel blocks
were demineralized with citric acid and then remineralized using toothpaste slurries
(a mixture of toothpaste with artificial saliva). After 5 minutes and 24 hours, mean
enamel volume changes were evaluated by microcomputed tomography, and mean
surface loss or gain was investigated using a profilometer. It was demonstrated
through the results of this study that BiominF specimens showed better remineralization potential, especially after 5 minutes. The possible reason for the better performance of BiominF could be that it contains fluoride in its BG composition with
high PO432 content, which could serve as a source of the delivery of all essential
ions (Ca21, PO432, and F2) together to form FAP, rather than fluorite (CaF2)
(Mneimne et al., 2011). Another difference between Novamin and BiominF is the
difference between their particle size (BiominF being smaller than Novamin),
which can result in better tubule occlusion. The difference between the particle size
of these two materials is shown in Table 17.2.
Bioactive glasses—structure and applications
465
Table 17.2 Showing particle size difference between Novamin and BiominF
(http://www.biomin.co.uk/science/bioactive-glasses/biomintm-vs-novaminr).
Particle size
Novamin (µm)
BiominF (µm)
D10
D50
D90
0.177
14.47
45.55
0.62
5.92
0.62
17.6.6 Antibacterial activity
Besides remineralization, these glasses can show antibacterial activity as well by
raising the pH of an aqueous solution. It is very common to use antimicrobials in
certain dental procedures used in the fields of periodontics and endodontics (Khalid
et al., 2017). In a previous study the insertion of BG in periodontal defects has
shown inhibition of bacterial colonization due to the rise in the pH and possibly
because it provided calcium ions to the defective site (Allan et al., 2001).
17.6.7 Role in minimal invasive dentistry
BGs have a shown significant potential in minimally invasive dentistry. BG powder
can also be utilized in cutting cavities with air abrasion, causing less damage to
tooth enamel as compared to conventional cavity preparation performed by a highspeed handpiece. Alumina powder is commonly used in air abrasion machines, as it
has coarse particles (Fig. 17.2) (Hassan et al., 2017), but it is an inert material having no benefit other than quick cutting.
Alumina can be replaced with BGs, as they possess apatite-forming ability, and
also have coarse angular particles with sharp edges (Fig. 17.3) for efficient cutting.
Farooq et al. (2013) synthesized a few new, different compositions of BGs with
fluoride and reported the formation of apatite in vitro within 6 hours (which was
quicker than traditional 45S5) and with comparable cutting efficiency to that of alumina (Fig. 17.4).
17.6.8 Bioactive glass scaffolds
Tissue engineering has developed extensively in the past two decades as an
approach for the repair and regeneration of tissues and organs which are lost or
damaged due to traumatic injuries, diseases, or the aging process (Nerem, 1991).
Autografts, bone allografts, synthetic biomaterials, and metallic implants have been
reported in the literature for the rejuvenation of tissue and bony defects. The limitations of current treatments and the higher costs have encouraged interest in the
engineering of new bone substitutes. The target of scaffold-based bone tissue engineering is to repair and regenerate bony defects with minimum side effects
(Hutmacher et al., 2007). A scaffold is a porous structure which, preferably, should
direct new tissue formation by providing a matrix with interconnected porosity and
466
Advanced Dental Biomaterials
Figure 17.2 Scanning electron microscopy micrograph of alumina particles at 500 3 , scale
bar 300 μm.
Source: Adapted from Hassan, U., Farooq, I., Moheet, I.A., AlShwaimi, E., 2017. Cutting
efficiency of different dental materials utilized in an air abrasion system. Int. J. Health. Sci.
(Qassim) 11 (4), 23 27.
Figure 17.3 Scanning electron microscopy micrograph of 45S5 at 1000 3 , scale bar 100 μm.
tailored surface chemistry for the cell growth and proliferation and the transport of
nutrients and metabolic waste (Hansbrough et al., 1994). Ideally a scaffold should
mimic the bone morphologically, structurally, and functionally in order to augment
integration with its surrounding tissues (Johnson and Herschler, 2011; Karageorgiou
and Kaplan, 2005).
Bioactive glasses—structure and applications
467
Figure 17.4 FTIR spectra for a BG batch which shows formation of apatite at 6 h. BG,
Bioactive glass; FTIR, Fourier-transform infrared spectroscopy.
Source: Adapted from Farooq, I., Tylkowski, M., Müller, S., Janicki, T., Brauer, D.S., Hill,
R.G., 2013. Influence of sodium content on the properties of bioactive glasses for use in air
abrasion. Biomed. Mater. 8 (6), 065008.
BGs have etching characteristics as a scaffold material for bone tissue engineering. These glasses undergo specific reactions that lead to the formation of amorphous calcium phosphate or crystalline HAP phase on the glass surface, which
results in a stable bonding with the surrounding tissue (Jones et al., 2006). The activation of expression of osteogenic genes (Xynos et al., 2001) and stimulation of
angiogenesis have been reported by BGs (Gorustovich et al., 2009). Although the
low mechanical strength of BG scaffolds limits their usage for the repair of defects
in load-bearing bones (Yunos et al., 2008), researchers have tried to overcome this
issue by optimizing the composition, sintering conditions, and processing, and now
BG scaffolds can be created with predesigned pore architecture and with strength
comparable to human trabecular and cortical bones (Liu et al., 2011). In addition to
strength and elastic modulus other mechanical properties such as reliability and
fracture toughness are also of decisive importance for scaffolds implanted in loadbearing bone defects. As mentioned earlier, BG scaffolds can be created with the
preferred compressive strength for the restoration of load-bearing bone defects. Still
their practice in these applications may be restricted due to their intrinsic brittleness, which is also called fracture toughness. Adding a biocompatible polymer coating is suggested to improve the toughness of BG scaffolds by providing a crack
bridging mechanism through the polymer layer for energy dissipation. Regardless
of its innate brittleness, BG has numerous appealing characteristics to be used as a
scaffold material in bone tissue engineering, especially novel innovative BGs
468
Advanced Dental Biomaterials
established on borosilicate and borate compositions that have displayed the capability to develop new bone formation (Rahaman et al., 2011) with the least side
effects.
Literature reports various methods for the fabrication of BG scaffolds, which
include sol gel, freeze casting, thermal bonding of particles, polymer foam replication, fibers or spheres, and solid free-form fabrication. The capability of BG
scaffolds to support cell function and proliferation in laboratories and clinical tissue ingrowth has been publicized in many studies (Fu et al., 2010a; Goodridge
et al., 2007; Fu et al., 2010b; Zhao et al., 2008). Regardless of brittleness,
BGs have a distinctive set of properties such as formation of HAP layer, intimate
bond formation with hard tissues, and release of ions during the degradation process, which are favorable for osteogenesis, angiogenesis, and chondrogenesis
(Rahaman et al., 2011).
Prospective research is expanding on the favorable properties of BGs, considering brittleness through innovative scaffold design and processing, predominantly
when used for the repair of load-bearing bones.
17.6.9 Particle size of bioactive glasses and its effect on various
clinical applications
Before concluding this section, another key area to discuss is the importance of particle size of BGs and its impact on various clinical applications. In general, a smaller sized BG particle is preferred as it can produce better results. A few common
BG-based materials along with their particle sizes and uses are summarized in
Table 17.3.
In dentistry an increased particle size of the glass in toothpaste can cause more
abrasion of the enamel (Mahmood et al., 2014). Therefore one solution is to use
smaller sized particles in dentifrices. To comminute the glass frit, percussion milling (ball milling) is usually performed (Mahmood et al., 2014). But grinding the
particles to a smaller size (after milling) usually involves higher costs; therefore
another alternative is to reduce the abrasivity of the existing glass by incorporating
Table 17.3 Showing particle size of different bioactive glass based products used for
various clinical application.
Product
Particle size
Uses
Novamin
PerioGlas
(D50 value)
of 18 μm
90 710 μm
Biogran
300 360 μm
Used in toothpaste to treat hypersensitivity by blocking
open dentinal tubules
Used for bone regeneration around the tooth or bone repair
in the jaw for anchoring implants
Used as a bone graft in jaw defects
Source: Values adapted from Jones, J.R., 2013. Review of bioactive glass: from Hench to hybrids. Acta Biomater. 9
(1), 4457 4486.
Bioactive glasses—structure and applications
469
ions such as fluoride, which can produce a softer glass that will form FAP
(Mneimne et al., 2011).
Wilson and Low (1992) reported the effect of different sizes of 45S5 particulates
on the regeneration of bone in periodontal defects produced in a monkey model.
The study demonstrated the ideal rate of bone repair when a range of 45S5 particle
sizes were used. In another study Ajita et al. (2015) studied the effect of the size of
nanostructured BG particles on mouse mesenchymal stem cell (MSC) proliferation.
It was concluded from this study that smaller sized nano-BG particles were able to
increase proliferation of MSCs, thus implicating that they could produce desirable
results in various clinical applications.
17.7
Future of bioactive glasses
The development of composite materials combining biodegradable polymers (synthetic and natural) with nanoscale BG particles or fibers is emerging as a robust
approach toward third-generation bioactive materials. The biomedical applications
of these novel materials are bound to expand, for example, as bone filler materials, temporary orthopedic implants, as 3D biocompatible scaffolds in the field of
tissue engineering (Guarino et al., 2007), and in the dental industry for tooth remineralization, dentin regeneration, and reconstruction of bony defects. Composite
materials add strength and bioactivity through an inorganic bioactive filler while
polymers enhance flexibility and capacity to distort under loads (Boccaccini
et al., 2010). The 45S5 particulate has been used in many oral care products for
the treatment of tooth hypersensitivity as 45S5 particles stick to the dentin by
forming a HAP layer that is comparable in composition to tooth enamel, and it
blocks the dentinal tubules, thus relieving the pain for extended periods (Gillam
et al., 2002). Dental care with 45S5 is not limited to toothpaste only. Sodium
bicarbonate abrasives are used to remove stains by dentists, but the use of 45S5
through air polishing can stimulate remineralization; thus it reduces dentin hypersensitivity along with better stain removal and results in much whiter teeth
(Banerjee et al., 2010).
The use of BG, as or in a restorative material, is a debatable topic, as it is meant
to degrade in an aqueous solution (saliva in case of the oral cavity). However, a
recent study by Khvostenko et al. (2016) reported that the use of BG as filler for
resin-based composite restorations could decrease biofilm penetration into marginal
gaps of simulated tooth restorations, thus implicating that composite restorations
containing BG can reduce the development and propagation of secondary tooth
decay at the margins of the restoration.
Another potential area (related to dentistry) for the BG is their use as pits and
fissure sealant. Previously, Yang et al. (2016) reported in an in vitro study that BGcontaining sealants can inhibit the demineralization of the enamel surface within
microgaps between the material and the tooth when disclosed to a cariogenic
environment.
470
17.8
Advanced Dental Biomaterials
Conclusion
BGs make a firm bond with the host and have the ability to degrade and form apatite in physiological solutions. The easy manipulation of their composition makes
them the material of choice for extensive clinical applications. With their current
use in different medical and dental applications, an optimistic future for these
glasses can easily be anticipated.
References
Abbasi, Z., Bahrololoom, M.E., Shariat, M.H., Bagheri, R., 2015. Bioactive glasses in dentistry: a review. J. Dent. Biomater. 2 (1), 1 9.
Aguiar, H., Serra, J., González, P., León, B., 2009. Structural study of sol-gel silicate glasses
by IR and Raman spectroscopies. J. Non-Cryst. Solids 355, 475 480.
Ajita, J., Saravanan, S., Selvamurugan, N., 2015. Effect of size of bioactive glass nanoparticles on mesenchymal stem cell proliferation for dental and orthopedic applications.
Mater. Sci. Eng. C Mater. Biol. Appl. 53, 142 149.
Ali, S., Farooq, I., Iqbal, K., 2014. A review of the effect of various ions on the properties
and the clinical applications of novel bioactive glasses in medicine and dentistry. Saudi
Dent. J. 26 (1), 1 5.
Allan, I., Newman, H., Wilson, M., 2001. Antibacterial activity of particulate Bioglasss
against supra- and subgingival bacteria. Biomaterials 22 (12), 1683 1687.
Arcos, D., Ragel, C.V., Vallet-Reg, M., 2001. Bioactivity in glass/PMMA composites used
as drug delivery system. Biomaterials 22 (7), 701 708.
Baino, F., Novajra, G., Vitale-Brovarone, C., 2014. Bioceramics and scaffolds: a winning
combination for tissue engineering. Front. Bioeng. Biotechnol. 3, 202.
Banerjee, A., Hajatdoost-Sani, M., Farrell, S., Thompson, I., 2010. A clinical evaluation and
comparison of bioactive glass and sodium bicarbonate air-polishing powders. J. Dent. 38
(6), 475 479.
Benoit, M., Ispas, S., Tuckerman, M.E., 2001. Structural properties of molten silicates from
ab initio molecular-dynamics simulations: comparison between CaO-Al2O3-SiO2 and
SiO2. Phys. Rev. B 64, 224205.
Boccaccini, A.R., Erol, M., Stark, W.J., Mohn, D., Hong, Z., Mano, J.F., 2010. Polymer/bioactive glass nanocomposites for biomedical applications: a review. Compos. Sci.
Technol. 70 (13), 1764 1776.
Brauer, D.S., 2015. Bioactive glasses—structure and properties. Angew. Chem. Int. Ed. Engl.
54 (14), 4160 4181.
Brauer, D.S., Karpukhina, N., O’Donnell, M.D., Law, R.V., Hill, R.G., 2010. Fluoridecontaining bioactive glasses: effect of glass design and structure on degradation, pH and
apatite formation in simulated body fluid. Acta Biomater. 6 (8), 3275 3282.
Brink, M., 1997. The influence of alkali and alkaline earths on the working range for bioactive glasses. J. Biomed. Mater. Res. 36, 109 117.
Brown, R.F., Rahaman, M.N., Dwilewicz, A.B., et al., 2009. Effect of borate glass composition on its conversion to hydroxyapatite and on the proliferation of MC3T3-E1cells.
J. Biomed. Mater. Res. A 88 (2), 392 400.
Bioactive glasses—structure and applications
471
Burwell, A.K., Litkowski, L.J., Greenspan, D.C., 2009. Calcium sodium phosphosilicate
(NovaMins): remineralization potential. Adv. Dent. Res. 21 (1), 35 39.
Chen, Q.Z., Li, Y., Jin, L.Y., Quinn, J.M., Komesaroff, P.A., 2010. A new sol-gel process for
producing Na(2)O-containing bioactive glass ceramics. Acta Biomater. 6 (10),
4143 4153.
Cheng, Y., Xiao, H., Shuguang, C., Tang, B., 2009. Structure and crystallization of B2O3Al2O3-SiO2 glasses. Physica B: Condens. Matter 404, 1230 1234.
Cho, J.S., Kang, Y.C., 2009. Synthesis of spherical shape borate-based bioactive glass powders prepared by ultrasonic spray pyrolysis. Ceram. Int. 35, 2103 2109.
Dababneh, R.H., Khouri, A.T., Addy, M., 1999. Dentine hypersensitivity—an enigma? A review
of terminology, mechanisms, aetiology and management. Br. Dent. J. 187 (11), 606 611.
Diba, M., Tapia, F., Boccaccini, A.R., Stro, L.A., 2012. Magnesium-containing bioactive
glasses for biomedical applications. Int. J. Appl. Glass Sci. 3, 221 253.
Dietzel, A., 1941. Structural chemistry of glasses. Naturwissenschaften 29, 537 547.
Dimarzio, E.A., Gibbs, J.H., 1959. Glass temperature of copolymers. J. Polym. Sci. 40 (136),
121 131.
Domingues, Z.R., Cortés, M.E., Gomes, T.A., et al., 2004. Bioactive glass as a drug delivery
system of tetracycline and tetracycline associated with β-cyclodextrin. Biomaterials 25
(2), 327 333.
Dudowicz, J., Freed, K.F., Douglas, J.F., 2005. The glass transition temperature of polymer
melts. J. Phys. Chem. B 109 (45), 21285 21292.
Elshahat, A.H., 2006. Correction of craniofacial skeleton contour defects using bioactive
glass particles. Egypt J. Plast. Reconstr. Surg. 30 (2), 113 119.
Farooq, I., Imran, Z., Farooq, U., Leghari, A., Ali, H., 2012. Bioactive glass: a material for
the future. World J. Dent. 3 (2), 199 201.
Farooq, I., Tylkowski, M., Müller, S., Janicki, T., Brauer, D.S., Hill, R.G., 2013. Influence of
sodium content on the properties of bioactive glasses for use in air abrasion. Biomed.
Mater. 8 (6), 065008.
Farooq, I., Moheet, I.A., AlShwaimi, E., 2015. In vitro dentin tubule occlusion and remineralization competence of various toothpastes. Arch. Oral. Biol. 60 (9), 1246 1253.
Farooq, I., Majeed, A., AlShwaimi, E., Almas, K., 2018. Efficacy of a novel fluoride containing bioactive glass based dentifrice in remineralizing artificially induced demineralization in human enamel. Fluoride (in press).
Fathi, M.H., Salehi, M.A., Saatchi, A., Mortazavi, V., Moosavi, S.B., 2003. In vitro corrosion
behavior of bioceramic, metallic, and bioceramic metallic coated stainless steel dental
implants. Dent. Mater. 19 (3), 188 198.
Featherstone, J.D., 2000. The science and practice of caries prevention. J. Am. Dent. Assoc.
131 (7), 887 899.
Felipe, M.E., Andrade, P.F., Novaes, A.B., Grisi, M.F., Souza, S.L., Taba, M., et al., 2009.
Potential of bioactive glass particles of different size ranges to affect bone formation in
interproximal periodontal defects in dogs. J. Periodontol. 80 (5), 808 815.
Ferraris, M., Rabajoli, P., Paracchini, L., Brossa, F., 1996. Vacuum plasma spray deposition
of titanium particle/glass-ceramic matrix biocomposites. J. Am. Ceram. Soc. 79 (6),
1515 1520.
Fetner, A.E., Hartigan, M.S., Low, S.B., 1994. Periodontal repair using PerioGlas in nonhuman primates: clinical and histologic observations. Compendium 15 (7), 932 935.
Fu, Q., Rahaman, M.N., Bal, B.S., Huang, W., Day, D.E., 2007. Preparation and bioactive
characteristics of a porous 13-93 glass, and fabrication into the articulating surface of a
proximal tibia. J. Biomed. Mater. Res. A 82, 222 229.
472
Advanced Dental Biomaterials
Fu, Q., Rahaman, M.N., Fu, H., Liu, X., 2010a. Silicate, borosilicate, and borate bioactive
glass scaffolds with controllable degradation rate for bone tissue engineering applications. J. Biomed. Mater. Res. A 95 (1), 164 171.
Fu, Q., Rahaman, M.N., Bal, B.S., Kuroki, K., Brown, R.F., 2010b. In vivo evaluation of 1393 bioactive glass scaffolds with trabecular and oriented microstructures in a subcutaneous rat implantation model. J. Biomed. Mater. Res. A 95 (1), 235 244.
Fuchs, M., Gentleman, E., Shahid, S., Hill, R., Brauer, D., 2015. Therapeutic ion-releasing
bioactive glass ionomer cements with improved mechanical strength and radiopacity.
Front. Mater. 2, 63.
Garcia, C., Cere, S., Duran, A., 2004. Bioactive coatings prepared by sol gel on stainless
steel 316L. J. Non-Cryst. Solids 348, 218 224.
Gerhardt, L.C., Boccaccini, A.R., 2010. Bioactive glass and glass-ceramic scaffolds for bone
tissue engineering. Materials (Basel) 3 (7), 3867 3910.
Gillam, D., Tang, J., Mordan, N., Newman, H., 2002. The effects of a novel bioglass dentifrice on dentine sensitivity: a scanning electron microscopy investigation. J. Oral
Rehabil. 29 (4), 305 313.
González, P., Serra, J., Liste, S., Chiussi, S., León, B., Pérez-Amor, M., et al., 2003. New
biomorphic SiC ceramics coated with bioactive glass for biomedical applications.
Biomaterials 24, 4827 4832.
Goodridge, R.D., Woodm, D.J., Ohtsuki, C., Dalgarno, K.W., 2007. Biological evaluation of
an apatite mullite glass-ceramic produced via selective laser sintering. Acta Biomater.
3 (2), 221 231.
Gorustovich, A.A., Roether, J.A., Boccaccini, A.R., 2009. Effect of bioactive glasses on
angiogenesis: a review of in vitro and in vivo evidences. Tissue Eng. Part B Rev. 16 (2),
199 207.
Greenspan, D.C., 1999. Bioactive glass: mechanisms of bone bonding. Tandlakartidningen
91, 31 35.
Guarino, V., Causa, F., Ambrosio, L., 2007. Bioactive scaffolds for bone and ligament tissue.
Expert Rev. Med. Devices 4 (3), 405 418.
Gubler, M., Brunner, T.J., Zehnder, M., Waltimo, T., Sener, B., Stark, W.J., 2008. Do bioactive glasses convey a disinfecting mechanism beyond a mere increase in pH? Int.
Endod. J. 41 (8), 670 678.
Hansbrough, J.F., Morgan, J., Greenleaf, G., Parikh, M., Nolte, C., Wilkins, L., 1994.
Evaluation of Graftskin composite grafts on full-thickness wounds on athymic mice. J.
Burn Care Rehabil. 15 (4), 346 353.
Hassan, U., Farooq, I., Moheet, I.A., AlShwaimi, E., 2017. Cutting efficiency of different
dental materials utilized in an air abrasion system. Int. J. Health Sci. (Qassim) 11 (4),
23 27.
Heikkilä, J.T., Aho, H.J., Yli-Urpo, A., Happonen, R.P., Aho, A.J., 1995. Bone formation in
rabbit cancellous bone defects filled with bioactive glass granules. Acta Orthop. Scand.
66 (5), 463 467.
Hench, L.L., 1991. Bioceramics: from concept to clinic. J. Am. Ceram. Soc. 74, 1487 1510.
Hench, L.L., 1998. Biomaterials: a forecast for the future. Biomaterials 19, 1419 1423.
Hench, L.L., 2006. The story of Bioglasss. J. Mater. Sci. Mater. Med. 17, 967 978.
Hench, L.L., 2013. Chronology of bioactive glass development and clinical applications.
New J. Glass Ceram. 3 (2), 67 73.
Hench, L.L., Andersson, O.H., 1993. An introduction to bioceramics. In: Hench, L.L.,
Wilson, J. (Eds.), Advanced Series in Ceramics., 1. Scientific Publishing Co Ltd,
Singapore, pp. 41 46.
Bioactive glasses—structure and applications
473
Hench, L.L., Jones, J.R., 2015. Bioactive glasses: frontiers and challenges. Front. Bioeng.
Biotechnol. 3, 194.
Hill, R.G., 1996. An alternative view of degradation of Bioglasss. J. Mater. Sci. Lett. 15,
1122 1125.
Hill, R.G., Brauer, D.S., 2011. Predicting the bioactivity of glasses using the network connectivity or split network models. J. Non-Cryst. Solids 357, 3884 3887.
Hoppe, A., Güldal, N.S., Boccaccini, A.R., 2011. A review of the biological response to ionic
dissolution products from bioactive glasses and glass-ceramics. Biomaterials 32 (11),
2757 2774. Available from: http://www.biomin.co.uk/science/bioactive-glasses/biomintm-vs-novaminr (accessed 02.02.18.).
Huang, W., Rahaman, M.N., Day, D.E., Li, Y., 2006a. Mechanisms for converting bioactive
silicate, borate, and borosilicate glasses to hydroxyapatite in dilute phosphate solution.
Phys. Chem. Glasses 47, 647 658.
Huang, W., Day, D.E., Kittiratanapiboon, K., et al., 2006b. Kinetics and mechanisms of the
conversion of silicate (45S5), borate, and borosilicate glasses to hydroxyapatite in dilute
phosphate solutions. J. Mater. Sci. Mater. Med. 17, 583 596.
Hutmacher, D.W., Schantz, J.T., Lam, C.X.F., Tan, K.C., Lim, T.C., 2007. State of the art
and future directions of scaffold-based bone engineering from a biomaterials perspective. J. Tissue Eng. Regen. Med. 1 (4), 245 260.
Jia, W.T., Zhang, X., Luo, S.H., et al., 2010. Novel borate glass/chitosan composite as a
delivery vehicle for teicoplanin in the treatment of chronic osteomyelitis. Acta
Biomater. 6 (3), 812 819.
Johnson, A.J.W., Herschler, B.A., 2011. A review of the mechanical behavior of CaP and
CaP/polymer composites for applications in bone replacement and repair. Acta
Biomater. 7 (1), 16 30.
Jones, J.R., 2013. Review of bioactive glass: from hench to hybrids. Acta Biomater. 9 (1),
4457 4486.
Jones, J.R., Ehrenfried, L.M., Hench, L.L., 2006. Optimising bioactive glass scaffolds for
bone tissue engineering. Biomaterials 27 (7), 964 973.
Kanzaki, N., Onuma, K., Treboux, G., Tsutsumi, S., Ito, A., 2000. Inhibitory effect of magnesium and zinc on crystallization kinetics of hydroxyapatite (0001) face. J. Phys. Chem.
B 104, 4189 4194.
Karageorgiou, V., Kaplan, D., 2005. Porosity of 3D biomaterial scaffolds and osteogenesis.
Biomaterials 26 (27), 5474 5491.
Kaur, G., Pandey, O.P., Singh, K., Homa, D., Scott, B., Pickrell, G., 2014. A review of bioactive glasses: their structure, properties, fabrication and apatite formation. J. Biomed.
Mater. Res. A 102, 254 274.
Kawanabe, K., Okada, Y., Matsusue, Y., Iida, H., Nakamura, T., 1998. Treatment of osteomyelitis with antibiotic-soaked porous glass ceramic. J. Bone Joint Surg. Br. 80 (3), 527 530.
Khalid, M.D., Khurshid, Z., Zafar, M.S., et al., 2017. Bioactive glasses and their applications
in dentistry. J. Pak. Dent. Assoc. 26 (1), 32 38.
Khvostenko, D., Hilton, T.J., Ferracane, J.L., Mitchell, J.C., Kruzic, J.J., 2016. Bioactive
glass fillers reduce bacterial penetration into marginal gaps for composite restorations.
Dent. Mater. 32 (1), 73 81.
Kobayashi, M., Saito, H., Mase, T., et al., 2010. Polarization of hybridized calcium phosphoaluminosilicates with 45S5-type bioglasses. Biomed. Mater. 5 (2), 25001.
Koller, G., Cook, R.J., Thompson, I.D., Watson, T.F., Di-Silvio, L., 2007. Surface modification of titanium implants using bioactive glasses with air abrasion technologies. J.
Mater. Sci. Mater. Med. 18 (12), 2291 2296.
474
Advanced Dental Biomaterials
Kundu, B., Nandi, S.K., Dasgupta, S., et al., 2011. Macro-to-micro porous special bioactive
glass and ceftriaxone sulbactam composite drug delivery system for treatment of
chronic osteomyelitis: an investigation through in vitro and in vivo animal trial. J.
Mater. Sci. Mater. Med. 22 (3), 705 720.
Kwakye-Awuah, B., Williams, C., Kenward, M.A., Radecka, I., 2008. Antimicrobial action
and efficiency of silver-loaded zeolite X. J. Appl. Microbiol. 104 (5), 1516 1524.
Lai, W., Garino, J., Ducheyne, P., 2002. Silicon excretion from bioactive glass implanted in
rabbit bone. Biomaterials 23, 213 217.
Liu, X., Xie, Z., Zhang, C., Pan, H., Rahaman, M.N., Zhang, X., et al., 2010. Bioactive
borate glass scaffolds: in vitro and in vivo evaluation for use as a drug delivery system
in the treatment of bone infection. J. Mater. Sci. Mater. Med. 21 (2), 575 582.
Liu, X., Rahaman, M.N., Fu, Q., 2011. Oriented bioactive glass (13-93) scaffolds with controllable pore size by unidirectional freezing of camphene-based suspensions: microstructure and mechanical response. Acta Biomater. 7 (1), 406 416.
Lynch, E., Brauer, D.S., Karpukhina, N., Gillam, D.G., Hill, R.G., 2012. Multi-component
bioactive glasses of varying fluoride content for treating dentin hypersensitivity. Dent.
Mater. 28 (2), 168 178.
Macedo, N.L.D., Matuda Fda, S., Macedo, L.G., et al., 2004. Bone defect regeneration with
bioactive glass implantation in rats. J. Appl. Oral Sci. 12, 137 143.
Mahmood, A., Mneimne, M., Zou, L.F., Hill, R.G., Gillam, D.G., 2014. Abrasive wear of
enamel by bioactive glass-based toothpastes. Am. J. Dent. 27 (5), 263 267.
Mehta, A.B., Kumari, V., Jose, R., Izadikhah, V., 2014. Remineralization potential of bioactive glass and casein phosphopeptide-amorphous calcium phosphate on initial carious
lesion: an in-vitro pH-cycling study. J. Conserv. Dent. 17 (1), 3 7.
Mercier, C., Follet-Houttemane, C., Pardini, A., Revel, B., 2011. Influence of P2O5 content
on the structure of SiO2-Na2O-CaO-P2O5 bioglasses by 29Si and 31P MAS-NMR. J.
Non-Cryst. Solids 357, 3901 3909.
Meseguer-Olmo, L., Ros-Nicolás, M.J., Vicente-Ortega, V., et al., 2006. A bioactive sol-gel
glass implant for in vivo gentamicin release. Experimental model in rabbit. J. Orthop.
Res. 24 (3), 454 460.
Mistry, S., Kundu, D., Datta, S., Basu, D., 2011. Comparison of bioactive glass coated and
hydroxyapatite coated titanium dental implants in the human jaw bone. Aust. Dent. J. 56
(1), 68 75.
Mneimne, M., Hill, R.G., Bushby, A.J., Brauer, D.S., 2011. High phosphate content significantly increases apatite formation of fluoride-containing bioactive glasses. Acta
Biomater. 7 (4), 1827 1834.
Moimas, L., Biasotto, M., Di-Lenarda, R., Olivo, A., Schmid, C., 2006. Rabbit pilot study on
the resorbability of three-dimensional bioactive glass fibre scaffolds. Acta Biomater. 2
(2), 191 199.
Najeeb, S., Khurshid, Z., Matinlinna, J.P., et al., 2015. Nanomodified peek dental implants:
bioactive composites and surface modification—a review. Int. J. Dent. 2015, 381759.
Najeeb, S., Zafar, M.S., Khurshid, Z., et al., 2017. Bisphosphonate releasing dental implant
surface coatings and osseointegration: a systematic review. J. Taibah Univ. Med. Sci. 12
(5), 369 375.
Nejatain, T., Khurshid, Z., Zafar, M.S., et al., 2017. Dental biocomposites. Biomaterials for
Oral and Dental Tissue Engineering. Woodhead Publishing, pp. 65 84.
Nerem, R.M., 1991. Cellular engineering. Ann. Biomed. Eng. 19 (5), 529 545.
Newby, P.J., El-Gendy, R., Kirkham, J., Yang, X.B., Thompson, I.D., Boccaccini, A.R.,
2011. Ag-doped 45S5 Bioglasss-based bone scaffolds by molten salt ion exchange:
processing and characterisation. J. Mater. Sci. Mater. Med. 22 (3), 557 569.
Bioactive glasses—structure and applications
475
O’Donnell, M.D., 2011. Predicting bioactive glass properties from the molecular chemical
composition: glass transition temperature. Acta Biomater. 7, 2264 2269.
O’Donnell, M.D., 2012. Melt-derived bioactive glass. In: Jones, J.R., Clare, A.G. (Eds.), BioGlasses. Wiley, Chichester, UK, pp. 13 28.
O’Donnell, M.D., Watts, S.J., Hill, R.G., Law, R.V., 2009. The effect of phosphate content
on the bioactivity of soda-lime-phosphosilicate glasses. J. Mater. Sci. Mater. Med. 20
(8), 1611 1618.
Oonishi, H., Kushitani, S., Yasukawa, E., Iwaki, H., Hench, L.L., Wilson, J., et al., 1997.
Particulate Bioglasss compared with hydroxyapatite as a bone graft substitute. Clin.
Orthop. Relat. Res. 334, 316 325.
Oonishi, H., Hench, L.L., Wilson, J., et al., 2000. Quantitative comparison of bone growth
behavior in granules of Bioglasss, A-W glass-ceramic, and hydroxyapatite. J. Biomed.
Mater. Res. 51 (1), 37 46.
Paolinelis, G., Banerjee, A., Watson, T.F., 2008. An in vitro investigation of the effect and
retention of bioactive glass air-abrasive on sound and carious dentine. J. Dent. 36 (3),
214 218.
Peitl, O., Dutra, E., Hench, L.L., 2001. Highly bioactive P2O5 6 Na2O 6 CaO 6 SiO2 glassceramics. J. Non-Cryst. Solids 292, 115 126.
Rahaman, M.N., Day, D.E., Sonny, B.B., et al., 2011. Bioactive glass in tissue engineering.
Acta Biomater. 7, 2355 2373.
Rao, M.C., Ravindranadh, K., 2016. Bioactive glasses for technological and clinical applications. Int. J. Chem. Sci. 14 (3), 1339 1348.
Reynolds, E.C., 2008. Calcium phosphate-based remineralization systems: scientific evidence? Aust. Dent. J. 53 (3), 268 273.
Roessler, S., Zimmermann, R., Scharnweber, D., Werner, C., Worch, H., 2002.
Characterization of oxide layers on Ti6Al4V and titanium by streaming potential and
streaming current measurements. Colloids Surf., B: Biointerfaces 26 (4), 387 395.
Sen, S., Youngman, R.E., 2003. NMR study of Q-speciation and connectivity in K2O SiO2
glasses with high silica content. J. Non-Cryst. Solids 331, 100 107.
Serra, J., González, P., Liste, S., Chiussi, S., León, B., Pérez-Amor, M., et al., 2002.
Influence of the non-bridging oxygen groups on the bioactivity of silicate glasses.
J. Mater. Sci. Mater. Med. 13, 1221 1225.
Serra, J., González, P., Liste, S., Serra, C., Chiussi, S., León, B., et al., 2003. FTIR and XPS
studies of bioactive silica based glasses. J. Non-Cryst. Solids 332, 20 27.
Srivastava, A.K., Pyare, R., Singh, S.P., 2012. In vitro bioactivity and physical—mechanical
properties of Fe2O3 substituted 45S5 bioactive glasses and glass—ceramics. Int. J. Sci.
Eng. Res. 3 (2), 1 15.
Stanley, H.R., Clark, A.E., Pameijer, C.H., Louw, N.P., 2001. Pulp capping with a modified
Bioglasss formula (# A68-modified). Am. J. Dent. 14 (4), 227 232.
Stoor, P., Apajalahti, S., Kontio, R., 2017. Regeneration of cystic bone cavities and bone
defects with bioactive glass S53P4 in the upper and lower jaws. J. Craniofac. Surg. 28
(5), 1197 1205.
Tahriri, M., Bader, R., Yao, W., Dehghani, S., Khoshroo, K., et al., 2017. Bioactive glasses
and calcium phosphates. Biomaterials for Oral and Dental Tissue Engineering.
Woodhead Publishing, pp. 7 24.
Toosi, S., Behravan, J., 2017. An update on bioactive glass in bone tissue engineering.
Bioceram. Dev. Appl. 7, e111.
Van-Gestel, N.A., Geurts, J., Hulsen, D.J., Van-Rietbergen, B., Hofmann, S., Arts, J.J., 2015.
Clinical applications of S53P4 bioactive glass in bone healing and osteomyelitic treatment: a literature review. Biomed. Res. Int. 2015, 684826.
476
Advanced Dental Biomaterials
Vichery, C., Nedelec, J.-M., 2016. Bioactive glass nanoparticles: from synthesis to materials
design for biomedical applications. Materials (Basel) 9 (4), 288.
Wallace, K.E., Hill, R.G., Pembroke, J.T., Brown, C.J., Hatton, P.V., 1999. Influence of
sodium oxide content on bioactive glass properties. J. Mater. Sci. Mater. Med. 10 (12),
697 701.
Wang, W., Yeung, K.W.K., 2017. Bone grafts and biomaterials substitutes for bone defect
repair: a review. Bioact. Mater. 2 (4), 224 247.
Wilson, J., Low, S.B., 1992. Bioactive ceramics for periodontal treatment: comparative studies in the patus monkey. J. Appl. Biomater. 3 (2), 123 129.
Wilson, J., Clark, A.E., Hall, M., et al., 1993. Tissue response to Bioglasss endosseous ridge
maintenance implants. J. Oral. Implantol. 19, 295 302.
Xynos, I.D., Hukkanen, M.V., Batten, J.J., Buttery, L.D., Hench, L.L., Polak, J.M., 2000.
Bioglasss 45S5 stimulates osteoblast turnover and enhances bone formation in vitro:
implications and applications for bone tissue engineering. Calcif. Tissue Int. 67 (4),
321 329.
Xynos, I.D., Edgar, A.J., Buttery, L.D., Hench, L.L., Polak, J.M., 2001. Gene-expression profiling of human osteoblasts following treatment with the ionic products of Bioglasss
45S5 dissolution. J. Biomed. Mater. Res. A 55 (2), 151 157.
Yang, S.Y., Kwon, J.S., Kim, K.N., Kim, K.M., 2016. Enamel surface with pit and fissure
sealant containing 45S5 bioactive glass. J. Dent. Res. 95 (5), 550 557.
Yang, X., Zhang, L., Chen, X., Sun, X., Yang, G., et al., 2012. Incorporation of B2O3 in
CaO-SiO2-P2O5 bioactive glass system for improving strength of low-temperature
co-fired porous glass ceramics. J. Non-Cryst. Solids 358, 1171 1179.
Yao, A., Wang, D., Huang, W., Fu, Q., Rahaman, M.N., Day, D.E., 2007. In vitro bioactive
characteristics of borate-based glasses with controllable degradation behavior. J. Am.
Ceram. Soc. 90, 303 306.
Yunos, D.M., Bretcanu, O., Boccaccini, A.R., 2008. Polymer-bioceramic composites for tissue engineering scaffolds. J. Mater. Sci. 43 (13), 4433.
Zadpoor, A.A., 2014. Relationship between in vitro apatite-forming ability measured using
simulated body fluid and in vivo bioactivity of biomaterials. Mater. Sci. Eng. C 35,
134 143.
Zhang, X., Jia, W., Gu, Y., et al., 2010. Teicoplanin-loaded borate bioactive glass implants
for treating chronic bone infection in a rabbit tibia osteomyelitis model. Biomaterials 31
(22), 5865 5874.
Zhao, D., Moritz, N., Vedel, E., Hupa, L., Aro, H.T., 2008. Mechanical verification of softtissue attachment on bioactive glasses and titanium implants. Acta Biomater. 4 (4),
1118 1122.
Further reading
Hench, L.L., 1981. Bioceramics. J. Am. Ceram. Soc. 81 (7), 1705 1728.
Owens, G.J., Singh, R.K., Forouton, F., et al., 2016. Sol gel based materials for biomedical
applications. Prog. Mater. Sci. 77, 1 79.
Nanotechnology and
nanomaterials in dentistry
18
Muhammad S. Zafar1,2, Ahmad A. Alnazzawi3, Mothanna Alrahabi1,
Muhammad A. Fareed4, Shariq Najeeb5 and Zohaib Khurshid6
1
Department of Restorative Dentistry, College of Dentistry, Taibah University, Medina,
Saudi Arabia, 2Department of Dental Materials, Islamic International Dental College,
Riphah International University, Islamabad, Pakistan, 3Department of Substitutive Dental
Sciences, College of Dentistry, Taibah University, Medina, Saudi Arabia, 4Adult
Restorative Dentistry, Dental Biomaterials and Prosthodontics Oman Dental College,
Muscat, Sultanate of Oman, 5National Center for Proteomics, University of Karachi,
Pakistan, 6Department of Prosthodontics and Dental Implantology, College of Dentistry,
King Faisal University, Al-Ahsa, Saudi Arabia
Chapter Outline
18.1
18.2
18.3
18.4
Introduction 477
Natural biomaterials and nanoscience 478
General properties of nanomaterials 480
Dental applications of nanobiomaterials 481
18.4.1
18.4.2
18.4.3
18.4.4
18.4.5
18.4.6
18.4.7
18.4.8
Nanobiomaterials for preventive dentistry 482
Nanomaterials for periodontics 483
Nanomaterials for dental implants 484
Restorative nanobiomaterials 486
Endodontic nanobiomaterials 488
Nanomaterials and endodontic regeneration 490
Nanomaterials and tissue engineering 490
Electrospun nanomaterials 491
18.5 Potential of nanomaterials
18.6 Conclusive remarks 494
References 494
18.1
492
Introduction
In the last few decades, clinical applications of nanotechnology and nanomaterials
have expanded in biomedical and dental care. Plenty of research has been conducted to investigate the excellent properties of various nanoscale biomaterials
including carbon-based nanoparticles; nanoceramics (Najeeb et al., 2016a; Elgendy and
Abo Shady, 2015; Vallet-Regı́ and Arcos, 2008), graphene oxide (Sun et al., 2008;
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00018-9
Copyright © 2019 Elsevier Ltd. All rights reserved.
478
Advanced Dental Biomaterials
Gahlot et al., 2014; Rodrı́guez-Lozano et al., 2014), carbon nanotubes (Silva et al.,
2014; Kang et al., 2009; Kostarelos et al., 2009), nanodiamonds (Gismondi et al., 2015;
Passeri et al., 2015; Setyawati et al., 2015; Huynh et al., 2013; Najeeb et al., 2016d),
and nanofibers (Zafar et al., 2015a,b, 2016; Kim et al., 2014a,b; Zafar and
Al-Samadani, 2014) for potential biodental applications. The word “nano” is a Greek
word that means dwarf. In the metric system, one billionth of 1 m is called a nanometer
(nm) (1 nm 5 1029 m) (Sheeparamatti et al., 2007). A nanomaterial has at least one
dimension in the range of 1 100 nm and demonstrates size dependent characteristic
properties (Gouma, 2009). Nanotechnology deals with the engineering of nanomaterials
(scale range of 1 100 nm) and miniaturized devices based on nanomaterials.
Nanodentistry is the use of nanomaterials and nanotechnology applications for diagnosis,
prevention, and treatment of oral and dental diseases (Hieber and Müller, 2012).
The concept of nanotechnology was introduced by Richard Feynman while presenting his conceptual theory “There’s Plenty of Room at the Bottom” at the
California Institute of Technology that was later published in “Engineering and
Science” (Feynman, 1960). However, the actual term “Nanotechnology or
Nanosciences” was described by Prof. Norio Taniguchi (Tokyo Science University)
for the first time in 1974 (Taniguchi, 1974). In the early 1980s, physicists achieved
major developments in the field of scanning microscopy enabling image analysis at an
atomic/molecular level, advancing the science of nanotechnology. Nanotechnology
engages the fabrication and characterization of materials at molecular levels and
purposeful engineering on a nanoscale ( . 100 nm) (Zhang et al., 2005). Natural
and synthetic materials at various scales are compared in Fig. 18.1.
The physical, chemical, mechanical, and biological properties of materials at an
individual molecular level may differ compared to their bulk properties at the nanoscale (Lieber, 1998). Nanomaterials characterization means the use of different
techniques and methods to probe materials structures and properties. Regarding
nanomaterials characterization, a variety of techniques are used to assess the structure and properties of existing and developing nanomaterials (Fig. 18.2).
Nanobiomaterials have been explored for all types of biomaterials (metals, polymers, ceramics, and composites) for clinical applications. Due to favorable features
and promising outcomes, nanomaterials have attracted researchers and biomaterials
scientist looking to provide benefits for biomedical and dental applications
(Moszner and Klapdohr, 2004). Therefore, the aim of this chapter is to discuss the
current and potential dental applications of nanobiomaterials, recent innovations,
and future expectations.
18.2
Natural biomaterials and nanoscience
Natural biomaterials such as bone, teeth, shells, and wood are composed of nanoscale components (Hussain et al., 2006), having great performance and structural/
functional relationships. Nature has taught us a lot of lessons as the majority of
natural biomaterials are synthesized in the biological environment and conditions
(Broderick et al., 2007). In addition, a range of hierarchical levels (ranging from
Nanotechnology and nanomaterials in dentistry
479
Figure 18.1 Comparison of natural and synthetic materials at various metric scales.
the macro- to microscale) and nanometer-sized inorganic materials are implanted
into the soft organic matrix (Mano and Reis, 2005). The formation of nanomaterials
in nature takes place in ambient conditions of the surrounding environment
480
Advanced Dental Biomaterials
Nanomaterials' characterization
Morphology
Surface
Topography
Particle size
Porosity
Surface area
Scanning tunnel
microscope (STM)
Atomic force
microscope (AFM)
Transmission electron
microscope (TEM)
Scanning electron
microscope (SEM)
Dynamic light
scattering (DLS)
Gas adsorption
Scanning probe
microscope
Small angle X-ray
scattering (SAXS)
Crystallography
Crystallinity
and defects
Grain size
X-ray diffraction (XRD)
Electron
crystallography
Wide-angle X-ray
scattering
Scanning electron
microscope (SEM)
Chemical structure
Elements
Molecules
Chemistry
Chemical bond
Concentration
Energy-dispersive X-ray
spectroscopy (EDX)
Neutron diffraction
Mass Spectroscopy
Infra-red spectroscopy
(FTIR)
UV–Vis spectroscopy
Scanning electron
microscope (SEM)
Thermal properties
Thermal conductivity
Melting point
Thermal stability
Glass transition
Thermogravimetric
analysis (TGA)
Differential scanning
calorimetry (DSC)
Thermomechanical
analysis (TMA)
Dynamic mechanical
analysis (DMA)
Mechanical properties
Strength
Hardness
Modulus
Wear
Viscoelastic
behavior
AFM
Nanoindentation
Mechanical tester
Dynamic mechanical
analysis (DMA)
Figure 18.2 Commonly used techniques for the characterization of nanomaterials.
(Broderick et al., 2007); for instance, the formation of enamel hydroxyapatite (HA)
is a matter of simple dissolution precipitation during amelogenesis (LeGeros,
1991). In contrast, the formation of the same product in the laboratory requires calcium fluoride and high temperature (900 C 1100 C) (Emsley, 1976). Moreover,
mineralized body tissues are primarily nanocomposites composed of inorganic/
organic components in order to tailor the tissue properties from one tissue to the
other (Low et al., 2008). The inorganic component HA comprises the major part of
enamel, dentin, cementum, and bone. HA crystalizes in a hexagonal shape (Jones,
2001) with its chemistry known for more than 85 years (Naray-Szabo, 1930).
However, the morphology and structure varies among biological tissues (Summit
et al., 2000; Nanci, 2008; Ten Cate, 1994). For instance, HA crystals in tooth
enamel are remarkably larger (45 90 nm 3 25 39 nm 3 2 3 nm) than in dentin
(3.5 nm 3 20 nm 3 20 nm) (Summit et al., 2000).
18.3
General properties of nanomaterials
Nanomaterials are expected to exhibit novel and significantly better physical, chemical,
and biological properties (Kelsall et al., 2005). The properties of nanomaterials may
vary based on multiple factors such as the materials’ type (metal, ceramic, polymer,
or composites) and morphological structure. However, certain properties and materials
characteristics are expected from nanomaterials. The detailed discussion of these
Nanotechnology and nanomaterials in dentistry
481
Table 18.1 Classification of nanomaterials.
Classification
A—Based on
morphology
B—Based on
materials chemistry
Nanoclusters
Nanofibers
Nanowire/tubes
Nanoparticles
Carbon-based
nanomaterials
Polymer nanomaterials
Metallic nanomaterials
Nanoceramics
Nanocomposites
C—Based on
dimensions
Zero-dimensional
One-dimensional
Two-dimensional
Three-dimensional
Examples
Electrospun polymers/silk
Carbon-based nanomaterials
Silica, HA, gold, silver
Fullerenes nanotubes
Electrospun silk nanofibers
Nanogold and nanosilver
Silica, titanium oxide, and HA
nanoparticles
Ceramic/polymer nanocomposites
silica/resin nanocomposites
Nanoclusters
Nanowires and nanotubes
Nanolayer/films coatings
Tissue engineering scaffolds
polymers and/or composites
HA, Hydroxyapatite.
properties is beyond the scope of this book; but a few main features of nanoscale materials are enumerated here:
G
G
G
G
G
G
At nanoscale, greater surface area the surface functionalities.
High surface area facilitates better mechanical interlocking of nanoparticles to the polymer matrix (Arcı́s et al., 2002).
Inorganic ceramic nanoparticles are brittle and hard and can reinforce to provide superior
mechanical properties (Mota et al., 2006).
The areas of stress concentration are reduced, resulting in improved resistance to the crack
propagation and higher fatigue strength (Turssi et al., 2005).
Optical properties (translucency) and surface finish are improved while using nano-sized
fillers (Mota et al., 2006).
The biodegradability and biodegradation rates can be better controlled compared to conventional composite materials (Ray and Okamoto, 2003; Mohanty et al., 2003).
The various types of nanomaterials can be categorized based on their chemistry,
morphology, and dimensional existence (Table 18.1).
18.4
Dental applications of nanobiomaterials
Nanobiomaterials have been extensively explored for various dental applications
(Najeeb et al., 2016; Zafar et al., 2017; Khurshid et al., 2015), covering almost all
dental specialties (Fig. 18.3). The following describes the key nanomaterials being
used in various disciplines of dentistry.
482
Advanced Dental Biomaterials
Figure 18.3 Applications of nanomaterials in various disciplines of dentistry.
18.4.1 Nanobiomaterials for preventive dentistry
“Prevention is better than cure.” Teeth perform in the dynamic environment of the
oral cavity where the prevention of tooth decay is very challenging. Due to all the
advancements and the better understanding of oral diseases, the role of preventive
dentistry is still vital and cannot be denied. Nanomaterials are used for preventive
dental care, for the management of biofilm at the tooth surface using nanoapatites,
and for the demineralization of early stage submicron-sized enamel lesions (Hannig
and Hannig, 2010).
18.4.1.1 Preventive nanocomposites surface coatings
The nanocomposites surface coatings are prepared by the incorporation of inorganic
nanoparticles in fluoropolymer matrix (Hannig et al., 2007). These materials play
beneficial roles by detaching the pellicle and bacterial plaque under the effect of
physiological activities in the oral cavity and decreasing the surface energy to
inhibit biofilm attachment to the tooth structure. Key benefits include the following
(Hannig et al., 2007):
G
G
G
G
Modification of tooth surface.
Easy to clean when used as coating or fissure sealants.
Wear resistant.
Biocompatible.
Nanotechnology and nanomaterials in dentistry
G
G
483
Low surface energy that helps in the detachment of bacteria and biofilm.
Can be beneficial in compromised patients having xerostomia, poor oral hygiene, and
high caries rate.
18.4.1.2 Casein phosphopeptide and amorphous calcium
phosphate nanocomplexes
Casein phosphopeptide (CPP) and amorphous calcium phosphate (ACP) are thought
to accelerate the remineralization of the enamel surface (Madhavan et al., 2012;
Rizvi et al., 2016). CPP ACP nanomaterials (B2.12 nm) are used for the prevention of enamel caries, remineralization (Reynolds, 2008) and for the management of
oral biofilm (Cross et al., 2007). Nanocomplexes in CPP ACP are significantly
smaller in size than microorganisms, therefore establishing an effective interaction
with oral microorganisms (Hannig and Hannig, 2010) and binding to the bacterial
cell surface to interfere with their adherence with the tooth (Cross et al., 2007).
This sequence delays the formation of biofilm (Rahiotis et al., 2008), inhibits
demineralization, and promotes remineralization of initial carious lesions
(Reynolds, 2008). Furthermore, CPP ACP nanomaterials are used in sugar-free
gums due to their proven role in preventing proximal caries (Morgan et al., 2008).
18.4.1.3 Nanohydroxyl apatite toothpaste
Carbonate hydroxyl apatite nanoparticles (20 100 nm) were used to repair micronsized carious lesions (Roveri et al., 2009) as a result of hydroxyl apatite deposition in
to the demineralized tissues. These toothpastes contain spheroid or needle-like
hydroxyl apatite nanoparticles as an active constituent (Lv et al., 2007). Key benefits
include ease of application as the medium of delivery is toothpaste and deposition of
apatite nanoparticles in the defect. The remineralization of decaying tissues was
better in comparison to sodium fluoride-containing formulations (Lv et al., 2007).
18.4.2 Nanomaterials for periodontics
Uncontrolled periodontal lesions cause bone resorption and tooth loss (Pihlstrom
et al., 2005). Nanomaterials used for the cure of periodontal diseases have shown
promising outcomes (Piñón-Segundo et al., 2005). A delivery system based on
nanoparticles loaded with triclosan was developed for the cure of periodontal diseases. Poly(D,L-lactide-co-glycolide), poly(D,L-lactide), and cellulose phthalate were
used to prepare nanoparticles (,500 nm). Various quantities of triclosan as an
active nanomaterial ingredient were proved to reduce the inflammation in animal
studies (Piñón-Segundo et al., 2005). A site-specific delivery system such as
Arestin is used for clinical applications where microspheres containing tetracycline
are introduced directly into the periodontal pocket (Paquette et al., 2004).
In recent decades, resorbable guided tissue regeneration (GTR) membranes to
stimulate the regeneration of periodontal bone have been explored. The GTR
membrane acts as a barrier between the bone and the gingival epithelium
484
Advanced Dental Biomaterials
(Bottino et al., 2012). The limitations of using biodegradable GTR materials are
poor mechanical properties and the possibility of adverse tissue reactions (Bottino
et al., 2012). To reinforce the mechanical properties, poly-L-lactide fibrous and
membranous scaffolds loaded with octadecylamine-functionalized diamond nanoparticles showed better strength (Zhang et al., 2011, 2012). Growth factors such as
bone morphogenetic protein-2 and fibroblast growth factor carried by nanodiamonds in injectable form were observed to stimulate osteoblast differentiation
in vitro (Moore et al., 2013). It is suggested that nanoparticles reinforced membranes can overcome the limitations of existing GTR membranes in addition to
delivering bioactive growth factors to the periodontal tissues. Nanodiamond-loaded
poly(lactide-co-glycolide) (Parizek et al., 2012; Brady et al., 2015), poly(L-lactide)co-(ε-caprolactone), and poly(LLA-co-CL) scaffolds (Xing et al., 2013) have been
electrospun and showed promising results for proliferation and growth of human
osteoblast-like MG-63 and mesenchymal cells. Furthermore, the nanodiamondloaded poly(LLA-co-CL) scaffolds were used for periodontal tissues in vivo and
showed significantly greater bone growth compared to unmodified scaffolds (Xing
et al., 2013; Suliman et al., 2015). Recently, the natural polymeric material chitosan
was explored for potential applications in dentistry and tissue regeneration (Qasim
et al., 2018; Husain et al., 2017). Chitosan is a natural bioresorbable material used
in the form of nanoparticles or films which can be used to deliver medicaments
(chlorhexidine, metronidazole, and nystatin) to periodontium (Qasim et al., 2017;
Al-Bayaty et al., 2013; Pichayakorn and Boonme, 2013). The drug release is
improved, corresponding to the higher surface area and reactivity of nanoparticles
(Khurshid et al., 2015; Paul and Robeson, 2008). There is a potential of developing
nanodiamond scaffolds in the form of membranes or injectable hydrogels to deliver
regenerative growth factors to the dental tissues. It is expected to develop more
materials for periodontal applications including periodontal tissue regeneration.
18.4.3 Nanomaterials for dental implants
The concept of using dental implants is not new; however, the modern dental
implants became popular after Brånemark’s novel work on titanium (Brånemark
et al., 1969). Although dental implants have a high success rate (95%), failure may
be caused by infection, accelerated bone loss, or lack of osseointegration (Pye
et al., 2009). The metallic dental implants have been used successfully for last four
decades; however, there are certain shortcomings related to the osseointegration
and the mismatch of the mechanical properties of biomaterials and bone (Tomsia
et al., 2011). For example, the Young’s modulus is almost five times higher than
that of cortical bone (Oh et al., 2002), which may cause areas of stress concentration around the implant biomaterials resulting in bone resorption and failure. The
implant’s surface is required to be modified in order to improve the surface biocompatibility, hydrophilicity, and enhanced osseointegration with alveolar bone
(Le Guéhennec et al., 2007). Failures of dental implants are mainly associated with
peri-implantitis or failure of the bioactive surface coating (Esposito et al., 1998;
Esposito, 1998). Plenty of research is being performed on surface modifications of
Nanotechnology and nanomaterials in dentistry
485
dental implants to overcome these shortcomings (Najeeb et al., 2017; Kulkarni
Aranya et al., 2017; Matinlinna et al., 2013; Najeeb et al., 2016b). Nanomaterials
coatings improved the mechanical as well as biological properties of titanium
implants (Valiev et al., 2007). There are high expectations from nanomaterials
research to improve the properties and to manufacture new generations of implant
materials. Some modifications of the implant surface involving nanomaterials are
described here.
18.4.3.1 Nanozirconia and alumina materials
These materials were developed using tetragonal zirconia (ZrO2) nanoparticles and
alumina matrix and exhibited improved mechanical properties (Pecharroman et al.,
2003; Deville et al., 2003).
18.4.3.2 Titanium and silica nanocomposites
Silica is well known for its bioactivity for calcified tissue as it promotes the formation of HA (Cao and Hench, 1996). The addition of silica on the implant surface
enhanced the bioactivity by forming Si OH groups on the surface. Titanium was
added to improve mechanical properties for load-bearing applications (Jurczyk
et al., 2013). These nanocomposites have better hardness and facilitate the tissue
and bone growth in the micro- and macro-sized pores present in their surface
(Jurczyk et al., 2013).
18.4.3.3 Calcium phosphorous nanoparticles
Titanium implant surfaces can be modified using calcium phosphorous (Ca P)
nanoparticles. Ca P nanoparticles (B20 nm) can be deposited on the implant surface by sol gel technique (Mendonça et al., 2008). There was a rise in bone growth
in Ca P-modified surfaces compared to the commercially pure titanium and titanium alloys (Mendes et al., 2007, 2008).
18.4.3.4 Hydroxyapatite nanocrystals
HA nanocrystals/particles have been used for the surface modification of dental
implants. HA nanocrystals powder can be prepared using the wet chemical process,
that can be used to produce either microcrystalline HA (sintering at B1100 C for
60 minutes) or nanocrystalline HA (hydrothermal treatment at 200 C for 24 hours).
HA powder deposited on to the implant surface at room temperature resulted in
better adhesion of osteoblasts and more calcium deposition in the case of nanocrystalline HA coating compared to traditional HA coating (Sato et al., 2006).
18.4.3.5 Nanodiamond coatings
Recently, silanization and immobilization techniques have been used to coat dental
implant surface with nanodiamonds (Gonçalves et al., 2014). Nanodiamond
coatings have the potential to deliver drugs and growth factors and overcome the
486
Advanced Dental Biomaterials
shortcomings of surface modifications (Xu et al., 2014). Nanodiamond coatings are
capable of improving the mechanical and biological properties (Khurshid et al.,
2015; Najeeb et al., 2015, 2016c; Sheikh et al., 2015); therefore surface nanocoatings can improve the materials tissue interface and provide better stability.
18.4.4 Restorative nanobiomaterials
18.4.4.1 Nanocomposites
Resin-based dental composites are the most popular dental restorative materials and
are mainly composed of resin polymeric matrix, inorganic fillers particles, and
silane coupling agents. The inorganic (quartz, glass, or silica) filler particles
(B60 80 vol.%) are added to reinforce the mechanical properties. Considering
fillers as a major component, the resin composites are often classified as microfilled, hybrid, and nanocomposites on the basis of filler size and morphology
(Sakaguchi and Powers, 2012). In addition, it is well accepted that the properties of
resin composites (physical and mechanical) are modified by altering size, proportion, and distribution of filler particles (Terry, 2004).
Since the discovery of resin composites, a range of modifications have been
introduced to the conventional materials in order to improve the materials’ properties (Buonocore, 1955). The nanocomposites were developed to overcome the shortcomings of conventional resin composites and to gain better performance by
incorporating various nanostructures (nanoparticles, nanofibers, and nanoclusters).
However, for a true nanocomposites material, the size of all particles must be
B1 100 nm. Alternatively, nanohybrid composites contain nanoparticles as well
as larger filler particles (0.4 5.0 μm) in the resin matrix (Sakaguchi and Powers,
2012). Incorporation of nanostructures resulted in significantly improved properties
of dental composites (Sakaguchi and Powers, 2012) due to the following:
G
G
G
G
G
G
G
G
Larger surface area and availability of more sites for bonding.
Nanoparticles size is closer to polymer molecules and results in molecular scale interaction with polymer resin matrix.
As particle size is smaller than visible light wavelength (400 800 nm) and responsible
for higher translucency and aesthetic.
Better smoothness and gloss finish of restorations.
Mechanical properties are as good as of microhybrid composites.
The values (Mitra et al., 2003) of compressive strength (460 MPa), flexural strength
(180 MPa), and diametral tensile strength (81 MPa) are higher than any other types of
resin composites and glass-ionomers cement.
Excellent wear resistance; as good as that of natural human enamel in 3 and 5 years clinical
studies.
Nanozirconia particles (5 7 nm) can bring radiopacity without affecting the other
properties.
The fillers particles size in conventional restorative macroscopic materials is significantly greater (0.04 7 μm) compared to the HA crystal present in tooth enamel
(B1 10 nm). This kind of mismatch of properties has an adverse effect on the
Nanotechnology and nanomaterials in dentistry
487
bonding of tooth and synthetic materials (Musselman, 2003). This disparity has
remarkably been overcome using nanoparticles in the case of nanocomposites
(nanofillers), and therefore having a better capability of establishing a smooth transition and native interface with tooth tissues (Terry, 2004). Conclusively, the incorporation of nanofillers (in the case of nanocomposites and hybrids) improved the
physical, mechanical, and optical properties of the resin composites.
18.4.4.2 Nanoglass ionomers (nanoionomers)
The conventional glass-ionomer cement (GIC) was introduced by Wilson and Kent
(1971) in the 1970s. Since then GIC has emerged as promising dental restorative
material. Although there are not many differences, there are a variety of GICs available commercially. Conventionally, GICs are available in powder/liquid form to
start the reaction upon mixing. The main component of powder is fluoroaluminosilicate glass with added calcium, strontium, and lanthanum ions. The liquid copolymer (acrylic acid/itaconic acid or maleic acid) is used to start the reaction
(Sakaguchi and Powers, 2012). GIC gained popularity due to its unique features
such as fluoride release, bonding to the dental tissues, and excellent biocompatibility
(Ten Cate and van Duinen, 1995). The shortcomings of GIC included poor mechanical
properties (Mount, 1998), aesthetics, longer setting reaction (Mount, 1998; Tyas, 2006),
and poor adhesive strength (Mickenautsch et al., 2012). To overcome the shortcomings,
research is actively being conducted to modify the properties, such as addition of HA
and fluorapatite (Moshaverinia et al., 2008), cellulose fibers (Silva et al., 2013), and
nanotechnologies (Jevnikar et al., 2012).
Recently, nanotechnology modified the resin-modified glass ionomers (RMGIC)
using nanoparticles (nanomers) and nanoclusters. These nanoionomers (such as
Ketac Nano) have been used in clinical applications for more than a decade. The
addition of nanoparticles improved the aesthetic properties and surface finish without influencing the fluoride releasing properties (Sakaguchi and Powers, 2012). The
Knoop hardness of Ketac Nano (B39 KHN) was noticeably lower compared to
RMGIC, Vitremer (B70 KHN) (Raggio et al., 2009). In addition, the Knoop hardness of Ketac Nano (B48 KHN) was also lower than the restoration hardness specified by the American Dental Association; therefore it is not recommended for stress
bearing areas (Anusavice and Phillips, 2003). It is recommended to use this material
for lower stress bearing areas including class I, III, and V restorations or beneath
resin composite and in deciduous teeth.
Another nanomaterial, Equia system, contains inorganic silica nanofiller particles (B40 nm) homogeneously dispersed into the matrix. The addition of silica
nanoparticles (15 wt.%) improveed the wear resistance alongside controlling the
initial setting time. The improved wear resistance enables these materials to maintain the surface finish for a prolonged time compared to the original composition.
In terms of physical properties, optical properties (translucency and hue) and aesthetics were improved significantly compared to conventional GIC (Basso, 2011).
Considering the promising results of adding inorganic nanoparticles (HA, silica,
488
Advanced Dental Biomaterials
and fluorapatite) to GIC, it has been a cutting edge research area for scientists for
the last few years.
Crystalline HA is the main inorganic component of mineralized oral tissues and
there are no biocompatibility issues, and synthetic HA is used for biological applications. The nanoscale facilitates additional benefits, for instance, RMGICs’ bond
strength to the tooth tissues (B0.75 MPa) was improved (1.02 MPa) by replacing
conventional particles with micro-HA (5 10 μm) and further reinforced in the case
of nano-HA (1.91 MPa). The higher surface area in the case of HA nanoparticles
results in improving the bond strength possibility of better surface finish and bioactivity (Lee et al., 2010). In a similar study, nano-sized HA and fluorapatite synthesized sol gel method were added to modify Fuji II GIC. Such modifications
resulted in the improvement of mechanical strengths (compressive, diametral tensile, and biaxial flexural) of GIC (Moshaverinia et al., 2008). In addition, materials
such as yttria-stabilized zirconia (Gu et al., 2005), alumina (Jevnikar et al., 2012;
Khademolhosseini et al., 2012), and alumina/titania (Khademolhosseini et al., 2012)
have been explored to modify existing GICs. On the basis of ongoing research on
nano-GIC, further improvement in existing GIC materials may be expected soon.
18.4.5 Endodontic nanobiomaterials
Nanomaterials have been explored for various endodontic applications including
sealants, irrigators, obturation materials, and endodontic regeneration. This section
describes various materials that have been introduced for current and potential
endodontic applications.
18.4.5.1 Nanoparticles-based endodontic sealer
Biological nanoceramics comprises bioactive components, such as calcium hydroxide, calcium phosphate, calcium silicate, and zirconia, and thickening agent
were used to develop EndoSequence BC sealer. The addition of bioactive nanoparticles aimed to improve the materials’ manipulation and physical properties. The
EndoSequence BC sealer uses moisture available in the apical area and hydrate to
form nano-HA and calcium silicate. Therefore the reaction and setting time may be
influenced by canal moisture; for instance, lack of moisture (overly dried canals)
results in prolonged setting time (Koch and Brave, 2009). In terms of the material’s
properties, EndoSequence BC sealer has a number of benefits, for example, it is
available as a premixed injectable paste giving the benefits of a homogeneous mix,
being convenient to apply, and saving time (Koch and Brave, 2009; Zoufan et al.,
2011). In addition, nano-sized particles facilitate extrusion of materials from capillary needles and adopt to surface irregularities. The setting reaction does not require
absolute drying of root canals as the residual moisture ignites the setting reaction to
set it hard and formation of bioactive HA (Koch and Brave, 2009; Zoufan et al.,
2011). It forms bonding tooth structure and obturation material without any cytotoxicity or biocompatibility issues. It shows excellent dimensional stability and
Nanotechnology and nanomaterials in dentistry
489
antimicrobial properties due to an alkaline pH (12.8). Setting time is B3 4 hours
and it provides excellent sealing (Koch and Brave, 2009; Zoufan et al., 2011).
18.4.5.2 GuttaFlow sealer
GuttaFlow sealer is a silicon-based material with added silver nanoparticles and
gutta percha dust. For convenient application, it is supplied as single-dose capsule
to be mixed and injected in to the root canals (Zoufan et al., 2011). Key properties
are as follows:
G
G
G
G
G
Good compatibility and limited toxicity to tissue are acceptable.
Excellent sealing of the root canal and better resistance to bacterial penetration.
No heating required hence no shrinkage and improved sealing capability.
Working time is 15 minutes and setting time is 30 minutes.
Dimensionally stable and insoluble after setting.
18.4.5.3 Antibacterial nanoparticle modified endodontic sealer
Considering the magnificent benefits of antibacterial activity for endodontic sealers, conventional sealers (AH Plus, GuttaFlow, and Epiphany) were modified using quaternary
ammonium polyethyleneimine (QPEI) antibacterial nanoparticles (Abramovitz et al.,
2012). The addition of QPEI nanoparticles to composites enabled antibacterial activity
for a longer period of time without affecting the mechanical properties (Beyth et al.,
2008). Itzhak et al. added QPEI nanoparticles (0 2 wt.%) to various endodontic sealers
to introduce bactericidal properties (Abramovitz et al., 2012). This study reported the
following features while adding antibacterial nanoparticles (Abramovitz et al., 2012):
G
G
G
G
Excellent antibacterial, that is expected to last longer when nanoparticles are encapsulated
in the matrix.
QPEI nanoparticles are very stable, prepolymerized, and no by-product or unwanted products are released into the surrounding biological environment.
Addition of QPEI nanoparticles (1 wt.%) does not cause any cytotoxicity whereas a higher
concentration (2 wt.%) is slightly cytotoxic.
No effect on the biocompatibility of modified sealers.
18.4.5.4 Nanohydroxyapatite gutta percha
Nano-HA-modified gutta percha was introduced in recent years. In addition to
nano-HA, the sealer comprises a powder component, bismuth oxide (opacifier),
hexamethylenetetramine (activator), and liquid component (bisphenol-A-diglycidylether). Wet chemistry route with calcium hydroxide and phosphoric acid precursors
were used to fabricate nano-HA in the range of B40 60 nm (Farea et al., 2010).
These materials showed excellent sealing abilities comparable to AH 26 and
Epiphany sealers. There were no unwanted effects during the root canal obturation
(Abdo et al., 2012). Recently, diamond nanoparticle reinforced gutta percha has
shown better mechanical and antibacterial properties (Lee et al., 2015b).
490
Advanced Dental Biomaterials
18.4.5.5 Bioactive nanoscale glass for root canal disinfection
The bioactive glass nanoparticles have demonstrated antibacterial activity. For this
purpose, the sol gel route was used to fabricate glass nanoparticles (B20 90 nm)
(Mortazavi et al., 2010). Bioactive glasses containing SiO2 CaO P2O5 (such as
58S, 63S, and 72S) have been assessed for the antimicrobial potentials. At the optimal concentration (100 mg/mL) of 58S and 63S for antibacterial affects, it effectively showed control of the bacterial growth on agar plates. The antibacterial
activity is further enhanced due to the alkaline nature of nanoglasses. The solution
pH rises from B7.3 to 8.8 in a few hours and may become more alkaline (B9.0)
in 5 days (Mortazavi et al., 2010). Therefore these nanomaterials release alkaline
species in the biological environment and further enhance the antibacterial activity
(Waltimo et al., 2007). Bioceramics have proven benefits of bioactivity and excellent biocompatibility; in addition, the release of antibacterial alkaline species
highlighted the potential of these materials for root canal disinfection applications
(Mortazavi et al., 2010).
18.4.6 Nanomaterials and endodontic regeneration
The conventional endodontic treatment involves the extirpation of residual pulp tissues and infected dentin debris using mechanical instrumentation and antimicrobial
irrigants (Rizvi et al., 2014; Madarati et al., 2017). Following cleaning and shaping,
root canals are filled using gutta purcha (Friedman et al., 1975). However, conventional endodontics has a number of limitations such as loss of vitality, poor
mechanical properties, and compromised disinfection (Fouad et al., 2008; Saunders
and Saunders, 1994; Siqueira, 2001; AlRahabi, 2017). The endodontic regenerative
approaches have the benefit of maintaining pulp vitality and regenerating dental
tissues (Horst et al., 2012; Zafar et al., 2015a,b). For the pulp tissue engineering,
purified dental pulp stem cells were grown in sheets on scaffolds. The beneficial
role of nanomaterials for tissue engineering scaffolds is well accepted because of
high surface area and surface energy. For instance, nanofibrous scaffolds made
of biodegradable organic matrix (such as collagen and fibronectin) (Venugopal and
Ramakrishna, 2005; Fukuda et al., 2006) and hydrogels were explored for regeneration of pulp and showed the formation of nanofibrous mesh supporting cellular
growth (Galler et al., 2008). Collagen is the most numerous fibrous protein originating from bone and dentin (Wiesmann et al., 2004). Injectable collagen (type I)
scaffolds loaded with exfoliated dental stem cells lead to growth of functional odontoblasts and pulp tissues (Demarco et al., 2011). These findings are suggestive that
type I collagen scaffolds encourages odontogenic differentiation and mineralization
(Kim et al., 2009; Mizuno et al., 2003).
18.4.7 Nanomaterials and tissue engineering
Tissue regeneration is an interdisciplinary approach involving multiple scientific
disciplines including biology and engineering (Galler et al., 2010). It was
Nanotechnology and nanomaterials in dentistry
491
considered as a part of biomaterials initially. However, it later developed as an individual subject on its own because of promising and remarkable development. There
are a variety of definitions available for tissue engineering in the literature. Simply
put, “Tissue engineering applies the principles of biology and engineering to the
development of functional substitutes for damaged tissue” (Duncan and Sprehe,
2008; Langer and Vacanti, 1993). For any tissue engineering application, there are
three main components: cells (mainly stem cells capable of differentiating into
various cell lines), bioactive molecular signals (to assist the cellular differentiation
and tissue regeneration), and a material scaffold to expand and carry cellular components (Galler et al., 2010; Hargreaves, 2010). Nanomaterials have been explored
for the fabrication of tissue engineering scaffolds. To construct a scaffold of a
suitable material and to mimic extracellular matrix to support cell growth, differentiation and functionality are the foremost challenges for researchers. There are different
techniques used for constructing nanofibrous polymer scaffolds. Electrospinning is a
potential method of fabricating nanomaterials for such applications and is commonly
used (Gouma, 2009).
18.4.8 Electrospun nanomaterials
Electrospinning technique is used for fabricating nanofibers (Fig. 18.4) (from a few
nanometers in diameter to tens of micron); additives such as biomolecules or medicaments can also be incorporated to get the desired properties in the final materials
Figure 18.4 SEM images of typical electrospun materials: (A and B) as electrospun mats of
natural silk and (C and D) condensation of silica to in order to fabricate silica silk
nanocomposites.
492
Advanced Dental Biomaterials
(Greiner and Wendorff, 2007). Electrospun nonwoven mats are porous in a threedimensional format, providing support to cells similar to the extracellular matrix
(Li et al., 2002; Agarwal et al., 2008).
Electrospun nanofibers have useful properties such as availability of high surface
area for protein absorption and binding sites (Stevens and George, 2005) and
enhanced cellular attachment and interaction (Bosworth and Downes, 2011). There
are various properties of electrospun scaffolds, such as material strength, the porosity can be tailored by nanofiber alignment, and orientation, that can facilitate
maximum volume fractions (Bosworth and Downes, 2011). In addition, characteristics such as surface morphology and topography can also be controlled adjusting
various solution dope and spinning parameters (Liang et al., 2007). Due to such
unique properties, electrospun nanofiber scaffolds have emerged as an excellent
candidate for various biological applications such as wound dressings (He et al.,
2015a; Zhou et al., 2013; Rho et al., 2006), drug delivery (He et al., 2015a;
Li et al., 2005; Sill and von Recum, 2008), tissue engineering scaffolds
(Ardeshirzadeh et al., 2015; Dinis et al., 2015; He et al., 2015b; Tang et al., 2015),
and dental applications (Zafar et al., 2016; Qasim et al., 2017; Samprasit et al.,
2015; Ohkawa et al., 2009). Various types of nanofibers that have been electrospun
for dentistry are shown in Table 18.2.
Nanomaterial scaffolds, either electrospun or fabricated by any other technique,
are being used for a variety of dental tissue regenerations, such as dentin (VallésLluch et al., 2010), pulp (Cavalcanti et al., 2013), ligament (Peh et al., 2007; Park
et al., 2010), bone (Saiz et al., 2013), neural tissues (Lee and Livingston Arinzeh,
2011; Yang, 2004), and tooth (Honda et al., 2010). Although electrospun materials
exhibited beneficial properties such as biocompatibility, surface smoothness, and
controlled release of the incorporated drugs (Zafar et al., 2016; Li et al., 2005;
Norowski et al., 2015), further research is needed to translate these materials to
clinical applications.
18.5
Potential of nanomaterials
Although a lot of research has been carried out to improve the properties of existing
materials, there is no dental material that has ideal properties for any specific application (Anusavice and Phillips, 2003). For example, dental amalgam has been used
successfully for more than a century however, there are major concerns about mercury toxicity (Eley, 1997a,b; Jones, 1998; Warfvinge, 1995; Smart et al., 1995) and
poor aesthetics (Eley, 1997c; Mclean, 1984; Yardley, 1984). Alternatively, the
adhesive composites overcome the aesthetic issues; however, poor mechanical
properties and technique sensitivity remain the major issues (Moszner and Salz,
2007). In addition, the synthetic materials lack intelligence to respond to environmental stimuli and activate self-repair and regeneration process (Mano and Reis,
2005). Biological components (such as biomolecules, materials scaffolds, and cells)
interact with biomaterials at the nanoscale. Materials scientists may benefit from
Nanotechnology and nanomaterials in dentistry
493
Table 18.2 Applications of electrospun nanofibers in dentistry.
Applications in
dentistry
Electrospun nanofibers
References
Nanocomposites
Polyvinyl alcohol/gelatin
Silk/silica
PVA, PDS
Linh and Lee (2012)
Foo et al. (2006)
Kim et al. (2008a, 2014),
Bottino et al. (2015)
Kim et al. (2008b, 2014),
Ranjbar-Mohammadi et al. (2016),
Zhang et al. (2003, 2007),
Jin et al. (2002)
Samprasit et al. (2015)
Tooth tissue
engineering
Periodontal
regeneration
Collagen, PLGA, PLLA,
PCL, PEO, silk
Prevention of
caries
Reinforcement
of resin
composites
Chitosan
Implant surface
modification
Cartilage tissue
engineering
PLGA, collagen
Drug delivery
Poly(ethylene-co-vinyl
acetate), PLLA, PLGA
Mucosal/wound
and repair
Poly-L-(lactic acid), PLGA,
chitin, chitosan, silk
fibroin, collagen
PVA, polyacrylonitrile,
polystyrene, nylon
PCL, PEO, chitosan
Wang et al. (2008), Behler et al.
(2009), Demir et al. (2014),
Borges et al. (2015),
Lee et al. (2015a)
Ravichandran et al. (2012)
Ainola et al. (2016), Subramanian
et al. (2004), Levorson et al.
(2013), Thorvaldsson et al. (2008),
Li et al. (2003)
Vacanti et al. (2012), Song et al.
(2013), Zeng et al. (2013), Xue
et al. (2014), Kim et al. (2004),
Verreck et al. (2003), Kenawy et al.
(2002)
He et al. (2015a), Tang et al. (2015),
Thakur et al. (2008), Noh et al.
(2006), Blackwood et al. (2008)
PCL, Poly carpolactone; PDS, polydiaxonone; PEO, polyethylene oxide; PLGA, poly(lactide-co-glycolide); PLLA,
poly-L-lactic acid; PVA, polyvinyl alcohol.
using nanotechnology approaches to improve the material tissues interaction as
pointed below:
1. To replace lost dental tissues following nature’s principles (biomimetic approaches) and
producing biomaterials resembling the properties very closely of the replaced materials.
2. To produce synthetic materials matching morphology and properties similar to natural
dental tissues.
3. Use of regenerative medicine and tissue engineering to replace lost dental tissue by
regeneration.
There are plenty of hopes for nanomaterials in terms of either developing new
materials or significant improvements in the properties of existing materials. The
scope of nanomaterials in dentistry is bright and will be helpful to enhance the
quality of life in patients.
494
18.6
Advanced Dental Biomaterials
Conclusive remarks
The application of nanomaterials is the most challenging in the field of medicine
and biomedical purposes (Bauer et al., 2004). Nanomaterials exhibited promising
results for a range of current and potential applications in various disciplines of
dentistry. In addition to new materials, nanotechnology helped researchers to
improve the physical and mechanical properties of existing materials. For instance,
adding nanoparticles can reinforce strength of polymer composites and facilitate a
greater surface area for cellular attachment in tissue engineering scaffolds. This is
an area of very active research all around the globe involving a lot of research funding. It can be expected in the future that the science of dental materials may change
significantly with the better understanding and the introduction of new nanobiomaterials. It can be hoped that promising nanomaterials will provide a variety of materials for dental applications in the next decade.
References
Abdo, S.B., Al Darrat, A., Luddin, N., Husien, A., 2012. Sealing ability of gutta-percha/nano
HA versus resilon/epiphany after 20 months using an electrochemical model—an
in vitro study. Braz. J. Oral Sci. 11, 387 391.
Abramovitz, I., Beyth, N., Weinberg, G., Borenstein, A., Polak, D., Kesler-Shvero, D., et al.,
2012. In vitro biocompatibility of endodontic sealers incorporating antibacterial nanoparticles. J. Nanomater. 2012, 1 9.
Agarwal, S., Wendorff, J.H., Greiner, A., 2008. Use of electrospinning technique for biomedical applications. Polymer (Guildf.) 49, 5603 5621.
Ainola, M., Tomaszewski, W., Ostrowska, B., Wesolowska, E., Wagner, H.D.,
Swieszkowski, W., et al., 2016. A bioactive hybrid three-dimensional tissue-engineering
construct for cartilage repair. J. Biomater. Appl. 30, 873 885. Available from: https://
doi.org/10.1177/0885328215604069.
Al-Bayaty, F.H., Kamaruddin, A.A., Ismail, M.A., Abdulla, M.A., 2013. Formulation and
evaluation of a new biodegradable periodontal chip containing thymoquinone in a chitosan base for the management of chronic periodontitis. J. Nanomater. 2013, 16.
AlRahabi, M.K., 2017. Evaluation of complications of root canal treatment performed by
undergraduate dental students. Libyan J. Med. 12, 1345582.
Anusavice, K., Phillips, R., 2003. Phillips’ Science of Dental Materials. Saunders, St. Louis,
MO; Great Britain.
Arcı́s, R.W., López-Macipe, A., Toledano, M., Osorio, E., Rodrı́guez-Clemente, R., Murtra,
J., et al., 2002. Mechanical properties of visible light-cured resins reinforced with
hydroxyapatite for dental restoration. Dent. Mater. 18, 49 57.
Ardeshirzadeh, B., Anaraki, N.A., Irani, M., Rad, L.R., Shamshiri, S., 2015. Controlled
release of doxorubicin from electrospun PEO/chitosan/graphene oxide nanocomposite
nanofibrous scaffolds. Mater. Sci. Eng. C 48, 384 390.
Basso, M., 2011. Teeth restoration using a high-viscosity glass ionomer cement: the Equias
system. J. Minimum Intervention Dent. 4, 74 76.
Nanotechnology and nanomaterials in dentistry
495
Bauer, L.A., Birenbaum, N.S., Meyer, G.J., 2004. Biological applications of high aspect ratio
nanoparticles. J. Mater. Chem. 14, 517 526.
Behler, K.D., Stravato, A., Mochalin, V., Korneva, G., Yushin, G., Gogotsi, Y., 2009.
Nanodiamond-polymer composite fibers and coatings. ACS Nano 3, 363 369.
Beyth, N., Houri-Haddad, Y., Baraness-Hadar, L., Yudovin-Farber, I., Domb, A.J., Weiss, E.I.,
2008. Surface antimicrobial activity and biocompatibility of incorporated polyethylenimine nanoparticles. Biomaterials 29, 4157 4163.
Blackwood, K.A., McKean, R., Canton, I., Freeman, C.O., Franklin, K.L., Cole, D., et al.,
2008. Development of biodegradable electrospun scaffolds for dermal replacement.
Biomaterials 29, 3091 3104.
Borges, A.L., Münchow, E.A., de Oliveira Souza, A.C., Yoshida, T., Vallittu, P.K., et al.,
2015. Effect of random/aligned nylon-6/MWCNT fibers on dental resin composite reinforcement. J. Mech. Behav. Biomed. Mater. 48, 134 144.
Bosworth, L.A., Downes, S., 2011. Electrospinning for Tissue Regeneration. Woodhead
Publishing, Oxford.
Bottino, M.C., Thomas, V., Schmidt, G., Vohra, Y.K., Chu, T.G., Kowolik, M.J., et al.,
2012. Recent advances in the development of GTR/GBR membranes for periodontal
regeneration—a materials perspective. Dent. Mater. 28, 703 721.
Bottino, M.C., Yassen, G.H., Platt, J.A., Labban, N., Windsor, L.J., Spolnik, K.J., et al.,
2015. A novel three-dimensional scaffold for regenerative endodontics: materials and
biological characterizations. J. Tissue Eng. Regen. Med. 9, E116 E123.
Brady, M.A., Renzing, A., Douglas, T.E.L., Liu, Q., Wille, S., Parizek, M., et al., 2015.
Development of composite poly(lactide-co-glycolide)-nanodiamond scaffolds for bone
cell growth. J. Nanosci. Nanotechnol. 15, 1060 1069.
Brånemark, P., Breine, U., Adell, R., Hansson, B., Lindström, J., Ohlsson, Å., 1969. Intraosseous anchorage of dental prostheses: I. Experimental studies. Scand. J. Plast.
Reconstr. Surg. Hand. Surg. 3, 81 100.
Broderick, M., Neville, F., Gibson, T., Millner, P., 2007. Practical nanobiotechnology: functional nanoparticle production using silaffin R5 peptide. J. Biotechnol. 131, S11.
Buonocore, M.G., 1955. A simple method of increasing the adhesion of acrylic filling materials
to enamel surfaces. J. Dent. Res. 34, 849 853.
Cao, W., Hench, L.L., 1996. Bioactive materials. Ceram. Int. 22, 493 507.
Cavalcanti, B.N., Zeitlin, B.D., Nör, J.E., 2013. A hydrogel scaffold that maintains viability
and supports differentiation of dental pulp stem cells. Dent. Mater. 29, 97 102.
Cross, K., Huq, N., Reynolds, E., 2007. Casein phosphopeptides in oral health-chemistry and
clinical applications. Curr. Pharm. Des. 13, 793 800.
Demarco, F.F., Conde, M., Cavalcanti, B.N., Casagrande, L., Sakai, V.T., Nör, J.E., 2011.
Dental pulp tissue engineering. Braz. Dent. J. 22, 3 14.
Demir, M.M., Horzum, N., Ta demirci, A., Turan, K., Güden, M., 2014. Mechanical interlocking between porous electrospun polystyrene fibers and an epoxy matrix. ACS Appl.
Mater. Interfaces 6, 21901 21905.
Deville, S., Chevalier, J., Fantozzi, G., Bartolomé, J.F., Requena, J., Moya, J.S., et al., 2003.
Low-temperature ageing of zirconia-toughened alumina ceramics and its implication in
biomedical implants. J. Eur. Ceram. Soc. 23, 2975 2982.
Dinis, T.M., Elia, R., Vidal, G., Dermigny, Q., Denoeud, C., Kaplan, D.L., et al., 2015. 3D
multi-channel bi-functionalized silk electrospun conduits for peripheral nerve regeneration. J. Mech. Behav. Biomed. Mater. 41, 43 55.
Duncan, L., Sprehe, C., 2008. Mosby’s Dental Dictionary. Mosby, St. Louis, MO.
496
Advanced Dental Biomaterials
Eley, B.M., 1997a. The future of dental amalgam: a review of the literature. 2. Mercury
exposure in dental practice. Br. Dent. J. 182, 293 297.
Eley, B.M., 1997b. The future of dental amalgam: a review of the literature. 4. Mercury
exposure hazards and risk assessment. Br. Dent. J. 182, 373 381.
Eley, B.M., 1997c. The future of dental amalgam: a review of the literature. 7. Possible alternative materials to amalgam for the restoration of posterior teeth. Br. Dent. J. 183,
11 14.
Elgendy, E.A., Abo Shady, T.E., 2015. Clinical and radiographic evaluation of nanocrystalline hydroxyapatite with or without platelet-rich fibrin membrane in the treatment of
periodontal intrabony defects. J. Indian Soc. Periodontol. 19, 61 65.
Emsley, J., 1976. The Chemistry of Phosphorus: Environmental, Organic, Inorganic,
Biochemical and Spectroscopic Aspects. Harper & Row, London.
Esposito, M., 1998. Biological factors contributing to failures of osseointegrated oral
implants. (l). Success criteria and epidemiology. Eur. J. Oral Sci. 106, 527 551.
Esposito, M., Hirsch, J., Lekholm, U., Thomsen, P., 1998. Biological factors contributing to
failures of osseointegrated oral implants, (II). Etiopathogenesis. Eur. J. Oral Sci. 106,
721 764.
Farea, M., Masudi, S., Bakar, W., Zaripah, W., 2010. Apical microleakage evaluation of
system B compared with cold lateral technique: in vitro study. Aust. Endod. J. 36, 48 53.
Feynman, R.P., 1960. There’s plenty of room at the bottom. Eng. Sci. 23, 22 36.
Foo, C.W.P., Patwardhan, S.V., Belton, D.J., Brandon, K., Anastasiades, D., Huang, J., et al.,
2006. Novel nanocomposites from spider silk-silica fusion (chimeric) proteins. Proc.
Natl. Acad. Sci. U.S.A. 103, 9428 9433.
Fouad, A., Torabinejad, M., Walton, R.E., 2008. Endodontics: Principles and Practice.
Elsevier Health Sciences.
Friedman, C.M., Sandrik, J.L., Heuer, M.A., Rapp, G.W., 1975. Composition and mechanical
properties of gutta-percha endodontic points. J. Dent. Res. 54, 921 925.
Fukuda, J., Khademhosseini, A., Yeh, J., Eng, G., Cheng, J., Farokhzad, O.C., et al., 2006.
Micropatterned cell co-cultures using layer-by-layer deposition of extracellular matrix
components. Biomaterials 27, 1479 1486.
Gahlot, S., Sharma, P.P., Gupta, H., Kulshrestha, V., Jha, P.K., 2014. Preparation of graphene
oxide nano-composite ion-exchange membranes for desalination application. RSC Adv.
4, 24662 24670.
Galler, K.M., Cavender, A., Yuwono, V., Dong, H., Shi, S., Schmalz, G., et al., 2008. Selfassembling peptide amphiphile nanofibers as a scaffold for dental stem cells. Tissue
Eng. Part A 14, 2051 2058.
Galler, K.M., D’Souza, R.N., Hartgerink, J.D., 2010. Biomaterials and their potential applications for dental tissue engineering. J. Mater. Chem. 20, 8730 8746.
Gismondi, A., Reina, G., Orlanducci, S., Mizzoni, F., Gay, S., Terranova, M.L., et al., 2015.
Nanodiamonds coupled with plant bioactive metabolites: a nanotech approach for cancer
therapy. Biomaterials 38, 22 35.
Gonçalves, J.P.L., Shaikh, A.Q., Reitzig, M., Kovalenko, D.A., Michael, J., Beutner, R.,
et al., 2014. Detonation nanodiamonds biofunctionalization and immobilization to titanium alloy surfaces as first steps towards medical application. Beilstein J. Org. Chem.
10, 2765 2773.
Gouma, P., 2009. Nanomaterials for Chemical Sensors and Biotechnology. World Scientific,
Singapore; London.
Greiner, A., Wendorff, J.H., 2007. Electrospinning: a fascinating method for the preparation
of ultrathin fibres. Angew. Chem. Int. Ed. Engl. 46, 5670 5703.
Nanotechnology and nanomaterials in dentistry
497
Gu, Y., Yap, A., Cheang, P., Koh, Y., Khor, K., 2005. Development of zirconia-glass ionomer cement composites. J. Non-Cryst. Solids 351, 508 514.
Hannig, M., Hannig, C., 2010. Nanomaterials in preventive dentistry. Nat. Nanotechnol. 5,
565 569.
Hannig, M., Kriener, L., Hoth-Hannig, W., Becker-Willinger, C., Schmidt, H., 2007.
Influence of nanocomposite surface coating on biofilm formation in situ. J. Nanosci.
Nanotechnol. 7, 4642 4648.
Hargreaves, K.M., 2010. Cohen’s Pathways of the Pulp. Mosby, Edinburgh.
He, T., Wang, J., Huang, P., Zeng, B., Li, H., Cao, Q., et al., 2015a. Electrospinning polyvinylidene fluoride fibrous membranes containing anti-bacterial drugs used as wound
dressing. Colloids Surf., B: Biointerfaces 130, 278 286.
He, X., Cheng, L., Zhang, X., Xiao, Q., Zhang, W., Lu, C., 2015b. Tissue engineering scaffolds electrospun from cotton cellulose. Carbohydr. Polym. 115, 485 493.
Hieber, S., Müller, B., 2012. In: Logothetidis, S. (Ed.), Nanodentistry. Springer, Berlin
Heidelberg.
Honda, M.J., Tsuchiya, S., Shinohara, Y., Shinmura, Y., Sumita, Y., 2010. Recent advances
in engineering of tooth and tooth structures using postnatal dental cells. Jpn. Dent. Sci.
Rev. 46, 54 66.
Horst, O.V., Chavez, M.G., Jheon, A.H., Desai, T., Klein, O.D., 2012. Stem cell and biomaterials research in dental tissue engineering and regeneration. Dent. Clin. North Am. 56,
495 520.
Husain, S., Al-Samadani, K.H., Najeeb, S., Zafar, M.S., Khurshid, Z., Zohaib, S., et al., 2017.
Chitosan biomaterials for current and potential dental applications. Materials 10, 602.
Hussain, F., Hojjati, M., Okamoto, M., Gorga, R.E., 2006. Review article: polymer-matrix
nanocomposites, processing, manufacturing, and application: an overview. J. Compos.
Mater. 40, 1511.
Huynh, V.T., Pearson, S., Noy, J., Abboud, A., Utama, R.H., Lu, H., et al., 2013.
Nanodiamonds with surface grafted polymer chains as vehicles for cell imaging and cisplatin delivery: enhancement of cell toxicity by POEGMEMA coating. ACS Macro Lett.
2, 246 250.
Jevnikar, P., Golobič, M., Kocjan, A., Kosmač, T., 2012. The effect of nano-structured alumina coating on the bond strength of resin-modified glass ionomer cements to zirconia
ceramics. J. Eur. Ceram. Soc. 32, 2641 2645.
Jin, H.J., Fridrikh, S., Rutledge, G.C., Kaplan, D., 2002. Electrospinning Bombyx mori silk
with poly(ethylene oxide). Biomacromolecules 3, 1233 1239.
Jones, D.W., 1998. A Canadian perspective on the dental amalgam issue. Br. Dent. J. 184,
581 586.
Jones, F.H., 2001. Teeth and bones: applications of surface science to dental materials and
related biomaterials. Surf. Sci. Rep. 42, 75 205.
Jurczyk, M.U., Jurczyk, K., Niespodziana, K., Miklaszewski, A., Jurczyk, M., 2013.
Titanium SiO2 nanocomposites and their scaffolds for dental applications. Mater
Charact. 77, 99 108.
Kang, M., Chen, P., Jin, H., 2009. Preparation of multiwalled carbon nanotubes incorporated
silk fibroin nanofibers by electrospinning. Curr. Appl. Phys. 9, S95 S97.
Kelsall, R., Hamley, I.W., Geoghegan, M., 2005. Nanoscale Science and Technology. Wiley,
John Wiley & Sons, Ltd.
Kenawy, E., Bowlin, G.L., Mansfield, K., Layman, J., Simpson, D.G., Sanders, E.H., et al.,
2002. Release of tetracycline hydrochloride from electrospun poly(ethylene-co-vinylacetate), poly(lactic acid), and a blend. J. Controlled Release 81, 57 64.
498
Advanced Dental Biomaterials
Khademolhosseini, M., Barounian, M., Eskandari, A., Aminzare, M., Zahedi, A.,
Ghahremani, D., 2012. Development of new Al2O3/TiO2 reinforced glass-ionomer
cements (GICs) nano-composites. J. Basic Appl. Sci. Res. 2, 7526 7529.
Khurshid, Z., Zafar, M., Qasim, S., Shahab, S., Naseem, M., AbuReqaiba, A., 2015.
Advances in nanotechnology for restorative dentistry. Materials 8, 717 731.
Kim, K., Luu, Y.K., Chang, C., Fang, D., Hsiao, B.S., Chu, B., et al., 2004. Incorporation
and controlled release of a hydrophilic antibiotic using poly(lactide-co-glycolide)-based
electrospun nanofibrous scaffolds. J. Controlled Release 98, 47 56.
Kim, G., Asran, A.S., Michler, G.H., Simon, P., Kim, J., 2008a. Electrospun PVA/HAp nanocomposite nanofibers: biomimetics of mineralized hard tissues at a lower level of complexity. Bioinspir. Biomim. 3, 046003.
Kim, I., Seo, S., Moon, H., Yoo, M., Park, I., Kim, B., et al., 2008b. Chitosan and its derivatives for tissue engineering applications. Biotechnol. Adv. 26, 1 21.
Kim, N.R., Lee, D.H., Chung, P., Yang, H., 2009. Distinct differentiation properties of
human dental pulp cells on collagen, gelatin, and chitosan scaffolds. Oral Surg. Oral
Med. Oral Pathol. Oral Radiol. Endod. 108, e94 e100.
Kim, B., Nguyen, T.B.L., Min, Y., Lee, B., 2014a. In vitro and in vivo studies of BMP-2loaded PCL gelatin BCP electrospun scaffolds. Tissue Eng. Part A 20, 3279 3289.
Kim, J.J., Bae, W.J., Kim, J.M., Kim, J.J., Lee, E.J., Kim, H.W., et al., 2014b. Mineralized
polycaprolactone nanofibrous matrix for odontogenesis of human dental pulp cells. J.
Biomater. Appl. 28, 1069 1078.
Koch, K., Brave, D., 2009. A new day has dawned: the increased use of bioceramics in endodontics. Dent. Town 10, 39 43.
Kostarelos, K., Bianco, A., Prato, M., 2009. Promises, facts and challenges for carbon nanotubes in imaging and therapeutics. Nat. Nanotechnol. 4, 627 633.
Kulkarni Aranya, A., Pushalkar, S., Zhao, M., LeGeros, R.Z., Zhang, Y., Saxena, D., 2017.
Antibacterial and bioactive coatings on titanium implant surfaces. J. Biomed. Mater.
Res. A 105, 2218 2227.
Langer, R., Vacanti, J., 1993. Tissue engineering. Science 260, 920 926.
Le Guéhennec, L., Soueidan, A., Layrolle, P., Amouriq, Y., 2007. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 23, 844 854.
Lee, Y., Livingston Arinzeh, T., 2011. Electrospun nanofibrous materials for neural tissue
engineering. Polymers 3, 413 426.
Lee, J., Lee, Y., Choi, B., Lee, J., Choi, H., Son, H., et al., 2010. Physical properties of
resin-reinforced glass ionomer cement modified with micro and nano-hydroxyapatite. J.
Nanosci. Nanotechnol. 10, 5270 5276.
Lee, M.W., An, S., Jo, H.S., Yoon, S.S., Yarin, A.L., 2015a. Self-healing nanofiber-reinforced polymer composites: tensile testing and recovery of mechanical properties. ACS
Appl. Mater. Interfaces 7, 19546 19554.
Lee, D., Kim, S.V., Limansubroto, A.N., Yen, A., Soundia, A., Wang, C., et al., 2015b.
Nanodiamond-gutta percha composite biomaterials for root canal therapy. ACS Nano 9,
11490 11501.
LeGeros, R.Z., 1991. Calcium Phosphates in Oral Biology and Medicine. Karger, Basel.
Levorson, E.J., Sreerekha, P.R., Chennazhi, K.P., Kasper, F.K., Nair, S.V., Mikos, A.G.,
2013. Fabrication and characterization of multiscale electrospun scaffolds for cartilage
regeneration. Biomed. Mater. 8, 014103.
Li, W., Laurencin, C.T., Caterson, E.J., Tuan, R.S., Ko, F.K., 2002. Electrospun nanofibrous
structure: a novel scaffold for tissue engineering. J. Biomed. Mater. Res. 60, 613 621.
Nanotechnology and nanomaterials in dentistry
499
Li, W., Danielson, K.G., Alexander, P.G., Tuan, R.S., 2003. Biological response of chondrocytes cultured in three-dimensional nanofibrous poly(E-caprolactone) scaffolds. J.
Biomed. Mater. Res. A 67, 1105 1114.
Li, W., Mauck, R.L., Tuan, R.S., 2005. Electrospun nanofibrous scaffolds: production, characterization, and applications for tissue engineering and drug delivery. J. Biomed.
Nanotechnol. 1, 259 275.
Liang, D., Hsiao, B.S., Chu, B., 2007. Functional electrospun nanofibrous scaffolds for biomedical applications. Adv. Drug Deliv. Rev. 59, 1392 1412.
Lieber, C.M., 1998. One-dimensional nanostructures: chemistry, physics & applications.
Solid State Commun. 107, 607 616.
Linh, N.T.B., Lee, B., 2012. Electrospinning of polyvinyl alcohol/gelatin nanofiber composites and cross-linking for bone tissue engineering application. J. Biomater. Appl. 27,
255 266.
Low, I.M., Duraman, N., Mahmood, U., 2008. Mapping the structure, composition and
mechanical properties of human teeth. Mater. Sci. Eng. C 28, 243 247.
Lv, K.L., Zhang, J.X., Meng, X.C., Li, X.Y., 2007. Remineralization effect of the nano-HA
toothpaste on artificial caries. Key Eng. Mat. 330, 267 270.
Madarati, A.A., Zafar, M.S., Sammani, A.M., Mandorah, A.O., Bani-Younes, H.A., 2017.
Preference and usage of intracanal medications during endodontic treatment. Saudi Med.
J. 38, 755 763.
Madhavan, S., Nayak, M., Shenoy, A., Shetty, R., Prasad, K., 2012. Dentinal hypersensitivity: a comparative clinical evaluation of CPP-ACP F, sodium fluoride, propolis, and placebo. J. Conserv. Dent. 15, 315.
Mano, J.F., Reis, R.L., 2005. Some trends on how one can learn from and mimic nature in
order to design better biomaterials. Mater. Sci. Eng. C 25, 93 95.
Matinlinna, J.P., Tsoi, J.K., de Vries, J., Busscher, H.J., 2013. Characterization of novel
silane coatings on titanium implant surfaces. Clin. Oral Implants Res. 24, 688 697.
Mclean, J.W., 1984. Alternatives to amalgam alloys. 1. Br. Dent. J. 157, 432 433.
Mendes, V.C., Moineddin, R., Davies, J.E., 2007. The effect of discrete calcium phosphate
nanocrystals on bone-bonding to titanium surfaces. Biomaterials 28, 4748 4755.
Mendes, V.C., Moineddin, R., Davies, J.E., 2008. Discrete calcium phosphate nanocrystalline
deposition enhances osteoconduction on titanium-based implant surfaces. J. Biomed.
Mater. Res. A 90, 577 585.
Mendonça, G., Mendonça, D.B.S., Aragão, F.J.L., Cooper, L.F., 2008. Advancing dental
implant surface technology—from micron- to nanotopography. Biomaterials 29,
3822 3835.
Mickenautsch, S., Yengopal, V., Banerjee, A., 2012. Retention of orthodontic brackets
bonded with resin-modified GIC versus composite resin adhesives—a quantitative systematic review of clinical trials. Clin. Oral Investig. 16, 1 14.
Mitra, S.B., Wu, D., Holmes, B.N., 2003. An application of nanotechnology in advanced dental materials. J. Am. Dent. Assoc. 134, 1382 1390.
Mizuno, M., Miyamoto, T., Wada, K., Watatani, S., Zhang, G.X., 2003. Type I collagen regulated dentin matrix protein-1 (Dmp-1) and osteocalcin (OCN) gene expression of rat
dental pulp cells. J. Cell. Biochem. 88, 1112 1119.
Mohanty, A., Drzal, L., Misra, M., 2003. Nano reinforcements of bio-based polymers—the
hope and the reality. J. Am. Chem. Soc. 225, 33.
Moore, L., Gatica, M., Kim, H., Osawa, E., Ho, D., 2013. Multi-protein delivery by nanodiamonds promotes bone formation. J. Dent. Res. 92, 976 981.
500
Advanced Dental Biomaterials
Morgan, M.V., Adams, G.G., Bailey, D.L., Tsao, C.E., Fischman, S.L., Reynolds, E.C.,
2008. The anticariogenic effect of sugar-free gum containing CPP-ACP nanocomplexes
on approximal caries determined using digital bitewing radiography. Caries Res. 42,
171 184.
Mortazavi, V., Nahrkhalaji, M.M., Fathi, M.H., Mousavi, S.B., Esfahani, B.N., 2010.
Antibacterial effects of sol-gel-derived bioactive glass nanoparticle on aerobic bacteria.
J. Biomed. Mater. Res. A 94A, 160 168.
Moshaverinia, A., Ansari, S., Moshaverinia, M., Roohpour, N., Darr, J.A., Rehman, I., 2008.
Effects of incorporation of hydroxyapatite and fluoroapatite nanobioceramics into conventional glass ionomer cements (GIC). Acta Biomater. 4, 432 440.
Moszner, N., Klapdohr, S., 2004. Nanotechnology for dental composites. Int. J. Nanotechnol.
1, 130 156.
Moszner, N., Salz, U., 2007. Recent developments of new components for dental adhesives
and composites. Macromol. Mater. Eng. 292, 245 271.
Mota, E.G., Oshima, H., Burnett Jr., L.H., Pires, L., Rosa, R.S., 2006. Evaluation of diametral tensile strength and Knoop microhardness of five nanofilled composites in dentin
and enamel shades. Stomatologija 8, 67 69.
Mount, G.J., 1998. Clinical performance of glass-ionomers. Biomaterials 19, 573 579.
Musselman, M., 2003. Composites make large difference in “small” medical, dental applications. Compos. Technol. 9, 24 27.
Najeeb, S., Khurshid, Z., Matinlinna, J.P., Siddiqui, F., Nassani, M.Z., Baroudi, K., 2015.
Nanomodified peek dental implants: bioactive composites and surface modification—a
review. Int. J. Dent. 2015, (Article ID 381759, in press).
Najeeb, S., Khurshid, Z., Zafar, M.S., Khan, A.S., Zohaib, S., Martı́, J.M.N., et al., 2016a.
Modifications in glass ionomer cements: nano-sized fillers and bioactive nanoceramics.
Int. J. Mol. Sci. 17, 1134.
Najeeb, S., Khurshid, Z., Zohaib, S., Zafar, M.S., 2016b. Bioactivity and osseointegration of
PEEK are inferior to those of titanium—a systematic review. J. Oral Implantol. 42,
512 516.
Najeeb, S., Zafar, M.S., Khurshid, Z., Siddiqui, F., 2016c. Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J. Prosthodont. Res. 60, 12 19.
Najeeb, S., Khurshid, Z., Agwan, A.S., Zafar, M.S., Alrahabi, M., Qasim, S.B., et al., 2016d.
Dental applications of nanodiamonds. Sci. Adv. Mater. 8, 2064 2070.
Najeeb, S., Zafar, M.S., Khurshid, Z., Zohaib, S., Hasan, S.M., Khan, R.S., 2017.
Bisphosphonate releasing dental implant surface coatings and osseointegration: a systematic review. J. Taibah Univ. Med. Sci. 12, 369 375.
Nanci, A., 2008. Ten Cate’s Oral Histology: Development, Structure, and Function. Mosby,
St. Louis, MO; London.
Naray-Szabo, S., 1930. Structure of apatite (CaF)Ca4(PO4)3. Z. Kristallogr. 75, 387 398.
Noh, H.K., Lee, S.W., Kim, J., Oh, J., Kim, K., Chung, C., et al., 2006. Electrospinning of
chitin nanofibers: degradation behavior and cellular response to normal human keratinocytes and fibroblasts. Biomaterials 27, 3934 3944.
Norowski, P.A., Fujiwara, J., Clem, T., Adatrow, W.C., Eckstein, P.C., Haggard, E.C., et al.,
2015. Novel naturally crosslinked electrospun nanofibrous chitosan mats for guided
bone regeneration membranes: material characterization and cytocompatibility. J. Tissue
Eng. Regen. Med. 9, 577 583.
Oh, T., Yoon, J., Misch, C.E., Wang, H., 2002. The causes of early implant bone loss: myth
or science? J. Periodontol. 73, 322 333.
Nanotechnology and nanomaterials in dentistry
501
Ohkawa, K., Hayashi, S., Kameyama, N., Yamamoto, H., Yamaguchi, M., Kimoto, S., et al.,
2009. Synthesis of collagen-like sequential polypeptides containing O-phospho-Lhydroxyproline and preparation of electrospun composite fibers for possible dental
application. Macromol. Biosci. 9, 79 92.
Paquette, D., Hanlon, A., Lessem, J., Williams, R., 2004. Clinical relevance of adjunctive
minocycline microspheres in patients with chronic periodontitis: secondary analysis of a
phase 3 trial. J. Periodontol. 75, 531 536.
Parizek, M., Douglas, T.E.L., Novotna, K., Kromka, A., Brady, M.A., Renzing, A., et al.,
2012. Nanofibrous poly(lactide-co-glycolide) membranes loaded with diamond nanoparticles as promising substrates for bone tissue engineering. Int. J. Nanomed. 7, 1931.
Park, C.H., Rios, H.F., Jin, Q., Bland, M.E., Flanagan, C.L., Hollister, S.J., et al., 2010.
Biomimetic hybrid scaffolds for engineering human tooth-ligament interfaces.
Biomaterials 31, 5945 5952.
Passeri, D., Rinaldi, F., Ingallina, C., Carafa, M., Rossi, M., Terranova, M., et al., 2015.
Biomedical applications of nanodiamonds: an overview. J. Nanosci. Nanotechnol. 15,
972 988.
Paul, D.R., Robeson, L.M., 2008. Polymer nanotechnology: nanocomposites. Polymer
(Guildf.) 49, 3187 3204.
Pecharroman, C., Bartolomé, J.F., Requena, J., Moya, J.S., Deville, S., Chevalier, J., et al.,
2003. Percolative mechanism of aging in zirconia containing ceramics for medical applications. Adv. Mater. 15, 507 511.
Peh, R.F., Suthikum, V., Goh, C.H., Toh, S.L., 2007. Novel electrospun-knitted silk scaffolds
for ligament tissue engineering. World Congr. Med. Phys. Biomed. Eng. 2006 (4),
3287 3290. Pts 1-6. 14.
Pichayakorn, W., Boonme, P., 2013. Evaluation of cross-linked chitosan microparticles
containing metronidazole for periodontitis treatment. Mater. Sci. Eng. C 33,
1197 1202.
Pihlstrom, B.L., Michalowicz, B.S., Johnson, N.W., 2005. Periodontal diseases. Lancet 366,
1809 1820.
Piñón-Segundo, E., Ganem-Quintanar, A., Alonso-Pérez, V., Quintanar-Guerrero, D., 2005.
Preparation and characterization of triclosan nanoparticles for periodontal treatment. Int.
J. Pharm. 294, 217 232.
Pye, A., Lockhart, D., Dawson, M., Murray, C., Smith, A., 2009. A review of dental implants
and infection. J. Hosp. Infect. 72, 104 110.
Qasim, S.B., Najeeb, S., Delaine-Smith, R.M., Rawlinson, A., Rehman, I.U., 2017. Potential
of electrospun chitosan fibers as a surface layer in functionally graded GTR membrane
for periodontal regeneration. Dent. Mater. 33, 71 83.
Qasim, S.B., Zafar, M.S., Najeeb, S., Khurshid, Z., Shah, A.H., Husain, S., et al., 2018.
Electrospinning of chitosan-based solutions for tissue engineering and regenerative medicine. Int. J. Mol. Sci. 19, 407.
Raggio, D.P., Calvo, A.F.B., Branco, E.C., Bonifácio, C.C., Imparato, J.C.P., Camargo, L.B.,
2009. Knoop hardness of resin-modified glass-ionomer cements. Int. J. Dent. 8,
119 123.
Rahiotis, C., Vougiouklakis, G., Eliades, G., 2008. Characterization of oral films formed in
the presence of a CPP ACP agent: an in situ study. J. Dent. 36, 272 280.
Ranjbar-Mohammadi, M., Zamani, M., Prabhakaran, M., Bahrami, S.H., Ramakrishna, S.,
2016. Electrospinning of PLGA/gum tragacanth nanofibers containing tetracycline
hydrochloride for periodontal regeneration. Mater. Sci. Eng. C 58, 521 531.
502
Advanced Dental Biomaterials
Ravichandran, R., Ng, C.C., Liao, S., Pliszka, D., Raghunath, M., Ramakrishna, S., et al.,
2012. Biomimetic surface modification of titanium surfaces for early cell capture by
advanced electrospinning. Biomed. Mater. 7, 015001.
Ray, S.S., Okamoto, M., 2003. Biodegradable polylactide and its nanocomposites: opening a
new dimension for plastics and composites. Macromol. Rapid Commun. 24, 815 840.
Reynolds, E., 2008. Calcium phosphate-based remineralization systems: scientific evidence?
Aust. Dent. J. 53, 268 273.
Rho, K.S., Jeong, L., Lee, G., Seo, B.M., Park, Y.J., Hong, S.D., et al., 2006. Electrospinning
of collagen nanofibers: effects on the behavior of normal human keratinocytes and
early-stage wound healing. Biomaterials 27, 1452 1461.
Rizvi, A., Zafar, M.S., Farid, W.M., Gazal, G., 2014. Assessment of antimicrobial efficacy of
MTAD, sodium hypochlorite, EDTA and chlorhexidine for endodontic applications: an
in vitro study. Middle East J. Sci. Res. 21, 353 357.
Rizvi, A., Zafar, M., Al-Wasifi, Y., Fareed, W., Khurshid, Z., 2016. Role of enamel deminerlization and remineralization on microtensile bond strength of resin composite. Eur. J.
Dent. 10, 376 380.
Rodrı́guez-Lozano, F.J., GarcÃa-Bernal, D., Aznar-Cervantes, S., Ros-Roca, M., AlguerÃ,
M.C., Atucha, N.M., et al., 2014. Effects of composite films of silk fibroin and graphene
oxide on the proliferation, cell viability and mesenchymal phenotype of periodontal ligament stem cells. J. Mater. Sci. Mater. Med. 25, 2731 2741.
Roveri, N., Battistella, E., Bianchi, C.L., Foltran, I., Foresti, E., Iafisco, M., et al., 2009.
Surface enamel remineralization: biomimetic apatite nanocrystals and fluoride ions
different effects. J. Nanomater. 2009, 8.
Saiz, E., Zimmermann, E.A., Lee, J.S., Wegst, U.G.K., Tomsia, A.P., 2013. Perspectives on
the role of nanotechnology in bone tissue engineering. Dent. Mater. 29, 103 115.
Sakaguchi, R.L., Powers, J.M., 2012. Craig’s Restorative Dental Materials. Elsevier/Mosby,
Philadelphia, PA.
Samprasit, W., Kaomongkolgit, R., Sukma, M., Rojanarata, T., Ngawhirunpat, T.,
Opanasopit, P., 2015. Mucoadhesive electrospun chitosan-based nanofibre mats for dental caries prevention. Carbohydr. Polym. 117, 933 940.
Sato, M., Sambito, M.A., Aslani, A., Kalkhoran, N.M., Slamovich, E.B., Webster, T.J., 2006.
Increased osteoblast functions on undoped and yttrium-doped nanocrystalline hydroxyapatite coatings on titanium. Biomaterials 27, 2358 2369.
Saunders, W.P., Saunders, E.M., 1994. Coronal leakage as a cause of failure in root-canal
therapy: a review. Dent. Traumatol. 10, 105 108.
Setyawati, M.I., Mochalin, V.N., Leong, D.T., 2015. Tuning endothelial permeability with
functionalized nanodiamonds. ACS Nano 10, 1170 1181.
Sheeparamatti, B., Sheeparamatti, R., Kadadevaramath, J., 2007. Nanotechnology: inspiration
from nature. IETE Tech. Rev. 24, 5 8.
Sheikh, Z., Najeeb, S., Khurshid, Z., Verma, V., Rashid, H., Glogauer, M., 2015.
Biodegradable materials for bone repair and tissue engineering applications. Materials 8,
5744 5794.
Sill, T.J., von Recum, H.A., 2008. Electrospinning: applications in drug delivery and tissue
engineering. Biomaterials 29, 1989 2006.
Silva, R.M., Santos, P.H.N., Souza, L.B., Dumont, V.C., Soares, J.A., Santos, M.H., 2013.
Effects of cellulose fibers on the physical and chemical properties of glass ionomer
dental restorative materials. Mater. Res. Bull. 48, 118 126.
Silva, L.H., Belli, R., Lazar, D.R.R., Tango, R.N., Lohbauer, U., Cesar, P.F., 2014. Y-TZP reinforced
with carbon nanotubes: synthesis, microstructure and flexural strength. Dent. Mater. 30, e9.
Nanotechnology and nanomaterials in dentistry
503
Siqueira, J.F., 2001. Aetiology of root canal treatment failure: why well-treated teeth can fail.
Int. Endod. J. 34, 1 10.
Smart, E.R., Macleod, R.I., Lawrence, C.M., 1995. Resolution of lichen-planus following
removal of amalgam restorations in patients with proven allergy to mercury salts—a
pilot-study. Br. Dent. J. 178, 108 112.
Song, W., Yu, X., Markel, D.C., Shi, T., Ren, W., 2013. Coaxial PCL/PVA electrospun nanofibers: osseointegration enhancer and controlled drug release device. Biofabrication 5,
035006.
Stevens, M.M., George, J.H., 2005. Exploring and engineering the cell surface. Interface Sci.
310, 1135 1138.
Subramanian, A., Lin, H.Y., Vu, D., Larsen, G., 2004. Synthesis and evaluation of scaffolds
prepared from chitosan fibers for potential use in cartilage tissue engineering. Biomed.
Sci. Instrum. 40, 117 122.
Suliman, S., Xing, Z., Wu, X., Xue, Y., Pedersen, T.O., Sun, Y., et al., 2015. Release and
bioactivity of bone morphogenetic protein-2 are affected by scaffold binding techniques
in vitro and in vivo. J. Controlled Release 197, 148 157.
Summit, J., Robins, W., Hilton, T., Schwartz, R., 2000. Fundamentals of Operative
Dentistry: A Contemporary Approach. Quintessence Publishing, Chicago, IL; London.
Sun, X., Liu, Z., Welsher, K., Robinson, J.T., Goodwin, A., Zaric, S., et al., 2008. Nanographene oxide for cellular imaging and drug delivery. Nano Res. 1, 203 212.
Tang, J., Han, Y., Zhang, F., Ge, Z., Liu, X., Lu, Q., 2015. Buccal mucosa repair with electrospun silk fibroin matrix in a rat model. Int. J. Artif. Organs 38, 105 112.
Taniguchi, N., 1974. On the Basic Concept of ‘Nano-Technology’ Proceedings of the
International Conference of Production Engineering. Society of Precision Engineering,
Tokyo, Japan.
Ten Cate, A.R., 1994. Oral Histology: Development, Structure, and Function. Mosby,
St. Louis, MO; London.
Ten Cate, J.M., van Duinen, R.N.B., 1995. Hypermineralization of dentinal lesions adjacent
to glass-ionomer cement restorations. J. Dent. Res. 74, 1266 1271.
Terry, D.A., 2004. Direct applications of a nanocomposite resin system: Part 1—The evolution of contemporary composite materials. Pract. Proced. Aesthet. Dent. 16, 417 432.
Thakur, R., Florek, C., Kohn, J., Michniak, B., 2008. Electrospun nanofibrous polymeric
scaffold with targeted drug release profiles for potential application as wound dressing.
Int. J. Pharm. 364, 87 93.
Thorvaldsson, A., Stenhamre, H., Gatenholm, P., Walkenström, P., 2008. Electrospinning of
highly porous scaffolds for cartilage regeneration. Biomacromolecules 9, 1044 1049.
Tomsia, A.P., Launey, M.E., Lee, J.S., Mankani, M.H., Wegst, U.G., Saiz, E., 2011.
Nanotechnology approaches for better dental implants. Int. J. Oral Maxillofac. Implants
26, 25.
Turssi, C.P., Ferracane, J.L., Vogel, K., 2005. Filler features and their effects on wear and
degree of conversion of particulate dental resin composites. Biomaterials 26, 4932 4937.
Tyas, M.J., 2006. Clinical evaluation of glass-ionomer cement restorations. J. Appl. Oral Sci.
14, 10.
Vacanti, N.M., Cheng, H., Hill, P.S., Guerreiro, J.D., Dang, T.T., Ma, M., et al., 2012.
Localized delivery of dexamethasone from electrospun fibers reduces the foreign body
response. Biomacromolecules 13, 3031 3038.
Valiev, R.Z., Zehetbauer, M.J., Estrin, Y., Höppel, H.W., Ivanisenko, Y., Hahn, H., et al.,
2007. The innovation potential of bulk nanostructured materials. Adv. Eng. Mater. 9,
527 533.
504
Advanced Dental Biomaterials
Vallés-Lluch, A., Novella-Maestre, E., Sancho-Tello, M., Pradas, M.M., Ferrer, G.G.,
Batalla, C.C., 2010. Mimicking natural dentin using bioactive nanohybrid scaffolds for
dentinal tissue engineering. Tissue Eng. Part A 16, 2783 2793.
Vallet-Regı́, M., Arcos, D., 2008. Biomimetic Nanoceramics in Clinical Use: From Materials
to Applications. Royal Society of Chemistry.
Venugopal, J., Ramakrishna, S., 2005. Applications of polymer nanofibers in biomedicine
and biotechnology. Appl. Biochem. Biotechnol. 125, 147 157.
Verreck, G., Chun, I., Peeters, J., Rosenblatt, J., Brewster, M.E., 2003. Preparation and characterization of nanofibers containing amorphous drug dispersions generated by electrostatic spinning. Pharm. Res. 20, 810 817.
Waltimo, T., Brunner, T.J., Vollenweider, M., Stark, W.J., Zehnder, M., 2007. Antimicrobial
effect of nanometric bioactive glass 45S5. J. Dent. Res. 86, 754 757.
Wang, W., Ciselli, P., Kuznetsov, E., Peijs, T., Barber, A.H., 2008. Effective reinforcement
in carbon nanotube-polymer composites. Philos. Trans. A Math. Phys. Eng. Sci. 366,
1613 1626.
Warfvinge, K., 1995. Mercury exposure of a female dentist before pregnancy. Br. Dent. J.
178, 149 152.
Wiesmann, H., Meyer, U., Plate, U., Höhling, H., 2004. Aspects of collagen mineralization
in hard tissue formation. Int. Rev. Cytol. 242, 121 156.
Wilson, A.D., Kent, B.E., 1971. The glass-ionomer cement, a new translucent dental filling
material. J. Appl. Chem. Biotechnol. 21, 313.
Xing, Z., Pedersen, T.O., Wu, X., Xue, Y., Sun, Y., Finne-Wistrand, A., et al., 2013.
Biological effects of functionalizing copolymer scaffolds with nanodiamond particles.
Tissue Eng. Part A 19, 1783 1791.
Xu, T., Wu, L., Yu, Y., Li, W., Zhi, J., 2014. Synthesis and characterization of diamond silver composite with anti-bacterial property. Mater. Lett. 114, 92 95.
Xue, J., He, M., Niu, Y., Liu, H., Crawford, A., Coates, P., et al., 2014. Preparation and
in vivo efficient anti-infection property of GTR/GBR implant made by metronidazole
loaded electrospun polycaprolactone nanofiber membrane. Int. J. Pharm. 475, 566 577.
Yang, F., 2004. Fabrication of nano-structured porous PLLA scaffold intended for nerve tissue engineering. Biomaterials 25, 1891.
Yardley, R.M., 1984. Alternatives to amalgam alloys. 2. Br. Dent. J. 157, 434 435.
Zafar, M.S., Al-Samadani, K.H., 2014. Potential use of natural silk for bio-dental applications. J. Taibah Univ. Med. Sci. 9, 171 177.
Zafar, M., Khurshid, Z., Almas, K., 2015a. Oral tissue engineering progress and challenges.
Tissue Eng. Regener. Med. 12, 387 397.
Zafar, M.S., Belton, D.J., Hanby, B., Kaplan, D.L., Perry, C.C., 2015b. Functional material
features of Bombyx mori silk light vs. heavy chain proteins. Biomacromolecules 16,
606 614.
Zafar, M., Najeeb, S., Khurshid, Z., Vazirzadeh, M., Zohaib, S., Najeeb, B., et al., 2016.
Potential of electrospun nanofibers for biomedical and dental applications. Materials 9, 73.
Zafar, M.S., Khurshid, Z., Najeeb, S., Zohaib, S., Rehman, I.U., 2017. Chapter 26—
Therapeutic applications of nanotechnology in dentistry. In: Andronescu, E.,
Grumezescu, A.M. (Eds.), Nanostructures for Oral Medicine. Elsevier.
Zeng, H., Li, F., Wei, H., Shi, J.F., Rao, G.Z., Li, A., et al., 2013. Preliminary study of the
dual release baicalin and rhBMP-2 system to improve periodontal tissue regeneration in
minipigs. Shanghai Kou Qiang Yi Xue 22, 126 131.
Zhang, Y., Ni, M., Zhang, M., Ratner, B., 2003. Calcium phosphate-chitosan composite scaffolds for bone tissue engineering. Tissue Eng. 9, 337 345.
Nanotechnology and nanomaterials in dentistry
505
Zhang, Y., Lim, C.T., Ramakrishna, S., Huang, Z.M., 2005. Recent development of polymer
nanofibers for biomedical and biotechnological applications. J. Mater. Sci. Mater. Med.
16, 933 946.
Zhang, Y., Su, B., Ramakrishna, S., Lim, C., 2007. Chitosan nanofibers from an easily electrospinnable UHMWPEO-doped chitosan solution system. Biomacromolecules 9,
136 141.
Zhang, Q., Mochalin, V.N., Neitzel, I., Knoke, I.Y., Han, J., Klug, C.A., et al., 2011.
Fluorescent PLLA-nanodiamond composites for bone tissue engineering. Biomaterials
32, 87 94.
Zhang, Q., Mochalin, V.N., Neitzel, I., Hazeli, K., Niu, J., Kontsos, A., et al., 2012.
Mechanical properties and biomineralization of multifunctional nanodiamond-PLLA
composites for bone tissue engineering. Biomaterials 33, 5067 5075.
Zhou, Y., Yang, H., Liu, X., Mao, J., Gu, S., Xu, W., 2013. Electrospinning of carboxyethyl
chitosan/poly(vinyl alcohol)/silk fibroin nanoparticles for wound dressings. Int. J. Biol.
Macromol. 53, 88 92.
Zoufan, K., Jiang, J., Komabayashi, T., Wang, Y., Safavi, K.E., Zhu, Q., 2011. Cytotoxicity
evaluation of Gutta Flow and Endo Sequence BC sealers. Oral Surg. Oral Med. Oral
Pathol. Oral Radiol. Endod. 112, 657 661.
19
Digital dentistry
Touraj Nejatian1,2, Sanam Almassi3, Azita Farhadi Shamsabadi4,
Gaurav Vasudeva5,6, Zoe Hancox7, Amritpaul Singh Dhillon9 and
Farshid Sefat7,8
1
Eastman Dental Institute, University College of London, London, United Kingdom,
2
Notthingham Dental Clinic, Nottingham, United Kingdom, 3Almassi Specialist Clinic,
Tehran, Iran, 4Centre for English Language Education, Nottingham University,
Nottingham, United Kingdom, 5School of Dentistry, James Cook University, Townsville,
QLD, Australia, 6Oral Health Services, Hobart, TAS, Australia, 7Biomedical and Electrical
Engineering Department, School of Engineering, University of Bradford, Bradford, United
Kingdom, 8Interdisciplinary Research Center in Polymer Science & Technology (IRC
Polymer), University of Bradford, Bradford, United Kingdom, 9Dental Institute, King’s
College London, London, United Kingdom
Chapter Outline
19.1 Introduction 508
19.2 Digital radiography and magnetic resonance imaging
508
19.2.1 Intraoral, extraoral, including cone beam computed tomography 508
19.2.2 Clinical applications 509
19.2.3 Limitations 512
19.3 Caries detection 516
19.4 Photography and shade selection 516
19.5 Computer-aided design computer-aided manufacturing systems in
dentistry 517
19.5.1
19.5.2
19.5.3
19.5.4
Chairside milling 518
Laboratory and industrial milling 518
Machining of the restorations 519
Three-dimensional printing 519
19.6 Computer-supported implant dentistry
19.6.1
19.6.2
19.6.3
19.6.4
19.6.5
19.6.6
19.6.7
19.6.8
19.6.9
521
Three-dimensional printing in implant dentistry 521
Recent advances in implant technologies 522
Computer-guided implant surgery 524
Computer-navigated implant surgery 524
Computer-aided design computer-aided manufacturing systems in implant restorative
dentistry 527
Prosthetic abutments 528
Computer-aided design computer-aided manufacturing abutments in implant dentistry 528
Materials used 529
Computer-aided design computer-aided manufacturing custom implant abutments 529
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00019-0
Copyright © 2019 Elsevier Ltd. All rights reserved.
508
Advanced Dental Biomaterials
19.7 Lasers and dental applications
530
19.7.1 History of lasers in dentistry 531
19.7.2 Types of lasers 531
19.7.3 Mechanism of laser action 532
19.8 Technology and dental education
References 535
Further reading 540
19.1
533
Introduction
Dentistry like other branches of health science has benefited enormously from digital technologies. Computers are faster and more accurate than their human counterparts. Nowadays almost all aspects of contemporary clinical dentistry from
admission to treatment are assisted by digital technology. Computers have also
helped to balance the cost of dental services despite the increasing price of dental
products and materials. This chapter provides an insight into the various aspects of
dental care which have benefited from digital technology.
19.2
Digital radiography and magnetic resonance
imaging
19.2.1 Intraoral, extraoral, including cone beam computed
tomography
Without computer imaging of the teeth and underlying bone, dentists and orthodontists cannot adequately assess the condition of the mouth. This could mean that a
subgingival tissue could be missed and treatment may be planned without addressing this hidden problem. Noninvasive radiography can provide more detailed
images of the structures inside of the mouth, rather than a dentist merely probing
and examining the teeth and soft tissue by eye. In this section, a variety of dental
imaging techniques will be discussed, later followed by clinical applications and
limitations of these techniques.
Digital radiography is a way of obtaining radiographed scans without the use of
conventional films. To capture an image of a patient’s teeth using conventional
films for a long time requires recording of the image, which increases the dosage of
radiation compared to digital imaging (Masri and Driscoll, 2015). The time is
needed so that the X-rays can combine with the film electrons, and then chemicals
need to be used so that the image can be distinguished (Parks and Williamson,
2002; Ti-Sun et al., 2002). By using digital radiography instead of the conventional
films not only is less waste created as the developing chemicals are not required,
but also time and money are saved for the dental practices (Masri and Driscoll,
2015). For a digital radiograph, the following equipment is needed: a computer
Digital dentistry
509
with an analog-to-digital converter, a digital interface card, an electronic sensor to
react to X-rays, and, finally, an X-ray emitting source.
Digital radiography uses electronic pixels sensors instead of conventional films.
Digital images require the change from analog photos to digital images to show the
picture on a computer screen. This is done by the computer assigning a number to
every single shade between white and black; this is based on the voltage present in
the analog form, with 0 being black and 255 being white and this then creates a
binary image which can be used by dentists (Parks and Williamson, 2002).
Intraoral and extraoral determines whether an X-ray sensor is internally or
externally placed in the mouth. Intraoral radiography is one of the most frequently used assessment techniques by dentists, due to the high-quality image
provided and the ease of adjusting equipment (Vandenberghe et al., 2010).
There are two forms of digital radiography, direct and indirect. The direct
imaging means that the X-ray picture has been stored digitally straight away,
whereas indirect requires analog information to be converted to digital information. Either method can be used for both intraoral and extraoral scanning (Parks
and Williamson, 2002).
Cone beam computed tomography (CBCT) creates images by having an X-ray
source and a detector mounted to moving platforms, these two devices rotate about
a pivot, placed appropriately to circle the area that needs to be imaged. The cone
beam part of the name CBCT comes from the cone-shaped X-ray beam, which is
pointed through a specific location on a patient, depending on the specialists need.
This X-ray is then received by the detector opposite the X-ray source (Scarfe and
Farman, 2008).
MRI is a form of digital imaging that does not involve irradiating a patient,
which enables analysis of soft and to some extent hard tissues. MRI works by picking up the energy emitted from protons located in the atoms of water within the
body. This energy occurs after a magnetic field is introduced to the biological tissue; the protons line up with the magnetic field, then a radio frequency pulse is
applied by the tissue causing the protons to become unaligned from the magnetic
field. When this radio frequency is removed, the protons realign once more and
release energy. This energy is picked up by the MRI machine, and differentiation
between tissues can be shown based on the speed of energy release. Teeth have a
higher density than soft tissues; this means water content is less and so proton
energy is very quickly emitted, resulting in an unclear image as the MRI cannot
pick up the energy fast enough (Idiyatullin et al., 2011).
Extraoral MRI is the most regularly used technique because of its ease and practicality. However, intraoral MRI can also be performed by placing wireless coils
inside the mouth; this provides a more precise image, which is more focused than
common extraoral MRI techniques (Flügge et al., 2016).
19.2.2 Clinical applications
Radiography and MRI can produce three-dimensional (3D) images that can aid a
dentist in decision-making, especially to assess bone quality and structure before
510
Advanced Dental Biomaterials
planning for surgery or implants that improve the outcome for patients. Tables 19.1
and 19.2 give examples of types of digital dental imaging techniques for both
intraoral and extraoral (adapted from Vandenberghe et al., 2010; Cleveland Clinic,
2018; WebMD, Boots, 2018).
CBCT takes only a short amount of time to scan the maxillofacial area, with the
ability to produce a clear image of the bone (Scarfe et al., 2006), allowing dentists
to quickly analyze the situation of the patient’s mouth and act there and then if
required. The resolution of the images can be improved by increasing the thickness
of the image layer/slice taken of the person. CBCT allows cross-sectional images to
be acquired; this is useful for surgical needs, as a dentist can gain knowledge of the
bone quality and structure locations prior to surgery to prepare appropriately
(Vandenberghe et al., 2010), and also allowing the development of implants that
suit the need of the shape of the patients’ mouth. CBCT can assess the hard tissue
within the mouth. This type of radiograph can be used to show the outcomes associated with periodontal diseases, such as bony attachment loss, compared to computed tomography (CT) radiography which lacks the inability to show the
attachment of teeth to the periodontal tissue (Sedentexct.eu, 2012).
Table 19.1 Intraoral digital imaging.
Type of
imaging
technique
Image location
Applications
Occlusal
Can provide an image of the entire
maxillary arch or mandibular arch
Bitewing
Allows imaging of upper and lower
teeth, this type of X-ray shows the
tooth from the crown down to the
top of the bone holding the tooth
Periapical
Gives an image of the whole length of
the teeth on the top or bottom of
the mouth, displaying the crown all
the way to the root attachment to
the bone
Aids orthodontists with the
progression of teeth
movement and development
to correct alignment via the
use of braces
As the bottom and top teeth can
both be seen, areas between
the teeth can be viewed with
ease. Shows bone and teeth
relation, aiding detection of
caries, periodontal disease,
and quality of the
restorations. Also, it can
support dentists with
correctly fitting replacement
restorations such as crowns
Commonly used to show any
abnormalities of root
structures or nearby bone
changes, good for producing
images with reasonable
resolution
Table 19.2 Extraoral digital imaging.
Type of
imaging
technique
Image location
Applications
Tomography
X-ray tube and plate move in
opposite directions, resulting
in a clear focused point. One
layer of an image with other
structures blurred
Panoramic
Gives an image of the whole
mouth including upper and
lower jaws
CT
Shows a 3D image of the mouth,
made up of layers of 2D scans,
from a triangle-shaped ray
CBCT
Rotates around the patients’
head, creating a 3D picture of
both hard and soft tissues
Digital
imaging
Creates a 2D image of a chosen
area on a screen rather than
using film
MRI imaging
Provides a 3D image of the
desired location of the oral and
maxillofacial area
Sialogram
A dye called radiopaque contrast
agent is injected into the
salivary gland, this allows the
X-rays to pick up soft tissue
structures that would not
normally be picked up
Gives an image of the left or
right side of the head
Surrounding structures of an area
that needs to be scanned can be
blocked out so that the
practitioner is able to just see a
focused image of the structures
they what to analyze and
ignore the others
Panoramic X-rays can be used to
help in tumor diagnosis.
However, it is more frequently
used to show teeth positioning,
whether they are visible, still
submerged, or whether they are
impacted
Can be used to find problems in
the bone or face. Enables
discovery of fractures of the
bone, and cysts or tumor
findings
CBCT for dentistry has many
applications, of which will be
discussed further in
Section 19.2.2
Creates very quick images so can
allow quick diagnosis, also can
be zoomed in on giving a
dentist better clarity
There are many applications for
MRI imaging in dentistry,
Section 19.2.2 will go through
this in detail
Allows dentists to uncover any
underlying salivary problems,
such as duct blockages
Cephalometric
projections
Used in orthodontic applications
to examine teeth locations
concerning the patient’s
specific features, allowing
them to make the best
judgment for treatment to
correct teeth positioning
2D, Two-dimensional; 3D, three-dimensional; CBCT, cone beam computed tomography; MRI, magnetic resonance
imaging.
512
Advanced Dental Biomaterials
A study took place involving the use of dry skulls, which had periodontal defects
created artificially imposed on a variety of teeth, using wax to act as soft tissue
(Bagis et al., 2015). All of the skulls had a bite block between the teeth and were
scanned by CBCT equipment and an intraoral X-ray. Experienced dentists were
then asked to identify the defects present, using the images created by both the
intraoral and CBCT techniques. Bagis et al. concluded that CBCT allowed the most
accurate diagnosis to be made, this was due to the clarity of the image and the sensitivity of the equipment compared to the intraoral X-ray techniques used.
Commonly, endodontic imaging uses intraoral radiography techniques at different stages throughout, from a patient diagnosis, during the correction procedure,
and after the procedure to check a patients’ situation. CBCT can be used extraorally, and operating microscopes could be used to reduce radiation dose
(Sedentexct.eu, 2012). Temporomandibular joint disorders can be seen clearly using
MRI, producing a more transparent image than the other radiography methods. The
MRI can also show the alteration of disk placement within the joint (Niraj, 2016).
Due to MRI enabling both hard and soft tissue to be viewed via imaging, a more
in-depth diagnosis can be made as a wider variety of structures can be evaluated.
Although standard MRI has been shown to reduce the resolution of hard tissue
structures, Flügge et al. showed that using an intraoral coil within the mouth
allowed hard tissues to appear clearer and would enable dentists to examine the
structures accurately to make a diagnosis. In abnormality investigations, MRI can
be used to carefully allow a tumor, within the salivary gland, to be identified as
either benign or malignant so further measurement can be taken (Niraj, 2016). This
is useful as the method is completely noninvasive and gives extremely accurate
results. Development of MRI techniques is further improved, using methods such as
Sweep Imaging Fourier Transformations, such developments aim to improve the
quality of bone resolution and increase the availability of these devices to reduce
the amount of patient radiation (Idiyatullin et al., 2011). Advancements of MRI are
promising to reduce the amount of ionizing radiation that dental patients are
exposed to, which is beneficial as dental applications apply more radiation dosage
onto people than any other medical application. Despite the possible inaccuracy of
hard tissue, MRI sometimes can be the only option for dental diagnosis, for example, in some stages of pregnancy where ionizing radiation should avoided due to
the ill effects that it may have on an unborn child. It is also notable that MRI is
used in caries detection, which will be discussed further in its own section later.
19.2.3 Limitations
The radiation dose on a patient can be a limitation itself, as the risks implied from
uncontrolled radiation may be worse than the dental condition itself. Digital technology has reduced the amount of patient radiation. Table 19.3 shows the approximate range of radiation dose that can be present from the different types of digital
imaging techniques used in dentistry. This data is only a rough estimate of the
ranges, these ranges can depend on the equipment/system brands and can be
Digital dentistry
513
Table 19.3 The radiation dose received for different types of dental imaging techniques.
Type of digital imaging
technique used in
dental application
Approximate radiation dose received by patient
(Sieverts, Sv)
Intraoral digital imaging
Bitewing imaging
Entire mouth imaging
,1.5 µSv (Sedentexct.eu, 2012)
5 µSv, with a skin dose of 26 µSv (Ritenour and Gibbs, 2010)
34.9 170.7 µSv, with skin dose of B107 µSv and thyroid
dose of B330 µSv (Ritenour and Gibbs, 2010)
29 477 µSv (Scarfe and Farman, 2008) and can reach
1073 µSv if the field of view is increased (Sedentexct.eu,
2012)
2.7 24 µSv (Sedentexct.eu, 2012) with a thyroid dose of
B42 µSv and skin dose of B5 µSv (Ritenour and Gibbs,
2010)
0 Sv
CBCT
Panoramic radiography
MRI
CBCT, Cone beam computed tomography; MRI, magnetic resonance imaging.
different based on the area in which the X-ray is applied to, as tissues of varying
densities can undergo less or more radiation than other areas (Sedentexct.eu, 2012).
The two main units for radiation dose that are commonly used are Gray (Gy)
and Sieverts (Sv), Gray is the unit given to state the skin or organ absorption of
radiation which is measured in joules per kg, whereas Sieverts is the unit used to
measure equivalent dosage of various radiation sources (e.g., gamma or beta) within
the body (Masri and Driscoll, 2015). The 2007 recommendations of the
International Commission on Radiological Protection (from here on abbreviated to
2007RICRP) states that there is a division between the types of the effects that radiation can have on a person; this can be either a deterministic effect or a stochastic
effect. A deterministic effect is only when a radiation level has been exceeded will
cell death or fault occur, whereas stochastic effects are from the damage to genetic
material commonly resulting in impacts on cell mutation. In both types of these
effects, insignificant results are shown for radiation below 100 mSv; under this
value 2007RICRP does not believe that health risks can occur to adults. Above
100 mSv there has been evidence to show that the risk of carcinogenesis increases
linearly to that of radiation increase. Although to be on the cautious side,
2007RICRP recommended that over a 5-year period a maximum of 20 mSv is the
most a patient should be exposed to each year and that one single dose should be
no more than 50 mSv at a time (2007). There are a variety of calculations that can
be done to find the maximum dose of radiation a person should undergo, this takes
into consideration variables such as age, gender, weight, health condition, and
many more factors such as genetic conditions, working out an individual’s risk
when exposed to radiation (2007RICRP). It should be noted that younger people
(under 10 years old) have more radiosensitive tissues and can be three times as susceptible to radiation consequences than people over 80 years old (Sedentexct.eu,
2012).
514
Advanced Dental Biomaterials
Due to the possible outcomes of too much radiation, it is sensible for dental professionals to limit and reduce the number of exposures patients received from digital
radiography. Some methods are used to reduce the amount of radiation exposure, the
system itself and radiographers can perform these measures. X-ray beams can turn
on and off to work in time to the capturing from the detector, this reduces radiation
to a patient rather than an unnecessary constant beam, while maintaining image quality (Scarfe and Farman, 2008). FDI World Dental Federation also suggests several
other methods for exposure reduction. These include ensuring the beam is of the
smallest possible diameter and accurately setting the alignment up to get the correct
area, taking care on the first exposure to reduce the likelihood of necessary retakes,
and wearing leaded aprons and thyroid collars to minimize tissue exposure in other
areas. On top of that, the radiographer should take their safety into consideration too,
they should either leave the room and remotely switch on the X-ray, or stand behind
a protective screen (FDI World Dental Federation, 2018). Radiograph operators can
also wear a badge that shows how much radiation they have been exposed to, so they
can stay within the safe limit when working with X-rays.
Comparisons of radiographic measurement techniques to the intrasurgical assessment of patients with periodontal disease have taken place to analyze the difference
in the interproximal bone loss. One study compared linear measurement (LMSRT)
and FRIACOM (a type of computer-assisted analysis device to compare radiographic images) as their computer-assisted analysis devices against intrasurgical
assessment (Kim et al., 2002). Using statistical methods to find the difference
between these assessments, they showed that the computer-assisted analysis methods overestimated bone loss when calculating the distance between the cementoenamel junction to the alveolar crest, by approximately 1.5 2 mm. On the other hand,
LMSRT and FRIACOM appeared to be reliable and produce the same results as
each other. Another study compared LMSRT to a loupe, in this case, these two
techniques underestimated interproximal bone loss in comparison with intrasurgical
methods (Eickholz et al., 1998). Digital X-ray systems utilize different types of sensors including charged-coupled device (CCD), photostimulable phosphor plates
(PSP), or complementary metal oxide semiconductor active pixel sensor (CMOSAPS). These sensors used for direct digital imaging have various disadvantages and
limitations. CMOS sensors can only create an image over a small area and have
noise that hinders the quality, therefore reducing diagnosis ease. Hygiene is vital
for CCD usage as otherwise infections could spread between patients. This requires
the sensors to be covered with a clean protective material, and for every patient,
this cover needs to be replaced. CCDs can be uncomfortable when used intraorally
and because of this more X-rays may need to be taken due to patient movement
(Parks and Williamson, 2002). PSP can be made to a variety of sizes meaning the
patient’s comfort can be improved, and fewer retakes are needed (Vandenberghe
et al., 2010), PSP is an indirect system however and so can result in information
lost when converting from analog-to-digital images.
Intraoral digital radiography sometimes can, unfortunately, result in an unclear
picture; this is from the appearance of overlapping structures within the mouth in
Digital dentistry
515
the form of a two-dimensional (2D) image. Similar to intraoral digital radiography,
extraoral 2D photos are commonly overlapping, blurry, and can be misleading due
to the magnification differences present (Vandenberghe et al., 2010).
CT and CBCT both cannot display soft tissue. Clearly, this means the investigation of issues with soft tissues such as dental pulp, mucosa, and the neurovascular
bundle cannot be explored with clarity (Flügge et al., 2016).
Image intensifier tubes (IIT) and CCDs can be used in unison for CBCT imaging, or flat-panel imagers can be used for detectors, these are indirect imaging
methods. IITs compared to flat-panel detectors can produce falsifications, in turn
causing an unreliable result. Flat-panel detectors can sometimes produce incorrect
pixelations; however, this can be easily corrected by these pixels being replaced
digitally to appear as a mean pixel based on the surrounding pixels (Scarfe and
Farman, 2008).
Despite CBCT having an improved image quality compared to intraoral X-rays,
CBCT should not replace the use of intraoral X-rays, this is because CBCT inflicts
a higher dose of radiation onto patients (Bagis et al., 2015). Therefore CBCT should
only be used in cases where intraoral X-rays are inadequate or where the risk of
radiation dose outweighs the risk of dental problems. Also, if a dentist wishes to
analyze soft tissue, CBCT is an unwise choice as soft tissue image quality is low
due to noise so that the only bone can be picked up clearly (Scarfe and Farman,
2008). The areas that sustain the highest dose of radiation, when using CBCT for a
dental application, are the salivary glands and thyroid (Sedentexct.eu, 2012), this
definitely indicates that it would be sensible to distribute a protective thyroid collar
to patients undergoing CBCTs.
MRI is less commonly used in dentistry; this is due to the cost and size of
MRI machines, also scanning the patient can take a long time. Image quality for
hard tissues is not as good as that of soft tissues, hindering the usability of MRI,
as often bone and enamel examinations need to be determined more importantly
(Flügge et al., 2016). It should also be noted that patients may be claustrophobic
and placing them in a confined MRI machine may cause them to move; this
movement may distort the imaging and require longer imaging time (Niraj, 2016).
Although MRI does not emit damaging radiation, some very powerfull types of
MRI can create such strong magnetic filed that moves magnetizable objectes
uncontroablly towards the machine within the same room. Unfortunately, this
means that patients with metal implants cannot have this type of MRI, otherwise
these implants may be dislodged (Magnetic Resonance Imaging (MRI) National
Institute of Biomedical Imaging and Bioengineering, 2018). Commonly, dental
fixtures are made of magnetic materials and need to be assessed before an MRI
can take place; examples of these restorations that might cause health concerns if
used in MRI include orthodontic braces, crowns, and dentures (Mathew et al.,
2013). In particular, it is necessary to emphasize the importance of undergraduate
dental students knowing what types of implants are magnetic, so that they can
avoid health risks, which could be as severe as a ferromagnetic implant being
pulled out of the body by the magnetic field.
516
19.3
Advanced Dental Biomaterials
Caries detection
Caries is the most common chronic disease in the world, and its diagnosis forms an
essential skill the dental healthcare professional must master. However, their early
reliable and predictable diagnosis remains one of the most challenging conditions in
dentistry. Traditional methods of caries detection involve visual and tactile examination of the tooth surface with the use of air drying and probes, respectively.
Radiographs using the bitewing technique are most commonplace in practice to
identify and monitor carious lesions of a tooth, as well as help assess any existing
restorations and surrounding bone levels, all of which cannot be detected solely by
visual inspection. Automated computer diagnosis of dental radiographic imaging
has been of limited success; the image analysis is a 2D representation of a 3D tissue; it, therefore, requires an evaluation by the practitioner to then achieve a
computer-aided diagnosis (Masri and Driscoll, 2015). Nevertheless, the accuracy
with which dental caries is identified remains to be significantly improved, leading
to the market demand for a technology which can successfully detect caries. The
introduction of the International Caries Assessment and Detection System (ICADS)
over 10 years ago highlighted the importance of having a universal framework for
grading caries within a tooth and has subsequently allowed for comparisons on the
performance of different technologies. Light fluorescence technology has undergone much research and development; it involves measuring the difference in the
amount of light reflected off a sound and carious tooth surface. A significant drawback is that any plaque or staining could distort the result and therefore it is necessary to ensure the tooth is cleaned thoroughly before assessment (Gomez, 2015). A
further variation of this technology is to direct infrared light at the tooth surface
and use a digital camera to measure the amount of light which passes through
(healthy enamel) or scatters in all directions because of caries or demineralization
present.
19.4
Photography and shade selection
Advances in computer, camera, and Internet technology have hugely changed modern society. With an ever-increasing demand for improved esthetics in dentistry,
numerous technologies have been developed to improve shade analysis, laboratory
communication, dental material selection, as well as reproduction, and, finally, verification in the clinical setting (Chu et al., 2010). Successful shade matching is both
art and science combined with any mistakes potentially being costly. It is an important yet difficult task being a matter of color perception and subjective interpretation. Objectively, there are three components to shade: “hue” is the color, “chroma”
is the intensity of the hue, and “value” is the brightness of the hue. The most commonly used shade-matching technique is a visual method using a Vitapan Chart system (Chu et al., 2010). This involves the dentist holding a series of colored tabs of
distinctive shades next to the patient’s teeth. However, there are strict conditions to
Digital dentistry
517
try and improve the accuracy of color perception; the patient must be sat upright
and assessed at eye level at a conversational distance, nonfluorescent color corrected light should be used, and the teeth kept hydrated. Spectrophotometer technologies available on the market offer a greater accuracy with color matching over the
human eye (Chu et al., 2010). They work by measuring the quality of light reflected
off the tooth’s surface. The main limitation, however, is that the software will average out the color data received for a given area leading to inaccuracies and major
errors where the tooth exhibits translucency, especially around the tooth’s edges
(Chu et al., 2010; Tam and Lee, 2017).
Digital camera and imaging systems are prevalent devices from single-lens
reflex cameras to smartphones. They offer an alternative to color matching and
measurement instruments with the significant advantage of communicating color
distribution and dental morphology (Tam and Lee, 2012). Computer software can
analyze images and compare the shade of the teeth with reference shade tabs adjacent to the teeth in the oral cavity. The use of consumer smartphone cameras allows
for easier and immediate wireless communication with the laboratory to fabricate
dental prostheses which not only match in color but also compliment the natural
dentition in shape and design (Tam and Lee, 2012, 2017). Furthermore, the use of
camera technology alongside a shade reference is playing an increasing part in
monitoring those undergoing tooth whitening (Chu et al., 2010).
19.5
Computer-aided design computer-aided
manufacturing systems in dentistry
Dr. Duret in 1971 was one of the pioneers to employ an optical impression system
linked to a crown designing and milling system (Miyazaki et al., 2009), which was
later developed into the current computer-aided design computer-aided
manufacturing (CAD CAM) system. A CAD CAM system is generally composed
of three stages of data acquisition, data processing, and machining (Qualtrough and
Piddock, 1995). A 3D image of the prepared tooth can be either recorded directly
using an intraoral scanner or indirectly by scanning either an impression of tooth
replicas, cast, or die. A virtual restoration or coping is designed on the virtual replica using dedicated software. Some CAD CAM systems are equipped with a virtual articulator to help to develop the occlusal surface of the restoration accurately.
The final design is transferred to a milling machine which carves out a coping or a
fully shaped restoration (monolithic restoration) from a high strength ceramic block.
Machining the restoration, which is referred to as “subtractive manufacturing,” can
take place either chairside or in a laboratory or an industrial milling center. Later
the ceramic cores are veneered either by sintering ceramic powders or pressing softened ceramic onto.
The CAD CAM technology has been primarily used to fabricate fixed prosthetic restorations, such as onlays, inlays, veneers, and crowns. Further advancements on CAD CAM during the past decade have provided alternative restorative
518
Advanced Dental Biomaterials
materials such as composite resin, porcelain, and metallic blocks, all of which have
improved the quality of prostheses (Raigrodski, 2004). The CAD CAM system
can now be used for fabrication of implant-supported prostheses and implant abutments (Kucey and Fraser, 2000).
The CAD CAM systems have three major functional components (Strub et al.,
2006):
1. Data gathering or scanning to receive the oral information. To receive this information
there are various trading systems:
a. Intraoral capture. This approach utilizes 3D optical systems to obtain single components anatomy. Some examples include Interférométrie Moire, laser scan, color coding
(e.g., CEREC 79 and Evolution 4D).
b. Anatomical dental duplicate capture (plaster cast), often utilizing a laser scan system.
Some commercial products include RapidForm (RapidForm), Slim (Slim), poly-Works
(polyWorks), and Geometric Studio (Geometric Studio), which are used for the 3D
meshes following the process.
2. The CAD technique for geometric design of the restoration. Such CAD systems have their
own basic functions to modify the geometry of the restoration.
3. The CAM system to fabricate the restoration. The CAM systems utilize information gathered from the computer to outline a physical object, using subtraction methods which
remove the material from a starting block and finalize it to the desired shape, or using
additive methods (rapid prototyping) that are increasingly used in the CAD CAM oral
technology.
Since the introduction of CAD CAM technology in the early 1980s, further
advancements have progressed in three directions, depending on the type of production line: (1) chairside production, for example, Cerec System (Sirona Dental
GmbH; Salzburg, Austria); (2) laboratory production, for example, inEos X5 scanner and inLab MC XL milling unit (Sirona Dental GmbH; Salzburg, Austria); and
(3) centralized fabrication in a production center, for example, Nobel Procera
(Nobel Biocare, Zürich, Switzerland).
19.5.1 Chairside milling
The Cerec system was the first commercially successful chairside CAD CAM system equipped with an intraoral scanner, a computer for designing virtual restoration,
and a chairside milling machine. This system, which was introduced in 1987 by
Sirona, initially could produce ceramic inlays. However, further development of
this system resulted in the production of a range of ceramic and metal restorations.
Joining Dentsply and Sirona provided a new opportunity to develop the system
even more.
19.5.2 Laboratory and industrial milling
Chairside scan and design data or conventionally made impressions can be sent to a
laboratory for machining. Cerec and Planmeca Planmill are two popular
CAD CAM systems used by UK dental labs for milling the restorations out of
Digital dentistry
519
various ceramic blocks and disks. Also, the data could be sent to an industrial milling center, which may be in another country, to design and mill the restorations or
copings and deliver them within a few days. Straumann, Lava 3M, and Nobel
Biocare are examples of industrial machining centers. These systems are classified
as “closed systems” because they only serve their own software processed data,
whereas there are other machining centers such as Zirkonzahn that use “open systems” which are compatible with the main manufacturer’s scanners, software, and
materials.
19.5.3 Machining of the restorations
Final restorations are carved out of presintered block or disks of materials using a
range of burs set by operating computer to work in four or five different axes. The
burs are selected to mill the fitting and external surface of single or multiple
restorations in one run. Multiple axes help in cutting occlusal and fitting surface
detail with more accuracy. Nowadays, various materials including alloys, ceramics,
composites, resins, and waxes are available to be used by CAD CAM machines.
Some of these materials are too hard to mill, therefore to facilitate the milling and
reduce wear and tear of the milling machines and its burs; they are milled in partially sintered forms. After this milling technique that is referred to as “green
machining,” the fully formed restorations are sintered to achieve optimum strength
(Kelly and Benetti, 2011). Milled resin and wax copings or partial denture frameworks are converted to the restorations through conventional techniques. The early
developed single-shaded ceramic blocks barely simulated the natural tooth color,
whereas newly developed multilayered ones offer a better color match. However, to
achieve a good result, operator experience in the correct orientation of the virtual
design on the block is important.
The diameter of the milling bur is a restricting factor in the amount of the detail
that can be produced by the milling systems. Also, the length of the milling burs
limits the depth of the fitting surface of the crown and the height of the preparation
as a result (CEREC, 2016). Generally, it is advised to round the line angles and
avoid preparation of long and parallel axial walls.
19.5.4 Three-dimensional printing
Several industry subsectors including automotive, aerospace, electronics, machinery, and medical products have utilized additive manufacturing (AM) systems
known as 3D printing (3D Printing, 2012). 3D printing, also known as rapid prototyping, is a technology in which objects are fabricated layer by layer at a time.
Layers are added to previous ones until a duplicate of an object is formed
(Fig. 19.1). The technologies associated with the 3D printing have been used
before. However, the “3D printing” concept is quite new and has captured the public’s attention. Mechanically speaking, 3D printers have a simple design. The apparatus could not operate without the presence of the CAD software. The CAD
software allows any object to be virtually reassembled. The CAD is commonly
520
Advanced Dental Biomaterials
Figure 19.1 3D printed fixed metal restorations, copings, and frameworks on one plate.
used in industrial design, manufacturing environments, engineering, and dental laboratories. Some aspects of various dental surgeries can also benefit from this software as well. 3D printing is used to duplicate objects. The CAD software helps us
print objects from scratch. In dentistry and surgery, CT and CBCT provide detailed
volumetric data as well as intraoral or laboratory optical surface scan data. Recent
advancements in CBCT and optical scan technology have significantly improved
various aspects of restorative and implant dentistry.
Fabrication of anatomical “study models” can be one of the primary applications
of 3D printing in the fields of surgery and medical modeling. CBCT access in dental practice has significantly increased over the years and has significantly improved
diagnosis and treatment planning in implant dentistry. CT and CBCT provide us
with volumetric data that is transferred to a 3D printer before the surgery to duplicate a patient’s jaws precisely. A reproduction of the exact anatomy in detail, particularly in complex, atypical, or unfamiliar cases, can be carefully reviewed
beforehand and a suitable surgical approach can be planned accordingly.
Fabrication of implant drill guides necessitates the access to precise 3D printers
and high-resolution printing materials. Unfortunately, some of the ideal materials
that should be incorporated in the fabrication of these drills are not autoclavable.
The traditional precious metal casting has been substituted for more modern materials that are utilized in CAD CAM technology (Bammani et al., 2013). Advantages
associated with CAD CAM include easier manipulation of materials and elimination of labor-intensive artisanal production techniques (Venkatesh and Nandini,
2013). It also enables mass production of restorations and offers more time to dental
technicians to focus on more creative aspects of the fabrication process, including
esthetic layering of porcelain. Incremental layers of polymers, ceramics, or metal
alloys are laid down and fused together using a high-powered laser that is called
selective laser sintering. The term direct metal layer sintering (DMLS) is used
when a laser is used to fuse metal alloy powders. Studies show that Co Cr restorations produced by either milling or SLM systems are less porous microstructurally
and more homogenous than the conventionally casted ones. Also, internal and marginal accuracy of SLM-made restorations are either equal or better than casted
Digital dentistry
521
restorations, whereas milled restorations were the worst. However, the clinical significance of the differences is not clear (Koutsoukis et al., 2015). Several restorations can be made in one run in the same plate, which saves manufacturing time
remarkably (Fig. 19.1). However, the initial cost of 3D laser printing systems are
still more than that of milling systems and the production of metal fumes are potentially more hazardous to health than grinding debris (Dawood et al., 2015). Some
other challenges include the need for meticulous cleaning and difficult
postaccessing.
19.6
Computer-supported implant dentistry
New advances in implant technology have allowed the application of CAD CAM
to improve implant treatment further. In complex cases where the application of
standard abutments is not feasible, CAD CAM technology can be utilized to produce customized implant abutments. Also, customized copings have also been manufactured in such cases to facilitate taking more accurate impressions (Priest, 2005).
Recent advancements in 3D printing and CAD CAM make them suitable means
for making various components of prostheses and planning different phases of
implantation. CBCT can be used in conjunction with CAD CAM technology in
fabricating surgical guides for implant placement. Although it is predicted that 3D
printing technology will eventually produce customized implants with analogs that
closely resemble the roots of the missing teeth, dental implants themselves are still
manufactured using conventional techniques.
19.6.1 Three-dimensional printing in implant dentistry
Fabrication of dental implants is a multistep process including machining of titanium
rods, followed by modification of implant surface design through sandblasting, acidetching, anodization (Choi et al., 2012; Degidi et al., 2012), discrete calcium phosphate crystal deposition (Li et al., 2015), and chemical modifications (Monjo et al.,
2012; Choi et al., 2012; Elias et al., 2012). The goal is to improve implant stability
and increase osseointegration. Clinical studies have demonstrated excellent longterm success or survival rates for rough surface implants (Mangano et al., 2014a;
Degidi et al., 2012; Sesma et al., 2012). The application of conventional methods in
implant dentistry does not allow the construction of a precisely controlled exterior
and interior porous pattern. To address these shortcomings, AM methods have been
proposed (Mullen et al., 2009). DMLS is a laser-based AM technology that employs
powdered metals, radiant heaters, and a computer-controlled laser machine to construct an object by adding layers of material together. This technology uses CAD
data to construct the object without the need for further tooling costs or inventories.
No cutting or milling procedures are involved in this technique, which makes DMLS
an efficient technology with less waste and almost zero loss of material (Mangano
et al., 2009; Dabrowski et al., 2010). There is insufficient evidence on DMLS
522
Advanced Dental Biomaterials
titanium implants within the current literature, even though the AM and DMLS concepts pertaining to implant and biomaterial manufacturing are well accepted. The
application of DMLS technology allows fabrication of patient-specific implants.
DMLS can be used to make custom-made titanium implants, such as root analogs
(Moin et al., 2013; Mangano et al., 2014b) or blade implants (Mangano et al., 2013),
causing more adaptation of the implant to the patient’s anatomy compared with preformed standardized fixtures. 3D printing offers the ability to produce batches of
dental implants of complex geometries highly adaptive to the patient’s bone. Milling
alone is not capable of producing such products; however, the milling/machining
procedures can refine the printed object such as the implant platform. It is possible to
make implants of complex geometry. However, the ultimate insertion of dental
implants with the aid of screws is still the favorable approach.
Although the 3D printing technology concepts are straightforward, the postprocessing concepts are not. There are significant health and safety challenges associated with the fine metal powders and nanoparticle wastes created with 3D printing.
The 3D printers are readily available in many dental laboratories and the associated
postproduction equipment and accessories do not take up much space. Although the
use of 3D printers in the fabrication of any material seems logically possible, the
maintenance of the machine, particularly switching between an implantable metal
and a restorative material, is extremely challenging.
19.6.2 Recent advances in implant technologies
The implant dentistry is nowadays computerized due to the introduction of 3D
imaging, implant-planning software, CAD CAM technology, computer-guided
(CGIS), and computer-navigated implant surgery (CNIS). Implant surgery treatment
planning via 3D computer software enables proper preoperative evaluation of anatomic limitations. In addition, CAD CAM technology allows preoperative planning of implant positions along with virtual implant placement and accomplishment
of the surgical phase through static (guided) or dynamic (navigated) systems.
Presurgical 2D radiograph imaging has traditionally been used to determine
implant position, size, number, direction, and placement of the implant. The guiding
acrylic stents were prepared over duplicated casts of diagnostic wax-up. Limitations
associated with 2D radiography as well as inaccuracies in the fabrication of the
stent or guide channels led to improper implant placement, which may cause complications and eventual implant failures, particularly in anatomically complicated
cases.
3D CT imaging allows scanning of the patient either with fiducial (artificial)
radiographic markers embedded in stents, jaws, etc. or with anatomic (natural) markers that are teeth or bony landmarks. The digital image is taken and imported into
one of the available implant-planning software programs. The data are converted
into a virtual 3D model that replicates the patient’s bone anatomy, making the execution of the surgery and prosthetic treatments accurate. An undistorted 3D view of
the jawbone in axial, sagittal, coronal, panoramic, and cross-sectional views is possible by means of implant-planning software. The software also creates a 3D
Digital dentistry
523
reformatted reconstruction of the jaw. Some additional advantages associated with
this software are as follows (Ganeles et al., 2011; Rubio Serrano et al., 2008):
G
G
G
G
digital planning and fabrication of virtual wax-ups, implant positioning, abutment designing, surgical guidance, fabrication of provisional and final restorations;
predetermining size of the implant, the abutment, and the provisional restoration;
avoiding possible complications due to inaccuracies in the selection of implant size or
positioning during virtual planning by appropriate use of the software; and
helping with treatment planning on dental procedures, for example, alveolectomy, alveoplasty, implant positioning in anatomically challenging cases, visualization of bone quantity in each location and assisting in choosing the ideal donor site for osseous grafts, graft
location, volume and shape of the graft, sinus lift procedures and placement of implants
in a single step, atrophic maxillae treatment, and placement of trans-zygomatic implants.
Even though there are many advantages associated with the use of these software
programs, there are some drawbacks associated with these programs, including the time
required to learn to operate these programs, the high cost associated with investment in
these programs, and the need for accurately localizing natural or fiducial markers in
image data and on cases. There are many commercial software programs available on
the market. Some examples include the following (D’souza and Aras, 2012):
G
G
G
G
G
G
G
G
G
G
G
Procera-Software (Nobel Biocare, Göteborg, Sweden)
coDiagnostiX (IVS Solutions AG, Chemnitz, Germany)
Easy Guide (Keystone-Dental, Burlington, Massachusetts, United States)
SICAT (SICAT GmbH and Co. KG, Brunnenallee, Bonn, Germany)
Virtual Implant Planning (BioHorizons, Birmingham, Alabama, United States)
ImplantMaster TM (I-Dent Imaging Ltd., Hod Hasharon, Israel)
Simplant, SurgiCase (Materialize Inc., Leuven, Belgium)
Implant3D Media Lab Software [Media Lab Srl, Follo (SP), Italy]
DentalSlice (Bioparts, Brazil)
Scan2Guide or S2G (iDent, Ft. Lauderdale, Florida)
Tx Studio software (i-CAT, Imaging Sciences International, Hatfield, Pennsylvania)
In their paper Martins and Lederman (2013) investigated the efficacy of virtual
planning by DentalSlice software and reported the software as being efficient on
treatment planning prototype guides for implant positioning and for quantifying and
locating bone grafts, hence assuring overall higher success rates. Nkenke et al.
(2012) included virtual dental implant-planning software in their undergraduate curriculum after receiving positive feedback from dental students. By means of the
CAD CAM technology, turning the virtual treatment plan into actual patient treatment is possible. This possibility has been applied in two guided surgery systems
that are either static (template-based system) or dynamic (surgical navigation/computer-aided navigation).
Some advantages associated with CAD CAM technology are as follows:
G
G
Minimally invasive surgical procedures with surgical guides (CGIS) for implant placement are better executed with improved predictability.
Immediate loading of the implant is possible by fabricating presurgical master cast and
accurately fitting custom-designed restorations (Spector, 2008; Fortin et al., 2006).
524
Advanced Dental Biomaterials
19.6.3 Computer-guided implant surgery
The static system which takes advantage of a static surgical template/guide to
reproduce virtual implant positioning in the surgical field is divided into two types
depending on the CAD CAM technology used for fabrication of the surgical
guide:
1. static system using rapid prototyping technology and
2. static system using computer-driven drilling technology
Some benefits associated with the application of CGIS and surgical template
include the following (Spector, 2008; Fortin et al., 2006; Nikzad and Azari, 2008):
G
G
G
G
G
G
Directs the osteotomy drills precisely to the location.
Guides the surgeon to the exact location and angulation to place the implant based on the
virtual treatment plan.
Allows flapless surgery, causing less bleeding and swelling, reduced healing time and
postoperative pain.
Promotes the preservation of both hard and soft tissues and maintains sufficient blood
flow to the surgical site.
Avoids disturbing vital structures.
Reduces surgical time.
Even though the CGIS technology is very accurate, still there are some disadvantages associated with it that need further attention. Some drawbacks are as follows
(Neugebauer et al., 2010; Valente et al., 2009):
G
G
G
G
G
G
G
G
G
G
inaccuracies in data acquisition or errors in image processing;
possible deviations from previously planned implant positions/angulation particularly in
coronal and apical portions of the implants;
probable displacement during perforation due to inaccurate fixation of the guide;
mechanical faults caused due to inappropriate angulation of the drills during bone
perforation;
the altered positioning of surgical instruments caused by limited mouth opening;
possible surgical guide fracture;
complicated cases causing unexpected errors;
high costs associated with tools needed such as software programs and surgical templates;
the possibility of thermal injury during placement of implant by using a flapless surgical
approach and application of surgical guides due to reduced access for external irrigation
while preparing the osteotomy site; and
inability in the intraoperative modification of implant positioning.
Due to these drawbacks, the application of this technique needs further caution
and care. However, due to improvements with CNIS many of the mentioned disadvantages associated with CGIS can be ignored.
19.6.4 Computer-navigated implant surgery
CNIS employs a surgical navigation dynamic system that uses CT data to reproduce
the virtual implant position. This is accomplished by an optical bur tracking system
Digital dentistry
525
without a need for an intraoral surgical guide. There are many navigations or positional tracking systems. In CNIS, the natural (fiducial) markers/reference points are
required for registration of the instruments (Neugebauer et al., 2010). Watzinger
et al. (1999) discussed in their case report the application of an optical tracking system for intraoperatively transferring preoperative planning into CT scans as the
implant drill motor caused distortion of the magnetic field and obstructed direct
visualization of the implant socket drilling during application of the electromagnetic
tracking system. The 3D positional data are transferred to a camera or detector
through sensors that are attached to both the patient and the surgical handpiece.
These data make it possible for the computer to instantaneously calculate the virtual
position of instruments relative to the image data. They also allow visualization of
instrument movements in real time to the surgeon through side viewers or advanced
see-through viewers (Winter et al., 2005). Some advantages associated with
computer-CNIS over CGIS include the following (Jung et al., 2009):
G
G
G
G
Permitting intraoperative alterations in implant positioning so that the virtual surgical plan
could be modified during surgery and helping the surgeon navigate the system and visualize the patient’s anatomy at the same time. This allows the clinician to address obstacles
and defects that were not diagnosed preoperatively.
Allowing the drill to be tracked and continuously visualized on the computer screen three
dimensionally (x, y, and z).
Not suffering the limitations associated with CGIS application, that is, thermal injury, displacement, or fracture of the guide.
The image-guided implantology (IGI), a subcategory of the CNIS system, is highly accurate in regard to navigation with an acceptable overall mean spatial navigation error of
0.35 mm (Casap et al., 2004).
Elian et al. have demonstrated the high accuracy of implant placement using the
CNIS system (IGI) by reporting a mean linear accuracy of less than 1 mm at both
the implant neck and apical tip levels. They also showed the mean angular deviation of less than 4 degrees for the implants placed through the CNIS system. In
fact, there was a precise match between the planned implant and the final implant
(Elian et al., 2008). However, a mean linear accuracy ranging between 1.1 and
1.45 mm at the implant coronal third and between 1.41 and 2.99 mm at the implant
apical third along with a mean angular deviation ranging between 2 and 7.25
degrees within implants placed using stereolithographic guides has been illustrated
(Ozan et al., 2009; Di Giacomo et al., 2005). Considering all previous researches
on this subject, it can be assumed that the CNIS system is more accurate than the
CGIS system. One study, however, evaluating the accuracy of optical tracking versus stereolithographic system for implant placement found no significant difference
between the two systems (J et al., 2008). Research conducted in 2014 compared the
accuracy of a dynamic CNIS system with three commercial CGIS static systems
and the application of an acrylic stent for implant osteotomy preparation. The
results illustrated that the static and dynamic systems offered higher accuracy compared to laboratory-made acrylic guides and that both static and dynamic systems
had an average error of less than 2 mm and 5 degrees (Somogyi-Ganss et al., 2015).
526
Advanced Dental Biomaterials
Although the CNIS technology takes advantage of optical tracking systems and is
highly accurate, it still has some limitations (Birkfellner et al., 2008; Widmann and
Bale, 2006):
G
G
G
G
The technology is sensitive to reflections and interference with the line of sight between
the sensors and the cameras. This may cause some inconvenience, particularly with the
common seating arrangement of the dental professional and the assistant, making tracking
of the instruments very challenging.
An expensive technology with an expensive hardware.
Requiring demanding intraoperative referencing.
The significantly high learning curve.
The significant benefit of the technique is the ability to position dental implants
based upon surgical and prosthetic requirements, making the entire surgical procedure safer, faster, and easier. Also, it reduces the postoperative pain and discomfort
of the patient (Greenberg, 2015). Considering all the advantages, the accuracy of
the guided surgery and success rates associated with the procedure are still
controversial.
Guided surgery is the digital workflow upon which the entire implant placement
is virtually treatment planned after the consideration of the unique surgical and
prosthetic needs of the patient. However, this technique has its drawbacks. The
deviation of the implant from a correct position is possible following fabrication of
an inaccurate surgical guide. Hence, the guided surgery is contraindicated in cases
with limited mouth opening within which wrong positioning of the surgical instruments is likely (Gulati et al., 2015). There are three types of surgical guides according to the tissue type used as support: bone, mucosa, or tooth-supported guides. The
bone-supported guide is more precise compared to the other two types because it
offers better visualization of the surgical field. The mucosa-supported guide, on the
other hand, is the most minimally invasive approach, when performing the flapless
surgical technique (Raico Gallardo et al., 2016).
With all the abovementioned limitations, when correctly performed, the technique is quite safe and precise (Katsoulis et al., 2009). The survival rate is comparable to the conventional technique (Hultin et al., 2012). Schneider et al. (2009)
reported different errors and discrepancies that could occur during treatment planning and surgical procedures. It appears that the technique still requires further
improvements to avoid any potential prosthetic complications in the future. Arisan
et al. (2013) investigated the deviation of 108 implants that were placed using
mucosa-supported surgical guides when CT or CBCT was used for virtual planning.
Both CT and CBCT showed comparable deviations (Arisan et al., 2013). Petersson
et al. assessed the accuracy of the technique by comparing the virtually planned
position of implants with the actual implant positions following the surgical procedure. They concluded that a stricter protocol is required to avoid errors and complications (Pettersson et al., 2010).
The precision related to guided surgery depends on the surgical guide’s stability
inside a patient’s mouth (Gulati et al., 2015). There is still controversy among studies pertaining to fidelity presented by surgical guides to transfer the implant
Digital dentistry
527
positioning from virtual planning to the actual location. Instability of the surgical
guide can cause deviations up to 6 mm on implant positioning, particularly in
patients with multiple implants (Widmann and Bale, 2006). The conventional
method has been compared against computer-aided implant surgery when bone and
mucosa-supported guides have been used (Arisan et al., 2010). The authors considered the duration of the surgery and postoperative complications in their comparison. They reported reduced surgical time and postoperative pain and discomfort
following application of the mucosa-supported guides for flapless technique. Vasak
et al. (2011) discussed flapless surgery as a reliable technique since any implant
deviation from the expected position did not exceed the safety distance initially
recommended by the planning software.
Any minor movements of the surgical guide during the surgery can mainly lead
to instability of the template. Di Giacomo et al. (2012) reported a 34% 43% complications from guided surgeries. The potential for implant deviation is higher in
the posterior region, particularly in patients with limited mouth opening, which
challenges the clinician in positioning the surgical guide. Fortin et al. (2000) concluded the technique was an effective mean for complex rehabilitation and minimally invasive surgeries.
19.6.5 Computer-aided design computer-aided manufacturing
systems in implant restorative dentistry
The CAD CAM technology has been applied in restorative dentistry for two decades, and now it has been extended into implant dentistry. This technology was
introduced to restorative dentistry by Francois Duret in 1971 (Duret et al., 1988)
and the first dental CAD CAM restoration was fabricated in 1983 (Priest, 2005).
The CAD CAM can be used to fabricate patient-specific abutments which fit very
well and are more stringent as they incorporate elements such as titanium, alumina,
and zirconium into the abutment. Stereolithography can be utilized to manufacture
CAD CAM surgical templates, which can improve accuracy during implant placement. Stereolithography allows flapless, minimally invasive surgery, accomplishing
immediate functional loading to the implant and delivery of the prosthesis.
The list of products which can be fabricated by the CAD CAM technique
depends on the respective production system. Some milling machines can produce
ZrO2 frames, while more sophisticated units can accommodate a variety of materials including metals, glass ceramics, resins, and high-performance ceramics. The
glass ceramic blocks are grindable silica materials with high stability values.
Lithium disilicate ceramic blocks are critical silica-based materials which can be
used for the production of full anatomical crowns and copings in both anterior and
posterior locations and for three-unit FPD frameworks in the anterior region
because of the high mechanical stability, equivalent to 360 MPa, of this material
(Sorensen et al., 1998; Taskonak and Sertgöz, 2006). High-performance oxide ceramics are categorized into two groups: aluminum oxide (Al2O3) and yttriumstabilized zirconium oxide (ZrO2, Y-TZP), a high-performance oxide ceramic that
528
Advanced Dental Biomaterials
in comparison with other all-ceramic materials, express better mechanical properties, high flexural strength of 900 1200 MPa, and higher fracture toughness of
6 10 MPa (Komine et al., 2010; Kunii et al., 2007).
19.6.6 Prosthetic abutments
For various reasons, the application of CAD CAM technology in implant dentistry is increasing. First, the implant frameworks produced by CAD CAM systems are made out of a solid and homogeneous block of material with high
mechanical properties. Second, since no waxing, investing, or casting procedure
is involved, the chances of any errors or inaccuracies are minimal. Due to this
reason, the overall production costs are reduced. Also, by application of
CAD CAM technology, any potential for unfavorable implant angulations is
minimized, and an appropriate emergence profile is accomplished. Furthermore,
the ceramic abutments fabricated by CAD CAM have optimal optical properties similar to natural dentition with expected highly esthetic results for the surrounding soft tissues. Preferably, the abutment head must be similar to a
prepared tooth with good stability, morphology, and emergence profile. The
appropriate positioning of the implant and proper manipulation of hard and soft
tissues are of importance in producing ideal emergence profile, function,
esthetics, and periodontal health.
19.6.7 Computer-aided design computer-aided manufacturing
abutments in implant dentistry
The custom abutments which have been produced via CAD CAM technology have
advantages compared with stock and laboratory processed custom abutments
(Priest, 2005). Similar to laboratory-made abutments, CAD CAM-fabricated custom abutments are specific for each patient. It is easier for a technician to learn and
employ this technique than that of handmade components. By using CAD software,
the laboratory technician has control over abutment design. The virtual abutment
design is electronically transferred into a CAM milling machine so that the abutment can be fabricated out of a block of selected material. With this approach, any
dimensional inaccuracies related to waxing, investing, and casting are omitted. In
contrast to stock or cast custom abutments, the surfaces of abutments fabricated
from CAD CAM system do not require further modifications following the
machining procedure due to their high precision and fitness. The cost associated
with implant abutment manufacturing with CAD CAM technology lies somewhere
between the cost of fabrication for a stock and cast abutment. As the use of
CAD CAM technology grows over time, the cost will most probably drop.
However, the labor and laboratory costs are most likely going to increase. The overall effect would be that the cost of prepared stock abutments or handmade cast custom abutments is going to escalate.
Digital dentistry
529
19.6.8 Materials used
Metals such as titanium and titanium alloys as well as ceramics such as aluminum
oxide and zirconium oxide have been used in CAD CAM technology to fabricate
implant abutments (Sherry et al., 2007). The longevity of the restorations fabricated
by CAD CAM has increased with the incorporation of such materials of high
strength and quality, making this technology favorable among dentists. Some products include CEREC 3D (Sirona Dental Systems) (CEREC 3D), Everest (Everest),
and Lava (LAVA).
19.6.9 Computer-aided design computer-aided manufacturing
custom implant abutments
Many types of implants employ these forms of abutments (Raigrodski, 2004). The
process is initiated by using CAD CAM technology and related software to gather
information from the patient’s mouth. The laboratory technician uses the data to
wax the prosthesis over the corresponding abutment and then scans it. The antagonist arch is used to adapt the structure and the emergence profile. The collected
data is then transported to the CAM center so that the designed abutment is milled,
and the ceramic is added (Raigrodski, 2004).
Recently, with the exception of the external or internal hex, this method has
been extensively used to design and fabricate the implant abutment. The available
CAD software programs are supplied with databases which can be used to select
the abutment. Another choice is to scan and enter the data into the software to
achieve the desired shape and design. The designed outline can then be altered
depending on the complexity and uniqueness of the case. The digital data is transported to a milling machine that is attached to a computer. This data is used to mill
the abutment from a solid block of titanium alloy. The shape and fit of the abutment
are then evaluated on the cast (Schneider et al., 2009). A few examples of the commercially available CAD CAM abutment systems include the following:
G
G
G
Cerec (Sirona, Patterson Dental Co., Milwaukee, Wisconsin), Atlantis Abutments
(Atlantis Components, Inc., Cam-bridge, Massachusetts), and Encode Restorative System
(3i Implant Innovations Inc., Palm Beach Gardens, Florida)
Computer-aided design and computer-assisted manufacturing
Manufacturing of prosthetic implant dentistry
Nowadays there are various CAD CAM systems available in the market that
can be used in implant dentistry. Some examples include the following:
G
G
G
G
G
G
CAD CAM Custom Implant Abutment Systems.
The Procera system (Nobel Biocare).
The Atlantis abutment (Astra Tech).
CARES (Computer-Aided Restoration Service; Straumann).
Etkon is another available CAD CAM system which supports the prosthetic portfolio of
the Straumann dental implant.
CAD CAM Custom Implant Frameworks Systems.
530
G
G
G
G
Advanced Dental Biomaterials
Procera (Nobel Biocare).
CAM StructSURE precision milled bars (Biomet 3i).
BioCad milled bars (BioCad Medical).
Etkon System.
Implant frameworks are divided into four groups depending on the fabrication
technique employed: first, the conventional cast frameworks; second, the frameworks produced from carbon/graphite fiber-reinforced polymethylmethacrylate
(Björk et al., 1986); third, the laser-welded titanium frameworks (Jemt and Linden,
1992); and finally the most recent, the CAD CAM milled frameworks (Ehrenkranz
et al., 2008; Kupeyan et al., 2006).
A precise virtual model can be designed by using intraoral optical or laboratory
scanners of a prepared tooth, implant position, and the dental arch. The
CAD CAM technology can also be used in treatment planning of various aspects
of fixed and removable prosthodontics. The scanned data and CAD design are used
in milling or printing crown or bridge copings, implant abutments, and dental
bridges.
The 3D printing can be applied in producing metal structures (Kruth et al., 2005)
either directly from metals or metal alloys or indirectly from printing in burnout
resins or waxes for a lost-wax process. Printing in resin or wax and then incorporating a traditional casting approach is advantageous because there is not much need
for postprocessing procedures compared to the direct 3D printing of metals
(Kasparova et al., 2013). In fact, the procedure of casting alloys and facilities is
quite routine in dentistry. Some downsides associated with direct printing in metals
or metal alloys include higher costs, health and safety concerns, and the need for
extra postprocessing care (Ortorp et al., 2011). The 3D printing and the milling/
machining technologies can be used in combination to fabricate a mechanical connection to the implant with high accuracy: reproduction of complex geometry with
slight waste due to the application of 3D printing and fabrication of high-precision
mechanical connecting surfaces due to the application of milling/machining technology. Although the milling procedure causes some waste of the material, it has
advantages because the incorporated material is homogeneous and undisturbed by
operating procedures. In fact, the cost is significantly lower, and there is little
requirement for postprocessing procedures.
19.7
Lasers and dental applications
Lasers in dentistry are not new, but their clinical applications have evolved and
diversified in the past decade, making it very popular in a wide range of dental
treatments. Lasers give dentists the capability to perform a variety of hard and soft
tissue procedures with improved patient outcomes, fewer traumas, and reduced
postoperative complications. This new technology dramatically expands the scope
of methods a dentist can offer their patients.
Digital dentistry
531
19.7.1 History of lasers in dentistry
The term LASER is an acronym for “light amplification by the stimulated emission
of radiation” and was first introduced to the public in 1959, in an article by a
Columbia University graduate student Gordon Gould (Gross and Hermann, 2007).
Theodore Maiman, at the Hughes Research Laboratories in Malibu, California, built
the first functioning laser by using a mixture of helium and neon. A laser generated
from crystals of yttrium aluminum garnet treated with 1% 3% neodymium (Nd:
YAG) was developed in 1961 (Gross and Hermann, 2007) and further led to the
development of the argon laser in 1962. The ruby laser became the first medical
laser to coagulate retinal lesions when it was used in 1963 (Gross and Hermann,
2007). In 1964 Patel at Bell Laboratories developed the CO2 laser (Gross and
Hermann, 2007). The first reported oral surgical application using a CO2 laser
occurred in 1977 (Lenz et al., 1977). Because of the thermal nature of these soft tissue lasers, injections were required in most cases. In January 1987 the first FDA
clearance for a CO2 laser used in oral surgery paved the way for the acceptance and
viability of using lasers in the oral cavity in a clinical environment. Dr. Terry
Meyers and his brother William, an ophthalmologist, selected the Nd:YAG laser for
experiments on the removal of incipient caries (Meyers and Meyers, 1985). This set
the stage for all future lasers to be developed and approved.
19.7.2 Types of lasers
19.7.2.1 Carbon dioxide laser
The CO2 laser wavelength has a very high affinity for water, resulting in rapid soft
tissue removal and hemostasis with a very shallow depth of penetration. Although
it possesses the highest absorbance of any laser, disadvantages of the CO2 laser are
its relatively large size and the high cost and hard tissue destructive interactions
(Fujiyama et al., 2008).
19.7.2.2 Neodymium:yttrium aluminum garnet laser
The Nd:YAG wavelength is highly absorbed by the pigmented tissue, making it a
very effective surgical laser for cutting and coagulating dental soft tissues with
good hemostasis. In addition to its surgical applications (Fujiyama et al., 2008),
there has been research on using the Nd:YAG laser for nonsurgical debridement in
periodontal disease control (Aoki et al., 2008) and the laser-assisted new attachment
procedure (Slot et al., 2009).
19.7.2.3 Erbium laser
The erbium lasers have two distinct wavelength options: Er,Cr:YSGG (yttrium scandium gallium garnet) lasers and Er:YAG (yttrium aluminum garnet) lasers.
The erbium wavelengths have a high affinity for hydroxyapatite and the highest
absorption of water in any dental laser wavelengths (Harashima et al., 2005). It is
532
Advanced Dental Biomaterials
the laser of choice for treatment of dental hard tissues but can also be used for soft
tissue ablation (Ishikawa et al., 2008).
19.7.2.4 Diode laser
All diode wavelengths are absorbed primarily by tissue pigment (melanin) and
hemoglobin. The active medium of the diode laser is a solid-state semiconductor
made of aluminum, gallium, arsenide, and, occasionally, indium, which produces
laser wavelengths, ranging from approximately 810 to 980 nm. Conversely, they
are poorly absorbed by the hydroxyapatite and water present in the enamel. They
are useful for specific procedures, such as esthetic gingival recontouring, soft tissue
crown lengthening, exposure of soft tissue impacted teeth, removal of inflamed and
hypertrophic tissue, frenectomies, and photostimulation of some soft tissue lesions
(Hilgers and Tracey, 2004).
19.7.3 Mechanism of laser action
Laser light is a monochromatic light and consists of a single wavelength of light. It
consists of three principal parts: an energy source, an active lasing medium, and
two or more mirrors that form an optical cavity or resonator. Energy is supplied to
the laser system by a pumping mechanism, such as a flash-lamp strobe device, an
electrical current, or an electrical coil. This energy is pumped into an active
medium contained within an optical resonator, producing a spontaneous emission of
photons. Subsequently, amplification by stimulated emission takes place as the
photons are reflected back and forth through the medium by the highly reflective
surfaces of the optical resonator, prior to their exit from the cavity via the output
coupler.
In dental lasers, the laser light is delivered from the laser to the target tissue via
a fiber optic cable, hollow waveguide, or articulated arm. The wavelength and other
properties of the laser are determined primarily by the composition of an active
medium, which can be a gas, a crystal, or a solid-state semiconductor.
The light energy produced by a laser can have four different interactions with a
target tissue (Hilgers and Tracey, 2004; Carroll and Humphreys, 2006): reflection,
transmission, scattering, and absorption. When a laser is absorbed, it elevates the
temperature and produces photochemical effects depending on the water content of
the tissues. When a temperature of 100 C is reached, vaporization of the water
within the tissue occurs, a process called ablation. At temperatures below 100 C,
but above approximately 60 C, proteins begin to denature, without vaporization of
the underlying tissue. Conversely, at temperatures above 200 C, the tissue is dehydrated and then burned, resulting in an undesirable effect called carbonization
(Sulieman, 2005).
The primary chromophores in the intraoral soft tissue are melanin, hemoglobin,
and water, and in dental hard tissues are water and hydroxyapatite. Different laser
wavelengths have different absorption coefficients with respect to these primary tissue components, making the laser selection procedure dependent (Weiner, 2004).
Digital dentistry
533
Depending on the application of various tissues, use of lasers in dentistry can be
categorized as follows:
Soft tissue:
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
Incision, excision, vaporization, ablation, and coagulation of oral soft tissues
Exposure of unerupted teeth
Sulcular debridement
Flap preparation—incision of soft tissue to prepare a flap and expose the bone
Frenectomy and frenotomy
Gingival troughing for crown impressions
Gingivectomy or gingivoplasty
Hemostasis
Implant recovery
Incision and drainage of abscesses
Operculectomy
Oral papillectomies
Reduction of gingival hypertrophy
Soft tissue crown lengthening
Treatment of canker sores, herpetic, and aphthous ulcers of the oral mucosa
Hard tissue:
G
G
G
G
G
G
G
G
G
G
G
G
G
Class I, II, III, IV, and V cavity preparation
Caries removal
Hard tissue surface roughening and etching
Enameloplasty, excavation of pits, and fissures for placement of sealants
Tooth preparation to obtain access to a root canal
Root canal preparation including enlargement
Root canal debridement and cleaning
Cutting bone to prepare a window access to the apex (apices) of the root(s)
Apicoectomy—amputation of the root end
Root end preparation for retrofill amalgam or composite
Cutting, shaving, contouring, and resection of oral osseous tissues
Osteoplasty and osseous recontouring
Ostectomy
Laser technology is constantly refining and evolving itself over years of development. Laser-based photochemical reactions hold a great future for additional applications, particularly for targeting specific cells, pathogens, or molecules. Future
growth is expected to be a combination of diagnostic and therapeutic laser techniques. It is expected that laser technologies will become an essential component of
contemporary dental practice in the future.
19.8
Technology and dental education
Digital technology has been increasingly utilized in dental education. Many
dental schools in the United Kingdom have adopted computer-assisted learning
534
Advanced Dental Biomaterials
tools/platforms such as virtual learning environments, virtual simulators, and
computer-based assessments in their undergraduate and postgraduate education.
E-learning tools made distance learning possible in postgraduate education in the
dental schools. Various learning management systems, such as Blackboard, First
Class, and Luvit, along with various shareware or freeware, such as Moodle platforms, have been commonly used worldwide. In addition to day-to-day practice,
virtual learning environments assist graduates in their professional development
and further education. Advantages such as remote and timeless access make it
possible for students to learn anywhere, at any time, and at their own pace.
Education providers and practitioners and audience can interact and exchange
information while being away from their own place. This is critical when local
access to education sources is either limited by time, distance, or resources.
Education materials can be customized for individuals’ needs, coauthored, shared,
retrieved, or updated easily. Interactive learning, self-assessment, feedback, and
scoring systems, which are embedded in e-learning platforms, encourage studentcentered learning. Fast development of hardware technologies such as smartphones has progressively facilitated accessibility to digital learning environments
(Mattheos et al., 2008). However, the availability of such devices or Internet is
not possible for everybody everywhere. Besides, some dental and dental hygiene
students prefer e-learning as an adjunct learning method along with conventional
classroom teaching, rather than replacing it entirely (McCann et al., 2010); this
method is referred as blended learning.
Along with theoretical subjects, digital technology has been vastly used in teaching, learning, and assessing skills in dentistry. Examples of this type of system are
SIMODONT dental trainer, PerioSim, and Voxel-Man in which tactile sense
(Haptic technology), in combination with 3D graphics, helps in learning the preclinical skills. Clinical scenarios can be fed into the system and students can provide
the treatment in a completely digital environment. These systems simulate visual,
verbal, and tactile senses and the trainee can examine the dummy patient and experience tooth preparation in a virtual environment. This procedure can be observed
and assessed remotely by the tutors and feedback will also be provided. This provides an opportunity to retrieve and review the procedure of the tooth preparation
by the tutor and tutee rather than the final product. However, digital simulators
need further development to mimic the real clinical conditions such as saliva and
water spray, patient movements, and pain, and exercises such as placing restorations
and minor surgeries still need to be incorporated into the systems.
The complexity of learning management systems makes it necessary for the teachers to be familiar with the function of such systems or receive close technical
support to be able to simplify the interface for the users. Also, the content of the
virtual learning environments should be evaluated in terms of validity, accuracy,
and currency through a peer-review procedure and feedback should be collected
from the users to improve the system constantly (McCann et al., 2010). Despite various advantages, some studies have showed that students still prefer conventional
teaching methods over digital interactive systems (Arús et al., 2017).
Digital dentistry
535
References
ICRP. 2007. Preface, executive summary and glossary. Ann. ICRP, 37, 9 34.
3D Printing. 2012. Report on Additive Manufacturing and 3D Printing State of the Industry.
Wohlers Associates, Inc.: Annual Worldwide.
Aoki, A., Mizutani, K., Takasaki, A., Sasaki, K., Nagai, S., Schwarz, F., 2008. Current status
of clinical laser applications in periodontal therapy. Gen. Den. 56, 674 687.
Arisan, V., Karabuda, C., Ozdemir, T., 2010. Implant surgery using bone- and mucosasupported stereolitho-graphic guides in totally edentulous jaws: surgical and postoperative outcomes of computer-aided vs. standard techniques. Clin. Oral Implant Res. 21,
980 988.
Arisan, V., Karabuda, Z., Piskin, B., Ozdemir, T., 2013. Conventional multi-slice computed
tomography (CT) and cone-beam CT (CBC T) for computer-aided implant placement.
Part II: Reliability of mucosa-supported stereolithographic guides. Clin. Implant Dent.
Relat. Res. 15, 907 914.
Arús, N.A., da Silva, A.M., Duarte, R., Silveira, H., Silveira, H., 2017. Teaching dental students to understand the temporomandibular joint using MRI: comparison of conventional and digital learning methods. J. Dent. Educ. 81, 752 758.
Bagis, N., Kolsuz, M.E., Kursun, S., Orhan, K., 2015. Comparison of intraoral radiography
and cone-beam computed tomography for the detection of periodontal defects: an
in vitro study. BMC Oral Health 15, 64.
Bammani, S.S., Birajdar, P., Metan, S.S., 2013. Application of CAD and SLA method in dental prosthesis. AMAE Int. J. Manuf. Mater. Sci. 3, 14 18.
Birkfellner, W., Hummel, J., Wilson, E., Cleary, K., 2008. Tracking devices. In: Peters, T.,
Cleary, K. (Eds.), Text Book of Image-Guided Interventions, first ed. Springer Science.
Björk, N., Ekstrand, K., Ruyter, I., 1986. Implant-fixed, dental bridges from carbon/graphite
fibre reinforced poly(methyl methacrylate). Biomaterials 7, 73 75.
Carroll, L., Humphreys, T., 2006. Laser-tissue interactions. Clin. Dermatol. 24, 2 7.
Casap, N., Wexler, A., Persky, N., Schneider, A., Lustmann, J., 2004. Navigation surgery for
dental implants: assessment of accuracy of the image guided implantology system. J.
Oral Maxillofac. Surg. 62, 116 119.
CEREC, 2016. CEREC 3D Preparation Guidelines.
Choi, J.Y., Lee, H.J., Jang, J.U., Yeo, I.S., 2012. Comparison between bioactive fluoride
modified and bioinert anodically oxidized implant surfaces in early bone response using
rabbit tibia model. Implant Dent. 21, 124 128.
Chu, S.J., Rd, T., Rd, P., 2010. Dental color matching instruments and systems. Review of
clinical and research aspects. J. Dent. 38, e2 e16.
Cleveland Clinic 2018. Dental X-rays: Intraoral & Extraoral | Cleveland Clinic. [online]
Available at: https://my.clevelandclinic.org/health/articles/11199-types-of-dental-x-rays
[Accessed 18 Mar. 2018].
Dabrowski, B., Swieszkowski, W., Godlinski, D., Kurzyd-Lowski, K.J., 2010. Highly porous
titanium scaffolds for orthopaedic applications. J. Biomed. Mater. Res. B. Appl.
Biomater. 95, 53 61.
Dawood, A., Marti Marti, B., Sauret-Jackson, V., Darwood, A., 2015. 3D printing in dentistry. Br. Dent. J. 219, 521 529.
Degidi, M., Nardi, D., Piattelli, A., 2012. 10-Year follow-up of immediately loaded implants
with TiUnite porous anodized surface. Clin. Implant Dent. Relat. Res. 14, 828 838.
536
Advanced Dental Biomaterials
Di Giacomo, G., Cury, P., de Araujo, N., Sendyk, W., Sendyk, C., 2005. Clinical application
of stereolithographic surgical guides for implant placement: preliminary results. J.
Periodontol. 76, 503 507.
Di Giacomo, G., Silva, J., Silva, A., Paschoal, G.H., Cury, P., Szarf, G., 2012. Accuracy and
complications of computer-designed selective laser sintering surgical guides for flapless
dental implant placement and immediate definitive prosthesis installation. J. Period.
Ontol. 83, 410 419.
D’souza, K., Aras, M., 2012. Applications of computer-aided design/computer-assisted
manufacturing technology in dental implant planning. J. Dent. Implant 2, 37 41.
Duret, F., Blouin, J., Duret, B., 1988. CAD-CAM in dentistry. J. Am. Dent. Assoc. 117, 715 720.
Ehrenkranz, H., Langer, B., Marotta, L., 2008. Complete-arch maxillary rehabilitation using
a custom-designed and manufactured titanium framework: a clinical report. J. Prosthet.
Dent. 99, 8 13.
Eickholz, P., Kim, T., Benn, D., Staehle, H., 1998. Validity of radiographic measurement of
interproximal bone loss. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 85,
99 106.
Elian, N., Jalbout, Z., Classi, A., Wexler, A., Sarment, D., Tarnow, D., 2008. Precision of
flapless implant placement using real-time surgical navigation: a case series. Int. J. Oral
Maxillofac. Implants 23, 1123 1127.
Elias, C.N., Gravina, P., Silva Filho, C., Nascente, P., 2012. Preparation of bioactive titanium
surfaces via fluoride and fibronectin retention. Int. J. Biomater. 2012, 7.
FDI World Dental Federation 2018. Radiation Safety in Dentistry. [online] Available at:
https://www.fdiworlddental.org/resources/policy-statements-and-resolutions/radiation-safety-in-dentistry [Accessed 23 Mar. 2018].
Flügge, T., Hövener, J., Ludwig, U., Eisenbeiss, A.-K., Spittau, B., Hennig, J., et al., 2016.
Magnetic resonance imaging of intraoral hard and soft tissues using an intraoral coil and
FLASH sequences. Eur. Radiol. 26, 4616 4623.
Fortin, T., Champleboux, G., Lormee, J., Coudert, J., 2000. Precise dental implant placement
in bone using surgical guides in conjunction with medical imaging techniques. J. Oral
Implants 26, 300 303.
Fortin, T., Bosson, J., Isidori, M., Blanchet, E., 2006. Effect of flapless surgery on pain experienced in implant placement using an image-guided system. Int. J. Oral Maxillofac.
Implants 21, 298 304.
Fujiyama, K., Deguchi, T., Murakam, I.T., Fujii, A., Kushima, K., Takano-Yamamoto, T.,
2008. Clinical effect of CO2 laser in reducing pain in orthodontics. Angle Orthod. 78,
299 303.
Ganeles, J., Mandelaris, G., Rosenfeld, A., Rose, L., 2011. Image guidance for implants
improves accuracy and predictability. Compend. Contin. Educ. Dent. 32, 52 55.
Gomez, J., 2015. Detection and diagnosis of the early caries lesion. BMC Oral Health .
Greenberg, A., 2015. Digital technologies for dental implant treatment planning and guided
surgery. Oral Maxillofac. Surg. Clin. N. Am. 27, 319 340.
Gross, A., Hermann, T., 2007. History of lasers. World J. Urol. 25, 217 220.
Gulati, M., Anand, V., Salaria, S., Jain, N., Gupta, S., 2015. Computerized implant dentistry:
advances toward automation. J. Indian Soc. Periodontol. 19, 5 10.
Harashima, T., Kinoshita, J., Kimura, Y., Brugnera, A., Zanin, F., Pecora, J., 2005.
Morphological comparative study on ablation of dental hard tissue at cavity preparation
by Er:YAG and Er,CR:YSGG lasers. Photomed. Laser. Surg. 23, 52 55.
Hilgers, J., Tracey, S., 2004. Clinical uses of diode lasers in orthodontics. J. Clin. Orthod. 38,
266 273.
Digital dentistry
537
Hultin, M., Svensson, K., Trulsson, M., 2012. Clinical advantages of computer guided
implant placement: asystematic review. Clin. Oral Implants Res. 23, 124 135.
Idiyatullin, D., Corum, C., Moeller, S., Prasad, H.S., Garwood, M., Nixdorf, D.R., 2011. Dental
magnetic resonance imaging: making the invisible visible. J. Endod. 37, 745 752.
Ishikawa, I., Aoki, A., Takasaki, A., 2008. Clinical application of erbium:YAG Laser in periodontology. J. Int. Acad. Periodontol. 10, 22 30.
Jemt, T., Linden, B., 1992. Fixed implant-supported prostheses with welded titanium frameworks. Int. J. Periodontics Restorative Dent. 12, 177 184.
Jung, R., Schneider, D., Ganeles, J., Wismeijer, D., Zwahlen, M., Hämmerle, C., 2009.
Computer technology applications in surgical implant dentistry: a systematic review.
Int. J. Oral Maxillofac. Implants 24, 92 109.
Kasparova, M., Grafova, L., Dvorak, P., Dostalova, T., Procházka, A., Kakawand, S., et al.,
2013. Possibility of reconstruction of dental plaster cast from 3D digital study models.
Biomed. Eng. Online 12, 49.
Katsoulis, J., Panzera, P., Mericske-Stern, R., 2009. Prosthetically driven, computer-guided
implant planning for the edentulous maxilla: a model study. Clin. Implant Dent. Rel.
Res. 11, 238 244.
Kelly, J.R., Benetti, P., 2011. Ceramic materials in dentistry: historical evolution and current
practice. Aust. Dent. J. 56 (Suppl. 1), 84 96.
Kim, T., Benn, D., Eickholz, P., 2002. Accuracy of computer-assisted radiographic measurement of interproximal bone loss in vertical bone defects. Oral Surg. Oral. Med. Oral
Pathol. Oral Radiol. Endod. 94, 379 387.
Komine, F., Blatz, M., Matsumura, H., 2010. Current status of zirconia-based fixed restorations. J. Oral Sci. 52, 531 539.
Koutsoukis, T., Zinelis, S., Eliades, G., Al-Wazzan, K., Rifaiy, M.A., Al Jabbari, Y.S., 2015.
Selective laser melting technique of Co-Cr dental alloys: a review of structure and properties and comparative analysis with other available techniques. J. Prosthodont. 24,
303 312.
Kruth, J., Vandenbroucke, B., Van Vaerenbergh, J., Naert, I., 2005. Digital manufacturing of
biocompatible metal frameworks for complex dental prostheses by means of SLS/SLM.
In: Proceedings of the Second International Conference on Advanced Research in
Virtual and Rapid Prototyping, Leiria.
Kunii, J., Hotta, Y., Tamaki, Y., Ozawa, A., Kobayashi, Y., Fujishima, A., et al., 2007.
Effect of sintering on the marginal and internal fit of CAD/CAM-fabricated zirconia frameworks. Dent. Mater. J. 26, 820 826.
Kupeyan, H., Shaffner, M., Armstrong, J., 2006. Definitive CAD/CAM-guided prosthesis for
immediate loading of bone-grafted maxilla: a case report. Clin. Implant Dent. Relat.
Res. 8, 161 167.
Li, J., Pow, E., Zheng, L., Ma, L., Kwong, D., Cheung, L., 2015. Effects of calcium phosphate nanocrystals on osseointegration of titanium implant in irradiated bone. Biomed.
Res. Int. 2015, 6.
Mangano, C., Piattelli, A., Mangano, F., Perrotti, V., Iezzi, G., 2009. Immediate loading of
modified acid etched dental implants in postextraction sockets: a histological and histomorphometrical comparative study in nonhuman primate papio ursinus. Implant Dent.
18, 142 150.
Mangano, F., Bazzoli, M., Tettamanti, L., Mangano, C., 2013. Custom-made, selective
laser sintering (SLS) blade implants as a non-conventional solution for the prosthetic rehabilitation of extremely atrophied posterior mandible. Lasers Med. Sci. 28,
1241 1247.
538
Advanced Dental Biomaterials
Mangano, F., Luongo, F., Shibli, J., Anil, S., Mangano, C., 2014a. Maxillary overdentures
supported by four splinted direct metal laser sintering implants: a 3-year prospective
clinical study. Int. J. Dent. 2014, 9.
Mangano, F.G., De Franco, M., Caprioglio, A., Macchi, A., Piattelli, A., Mangano, C.,
2014b. Immediate, non-submerged, root-analogue direct laser metal sintering (DLMS)
implants: a 1-year prospective study on 15 patients. Lasers Med. Sci. 29, 1321 1328.
Martins, R., Lederman, H., 2013. Virtual planning and construction of prototyped surgical
guide in implant surgery with maxillary sinus bone graft. Acta Cir. Bras. 28, 683 690.
Masri, R., Driscoll, C., 2015. Clinical Applications of Digital Dental Technology. Wiley
Blackwell Publishing.
Mathew, C., Maller, S., Maheshwaran, 2013. Interactions between magnetic resonance imaging and dental material. J. Pharm. Bioallied Sci. 5, 113 116.
Mattheos, N., Stefanovic, N., Apse, P., 2008. Potential of information technology in dental
education. Eur. J. Dent. Educ. 12, 85 92.
McCann, A., Schneiderman, E., Hinton, R., 2010. E-teaching and learning preferences of
dental and dental hygiene students. J. Dent. Educ. 74, 65 78.
Miyazaki, T., Hotta, Y., Kunii, J., Kuriyama, S., Tamaki, Y., 2009. A review of dental CAD/
CAM: current status and future perspectives from 20 years of experience. Dent. Mater.
J. 28, 44 56.
Moin, D.A., Hassan, B., Mercelis, P., Wismeijer, D., 2013. Designing a novel dental root
analogue implant using cone beam computed tomography and CAD/CAM technology.
Clin. Oral Implants Res. 24, 25 27.
Monjo, M., Petzold, C., Ramis, J.M., Lyngstadaas, S.P., Ellingsen, E., 2012. In vitro osteogenic properties of two dental implant surfaces. Int. J. Biomater. 2012, 1 14.
Mullen, L., Stamp, R.C., Brooks, W.K., Jones, E., Sutcliffe, C.J., 2009. Selective laser melting: a regular unit cell approach for the manufacture of porous, titanium, bone in-growth
constructs, suitable for orthopedic applications. J. Biomed. Mater. Res. B. Appl.
Biomater. 89, 325 334.
Neugebauer, J., Stachulla, G., Ritter, L., Dreiseidler, T., Mischkowski, R., Keeve, E., et al.,
2010. Computer-aided manufacturing technologies for guided implant placement. Expert
Rev. Med. Devices 7, 113 129.
Nikzad, S., Azari, A., 2008. A novel stereolithographic surgical guide template for planning
treatment involving a mandibular dental implant. J. Oral Maxillofac. Surg. 1446 1454.
Niraj, L., 2016. MRI in dentistry—a future towards radiation free imaging—systematic
review. J. Clin. Diagnostic Res. 10, ZE14 ZE19.
Nkenke, E., Vairaktaris, E., Bauersachs, A., Eitner, S., Budach, A., Knipfer, C., 2012.
Acceptance of virtual dental implant planning software in an undergraduate curriculum:
a pilot study. BMC Med. Educ. 12, 12 90.
Ortorp, A., Jonson, D., Mouhsen, A., Vult Von Steyern, P., 2011. The fit of cobalt-chromium
three unit fixed dental prostheses fabricated with 4 different techniques: a comparative
in vitro study. Dent. Mater. J. 27, 356 363.
Ozan, O., Turkyilmaz, I., Ersoy, A., Mc Glumphy, E., Rosenstiel, S.F., 2009. Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical
guides in implant placement. J. Oral Maxillofac. Surg. 67, 94 401.
Parks, E., Williamson, G., 2002. Digital radiography: an overview. J. Contemp. Dent. Pract.
3, 1 10.
Pettersson, A., Kero, T., Gillot, L., Cannas, B., Faldt, J., Soderberg, R., et al., 2010.
Accuracy of CAD /CAM-guided surgical template implant surgery on human cadavers:
Part I. J. Prosthet. Dent. 103, 335 342.
Digital dentistry
539
Priest, G., 2005. Virtual-designed and computer-milled implant abutments. J. Oral
Maxillofac. Surg. 63, 22 32.
Qualtrough, A.J., Piddock, V., 1995. Dental CAD/CAM: a millstone or a milestone? Dent.
Update 22, 200 204.
Raico Gallardo, Y., da Silva-Olivio, I.R.T., Mukai, E., Morimoto, S., Sesma, N., Cordaro, L.,
2016. Accuracy comparison of guided surgery for dental implants according to the tissue
of support: a systematic review and meta-analysis. Clin. Implant Dent. Relat. Res. 28,
602 612.
Raigrodski, A., 2004. Contemporary materials and technologies for all-ceramic fixed partial
dentures: a review of the literature. J. Prosthet. Dent. 92, 557 562.
Ritenour, E., Gibbs, S., 2010. Dental Patient Doses Information. Health Physics Society.
Rubio Serrano, M., Albalat Estela, S., Peñarrocha Diago, M., Peñarrocha Diago, M., 2008.
Software applied to oral implantology. Med. Oral Patol. Oral Cir. Buca 13, 661 665.
Scarfe, W.C., Farman, A.G., 2008. What is cone-beam CT and how does it work?. Dent.
Clin. 52, 707 730.
Scarfe, W.C., Farman, A.G., Sukovic, P., 2006. Clinical applications of cone-beam computed
tomography in dental practice. J. Can. Dent. Assoc. 72, 75 80.
Schneider, D., Marquardt, P., Zwahlen, M., Jung, R., 2009. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry.
Clin. Oral Implant Res. 20, 73 86.
Sedentexct.eu 2012. Radiation Protection Cone Beam CT for Dental and Maxillofacial
Radiology. [online] Available at: http://www.sedentexct.eu/files/radiation_protection_172.pdf [Accessed 24 Mar. 2018].
Sesma, N., Pannuti, C.M., Cardaropoli, G., 2012. Retrospective clinical study of 988 dual
acid-etched implants placed in grafted and native bone for single-tooth replacement. Int.
J. Oral Maxillofac. Implants 27, 1243 1248.
Sherry, J., Sims, L., Balshi, S., 2007. A simple technique for immediate placement of definitive engaging custom abutments using computerized tomography and flapless guided
surgery. Quintessence Int. 38, 755 762.
Slot, D., Kranendonk, A., Paraskevas, S., Van der Weijden, F., 2009. The effect of a pulsed
Nd:YAG laser in non-surgical periodontal therapy. J. Periodont. 80, 1041 1056.
Somogyi-Ganss, E., Holmes, H., Jokstad, A., 2015. Accuracy of a novel prototype dynamic
computer-assisted surgery system. Clin. Oral Implants Res. 26, 882 890.
Sorensen, J., Choi, C., Fanuscu, M., Mito, W., 1998. IPS empress crown system: three-year
clinical trial results. J. Calif. Dent. Assoc. 26, 130 136.
Spector, L., 2008. Computer-aided dental implant planning. Dent. Clin. North Am. 52, 761 775.
Sulieman, M., 2005. An overview of the use of lasers in general dentist practice, laser wavelengths, soft and hard tissue clinical applications. Dent. Update 32, 286 288. 291 294.
Tam, W., Lee, H., 2012. Dental shade matching using a digital camera. J. Dent. 40 (Suppl.),
e3 e10.
Tam, W., Lee, H., 2017. Accurate shade image matching by using a smartphone camera. J.
Prosthodont. Res. 61, 168 176.
Taskonak, B., Sertgöz, A., 2006. Two-year clinical evaluation of lithia-disilicate-based allceramic crowns and fixed partial dentures. Dent. Mater. 22, 1008 1013.
Ti-Sun, K., Benn, D.K., Eickholz, P., 2002. Accuracy of computer-assisted radiographic measurement of interproximal bone loss in vertical bone defects. Oral Surg. Oral Med. Oral
Pathol. Oral Radiol. Endod. 94, 379 387.
Valente, F., Schiroli, G., Sbrenna, A., 2009. Accuracy of computer-aided oral implant surgery: a clinical and radiographic study. Int. J. Oral Maxillofac. Implants 24, 234 242.
540
Advanced Dental Biomaterials
Vandenberghe, B., Jacobs, R., Bosmans, H., 2010. Modern dental imaging: a review of the
current technology and clinical applications in dental practice. Eur. Radiol. 20,
2637 2655.
Vasak, C., Watzak, G., Gahleitner, A., Strbac, G., Schemper, M., Zechner, W., 2011.
Computed tomography-based evaluation of template (NobelGuidet)-guided implant positions: a prospective radiological study. Clin. Oral Implants Res. 22, 1157 1163.
Venkatesh, K.V., Nandini, V.V., 2013. Direct metal laser sintering: a digitised metal casting
technology. J. Indian Prosthodont. Soc. 13, 389 392.
Watzinger, F., Birkfellner, W., Wanschitz, F., Millesi, W., Schopper, C., Sinko, K., et al.,
1999. Positioning of dental implants using computer-aided navigation and an optical
tracking system: case report and presentation of a new method. J. Craniomaxillofac.
Surg. 27, 77 81.
WebMD Boots 2018. Learn more about dental X-rays. [online] Available at: https://www.
webmd.boots.com/oral-health/guide/dental-x-rays [Accessed 18 Mar. 2018].
Weiner, G.P., 2004. Laser dentistry practice management. Dent. Clin. North Am. 48,
1105 1126.
Widmann, G., Bale, R., 2006. Accuracy in computer-aided implant surgery—a review. Int. J.
Oral Maxillofac. Implants 21, 305 313.
Winter, A., Pollack, A., Frommer, H., Koenig, L., 2005. Cone beam volumetric tomography
vs. medical CT scanners. N. Y. State Dent. J. 71, 28 33.
Further reading
Ruppin, J., Popovic, A., Strauss, M., Spüntrup, E., Steiner, A., Stoll, C., 2008. Evaluation of
the accuracy of three different computer-aided surgery systems in dental implantology:
optical tracking vs. stereolithographic splint systems. Clin. Oral Implants Res. 19,
709 716.
Biomaterials used in
orthodontics: brackets, archwires,
and clear aligners
20
Mohamed-Nur Abdallah1, Tiantong Lou1, Jean-Marc Retrouvey2
and Sunjay Suri1
1
Faculty of Dentistry, University of Toronto, Toronto, ON, Canada, 2Division of
Orthodontics, Faculty of Dentistry, McGill University, Montreal, QC, Canada
Chapter Outline
20.1 Introduction 541
20.2 Orthodontic brackets
542
20.2.1 Metal brackets 542
20.2.2 Plastic brackets 550
20.2.3 Ceramic brackets 551
20.3 Orthodontic archwires 553
20.3.1 Properties of orthodontic archwires 553
20.3.2 Classification of orthodontic archwires 555
20.4 Clear aligners
20.4.1
20.4.2
20.4.3
20.4.4
20.4.5
20.4.6
20.5 Final remarks
References 572
20.1
562
Material composition 562
The thermoforming process 565
Forces of thermoplastic aligners 565
Mechanical properties 567
Attachments 569
Cytotoxicity 571
572
Introduction
Orthodontics, similar to other fields in dentistry, is in constant need for research
and improvement in the biomaterials used. Indeed, the field of orthodontic materials
has vastly expanded in the recent decades with the fabrication of new archwire
materials, new brackets materials and systems, as well as the introduction of clear
aligners. Box 20.1 summarizes the different classes of orthodontics materials. This
chapter will focus on the materials used for manufacturing the orthodontic brackets,
archwires, and clear aligners. Most of the other materials are covered under different chapters in this book.
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00020-7
Copyright © 2019 Elsevier Ltd. All rights reserved.
542
Advanced Dental Biomaterials
Box 20.1 Classification of orthodontic materials
According to their usage:
1. Orthodontic brackets: stainless steel, titanium, plastic or polycarbonates, and
ceramic.
a. Wire alloys
b. Metallic wires (e.g., stainless steel, β-titanium, nickel titanium)
2. Nonmetallic wires (e.g., Optiflex, composite coated wires)
3. Elastomeric ligatures and chains: conventional ligatures, fluoride-releasing
elastomerics
4. Adhesive composite resins: (e.g., chemically cured, light cured, dual cured)
5. Cements (e.g., zinc polycarboxylate, glass ionomer)
6. Miscellaneous materials (e.g., alginate impression materials, brass lock pins)
According to the structures of orthodontic materials
1. Metallic materials: Used to manufacture brackets, wires, and orthodontics bands.
2. Ceramic materials: Used for fabricating ceramic brackets and as filler
particles in cements.
3. Polymeric materials: A broad range of polymeric materials are used in
orthodontics including adhesive resins for bonding, impression materials,
polycarbonates for brackets, and polyurethane elastomers for tooth movement.
20.2
Orthodontic brackets
Orthodontic brackets are attachments that are bonded to the outer surface of the
crown of the tooth in order to transmit forces from the appliance to the teeth, with
the ultimate aim to induce the desired tooth movement. Orthodontic brackets can be
classified according to the following:
1. Morphology: single bracket, Siamese (twin bracket), Lewis bracket, mini-twin, selfligating, etc.
2. Technique used: Begg light wire appliance, edgewise appliance, straight wire appliance,
tip-edge appliance, lingual preadjusted edgewise appliance, etc.
3. Bracket slot dimension: 0.018v 3 0.025v, 0.022v 3 0.022v 3 0.028v, etc.
4. Core manufacturing material: metal brackets, plastic brackets, and ceramic brackets
(Table 20.1). Materials used for manufacturing brackets have undergone a vast improvements in the past few decades, particularly, with the use of materials other than metals to
meet the esthetic demands of patients. Yet, the metal brackets remain the most frequently
used for routine orthodontic treatment. This section will focus on the materials used for
manufacturing the brackets.
20.2.1 Metal brackets
Orthodontic brackets were originally fabricated stainless steel (SS) alloys where the
wings and the base were manufactured by machining and/or casting and then the
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
543
Table 20.1 Classification of brackets according to the manufacturing material.
Type of bracket
Examples
Metal
Stainless steel brackets
Cobalt chromium brackets
Titanium brackets
Precious metal brackets
Polycarbonate brackets
Polyurethane-composite brackets
Thermoplastic-polyurethane brackets
Monocrystalline alumina
Polycrystalline alumina
Polycrystalline alumina
Plastic
Ceramic
different parts were connected by soldering (Eliades and Brantley, 2016). Recent
advances in developing new materials as well as the fabrication techniques (e.g.,
metal injection molding and laser welding) have supplied the orthodontic field with
brackets made of cobalt chromium alloys, gold alloys, and titanium alloys (Eliades
and Brantley, 2016). Furthermore, these improvements have led to the fabrication
of brackets having a wide array of contradicting properties for each component
according to its function. For instance, the wing of the brackets, which is in contact
with the archwire, should be manufactured from a material that possesses a
relatively high modulus of elasticity to minimize the undesirable plastic deformation and be hard enough to resistant wear induced during the movement of the wire
in the slot as well as expression of torque, whereas the base of the bracket should
bond sufficiently to the tooth enamel but also allow some degree of deformation in
order to facilitate debonding from the tooth after the completion of the orthodontic
treatment (Eliades and Brantley, 2016).
There are four main types of metal brackets used in contemporary orthodontics:
1.
2.
3.
4.
SS brackets;
cobalt chromium brackets;
titanium brackets; and
precious metal brackets.
20.2.1.1 Stainless steel brackets
SS alloys were first introduced by Hauptmeyer into dentistry in 1919 to make
prostheses, and it was not until the 1930s that Angle introduced them into orthodontics as ligature wires. Following this, SS became the standard material to fabricate
brackets because of its superior mechanical properties, corrosion resistance, and relatively acceptable appearance (Brantley and Eliades, 2017).
From a material science perspective, SS, also called inox steel, is a steel alloy
that contains a minimum of 10.5% chromium content by mass. SS alloy is primarily
composed of iron, carbon, and chromium. Iron is the main ingredient of SS alloys,
but because of the brittle nature of pure iron, carbon is added to provide strength.
Moreover, by means of a process known as sensitization, carbon facilitates at high
544
Advanced Dental Biomaterials
temperatures the precipitation of chromium as chromium carbide at the grain
boundaries, and thus increases the intergranular corrosion. Chromium protects the
alloy from corrosion by forming an impermeable, corrosion-resistant chromium
oxide layer. Furthermore, relatively high concentrations of chromium promote the
stability of the body-centered cubic (bcc) lattice structure. On the other hand, other
elements that might be present in the alloy such as copper, manganese, nickel, and
nitrogen favor the stability of the face-centered cubic (fcc) lattice. Table 20.2 summarizes the effect of the different elements on the SS alloy.
Classifications of stainless steel alloys
SS alloys can be classified into different types of crystalline structures and each
type of SS has been designated a specific AISI (American Iron and Steel Institute)
or UNS (unified number system) or Society of Automotive Engineers number
depending upon the elemental composition of the alloy. Box 20.2 enumerates the
different types of SS alloys. In orthodontics, different types of SS alloys are used in
manufacturing the wings and the base components of the brackets. The SS alloys
vary in composition and demonstrate a specific crystalline structure with the
Table 20.2 Effect of different elements on the properties of stainless steel (SS) alloys.
Element
Effect
Carbon
Provides hardness and strength
Increases chromium carbide formation due to localized
corrosion from oral fluids
Increases resistance to oxidation by forming a passive surface
oxide layer, and thus prevents surface corrosion by
blocking oxygen diffusion
Stabilizes the austenitic phase
Increases resistance to corrosion and oxidation
Ion release might cause hypersensitivity reactions
Stabilizes the austenitic phase and has been used as a
substitute for nickel
Similar to nickel and manganese, it is an austenite forming
element
Increases resistance to pitting corrosion, particularly, by
chlorides
Stabilizes carbide and increases resistance to corrosion
Decreases sintering temperature and increases both strength
and corrosion resistance
Stabilizes carbon and improves corrosion resistance
Chromium
Nickel
Manganese
Nitrogen
Molybdenum
Titanium
Phosphorous
Niobium (columbium)
and tantalum
Copper
Selenium
Produces precipitation hardening properties
Makes SS more machinable and workable but decreases both
strength and hardness
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
545
Box 20.2 Types of stainless steel materials
1.
2.
3.
4.
5.
6.
Austenitic steels (300 series)
Martensitic steels (400 series)
Precipitation-hardenable steels
Ferrite steel
Duplex stainless steel (SAF 2205)
Cobalt-containing alloys
austenitic SS (303, 304L, 316L) and precipitation-hardenable steels (17-4 PH) being
the most commonly used (Eliades et al., 2003; Oh et al., 2005). Table 20.3 lists the
composition of some of the commercially available SS brackets.
Austenitic stainless steel (300 series)
Austenitic SS is one of the SS alloys most commonly used as orthodontic bracket
or wire materials due to its superior corrosion resistance, excellent formability, and
relative low cost. The SS alloys that fall the 300 series in the AISI system are all
austenitic SS alloys. According to this classification, the increase in number
indicates an increase in the number of metals added to the iron, whereas the carbon
concentration is decreased and the letter “L” indicates a low carbon content. Even
though the lower carbon content decreases corrosion susceptibility by minimizing
the harmful carbide precipitation, it also decreases the alloy’s strength. 304L steel
is one of the popular SS alloys, which is also called 18-8 stainless steel, as it is
composed of B18% chromium and B8% nickel, in addition to, B71% iron and
B , 0.02% carbon. 18-8 stainless steel brackets are most frequently milled,
whereas AISI 316L steel, which is also used to manufacture brackets, is too hard to
be milled, and thus manufacturers follow a casting technique to fabricate one-piece
brackets with no separate mesh-base. Standard orthodontic brackets are usually
manufactured (Oh et al., 2005; Platt et al., 1997; Eliades, 2007; Matasa, 1992). 316
and 316L SS have higher corrosion resistance, particularly to chloride, and have
been shown to release less nickel; therefore they are more commonly used for fabricating the base of the bracket (Eliades et al., 2002).
SS alloys form as an fcc crystal by heating the alloy above 912 C (Anusavice
et al., 2013). Nickel is added to the alloy to stabilize the SS in the austenitic form
after cooling. Other austenitizing elements, such as manganese and nitrogen, are
added to the alloy to preserve these alloys from turning into the bcc structure (also
known as ferrite) at room temperature. Chromium is also important to increase the
corrosion resistance, which maximizes the control of the nickel ion release and
decreases the possibility of any associated hypersensitivity reactions. Nonetheless,
the hostile environment of the oral cavity renders the austenitic SS susceptible to
corrosion, particularly in an acidic environment and the presence of chlorine ions
that may penetrate the outer protective oxide layer and cause pitting corrosion
(Grimsdottir et al., 1992).
Table 20.3 Composition of stainless steel alloys used in manufacturing orthodontic brackets.
Designation
Example
AISI
UNS
303
S-30300
304L
S-30403
316L
Composition (wt.%)
Fe
Cr
Ni
Mn
Mo
C
P
Si
S
Ormco diamond
Bal.
17 19
8 10
2
0.6
0.15
0.2
1.0
0.15
Advanced orthod
Bal.
18 20
8 12
2
0.03
0.04
1.0
0.03
S-31603
“A” company
Bal.
16 18
10 14
2
0.03
0.04
1.0
0.03
630/17-4
S-17400
Ormco min diam
Bal.
15 17
3 5
1
0.07
0.04
1.0
0.04
4 Cu/ 3 Nb
630/17-7
S-17700
Ormco edge lock
Bal.
16 18
6.5 7.5
1
0.09
0.04
1.0
0.04
0.08 1.5 Al
SAF 2205
S-31803
CEOSA low nickel
Bal.
22
5.5
2
3
0.03
0.03
1.0
0.02
0.16 N
18-8 Plus
S-28200
18-8 Plus
Bal.
8
0.16
18
1
0.15
0.045
1.0
0.03
0.5 N
431
AI29
S-43100
S-44735
Potential
Potential
Bal.
Bal.
26
29
0.3
0.5
4
4
0.02
0.035
0.35
0.01
0.5 Ti
2.5
Bal. indicates that the rest of the alloy is iron (Fe) by % weight. AISI, American Iron and Steel Institute; Bal., balance iron; UNS, unified number system.
Source: Anusavice (1996), K.J. Philips’ Science of Dental Materials, tenth ed. W.B. Saunders Company.
Other
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
547
Super austenitic SS (SR-50A or UNS no. S32050) is defined as an SS alloy with
a pitting resistance equivalent value of 40 and contains higher molybdenum and
nitrogen content than conventional SS (Oh et al., 2002). Super SS exhibits higher
resistance to chloride pitting and corrosion as well as good frictional properties
(Oh et al., 2005). However, Super SS has been tested only in vitro studies
(Oh et al., 2005), and to the best of our knowledge, no information is listed in any
company catalogue indicating its use in manufacturing brackets.
Precipitation-hardenable steels
These alloys are formed through hardening by heat treatment. This type of SS
presents a corrosion resistance equivalent to 304SS but with higher strength.
The 17-4 PH SS or S174000 PH alloys are widely used to fabricate the wings of
normal size or as “mini” brackets due to their relatively higher hardness and
strength (Flores et al., 1994). Indeed, an in vitro study tested the microhardness of
12 direct-bonding metal brackets and concluded that the PH 17-4 showed the highest hardness values, while the austenitic 316L presented the lowest hardness values
(Matasa, 1998). Despite having lower nickel content, 17-4 PH SS has poorer localized corrosion resistance and more nickel release than 316SS (Oh et al., 2005;
Eliades et al., 2002).
Ferrite steel
These alloys exist in an bcc crystal structure which is similar to the crystal structure
of iron, and thus these SS alloys have the designated name “ferrite”. The main
alloying element includes chromium, titanium, molybdenum, and a small amount of
carbon but no nickel. Generally, ferrite steel exhibits less corrosion resistance than
austenitic SS; however, stabilized ferritic SS (AISI 441) has comparable corrosion
resistance to that of 316SS. Ferritic SS demonstrates less strength than austenitic
hardness because it presents with lower amounts of carbon. In orthodontics, ferrite
SS with 19% 30% carbon content, also known as super ferrite SS, is utilized to
construct nickel-free brackets.
Martensitic steels (400 series)
These alloys demonstrate an increased tensile strength and less corrosion resistance
than the austenitic counterparts. Due to these properties, their use in dentistry is
limited to manufacturing tools that need sharp or wear-resistant cutting edges.
Duplex stainless steel (SAF 2205)
This SS alloy has a duplex microstructure consisting of austenite and delta-ferrite
and is used to manufacture one-piece brackets. It consists of high chromium
contents (19% 32%), molybdenum (up to 5%), and relatively low nickel content
compared to austenitic SS. This combination of more ductile and softer austenite
crystal phases and less ductile harder delta-ferrite crystal phases results in an SS
that is harder than the single-phase austenitic 316L SS, but more ductile than the
single-phase ferritic 430 SS.
548
Advanced Dental Biomaterials
20.2.1.2 Cobalt chromium brackets
Cobalt chromium (CoCr) brackets were introduced in the 1990s as a low nickel
alternative to SS. Generally, cobalt-based alloys can be categorized into following:
1. wear-resistant alloys;
2. high-temperature alloys; and
3. corrosion-resistant alloys.
From these categories, the cobalt-based wear-resistant alloy is utilized for
manufacturing orthodontic brackets (Haddad et al., 2009). According to the ASTM
(American Society for Testing and Materials), CoCr brackets are fabricated from
ASTM F-75 (Table 20.4), in which the nickel content is kept low (up to 0.05%)
(Haddad et al., 2009). CoCr brackets exhibit comparable friction to that of SS
brackets when used in combination with SS wires (Moore et al., 2004), while CoCr
brackets demonstrate higher frictions than titanium brackets when used with SS
wires or β-titanium wires (Titanium brackets and wires are explained in more detail
in sections 20.2.1.3 and 20.3) (Nair et al., 2012). Moreover, due to the relatively
higher content of chromium, CoCr brackets show a lesser degree of corrosion when
compared to titanium-based brackets (Schiff et al., 2005).
20.2.1.3 Titanium brackets
Titanium (Ti) and its alloys possess excellent biocompatibility and increased corrosion resistance, as well as adequate mechanical properties; therefore they have been
used for several biomedical applications ranging from artificial heart valves to limb
prostheses and dental implants (Ratner et al., 2012). Ti brackets were first introduced by Dentaurums in 1995 to overcome nickel hypersensitivity, inadequate
retention, and the susceptibility of SS to corrosion in the acidic oral environment
(Hamula et al., 1996; Michelberger et al., 2000). In metallurgy, Ti can be classified
into the following three types: αTi, βTi, or α β Ti.
Table 20.4 Composition of the cobalt-based wear-resistant
alloy (ASTM F-75).
Element
Weight %
Cr
Mo
W
C
Fe
Ni
Si
Mn
Co
25 30
7 max
2 15
0.25 3.3
3 max
0.5 max
2
1
Balanced
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
549
αTi is an unalloyed commercially pure (CP) Ti, whereas the other two types are
considered Ti alloys. βTi includes Ti 15V 3Cr 3Sn 3Al alloy, while α β Ti
includes Ti 6Al 4V alloy. CP-Ti can be further classified into four grades
according to the degree of purity and primary oxygen content. Grade 1CP-Ti
exhibits the highest purity, corrosion resistance, and formability but lowest strength
when compared to grade 4 CP-Ti, which demonstrates the highest strength and
moderate formability. The composition of the different grades of CP-Ti and Ti
alloys are shown in Table 20.5.
In contemporary orthodontics, αTi (grade 2 and 4) and α β Ti (Ti 6Al 4V)
are used to manufacture brackets (Zinelis et al., 2003; Gioka et al., 2004). Grade 2
CP-Ti is usually used to fabricate the base of the brackets because of its relatively
lower strength. The stronger and harder Ti 6Al 4V alloy is used to make the
wing components, which are then laser welded together. However, the welding
process may leave gaps between the different parts, leading to decreased mechanical strength, plaque retentive areas, and increased crevice corrosion (Gioka et al.,
2004). In addition to the previous drawbacks, due to reports of vanadium release
from Ti 6Al 4V, which could be hazardous (Rodriguez-Mercado et al., 2003),
some manufacturers fabricate single-unit brackets from metal injection molded or
milled from grade 4 CP-Ti (Gioka et al., 2004).
Ti and its alloys exhibit higher corrosion resistance than SS, due to the presence
of a thin outer protective layer of passive Ti dioxide (also known as rutile), which
is more stable than the chromium layer on the surface of SS (Brantley and Eliades,
2001). Moreover, the Ti dioxide layer remains stable during sliding mechanics
process and can be effectively used with SS wires. Ti brackets demonstrate comparable friction resistance to SS brackets when SS archwires were used (Kusy et al.,
1998; Kapur et al., 1999; Kusy and O’Grady P, 2000). Ti brackets exhibit lower
friction with βTi wires when compared to other metal brackets (Nair et al., 2012).
Compared to SS brackets, titanium brackets are more expensive, grayer in color
and show a rougher surface texture, and exhibit greater amount of plaque accumulation and staining (Harzer et al., 2004). Ti brackets demonstrate pitting corrosion
when used with fluoride containing mouthwashes or toothpaste (Toumelin-Chemla
et al., 1996; Reclaru and Meyer, 1998). However, titanium exhibits a low thermal
conductivity, which alleviates the patient’s sensitivity to extreme temperature
changes.
Table 20.5 Composition of different grades of commercially pure titanium.
Grade
1
2
3
4
Composition (maximum weight %)
Ti
N
C
H
Fe
O
Balanced
Balanced
Balanced
Balanced
0.03
0.03
0.05
0.05
0.08
0.08
0.08
0.08
0.015
0.015
0.015
0.015
0.20
0.30
0.30
0.50
0.18
0.25
0.35
0.40
550
Advanced Dental Biomaterials
20.2.1.4 Precious metal brackets
Historically, traditional edgewise brackets were fabricated from gold as they have
good mechanical properties and are nonreactive; however, due to their high cost,
they were replaced with SS. This type of bracket is usually a steel bracket plated
with precious metals including gold, palladium, or platinum. Among these brackets,
gold plated brackets (16, 18, 24 carats) are the ones most commonly used, particularly in lingual orthodontics.
20.2.2 Plastic brackets
Plastic brackets were first introduced in the early 1970s as an esthetic alternative to
the metal brackets. They were initially made of acrylic resins and later from
unfilled polycarbonate (Eliades et al., 2004). Plastic brackets are more transparent
than SS brackets, and thus more esthetically adaptive to the natural surface color of
teeth (Eliades et al., 2004). The bond strength of these brackets to the adhesive
bonding agent depends on the mechanical retention of the bracket base and the
plastic bracket primer. Although the shear bond strength of plastic brackets was
demonstrated to be significantly lower than metal brackets, it was found to be clinically acceptable (Pithon et al., 2007).
There were several major inherent disadvantages of plastic brackets that led to
its decreased acceptance and use by orthodontists. These problems included slot
distortion and creep deformation, tie-wing fractures, water absorption, discoloration,
odors, increased friction between the slot and archwire during tooth sliding, as well
as inadequate strength and stiffness resulting in debonding problems (Matsui et al.,
2015). For instance, polycarbonate brackets undergo permanent deformation or
creep with time when subjected to a constant stress in the range of 2000 g/mm
(Dobrin et al., 1975). Furthermore, it was shown that polycarbonate brackets exhibit
higher torque losses and lower torquing moments when compared with the metal
brackets (Harzer et al., 2004).
To overcome the lack of strength and rigidity of the polycarbonate (PC) bracket,
manufacturers introduced high-grade medical polyurethane brackets (Eliades et al.,
2004) and polycarbonate brackets reinforced with ceramic (Arici and Regan, 1997)
or fiberglass fillers (Faltermeier et al., 2007) and/or metal slots (Zinelis et al.,
2005). Also, the bracket base was modified to strengthen the resin bonding without
primers and minimize enamel damage related to debonding procedures (Arici and
Regan, 1997). In a study comparing torque deformation of seven commercially
available plastic brackets against SS brackets, results demonstrated that the metal
reinforced PC brackets undergo the lowest degree of deformation followed by pure
PC, pure polycarbonate, fiberglass-reinforced PC brackets, and then ceramicreinforced PC brackets (Sadat-Khonsari et al., 2004). However, it was reported that
the addition of ceramic and glass fibers to PC brackets had no beneficial effect
regarding frictional forces (Feldner et al., 1994; Sadat-Khonsari et al., 2004; Ali
and Mann, 2004; Moller et al., 2009). Even though ceramic reinforcement and the
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
551
addition of metal slot decreased the creep, there was still a 15% loss in torque
expression over 24 hours when using the PC brackets (Feldner et al., 1994).
Nevertheless, it seems that PC brackets reinforced with metal slot are capable
of generating clinically acceptable torque expression and their decreased slot
roughness is beneficial when applying sliding mechanics during orthodontic tooth
movement (Sadat-Khonsari et al., 2004). Accordingly, it was recommended to use
PC brackets only if they had a metal slot in order to decrease the frictional resistance, slot deformation, and to avoid damage from the sliding movements of the
archwire (Sadat-Khonsari et al., 2004; Choi et al., 2014). Further recent advancements include plastic self-ligating brackets which have been shown to exhibit lower
frictional forces when compared to the conventional counterparts (Russell, 2005).
Table 20.6 summarizes the features of the different types of plastic brackets.
20.2.3 Ceramic brackets
The first ceramic brackets were introduced into the field of orthodontics in the
mid-1980s (Swartz, 1988). Ceramic brackets are composed of tridimensional macromolecules of aluminum oxide or zirconia oxide (Birnie, 1990). Box 20.3 lists the
different types of ceramic brackets. These brackets are optically more esthetic than
SS brackets, offer the advantage of resisting staining and slot distortion, as well as
being chemically inert to oral fluids (Reddy et al., 2013; Ansari et al., 2016).
Table 20.6 Characteristics of the different types of plastic brackets.
Type of bracket
Examples
Polycarbonate
Polyurethane
Reinforced
polycarbonate
Polyurethane composite
Thermoplastic polyurethane
Polymer fiber reinforced
Ceramic reinforced
Fiberglass reinforced
Metal slot reinforced
Metal slot and ceramic
reinforced
Characteristics
Undergoes creep deformation
Water absorption leading to
swelling and increased friction
Discoloration and odor
Improved strength
Improved frictional resistance
Increased deformation resistance
Box 20.3 Types of ceramic brackets
1. Monocrystalline alumina (sapphire)
2. Polycrystalline alumina
3. Polycrystalline zirconia yttrium partially stabilized zirconia
552
Advanced Dental Biomaterials
20.2.3.1 Polycrystalline zirconia
Currently, the use of zirconia brackets is limited in the orthodontic field due to their
higher friction coefficient (Keith et al., 1994), lower shear bond strength, and inferior esthetic properties (i.e., less transparent and with a yellowish tint) than alumina
brackets (Springate and Winchester, 1991; Brantley and Eliades, 2001). Therefore
this chapter will only focus on the alumina brackets.
20.2.3.2 Alumina ceramic brackets
Contemporary ceramic brackets are mostly made of alumina. According to the
manufacturing process, these brackets are categorized into two broad classes with
different optical and mechanical properties: monocrystalline (sapphire) and
polycrystalline (Birnie, 1990). Polycrystalline alumina brackets are composed of
aluminum oxide particles that are fused by a sintering process. This procedure is
relatively inexpensive and less complicated than the manufacturing of monocrystalline ceramics, making these brackets more popular (Kusy, 1988; Saunders and
Kusy, 1994). During manufacturing, the aluminum oxide particles are first blended
using a binder machine and then molded into a certain shape from which the different components of the brackets are cut. The molded mixture is afterward heated at
temperatures that fuse the alumina particles and burns out the binder. This firing
process is known as “sintering” (Brantley and Eliades, 2001). Of note, polycrystalline zirconia brackets are manufactured following a different process than alumina
brackets which entails impression molding followed hot isostatic pressing (Brantley
and Eliades, 2001).
On the other hand, the process of manufacturing monocrystalline alumina brackets begins with melting pure aluminum oxide particles at temperatures above
2100 C; the resulting mass is slowly cooled to form a large single-crystal alumina
rod (Birnie, 1990). The single-crystal alumina rod is then milled into brackets by
using ultrasonic cutting or Nd:YAG lasers and heat treated to remove surface
imperfections or stresses resulting from the milling process. These steps minimize
the imperfections and stress-inducing impurities present in the polycrystalline ceramics. However, this process is relatively more expensive and more difficult than
the polycrystaline sintering technique, and introduces sharp corners that may make
the tie wings of the brackets more prone to fracture (Brantley and Eliades, 2001).
Esthetically, monocrystalline brackets are clearer than the polycrystalline counterparts due to the reduction of grain boundaries and impurities which are responsible
for reflecting light, thus making the polycrystalline brackets appear more radiopaque (Swartz, 1988; Birnie, 1990).
The main disadvantages of alumina ceramic brackets include the following:
G
G
Brittleness and low fracture toughness that may lead to tie-wing fracture.
Increased frictional resistance: In addition to the already increased resistance to sliding
between the archwires and ceramic brackets, the harder aluminum oxides can create nicks
in the softer SS archwire during orthodontic tooth movement, which, in turn, further
increases the binding and frictional resistance (Voudouris et al., 2010; Williams and
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
G
G
G
553
Khalaf, 2013; Kumar et al., 2014). Moreover, polycrystalline ceramics with their rougher
surface finish present a higher friction resistance than monocrystalline brackets (Arici
et al., 2015; Arash et al., 2015). To overcome this drawback, manufacturers have
attempted to improve the frictional characteristics by the addition of metal lined/reinforced slots (Pasha et al., 2015; Arici et al., 2015).
High levels of hardness: Ceramic brackets are nine times harder than tooth enamel
(Swartz, 1988). Indeed, attrition of the opposing teeth in contact with ceramic brackets is
a common clinical finding. Accordingly, these brackets should be avoided in deep bite
cases or situations where teeth might be in contact with the bracket even for a short
period.
Other clinical complications include enamel fractures, flaking, or cracks, especially during
debonding procedures, due to the increased bond strength from the silane coupling agent
(Reddy et al., 2013; Ansari et al., 2016). Therefore ceramic brackets should be avoided in
patients with developmental tooth defects, enamel cracks, several nonvital teeth, or teeth
with large restorations (Olsen et al., 1996). To address this problem, ceramic brackets
with a polymeric base or with various mechanical base designs have been introduced,
such as a mechanical ball, dovetail, silane-coated buttons, or microcrystalline. By utilizing
these mechanical retentive modifications, ceramic brackets can be cemented directly to
the tooth surface using standard light-cured or chemically cured adhesives without the
need for additional saline bonding agents. Moreover, it is argued that these modifications
render the bond strengths and debonding characteristics of ceramic brackets comparable
to that of metal brackets (Gwinnett, 1988; Bishara et al., 1993). In addition, it was demonstrated that ceramic brackets with polymeric mesh bases exhibited adequate bond strength
and resulted in less tooth enamel damage at debonding when compared to conventional
ceramic brackets (Ansari et al., 2016; Elekdag-Turk et al., 2009).
Ceramic brackets cause less image distortion to the diagnostic quality of magnetic resonance (MRI) images of the head when compared to SS brackets (Zhylich et al., 2017).
20.3
Orthodontic archwires
Orthodontic archwires and auxiliaries constitute the basic active components for
moving teeth in the fixed appliance system. Orthodontic wires are engaged into the
brackets to produce the desired tooth movement or can be utilized as a stable base
to which force elements are connected to yield the tooth movement.
20.3.1 Properties of orthodontic archwires
The clinician should consider a variety of wire parameters and characteristics
according to the stage of treatment and the purpose for which the archwire is being
used. A single type of archwire is not appropriate for all treatment stages and there
is no archwire that is considered ideal. Some of the main properties of orthodontic
wires are discussed below:
G
Modulus of elasticity or Young’s modulus is defined as the ratio between the stress
applied to the wire and the resulting strain. It is used to describe the rigidity or the stiffness of the wire (Fig. 20.1).
554
Advanced Dental Biomaterials
Figure 20.1 Diagram illustrating the properties of orthodontic wires according to the
stress strain curve.
G
G
G
G
G
Stiffness (or load deflection rate) is defined as the magnitude of force delivered by the
appliance and is proportional to the modulus of elasticity. It can also be defined as the
resistance of the wire to deformation or to the force required to bend the wire to a certain
distance. To illustrate this point with a clinical example, the initial archwires used during
the leveling and alignment phase of orthodontic treatment should be flexible, while the
working archwires used for space closure or anterior posterior correction need to be stiff
enough to sustain the forces applied.
Modulus of resilience is the characteristic that reflects the energy storing capacity of the
wire and it is represented by the area under the line describing the elastic deformation of
the wire (Fig. 20.1). Elastic deformation is a temporary shape change and the material
returns to its original dimensions it had before the stress was applied.
Range of activation, range of deflection, or working range are defined as the distance that
the archwire can be deflected or bent without permanent deformation. This range can also
be referred to as springback, maximum elastic deflection, or maximum flexibility.
Springback is related to the ratio of yield strength to the modulus of elasticity of the material.Yield strength can be defined as the stress at which a specific amount of permanent
plastic deformation is produced, and it is usually determined at a 0.2 percent of the
unstressed length. The archwire used for aligning and leveling teeth should have a large
working range or high springback in order to engage brackets attached of severely displaced or rotated teeth, while the modulus of elasticity should be low enough for the wire
to exert low forces on teeth even at large deflections. Higher springback values refer to
the ability of applying large activations while increasing the working time of the appliance. This results in a decrease in the number of archwire changes during treatment. It
should be noted that if a wire is stretched beyond its yield strength, it will undergo permanent deformation and will not return to its original shape; however, a certain amount of
springback will still occur until the failure point is reached.
Strength is defined as the maximum force that an archwire can withstand before undergoing permanent deformation. Plastic or permanent deformation is the permanent distortion
that occurs when a material is subjected to stresses beyond its yield strength.
Formability is the property that permits bending the wire into any desired configurations
(e.g., loops, springs, coils) without fracturing (i.e., without reaching the break point) the
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
G
G
G
G
555
wire. Ideally, an archwire should present a combination of formability for ease of preengagement wire bending as well as an appropriate resilience for engagement and subsequent activation (Fig. 20.1).
The friction between the archwire and the bracket should be as minimal as possible as
excessive friction may slow down tooth movement and lead to loss of anchorage.
The archwire material should be biocompatible, highly corrosion resistant to the oral environment, and not favor the growth of microorganisms. It should demonstrate also environmental stability that guarantees the maintenance of the desirable wire properties for an
adequate period after manufacturing as well as to ensure a predictable behavior of the
wire when in use during treatment.
As feasible as possible, the archwires should be manufactured from a relatively inexpensive material.
In certain clinical situations, it is preferable that the archwire can be welded or soldered
to auxiliaries and attachments.
20.3.2 Classification of orthodontic archwires
Orthodontic archwires can be classified according to their composition, sizes, cross
sections, configurations, or preformed shapes (Fig. 20.2). Orthodontic archwires are
generally manufactured from metal alloys. The manufacturing process begins with
cross-sectional reduction and lengthening of the alloy to induce strain hardening
and brittleness in the alloy. The wires then undergo various heat treatments to
release any residual stresses and accumulated strain energy to restore their ductility
and toughness. The fabrication of multistranded wires involves manufacturing of
the individual strand and braiding or twisting the wire to produce the final desired
configuration (Nikolai, 1997).
20.3.2.1 Gold
Gold alloys were initially used to fabricate archwires because they are inert, biocompatible, and stable. Furthermore, before the widespread use of the SS wire, gold
alloys were used due to the lack of the availability of other materials that can
Figure 20.2 Classification of some of the main orthodontic wires.
556
Advanced Dental Biomaterials
tolerate the oral conditions. Gold wires are generally composed by of gold
(15 65 wt.%), copper (11 15 wt.%), silver (10 25 wt.%), palladium (5 10 wt.%),
platinum (5 10 wt.%), nickel (1 2 wt.%), and traces of zinc. Table 20.7
summarizes the advantage and disadvantages of these wires. To the best of our
knowledge, archwires made of gold alloys are not currently used in the clinical
orthodontic practice.
20.3.2.2 Stainless steel
Ever since it was introduced in 1929 by Wilkinson, SS forms the basis of most
orthodontic wires. The composition of the SS archwires is similar to that used in
the manufacturing of brackets with the austenitic form, especially the 18-8 SS,
being the mostly commonly used. The use of SS wires is dependent on the technique, the stage of treatment, and the required stiffness (aligning, retraction to close
space, finishing, etc.). It should be noted that aside from manufacturing brackets
and archwires, SS is used to fabricate orthodontic band, auxiliaries (e.g., lingual
buttons, lingual cleats), ligature wires, and orthodontic pliers. Table 20.8 describes,
in general, the advantages and disadvantages of SS wires.
Table 20.7 Advantages and disadvantages of gold wires.
Advantages
G
G
G
G
G
G
Disadvantages
Low modulus of elasticity
Strength can be increased by heat treatment
or cold working
High formability
Excellent biocompatibility
Good environmental stability
Can be soldered or welded
G
G
G
Low springback
Low yield strength
Relatively expensive
Table 20.8 Advantages and disadvantages of stainless steel (SS) wires.
Advantages
G
G
G
G
G
G
G
G
G
High stiffness
High resilience
Good formability
High yield strength
Adequate springback
Relatively economical
Good joinability (i.e., can be
welded and soldered)
Corrosion resistant (except
at weld and solder sites)
Biocompatible
Disadvantages
G
G
G
G
G
Lower springback than NiTi alloys
Higher modulus of elasticity
More frequent activations are required to maintain
the same force levels
Soldering is demanding
Delivers high forces, relatively lower springback
and high deflection rate, therefore requires more
attention to detail to avoid harmful/unwanted
effects on teeth (smaller diameter archwires are
recommended when using SS wires in the initial
stages of aligning crowded teeth)
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
557
Australian stainless steel wires
These wires were developed by an Australian metallurgist, Arthur J Wilcock to be
used for the Begg light archwire technique. His aim was to produce SS wires that
are more tensile and thin enough to exhibit optimal tooth moving forces for an adequate period over long distances, with minimal loss in force intensity. These wires
are round in cross section and are available as spools as well as in various straight
lengths, grades, and diameters. Over time, the diameter of these wires has been
decreasing to accommodate the changing concepts of using lower force levels in
orthodontics. The wires that are manufactured using the pulse straightening technique (e.g., newer premium and supreme wires) demonstrate high tensile strength,
high load deflection rate (i.e., high working range) good recovery patterns, and a
relatively smoother surface finish.
Braided or twisted wires (or multistranded stainless steel wires)
In these types of wires, SS wires with relatively small diameters (e.g., 0.178 mm)
are braided or twisted to fabricate larger wires with round or rectangular cross sections. The resulting larger-diameter wires are capable of sustaining larger elastic
deflections with lower load deflection rates when compared with the conventional
round SS wires of similar dimensions. On the other hand, the springback of multistranded SS wires is larger than that of conventional SS or β-Ti wires but similar to
that of nitinol archwires. It should be noted that the springback is independent of
the thickness of twisted archwires.
20.3.2.3 Cobalt chromium-based archwires (also known as
Elgiloy)
A major disadvantage of SS wires is the inability for the clinician to alter their
resilience if required, since it cannot undergo heat hardening treatment. In contrast,
Elgiloy wires present somewhat similar properties to those of SS wires but can be
supplied in the softer and more formable form which can then hardened by heat
treatment to modify their resilience or increase the strength of the wire. Elgiloy or
cobalt chromium-based wires were originally developed by the Elgin Watch company for manufacturing watch springs and were introduced to orthodontics in the
mid-1950s. Cobalt is the main constituent of these wires, which is present as a solid
solution with chromium. Chromium provides the required stiffness and corrosion
resistance, whereas nickel strengthens the alloy and improves its ductility. Other
elements including iron, copper, molybdenum, tungsten are effective solid solutions
hardeners, while manganese and silicon act as oxide scavengers (Table 20.9 shows
the composition of Elgiloy wires).
There are four main categories of Elgiloy archwires, separated by color coding,
which have the same composition but differ in their resilience and other properties
by variations in the manufacturing process (Kapila and Sachdeva, 1989):
G
Blue Elgiloy (soft) is recommended when the wire needs substantial bending, welding, or
soldering.
558
Advanced Dental Biomaterials
Table 20.9 Composition of cobalt chromium based archwires
(Elgiloy).
G
G
Element
Weight %
Co
Cr
Ni
Fe
Mo
Mn
Be
Others
40
20
15
15.4
7
2
0.4
0.5
Yellow Elgiloy (ductile and slightly harder than blue) can be welded or soldered. Yellow
Elgiloy is recommended for preadjusted edgewise appliance that requires greater springback properties than those provided by blue Elgiloy. Moreover, Yellow Elgiloy can be
used as provided by the manufacturer or can be heat treated, if greater resiliency or
springback properties are needed.
Green Elgiloy (semiresilient) and Red Elgiloy (resilient) can be plier manipulated before
heat treating and recommended for use where adjustments will not be required after heat
treating.
The advantages of Elgiloy over SS wires include excellent corrosion and tarnish
resistance, higher springback efficiency (greater than SS by 20%), and they functionally remain active for a longer duration when used as resilient spring (i.e.,
greater resistance to fatigue and distortion) (Kapila and Sachdeva, 1989). Elgiloy
wires demonstrate a modulus of elasticity that is somewhat comparable or higher to
that of SS, and thus, the amount of force delivered to teeth is twice and four times
that of β-Ti and NiTi wires, respectively (Goldberg et al., 1983). Even though
Elgiloy wires exhibit a 17% higher corrosion resistance than SS wires, the relatively
high nickel content could present a biocompatibility problem. Also, the frictional
resistance of Elgiloy is comparable or slightly higher than that of SS wires (Frank
and Nikolai, 1980). Other disadvantages of Elgiloy wires include the need for heat
treatment and the demanding soldering process.
20.3.2.4 Nickel titanium wires
NiTi alloys were first developed in the 1960s by William F Buehler for a space program at the Naval Ordnance Laboratory and were marketed as nitinol, which is
derived from the elements comprising the alloy and the name of the developing lab
—nickel (Ni, 55%), titanium (Ti, 45%), and Naval Ordinance Laboratory (nol).
Over the years, several modifications have added additional desired properties such
as low stiffness, shape memory, and superelasticity. In addition, the high springback
property of nitinol permits the delivery of low forces even at large deflection, which
is particularly useful in cases with severe crowding. Moreover, newer NiTi-based
alloys are thermally activated (i.e., deliver tooth moving forces only after reaching
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
559
Table 20.10 Advantages and disadvantages of NiTi wires.
Advantages
G
G
G
G
High elasticity
High springback
High stored energy
Biocompatible and environmentally
stable (However, some corrosion and
failure have been observed in certain
occasions)
Disadvantages
G
G
G
G
G
G
Higher friction than SS but less than
TMA wires (friction of NiTi wires can
be reduced by coating the surface using
metal plating, chemical vapor deposition,
ion implantation, etc.)
Lower stiffness than SS and is not
recommended to be used at the
completion stages of orthodontic
treatment
Fractures easily when bent over a sharp
edge
Cannot be welded or soldered
More expensive than SS wires
Poor formability
SS, stainless steel; TMA, titanium molybdenum alloy.
a certain temperature), which was achieved by the incorporation of a small amount
of copper. Table 20.10 summarizes the advantages and disadvantages of NiTi
wires.
Thermoelasticity of NiTi alloys
NiTi alloys are present in two crystalline forms: austenitic and martensitic. The
temperature during which the alloy transitions from martensitic to austenitic is
called the temperature transition range (TTR). The TTR is dependent on the nickel
percentage; the lower the nickel content, the higher will be the TTR. Below the
TTR, the crystals form in a martensitic form at low temperatures and high stresses
and the crystals can exist in a distorted monoclinic, triclinic, or hexagonal structure.
Above the TTR, the crystals form in an austenitic phase under high temperatures
and low stresses and demonstrate an ordered bcc system structure. Some variations
of the NiTi alloy have been developed in orthodontics. In general, the archwires are
manufactured in the desired shape in the martensite phase and then they undergo
the TTR to transform into the austenite form. In the austenite form, the NiTi wire is
deformed to conform to the irregularities in the arch form.
Different generations of NiTi alloys
G
Stabilized martensitic NiTi or first-generation M-NiTi
These wires were marketed as nitinol by Unitek/3M. As the name implies, M-NiTi is
manufactured through a work hardening process and stabilized in a martensitic crystallographic form; therefore they do not exhibit shape memory or superelastic properties as the
phase transition does not occur. They also possess relatively high springback properties,
low elastic modulus, and a wide working range when compared to SS wires, but exhibit
poor formability.
560
G
G
Advanced Dental Biomaterials
Superelastic NiTi or austenitic NiTi (A-NiTi) wires
A-NiTi wires were introduced in orthodontics in the late 1980s and possess an active
austenitic phase. Accordingly, they demonstrate superelasticity and good shape memory.
Examples of this group include Chinese NiTi marketed as “NiTi” by Ormco and Japanese
NiTi by Miura et al. (“Sentalloy” by GAC International) (Burstone et al., 1985; Miura
et al., 1986).
Thermoelastic NiTi or copper NiTi or martensitic active NiTi
These thermally active wires exhibit a TTR close to the human body temperature
and were introduced by Rohit Sachdeva in 1994. Copper is added in order to control the TTR of NiTi alloys as well as to reduce friction and increase strength.
Generally, copper NiTi wires are composed of 42.99% Ti, 49.87% Ni, 0.5% Cr,
and 5.6% Cu. These wires exploit the thermoelastic effect to achieve shape memory. The wire is cooled down into a martensitic form by means of an ice bath, cold
water, or refrigerant spray to make it flexible before engagement into the brackets.
At body temperature, the deformed wire transitions back to the austenitic form and
its original structure, thus delivering light and continuous forces that are used to
align crowded teeth. Moreover, copper NiTi wires possess excellent springback, are
more resistant to permanent deformation, and deliver constant continuous forces
over a long activation range.
Four different types of copper NiTi wires are manufactured with variable transformations temperatures for a variety of applications:
G
G
G
G
Type I (TTR of 15 C) is not suitable for clinical usage due to its high force levels.
Type II (TTR of 27 C) produces heavy forces and it is best used where rapid tooth movement is required in patients with a normal periodontal health and average to high pain
threshold.
Type III (TTR of 35 C) generates relatively midrange forces and is recommended to be
used in patients with a compromised periodontal health and low to normal pain threshold.
Type IV (TTR of 40 C) is best used as an initial rectangular wire in patients who are periodontally compromised and are sensitive to pain.
Multistranded or braided NiTi wires (Supercable NiTi)
Braided NiTi exhibits increased superelastic properties as well as high deflection
rate with very light forces, thus allowing these wires to be used as initial archwires for
the alignment and leveling of moderate to severely crowded teeth.
Plastic-coated NiTi
The plastic coating improves the esthetic properties of the wires as they blend with
the surrounding dentition and decrease the friction with ceramic, composite, and plastic
wires.
BioForce wires
These newer NiTi wires exhibit superelastic shape memory properties that generate
gradually increasing forces from anterior to posterior within the same dental arch. The
same BioForce wire is manufactured with variable material composition or structure (i.e.,
variable transition temperatures) leading to the formation of a graded force delivery system throughout the arch length according to the periodontal surface of the tooth. It is
claimed that these wires produce light forces (80 g) anteriorly and heavier forces posteriorly (300 g).
G
G
G
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
561
20.3.2.5 Pure titanium wires and other titanium-based wires
As mentioned earlier, pure Ti exists in two forms: α-phase and β-phase.
α-Titanium wires are fabricated from grade V Ti that contains 6% aluminum and
4% vanadium. These wires possess good formability and exhibit stiffness comparable to that of SS. However, they demonstrate poor springback and their use is limited to torque control during the finishing stage of orthodontic treatment.
β-Titanium or titanium molybdenum alloys
Burstone and Goldberg developed β-Ti by alloying pure Ti with molybdenum in
order to stabilize the crystals in β-phase at room temperature (Burstone and
Goldberg, 1980; Goldberg and Burstone, 1979). β-Ti wires are commercially available as a titanium molybdenum alloy (TMA). The properties and some clinical
applications of TMA wires are summarized in Box 20.4 (Burstone and Goldberg,
1980; Goldberg and Burstone, 1979; Cash et al., 2004).
Titanium niobium wires
Rohit Sachdeva introduced this alloy in orthodontics in 1995. Titanium niobium
has a stiffness lower than that of TMA and SS wires but exhibits a springback comparable to that of SS. Furthermore, titanium niobium wires can welded and soldered and can be used to incorporate third-order corrections as well as used as a
finishing archwire (Dalstra et al., 2000; Krishnan and Kumar, 2004).
Box 20.4 Properties of titanium molybdenum alloy (TMA) wires
G
G
G
G
G
G
Springback of TMA is twice that of SS wires with a relatively low deflection rate.
This allows full bracket engagement with greater torque control than smaller SS
wires.
Good formability with adequate strength and springiness are ideal for fabrication of
springs. Accordingly, TMA is recommended for fabricating closing loop archwires
and auxiliary springs as well as intermediate and finishing archwires during treatment with preadjusted edgewise appliances.
Modulus of elasticity of TMA is twice that of NiTi but less than that of SS. The
low modulus of TMA combined with its good springback simplify the appliance
design by eliminating the need of incorporating complex helices and loops in the
archwires as compared to SS wires.
TMA wires possess corrosion resistance comparable to that of SS and Elgiloy
wires.
TMA wires exhibit higher bracket/wire friction than either SS or Elgiloy wires and
thus are not recommended for space closure with friction mechanics. However,
newer ion-guarded TMA wires are available for decreasing the bracket/wire
frictions.
TMA wires can be used in all stages of orthodontic treatment from aligning and
retraction to the final stages for torque expression.
562
Advanced Dental Biomaterials
Timolium wires or titanium vanadium wires
These wires are nickel free and can be used in patients with nickel hypersensitivity.
Compared to TMA, timolium wires have a smoother surface which significantly
reduces friction with the bracket and exhibits a higher yield strength with good
formability which permits introducing bends in the wire without breakage.
Moreover, the stiffness of timolium is lower than that of SS but higher than that of
TMA. This section of the chapter has discussed the major types of metal wires with
an overview of some clinical orthodontic applications. Table 20.11 provides a comparison between the most frequently used orthodontic wires.
20.4
Clear aligners
Due to increasing demands for esthetic orthodontic treatment, the popularity of
clear aligner therapy (CAT) has greatly increased over the years (Boyd, 2008).
Surveys have shown that a significant number of patients do not find the
commonly used metallic orthodontic appliances attractive and are willing to pay a
higher fee for more esthetic options (Rosvall et al., 2009). Contemporary aligners
of the 21st century combine the principles pioneered by Remensnyder (1926),
Kesling (1945), Nahoum (1964), and others (Ponitz, 1971; McNamara et al.,
1985; Sheridan et al., 1993) and integrate them with the modern CAD/CAM
technology. The Invisaligns appliance by Align Technology is currently the most
popular clear aligner system and it consists of a series of digitally generated
thermoplastic aligners created using stereolithographic models (Wong, 2002). The
main advantages of CAT include removability for ease of eating, comfort, and
oral hygiene maintenance, improved esthetics, and possibly reduced periodontal
risk (Boyd, 2008; Kravitz et al., 2009; Miethke and Brauner, 2007; Chhibber
et al., 2018). In addition, its smaller size compared to traditional orthodontic
appliances has led to improved patient acceptance of orthodontic treatment (Sergl
and Zentner, 1998; Miller et al., 2007).
The orthodontic force exerted by the thermoplastic appliance in CAT is highly
dependent on the mechanical properties of its fabrication material (Zhang et al.,
2011). To achieve the ideal treatment outcomes, it is important to understand the
numerous clear aligner products available on the market, and how they differ
regarding their construction material, thickness, and clinical protocol.
20.4.1 Material composition
Appliances used for CAT are mainly based on transparent thermoplastic-based resin
polymeric materials. The ideal material properties would be large springback, high
stored energy, tolerance to the oral environment, biocompatible, and low surface
roughness (Barone et al., 2016). Various types of aligner materials exist, such as
polyethylene terephthalate (PET-G), thermoplastic PCs, polypropylene, polycarbonate, and ethylene-vinyl acetate (Table 20.12) (Gao and Wichelhaus, 2017).
Table 20.11 Comparison of the clinical characteristics of metal orthodontic wires.
Wire type
Stiffness
Stored
energy
Friction with
SS brackets
Springback
Formability
Biocompatibility and
environmental stability
Joinability
Stainless steel
High
Low
Low
Low
Good
Good
Cobalt chromium
High
Low
Low to
moderate
Low
Good
Good
Nickel titanium
Low
High
High
Poor
Goodc
β-Titanium
Multistranded
NiTi
Average
Low
Average
High
Low to
moderate
High
NA
Can be welded
and soldered
Can be weldeda
and
solderedb
Not joinable
Average
High
Good
Poor
Good
Good
SS, Stainless steel.
a
Only yellow and blue Elgiloy can be welded.
b
Solder with some difficulty.
c
Some corrosion and failure have been noted.
Can be welded
Can be welded
and soldered
564
Advanced Dental Biomaterials
Table 20.12 Materials used for thermoplastic aligners.
Material
Product(s)
Manufacturer(s)
Polyethylene
Hardcast
Biolon
Duran, Clear Aligner
Erkodur
Zendura
Invisalign
Copyplast
Imprelon “S”
Bioplast
Essix A 1
Scheu-Dental, GmbH
Dreve Dentamid
Scheu-Dental, GmbH
Erkodent
Bay Materials, LLC
Align Technology, Inc.
Scheu-Dental, GmbH
Scheu-Dental, GmbH
Scheu-Dental, GmbH
Dentsply Raintree Essix,
Inc.
Ortho Organisers Inc.
Keystoen Industries
Dentsply Raintree Essix,
Inc.
PET-G
Polyurethane
Polypropylene
Polycarbonate
Ethylene-vinyl acetate
Copolyester
Polypropylene/polyethylene
copolymer
Masel
Keystone
Essix C 1
PET-G, Polyethylene terephthalate glycol.
Source: Adapted from Ryokawa, H., Miyazaki, Y., Fujishima, A., Miyazaki, T., Maki, K. 2006. The mechanical
properties of dental thermoplastic materials in a simulated intraoral environment. Orthod. Waves 65, 64 72.
The current most commonly used thermoplastic polymers for aligners are based
on derivatives of PC and polypropylene. PET-G is a noncrystallizing amorphous
copolymer of PET, which has good mechanical properties, formability, optical
properties, fatigue resistance, and dimensional stability. Polyurethanes have a wide
gamut of applications beyond the scope of dentistry, ranging from engineering
materials to coatings to adhesives and films (Frick and Rochman, 2004). It combines the properties of vulcanized rubber with the processability of thermoplastic
polymers to provide improved physical properties with chemical and abrasion resistance (Lu and Macosko, 2004).
When Invisalign was first introduced to the market in 1999, it was made from a
single-layered rigid PC material, synthesized from methylene diphenyl diisocyanate
and 1,6-hexanediol (Morton et al., 2017). Subsequent generations of aligners were
made from Exceed-30, which were selected for improved material transparency,
flexibility, and breakage resistance (Brantley and Eliades, 2017). In 2013
SmartTrack was introduced as the latest generation of thermoplastic material,
designed to replace the previous Exceed-30 and Exceed-40 aligner materials.
SmartTracks is a multilayered thermoplastic-PC-based material combined with an
elastomeric component (Align Technology, 2013, 2017). Based on the manufacturer’s claims, this material can maintain more constant and lighter forces over time
when compared to previous generations, without losing force expression due to
stress relaxation cycles throughout its 2 weeks of usage (Morton et al., 2017). There
are currently no scientific studies available on the stress relaxation properties of
SmartTrack. Preliminary patient surveys suggest that SmartTrack may be more
comfortable than the older materials (Brascher et al., 2016), although further studies
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
565
are needed to verify this (White et al., 2017). A recent clinical study has showed
higher mean orthodontic tooth movement achieved by SmartTrack when compared
to Exceed-30 over a 25-day period (Wheeler et al., 2017).
20.4.2 The thermoforming process
The two basic ways for the creation of clear aligners are the vacuum-formed
method initially described by Nahoum (1964) and the positive air pressure method
described by Ponitz and McNamara (McNamara et al., 1985; Ponitz, 1971). In the
vacuum-form method, a vacuum device is used to apply suck-down pressure as
the heated sheet of thermoplastic material is being applied to the dental cast, under
atmospheric pressure (Ponitz, 1971). Although a theoretical maximum of 15 PSI is
expected, the actual pressure varies between 3 and 14 PSI, based on the efficiency
of the vacuum pump (Nahoum, 2014).
The positive air pressure method utilizes a pressure chamber to apply positive
air pressure, rather than partial vacuum pressure, to conform the softened sheet of
thermoplastic material to the shape of the cast (Hahn et al., 2009, 2011). In this system, the air can be compressed up to 100 PSI and the details of the inner surfaces
of the aligner improve as the air pressure increases, up to a certain level (Nahoum,
2014). Studies have shown that vacuum-formed aligners deliver lower forces on
average than clear aligners created under high-pressure methods (Hahn et al.,
2009). It has been hypothesized (Nahoum, 2014) that the improved fit from the
high-pressure method may lead to increased friction and; therefore, allows more
expression of the programmed forces (Hahn et al., 2009).
20.4.3 Forces of thermoplastic aligners
The ideal clear aligner material should be capable of delivering sufficient force
to create the desired orthodontic tooth movement in a programmed and
predictable fashion, while avoiding damage the surrounding periodontal tissues
(Lombardo et al., 2017). In addition, clear aligners should be able to apply light
and continuous forces on the teeth, while still providing enough stiffness with a
high yield strength to ensure that the force is applied within the elastic range of the
material (Lombardo et al., 2017).
20.4.3.1 Differences in force generation between clear aligner
therapy and fixed appliances
Orthodontic tooth movement is a biochemical process provided by a loading
system, represented by a combination of forces and moments applied to the
dentition (Ren et al., 2003, 2004). The load delivering modality depends on the
specific type of orthodontic appliance used. In traditional fixed appliances,
the brackets and bands bonded directly to the crowns of the teeth provide a highly
defined contact area. The stained applied is transferred to the center of the bracket
566
Advanced Dental Biomaterials
and the subsequent moment-to-force ratio can be defined with respect to the bracket
and the center of resistance of the tooth.
With CAT, the force system is created through a small geometrical mismatch
between the shape of the thermoplastic aligner and the patients’ dentition (dental
alignment). Relative to fixed appliances, the load in clear aligner therapy is transferred through a wider and lesser defined contact area. Facilitation of the load transfer can be achieved through usage of auxiliary elements, such as attachment or
divots, which modify the contact interface between the aligner and the dentition.
This could give rise to localized increases in a mismatch at specific areas of need,
as well as improved accuracy in load control in terms of intensity and direction
(Barone et al., 2016).
Generally, the generation of forces in CAT can be categorized into two systems:
(1) a displacement-driven system and (2) a force-driven system. Displacementdriven system is an older concept with limited usefulness today (Schupp and
Haubrich, 2016). It involves designing aligners that are formed to the geometry of
the dentition in the next stage of the virtual treatment plan (Schupp and Haubrich,
2016). It is considered that the tooth will move until it is lined up to the shape of
the aligner. This concept of creating geometric mismatches is effective for simple
movements, such as when tipping and intrusion are required, but it is less effective
for achieving control of root movements. This concept can still be used today for
cases requiring simple and limited movements, via the use of Essix retainers
(Sheridan et al., 1993).
In the force-driven system, creation of aligners is determined by the fundamental
principles of biomechanics. This concept forms aligners in the shapes required to
produce the desired forces and movements, not necessarily the shape of the next
stage of tooth movement. The aligners are shaped with the intention to deliver the
specific forces and movements that can result in the desired tooth movement. This
concept is often seen in the comprehensive aligner systems, such as ClearCorrects
and Invisaligns.
20.4.3.2 Material factors affecting force delivery
Orthodontic forces exerted by clear aligners are governed by numerous factors,
including tray thickness, amount of activation as predicted by the software, extension of the gingival edge, type of movement, as well as stiffness and other material
properties (Baldwin et al., 2008; Bollen et al., 2003; Clements et al., 2003).
Appliances with thicker material have been showed to apply significantly greater
orthodontic forces than those of thinner material (Gao and Wichelhaus, 2017; Hahn
et al., 2009, 2011; Kohda et al., 2013). The material hardness and elastic modulus
were also strongly correlated with the amount of force delivered (Kohda et al.,
2013). Furthermore, aligners with larger gingival edge extensions (3 mm) produce
more force than aligners with a minimal gingival edge extension (0 1 mm) (Gao
and Wichelhaus, 2017). It has been thought that the observed increase in force
might be due to enhanced stiffness caused by the changes in material shape.
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
567
Aligners with a 2 mm extension beyond the gingival margins have been shown to
be more retentive in nature than straight or scalloped edges (Cowley et al., 2012).
However, further studies are necessary to investigate the effect of the increased gingival edge extensions on periodontal tissues.
Finally, thermoplastic aligners are viscoelastic materials by nature; consequently,
the forces generated by its programmed movements will decrease as a function
of time (Zhang et al., 2011). The following section will discuss the current
progress in seeking aligner materials with the most linear elastic behavior and high
yield strength for an efficacious force output (Lombardo et al., 2017; Zhang et al.,
2011).
20.4.4 Mechanical properties
In general, the two main factors that influence the mechanical properties of
thermoplastic aligners are structural and environmental (Landel and Nielsen, 1993).
Structural factors refer to properties related to the molecular and crystal structures
of the polymer material. For example, PET-G, PCs, and polycarbonates are
amorphous plastics, while polyethylenes and polypropylenes are crystalline plastics.
The degree of crystallinity of these thermoplastic aligners affects its mechanical
properties, and ultimately, the nature of the force that can be delivered by the
aligner tray (Ryokawa et al., 2006).
Environmental factors refer to the various chemical and mechanical changes
that aligners could undergo once inserted into the oral cavity. Variables such as
temperature, humidity, pressure, heat, and salivary enzymes can lead to chemical
reactions that alter the physical properties of aligners (Hahn et al., 2011; Ryokawa
et al., 2006). Furthermore, aligners are also subject to both short- and long-term
mechanical forces, while they are worn by the patient (Tuncay, 2006). As the clear
aligner is being inserted over the patient’s dentition, it may experience immediate
deformation during the fitting process, but once fully seated, it is able to rebound to
its original shape due to its elasticity. During the period of prescribed appliance
usage, the aligners are further subjected to occlusal forces intermittently exerted
throughout the day and night (Zhang et al., 2011).
20.4.4.1 Elastic modulus
The elastic modulus (Young’s modulus or modulus of elasticity) is a measurement
for the stiffness of a given material and is calculated as a ratio of the elastic stress
to elastic strain (Anusavice et al., 2013). It is advantageous for aligners to be made
from thermoplastic polymers of high elastic modulus, as it increases its force delivery capability under constant strain (Alexandropoulos et al., 2015). In addition,
higher elastic modulus allows the same force delivery from materials of thinner
dimensions (Kohda et al., 2013). Polyurethanes of the Invisalign system exhibit a
higher elastic index than polyester and PET-G materials (Alexandropoulos et al.,
2015).
568
Advanced Dental Biomaterials
20.4.4.2 Creep resistance
Creep is defined as the propensity of a solid material to gradually undergo permanent deformation under the influence of a static load or constant stress (Anusavice
et al., 2013). With respect to clear aligner therapy, it is desirable for the aligner
material to have increased resistance to creep, as it allows for optimal expression of
the orthodontic force (Brantley and Eliades, 2017). Having a higher creep value
implies that under the constant forces of occlusal stress by the opposing dentition,
the material is more likely to deform and exhibit attenuated force levels. Under
indentation testing, the proprietary PC material of Invisalign demonstrated inferior
creep resistance than other PET-G thermoplastic materials (Alexandropoulos et al.,
2015).
20.4.4.3 Stress relaxation
Stress relaxation describes the material’s tendency to decrease its load generation
when held under a constant strain or deflection (Anusavice et al., 2013). An orthodontic aligner that exhibits rapid stress relaxation may express a decreasing amount
of orthodontic force once inserted intraorally, even before the tooth has begun to
move (Lombardo et al., 2017). This effect will undoubtedly have a negative impact
on the aligner’s performance and could be compounded when used in a sequential
fashion, leading to a tracking problem clinically.
The ideal aligner should exhibit a stress relaxation curve that is fairly flat, representing its capability to exert constant and continuous forces over time (Fang et al.,
2013). Unfortunately, stress relaxation curves for current aligner materials generally
follow a pattern of rapid decay within the first 8 hours of application, then diminish
to a plateau thereafter (Lombardo et al., 2017). This highlights the importance of
measuring forces exerted by aligners not only during the first hours after tray placement inside the oral cavity but also within the first 24- and 48-hours (Lombardo
et al., 2017). Both PET-G and PET polymers have a similar stress strain behavior,
although PET-G exhibits greater elastic recovery than PET polymers (Dupaix and
Boyce, 2005). Furthermore, stress relaxation appears to be temperature dependent,
as intraoral temperatures can accelerate this process as compared to ambient room
temperatures (Fang et al., 2013).
Similar results were found in an in vivo study of von Mises strains experienced
by aligners, a parameter used for assessing the amount of load that can be applied
before material failure (Jones, 2009). The aligners demonstrated peak von Mises
strain within the first 24 hours of wear, followed by a rapid decrease on day 2 and
subsequent plateauing throughout the remaining 2 weeks of wear (Vardimon et al.,
2010). This result further highlights the importance of wearing the aligners maximally within the first 24-hour period (Brantley and Eliades, 2017).
20.4.4.4 Water absorption
The mechanical properties of thermoplastic aligners can be affected by absorption
of water through the humidity in the air as well the oral cavity environment
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
569
(Brantley and Eliades, 2017). This could result in dimensional changes to the
aligner trays due to hygroscopic expansion, and thus leading to changes in the tray
fit to the dentition and force delivery system (Kwon et al., 2008). Moreover, it
should be noted that thermoplastic materials with a crystalline structure have a
lower water absorption rate than amorphous structures, due to their higher molecular density (Ryokawa et al., 2006).
20.4.4.5 Wear, abrasion, and intraoral aging
Assessment of aligner wear is a challenging and complex process, as in vitro
experiments may not be able to accurately represent the numerous simultaneous
mechanisms that lead to wear in vivo (Lutz et al., 1984; Wassell et al., 1994).
Laboratory studies simulating wear on polypropylene materials, including Essix
C 1 , and PET-G polymer, demonstrated an increased wear resistance for the latter
(Gardner et al., 2003). Furthermore, the increased wear resistance of PET-G polymers has been attributed to its increased hardness .
Intraorally used aligners can undergo significant structural deformation, including cracking, wear of contact points, and adsorption of proteinaceous materials
(Schuster et al., 2004). These changes can lead to a degradation of its mechanical
properties, including elasticity, hardness, and indentation creep (Gerard Bradley
et al., 2016), leading to attenuation of its force delivery capacity. These changes
were thought to be attributed to the alterations of the polymer crystallinity from
cold working produced by the masticatory forces (Gerard Bradley et al., 2016).
Similar results were found in PET-G aligners, including increased material stiffness,
hardness, and surface roughness (Ahn et al., 2015).
However, current studies still differ regarding whether clinically worn Invisalign
appliances will undergo changes in their chemical composition (Schuster et al.,
2004; Gracco et al., 2009) or remain stable throughout intraoral aging (Gerard
Bradley et al., 2016).
20.4.5 Attachments
Attachments are part of the armamentarium in clear aligner therapy for achieving
the desired tooth movement by improving accuracy and delivering higher levels of
forces (Rossini et al., 2015; Simon et al., 2014). Attachments are made out of dental
composite materials, including both flowable and packable, which are then
polymerized when cured on the crown surface using adhesives (Table 20.13)
(Barone et al., 2016).
Attachments provide an artificial, flat, and planar surface onto which the aligner
can apply additional strains. This portion of the attachment is known as the “active
surface” (Schupp and Haubrich, 2016) (Fig. 20.3). The active surface is of critical
importance, as it is the one being engaged by the aligner. The remaining portion
of the attachment material solely serves to keep the active surface in its desired
location. Force systems are applied at specific locations by designing the aligner to
only contact at the active surface while avoiding contact at the other areas of the
570
Advanced Dental Biomaterials
Table 20.13 Recommendation for composite materials used for attachments in clear
aligner therapy.
Composite material
Compatible adhesive
Manufacturer(s)
3M Filtek Supreme Plus & Z250
Tetric EvoCeram
3M Adper prompt L-Pop
G-ænial Bond
SonicFill
Venus Pearl & Diamond
GrandioSO
Optibond XTR
iBond Total Etch
Futurabond U
3M ESPE
Ivoclar Vivadent
GC America
Kerr Dental
Heraeus-Kulzer
VOCO GmbH
Packable
Flowable
Filtek Supreme Ultra Flowable
GrandioSO Heavy Flow
Tetric EvoFlow
Scotchbond Universal Adhesive
Futurabond U
G-ænial Bond
G-ænial Universal Flo
G-ænial Bond
3M ESPE
VOCO GmbH
Ivoclar Vivadent
GC America
GC America
Source: Adapted from Align Technology, 2018. List of recommended materials for bonding attachments. Available
from: ,https://learn.invisalign.com/attachments/bonding/recommendedmaterials. (accessed 26.05.18.) (Align
Technology, 2018).
Figure 20.3 Example of a horizontal rectangular attachment placed on a maxillary central
incisor, with bevel toward the gingival aspect, serving as the active surface (arrow).
attachment. This design allows for better control of the direction and magnitude of
forces applied, leading to more accurate force delivery and enhanced control of
tooth movement (Schupp and Haubrich, 2016).
Attachments are typically not meant to be fully engaged at the initial time of
bonding, as the patient progresses through the aligner trays, their successive
aligners gradually engage the active surfaces of the attachments more while
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
571
applying constant strain sresulting in tooth movement. Eventually, the attachment
will finally fill in the slot on the aligner. This concept is similar to working through
the archwires in preadjusted fixed appliances where the slot of the bracket is filled
by larger wires (Hennessy and Al-Awadhi, 2016).
20.4.6 Cytotoxicity
Isocyanates are a family of chemicals commonly used for the commercial synthesis
of PC-based products; this includes certain types of clear aligners, such as the
Invisalign system (Wisnewski et al., 2000). Its popularity in this industry is due to
its ability to efficiently react with polyols to form PCs with virtually no by-products
(Fig. 20.4). However, the usage of isocyanates does not come without its disadvantages as well, including numerous side effects that can pose significant health issues
to the patient (Liljelind et al., 2010). Isocyanates are the leading cause of occupational asthma in industrialized nations. They also cause hypersensitivity and allergic
reactions, as well as mucous membrane irritation (Liljelind et al., 2010).
It is thought that the cytotoxic properties of thermoplastic materials appear to be
influenced by the composition and structure of the polymer, as well as processing
and environmental factors, such as temperature, humidity, pressure, and thermal
history (Jorge et al., 2003). Polymer materials, especially amorphous plastic including Invisaligns, demonstrate high rates of water absorption, allowing long-term
leaching of unreacted chemicals into the oral environment (Ryokawa et al., 2006).
This characteristic is of particular concern in orthodontics, as patients are usually
prescribed to wear aligners throughout the day and night (Boyd et al., 2000). If a
PC-based aligner is used 24 hours a day, they are continuously in contact with the
dentition and gingiva. Any residual isocyanates may potentially leak and lead to
damage of the epithelial layer or loss of its integrity, leading to various immunologic reactions (Premaraj et al., 2014a,b, Wu, 2014).
Figure 20.4 The chemical reaction for the synthesis of polyurethanes from isocyanates.
572
Advanced Dental Biomaterials
Awosika et al. (2017) reported the case of a 23-year-old healthy Caucasian
female undergoing Invisalign treatment, who experienced intermittent urticarial on
her extremities and flanks 2 days after application of the aligners. Her symptoms
subsequently worsened, leading to facial and periorbital swelling, with erythema
and burning sensation of the lips and oral mucosa. Her treatment was the removal
of the aligners with administration of oral prednisone, which resolved her symptoms. Patch testing revealed strong positive reactions to Invisalign and questionable
reactions to isocyanates after 96 hours. These findings were consistent with sensitivity to isocyanates and contact sensitization to Invisalign.
20.5
Final remarks
Improvements in the orthodontic materials resulted in a great influence on the
orthodontic practice, with prominent changes in the types of materials used and biomechanics research. Metals, alloys, polymers, and composites are the materials
used for manufacturing orthodontic materials. Each type of material presents its
advantages over the other. Accordingly, the clinician should possess a thorough
knowledge of the physical and mechanical properties of these materials to determine their clinical behavior and to achieve a satisfactory and predictable outcome
that fits the treatment objectives. The rise of the digital age has transformed orthodontics as we know it. The advent of computer-aided design and computer-aided
manufacturing has brought clear aligner therapy to the masses and became a mainstay of contemporary orthodontic. Furthermore, digital advances may have a great
impact on the materials used for fabricating brackets, wires, and clear aligners.
Therefore, it is more important than ever that we use the best available evidence to
make sound clinical decisions.
References
Abolfathi, A., Chen, J.C., Li, C., Tricca, R.E., Wu, B.M., 2009. Systems and Methods for
Dental Appliance Compliance Indication. Google Patents.
Ahn, H.W., Ha, H.R., Lim, H.N., Choi, S., 2015. Effects of aging procedures on the molecular, biochemical, morphological, and mechanical properties of vacuum-formed retainers.
J. Mech. Behav. Biomed. Mater. 51, 356 366.
Alexandropoulos, A., Al Jabbari, Y.S., Zinelis, S., Eliades, T., 2015. Chemical and mechanical characteristics of contemporary thermoplastic orthodontic materials. Aust. Orthod. J.
31, 165 170.
Ali, S., Mann, D.A., 2004. Signal transduction via the NF-kappa B pathway: a targeted treatment modality for infection, inflammation and repair. Cell Biochem. Funct. 22, 67 79.
Align Technology, 2013. Align Technology Announces January 21st Availability of
SmartTrack(TM) Invisalign(R) Aligner Material. Align Technology.
Align Technology, 2017. Align Technology Receives U.S. Patents for SmartTrack(R)
Invisalign(R) Aligner Material. Align Technology.
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
573
Align Technology, 2018. List of recommended materials for bonding attachments. Available
from:
,https://learn.invisalign.com/attachments/bonding/recommendedmaterials.
(accessed 26.05.18).
Ansari, M.Y., Agarwal, D.K., Gupta, A., Bhattacharya, P., Ansar, J., Bhandari, R., 2016.
Shear bond strength of ceramic brackets with different base designs: comparative invitro study. J. Clin. Diagn. Res. 10, ZC64 ZC68.
Anusavice, K.J., Shen, C., Rawls, H.R., 2013. Phillips’ Science of Dental Materials. Elsevier
Health Sciences.
Arash, V., Rabiee, M., Rakhshan, V., Khorasani, S., Sobouti, F., 2015. In vitro evaluation of
frictional forces of two ceramic orthodontic brackets versus a stainless steel bracket in
combination with two types of archwires. J. Orthod. Sci. 4, 42 46.
Arici, S., Regan, D., 1997. Alternatives to ceramic brackets: the tensile bond strengths of two
aesthetic brackets compared ex vivo with stainless steel foil-mesh bracket bases. Br. J.
Orthod. 24, 133 137.
Arici, N., Akdeniz, B.S., Arici, S., 2015. Comparison of the frictional characteristics of
aesthetic orthodontic brackets measured using a modified in vitro technique. Korean J.
Orthod. 45, 29 37.
Awosika, O., Kao, S., Rengifo-Pardo, M., Ehrlich, A., 2017. Angioedema, stomatitis, and
urticaria caused by contact allergy to Invisalign. Dermatitis 28, 323 324.
Baldwin, D.K., King, G., Ramsay, D.S., Huang, G., Bollen, A.M., 2008. Activation time and
material stiffness of sequential removable orthodontic appliances. Part 3: Premolar
extraction patients. Am. J. Orthod. Dentofacial Orthop. 133, 837 845.
Barone, S., Paoli, A., Razionale, A.V., Savignano, R., 2016. Computational design and engineering of polymeric orthodontic aligners. Int. J. Numer. Method Biomed. Eng. 33, e2839.
Birnie, D., 1990. Ceramic brackets. Br. J. Orthod. 17, 71 74.
Bishara, S.E., Fehr, D.E., Jakobsen, J.R., 1993. A comparative study of the debonding
strengths of different ceramic brackets, enamel conditioners, and adhesives. Am. J.
Orthod. Dentofacial Orthop. 104, 170 179.
Bollen, A.M., Huang, G., King, G., Hujoel, P., Ma, T., 2003. Activation time and material
stiffness of sequential removable orthodontic appliances. Part 1: Ability to complete
treatment. Am. J. Orthod. Dentofacial Orthop. 124, 496 501.
Boyd, R.L., 2008. Esthetic orthodontic treatment using the Invisalign appliance for moderate
to complex malocclusions. J. Dent. Educ. 72, 948 967.
Boyd, R.L., Miller, R.J., Vlaskalic, V., 2000. The Invisalign system in adult orthodontics:
mild crowding and space closure cases. J. Clin. Orthod. 34, 203 212.
Brantley, W.A., Eliades, T., 2001. Orthodontic Materials: Scientific and Clinical Aspects.
Thieme.
Brantley, W.A., Eliades, T., 2017. Orthodontic Applications of Biomaterials: A Clinical
Guide, 2016, Elsevier Science.
Brascher, A.K., Zuran, D., Feldmann J.R., R.E., Benrath, J., 2016. Patient survey on
Invisalign(R) treatment comparen the SmartTrack(R) material to the previous aligner
material. J. Orofac. Orthop. 77, 432 438.
Burstone, C.J., Goldberg, A.J., 1980. Beta titanium: a new orthodontic alloy. Am. J. Orthod.
Dentofacial Orthop. 77, 121 132.
Burstone, C.J., Qin, B., Morton, J.Y., 1985. Chinese NiTi wire—a new orthodontic alloy.
Am. J. Orthod. 87, 445 452.
Cash, A., Curtis, R., Garrigia-Majo, D., Mcdonald, F., 2004. A comparative study of the
static and kinetic frictional resistance of titanium molybdenum alloy archwires in stainless steel brackets. Eur. J. Orthod. 26, 105 111.
574
Advanced Dental Biomaterials
Chhibber, A., Agarwal, S., Yadav, S., Kuo, C.L., Upadhyay, M., 2018. Which orthodontic
appliance is best for oral hygiene? A randomized clinical trial. Am. J. Orthod.
Dentofacial Orthop. 153, 175 183.
Choi, S.H., Kang, D.Y., Hwang, C.J., 2014. Surface roughness of three types of modern plastic bracket slot floors and frictional resistance. Angle Orthod. 84, 177 183.
Clements, K.M., Bollen, A.M., Huang, G., King, G., Hujoel, P., Ma, T., 2003. Activation
time and material stiffness of sequential removable orthodontic appliances. Part 2:
Dental improvements. Am. J. Orthod. Dentofacial Orthop. 124, 502 508.
Cowley, D.P., Mah, J., O’toole, B., 2012. The effect of gingival-margin design on the retention of thermoformed aligners. J. Clin. Orthod. 46, 697 702. quiz 705.
Dalstra, M., Denes, G., Melsen, B., 2000. Titanium-niobium, a new finishing wire alloy.
Clin. Orthod. Res. 3, 6 14.
Dobrin, R.J., Kamel, I.L., Musich, D.R., 1975. Load-deformation characteristics of polycarbonate orthodontic brackets. Am. J. Orthod. 67, 24 33.
Dupaix, R.B., Boyce, M.C., 2005. Finite strain behavior of poly(ethylene terephthalate)
(PET) and poly(ethylene terephthalate)-glycol (PETG). Polymer 46, 4827 4838.
Elekdag-Turk, S., Isci, D., Ozkalayci, N., Turk, T., 2009. Debonding characteristics of a
polymer mesh base ceramic bracket bonded with two different conditioning methods.
Eur. J. Orthod. 31, 84 89.
Eliades, T., 2007. Orthodontic materials research and applications: Part 2. Current status and
projected future developments in materials and biocompatibility. Am. J. Orthod.
Dentofacial Orthop. 131, 253 262.
Eliades, T., Brantley, W.A., 2016. Orthodontic Applications of Biomaterials: A Clinical
Guide. Elsevier Science.
Eliades, T., Zinelis, S., Eliades, G., Athanasiou, A.E., 2002. Nickel content of as-received,
retrieved, and recycled stainless steel brackets. Am. J. Orthod. Dentofacial Orthop. 122,
217 220.
Eliades, T., Zinelis, S., Eliades, G., Athanasiou, A.E., 2003. Characterization of as-received,
retrieved, and recycled stainless steel brackets. J. Orofac. Orthop. 64, 80 87.
Eliades, T., Gioka, C., Zinelis, S., Eliades, G., Makou, M., 2004. Plastic brackets: hardness
and associated clinical implications. World J. Orthod. 5, 62 66.
Faltermeier, A., Rosentritt, M., Faltermeier, R., Muessig, D., 2007. Influence of fibre and
filler reinforcement of plastic brackets: an in vitro study. Eur. J. Orthod. 29, 304 309.
Fang, D., Zhang, N., Chen, H., Bai, Y., 2013. Dynamic stress relaxation of orthodontic thermoplastic materials in a simulated oral environment. Dent. Mater. J. 32, 946 951.
Feldner, J.C., Sarkar, N.K., Sheridan, J.J., Lancaster, D.M., 1994. In vitro torque-deformation
characteristics of orthodontic polycarbonate brackets. Am. J. Orthod. Dentofacial
Orthop. 106, 265 272.
Flores, D.A., Choi, L.K., Caruso, J.M., Tomlinson, J.L., Scott, G.E., Jeiroudi, M.T., 1994.
Deformation of metal brackets: a comparative study. Angle Orthod. 64, 283 290.
Frank, C.A., Nikolai, R.J., 1980. A comparative study of frictional resistances between orthodontic bracket and arch wire. Am. J. Orthod. 78, 593 609.
Frick, A., Rochman, A., 2004. Characterization of TPU-elastomers by thermal analysis
(DSC). Polym. Test. 23, 413 417.
Gao, L., Wichelhaus, A., 2017. Forces and moments delivered by the PET-G aligner to a
maxillary central incisor for palatal tipping and intrusion. Angle Orthod. 87, 534 541.
Gardner, G.D., Dunn, W.J., Taloumis, L., 2003. Wear comparison of thermoplastic materials
used for orthodontic retainers. Am. J. Orthod. Dentofacial Orthop. 124, 294 297.
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
575
Gerard Bradley, T., Teske, L., Eliades, G., Zinelis, S., Eliades, T., 2016. Do the mechanical
and chemical properties of InvisalignTM appliances change after use? A retrieval analysis. Eur. J. Orthod. 38, 27 31.
Gioka, C., Bourauel, C., Zinelis, S., Eliades, T., Silikas, N., Eliades, G., 2004. Titanium
orthodontic brackets: structure, composition, hardness and ionic release. Dent. Mater.
20, 693 700.
Goldberg, J., Burstone, C.J., 1979. An evaluation of beta titanium alloys for use in orthodontic appliances. J. Dent. Res. 58, 593 599.
Goldberg, A.J., Morton, J., Burstone, C.J., 1983. The flexure modulus of elasticity of orthodontic wires. J. Dent. Res. 62, 856 858.
Gracco, A., Mazzoli, A., Favoni, O., Conti, C., Ferraris, P., Tosi, G., et al., 2009. Short-term
chemical and physical changes in Invisalign appliances. Aust. Orthod. J. 25, 34 40.
Grimsdottir, M.R., Gjerdet, N.R., Hensten-Pettersen, A., 1992. Composition and in vitro corrosion of orthodontic appliances. Am. J. Orthod. Dentofacial Orthop. 101, 525 532.
Gwinnett, A.J., 1988. A comparison of shear bond strengths of metal and ceramic brackets.
Am. J. Orthod. Dentofacial Orthop. 93, 346 348.
Haddad, A.C., Tortamano, A., Souza, A.L., Oliveira, P.V., 2009. An in vitro comparison of
nickel and chromium release from brackets. Braz. Oral Res. 23, 399 406.
Hahn, W., Dathe, H., Fialka-Fricke, J., Fricke-Zech, S., Zapf, A., Kubein-Meesenburg, D.,
et al., 2009. Influence of thermoplastic appliance thickness on the magnitude of force
delivered to a maxillary central incisor during tipping. Am. J. Orthod. Dentofacial
Orthop. 136, 12 13. 12 e1-7; discussion.
Hahn, W., Engelke, B., Jung, K., Dathe, H., Kramer, F.J., Rodig, T., et al., 2011. The influence of occlusal forces on force delivery properties of aligners during rotation of an
upper central incisor. Angle Orthod. 81, 1057 1063.
Hamula, D.W., Hamula, W., Sernetz, F., 1996. Pure titanium orthodontic brackets. J. Clin.
Orthod. 30, 140 144.
Harzer, W., Bourauel, C., Gmyrek, H., 2004. Torque capacity of metal and polycarbonate
brackets with and without a metal slot. Eur. J. Orthod. 26, 435 441.
Hennessy, J., Al-Awadhi, E.A., 2016. Clear aligners generations and orthodontic tooth movement. J. Orthod. 43, 68 76.
Jones, R.M., 2009. Deformation Theory of Plasticity. Bull Ridge Pub.
Jorge, J.H., Giampaolo, E.T., Machado, A.L., Vergani, C.E., 2003. Cytotoxicity of denture
base acrylic resins: a literature review. J. Prosthet. Dent. 90, 190 193.
Kapila, S., Sachdeva, R., 1989. Mechanical properties and clinical applications of orthodontic
wires. Am. J. Orthod. Dentofacial Orthop. 96, 100 109.
Kapur, R., Sinha, P.K., Nanda, R.S., 1999. Frictional resistance in orthodontic brackets with
repeated use. Am. J. Orthod. Dentofacial Orthop. 116, 400 404.
Keith, O., Kusy, R.P., Whitley, J.Q., 1994. Zirconia brackets: an evaluation of morphology
and coefficients of friction. Am. J. Orthod. Dentofacial Orthop. 106, 605 614.
Kesling, H.D., 1945. The philosophy of the tooth positioning appliance. Am. J. Orthod. Oral
Surg. 31, 297 304.
Kohda, N., Iijima, M., Muguruma, T., Brantley, W.A., Ahluwalia, K.S., Mizoguchi, I., 2013.
Effects of mechanical properties of thermoplastic materials on the initial force of thermoplastic appliances. Angle Orthod. 83, 476 483.
Kravitz, N.D., Kusnoto, B., Begole, E., Obrez, A., Agran, B., 2009. How well does
Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement
with Invisalign. Am. J. Orthod. Dentofacial Orthop. 135, 27 35.
576
Advanced Dental Biomaterials
Krishnan, V., Kumar, K.J., 2004. Weld characteristics of orthodontic archwire materials.
Angle Orthod. 74, 533 538.
Kumar, B.S., Miryala, S., Kumar, K.K., Shameem, K., Regalla, R.R., 2014. Comparative
evaluation of friction resistance of titanium, stainless steel, ceramic and ceramic with
metal insert brackets with varying dimensions of stainless steel wire: an in vitro multicenter study. J. Int. Oral Health 6, 66 71.
Kusy, R.P., 1988. Morphology of polycrystalline alumina brackets and its relationship to
fracture toughness and strength. Angle Orthod. 58, 197 203.
Kusy, R.P., O’Grady, P.W., 2000. Evaluation of titanium brackets for orthodontic treatment:
Part II—The active configuration. Am. J. Orthod. Dentofacial Orthop. 118, 675 684.
Kusy, R.P., Whitley, J.Q., Ambrose, W.W., Newman, J.G., 1998. Evaluation of titanium
brackets for orthodontic treatment: Part I. The passive configuration. Am. J. Orthod.
Dentofacial Orthop. 114, 558 572.
Kwon, J.S., Lee, Y.K., Lim, B.S., Lim, Y.K., 2008. Force delivery properties of thermoplastic orthodontic materials. Am. J. Orthod. Dentofacial Orthop. 133, 228 234. quiz 328
e1.
Landel, R.F., Nielsen, L.E., 1993. Mechanical Properties of Polymers and Composites, second ed. Taylor & Francis.
Liljelind, I., Norberg, C., Egelrud, L., Westberg, H., Eriksson, K., Nylander-French, L.A.,
2010. Dermal and inhalation exposure to methylene bisphenyl isocyanate (MDI) in iron
foundry workers. Ann. Occup. Hyg. 54, 31 40.
Lombardo, L., Martines, E., Mazzanti, V., Arreghini, A., Mollica, F., Siciliani, G., 2017.
Stress relaxation properties of four orthodontic aligner materials: a 24-hour in vitro
study. Angle Orthod. 87, 11 18.
Lu, Q.-W., Macosko, C.W., 2004. Comparing the compatibility of various functionalized
polypropylenes with thermoplastic polyurethane (TPU). Polymer 45, 1981 1991.
Lutz, F., Phillips, R.W., Roulet, J.F., Setcos, J.C., 1984. In vivo and in vitro wear of potential
posterior composites. J. Dent. Res. 63, 914 920.
Matasa, C.G., 1992. Direct bonding metallic brackets: where are they heading? Am. J.
Orthod. Dentofacial Orthop. 102, 552 560.
Matasa, C.G., 1998. Metal strength of direct bonding brackets. Am. J. Orthod. Dentofacial
Orthop. 113, 282 286.
Matsui, S., Umezaki, E., Komazawa, D., Otsuka, Y., Suda, N., 2015. Evaluation of mechanical properties of esthetic brackets. J. Dent. Biomech. 6, 1758736015574401.
Mcnamara, J.A., Kramer, K.L., Juenker, J.P., 1985. Invisible retainers. J. Clin. Orthod. 19,
570 578.
Michelberger, D.J., Eadie, R.L., Faulkner, M.G., Glover, K.E., Prasad, N.G., Major, P.W.,
2000. The friction and wear patterns of orthodontic brackets and archwires in the dry
state. Am. J. Orthod. Dentofacial Orthop. 118, 662 674.
Miethke, R.R., Brauner, K., 2007. A comparison of the periodontal health of patients during
treatment with the Invisalign system and with fixed lingual appliances. J. Orofac.
Orthop. 68, 223 231.
Miller, K.B., Mcgorray, S.P., Womack, R., Quintero, J.C., Perelmuter, M., Gibson, J., et al.,
2007. A comparison of treatment impacts between Invisalign aligner and fixed appliance
therapy during the first week of treatment. Am. J. Orthod. Dentofacial Orthop. 131
(302), e1 e9.
Miura, F., Mogi, M., Ohura, Y., Hamanaka, H., 1986. The super-elastic property of the
Japanese NiTi alloy wire for use in orthodontics. Am. J. Orthod. Dentofacial Orthop. 90,
1 10.
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
577
Moller, M., Klocke, A., Sadat-Khonsari, R., Schlegel, V., Kahl-Nieke, B., 2009. Torque
stability of plastic brackets following multiple loading and artificial material aging—an
in-vitro comparison. J. Orofac. Orthop. 70, 385 395.
Moore, M.M., Harrington, E., Rock, W.P., 2004. Factors affecting friction in the pre-adjusted
appliance. Eur. J. Orthod. 26, 579 583.
Morton, J., Derakhshan, M., Kaza, S., Li, C.H., 2017. Design of the Invisalign system performance. Semin. Orthod. 23, 3 11.
Nahoum, H.I., 1964. The vacuum formed dental contour appliance. N.Y. State Dent. J. 9,
385 390.
Nahoum, H.I., 2014. Forces and moments generated by removable thermoplastic aligners.
Am. J. Orthod. Dentofacial Orthop. 146, 545 546.
Nair, S.V., Padmanabhan, R., Janardhanam, P., 2012. Evaluation of the effect of bracket and
archwire composition on frictional forces in the buccal segments. Indian J. Dent. Res.
23, 203 208.
Nikolai, R.J., 1997. Orthodontic wire: a continuing evolution. Semin. Orthod. 3, 157 165.
Oh, K.-T., Kim, K.-N., Lee, M., Park, Y.-S., 2002. Corrosion wear of high molybdenum and
nitrogen stainless steel for biomedical applications. J. Electrochem. Soc. 149,
B146 B153.
Oh, K.T., Choo, S.U., Kim, K.M., Kim, K.N., 2005. A stainless steel bracket for orthodontic
application. Eur. J. Orthod. 27, 237 244.
Olsen, M.E., Bishara, S.E., Boyer, D.B., Jakobsen, J.R., 1996. Effect of varying etching times
on the bond strength of ceramic brackets. Am. J. Orthod. Dentofacial Orthop. 109,
403 409.
Pasha, A., Vishwakarma, S., Narayan, A., Vinay, K., Shetty, S.V., Roy, P.P., 2015.
Comparison of frictional forces generated by a new ceramic bracket with the conventional brackets using unconventional and conventional ligation system and the selfligating brackets: an in vitro study. J. Int. Oral Health 7, 108 113.
Pithon, M.M., Oliveira, M.V., Ruellas, A.C., Bolognese, A.M., Romano, F.L., 2007. Shear
bond strength of orthodontic brackets to enamel under different surface treatment conditions. J. Appl. Oral Sci. 15, 127 130.
Platt, J.A., Guzman, A., Zuccari, A., Thornburg, D.W., Rhodes, B.F., Oshida, Y., et al.,
1997. Corrosion behavior of 2205 duplex stainless steel. Am. J. Orthod. Dentofacial
Orthop. 112, 69 79.
Ponitz, R.J., 1971. Invisible retainers. Am. J. Orthod. 59, 266 272.
Premaraj, T., Simet, S., Beatty, M., Premaraj, S., 2014a. Oral epithelial cell reaction after
exposure to Invisalign plastic material. Am. J. Orthod. Dentofacial Orthop. 145, 64 71.
Premaraj, T.S., Simet, S., Beatty, M., Premaraj, S., 2014b. Authors’ response. Am. J. Orthod.
Dentofacial Orthop. 145, 551.
Ratner, B.D., Hoffman, A.S., Schoen, F.J., Lemons, J.E., 2012. Biomaterials Science: An
Introduction to Materials in Medicine. Elsevier Science.
Reclaru, L., Meyer, J.M., 1998. Effects of fluorides on titanium and other dental alloys in
dentistry. Biomaterials 19, 85 92.
Reddy, Y.G., Sharma, R., Singh, A., Agrawal, V., Agrawal, V., Chaturvedi, S., 2013. The
shear bond strengths of metal and ceramic brackets: an in-vitro comparative study. J.
Clin. Diagn. Res. 7, 1495 1497.
Remensnyder, O., 1926. A gum-massaging appliance in the treatment of pyorrhea. Dent.
Cosmos 28, 381 384.
Ren, Y., Maltha, J.C., Kuijpers-Jagtman, A.M., 2003. Optimum force magnitude for orthodontic tooth movement: a systematic literature review. Angle Orthod. 73, 86 92.
578
Advanced Dental Biomaterials
Ren, Y., Maltha, J.C., Van’t Hof, M.A., Kuijpers-Jagtman, A.M., 2004. Optimum force magnitude for orthodontic tooth movement: a mathematic model. Am. J. Orthod.
Dentofacial Orthop. 125, 71 77.
Rodriguez-Mercado, J.J., Roldan-Reyes, E., Altamirano-Lozano, M., 2003. Genotoxic effects
of vanadium(IV) in human peripheral blood cells. Toxicol. Lett. 144, 359 369.
Rossini, G., Parrini, S., Castroflorio, T., Deregibus, A., Debernardi, C.L., 2015. Efficacy of
clear aligners in controlling orthodontic tooth movement: a systematic review. Angle
Orthod. 85, 881 889.
Rosvall, M.D., Fields, H.W., Ziuchkovski, J., Rosenstiel, S.F., Johnston, W.M., 2009.
Attractiveness, acceptability, and value of orthodontic appliances. Am. J. Orthod.
Dentofacial Orthop. 135, 276 277. 276 e1-12; discussion.
Russell, J.S., 2005. Current products and practice. J. Orthod. 32, 146 163.
Ryokawa, H., Miyazaki, Y., Fujishima, A., Miyazaki, T., Maki, K., 2006. The mechanical
properties of dental thermoplastic materials in a simulated intraoral environment.
Orthod. Waves 65, 64 72.
Sadat-Khonsari, R., Moshtaghy, A., Schlegel, V., Kahl-Nieke, B., Moller, M., Bauss, O.,
2004. Torque deformation characteristics of plastic brackets: a comparative study. J.
Orofac. Orthop. 65, 26 33.
Saunders, C.R., Kusy, R.P., 1994. Surface topography and frictional characteristics of
ceramic brackets. Am. J. Orthod. Dentofacial Orthop. 106, 76 87.
Schiff, N., Dalard, F., Lissac, M., Morgon, L., Grosgogeat, B., 2005. Corrosion resistance of
three orthodontic brackets: a comparative study of three fluoride mouthwashes. Eur. J.
Orthod. 27, 541 549.
Schott, T.C., Göz, G., 2011. Color fading of the blue compliance indicator encapsulated in
removable clear Invisalign Teens aligners. Angle Orthod. 81, 185 191.
Schupp, W., Haubrich, J., 2016. Aligner Orthodontics: Diagnostics, Biomechanics, Planning
and Treatment. Quintessence Publishing.
Schuster, S., Eliades, G., Zinelis, S., Eliades, T., Bradley, T.G., 2004. Structural conformation and leaching from in vitro aged and retrieved Invisalign appliances. Am. J. Orthod.
Dentofacial Orthop. 126, 725 728.
Sergl, H.G., Zentner, A., 1998. A comparative assessment of acceptance of different types of
functional appliances. Eur. J. Orthod. 20, 517 524.
Sheridan, J.J., Ledoux, W., Mcminn, R., 1993. Essix retainers: fabrication and supervision
for permanent retention. J. Clin. Orthod. 27, 37 45.
Simon, M., Keilig, L., Schwarze, J., Jung, B.A., Bourauel, C., 2014. Forces and moments
generated by removable thermoplastic aligners: incisor torque, premolar derotation, and
molar distalization. Am. J. Orthod. Dentofacial Orthop. 145, 728 736.
Springate, S.D., Winchester, L.J., 1991. An evaluation of zirconium oxide brackets: a preliminary laboratory and clinical report. Br. J. Orthod. 18, 203 209.
Swartz, M.L., 1988. Ceramic brackets. J. Clin. Orthod. 22, 82 88.
Toumelin-Chemla, F., Rouelle, F., Burdairon, G., 1996. Corrosive properties of fluoridecontaining odontologic gels against titanium. J. Dent. 24, 109 115.
Tuncay, O.C., 2006. In: Nguyen Cv, C.J. (Ed.), The Invisalign System. Quintessence Publ,
London [u.a.].
Vardimon, A.D., Robbins, D., Brosh, T., 2010. In-vivo von Mises strains during Invisalign
treatment. Am. J. Orthod. Dentofacial Orthop. 138, 399 409.
Voudouris, J.C., Schismenos, C., Lackovic, K., Kuftinec, M.M., 2010. Self-ligation esthetic
brackets with low frictional resistance. Angle Orthod. 80, 188 194.
Biomaterials used in orthodontics: brackets, archwires, and clear aligners
579
Wassell, R.W., Mccabe, J.F., Walls, A.W., 1994. A two-body frictional wear test. J. Dent.
Res. 73, 1546 1553.
Wheeler, T., Patel, N., Mcgorray, S., 2017. On orthodontic tooth movement. J. Aligner
Orthod. 1, 21 27.
White, D.W., Julien, K.C., Jacob, H., Campbell, P.M., Buschang, P.H., 2017. Discomfort
associated with Invisalign and traditional brackets: a randomized, prospective trial.
Angle Orthod. 87, 801 808.
Williams, C.L., Khalaf, K., 2013. Frictional resistance of three types of ceramic brackets. J.
Oral Maxillofac. Res. 4, e3.
Wisnewski, A.V., Srivastava, R., Herick, C., Xu, L., Lemus, R., Cain, H., et al., 2000.
Identification of human lung and skin proteins conjugated with hexamethylene diisocyanate in vitro and in vivo. Am. J. Respir. Crit. Care Med. 162, 2330 2336.
Wong, B.H., 2002. Invisalign A to Z. Am. J. Orthod. Dentofacial Orthop. 121, 540 541.
Wu, D., 2014. Oral epithelial cell reaction and Invisalign treatment. Am. J. Orthod.
Dentofacial Orthop. 145, 551.
Zhang, N., Bai, Y., Ding, X., Zhang, Y., 2011. Preparation and characterization of thermoplastic materials for invisible orthodontics. Dent. Mater. J. 30, 954 959.
Zinelis, S., Annousaki, O., Eliades, T., Makou, M., 2003. Metallographic structure and hardness of titanium orthodontic brackets. J. Orthop./Fortschritte der Kieferorthopädie 64,
426 433.
Zinelis, S., Eliades, T., Eliades, G., Makou, M., Silikas, N., 2005. Comparative assessment of
the roughness, hardness, and wear resistance of aesthetic bracket materials. Dent. Mater.
21, 890 894.
Zhylich, D., Krishnan, P., Muthusami, P., Rayner, T., Shroff, M., Doria, A., et al., 2017.
Effects of orthodontic appliances on the diagnostic quality of magnetic resonance
images of the head. Am J Orthod Dentofacial Orthop 151, 484 499.
21
Dental implants materials and
surface treatments
Shariq Najeeb1, Maria Mali2, Syed Azeem Ul Yaqin3,
Muhammad Sohail Zafar4, Zohaib Khurshid3, Abdullah Alwadaani3 and
Jukka P. Matinlinna5
1
National Center for Proteomics, Karachi University, Pakistan, 2Department of
Orthodontics, Islamic International Dental College & Hospital, Riphah International
University, Islamabad, Pakistan, 3Department of Prosthodontics and Dental Implantology,
College of Dentistry, King Faisal University, Al-Ahsa, Saudi Arabia, 4Department of
Restorative Dentistry, College of Dentistry, Taibah University, Almadinah Almunawwarah,
Saudi Arabia, 5Dental Materials Science, Applied Oral Sciences, Faculty of Dentistry, The
University of Hong Kong, Prince Philip Dental Hospital, Sai Ying Pun, Hong Kong SAR,
P.R. China
Chapter Outline
21.1
21.2
21.3
21.4
21.5
21.6
Introduction 581
Osseointegration: cellular and biomaterial aspects 583
Biomaterial properties and implant surface characteristics
Biomechanical properties of dental implants 584
Surface properties 585
Type of dental implant material 586
21.6.1 Alveolar bone properties 587
21.6.2 Influence of oral health and systemic disease on implant survival
21.7 Modification of the dental implants
584
587
588
21.7.1 Modification of titanium implants 588
21.8 Functionally graded/hierarchical dental implant surfaces 590
21.9 Modification of the polyetheretherketone dental implants 590
21.10 Modification of zirconia implants 592
21.11 Conclusion 592
References 592
21.1
Introduction
In general, a dental implant is a synthetic medical device that is surgically placed
directly into the alveolar bone and supports a prosthodontic or an orthodontic appliance (Adell, 1981). Ideally, there needs to be a direct physical, chemical, and biological interface between the human tissues and the implant material (Le Guéhennec
et al., 2007). There are two main components of a dental implant: the abutment and
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00021-9
Copyright © 2019 Elsevier Ltd. All rights reserved.
582
Advanced Dental Biomaterials
Figure 21.1 A titanium screw in the dog mandible. The implant is osseointegrated and the
soft tissue integration is present. The abutment connects the implants with the crown, which
is made of metal in this experimental setting.
Source: Adapted from Gruber, R., Bosshardt, D.D., 2014. Dental implantology and implants
—tissue interface. In: Stem Cell Biology and Tissue Engineering in Dental Sciences.
Academic Press, pp. 735 747. https://doi.org/10.1016/B978-0-12-397157-9.00078-3, with
publisher permission (Gruber and Bosshardt, 2014).
the screw (fixture). The abutment is the portion that is visible above the gingiva
level and retains or supports a prosthodontic or an orthodontic appliance, while the
screw or the root of the implant is submerged in the alveolar bone. As a dental
implant is a foreign object, it is imperative for the human hard and soft tissues to
“accept” it and form an intimate physical, stable, and functional interface with it
(Annunziata and Guida, 2015). The initial goal of implant therapy is to achieve
osseointegration, which is the direct stabilized physical and structural interface
between the implant and the surrounding bone. A diagram of an osseointegrated
implant is shown in Fig. 21.1.
Mankind has tried to use various materials as dental implants. Archeological evidence indicates the use of ivory, human teeth, bamboo, and some metal alloys as
implants in ancient civilizations. However, it was not until the 1950s that titanium
Dental implants materials and surface treatments
583
was attempted as an implant material when titanium chambers were placed into the
soft tissues of rabbit ears at the University of Cambridge (Brånemark and
Lindström, 1963). While studying the process of bone healing at Lund University,
Per-Ingvar Brånemark noticed that he was unable to remove the titanium chambers
from rabbit femurs. Following research on animal and human subjects, Brånemark
developed further the contemporary titanium dental implant. In 1965 he placed the
implants in the jaws of human volunteers. He termed this stable physical and biofunctional interface between bone and implant as osseointegration (Brånemark and
Lindström, 1963).
There are two possible scenarios when an implant is placed into the alveolar
bone. The first possibility is the formation of a connective tissue between the
implant and the bone (Smeets et al., 2016). This scenario is unfavorable as it may
cause the implant to be loosened and dislodged from the bone, leading to implant
failure. The most favorable outcome of dental implant therapy is osseointegration
(also called osteointegration) which is the formation of a direct, stable interface
between the implant and surrounding bone.
Although the most common material used in implant dentistry has been traditionally titanium and its alloys, more recently several other materials have been
used as implants (Lang and Matinlinna, 2014). The aim of this chapter is to provide
the reader with a comprehensive background on the concept of osseointegration
along with implant biomaterials, prosthodontic and clinical aspects of oral implantology. Moreover, factors governing the failure and success rates of implants will
be discussed.
21.2
Osseointegration: cellular and biomaterial aspects
Following placement in the alveolar bone, the first tissue that comes into contact
with the implant material is blood (Telleman et al., 2010). Just within around 1 minute of implantation, plasma proteins are adsorbed onto the implant surface. Platelets
are attracted to, and interact with, the adsorbed proteins. Platelets play a vital role
in healing, blood clotting, and thrombus formation. Eventually, other cells migrate
to the implant site and interact with the implant surface proteins through membrane
receptors. Plasma delivers nutrients (glucose, proteins, amino acids, and cholesterol)
and other substances to the surgical site. The interactions of these substances and
cells alter the surface properties of the implant.
Several cells interact with the dental implant fixture surface following blood
clotting. However, mesenchymal stem cells (MSCs) play a determining factor in
healing of tissues around the implant. Growth factors released following surgery
and during inflammation have been indicated to attract MSCs to the implant surface
and adhere to it. In the right environment, MSCs have the potential to differentiate
into many different types of cells, including bone-forming cells (osteoblasts),
cartilage-forming cells (chondroblasts), and fibroblastic cells. Ideally, MSCs should
differentiate into osteoblasts around the portion of the dental implant submerged in
584
Advanced Dental Biomaterials
the alveolar bone, leading to osteointegration. However, if a fibrous capsule forms
instead, implant failure occurs. There are a number of factors that affect osseointegration. Local factors include biomaterial properties and implant surface characteristics, the quality of the alveolar bone, periodontal disease, and oral hygiene.
Systemic factors include general health, immunity smoking status, genetics, and
metabolic disease (Marei and El Backly, 2018; Viña et al., 2014; Zafar et al.,
2015).
21.3
Biomaterial properties and implant surface
characteristics
As dental implant therapy primarily involves placement of a foreign object (i.e., the
artificial implant) in direct contact with a living tissue, the type of the implant
material used, and its surface properties play a pivotal role in the success—or failure—of a dental implant. The abutment (root connection) portion of a dental
implant may be divided into two areas: the core and the surface. The core is the
main bulk of the dental material used in the construction of the implant (Lang and
Matinlinna, 2014; Aboushelib and Matinlinna, 2014), while the surface is the portion of the implant in direct contact with living tissue (Guillaume, 2016).
21.4
Biomechanical properties of dental implants
The bone and its related soft tissues are dynamic. They remodel according to the
physiomechanical demands throughout life. Most dental implant materials used
today are significantly less elastic when compared to human bone. According to
Wolff’s Law, the amount of bone remodeling and formation is dependent upon the
mechanical load applied to it (Frost, 1994). As evident in Table 21.1, titanium has a
significantly higher elastic modulus and tensile strength compared to bone. If a
Table 21.1 Comparison of the different hard tissue with dental implants materials with
relation to tensile strength and modulus of elasticity.
Material
Tensile
strength
Modulus of
elasticity
References
Enamel
Dentine
Human cortical bone
Titanium
PEEK
CFR-PEEK
47.5
104
104 121
954 976
80
120
40 83
15
14
102 110
3 4
18
Rees and Jacobsen (1993)
Rees and Jacobsen (1993)
Rho et al. (1993)
Niinomi (1998)
Sandler et al. (2002)
Sandler et al. (2002)
CFR-PEEK, carbon-reinforced polyetheretherketone; PEEK, polyetheretherketone.
Dental implants materials and surface treatments
585
relatively inelastic material, such as a titanium implant, is placed in the bone, it
may prevent the load from being transferred to the surrounding bone. This may
lead to bone resorption. This process is known as stress-shielding (Asgharzadeh
Shirazi et al., 2017). That said, one of the ideal properties of a dental implant material would be to have physical properties identical to that of alveolar bone.
However, it is very difficult to replicate nature in a cost-effective fashion. Hence,
research has been conducted to produce various Ti alloys (Lang and Matinlinna,
2014) and dental implant biocomposites that have similar mechanical behavior to
bone (Asgharzadeh Shirazi et al., 2017).
Commercially pure titanium is the most commonly used dental implant material.
Titanium is graded 1 4 according to the purity, that is, oxygen and iron contents.
Commercially pure type 4 titanium (grade 4 cpTi) is used to fabricate dental
implants. For example, Ti6Al4V is a grade 5 titanium alloy that has a higher fatigue
resistance and strength than other grades. Hence, Ti6Al4V is also used as dental
implant material. More recently, materials such as reinforced polymeric composites
(e.g., glass fiber reinforced composites), ceramics, and silicon nitrate have been
studied for potential dental implant applications (Osman and Swain, 2015; Zhang
and Matinlinna, 2012).
At the implant surface, two factors affect the initial bone formation around the
dental implant: surface roughness and hydrophilicity (Eliasa et al., 2012). Other factors, such as the presence of biomimetic molecules and factors in the implant material, may also impact osteointegration (Khurshid et al., 2018; Najeeb et al., 2017b).
Surface roughness dramatically increases the surface area of the dental implant (1)
to achieve higher initial implant stability by mechanical interlocking and (2) to
maximize cell adhesion at the surface to promote bone ingrowth into the surface
porosities. Surface roughness can be introduced at three levels: macro, micro, and
nano (Khurshid et al., 2015; Najeeb et al., 2016b). Macrolevel surface roughness is
the introduction of certain geometrical features to the implant design which are visible to the naked eye or measuring more than 10 µm. A tapered, root-like design and
threading are examples of macrolevel surface modifications that improve initial
implant fixation (Cook et al., 1982). However, solely opting out to use macrolevel
surface treatments increases the chances of ion-leakage. This said, in order to minimize ion-leakage but maximize bone ingrowth, microlevel (1 10 µm) and nanolevel (,1 µm) implant modifications are more appropriate. They may also be
concurrently used with certain macrolevel surface treatments (Ryu et al., 2014).
21.5
Surface properties
In general, human tissues comprise up to 60% water. Hence, it is widely understood
that it is important for the implant surface to be highly hydrophilic (Ferraris et al.,
2015). The hydrophilicity of a material is the measure of its affinity for water.
Ideally, the surface of a perfectly hydrophilic material should form a 0 degree angle
with a water droplet. However, practically speaking, a material such as a dental
586
Advanced Dental Biomaterials
Table 21.2 Some examples of titanium implant surface modifications and their respective
properties.
Implant surface
Surface roughness (Ra)
References
Pure titanium
Titanium-sprayed plasma
Plasma-sprayed apatite
Biomimetic calcium
0.22 6 0.01
7.01 6 2.09
1.06 6 0.21
1.83 6 0.64
Mabboux et al. (2004)
Bagno and Di Bello (2004)
Giavaresi et al. (2003)
Le Guéhennec et al. (2007)
implant is modified to form an angle which is less than 90 degrees with a water
droplet (Ferraris et al., 2015; Hong et al., 2013). The more a liquid droplet spreads
out over the surface of the implant material, the lower the surface contact angle.
Over the last few decades, a significant amount of research has been conducted to
improve the hydrophilicity of dental implants (Ferraris et al., 2015; Held et al.,
2013; Hong et al., 2013). It has been observed that highly hydrophilic dental
implant surfaces not only exhibit closer bone implant contact (Rupp et al., 2014)
but they may also activate macrophages to produce antiinflammatory factors
(Hotchkiss et al., 2017). Several methods that increase the hydrophilicity of dental
implants will be described in this chapter.
In addition to having a hydrophilic surface, a dental implant fixture should also
possess osseoconductive and/or osseoinductive properties (Le Guéhennec et al.,
2007). A material is said to be osseoinductive when it promotes the undifferentiated
mesenchymal cells in a tissue to mature into bone-forming osteoblasts, whereas
osseoconductive materials promote bone formation on their surface. A significant
amount of research has been conducted to improve the osseoconductive/osseoinductive properties of implant materials to enhance the bone implant interface.
Methods include production of nanoporous implant surfaces (Carradò et al., 2017),
laser treatment only (Han et al., 2017), spraying of osseoconductive materials such
as hydroxyapatite and fluoroapatite (Mohseni et al., 2014), using a laser-assisted
biomimetic coating of calcium phosphate (Nathanael et al., 2018), and functionalized biomimetic coatings with adhesion peptides for dental implants (Roessler
et al., 2001). Moreover, even eicosapentaenoic acid has been attempted in vivo
(Mustafa et al., 2016) and some silane coatings in vitro (Villard et al., 2015) as
potential, beneficial dental implant coatings. Ultraviolet light treatment and some
other disinfection methods may also be worth further study and consideration (Han
et al., 2017) (Table 21.2).
21.6
Type of dental implant material
As discussed above, grade 4 cpTi and its alloy Ti6Al4V are the most commonly
used dental implant material by manufacturers. Apart from titanium, there are several other materials which have been used clinically as dental implants. Carbon
fiber reinforced carbon had been studied as a potential dental implant material in
Dental implants materials and surface treatments
587
the 1970 80s (Adams et al., 1978). In addition, E-glass fibers have been attempted
and introduced (Zhang and Matinlinna, 2012). However, due to the possible release
of fiber debris from the implant into the periimplant tissues, the US Food and Drug
Administration consequently did not approve the use of carbon fiber implants in the
human body (Petersen, 2016). Nevertheless, ceramics such as zirconia offer a more
esthetic alternative to titanium (Cionca et al., 2017). More recently, polymeric reinforced composites, such as polyetheretherketone (PEEK), have been attempted and
tested in animals in order to assess their osseointegration with alveolar bone
(Najeeb et al., 2016d). In addition, silicon nitride, a ceramic used in spinal reconstruction and maxillofacial rehabilitation, has also been tested as a dental implant
material (Webster et al., 2012). Each material does have a different way of interaction with the human tissues. Hence, choosing the right biocompatible material for
implant applications is a major factor which plays an absolutely important role in
the clinical success of implants.
21.6.1 Alveolar bone properties
As proposed by Lekholm and Zarb, human bone can be classified into four types,
depending on its density (Al-Ekrish et al., 2018), as follows:
1.
2.
3.
4.
Type I—Primarily compact bone
Type II—A core of dense spongy (trabecular) bone surrounded by compact bone
Type III—A core of dense spongy bone surrounded by a thin layer of compact bone
Type IV—A core of low-density spongy bone surrounded by a thin layer compact bone
Most studies suggest that implants exhibit the optimal survival rate when placed
in Type I or Type II bone. On the other hand, although a 5-year study on 1045 dental implants found no difference in the survival rate of Types I, II, and III implants,
a failure rate of 35% was observed in implants placed in Type IV bone (Jaffin and
Berman, 1991). Nonetheless, a recent systematic review of the latest studies has
suggested that implant surface modifications may improve the survival rate of
implants placed in osteoporotic animal bones (Ghanem et al., 2017). However,
more clinical studies are necessary before conclusive evidence can be ascertained
(Dereka et al., 2018). Conventional radiography and computerized tomography can
both be used to assess the bone density before implant placement (Norton and
Gamble, 2001). In addition, a meticulous periodontal screening and recording protocol should be employed to document the clinical signs and symptoms of periodontal
disease before initiation of implant therapy. The reader is encouraged to refer to
textbooks focusing on clinical periodontology and implantology to learn more about
periodontal and implant disease and the surgical steps involved in implant therapy.
21.6.2 Influence of oral health and systemic disease on implant
survival
Several systemic diseases have been implicated in dental implant failures. Smoking,
age, uncontrolled diabetes, and a history of radiation therapy in the head and neck
588
Advanced Dental Biomaterials
region have been implicated in early implant failures (Dawson and Jasper, 2015). A
recently published systematic review by the authors of this chapter has indicated a
negative impact of Down syndrome on successful dental implant therapy (Najeeb
et al., 2017a).
21.7
Modification of the dental implants
Before dental implants are placed in the alveolar bone, their fixture surfaces are
modified. They may be modified by several mechanisms such as plasma spraying,
ion dispersion, coatings of bioactive materials (Khurshid et al., 2019; Najeeb et al.,
2016c; Zafar et al., 2019; Aivazi et al., 2016; Han et al., 2018), and antimicrobial
proteins/peptides (Khurshid et al., 2018, 2017a, 2017b, 2016). The mechanism of
modification primarily depends on the type of the core implant material. As stated
above, implants can be modified at the following levels: macro, micro, and nano.
Most contemporary dental implants are endosseous, screw-type devices (Le
Guéhennec et al., 2007) which are further modified at the surface and/or by introduction of bioactive substances within the core.
21.7.1 Modification of titanium implants
21.7.1.1 Titanium plasma spraying
Titanium plasma spraying (TPS) involves injecting titanium powder through a hot
plasma torch, as shown in Fig. 21.2. The molten titanium particles fuse and condense at the surface of the implant to produce a rough surface, enhancing the surface area for improved bone deposition and contact. Studies have indicated that the
Figure 21.2 A schematic diagram of the plasma-spraying process. A molten jet of a
surfactant is coated onto the implant surface. The molten material solidifies and adheres to
the implant surface.
Dental implants materials and surface treatments
589
thickness of the plasma coating is in the range of 40 50 µm and has an average
roughness of approximately 7 µm (Buser et al., 1991).
However, TPS has a major drawback: residual particles. Not only have titanium
particles been found in bone adjacent to TPS implant surfaces (Urban et al., 2000),
organs such as liver, spleen, and abdominal lymph nodes have all been observed to
contain the metallic particles in patients who have received hip and knee replacements (Urban et al., 2004). Although the long-term effects of metal debris found in
organs are unknown, titanium debris may have local and systemic inflammatory or
carcinogenic effects (Le Guéhennec et al., 2007). Hence, more recently, studies
have been conducted to produce more stable and bioactive titanium surfaces, which
are described in the following subsections.
21.7.1.2 Grit-blasting
Grit-blasting (or sometimes called sand-blasting) involves production of a rough
implant surface by means of a jet of a particles of an abrasive material under high
pressure (Lung and Matinlinna, 2012). Two commonly used abrasives used to gritblast implants are alumina (Al2O3) and titanium dioxide (TiO2). Although gritblasted dental implant surfaces have been observed to exhibit enhanced boneimplant contact in animal subjects, they may, however, exhibit drawbacks. First,
it has been generally believed that residual ceramic particles can detach from the
implant surface and cause inflammation in the periimplant bone (Esposito et al.,
1998; Le Guéhennec et al., 2007). However, an animal study by Piattelli et al.
(2003) has found no significant negative effects of residual alumina particles.
Moreover, alumina particles may undermine the otherwise excellent corrosion resistance of titanium (Aparicio et al., 2003). Other materials that have been used to
grit-blast titanium implants are titanium oxide (Hotchkiss et al., 2017; Ivanoff
et al., n.d.) and resorbable materials such as calcium phosphates (Xuereb et al.,
2015). More recently, grit-blasting with alumina has also been combined with treatment with NaOH, followed by heat treatment at 600 C to produce rough implant
surfaces (Herrero-Climent et al., 2018).
21.7.1.3 Nanostructured titanium implant surfaces
To maximize the surface area for cellular adhesion and protein adsorption, modification of titanium surfaces at the nanometer-scale has been suggested. Laser and
lithography can be employed to produce nanometer-sized roughness on titanium
implants (Anselme et al., 2002; Zhu et al., 2004). Modern 3D-printing technology
may also give some answers. Indeed, in vitro studies on 3D-printed implant surfaces possessing surface roughness in the range of 32 6 4 nm on Ti microparticles
and 40 6 4 nm on underlying flat Ti have exhibited the potential to promote osteoblast proliferation (Gulati et al., 2017). Nonetheless, although the production of
nano-sized implant modifications has the potential to enhance osseointegration, due
to the lack of animal and clinical studies, nanostructured implant surfaces are not
yet widely used in routine implant dentistry.
590
Advanced Dental Biomaterials
21.7.1.4 Acid-etching of titanium surfaces
Another possible way to roughen titanium implants is acid-etching, which is a process
like enamel and dentine etching employed prior to bonding to resin composites.
However, titanium implants, being alloys, require much stronger acids to be etched.
Hydrofluoric acid (HF), hydrochloric acid (HCl), nitric acid (HNO3), and sulfuric acid
(H2SO4) have been used to produce rough implant surfaces in the micrometer range
(Klokkevold et al., 2001; Zinger et al., 2004). Acid-etched surfaces have been
observed to exhibit higher osseointegration when compared to TPS implant surfaces,
possibly due to a greater surface area and a higher wettability (Cho and Park, 2003).
Moreover, etching by HF incorporates fluoride ions onto the implant, and these make
the surface more osseoconductive (Cooper et al., 2006). Recently, fluoride-modified
dental implants have been introduced and marketed as OsseoSpeed (Dentsply Sirona).
21.7.1.5 Calcium phosphate coated titanium surfaces
Calcium hydroxyapatite (CHAp) is a form of calcium phosphate primarily found in
the mineralized component of animal and human hard tissues. In regenerative medicine, CHAp has been used to promote the regeneration and healing of calcified tissue such as bone and teeth (Zhou and Lee, 2011). Similarly, when coated on dental
implants, CHAp has been found to enhance bone implant contact and cellular proliferation (Xuereb et al., 2015).
21.8
Functionally graded/hierarchical dental implant
surfaces
Some recent research in regenerative periodontology has proposed producing “functionally graded” or “hierarchical” biomaterial surfaces (Qasim et al., 2017). Rather
than consisting of just a core with a coated or modified surface, functionally graded
materials (FGMs) have multiple layers, with each layer possessing different physical, chemical, and biological properties (Hedia and Fouda, 2013). Functionally
graded CHAp coatings on titanium implants have shown promising results in vivo
(Watari et al., 1997). Moreover, computer simulation studies have suggested that
using FGMs may reduce the adverse effects of dental implants on alveolar bone
(Lin et al., 2009). Nevertheless, FGMs have yet to see use in routine clinical practice, owing to the need for more clinical and preclinical research.
21.9
Modification of the polyetheretherketone dental
implants
The ability to modify polymeric composites has enabled them to be used in
multiple fields in dentistry. For instance, resin composites have been used as
Dental implants materials and surface treatments
591
tooth-colored materials for decades, poly(methylmethacrylate)-based denture materials have proven to be user-friendly and durable prosthodontic materials.
Moreover, polymeric impression materials produce excellent surface detail and
elastic properties for producing accurate impressions of soft and hard oral tissues.
More recently, PEEK, a polymer produced by the step-growth polymerization of
bis-phenolate salts by dialkylation, has been suggested for use as a dental implant
material (Najeeb et al., 2015). In addition to being tooth-colored, PEEK may also
exert less adverse effects on the periodontal structures due to its physical properties
being like that of human bone (as shown in Table 21.1). Studies have suggested
that PEEK implants exhibit lesser stress-shielding when compared to titanium
implants. However, in its unmodified form, the osseointegration and bioactivity
exhibited by PEEK is inferior to those demonstrated by titanium implants (Najeeb
et al., 2016a). To address this issue, a number of methods have been proposed to
modify the properties of PEEK implants in order to enhance their osseointegration.
As shown in Fig. 21.3, PEEK may be combined with various bioactive materials
via the process of melt-blending. PEEK may be coated by CHAp through plasma
spraying, similarly to titanium implants (Fauchais and Vardelle, 2012). However,
plasma spraying at high temperatures on a polymer like PEEK may have deleterious
effects on the physical properties of not only the core polymer but also the
PEEK coating interface (Molitor et al., 2001). Nonthermal processes such as
electron-beam (e-beam) deposition, spin-coating, and plasma gas etching treatment
may circumvent that problem (Balmer et al., 2018; Dawson and Jasper, 2015; Han
et al., 2017; Lung and Matinlinna, 2012; Najeeb et al., 2017a). E-beam coating
involves the formation of a thin, nanorough coating of material on a substrate via
electron-induced deposition. Spin-coating is carried out by slowly dropping a solution of apatites in organic solvents onto the implant spinning at high speeds. In
plasma gas etching, the implant surface is exposed to plasma gases at high pressure
to produce nanorough surfaces. That said, probably the most unique aspect of
PEEK implants would be their ability to be combined with bioactive materials such
as apatite to produce potentially osteoconductive fiber-reinforced dental implants
(Yabutsuka et al., 2018). So far, no large-scale clinical trials have demonstrated
Figure 21.3 A schematic diagram of the melt-blending process by which bioactive PEEK
composite implants are produced. During the process, the bioactive particles are codispersed
with PEEK in molten form in a suitable solvent. When placed in a mold, the bioactive
composite can cool down and produce a solid which is then shaped into an implant. PEEK,
Polyetheretherketone.
592
Advanced Dental Biomaterials
long-term clinical viability of PEEK biocomposites. Nevertheless, positive results
from recent animal studies may bring these implants into wider use in the dental
clinics.
21.10
Modification of zirconia implants
The surface treatments employed for zirconia implants (Aboushelib and Matinlinna,
2014) are like those carried out on titanium implants. Acid-etching, lasermodification, and grit-blasting have all been used to enhance the bone implant
interface of zirconia implants (Oliva et al., n.d.). However, clinical data regarding
the 5-year survival rate of modified zirconia implants is limited. A systematic
review (in 2008) of seven animal studies by Wenz et al. (n.d.) failed to state any
recommendation regarding the use of zirconia implants in the clinical setting.
Although some reviews of clinical studies show a promising outcome of zirconia
implants after 60 months, more comparative studies are required to ascertain their
performance when compared to titanium (Balmer et al., 2018; Montero et al., 2015;
Wenz et al., n.d.).
21.11
Conclusion
The surface of dental implants is a vital factor. It may be improved in various ways
but the systemic health of the implant-recipient, surgical procedures, and the oral
environmental factors has major impacts on osseointegration. Nonetheless, materials such as PEEK and zirconia may present a viable esthetic alternative to titanium
in the near future.
References
Aboushelib, M.N., Matinlinna, J.P., 2014. Zirconia in implant dentistry. In: Matinlinna, J.P.
(Ed.), Handbook of Oral Biomaterials. Pan Stanford Publishing, Singapore,
pp. 459 476. Available from: https://doi.org/10.1201/b15644.
Adams, D., Williams, D.F., Hill, J., 1978. Carbon fiber-reinforced carbon as a potential
implant material. J. Biomed. Mater. Res. 12, 35 42. Available from: https://doi.org/
10.1002/jbm.820120104.
Adell, R., 1981. A 15-year study of osseointegrated implants in the treatment of the edentulous
jaw. Int. J. Oral Surg. Available from: https://doi.org/10.1016/S0300-9785(81)80077-4.
Aivazi, M., Hossein Fathi, M., Nejatidanesh, F., Mortazavi, V., HashemiBeni, B., Matinlinna,
J.P., et al., 2016. The evaluation of prepared microgroove pattern by femtosecond laser on
alumina-zirconia nano-composite for endosseous dental implant application. Lasers Med.
Sci. 31, 1837 1843. Available from: https://doi.org/10.1007/s10103-016-2059-8.
Al-Ekrish, A., Widmann, G., Alfadda, S., 2018. Revised, computed tomography based
Lekholm and Zarb Jawbone quality classification. Int. J. Prosthodont. 31, 342 345.
Available from: https://doi.org/10.11607/ijp.5714.
Dental implants materials and surface treatments
593
Annunziata, M., Guida, L., 2015. The effect of titanium surface modifications on dental
implant osseointegration. Biomaterials for Oral and Craniomaxillofacial Applications.
Karger Publishers, pp. 62 77. Available from: https://doi.org/10.1159/000381694.
Anselme, K., Bigerelle, M., Noël, B., Iost, A., Hardouin, P., 2002. Effect of grooved titanium
substratum on human osteoblastic cell growth. J. Biomed. Mater. Res. 60, 529 540.
Available from: https://doi.org/10.1002/jbm.10101.
Aparicio, C., Javier Gil, F., Fonseca, C., Barbosa, M., Planell, J.A., 2003. Corrosion behaviour of commercially pure titanium shot blasted with different materials and sizes of
shot particles for dental implant applications. Biomaterials 24, 263 273. Available
from: https://doi.org/10.1016/S0142-9612(02)00314-9.
Asgharzadeh Shirazi, H., Ayatollahi, M.R., Asnafi, A., 2017. To reduce the maximum stress
and the stress shielding effect around a dental implant bone interface using radial functionally graded biomaterials. Comput. Methods Biomech. Biomed. Eng. 20, 750 759.
Available from: https://doi.org/10.1080/10255842.2017.1299142.
Balmer, M., Spies, B.C., Vach, K., Kohal, R.-J., Hämmerle, C.H.F., Jung, R.E., 2018. Threeyear analysis of zirconia implants used for single-tooth replacement and three-unit fixed
dental prostheses: a prospective multicenter study. Clin. Oral Implants Res. 29,
290 299. Available from: https://doi.org/10.1111/clr.13115.
Brånemark, P.-I., Lindström, J., 1963. A modified rabbit’s ear chamber high-power highresolution studies in regenerated and preformed tissues. Anat. Rec. 145, 533 540.
Available from: https://doi.org/10.1002/ar.1091450406.
Buser, D., Schenk, R.K., Steinemann, S., Fiorellini, J.P., Fox, C.H., Stich, H., 1991.
Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J. Biomed. Mater. Res. 25, 889 902. Available
from: https://doi.org/10.1002/jbm.820250708.
Carradò, A., Perrin-Schmitt, F., Le, Q.V., Giraudel, M., Fischer, C., Koenig, G., et al., 2017.
Nanoporous hydroxyapatite/sodium titanate bilayer on titanium implants for improved
osteointegration. Dent. Mater. 33, 321 332. Available from: https://doi.org/10.1016/j.
dental.2016.12.013.
Cho, S.-A., Park, K.-T., 2003. The removal torque of titanium screw inserted in rabbit tibia
treated by dual acid etching. Biomaterials 24, 3611 3617. Available from: https://doi.
org/10.1016/S0142-9612(03)00218-7.
Cionca, N., Hashim, D., Mombelli, A., 2017. Zirconia dental implants: where are we now,
and where are we heading? Periodontology 2000 73, 241 258. Available from: https://
doi.org/10.1111/prd.12180.
Cook, S.D., Klawitter, J.J., Weinstein, A.M., 1982. The influence of implant geometry on the
stress distribution around dental implants. J. Biomed. Mater. Res. 16, 369 379.
Available from: https://doi.org/10.1002/jbm.820160406.
Cooper, L.F., Zhou, Y., Takebe, J., Guo, J., Abron, A., Holmén, A., et al., 2006. Fluoride
modification effects on osteoblast behavior and bone formation at TiO2 grit-blasted c.p.
titanium endosseous implants. Biomaterials 27, 926 936. Available from: https://doi.
org/10.1016/J.BIOMATERIALS.2005.07.009.
Dawson, D.R., Jasper, S., 2015. Key systemic and environmental risk factors for implant failure. Dent. Clin. North Am. 59, 25 39. Available from: https://doi.org/10.1016/J.
CDEN.2014.09.002.
Dereka, X., Calciolari, E., Donos, N., Mardas, N., 2018. Osseointegration in osteoporotic-like
condition: a systematic review of preclinical studies. J. Periodontal Res. Available from:
https://doi.org/10.1111/jre.12566.
594
Advanced Dental Biomaterials
Eliasa, C.N., Rocha, F.A., Nascimento, A.L., Coelho, P.G., 2012. Influence of implant shape,
surface morphology, surgical technique and bone quality on the primary stability of dental implants. J. Mech. Behav. Biomed. Mater. 16, 169 180. Available from: https://doi.
org/10.1016/j.jmbbm.2012.10.010.
Esposito, M., Hirsch, J.M., Lekholm, U., Thomsen, P., 1998. Biological factors contributing
to failures of osseointegrated oral implants: (II). Etiopathogenesis. Eur. J. Oral Sci.
Available from: https://doi.org/10.1046/j.0909-8836.t01-6-.x.
Fauchais, P., Vardelle, A., 2012. Solution and suspension plasma spraying of nanostructure
coatings. Advanced Plasma Spray Applications. InTech. Available from: https://doi.org/
10.5772/34449.
Ferraris, S., Bobbio, A., Miola, M., Spriano, S., 2015. Micro- and nano-textured, hydrophilic
and bioactive titanium dental implants. Surf. Coat. Technol. 276, 374 383. Available
from: https://doi.org/10.1016/J.SURFCOAT.2015.06.042.
Frost, H.M., 1994. Wolff’s law and bone’s structural adaptations to mechanical usage: an
overview for clinicians. Angle Orthod. Available from: https://doi.org/10.1043/00033219(1994)064 , 0175:WLABSA . 2.0.CO;2.
Ghanem, A., Kellesarian, S.V., Abduljabbar, T., Al-Hamoudi, N., Vohra, F., Javed, F., 2017.
Role of osteogenic coatings on implant surfaces in promoting bone-to-implant contact in
experimental osteoporosis. Implant Dent. 26, 770 777. Available from: https://doi.org/
10.1097/ID.0000000000000634.
Gruber, R., Bosshardt, D.D., 2014. Dental implantology and implants—tissue interface. Stem
Cell Biology and Tissue Engineering in Dental Sciences. Academic Press, pp. 735 747.
Available from: https://doi.org/10.1016/B978-0-12-397157-9.00078-3.
Guillaume, B., 2016. Les implants dentaires: revue. Morphologie . Available from: https://
doi.org/10.1016/j.morpho.2016.02.002.
Gulati, K., Prideaux, M., Kogawa, M., Lima-Marques, L., Atkins, G.J., Findlay, D.M.,
et al., 2017. Anodized 3D printed titanium implants with dual micro- and nano-scale
topography promote interaction with human osteoblasts and osteocyte-like cells. J.
Tissue Eng. Regen. Med. 11, 3313 3325. Available from: https://doi.org/10.1002/
term.2239.
Han, A., Tsoi, J., Matinlinna, J., Chen, Z., 2017. Influence of grit-blasting and hydrofluoric
acid etching treatment on surface characteristics and biofilm formation on zirconia.
Coatings 7, 130. Available from: https://doi.org/10.3390/coatings7080130.
Han, A., Tsoi, J.K.H., Matinlinna, J.P., Zhang, Y., Chen, Z., 2018. Effects of different sterilization methods on surface characteristics and biofilm formation on zirconia in vitro.
Dent. Mater. 34, 272 281. Available from: https://doi.org/10.1016/j.dental.2017.11.012.
Hedia, H.S., Fouda, N., 2013. A new design of dental implant coating using functionally
graded material. Materialprufung 55, 765 771. Available from: https://doi.org/10.3139/
120.110499.
Held, U., Rohner, D., Rothamel, D., 2013. Early loading of hydrophilic titanium implants
inserted in low-mineralized (D3 and D4) bone: one year results of a prospective clinical
trial. Head Face Med. 9, 37. Available from: https://doi.org/10.1186/1746-160X-9-37.
Herrero-Climent, M., Romero Ruiz, M.M., Calvo, P.L., Santos, J.V.R., Perez, R.A., Gil Mur,
F.J., 2018. Effectiveness of a new dental implant bioactive surface: histological and histomorphometric comparative study in minipigs. Clin. Oral Investig. 22, 1423 1432.
Available from: https://doi.org/10.1007/s00784-017-2223-y.
Hong, J., Kurt, S., Thor, A., 2013. A hydrophilic dental implant surface exhibit thrombogenic
properties in vitro. Clin. Implant Dent. Relat. Res. 15, 105 112. Available from: https://
doi.org/10.1111/j.1708-8208.2011.00362.x.
Dental implants materials and surface treatments
595
Hotchkiss, K.M., Ayad, N.B., Hyzy, S.L., Boyan, B.D., Olivares-Navarrete, R., 2017. Dental
implant surface chemistry and energy alter macrophage activation in vitro. Clin. Oral
Implants Res. 28, 414 423. Available from: https://doi.org/10.1111/clr.12814.
Ivanoff, C.-J., Widmark, G., Johansson, C., Wennerberg, A., n.d. Histologic evaluation of
bone response to oxidized and turned titanium micro-implants in human jawbone. Int. J.
Oral Maxillofac. Implants 18, 341 348.
Jaffin, R.A., Berman, C.L., 1991. The excessive loss of Branemark fixtures in type IV bone:
a 5-year analysis. J. Periodontol. 62, 2 4. Available from: https://doi.org/10.1902/
jop.1991.62.1.2.
Khurshid, Z., Zafar, M., Qasim, S., Shahab, S., Naseem, M., AbuReqaiba, A., et al., 2015.
Advances in nanotechnology for restorative dentistry. Materials (Basel) 8, 717 731.
Available from: https://doi.org/10.3390/ma8020717.
Khurshid, Z., Naseem, M., Sheikh, Z., Najeeb, S., Shahab, S., Zafar, M.S., 2016. Oral antimicrobial peptides: types and role in the oral cavity. Saudi Pharm. J. Available from:
https://doi.org/10.1016/j.jsps.2015.02.015.
Khurshid, Z., Najeeb, S., Mali, M., Moin, S.F., Raza, S.Q., Zohaib, S., et al., 2017a. Histatin
peptides: pharmacological functions and their applications in dentistry. Saudi Pharm. J.
Available from: https://doi.org/10.1016/j.jsps.2016.04.027.
Khurshid, Z., Naseem, M., Asiri, F.Y.I., Mali, M., Sannam Khan, R., Sahibzada, H.A., et al.,
2017b. Significance and diagnostic role of antimicrobial cathelicidins (LL-37) peptides
in oral health. Biomolecules 7. Available from: https://doi.org/10.3390/biom7040080.
Khurshid, Z., Zafar, M.S., Naseem, M., Khan, R.S., Najeeb, S., 2018. Human oral defensins
antimicrobial peptides: a future promising antimicrobial drug. Curr. Pharm. Des. 24,
1130 1137. Available from: https://doi.org/10.2174/1381612824666180403114615.
Khurshid, Z., Husain, S., Alotaibi, H., Rehman, R., Zafar, M.S., Farooq, I., et al., 2019. Novel
techniques of scaffold fabrication for bioactive glasses. Biomed. Ther. Clin. Appl. Bioact.
Glasses 497 519. Available from: https://doi.org/10.1016/B978-0-08-102196-5.00018-5.
Klokkevold, P.R., Johnson, P., Dadgostari, S., Davies, J.E., Caputo, A., Nishimura, R.D.,
2001. Early endosseous integration enhanced by dual acid etching of titanium: a torque
removal study in the rabbit. Clin. Oral Implants Res. 12, 350 357. Available from:
https://doi.org/10.1034/j.1600-0501.2001.012004350.x.
Lang, N.P., Matinlinna, J.P., 2014. Titanium in implant dentistry. In: Matinlinna, J.P. (Ed.),
Handbook of Oral Biomaterials. Pan Stanford Publishing, Singapore, pp. 339 358.
Available from: https://doi.org/10.1201/b15644.
Le Guéhennec, L., Soueidan, A., Layrolle, P., Amouriq, Y., 2007. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. Available from: https://
doi.org/10.1016/j.dental.2006.06.025.
Lin, D., Li, Q., Li, W., Zhou, S., Swain, M.V., 2009. Design optimization of functionally
graded dental implant for bone remodeling. Compos. Part B Eng. 40, 668 675.
Available from: https://doi.org/10.1016/J.COMPOSITESB.2009.04.015.
Lung, C.Y.K., Matinlinna, J.P., 2012. Aspects of silane coupling agents and surface conditioning in dentistry: an overview. Dent. Mater. 28, 467 477. Available from: https://
doi.org/10.1016/j.dental.2012.02.009.
Mabboux, F., Ponsonnet, L., Morrier, J.J., Jaffrezic, N., Barsotti, O., 2004. Surface free
energy and bacterial retention to saliva-coated dental implant materials—an in vitro
study. Colloids and Surfaces B: Biointerfaces 39 (4), 199 205.
Marei, M.K., El Backly, R.M., 2018. Dental mesenchymal stem cell-based translational
regenerative dentistry: from artificial to biological replacement. Front. Bioeng.
Biotechnol. 6, 49. Available from: https://doi.org/10.3389/fbioe.2018.00049.
596
Advanced Dental Biomaterials
Mohseni, E., Zalnezhad, E., Bushroa, A.R., 2014. Comparative investigation on the adhesion
of hydroxyapatite coating on Ti-6Al-4V implant: a review paper. Int. J. Adhes. Adhes.
48, 238 257. Available from: https://doi.org/10.1016/j.ijadhadh.2013.09.030.
Molitor, P., Barron, V., Young, T., 2001. Surface treatment of titanium for adhesive bonding
to polymer composites: a review. Int. J. Adhes. Adhes. 21, 129 136. Available from:
https://doi.org/10.1016/S0143-7496(00)00044-0.
Montero, J., Bravo, M., Guadilla, Y., Portillo, M., Blanco, L., Rojo, R., et al., 2015.
Comparison of clinical and histologic outcomes of zirconia versus titanium implants
placed in fresh sockets: a 5-month study in Beagles. Int. J. Oral Maxillofac. Implants
30, 773 780. Available from: https://doi.org/10.11607/jomi.3668.
Mustafa, A., Lung, C.Y.K., Mustafa, N.S., Mustafa, B.A., Kashmoola, M.A., Zwahlen, R.A.,
et al., 2016. EPA-coated titanium implants promote osteoconduction in white New Zealand
rabbits. Clin. Oral Implants Res. 27, 303 309. Available from: https://doi.org/10.1111/
clr.12525.
Najeeb, S., Khurshid, Z., Matinlinna, J.P., Siddiqui, F., Nassani, M.Z., Baroudi, K., 2015.
Nanomodified peek dental implants: bioactive composites and surface modification—a
review. Int. J. Dent. Available from: https://doi.org/10.1155/2015/381759.
Najeeb, S., Bds, Z.K., Bds, S.Z., Bds, M.S.Z., 2016a. Bioactivity and osseointegration of
PEEK are inferior to those of titanium: a systematic review. J. Oral Implantol. 42,
512 516. Available from: https://doi.org/10.1563/aaid-joi-D-16-00072.
Najeeb, S., Khurshid, Z., Agwan, A.S., Zafar, M.S., Alrahabi, M., Qasim, S.B., et al., 2016b.
Dental applications of nanodiamonds. Sci. Adv. Mater. 8, 2064 2070. Available from:
https://doi.org/10.1166/sam.2016.2993.
Najeeb, S., Khurshid, Z., Zafar, M.S., Khan, A.S., Zohaib, S., Martı́, J.M.N., et al., 2016c.
Modifications in glass ionomer cements: nano-sized fillers and bioactive nanoceramics.
Int. J. Mol. Sci. Available from: https://doi.org/10.3390/ijms17071134.
Najeeb, S., Zafar, M.S., Khurshid, Z., Siddiqui, F., 2016d. Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J. Prosthodont. Res. Available
from: https://doi.org/10.1016/j.jpor.2015.10.001.
Najeeb, S., Khurshid, Z., Siddiqui, F., Zohaib, S., Zafar, M.S., 2017a. Outcomes of dental
implant therapy in patients with Down syndrome: a systematic review. J. Evid. Based
Dent. Pract. Available from: https://doi.org/10.1016/j.jebdp.2017.05.003.
Najeeb, S., Zafar, M.S., Khurshid, Z., Zohaib, S., Hasan, S.M., Khan, R.S., 2017b.
Bisphosphonate releasing dental implant surface coatings and osseointegration: a systematic review. J. Taibah Univ. Med. Sci. 12, 369 375. Available from: https://doi.org/
10.1016/J.JTUMED.2017.05.007.
Nathanael, A.J., Oyane, A., Nakamura, M., Koga, K., Nishida, E., Tanaka, S., et al., 2018.
Calcium phosphate coating on dental composite resins by a laser-assisted biomimetic process. Heliyon 4, e00734. Available from: https://doi.org/10.1016/j.heliyon.2018.e00734.
Niinomi, M., 1998. Mechanical properties of biomedical titanium alloys. Mater. Sci. Eng. A
243 (1 2), 231 236.
Norton, M.R., Gamble, C., 2001. Bone classification: an objective scale of bone density using
the computerized tomography scan. Clin. Oral Implants Res. 12, 79 84. Available
from: https://doi.org/10.1034/j.1600-0501.2001.012001079.x.
Oliva, J., Oliva, X., Oliva, J.D., n.d. Five-year success rate of 831 consecutively placed zirconia
dental implants in humans: a comparison of three different rough surfaces. Int. J. Oral
Maxillofac. Implants 25, 336 344. https://doi.org/10.1590/S0103-50532007000100020
Osman, R.B., Swain, M.V., 2015. A critical review of dental implant materials with an
emphasis on titanium versus zirconia. Materials (Basel) . Available from: https://doi.org/
10.3390/ma8030932.
Dental implants materials and surface treatments
597
Petersen, R., 2016. Carbon fiber biocompatibility for implants. Fibers 4, 1. Available from:
https://doi.org/10.3390/fib4010001.
Piattelli, A., Degidi, M., Paolantonio, M., Mangano, C., Scarano, A., 2003. Residual aluminum
oxide on the surface of titanium implants has no effect on osseointegration. Biomaterials
24, 4081 4089. Available from: https://doi.org/10.1016/S0142-9612(03)00300-4.
Qasim, S.B., Najeeb, S., Delaine-Smith, R.M., Rawlinson, A., Ur Rehman, I., 2017. Potential
of electrospun chitosan fibers as a surface layer in functionally graded GTR membrane
for periodontal regeneration. Dent. Mater. 33, 71 83. Available from: https://doi.org/
10.1016/J.DENTAL.2016.10.003.
Rees, J.S., Jacobsen, P.H., 1993. The elastic moduli of enamel and dentine. Clini. Mater. 14
(1), 35 39.
Rho, J.Y., Ashman, R.B., Turner, C.H., 1993. Young’s modulus of trabecular and cortical
bone material: ultrasonic and microtensile measurements. J. Biomech. 26 (2), 111 119.
Roessler, S., Born, R., Scharnweber, D., Worch, H., Sewing, A., Dard, M., 2001. Biomimetic
coatings functionalized with adhesion peptides for dental implants. J. Mater. Sci. Mater.
Med. 871 877. Available from: https://doi.org/10.1023/A:1012807621414.
Rupp, F., Gittens, R.A., Scheideler, L., Marmur, A., Boyan, B.D., Schwartz, Z., et al., 2014.
A review on the wettability of dental implant surfaces I: theoretical and experimental
aspects. Acta Biomater. 10, 2894 2906. Available from: https://doi.org/10.1016/J.
ACTBIO.2014.02.040.
Ryu, H.-S., Namgung, C., Lee, J.-H., Lim, Y.-J., 2014. The influence of thread geometry on
implant osseointegration under immediate loading: a literature review. J. Adv.
Prosthodont. 6, 547 554. Available from: https://doi.org/10.4047/jap.2014.6.6.547.
Sandler, J., Werner, P., Shaffer, M.S.P., Demchuk, V., Altstädt, V., Alan, H., 2002. Windle.
Carbon-nanofibre-reinforced poly (ether ether ketone) composites. Compos. Part A:
Appl. Sci. Manuf. 33 (8), 1033 1039.
Smeets, R., Stadlinger, B., Schwarz, F., Beck-Broichsitter, B., Jung, O., Precht, C., et al.,
2016. Impact of dental implant surface modifications on osseointegration. Biomed. Res.
Int. Available from: https://doi.org/10.1155/2016/6285620.
Telleman, G., Albrektsson, T., Hoffman, M., Johansson, C.B., Vissink, A., Meijer, H.J.A.,
et al., 2010. Peri-implant endosseous healing properties of dual acid-etched miniimplants with a nanometer-sized deposition of CaP: a histological and histomorphometric human study. Clin. Implant Dent. Relat. Res. 12, 153 160. Available from:
https://doi.org/10.1111/j.1708-8208.2009.00147.x.
Urban, R.M., Jacobs, J.J., Tomlinson, M.J., Gavrilovic, J., Black, J., Peoc’h, M., 2000.
Dissemination of wear particles to the liver, spleen, and abdominal lymph nodes of
patients with hip or knee replacement. J. Bone Joint Surg. Am. 82, 457 476.
Urban, R.M., Tomlinson, M.J., Hall, D.J., Jacobs, J.J., 2004. Accumulation in liver and
spleen of metal particles generated at nonbearing surfaces in hip arthroplasty. J.
Arthroplasty 19, 94 101. Available from: https://doi.org/10.1016/J.ARTH.2004.09.013.
Villard, N., Seneviratne, C., Tsoi, J.K.H., Heinonen, M., Matinlinna, J., 2015. Candida albicans aspects of novel silane system-coated titanium and zirconia implant surfaces. Clin.
Oral Implants Res. 26, 332 341. Available from: https://doi.org/10.1111/clr.12338.
Viña, J.A., El-Alami, M., Gambini, J., Borras, C., Viña, J., Peñarrocha, M.A., 2014.
Application of mesenchymal stem cells in bone regenerative procedures in oral implantology. A literature review. J. Clin. Exp. Dent. 6, e60 e65. Available from: https://doi.
org/10.4317/jced.51186.
Watari, F., Yokoyama, A., Saso, F., Uo, M., Kawasaki, T., 1997. Fabrication and properties
of functionally graded dental implant. Compos. Part B Eng. 28, 5 11. Available from:
https://doi.org/10.1016/S1359-8368(96)00021-2.
598
Advanced Dental Biomaterials
Webster, T.J., Patel, A.A., Rahaman, M.N., Sonny Bal, B., 2012. Anti-infective and osteointegration properties of silicon nitride, poly(ether ether ketone), and titanium implants. Acta
Biomater. 8, 4447 4454. Available from: https://doi.org/10.1016/j.actbio.2012.07.038.
Wenz, H.J., Bartsch, J., Wolfart, S., Kern, M., n.d. Osseointegration and clinical success of
zirconia dental implants: a systematic review. Int. J. Prosthodont. 21, 27 36.
Xuereb, M., Camilleri, J., Attard, N., 2015. Systematic review of current dental implant coating materials and novel coating techniques. Int. J. Prosthodont. 28, 51 59. Available
from: https://doi.org/10.11607/ijp.4124.
Yabutsuka, T., Fukushima, K., Hiruta, T., Takai, S., Yao, T., 2018. Fabrication of bioactive
fiber-reinforced PEEK and MXD6 by incorporation of precursor of apatite. J. Biomed.
Mater. Res. Part B Appl. Biomater. 106, 2254 2265. Available from: https://doi.org/
10.1002/jbm.b.34025.
Zafar, M.S., Khurshid, Z., Almas, K., 2015. Oral tissue engineering progress and challenges.
Tissue Eng. Regen. Med. 12, 387 397. Available from: https://doi.org/10.1007/s13770015-0030-6.
Zafar, M.S., Farooq, I., Awais, M., Najeeb, S., Khurshid, Z., Zohaib, S., 2019. Bioactive surface coatings for enhancing osseointegration of dental implants. Biomed. Ther. Clin.
Appl. Bioact. Glasses 313 329. Available from: https://doi.org/10.1016/B978-0-08102196-5.00011-2.
Zhang, M., Matinlinna, J.P., 2012. E-glass fiber reinforced composites in dental applications.
Silicon 4, 73 78. Available from: https://doi.org/10.1007/s12633-011-9075-x.
Zhou, H., Lee, J., 2011. Nanoscale hydroxyapatite particles for bone tissue engineering. Acta
Biomater. 7, 2769 2781. Available from: https://doi.org/10.1016/J.ACTBIO.2011.03.019.
Zhu, X., Chen, J., Scheideler, L., Altebaeumer, T., Geis-Gerstorfer, J., Kern, D., 2004.
Cellular reactions of osteoblasts to micron- and submicron-scale porous structures of
titanium surfaces. Cells Tissues Organs 178, 13 22. Available from: https://doi.org/
10.1159/000081089.
Zinger, O., Anselme, K., Denzer, A., Habersetzer, P., Wieland, M., Jeanfils, J., et al., 2004.
Time-dependent morphology and adhesion of osteoblastic cells on titanium model surfaces featuring scale-resolved topography. Biomaterials 25, 2695 2711. Available
from: https://doi.org/10.1016/J.BIOMATERIALS.2003.09.111.
Graphene to improve the
physicomechanical properties
and bioactivity of the cements
22
Vinicius Rosa1,2, Francisco Javier Rodrı´guez-Lozano3
and Kyung-san Min4
1
Faculty of Dentistry, National University of Singapore, Singapore, Singapore, 2Centre for
Advanced 2D Materials and Graphene Research Centre, National University of Singapore,
Singapore, Singapore, 3School of Dentistry, University of Murcia, Murcia, Spain,
4
School of Dentistry, Chonbuk National University, Jeonju, South Korea
Chapter Outline
22.1 Introduction
599
22.1.1 Graphene and its derivatives 599
22.2 Graphene to improve cementitious materials
22.3 Conclusion 609
References 609
22.1
600
Introduction
22.1.1 Graphene and its derivatives
Graphene is a single atomic sheet of conjugated sp2 carbon atoms arranged in a
honeycomb pattern (Geim and Novoselov, 2007). It has high electron mobility and
thermal conductivity (Nair et al., 2008; Neto et al., 2009; Khare et al., 2007).
Graphene films are atomically thin, flexible, and light (0.77 mg/m2) . They present
very high elastic modulus and ultimate tensile strength. Moreover, graphene films
have large specific surface areas (2630 m2/g) that can be chemically modified to
provide new capabilities (Zhang et al., 2013b; Castro Neto et al., 2009; Bunch
et al., 2008; Dreyer et al., 2010; Geim and Novoselov, 2007).
Pristine graphene films can be produced in a relatively pure form by chemical
vapor deposition (CVD), graphene oxide (GO) reduction, exfoliation of graphite,
segregation from silicon carbide, and other methods (Faugeras et al., 2008; Zhou
et al., 2009; Lotya et al., 2009). In the traditional CVD process a sacrificial substrate (Cu or Ni) is placed in a reaction chamber where precursor gases (H2 and
CH4) are burned at elevated temperatures ( . 800 C). The gaseous pyrolysis
induces the nucleation of carbon atoms on the sacrificial substrate which grows in
large domains producing the graphene film (Lopez and Mittemeijer, 2004; Li et al.,
2009a,b; Xie et al., 2015b). While the CVD process allows the production of films
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00022-0
Copyright © 2019 Elsevier Ltd. All rights reserved.
600
Advanced Dental Biomaterials
with high quality and purity, the chemical methods (e.g., exfoliation) emerge as viable routes to produce graphene-based sheets on a large scale at low cost (Zheng and
Kim, 2015; Morin et al., 2017; Geim and Novoselov, 2007).
Graphene has two derivatives, namely, GO and reduced GO (rGO). The first is a
highly oxidized and hydrophilic form of graphene (Dreyer et al., 2010; Zheng and
Kim, 2015). GO has several oxygen-containing groups (e.g., OH, COOH) that
allow the material to be dispersed in organic solvents, water, different matrices, and
be combined with several molecules and compounds (Dreyer et al., 2010; Goenka
et al., 2014; Liu et al., 2013a). The most widely used method to produce GO is the liquid phase exfoliation of graphite (Perera et al., 2012; Rosa et al., 2016). This low-cost
method has been used for several years and relies on the charge transfer between the
solvent molecules and graphite layers to induce the separation of graphene sheets with
several micrometers in lateral size (Stankovich et al., 2007; Dreyer et al., 2010).
Finally, rGO can be produced by removal (reduction) of the oxygen-containing groups
from GO by several techniques (Goenka et al., 2014; Dreyer et al., 2010).
22.2
Graphene to improve cementitious materials
The term “bioactive cement” is used for a variety of cements with distinct chemical
compositions (e.g., hydroxyapatite, calcium silicate, β-tricalcium phosphate, and
others) that can induce and increase the mineralization processes in cells. These
materials often release calcium ions and increase the production of calcium
hydroxides. Moreover, they can induce the formation of an interfacial layer between
the cement and host tissue and the formation of apatite crystals over the surface of the
materials (Parirokh et al., 2018). Bioactive cements are widely used in vital pulp therapies (direct pulp capping, indirect pulp capping, pulpotomy), apexification, regenerative endodontics, perforation repair, root canal filling, root-end filling, treatment of
root fractures, filling of bone defects, and cementation of prostheses (Main et al.,
2004; Caron et al., 2014; Parirokh et al., 2018; Torabinejad et al., 2018).
One of the most classical bioactive cements is the mineral trioxide aggregate
(MTA), first introduced by Torabinejad in the 1990s. This is a derivative of
Portland cement and was approved by the Food and Drug Administration in 1997
(Parirokh and Torabinejad, 2010a). The properties of MTA (including its biocompatibility, bioactivity, osteoconductivity) have fostered a race to develop new
bioceramics or bioactive cements incorporating MTA (Torabinejad et al., 2018).
Some of these are Biodentine, BioRoot RCS, calcium-enriched mixture cement,
Endo-CPM, Endocem, EndoSequence, EndoBinder, EndoSeal MTA, GuttaFlow
Bioseal, iRoot, MicroMega MTA, MTA Bio, MTA Fillapex, MTA HP Repair,
MTA Plus, NeoMTA Plus, OrthoMTA, Quick-Set, RetroMTA, Tech Biosealer, and
TheraCal LC (Torabinejad et al., 2018).
One of the main advantages of bioceramics is their ability to dissociate calcium
ions. Nonetheless, the materials differ dramatically in the amounts of calcium that
are released and in the kinetics of this process. For instance, Biodentine releases
Graphene to improve the physicomechanical properties and bioactivity of the cements
601
approximate 95 ppm of calcium ions in the first 3 hours decreasing to 18 ppm at
24 hours (Gandolfi et al., 2015), while MTA releases approximately 5 and 25 ppm
for the same time points (Natu et al., 2015). Although the values of calcium release
may change according to the methodology used, the literature agrees on the potential of these materials to alkalinize the environment and increase the pH to values
around 11 and above (Natu et al., 2015; Prati and Gandolfi, 2015; Dubey et al.,
2017). Together, the calcium release and alkaline potential can increase the
phosphatase activity and the expression of several genes related to mineralization
processes such as osteocalcin, bone sialoprotein, and dentine sialophosphoprotein
(Hakki et al., 2009; Min et al., 2009; Maeda et al., 2010; Natu et al., 2015).
Despite these key features, these materials can present some essential clinical disadvantages. The main shortcoming may include long setting time, the presence of toxic
elements in the material composition, the potential for discoloration, difficult handling
characteristics, and high material cost (Parirokh and Torabinejad, 2010b; Natu et al.,
2015). Considering the setting time, it can be as long as 18 minutes for MTA while
the final set of this type of material can take up to 170 minutes (Natu et al., 2015;
Gandolfi et al., 2009). Besides, some of these cements may present high solubility (up
to 4.6% of weight loss for Biodentine after 28 days) and low values for hardness (26.9
VHN for ProRoot MTA) (Kaup et al., 2015). Moreover, the materials are prone to
lose compressive strength upon contamination with the moisture of blood and modest
pushout bond strength (Sheykhrezae et al., 2017; Dubey et al., 2017). The potential
for tooth discoloration associated with the use of biocements, especially MTA, is a
clear clinical disadvantage (Torabinejad et al., 2018). Recent investigations have
shown that bismuth oxide is the major culprit of this discoloration. Consequently,
manufacturers have developed alternative bioactive cement in a similar composition
that should not cause tooth discoloration. In this context NeoMTA Plus contains tantalum oxide as radiopacifier instead of bismuth oxide, avoiding the discoloration
(Tomas-Catala et al., 2017, 2018). Another limitation of bioactive endodontic cements
is the difficulty of removing the material from the root canals during retreatment.
Although some new bioactive endodontic sealers such as MTA Fillapex,
EndoSequence BC sealer, MTA Plus, and iRoot SP can be more easily removed
(Torabinejad et al., 2018), the presence of residual filling material after retreatment
remains as a concern (Oltra et al., 2017). Thus the development of materials and strategies that can improve these aspects without compromising the bioactivity of cements
is of high interest.
In recent years several approaches have been developed to improve the properties of bioactive cements. Some of them focus on the modification of the liquids
that are used to mix the powder particles. For instance, the addition of propylene
glycol has been shown to increase the flowability and improve the handling of the
materials, but it increases setting time and decreases hardness (Natu et al., 2015).
Liquid extract of Casearia sylvestris increased the antimicrobial properties of MTA
but interfered in some of its physicochemical properties (Natu et al., 2015;
Cavenago et al., 2017). Also, thickening agents instead of water in
injectable calcium silicate endodontic sealers are commonly used to create gel-like
pastes that improve their handling (Ha et al., 2017). In the same line new
602
Advanced Dental Biomaterials
MTA-based with high-plasticity materials have been introduced. The new strategy
relies on the replacement of the distilled water by a liquid containing water Check
and an organic plasticizer that provides higher plasticity, improving handling and
placement of the material to the repair site (Cintra et al., 2017).
Other strategies focus on the modification of the powders by the addition of fractions of new components to it. For instance, the addition of wollastonite (CaSiO3), a
raw calcium metasilicate composed of calcium oxide and silicon dioxide, shortened
the setting time but decreased the compressive strength of a MTA cement
(Flores-Ledesma et al., 2017). The presence of MgO or ZnO improved the biological
properties (e.g., cell viability) of glass ionomer cements but failed to increase compressive strength (Kim et al., 2015). The addition of zirconia to hydroxyapatite increased
the fracture toughness and flexural strength by almost three times higher compared to
the unmodified materials (Kong et al., 2010). The insertion of niobium (Nb2O5) oxide
in bioactive cements can also increase the mineralization (Gomes-Cornelio et al.,
2017). Also, the incorporation of prereacted glass ionomer fillers in root repair cements
demonstrated significant antibacterial effects against endodontic pathogens, multiple
ion-releasing abilities, and significantly shorter initial and final setting times in comparison to MTA (Yassen et al., 2016). Regardless of the achievements, there are several
opportunities to further improve the properties of bioactive cements.
Recently, nanomaterials have been explored to improve several physical and
mechanical properties of industrial and biological cements. For instance, the addition of multiwalled carbon nanotubes (CNTs) can improve both the compressive
strength and modulus of rupture of cements (Musso et al., 2009). The addition of
0.02 wt.% of CNTs to cement mortar increased its compressive strength by 11%
(Mohsen et al., 2017). Improvements in these properties were observed when CNT
and carbon nanofibers increased the compressive strengths of ordinary Portland
cement mortar by 154% and 217% compared to the unmodified material (Yazdani
and Mohanam, 2016). The addition of 0.25 wt.% CNTs to Portland cement
increased in 55% the flexural strength of the set material (from 10.4 to 16.2 MPa)
(Mohsen et al., 2017). The addition of multiwalled CNTs (0.25%) to type I
Portland cement resulted in a composite with compressive and tensile strength higher than the control (20% and 40%, respectively) (Jang et al., 2016). Similar
improvements can be observed with the addition of single-walled CNTs which
increased the hardness by the hydration of cements at an early age (Makar et al.,
2005). In terms of setting reaction different alternatives have been shown to effectively speed up the setting reaction while decreasing the setting time. For instance,
nano-SiO2 added to Portland cement (42.5 grade) induces the early precipitation of
calcium silicate hydrate shortening the induction period. Notably, the initial setting
time decreased significantly with the presence of 5 wt.% of nano-SiO2 in the mix
(Qing et al., 2007).
All these enhancements observed in the past with different nanomaterials have
led researchers to explore graphene family materials to improve the physical,
mechanical, and biological properties of cements. The literature is vast on the
enhancements provided by GO to improve the properties of cementitious materials.
For instance, the presence of 0.03 wt.% of GO increased the tensile and compressive
Graphene to improve the physicomechanical properties and bioactivity of the cements
603
strength of Portland cement by 53% and 46%, respectively (Gong et al., 2015).
Similar enhancements have been observed with the addition of 0.05 wt.% GO to
cement that increased the flexural strength by 59% and the compressive strength by
33% (Pan et al., 2012). In fact very small quantities of GO (e.g., 0.01 wt.%) can significantly increase both the compressive and flexural strengths of Portland cements by
23% and 57%. Nevertheless, the values are even higher when the concentration rises
to 0.06 wt.% resulting in increases of 72% in the compressive strength and 63% in the
flexural strength after 7 days (Lv et al., 2014).
The improvements provided by GO-based materials are not limited to Portland
cements. Bioceramics, such as hydroxyapatite, β-tricalcium phosphate, and others,
also experience improvements in their properties when modified with the different
forms of graphene.
One of the most explored bioactive materials for bone regeneration is hydroxyapatite. It has high osteoconductivity potential and tissue compatibility (Jang et al.,
2014; LeGeros, 2002). The commercially available versions of hydroxyapatite can
induce bone repair in clinical settings and increase bone to implant contact (Ogose
et al., 2006; Jang et al., 2014; Tonetto et al., 2015b). Nonetheless, this material can
be very brittle, difficult to shape, and present slow resorption rates (Porter et al.,
2009). Notably, several studies have shown that graphene family materials can
overcome some of these disadvantages.
One of the potential uses of graphene is to improve the physical properties of
hydroxyapatite-based materials. The presence of 2 and 5 wt.% of GO in a hydroxyapatite coating can increase the adhesion of the coating to titanium from 1.5 to 2.7
and 3.3 MPa, respectively. Notably, the GO-modified hydroxyapatite also presented
higher corrosion resistance compared to the unmodified version of the material (Liu
et al., 2014a). Increased corrosion resistance has also been observed in ternary
GO chitosan hydroxyapatite (GO CS HA) coating. The corrosion current
density of titanium decreased from 6823 to 248 nA/cm2 after being coated with
chitosan hydroxyapatite and to 13.5 nA/cm2 when protected by GO CS HA
(Shi et al., 2016).
It is also possible to improve the mechanical properties of several bioactive cements.
For instance, GO nanoflakes (0.5%) added a scaffold of hydroxyapatite, and gelatin
increased both the compressive strength (from 37 to 52 MPa) and the yield strength
(from 12 to 47 MPa) (Nair et al., 2015). Also, the addition of 0.5 wt.% graphene to 58S
bioglass promoted a twofold increase in the compressive strength (from 23.6 to
48.7 MPa) and increased the fracture toughness from 1.4 to 1.9 MPa m1/2 (Gao et al.,
2014). The addition of 1 wt.% rGO to hydroxyapatite increases its fracture toughness by
more than 200% and elastic modulus by 47% (Yi et al., 2013). Similarly, enhancements
were observed by the addition of 1 wt.% of graphene nanosheets (GNS) to hydroxyapatite that nearly doubled the fracture toughness and increased hardness in almost 50%
(Zhang et al., 2013a). The addition of 3 wt.% of GNS to EndocemZr increased the hardness from 8 to 15 KHN (Fig. 22.1) (Dubey et al., 2017). Similarly, 1 wt.% rGO
increased the hardness of the hydroxyapatite from 322 to 425 HV (Baradaran et al.,
2014). Finally, the addition of 1.5 wt.% rGO increased both the elastic modulus and
fracture toughness of hydroxyapatite by 40% and 86%, respectively (Zanin et al., 2013).
604
Advanced Dental Biomaterials
Figure 22.1 The addition of given concentrations GNS to BIO and ECZ (top panels) can
decrease the setting time (A) and increase the hardness of the materials (B). Nonetheless, the
GNS negatively affects the pushout bond strength of ECZ to dentine (C). BIO, Biodentine;
ECZ, EndocemZR; GNS, graphene nanosheets.
Source: Adapted from Dubey, N., Rajan, S.S., Bello, Y.D., Min, K.-S., Rosa, V., 2017.
Graphene nanosheets to improve physico-mechanical properties of bioactive calcium silicate
cements. Materials, 10, 606.
These enhancements in mechanical properties are likely to be a result of the crack
deflection, bridging, and sheet pullout through promoted by the different forms of graphene inside the cementitious matrix that delays or prevents the crack propagation
(Baradaran et al., 2014; Li et al., 2016). For instance, the pullout energy of graphene
from hydroxyapatite varies from 3 to 40 J/m, which is higher than the fracture energy
of bulk hydroxyapatite (1 J/m). This forces the cracks to propagate within the hydroxyapatite matrix and not along the graphene/hydroxyapatite interface. In addition, graphene induces the formation of smaller hydroxyapatite crystals that could potentially
result in a fine-grain strengthening mechanism (Liu et al., 2013b).
The changes in properties of the bioactive cements by the addition of graphene
family materials are dependent on the concentration of the materials that are added
to the cements. The addition of 0.5 wt.% of GO into 45S5 Bioglass increases the
fracture toughness from B0.5 to 0.8 while the addition of 1 wt.% increases it further to 1.2 MPa m1/2 (Li et al., 2016). It deserves to be noted that the enhancements
in mechanical properties are dose-dependent, and the increase of concentrations of
graphene above a certain threshold does not translate into further enhancements in
the set materials (Lv et al., 2013, 2014). It has been shown that the mechanical
properties of ordinary Portland cement type 42.5R decrease when GO is added to a
concentration higher than 0.03 wt.% (Fig. 22.2). Whereas 0.03% increases the tensile strength from 2.47 to 2.93 MPa, the addition of 0.06% GO nanosheets
Figure 22.2 The addition of GO nanosheets increases the mechanical properties of Portland
cement in a dose-dependent manner: increases above 0.03% result in decreased tensile and
flexural strength. GO, Graphene oxide.
Source: Lv S.,Ting S., Liu J., and ZhouQ., Use of graphene oxide nanosheets to regulate the
microstructure of hardened cement paste to increase its strength and toughness, Cryst Eng
Comm 16, 2014, 8508.
606
Advanced Dental Biomaterials
decreases it to 2.4 MPa. Similar behavior has been observed for the flexural
strength that increases from 8.5 to 9.6 MPa for 0.03% and decreases to 7.2 with
0.06% (Lv et al., 2013). Similarly, GNS in high concentrations (5 and 7 wt.%)
decreased the hardness of both Biodentine and EndocemZr compared to concentrations equal to or lower than 3 wt.% (Dubey et al., 2017). Moreover, carbon-based
materials influence the formation of hydration products by accelerating the rate of
hydration processes, particularly at the early stages (Manzur and Yazdani, 2014; Lv
et al., 2014). Hence, the addition of these materials to cement can impact positively
or negatively on the time taken to set the cements. It has been observed that GNS
(1 and 3 wt.%) can decrease the setting time of both Biodentine and EndocemZr.
Interestingly, the addition of 5 and 7 wt.% of nanosheets results in setting times
that are similar to the unmodified cements (Dubey et al., 2017). This may be related
to the plausible agglomeration of the carbonaceous materials around the cement
grains that results in partial hydration (Siddique and Mehta, 2014).
Besides the improvements in physicomechanical properties, it is also desirable to
improve the bioactivity of cements. This is important since it can speed up the formation of bone and enhance the amount of the tissue formed. These two aspects can
enhance the development of alternative bone substitutes to overcome the main limitations related to autologous and allogenous grafts (e.g., high cost, batch-to-batch variability, and limited availability). In this regard several studies have shown that
graphene and its derivatives can improve the bioactivity of several bioactive cements.
Graphene and its derivatives have been shown to enhance the osteogenic differentiation of cells. Substrates and scaffolds made of pure graphene produced by
CVD have been shown to promote the spontaneous osteogenic differentiation of
several types of cells (e.g., bone marrow stem cells, periodontal ligament stem cells,
and dental pulp stem cells). The material, in both 2D and 3D arrangements,
increased the expression of RUNX2, collagen I, osteopontin, and osteocalcin at
both genetic and protein level (Fig. 22.3). These are key markers involved in the
early and final stages of the osteoblastic differentiation (Xie et al., 2015a, 2017).
Recently, a substrate made of GO has been shown to increase the expression of several genes commonly expressed by cells that secrete mineralized matrix such as
DSPP, DMP-1, RUNX2, and collagen I (Fig. 22.4) (Rosa et al., 2016). Notably, the
differentiation was further magnified in the presence of osteogenic induction media
in the presence of graphene compared to when the chemical inductors are used
alone (Nayak et al., 2011; Lee et al., 2011; Dubey et al., 2015). For these reasons,
graphene has been extensively investigated to increase the biological properties of
cementitious materials.
Graphene and its derivatives have been combined with scaffolds to increase their
potential for osteogenesis. Collagen sponge-form scaffolds modified with GO can
adsorb considerable amounts of albumin and lysozyme and induce the formation of
bone in vivo. When the GO-modified scaffolds were implanted into bone sockets,
they promoted the formation of new bone while the control scaffold presented
lesser bone formation and was mostly filled with connective tissue (Nishida et al.,
2016). These notable effects were further explored to improve scaffolds and
particles made of biocements. For example, the combination of GO to a
Graphene to improve the physicomechanical properties and bioactivity of the cements
607
Figure 22.3 CVD-grown graphene induces the osteoblastic differentiation of stem cells.
Cells on graphene films (2DGp) or scaffolds (3DGp) presented high expression of
osteocalcin (in green). Glass substrate (Gl) was used as a control for 2DGp (Xie et al.,
2015b). CVD, Chemical vapor deposition.
gelatin/hydroxyapatite scaffold has increased the alkaline phosphatase activity and
the protein expression of osteopontin compared to the unmodified scaffold (Nair
et al., 2015). Bone marrow mesenchymal stem cells (MSCs) cultured in
β-tricalcium phosphate scaffolds combined with GO flakes presented increased
alkaline phosphatase activity and higher expression of genes related to osteogenic
differentiation, probably via the activation of the canonical Wnt signalling pathway
(Wu et al., 2015). Scaffolds made of GO/calcium phosphate nanocomposites
induced higher levels of calcification, alkaline phosphatase activity, and increased
the protein expression of osteocalcin compared to cells treated with GO or calcium
phosphate alone (Tatavarty et al., 2014).
Graphene can also be combined with bioceramics and cements to increase the
bioactivity of these materials. For instance, colloidal dispersion of rGO-coated
hydroxyapatite increased the protein expression of osteopontin and osteocalcin calcium
nodule deposition and alkaline phosphatase activity of MSCs compared to rGO or
hydroxyapatite alone (Lee et al., 2015a). The addition of GNS to EndocemZr
and Biodentine increased the mineralization potential of dental pulp stem cells
608
Advanced Dental Biomaterials
Figure 22.4 (A and B) Dental pulp stem cells can efficiently adhere and proliferate on
GO-based substrate. (C) The material also increased the expression of several genes
commonly expressed by mineral-secreting cells.
Source: Adapted from Rosa, V., Xie, H., Dubey, N., Madanagopal, T.T., Rajan, S.S., Morin,
J.L.P., et al., 2016. Graphene oxide-based substrate: physical and surface characterization,
cytocompatibility and differentiation potential of dental pulp stem cells. Dent. Mater. 32,
1019 1025.
(Dubey et al., 2017). GO-modified β-tricalcium phosphate scaffold induced higher
bone formation in critical-sized calvarial defects created in rabbits compared to the
defects filled with the unmodified scaffold. The bone volume/total volume ratios were
44% for the GO-modified scaffold and 30% for β-tricalcium phosphate scaffold used
as control (Wu et al., 2015). Similarly, rGO/hydroxyapatite grafts increased the bone
density from 26% (hydroxyapatite alone) to 52%. The increment was even higher
when compared to the value obtained for the untreated control (17.7%) after 4 weeks
(Lee et al., 2015b). Hydroxyapatite/GNS composites increased the proliferation of
osteoblast cells when used as a coating on titanium substrates. Interestingly, the random
incorporation of curly graphene sheets allowed for higher protein absorption
(fibronectin) and provided active sites for cell binding (Liu et al., 2014b).
Graphene to improve the physicomechanical properties and bioactivity of the cements
609
The enhancements on the bioactivity of materials modified with graphene have
different origins. For hydroxyapatite, it has been observed that the presence of GNS
induced the formation of uniform apatite layers that are thicker than hydroxyapatite
alone. The GNS change the spatial distribution of the crystals that grow closely or
even inside the porous hydroxyapatite, while in the GNS/hydroxyapatite composites, they grow preferentially on the surface of material (Zhang et al., 2013a).
Furthermore, GO increases the nucleation and crystallization of hydroxyapatite.
This process results in GO/hydroxyapatite composites with dense hydroxyapatite
crystals (Gao et al., 2015). Notably, the presence of graphene nanofillers can
increase the formation of thick apatite surface of hydroxyapatite under simulated
body fluid (Zhang et al., 2013a). The changes in the compositions and characteristics of hydroxyapatite lead to different outcomes that eventually can increase the
bioactivity of the composites. For instance, graphene/hydroxyapatite composites are
less stable than hydroxyapatite alone. This leads to the fast dissolution of calcium
ions from the composites (Janković et al., 2015). The lower crystallinity of
graphene-modified materials can also increase the dissolution and the release of
ions from the composites (Mohandes and Salavati-Niasari, 2014a). Similarly, composites made of hydroxyapatite/GO with chitosan or gelatin can release more calcium ions compared to pure hydroxyapatite particles (Mohandes and SalavatiNiasari, 2014a,b). These can have a biological impact since these ions can induce
and enhance the osteoblastic differentiation (Natu et al., 2015; Jung et al., 2010).
22.3
Conclusion
The different forms of graphene can be functionalized and combined with several biomolecules and biomaterials, increasing their potential to improve bioactive cements. In
this area, graphene has been used as a physical additive or to modify the overall chemical composition of cementitious materials. The resultant materials often present
improved physical and mechanical properties and can present certain characteristics that
allow for higher bioactivity. Despite these exciting achievements, it is still necessary to
evaluate the potential risks and long-term performance of the graphene-modified
cements. Nevertheless, the findings obtained so far attest to the potential of graphene to
improve the physical, chemical, mechanical, and biological properties of cements.
References
Baradaran, S., Moghaddam, E., Basirun, W.J., Mehrali, M., Sookhakian, M., Hamdi, M.,
et al., 2014. Mechanical properties and biomedical applications of a nanotube
hydroxyapatite-reduced graphene oxide composite. Carbon N.Y. 69, 32 45.
Bunch, J.S., Verbridge, S.S., Alden, J.S., Van Der Zande, A.M., Parpia, J.M., Craighead, H.
G., et al., 2008. Impermeable atomic membranes from graphene sheets. Nano Lett. 8,
2458 2462.
Caron, G., Azerad, J., Faure, M.O., Machtou, P., Boucher, Y., 2014. Use of a new retrograde
filling material (Biodentine) for endodontic surgery: two case reports. Int. J. Oral Sci. 6,
250 253.
610
Advanced Dental Biomaterials
Castro Neto, A.H., Guinea, F., Peres, N.M.R., Novoselov, K.S., Geim, A.K., 2009. The electronic properties of graphene. Rev. Mod. Phys. 81, 109 162.
Cavenago, B.C., Del Carpio-Perochena, A.E., Ordinola-Zapata, R., Estrela, C., Garlet, G.P.,
Tanomaru-Filho, M., et al., 2017. Effect of using different vehicles on the physicochemical, antimicrobial, and biological properties of white mineral trioxide aggregate. J.
Endod. 43, 779 786.
Cintra, L.T.A., Benetti, F., De Azevedo Queiroz, I.O., De Araujo Lopes, J.M., Penha De oliveira, S.H., Sivieri Araujo, G., et al., 2017. Cytotoxicity, biocompatibility, and biomineralization of the new high-plasticity MTA material. J. Endod. 43, 774 778.
Dreyer, D.R., Park, S., Bielawski, C.W., Ruoff, R.S., 2010. The chemistry of graphene oxide.
Chem. Soc. Rev. 39, 228 240.
Dubey, N., Bentini, R., Islam, I., Cao, T., Castro Neto, A.H., Rosa, V., 2015. Graphene: a
versatile carbon-based material for bone tissue engineering. Stem Cells Int. 2015, 1 12.
Dubey, N., Rajan, S.S., Bello, Y.D., Min, K.-S., Rosa, V., 2017. Graphene nanosheets to improve
physico-mechanical properties of bioactive calcium silicate cements. Materials 10, 606.
Faugeras, C., Nerrière, A., Potemski, M., Mahmood, A., Dujardin, E., Berger, C., et al.,
2008. Few-layer graphene on SiC, pyrolitic graphite, and graphene: a Raman scattering
study. Appl. Phys. Lett. 92, 011914.
Flores-Ledesma, A., Barcelo Santana, F., Bucio, L., Arenas-Alatorre, J.A., Faraji, M.,
Wintergerst, A.M., 2017. Bioactive materials improve some physical properties of a
MTA-like cement. Mater. Sci. Eng. C Mater. Biol. Appl. 71, 150 155.
Gandolfi, M.G., Iacono, F., Agee, K., Siboni, F., Tay, F., Pashley, D.H., et al., 2009. Setting
time and expansion in different soaking media of experimental accelerated calciumsilicate cements and ProRoot MTA. Oral Surg. Oral. Med. Oral Pathol. Oral Radiol.
Endod. 108, e39 e45.
Gandolfi, M.G., Siboni, F., Botero, T., Bossù, M., Riccitiello, F., Prati, C., 2015. Calcium silicate
and calcium hydroxide materials for pulp capping: biointeractivity, porosity, solubility and
bioactivity of current formulations. J. Appl. Biomater. Funct. Mater. 13, 43 60.
Gao, C., Liu, T., Shuai, C., Peng, S., 2014. Enhancement mechanisms of graphene in nano58S bioactive glass scaffold: mechanical and biological performance. Sci. Rep. 4, 4712.
Gao, F., Xu, C., Hu, H., Wang, Q., Gao, Y., Chen, H., et al., 2015. Biomimetic synthesis and
characterization of hydroxyapatite/graphene oxide hybrid coating on Mg alloy with
enhanced corrosion resistance. Mater. Lett. 138, 25 28.
Geim, A.K., Novoselov, K.S., 2007. The rise of graphene. Nat. Mater. 6, 183 191.
Goenka, S., Sant, V., Sant, S., 2014. Graphene-based nanomaterials for drug delivery and tissue engineering. J. Control. Release 173, 75 88.
Gomes-Cornelio, A.L., Rodrigues, E.M., Salles, L.P., Mestieri, L.B., Faria, G., GuerreiroTanomaru, J.M., et al., 2017. Bioactivity of MTA Plus, Biodentine and an experimental
calcium silicate-based cement on human osteoblast-like cells. Int. Endod. J. 50, 39 47.
Gong, K., Pan, Z., Korayem, A.H., Qiu, L., Li, D., Collins, F., et al., 2015. Reinforcing
effects of graphene oxide on Portland cement paste. J. Mater. Civil Eng. 27, A4014010.
Ha, W.N., Nicholson, T., Kahler, B., Walsh, L.J., 2017. Mineral trioxide aggregate—a review
of properties and testing methodologies. Materials (Basel) 10.
Hakki, S.S., Bozkurt, S.B., Hakki, E.E., Belli, S., 2009. Effects of mineral trioxide aggregate
on cell survival, gene expression associated with mineralized tissues, and biomineralization of cementoblasts. J. Endod. 35, 513 519.
Jang, C.H., Cho, Y.B., Choi, C.H., Jang, Y.S., Jung, W.K., Lee, J.K., 2014. Comparison of
osteoconductivity of biologic and artificial synthetic hydroxyapatite in experimental
mastoid obliteration. Acta Otolaryngol. 134, 255 259.
Graphene to improve the physicomechanical properties and bioactivity of the cements
611
Jang, S.H., Kawashima, S., Yin, H., 2016. Influence of carbon nanotube clustering on
mechanical and electrical properties of cement pastes. Materials (Basel) 9, 220.
Janković, A., Eraković, S., Mitrić, M., Matić, I.Z., Juranić, Z.D., Tsui, G.C.P., et al., 2015.
Bioactive hydroxyapatite/graphene composite coating and its corrosion stability in simulated body fluid. J. Alloys Compd. 624, 148 157.
Jung, G.Y., Park, Y.J., Han, J.S., 2010. Effects of HA released calcium ion on osteoblast
differentiation. J. Mater. Sci. Mater. Med. 21, 1649 1654.
Kaup, M., Schäfer, E., Dammaschke, T., 2015. An in vitro study of different material properties of Biodentine compared to ProRoot MTA. Head. Face. Med. 11.
Khare, R., Mielke, S.L., Paci, J.T., Zhang, S., Ballarini, R., Schatz, G.C., et al., 2007.
Coupled quantum mechanical/molecular mechanical modeling of the fracture of defective carbon nanotubes and graphene sheets. Phys. Rev. B 75, 075412.
Kim, D.A., Abo-Mosallam, H., Lee, H.Y., Lee, J.H., Kim, H.W., Lee, H.H., 2015. Biological
and mechanical properties of an experimental glass-ionomer cement modified by partial
replacement of CaO with MgO or ZnO. J. Appl. Oral Sci. 23, 369 375.
Kong, Y.-M., Kim, S., Kim, H.-E., Lee, I.-S., 2010. ChemInform abstract: reinforcement of
hydroxyapatite bioceramic by addition of ZrO2 coated with Al2O3. ChemInform 31.
Lee, W.C., Lim, C.H.Y.X., Shi, H., Tang, L.A.L., Wang, Y., Lim, C.T., et al., 2011. Origin
of enhanced stem cell growth and differentiation on graphene and graphene oxide. ACS
Nano 5, 7334 7341.
Lee, J.H., Shin, Y.C., Jin, O.S., Kang, S.H., Hwang, Y.S., Park, J.C., et al., 2015a. Reduced
graphene oxide-coated hydroxyapatite composites stimulate spontaneous osteogenic
differentiation of human mesenchymal stem cells. Nanoscale 7, 11642 11651.
Lee, J.H., Shin, Y.C., Lee, S.M., Jin, O.S., Kang, S.H., Hong, S.W., et al., 2015b. Enhanced osteogenesis by reduced graphene oxide/hydroxyapatite nanocomposites. Sci. Rep. 5, 18833.
Legeros, R.Z., 2002. Properties of osteoconductive biomaterials: calcium phosphates. Clin.
Orthop. Relat. Res. 395, 81 98.
Li, X., Cai, W., An, J., Kim, S., Nah, J., Yang, D., et al., 2009a. Large-area synthesis of
high-quality and uniform graphene films on copper foils. Science 324, 1312 1314.
Li, X., Cai, W., Colombo, L., Ruoff, R.S., 2009b. Evolution of graphene growth on Ni and
Cu by carbon isotope labeling. Nano. Lett. 9, 4268 4272.
Li, Z., Khun, N.W., Tang, X.Z., Liu, E.J., Khor, K.A., 2016. Mechanical, tribological and
biological properties of novel 45S5 Bioglasss composites reinforced with in situ
reduced graphene oxide. J. Mech. Behav. Biomed. Mater. 65, 77 89.
Liu, J., Cui, L., Losic, D., 2013a. Graphene and graphene oxide as new nanocarriers for drug
delivery applications. Acta Biomater. 9, 9243 9257.
Liu, Y., Huang, J., Li, H., 2013b. Synthesis of hydroxyapatite reduced graphite oxide nanocomposites for biomedical applications: oriented nucleation and epitaxial growth of
hydroxyapatite. J. Mater. Chem. B 1, 1826.
Liu, H., Cheng, J., Chen, F., Hou, F., Bai, D., Xi, P., et al., 2014a. Biomimetic and cellmediated mineralization of hydroxyapatite by carrageenan functionalized graphene
oxide. ACS Appl. Mater. Interfaces 6, 3132 3140.
Liu, Y., Dang, Z., Wang, Y., Huang, J., Li, H., 2014b. Hydroxyapatite/graphene-nanosheet
composite coatings deposited by vacuum cold spraying for biomedical applications:
inherited nanostructures and enhanced properties. Carbon N.Y. 67, 250 259.
Lopez, G., Mittemeijer, E., 2004. The solubility of C in solid Cu. Scr. Mater. 51, 1 5.
Lotya, M., Hernandez, Y., King, P.J., Smith, R.J., Nicolosi, V., Karlsson, L.S., et al., 2009.
Liquid phase production of graphene by exfoliation of graphite in surfactant/water solutions. J. Am. Chem. Soc. 131, 3611 3620.
612
Advanced Dental Biomaterials
Lv, S., Ma, Y., Qiu, C., Sun, T., Liu, J., Zhou, Q., 2013. Effect of graphene oxide nanosheets
of microstructure and mechanical properties of cement composites. Construct. Build.
Mater. 49, 121 127.
Lv, S., Ting, S., Liu, J., Zhou, Q., 2014. Use of graphene oxide nanosheets to regulate the
microstructure of hardened cement paste to increase its strength and toughness.
CrystEngComm 16, 8508.
Maeda, H., Nakano, T., Tomokiyo, A., Fujii, S., Wada, N., Monnouchi, S., et al., 2010.
Mineral trioxide aggregate induces bone morphogenetic protein-2 expression and calcification in human periodontal ligament cells. J. Endod. 36, 647 652.
Main, C., Mirzayan, N., Shabahang, S., Torabinejad, M., 2004. Repair of root perforations
using mineral trioxide aggregate: a long-term study. J. Endod. 30, 80 83.
Makar, J., Margeson, J., Luh, J., 2005. Carbon nanotube/cement composites—early results
and potential application. In: Proceedings of the Third International Conference on
Construction Materials: Performance, Innovations and Structural Implications. August
22 24. Vancouver, B.C., pp. 1 10.
Manzur, T., Yazdani, N., 2014. Optimum mix ratio for carbon nanotubes in cement mortar.
KSCE J. Civil Eng. 19, 1405 1412.
Min, K.S., Yang, S.H., Kim, E.C., 2009. The combined effect of mineral trioxide aggregate
and enamel matrix derivative on odontoblastic differentiation in human dental pulp
cells. J. Endod. 35, 847 851.
Mohandes, F., Salavati-Niasari, M., 2014a. Freeze-drying synthesis, characterization and
in vitro bioactivity of chitosan/graphene oxide/hydroxyapatite nanocomposite. RSC
Adv. 4, 25993 26001.
Mohandes, F., Salavati-Niasari, M., 2014b. In vitro comparative study of pure hydroxyapatite
nanorods and novel polyethylene glycol/graphene oxide/hydroxyapatite nanocomposite.
J. Nanoparticle Res. 16, 1 12.
Mohsen, M.O., Taha, R., Abu Taqa, A., Shaat, A., 2017. Optimum carbon nanotubes’ content
for improving flexural and compressive strength of cement paste. Construct. Build.
Mater. 150, 395 403.
Morin, J.L.P., Dubey, N., Decroix, F.E.D., Luong-Van, E.K., Castro Neto, A.H., Rosa, V.,
2017. Graphene transfer to 3-dimensional surfaces: a vacuum-assisted dry transfer
method. 2D Mater. 4, 025060.
Musso, S., Tulliani, J.-M., Ferro, G., Tagliaferro, A., 2009. Influence of carbon nanotubes structure
on the mechanical behavior of cement composites. Compos. Sci. Technol. 69, 1985 1990.
Nair, R., Blake, P., Grigorenko, A., Novoselov, K., Booth, T., Stauber, T., et al., 2008. Fine
structure constant defines visual transparency of graphene. Science 320, 1308.
Nair, M., Nancy, D., Krishnan, A.G., Anjusree, G.S., Vadukumpully, S., Nair, S.V., 2015.
Graphene oxide nanoflakes incorporated gelatin-hydroxyapatite scaffolds enhance osteogenic differentiation of human mesenchymal stem cells. Nanotechnology 26, 161001.
Natu, V.P., Dubey, N., Loke, G.C., Tan, T.S., Ng, W.H., Yong, C.W., et al., 2015.
Bioactivity, physical and chemical properties of MTA mixed with propylene glycol. J.
Appl. Oral Sci. 23, 405 411.
Nayak, T.R., Andersen, H., Makam, V.S., Khaw, C., Bae, S., Xu, X., et al., 2011. Graphene
for controlled and accelerated osteogenic differentiation of human mesenchymal stem
cells. ACS Nano 5, 4670 4678.
Nishida, E., Miyaji, H., Kato, A., Takita, H., Iwanaga, T., Momose, T., et al., 2016.
Graphene oxide scaffold accelerates cellular proliferative response and alveolar bone
healing of tooth extraction socket. Int. J. Nanomed. 11, 2265 2277.
Graphene to improve the physicomechanical properties and bioactivity of the cements
613
Ogose, A., Kondo, N., Umezu, H., Hotta, T., Kawashima, H., Tokunaga, K., et al., 2006.
Histological assessment in grafts of highly purified beta-tricalcium phosphate
(OSferion) in human bones. Biomaterials 27, 1542 1549.
Oltra, E., Cox, T.C., Lacourse, M.R., Johnson, J.D., Paranjpe, A., 2017. Retreatability of two
endodontic sealers, EndoSequence BC Sealer and AH Plus: a micro-computed tomographic comparison. Restor. Dent. Endod. 42, 19 26.
Pan, Z., Duan, W., Li, D., Collins, F., 2012. Graphene Oxide Reinforced Cement and
Concrete Patent App. PCT/AU2012/001,582.
Parirokh, M., Torabinejad, M., 2010a. Mineral trioxide aggregate: a comprehensive literature
review—Part I: Chemical, physical, and antibacterial properties. J. Endod. 36, 16 27.
Parirokh, M., Torabinejad, M., 2010b. Mineral trioxide aggregate: a comprehensive literature
review—Part III: Clinical applications, drawbacks, and mechanism of action. J. Endod.
36, 400 413.
Parirokh, M., Torabinejad, M., Dummer, P.M.H., 2018. Mineral trioxide aggregate and other
bioactive endodontic cements: an updated overview—Part I: Vital pulp therapy. Int.
Endod. J. 51, 177 205.
Perera, S.D., Mariano, R.G., Vu, K., Nour, N., Seitz, O., Chabal, Y., et al., 2012.
Hydrothermal synthesis of graphene-TiO2 nanotube composites with enhanced photocatalytic activity. ACS Catal. 2, 949 956.
Porter, J.R., Ruckh, T.T., Popat, K.C., 2009. Bone tissue engineering: a review in bone biomimetics and drug delivery strategies. Biotechnol. Prog. 25, 1539 1560.
Prati, C., Gandolfi, M.G., 2015. Calcium silicate bioactive cements: biological perspectives
and clinical applications. Dent. Mater. 31, 351 370.
Qing, Y., Zenan, Z., Deyu, K., Rongshen, C., 2007. Influence of nano-SiO2 addition on properties of
hardened cement paste as compared with silica fume. Construct. Build. Mater. 21, 539 545.
Rosa, V., Xie, H., Dubey, N., Madanagopal, T.T., Rajan, S.S., Morin, J.L.P., et al., 2016.
Graphene oxide-based substrate: physical and surface characterization, cytocompatibility
and differentiation potential of dental pulp stem cells. Dent. Mater. 32, 1019 1025.
Sheykhrezae, M.S., Meraji, N., Ghanbari, F., Nekoofar, M.H., Bolhari, B., Dummer, P.M.H.,
2017. Effect of blood contamination on the compressive strength of three calcium
silicate-based cements. Aust. Endod. J. 44, 255 259.
Shi, Y.Y., Li, M., Liu, Q., Jia, Z.J., Xu, X.C., Cheng, Y., et al., 2016. Electrophoretic deposition of graphene oxide reinforced chitosan-hydroxyapatite nanocomposite coatings on Ti
substrate. J. Mater. Sci. Mater. Med. 27, 48.
Siddique, R., Mehta, A., 2014. Effect of carbon nanotubes on properties of cement mortars.
Construct. Build. Mater. 50, 116 129.
Stankovich, S., Dikin, D.A., Piner, R.D., Kohlhaas, K.A., Kleinhammes, A., Jia, Y., et al.,
2007. Synthesis of graphene-based nanosheets via chemical reduction of exfoliated
graphite oxide. Carbon N. Y. 45, 1558 1565.
Tatavarty, R., Ding, H., Lu, G., Taylor, R.J., Bi, X., 2014. Synergistic acceleration in the
osteogenesis of human mesenchymal stem cells by graphene oxide-calcium phosphate
nanocomposites. Chem Commun (Camb) 50, 8484 8487.
Tomas-Catala, C.J., Collado-Gonzalez, M., Garcia-Bernal, D., Onate-Sanchez, R.E., Forner,
L., Llena, C., et al., 2017. Comparative analysis of the biological effects of the endodontic bioactive cements MTA-Angelus, MTA Repair HP and NeoMTA Plus on human
dental pulp stem cells. Int. Endod. J. 50 (Suppl. 2), e63 e72.
Tomas-Catala, C.J., Collado-Gonzalez, M., Garcia-Bernal, D., Onate-Sanchez, R.E., Forner,
L., Llena, C., et al., 2018. Biocompatibility of new pulp-capping materials NeoMTA
614
Advanced Dental Biomaterials
plus, MTA repair HP, and biodentine on human dental pulp stem cells. J. Endod. 44,
126 132.
Tonetto, A., Lago, P.W., Borba, M., Rosa, V., 2015a. Effects of chrondro-osseous regenerative compound associated with local treatments in the regeneration of bone defects
around implants: an in vivo study. Clin. Oral. Investig. 20, 1 8.
Tonetto, A., Lago, P.W., Borba, M., Rosa, V., 2015b. Effects of chrondro-osseous regenerative compound associated with local treatments in the regeneration of bone defects
around implants: an in vivo study. Clin. Oral. Investig. 20, 267 274.
Torabinejad, M., Parirokh, M., Dummer, P.M.H., 2018. Mineral trioxide aggregate and other
bioactive endodontic cements: an updated overview—Part II: Other clinical applications
and complications. Int. Endod. J. 51, 284 317.
Wu, C., Xia, L., Han, P., Xu, M., Fang, B., Wang, J., et al., 2015. Graphene-oxide-modified
β-tricalcium phosphate bioceramics stimulate in vitro and in vivo osteogenesis. Carbon
N. Y. 93, 116 129.
Xie, H., Cao, T., Gomes, J.V., Castro Neto, A.H., Rosa, V., 2015a. Two and threedimensional graphene substrates to magnify osteogenic differentiation of periodontal
ligament stem cells. Carbon N.Y. 93, 266 275.
Xie, H., Cao, T., Gomes, J.V., Neto, A.H.C., Rosa, V., 2015b. Two and three-dimensional
graphene substrates to magnify osteogenic differentiation of periodontal ligament stem
cells. Carbon N.Y. 93, 266 275.
Xie, H., Chua, M., Islam, I., Bentini, R., Cao, T., Viana-Gomes, J.C., et al., 2017. CVDgrown monolayer graphene induces osteogenic but not odontoblastic differentiation of
dental pulp stem cells. Dent. Mater. 33, e13 e21.
Yassen, G.H., Huang, R., Al-Zain, A., Yoshida, T., Gregory, R.L., Platt, J.A., 2016.
Evaluation of selected properties of a new root repair cement containing surface prereacted glass ionomer fillers. Clin. Oral. Investig. 20, 2139 2148.
Yazdani, N., Mohanam, V., 2016. Strength, bleeding and setting time of cement mortar with
carbon nanotubes and nanofibers. Adv. Sci. Eng. Med. 8, 490 495.
Yi, L., Jing, H., Hua, L., 2013. Synthesis of hydroxyapatite reduced graphite oxide
nanocomposites for biomedical applications: oriented nucleation and epitaxial growth of
hydroxyapatite. J. Mater. Chem. B 1, 1826 1834.
Zanin, H., Saito, E., Marciano, F.R., Ceragioli, H.J., Campos Granato, A.E., Porcionatto, M.,
et al., 2013. Fast preparation of nano-hydroxyapatite/superhydrophilic reduced graphene
oxide composites for bioactive applications. J. Mater. Chem. B 1, 4947.
Zhang, L., Liu, W., Yue, C., Zhang, T., Li, P., Xing, Z., et al., 2013a. A tough graphene
nanosheet/hydroxyapatite composite with improved in vitro biocompatibility. Carbon N.
Y. 61, 105 115.
Zhang, L., Zhang, F., Yang, X., Long, G., Wu, Y., Zhang, T., et al., 2013b. Porous 3D
graphene-based bulk materials with exceptional high surface area and excellent conductivity for supercapacitors. Sci. Rep. 3, 1378.
Zheng, Q.,, Kim, J.-K.,, 2015. Synthesis, Structure, and Properties of Graphene and
Graphene Oxide. Springer, New York, pp. 29 94.
Zhou, M., Wang, Y., Zhai, Y., Zhai, J., Ren, W., Wang, F., et al., 2009. Controlled synthesis
of large-area and patterned electrochemically reduced graphene oxide films. Chemistry
15, 6116 6120.
Biomaterials for maxillofacial
prosthetic rehabilitation
23
Waqas Tanveer
Maxillofacial Prosthetic Service, Department of Prosthodontics, Faculty of Dentistry,
Mahidol University, Bangkok, Thailand
Chapter Outline
23.1
23.2
23.3
23.4
Highlights 616
Historical background 616
Ideal properties of maxillofacial material 617
Search for ideal materials for maxillofacial rehabilitation 617
23.4.1
23.4.2
23.4.3
23.4.4
23.4.5
23.4.6
Acrylic resins (1940 60) 617
Polyvinylchloride and copolymer 619
Chlorinated polyethylene 619
Polyurethane elastomers (1970 90) 619
Thermoset urethane elastomers 619
Silicones (1960 70) 620
23.5 Silicones
620
23.5.1 Polymer structures 620
23.6 Classification of maxillofacial silicones
622
23.6.1 Classification of silicones according to application 622
23.7 Types of maxillofacial silicones
23.7.1
23.7.2
23.7.3
23.7.4
625
Most common room temperature vulcanizing silicones 625
Medical grade liquid silicone elastomers 627
Recommendations 627
Medical grade VerSiTal silicone elastomers 628
23.8 M-511 platinum silicone rubber
23.8.1 Silicone fluids 629
23.8.2 Properties 629
23.8.3 Types of silicone fluids
628
629
23.9 Primers 632
23.10 Soft liners and tissue conditioners
633
23.10.1 Soft liner 633
23.10.2 Coe-Comfort and Coe-Soft 633
23.10.3 Sculpturing clays and waxes 635
23.11 Coloring agents
23.11.1
23.11.2
23.11.3
23.11.4
635
Colored flocking 635
Intrinsic stains 636
Extrinsic colors 636
Acetoxy silastic adhesives 636
23.12 Skin adhesives
References 639
638
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00024-4
Copyright © 2019 Elsevier Ltd. All rights reserved.
616
23.1
G
G
G
G
G
G
G
G
G
Advanced Dental Biomaterials
Highlights
Introduction
History of maxillofacial prosthetics
Ideal requirements of maxillofacial materials
Silicones
Primers
Soft liners and tissue conditioners
Waxes
Coloration
Adhesives
According to the Glossary of Prosthodontics Treatment (GPT), maxillofacial
prosthodontics is defined as “The branch of prosthodontics concerned with the restoration and replacement of stomatognathic and craniofacial structures with prostheses that may or may not be removed on a regular or elective basis” (GPT) (Keith
and Steven, 2017). Maxillofacial prosthodontics is a subgroup of prosthodontics,
which is concerned with the rehabilitation of congenital and acquired defects of the
craniofacial region with prostheses, which intends to restore the defects for optimal
esthetics and function. They are divided into two major categories: intraoral prostheses and extraoral prostheses. The intraoral prostheses include surgical obturators,
interim and definitive obturators, palatal lift and speech aid prostheses, palatal drop
prostheses, mandibular guidance prostheses, tongue, jaw prostheses, and conventional dentures which tend to restore esthetics, speech, and functions. While in
extraoral prostheses, oculars, auricular, orbital, nasal, mid-facial, and somatic prostheses (replaces a body part like fingers and hand) are included. There are various
materials, which can be used to fabricate prostheses to obturate the maxillofacial
defects.
23.2
Historical background
The prosthetic rehabilitation of craniofacial defects has not been well documented
in historical literature. There is some evidence that early Chinese and Egyptians
had used wood, metals, and resins to restore the maxillofacial defects; however, the
refined techniques for restoring maxillofacial defects were introduced after World
War II with introduction of acrylic resins. The introduction of the osseointegration
concept and improvement in physical and mechanical properties of silicones have
brought revolution in the field of maxillofacial rehabilitation due to the
predictable and long-lasting, esthetic, and functional outcome. The historical background and gradual advancement in maxillofacial prosthetic materials is briefly
summarized in Table 23.1.
Biomaterials for maxillofacial prosthetic rehabilitation
617
Table 23.1 Historical background of maxillofacial prosthetic materials.
Period
Investigator
Development
Before 1600
Ambroise Pare
Prosthetic nose made from silver, artificial ear made
from paper and leather
Artificial nose made from gold
Facial prosthesis with paper and silver
Nasal defect restoration by using enameled porcelain
Combined nasal and palatal prosthesis
Nasal prosthesis fabricated with ceramic
Nasal and auricular prosthesis made with vulcanite
rubber
Nasal prosthesis made of vulcanized rubber
Facial prosthesis made with gelatin-glycerin
Vulcanized latex and water-soluble dyes
1600 1800
1800 1900
1900 40
1940 60
1960 70
1970 90
1990 to
present
23.3
Tycho Brahe
Pierre Fauchard
William Morton
Kingsley
Claude Martin
Upham
Ottofy, Baird, and Baker
Bercowitsch
Kazanjian, Bulbulian,
Clarke
US Navy
Barnhart
Lontz
Gonzalez
Turner
Udagama and Drane
Antonucci and Stansbury
Gettleman
Artificial eyes made from acrylic resin
Silicone material with acrylic resin
Modified polysiloxane elastomers
Polyurethane elastomers
Isophorone polyurethane
Silastic medical grade adhesives
New acrylic resins
Polyphosphazenes
Ideal properties of maxillofacial material
The successful completion of maxillofacial prosthesis depends on multiple factors
such as the physical, mechanical, and biological properties of materials as well as
processing conditions (Beumer et al., 2011). The required properties of maxillofacial prosthetic materials are listed in Tables 23.2 and 23.3.
23.4
Search for ideal materials for maxillofacial
rehabilitation
23.4.1 Acrylic resins (1940 60)
Acrylic resin has been used in cases when the least movement of the tissue bed is
expected during function. It has various advantages including color stability, easy
to process, can be relined and repaired, has good strength, can be fabricated with
feather margin, and a good shelf-life of about 2 years. However, this material lacks
flexibility or the ability to absorb water or adaptability to adjacent soft tissues
(Khindria et al., 2009; Udita et al., 2010). Acrylic copolymers with elastic properties have disadvantages like poor edge strength and durability when exposed to
618
Advanced Dental Biomaterials
Table 23.2 Ideal properties of maxillofacial materials.
Ideal properties of maxillofacial prosthetic materials
Processing properties
Biological properties
Physical and mechanical
properties
Dimensionally stable
Should not affect
supporting tissues
Should be nonallergic to
tissues
Nontoxic and nonirritant
Should be chemically inert
Easy to stain
Easy to manipulate
Able to reproduce fine
details
Have stable composition
No access to microbial
colonization
Odorless
Should have enough
working time
Stable properties at higher
temperature
Long-term color stability
Nontoxic while handling
Should be easy to clean
Colorants should be
stable within materials
Able to tolerate cyclic loading
Able to maintain the surface
hardness
Resistant to abrasion
Low specific gravity
Low surface tension upon
curing
High tensile strength to resist
tearing
Optimum elastic properties
Table 23.3 Required mechanical and physical properties of maxillofacial
prosthetic materials (Lewis and Castleberry, 1980).
Desirable physical and mechanical characteristics
Values
Tear strength
Tensile strength
Elastic modulus
Elongation percent
Glass transition temperature
Heat distortion temperature
Critical surface tension
Coefficient of friction
Hardness
Water absorption
30 100 psi
1000 2000 psi
50 250 psi
400% 800%
,0 C
.120 C
30 45 dyn/cm
0.4 0.6
25 35 Shore A scale
None
sunlight. The prosthesis often turns tacky and prone to dust collection and stains.
The new generation of acrylic monomers, macromeres, and oligomers are chemical,
thermal, and UV initiated; therefore, they can overcome the shortcomings of conventional acrylic copolymers (Udita et al., 2010).
Biomaterials for maxillofacial prosthetic rehabilitation
619
23.4.2 Polyvinylchloride and copolymer
These copolymers are clear and odorless materials and have been used commonly
for maxillofacial prosthetic applications with the advantages of being adaptable,
flexible, suitable for intrinsic, and extrinsic staining. Plasticizers are inserted to
incorporate elastomeric effects at room temperature. Other constituents include ultraviolet stabilizers for color stability and cross-linking agents for additional strength.
23.4.3 Chlorinated polyethylene
The processing of chlorinated polyethylene involves high heat curing pigmented
sheets in metal molds. Dow Chemicals’ chlorinated elastomer is an industrial grade
thermoplastic elastomer. It is biocompatible, noncarcinogenic, and less toxic than
thermosetting silicone materials. Chlorinated polyethylene elastomer can be a
suitable alternative to silicones for extraoral maxillofacial prosthesis when cost of
prosthesis is a limiting factor.
23.4.4 Polyurethane elastomers (1970 90)
This material is composed of aliphatic di-isocyanate groups, polyol groups (mixture
of polyesters), and organotin catalyst for completion of the polymerization process.
The proportion of these groups dictate the Shore A hardness of these polyurethane
elastomers; therefore, their intended application varies accordingly, since the maxillofacial prosthetic materials require appropriate flexibility and adaptability with
adjacent structures. Epithane-3 and Calthane are the only polyurethanes currently
available for fabricating facial prostheses. They comprise three components, roomtemperature vulcanizing materials (Huber and Stephan, 2002). These materials can
be used to rehabilitate soft tissue defects, as they have the inherent flexibility
needed to adapt with tissues for stability and esthetics. These possess environmental
stability, low modulus, require no addition of plasticizers, and have higher tear
strength, optimum ultimate strength, and elongation. Intrinsic coloration is possible
with these materials; therefore, they are amenable to maxillofacial processing techniques. The disadvantages include lack of compatibility with adhesive systems, low
color stability, and moisture sensitivity resulting in gas bubbles during processing,
due to the presence of di-isocyanate. Hence, the reaction should be carried out in
dry atmosphere, as carbon dioxide would be produced, resulting in porous elastomer (Robert and John, 2002).
23.4.5 Thermoset urethane elastomers
Thermoset urethane elastomers are produced through the introduction of primary
chemical cross-linkers. If reactants are combined in stoichiometric ratios and reactions are preferentially catalyzed, a known controlled morphology can be developed. According to Yu et al. (1980), the aging process affects polyurethane
significantly.
620
Advanced Dental Biomaterials
23.4.6 Silicones (1960 70)
Silicones are known as polydimethylsiloxane, the most successful maxillofacial
prosthetic material to date. The silicones are popular materials due to their better
physical and mechanical properties over other materials (excellent tear, tensile, and
peel strength). Furthermore, they can be stained intrinsically and extrinsically to
provide more esthetic and lifelike appearance. When appropriately vulcanized, silicones elastomers can resist deposition of organic materials that may lead to bacterial colonization, therefore, with simple cleaning methods, these materials are
relatively safe and hygienic compared to other materials (Sharif et al., 2010).
23.5
Silicones
In general silicones exist in five different structures (Fig. 23.1). By changing the
structure of silicone, many different types of silicones can be produced.
23.5.1 Polymer structures (Deanin, 1972)
1. Linear polymers: Volatile and nonvolatile fluids (dimethicone).
2. Ring polymers: Volatile fluids (cyclomethicone).
3. Branched polymers: The ends of branches provide additional opportunities to connect
with other chains of polymers.
4. Cross-linked polymers: Gels, elastomers, sealants, rubber.
5. Resins: Structures that create three-dimensional films upon curing. This type of silicone
has industrial and commercial application.
The silicones are synthetic materials, which consist of long chains of polymer
units. Silicones have different chemical and physical properties that make them more
useful than other polymers, and they keep these desirable properties under different
environmental conditions (Dow Corning Corporation). Unlike organic polymers, silicone’s structure is made up of alternating chains of oxygen and silicon atoms.
Mostly organic or methyl groups are attached to sides of silicone atoms (Fig. 23.2).
Figure 23.1 Basic polymer structures (Deanin, 1972).
Biomaterials for maxillofacial prosthetic rehabilitation
621
Figure 23.2 Basic silicone unit (Colas and Curtis, 2005).
Figure 23.3 Basic steps in silicone polymer synthesis (Colas and Curtis, 2005).
By modifying the length of this oxygen silicone chain, scientists can produce
different forms of silicones, such as fluids, resins, or viscous elastomers. These longchain synthetic silicones are used in various products, including waxes, repellants,
polishes, nonstick coatings, and electrical insulation (Dow Corning Corporation).
Silicone does not exist naturally; therefore, it is completely synthetic in nature. It
is often bound with oxygen in materials like sand, granite, and quartzite. The highgrade quartz is reduced to elemental silicone by reacting in an electric furnace in a
process called carbothermic smelting. The next step in the procedure is producing
methylchloride by condensing methanol with hydrochloric acid (Dow Corning
Corporation). Generally, two methyl groups (CH3) attach to each silicone atom to
comprise each molecule of dimethyldichlorosilane, the principal unit of silicone.
Methylchloride is then allowed to flow through the fluid form of silicone powder; this reaction is accelerated by a copper-based catalyst and produces complex
units of methylchlorosilanes. The multiple methylchlorosilane groups are separated
by distillation reaction and then condensed to dimethyldichlorosilane. When water
is added to dimethyldichlorosilane (principal chlorosilane), the two (water and
dimethylchlorosilane) react to disilanols and hydrochloric acid. This reaction occurs
as oxygen has more affinity for silicone while chlorine has more affinity for hydrogen (Fig. 23.3). The final step is catalyzed by hydrochloric acid, which further
622
Advanced Dental Biomaterials
Table 23.4 Composition of silicone elastomer (Colas and Curtis, 2005).
Contents
Examples
Silicone polymer
Fillers
Catalyst/vulcanizing agent
Polydimethylsiloxane
Silica
Platinum salt
Dichlorobenzyl peroxide
Stannous octoate
Barium, tin
Hydromethylsiloxane
Opacifiers
Cross-linking agent
condenses disilanols into polydimethylsiloxanes and forms the backbone of silicone
atoms bounded by oxygen atoms (Dow Corning Corporation).
Dimethyldichlorosiloxane, which takes part in a catalyzed reaction, is the most
frequently used material for maxillofacial prosthetic rehabilitation. It forms a polymer upon reaction with water. These polymers appear as translucent, white fluids
and are watery in consistency. The extent of viscosity can be assessed by the length
of the polymer chain (Dow Corning Corporation). Most rubbery consistency silicones are manipulated with fillers, which provide the required strength.
Furthermore, additives provide different colors to translucent silicones. Vulcanizing
agents as well as antioxidants are used to convert the raw product from plastic to a
rubbery consistency, during processing. The long chain of polymer creates a network, which is difficult to disengage. This strong network makes the silicone resistant to adverse changes upon exposure to ultraviolet radiations. The general
composition of silicone elastomer is shown in Table 23.4.
23.6
Classification of maxillofacial silicones
23.6.1 Classification of silicones according to application
(Beumer et al., 2011)
1.
2.
3.
4.
Implant grade
Medical grade
Food grade
Industrial grade
23.6.1.1 Implant grade
These materials need extensive testing and should fulfill FDA requirements to be
used for medical purposes. According to literature, silicone breast implants have a
controversial outcome regarding the success and safety of interstitial implants
placement; therefore, these materials need further research.
Biomaterials for maxillofacial prosthetic rehabilitation
623
23.6.1.2 Medical grade
These materials were approved for external use only. Their use in health care is
widespread, mainly due to their biocompatibility and biodurability. Silicone use for
maxillofacial prosthetics started in 1943, but the medical use started in 1953. The
first silicone was investigated and developed by Dow Corning; they further developed a separate center to study medical applications of silicone materials in 1963.
Later, silicones because popular and the material of choice for facial prostheses due
to the physical properties similar to the skin texture (Fig. 23.4). Adverse reactions
can be caused by contact of silicone prostheses with skin, but these reactions are
very rare.
23.6.1.3 Food grade
These materials meet FDA rules and regulations for food content. Many manufacturers claim that food grade silicones are safe to be used as maxillofacial prosthesis.
VST-50 silicone material is a food grade silicone manufactured by Factor II Inc.,
the United States. Food grade silicones are more economical than medical grade
silicones and might be used as an alternative, but their properties need to be evaluated before regular use in the fabrication of maxillofacial prosthesis
23.6.1.4 Industrial grade
These materials have industrial application and their use in maxillofacial prosthetics
is not documented.
Figure 23.4 Medical grade silicones.
624
Advanced Dental Biomaterials
23.6.1.5 Maxillofacial silicones
Maxillofacial silicones can be divided into two major groups according to their vulcanization reactions (Beumer et al., 2011; Colas and Curtis, 2005) (Table 23.5).
1. Room-temperature vulcanization (RTV) silicone
2. High-temperature vulcanization (HTV) silicone
The vulcanization reaction of polymers includes the bonding of separate polymer
chains. The ties among the long chains of polymer units are called cross-linking of
polymers. The process through which cross-linking of polymer chains takes place is
called vulcanization. The reaction can occur either with or without the use of heat,
depending on the catalytic and/or cross-linking agents. The silicone elastomers used
for maxillofacial prosthetics (medical grade) contain fillers and specific vulcanizing
agents; however, they lack the huge variety of additives used in the organic rubber
industry.
23.6.1.6 Room temperature vulcanizing silicone elastomer
There are two types of RTV silicones (Mitra et al., 2014):
1. Cross-linking by condensation reaction
2. Cross-linking by addition reaction
Cross-linking by condensation reaction (Mitra et al., 2014)
They contain active groups such as silanols (hydroxyl-terminated polysiloxanes).
Cross-linking by this method requires a cross-linking agent, for example, tetraethyl
silicate, and a catalyst, for example, dibutyltin dilaurate, for example, Silastic
Medical Adhesive type A (Dow Corning), where methyl triacetoxy silane (II) will
be used as the cross-linking agent. However, cross-linking requires water molecules
to hydrolyze the silane and produces acetic acid (an irritant) as a by-product. These
types of silicones have limited use, mostly used to fix extrinsic staining.
Disadvantages (Mitra et al., 2014)
1. Releases by-products
2. Vulcanization time is excessively long
3. Includes degradation reaction such as hydrolysis
Table 23.5 Properties of the two types of silicone materials (Mitra et al., 2014).
S. no.
Properties
HTV
RTV
1.
2.
3.
Ultimate tensile strength (MPa)
Maximum elongation (%)
Pants tear strength (dyn/
cm 3 106)
4.
Dynamic modulus (MPa)
5.86
441
Does not tear but
stretches, as in
tensile elongation
4.66
4.20
445
Does not tear but
stretches, as in
tensile elongation
2.12
HTV, High temperature vulcanization; RTV, room temperature vulcanization.
Biomaterials for maxillofacial prosthetic rehabilitation
625
4. Relatively lower tear strength
5. Unable to maintain edge resistance
Cross-linking by addition reaction (Mitra et al., 2014)
The reactions usually involve the addition of silyl hydride groups ( SiH) to vinyl
groups (CH2QCH ) attached with the silicone by the help of a platinum catalyst.
These silicones are not strictly room-vulcanized silicones. The curing of these silicones requires exposure of dry heat at 150 C for an hour. These silicone elastomers
have enhanced tear strength as compared to the first type of RTV silicones.
Disadvantages (Mitra et al., 2014)
1. Very hydrophobic
2. No extrinsic coloration
3. Curing of the materials may be inhibited by: amines, sulfur, nitrogen oxides
23.6.1.7 High-temperature vulcanizing silicone elastomer
The synthesis of heat-vulcanized silicone includes use of a di-organo-polysiloxane
such as poly (dimethyl siloxane). When the liquid form of silicone is heated with
benzoyl peroxide activator, a reaction results between one of the methyl radicals in
the chain and an identical group in the adjacent chain. It results in cross-linking
between two polymeric chains occur and ultimately yields benzoic acid as a byproduct. HTV silicone has been manufactured in three different consistencies, soft,
medium, and hard. It is usually colorless or white in color with opaque appearance
and varying degree of consistency (Dow Corning Corporation; Colas and Curtis,
2005).
Advantages (Mitra et al., 2014):
1.
2.
3.
4.
Adequate tear strength
High tensile strength (5.87 MPa)
Excellent thermal, color, and chemical stability
Adequate percentage of elongation
Disadvantages (Mitra et al., 2014):
1.
2.
3.
4.
Poor esthetics due to opacity
Less elasticity
Low edge strength
Technique sensitive
23.7
Types of maxillofacial silicones
23.7.1 Most common room temperature vulcanizing silicones
Many materials have been tried to replace the lost hard and soft tissues of the body,
including wood, stones, metals, and ceramics. After World War II, acrylic was
introduced to rehabilitate the ocular defects. The greatest revolution in maxillofacial
626
Advanced Dental Biomaterials
prosthetics rehabilitation came with the introduction of maxillofacial silicones.
These maxillofacial silicones were considered superior to conventionally used
acrylic resins for facial prostheses due to their flexibility, biocompatibility, ease of
processing, and ability to adapt with adjacent soft tissues providing a lifelike
appearance.
Maxillofacial silicone MDX4-4210 is a translucent, two-component silicone
(10:1 base to catalyst ratio by weight). It was introduced in 1970 and has been the
most common silicone for facial prostheses. Silastic MDX4-4210 biomedical grade
elastomer is a room temperature vulcanizing silicone, supplied as pourable twocomponent silicone, which vulcanizes upon mixing with catalyst, resulting in a
translucent silicone elastomer. The vulcanization of silicone can be accelerated by a
dry heat oven without significantly affecting the physical properties.
The maxillofacial silicone A-2186 (Fig. 23.5) was introduced in 1986 for the
fabrication of facial prosthesis. This silicone has been claimed to have comparable
properties as MDX4-4210. It is a translucent silicone, composed of two parts silicone (10:1 ratio by weight for base to catalyst). The rapid vulcanization form of A2186 was introduced in 1987 with more platinum content to accelerate the curing
of silicone. According to a study by Sanchez, A-2186 had greater tensile strength,
tear resistance, and a higher percentage of elongation. A-2186 silicone also proved
to be softer at the surface than the MDX 4-4210. The combination of these physical
properties makes A-2186 silicone a better choice than the more conventionally used
MDX 4-4210 for the fabrication of maxillofacial prostheses. The properties of the
two most common maxillofacial silicones, MDX4-4210, and A-2186 are shown in
Table 23.6.
Figure 23.5 Maxillofacial silicone A-2186.
Biomaterials for maxillofacial prosthetic rehabilitation
627
Table 23.6 Comparative properties of two most common maxillofacial
silicones (Platinum silicone A-2186; MDX4-4210).
Properties
Silicone A-2186
MDX4-4210
Color
Consistency
Viscosity
Specific gravity
Working time
Durometer Shore A
Tensile (psi)
Elongation (%)
Translucent
Pourable
90 Pa s
1.10
2h
29
900
650
Translucent
Pourable
60
1.11
3
30
730
470
Table 23.7 Properties of different types of liquid silicone rubber silicone elastomers.
Silicones
Durometer
(Shore A)
Tensile
strength
(psi)
Elongation
(%)
Modulus
100%
(psi)
Tear
strength
(ppi)
Appearance
A-221-05
A-223-30
A-223-40
A-225-50
A-225-60
A-225-70
5
31
41
50
59
68
450
1400
1230
1225
1300
1300
980
790
615
570
480
450
15
90
190
295
350
530
60
195
255
265
250
240
Clear, thixotropic
Clear, paste-like
Clear, paste-like
Clear, paste-like
Clear, paste-like
Clear, paste-like
23.7.2 Medical grade liquid silicone elastomers
Liquid silicone rubber (LSR) is a colorless, translucent clear paste. This silicone is
composed of part-A and part-B that are mixed together in equal proportions, 1:1
ratio by weight. The LSR platinum-catalyzed addition-cured silicone appears
optically clear and is available in different types depending on the mechanical properties (Table 23.7). Conventionally, silicone A-221-05 is used for breast and delicate soft tissues prostheses due to very low Shore A hardness and modulus along
with high elongation properties, which makes it highly soft and flexible. Silicones
A-223-30 and A-223-40 are recommended for facial prostheses and somatic prostheses (fingers, hand, and foot prostheses), as the facial prosthesis needs to have
Shore A hardness in the range of 30 50. Silicones with higher Shore A hardness,
modulus, and low elongation properties are generally used to replace the hard tissues and molds fabrication.
23.7.3 Recommendations
05—Facial—breast prosthetics
30 40—Facial, finger, and hand prosthetics
50 70—Molds fabrication and restoration of hard tissue defects
628
Advanced Dental Biomaterials
23.7.4 Medical grade VerSiTal silicone elastomers
The VST groups of silicones are translucent, composed of part-A and part-B, that
are mixed in the ratio of 10:1 by weight (Fig. 23.6). These silicones have low viscosity; however, the viscosity can be increased by using thixotropic agents, depending upon the application. The VST groups of silicones are room temperature
vulcanizing, but the vulcanization reaction can be accelerated by exposure to high
temperature. These platinum-based addition-cured silicones are commonly used to
fabricate silicone facial prostheses. The VST silicones are available in different
types according to their vulcanization time and Shore A hardness. (Table 23.8) The
silicone VST-30 has a short working and curing time; therefore, it requires expertise
while mixing intrinsic stains according to patient’s skin tone. The curing times
mentioned in Table. 23.9 are according to RTV.
23.8
M-511 platinum silicone rubber
M-511 was specially formulated for the fabrication of maxillofacial prostheses. It is
the silicone elastomer of choice at many clinics and hospitals throughout England.
This silicone is ideal for implant-retained facial prostheses, as it has been claimed
to bond well with methyl methacrylate (acrylic) resin. The recommended base to
catalyst mixing ratio is 10:1, by weight. Upon vulcanization this silicone attains
25 30 Shore A hardness, which is considered appropriate to be used for the fabrication of facial silicone prosthesis. The M-511 silicone elastomer has 1 hour of
working time.
Silicone M-511 can be used with following components to modify its properties:
G
G
G
M-510 gel catalyst to fabricate gel-filled prosthesis
M-513 softening agent to modify Shore A hardness (Shore A 15 20)
M-514 antislump agent (thixotropic agent)
Figure 23.6 VST silicone elastomers for maxillofacial prosthetics.
Biomaterials for maxillofacial prosthetic rehabilitation
629
Table 23.8 Properties of different types of VST silicone materials.
Properties
VST-30
VST-50
VST-50F
VST-50HD
Translucent
Shore A
Cure time RTV
Pot life
Tear strength (ppi)
Tensile strength (psi)
Elongation (%)
Viscosity A
Viscosity B
Yes
23
25 30
10 13 min
115
985
610
12,000
10,000
Yes
30
Overnight
90 min
130
1035
660
12,000
10,000
Yes
28
2 3h
30 min
120
1095
625
12,000
10,000
Yes
38
Overnight
2h
110
950
550
15,000
10,000
Table 23.9 Shore A hardness of VST silicones.
Product
Cure
Shore A hardness
VST-30
VST-50
VST-50F
VST-50HD
25 30 min
Overnight
2 3h
Overnight
23
30
28
38
Note: The base of all VST silicone materials is similar. They vary according to their crosslinking agents.
23.8.1 Silicone fluids
These silicone fluids are supplied as thinning agents for all silicone elastomers and
are composed of straight-chained 100% polydimethylsiloxane. These agents have
been recommended to be used at no more than 20% by weight of silicone, during
silicone mixing to improve the working time (Table 23.10).
23.8.2 Properties
G
G
G
G
G
G
G
Optimum resistance to low and high temperatures
Good dielectric properties
Low surface tension
High compressibility
Absence of aging upon exposure to atmospheric changes
Better oxidation resistance
Minimal change in viscosity with temperature
23.8.3 Types of silicone fluids
G
G
G
A-313 functional silicone fluid (platinum compatible)
A-318 OH thinner
A-244 silicone fluid
630
Advanced Dental Biomaterials
Table 23.10 Research studies about maxillofacial silicones.
S.
no.
Author (year)
Study conducted
Materials used
Conclusion
1.
Andreopoulos
and
Evangelatou
(1994)
Silica fiber fillers (short
aramid fibers, glass
fibers, high modulus
polyethylene fibers)
Instead of ultrahighmodulus fibers, silica
fillers should be used
2.
Lai (1996)
Effect of fillers on the
mechanical properties
(tensile strength and
modulus) of poly
(dimethyl siloxane)
rubber (C-50, Bayer
AG, Leverkusen,
Germany) maxillofacial
material
Invention of polysiloxane
materials including
MPDS to reduce the
hydrophobicity of
silicones
Modification of polydimethyl-siloxanes.
Thermal initiator—
lauroyl peroxide
preferred over benzoyl
peroxide. Filler—
amorphous silica.
Cross-linker—
TEGDMA. Thermal
curing of the
polysiloxane MPDS
was conducted in a
stainless steel mold to
minimize the effects of
oxygen inhibition
MPDS has following
advantages over MDX44210:
Very long working time
Extended shelf-life
Higher tear and tensile
strength
Incorporation of
methacrylate group in
the silicones reduces the
hydrophobicity of the
silicones enhances the
adhesive bond strength
to the nonsilicone-based
adhesives. However, the
ultimate elongation is
slightly lower than that
of MDX4-4210
Tensile strength improved
with increasing silica
fillers up to 35%
significantly
3.
Andreopoulos
et al. (1998)
4.
Lai et al. (2002)
5.
Aziz et al.
(2003b)
Effect of reinforcement of
silica powder up to
50% concentration on
the mechanical
properties of silicone
maxillofacial materials
Introduction of new
organosilicone MPDSMF 606
Silica powder up to 50%
concentration
Effect of different
parameters on the
development of new
improved maxillofacial
material C-50
Silica fillers—R104, R106,
R202, R972, R974, and
R812. Silica filler
concentrations—
0 25 wt.%. Crosslinker concentration—
0.12 0.72 g (per 10 g
of base polymer)
Ratio of high and low
molecular weight
polymers
Modified MPDS and
comparing the
properties with A-2186
G
G
G
The hardness is similar to
A-2186, whereas tear,
tensile strength, ultimate
elongation, and
adhesive bond to
nonsilicones are higher
than A-2186. Suitable
for use in fabrication of
clinical prostheses
Increasing the R812 silica
filer concentration from
15 to 20 wt.% and
having cross-linker of
0.28% was associated
with significant increase
in tear strength
(Continued)
Biomaterials for maxillofacial prosthetic rehabilitation
631
Table 23.10 (Continued)
S.
no.
Author (year)
Study conducted
Materials used
Conclusion
6.
Karayazgan
et al. (2003)
Effect of tulle in
increasing the tear
strength of
maxillofacial
prosthesis at the edges
Tulle
7.
Aziz et al.
(2003a)
Analysis of the properties
of commonly used
silicone rubber
materials
Cosmesil HC and Nusil
(MED-4920), Prestige
(Premium facial and
body elastomer), Factor
II (A-2186)
8.
Gunay et al.
(2008)
Tulle
9.
Mirabedini et al.
(2008)
Investigation on the
incorporation of tulle
in silicone
maxillofacial
prosthesis
Effect of TiO2 on the
mechanical and
adhesion properties of
RTV silicone
elastomer coatings
Tulle resulted in having a
more stable and tearresistant silicone
prosthesis, which is less
likely to deform during
application or removal
of adhesives, cosmetics,
or cleaning agents
None of the commercially
available materials have
adequate properties.
Cosmesil HC and Nusil
(MED-4920) had
adequate mechanical
properties along with
good translucency but
have high viscosity.
Prestige (premium
facial and body
elastomer) was a soft
material; however,
together with Cosmesil
St, it had extremely
high water absorption
and low tears strength
Factor II (A-2186) had
well all round
mechanical properties
and had the highest tear
strength
Tensile and tear strengths
were significantly
higher
10.
Sharif et al.
(2010)
Effect of POSS on the
mechanical properties,
of maxillofacial
material (Factor II A2000)
TiO2 fillers—5.0, 10.0,
15.0, and 20.0 wt.%
POSS
Tensile stress, modulus,
and abrasion resistance
increased with the
increase in filler content
up to 15.9 wt.%.
Hardness was increased
with increasing filler
contents up to 25.0 wt.
%, but on the contrary,
elongation to fracture
was decreased with
increasing filler content
The POSS loading had a
significant effect on the
tear and tensile
properties of the
materials
(Continued)
632
Advanced Dental Biomaterials
Table 23.10 (Continued)
S.
no.
Author (year)
Study conducted
Materials used
Conclusion
11.
Liu et al. (2013)
Effect of silicone
elastomers filled with
hollow microspheres
Hollow microspheres were
mixed with MDX44210 silicone elastomer
using Q7-9180 silicone
fluid as diluents.
Volume fractions of
microspheres were 0%,
5%, 15%, and 30% v/v
(volume ratio to the
total volume of MDX44210 and microspheres)
were used
The microspheres dispersed
well in the matrix. Shock
absorption was the
greatest by the 5% v/v
composite and decreased
with increasing
concentrations of
microspheres. Other
properties except
elongation at break
decreased with increasing
concentration. Tear
strength of all composites
was markedly lower than
that of pure silicone
elastomer. Has good
biocompatibility. Novel
light and soft material
with good flexibility,
biocompatibility, and
properties at 5% holds a
promising prospect for
clinical application as
maxillofacial prosthesis
MPDS, Methacryloxyalkyl-terminated polydimethylsiloxanes; POSS, polyhedral silsesquioxane; RTV, room temperature vulcanization.
23.9
Primers
The primers used for maxillofacial silicones are usually platinum-cured, composed
of one component. These are designed to improve the adhesion of addition-cured
silicones to various substrates, including metals, glass, ceramics, some plastics,
and other silicone materials.
The platinum primers are transparent liquids with viscosity of 1.0 cps and specific gravity 0.77 (Table 23.11). The platinum primers contain VM&P Naphtha as
the main solvent. A uniform thin film is required for best bonding results. They
should be applied after thorough cleaning and degreasing of the surface of substrate
with a chlorinated solvent 1:1:1 trichloroethane acetone or MEK. After the substrate
dries, a uniform thin coat of primer is applied at room temperature with 50% relative humidity. The primer coat should be allowed to dry for a minimum of 30 minutes. The primer sets by exposure to moisture and higher humidity. The heavy
whitish haze or chalky appearance is indicative of a thick layer of primer, which
can adversely affect the bond strength; therefore, the primer should be cleaned and
reapplied. The most common primers used for maxillofacial silicones are A-330G,
A-304, A-306, and G-611 (A-306; A-330 G).
Biomaterials for maxillofacial prosthetic rehabilitation
633
Table 23.11 Properties of platinum primers.
23.10
Properties
Platinum primers
Color
Viscosity (cps)
Flash point
Solvent
Specific gravity
Nonvolatile content
Drying time at 77 F
Translucent
1.0
48 F
VM&P Naphtha
0.77
5
30 min
Soft liners and tissue conditioners
23.10.1 Soft liner
Soft liner material is used to reline the acrylic base temporarily for rebasing (relining) and tissue conditioning. It is available as a two-component (Fig. 23.7) powder
and liquid system, which when mixed at the recommended ratio, forms a paste-like
consistency.
Advantages:
Fast application
No heat irritation
Easy to trim
Good retention
Smooth surface minimizes unwanted food debris retention
Simple to remove from the denture at the end of the treatment
This material can be used in following conditions:
To reline immediate acrylic denture base after extraction to reline and improve retention.
To rebase the ill-fitting dentures to improve the adaptation with denture bearing areas.
To reline the denture base temporarily to improve the health of inflamed tissues.
After surgical resection of tumors, the bulb portion of immediate surgical obturators can
be reline postoperatively to close the fresh surgical defect.
5. To reline the denture base in fresh surgical sites to push the skin graft toward the tissue
bed.
1.
2.
3.
4.
23.10.2 Coe-Comfort and Coe-Soft
These are resilient, self-curing reline materials that are used when the patient
requires a soft, temporary liner in upper or lower dentures. Polymerization takes
place in or out of the mouth in approximately 15 minutes. The reline normally lasts
for approximately 3 months.
Coe-Comfort and Coe-Soft materials are supplied as two parts, powder and liquid (Fig. 23.8), which are mixed together to obtain a paste-like consistency.
634
Figure 23.7 Soft liner for denture base acrylic resin.
Figure 23.8 Coe-Soft and Coe-Comfort reline materials.
Advanced Dental Biomaterials
Biomaterials for maxillofacial prosthetic rehabilitation
635
Figure 23.9 Sculpturing wax for facial wax pattern.
These are used in the following conditions:
1.
2.
3.
4.
5.
Ideal for postsurgical applications; placement of immediate denture.
As functional impression materials during rebasing of dentures.
As tissue conditioners to recover the health of tissues.
To perform the functional molding of bulb portion of speech aid prosthesis.
Postoperatively to reline the obturators to close the oral communication for the purpose of
improved healing and prevention from infection.
23.10.3 Sculpturing clays and waxes
Modeling clays for use in maxillofacial prosthetics are available for sculpturing and
carving for face prosthesis. These clays are sulfur-free to prevent contamination of
molds before packing in platinum vulcanizing silicones. These are available in different colors and hardnesses (soft, medium, hard) to carve according to different
depth and layers (Fig. 23.9). Waxes, on the other hand, are easy to sculpt and need
less artistic skills than clays due to the advantage of being easy to melt and adjust
during trial procedures.
23.11
Coloring agents
23.11.1 Colored flocking
The skin is composed of different layers with different chroma value hues for
everyone; therefore it is important to match the skin tone individually as much as
possible to give a lifelike appearance. Flocking coloring agents are fine hair-like
nylon or rayon flocks of 0.75 mm length (Fig. 23.10), which are added into maxillofacial silicone and painted on to the mold with stains to give the superficial skin
636
Advanced Dental Biomaterials
Figure 23.10 Rayon flocking for silicone elastomers (Flocking).
tone. Flocking along with stains mimic the shade of melanomas, sebaceous glands,
and tiny blood vessels beneath the skin layers.
23.11.2 Intrinsic stains
The intrinsic colors are added in maxillofacial silicone during mixing of base and
catalyst according to the individual skin tone. These stains are created by the addition of cosmetic pigments within silicone cross-linking fluids to make silicone
stains. These stains chemically bind with addition-cured platinum silicones, therefore lasting longer in optimum conditions. Intrinsic stains have the major role in
fabricating an esthetically pleasing facial prosthesis. These are available from basic
colors to premixed average skin colors (Fig. 23.11).
23.11.3 Extrinsic colors
Extrinsic staining is useful if the intrinsic staining is not enough or to incorporate
some pigmentation to simulate the natural skin tone. Extrinsic stains are available
in dry earth powder pigments and silicone thixotropic paste forms (Fig. 23.12).
These stains are applied with appropriate-sized painting brushes after thorough
cleaning of prosthesis with acetone or alcohol to remove the greasy debris and dust.
23.11.4 Acetoxy silastic adhesives
The silicone adhesives are condensation-cured silicones, supplied as onecomponent, translucent silicones (Fig. 23.13) with low slump property. The acetoxy
Biomaterials for maxillofacial prosthetic rehabilitation
637
Figure 23.11 Silicone intrinsic colors compatible with platinum-cured silicones (Functional
Intrinsic Skin Colors).
Figure 23.12 Thixotropic silicone extrinsic stains (Extrinsic colors).
silicone adhesives cure at room temperature upon exposure to atmospheric moisture. During the curing process, the silicone adhesives release acetic acid vapor as a
by-product. After curing, the silicone elastomer has a texture, appearance, and composition like most other conventional silicone polydimethylsiloxane elastomers. The
initial curing takes place within 20 minutes, while the complete curing with optimum physical properties are achieved after 24 120 hours depending on the atmospheric moisture and humidity.
These medical adhesives are used to bond acrylic resin or metals to platinumcured silicone prostheses. The primary use of medical adhesives in maxillofacial
prosthetics is to fix the external staining of a silicone facial prosthesis by applying
a thin coating. The silicone prosthesis appears shiny upon fixation of stains with
medical adhesives; therefore, solutions like MD-564 can be used to matte the
appearance of the final silicone prosthesis.
638
Advanced Dental Biomaterials
Figure 23.13 Acetoxy silastic silicone adhesive and dispersion liquid (Extrinsic sealing kit).
Table 23.12 Properties of acetoxy silicone adhesives used for maxillofacial prostheses.
Properties
Medical adhesive A-100
A-564
Appearance
Specific gravity
Durometer hardness
Tensile strength (psi)
Elongation (%)
Translucent
1.06
38
480
450
Translucent
1.08
28
780
650
These adhesives can also be used to bond the dislodged acrylic housing containing retentive elements to the vulcanized silicone prosthesis for repair purposes, and
repair of small voids and tears in vulcanized silicone by mixing the adhesive with
intrinsic stains and applying a thin layer on chair-side. This is the time-saving alternative, which can be utilized temporarily for an emergency repair (Table 23.12).
23.12
Skin adhesives
Maxillofacial prostheses are retained by various methods, including craniofacial
implants, skin adhesives, anatomical undercuts, and mechanical retention by means
of spectacles. Craniofacial implants are considered the best option for optimum
retention of facial prosthesis; however, radiotherapy and systemic health are the relative contraindications for implants placement.
Biomaterials for maxillofacial prosthetic rehabilitation
639
Figure 23.14 Daro water-based skin adhesive for retention of silicone facial prosthesis.
The skin adhesives are supplied as silicone based and water based. The silicone
adhesives are difficult to clean from silicone prostheses compared to water-based
adhesives due to the compatibility of silicone adhesives with a silicone prosthesis.
Therefore, patients have shown more compliance toward water-based adhesives.
These are applied in a thin layer over the margins of the silicone prosthesis. The
white appearance of adhesive changes to a clear layer upon leaving at room temperature or exposure to compressed air. The water-based adhesives are available in different strengths as their application varies according to the weight and size of
silicone prosthesis.
The edge adhesives are available to be used on the thin margins of a silicone
prosthesis, which are more prone to tear with regular strength adhesives upon insertion and removal of the prosthesis. These adhesives provide minimal bond strength,
therefore protecting the thin margins of the prosthesis. The edge adhesives are used
to seal the margins and blend them with adjacent skin (Fig. 23.14).
References
A-306: Platinum Primer. Product Information. Factor II, Inc., Forest Avenue, Lakeside, AZ.
Available from: ,http://www.factor2.com/Primer_Silicone_Bond_Elastomer_p/a-306.
htm..
A-330 G: Platinum Primer. Product Information, Factor II, Inc., Forest Avenue, Lakeside,
AZ. Available from: ,http://www.factor2.com/Gold_Platinum_Primer_Silicone_
Bonding_Elastomer_p/a-330-gold.htm..
640
Advanced Dental Biomaterials
Andreopoulos, A.G., Evangelatou, M., 1994. Evaluation of various reinforcements for maxillofacial silicone elastomers. J. Biomater. Appl. 8 (4), 344 360.
Andreopoulos, A.G., Evangelatou, M., Tarantili, P.A., 1998. Properties of maxillofacial silicone elastomers reinforced with silica powder. J. Biomater. Appl. 13 (1), 66 73.
Aziz, T., Waters, M., Jagger, R., 2003a. Analysis of the properties of silicone rubber maxillofacial prosthetic materials. J. Dent. 31, 67 74.
Aziz, T., Waters, M., Jagger, R., 2003b. Development of a new poly (dimethylsiloxane) maxillofacial prosthetic material. J. Biomed. Mater. Res. B: Appl. Biomater. 65 (2),
252 261.
Beumer, J., Marunick, M.T., Esposito, S.J., 2011. Prosthodontic and Surgical Management of
Cancer-related Acquired, and Congenital Defects of Head and Neck, third ed.
Quintessence Pub. Co Inc..
Colas, A., Curtis, J., 2005. Silicone Biomaterials: History and Chemistry in Silicone
Biomaterials: History and Chemistry & Medical Applications of Silicones. Dow
Corning, pp. 80 86.
Deanin, R.D., 1972. Polymer Structure, Properties, and Applications. Cahners, Boston, MA,
p. 496.
Dow Corning Corporation. Product Information, Dow Corning. Available from: ,http://
www.dowcorning.com/content/discover/discoverchem..
Extrinsic Colors. Product Information, Factor II, Inc., Forest Avenue, Lakeside, AZ.
Available from: ,http://www.factor2.com/Extrinsic_Coloration_Individual_Colors_p/
fe-extrinsic-colors.htm..
Extrinsic Sealing Kit. Product Information. Factor II, Inc., Forest Avenue, Lakeside, AZ.
Available from: ,http://www.factor2.com/Extrinsic_Sealing_Kit_p/564-kit.htm..
Flocking. Product Information. Factor II, Inc., Forest Avenue, Lakeside, AZ. Available from:
,http://www.factor2.com/H_Flocking_Individual_Colors_p/h-100.htm..
Functional Intrinsic Skin Colors. Product Information. Factor II, Inc., Forest Avenue,
Lakeside,
AZ.
Available
from:
,http://www.factor2.com/
Functional_Intrinsic_Skin_Colors_p/fi-sk.htm..
Gunay, Y., Kurtoglu, C., Atay, A., Karayazgan, B., Gurbuz, C.C., 2008. Effect of tulle on the
mechanical properties of a maxillofacial silicone elastomer. Dent. Mater. J. 27 (6),
775 779.
Huber, H., Stephan, P.S., 2002. Materials and techniques in maxillofacial prosthodontic rehabilitation. Oral Maxillofacial Surg. Clin. N. Am. 14, 73 93.
Karayazgan, B., Gunay, Y., Evlioglu, G., 2003. Improved edge strength in a facial prosthesis
by incorporation of tulle. J. Prosthet. Dent. 90 (6), 526 529.
Keith, J.F., Steven, M.M., 2017. The glossary of prosthodontic terms 9th ed. J. Prosthet.
Dent. 117 (5), 6 92.
Khindria, S.K., Bansal, S., Kansal, M., 2009. Maxillofacial prosthetic materials—review article. J. Indian Prosthodont. Soc. 9 (1), 2 5.
Lai J.H., 1996. Maxillofacial Prosthetic Materials, US Patent No. 5, 584, 886.
Lai, J.H., Wang, L.L., Ko, C.C., DeLong, R.L., Hodges, J.S., 2002. New organosilicon maxillofacial prosthetic materials. Dent. Mater. 18, 281 286.
Lewis, D.H., Castleberry, D.J., 1980. An assessment of recent advances in external maxillofacial materials. J. Prosthet. Dent. 43 (4), 426 432.
Liu, Q., Shao, L.Q., Xiang, H.F., Zhen, D., Zhao, N., Yang, S.G., et al., 2013. Biomechanical
characterization of a low density silicone elastomer filled with hollow microspheres for
maxillofacial prostheses. J. Biomater. Sci. Polym. Ed. 24 (11), 1378 1390.
Biomaterials for maxillofacial prosthetic rehabilitation
641
MDX4-4210 Silicone Elastomer. Product Information. Available from: ,http://www.lookpolymers.com/pdf/Multibase-SILASTIC-MDX4-4210-Dow-Corning-Biomedical-GradeElastomer.pdf..
Mirabedini, S.M., Mohseni, M., Pazokifard, S.H., Esfandeh, M., 2008. Effect of TiO2 on the
mechanical and adhesion properties of RTV silicone elastomer coatings. Colloids Surf.
A: Physicochem. Eng. Asp. 317, 80 86.
Mitra, A., Choudhary, S., Garg, H.J., 2014. Maxillofacial prosthetic materials—an inclination
towards silicones. J. Clin. Diagn. Res. 8 (12), 8 13.
Platinum Silicone A-2186. Product Information. Factor II, Inc., Forest Avenue, Lakeside, AZ.
Available from: ,http://www.factor2.com/Silicone_Elastomer_RTV_Facial_Prosthetic_
p/a-2186.htm..
Robert, G.C., John, M.P., 2002. Restorative Dental Materials, eleventh ed. Mosby, Inc,
Philadelphia, PA.
Sharif, A.M., Alvin, G.W., Deborah, J.R., Scott, R.S., 2010. Maxillofacial materials reinforced with various concentrations of polyhedral silsesquioxanes. J. Dent. Biomech.
2010, 1 6.
Udita, S.M., Karthik, K.S., Sudhakara, V.M., 2010. Maxillofacial prostheric materials—past
& present trends. J. Acquir. Immune Defic. Syndr. 1 (2), 26 30.
Yu, R., Koran, A., Craig, R.G., 1980. Physical properties of maxillofacial elastomers under
conditions of accelerated aging. J. Dent. Res. 59 (6), 1041 1047.
Biomaterials for craniofacial
tissue engineering and
regenerative dentistry
24
Sukumaran Anil1, Elna Paul Chalisserry2, Seung Yun Nam2,3
and Jayachandran Venkatesan4
1
Department of Dentistry, Hamad Medical Corporation, Doha, Qatar, 2Interdisciplinary
Program of Marine-Biomedical, Electrical and Mechanical Engineering, Center for
Marine-Integrated Biomedical Technology (BK21 Plus), Pukyong National University,
Busan, South Korea, 3Department of Biomedical Engineering, Pukyong National
University, Busan, South Korea, 4Yenepoya Research Centre, Yenepoya University,
Mangalore, India
Chapter Outline
24.1 Introduction
644
24.1.1 Scaffolds for bone tissue engineering 645
24.1.2 Functions and features of scaffolds 646
24.1.3 Classification of biomaterials 646
24.2 Natural biomaterials
24.2.1
24.2.2
24.2.3
24.2.4
24.2.5
24.2.6
24.2.7
24.2.8
647
Collagen 647
Fibrin 648
Alginate 649
Silk 650
Hyaluronate 651
Chitosan 651
Agarose 653
Elastin 653
24.3 Synthetic biomaterials
654
24.3.1 Polyethyleneglycol 654
24.3.2 Poly-e-caprolactone 654
24.3.3 Polyglycolic acid 655
24.4 Bioceramics 655
24.4.1
24.4.2
24.4.3
24.4.4
Tricalcium phosphate 655
Hydroxyapatite 656
Tricalcium phosphate/hydroxyapatite biphasic ceramics (biphasic calcium phosphate) 657
Bioactive glasses 657
24.5 Metals 658
24.5.1 Biodegradable metal scaffolds 658
24.5.2 Titanium 659
24.5.3 Zirconia 660
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00025-6
Copyright © 2019 Elsevier Ltd. All rights reserved.
644
Advanced Dental Biomaterials
24.6 Bioactive restorative materials
661
24.6.1 Mineral trioxide aggregate 661
24.6.2 Biodentine 662
24.7 Three-dimensional printed scaffolds
24.8 Conclusion 664
References 664
24.1
663
Introduction
The craniofacial skeleton is complex and serves important functional demands.
Regeneration of craniofacial structures requires a sound understanding of complex
developmental processes, physiology, and the remodeling characteristics (Tevlin
et al., 2014). Regenerative tissue engineering deals with generating a biologic substitute capable of sustaining itself and integrating with functional native tissue from
living cells and biocompatible scaffolds. Cells, scaffolds, and growth-stimulating
signals are generally referred to as the tissue engineering triad, the key components
of engineered tissues (Chan and Leong, 2008). Scaffolds serve as space-holders,
provide a temporary support structure for the tissue that they are intended to
replace, create a substrate for cells to attach, grow, proliferate, migrate, and differentiate. They also serve as a delivery vehicle for cells and facilitate their retention
and distribution in the region where new tissue growth is desired (Hsu et al., 2013).
Biomaterials are generally used as biocompatible scaffold systems that allow for
the migration, proliferation, and differentiation of either resident or externally delivered cells, which are used to promote new bone formation. A wide variety of biomaterials have been used for craniofacial bone augmentation.
An ideal scaffold should be biocompatible, biodegradable, and their degradation
rates should match the healing rate of new tissues (Keane and Badylak, 2014; Jafari
et al., 2017). The various factors that contribute to tissue response by the scaffolds
are shape and size of the implant, chemical reactivity, the mechanism rate and byproducts of degradation, and ability of the material to promote cell material interactions (Schulte et al., 2000). Biodegradable and nonbiodegradable materials have
been utilized in bone tissue engineering. These materials should be chosen based on
their in vivo degradation rates with the idea that as the scaffold is degraded it
should gradually be replaced by newly formed tissue. When the biomaterials are
implanted in the body, cell biomaterial interactions depend on the surface characteristics of biomaterials such as chemical, topological, and macro microarchitectured conditions.
Naturally derived and synthetic scaffold materials have been used to exploit the
regenerative capacities of host tissues or transplanted cells. Scaffolds are defined as
three-dimensional porous solid biomaterials designed to perform some or all of
the following functions: (1) promote cell biomaterial interactions, cell adhesion,
and extra cellular matrix (ECM) deposition; (2) permit sufficient transport of
gases, nutrients, and regulatory factors to allow cell survival, proliferation, and
Biomaterials for craniofacial tissue engineering and regenerative dentistry
645
differentiation; (3) biodegrade at a controllable rate that approximates the rate of
tissue regeneration under the culture conditions of interest; and (4) provoke a minimal degree of inflammation or toxicity in vivo. The tissue engineered construct for
cartilage and bone repair and replacement poses a number of specific requirements
on scaffold materials including biocompatibility, osteoconduction or induction, temporary mechanical support, controlled degradation, and adequate interstitial fluid
flow (Elisseeff et al., 2005). Polymeric biomaterial scaffolds provide the structural
support for cell attachment and subsequent tissue development. The best scaffold
for an engineered tissue should imitate the (ECM) of the target tissue in its native
state. Nevertheless, the multiple functions, the complex composition, and the
dynamic nature of ECM in native tissues make it difficult to mimic exactly
(Giannitelli et al., 2014).
Bone grafts are selected based on its characteristics such as osteoinductiveness,
osteoconductiveness, mechanical stability, quality of transplantable bone, and preservation techniques. Osteoconductive grafts function as a scaffold for native bone
cells and stimulate progenitor cells to differentiate into osteoblasts. The application
of bone grafts is based on three biological drivers: the utilization of a bone graft
that will bring new bone-forming cells into the defect, the ability of the scaffold to
induce bone formation, and the presence of factors that may induce osteoblastic
proliferation and differentiation.
24.1.1 Scaffolds for bone tissue engineering
Bone tissue engineering utilizes scaffolds to deliver biofactors including cells,
genes, and proteins to generate bone, blood vessel formation and maturation into
the construct. The desirable characteristics of a scaffold for bone tissue engineering
should be three primary functions to ensure successful treatment of bone defects
(Arvidson et al., 2011).
1. Provide the correct anatomic geometry to define and maintain the space for tissue
regeneration.
2. Provide temporary mechanical load bearing within the tissue defect.
3. Enhance the regenerative capability of the chosen bio factor; a balance to a regenerative
capacity.
Achieving stiffness and strength equivalent to bone tissue requires minimally
porous scaffolds, whereas the enhanced delivery of biofactors requires highly connected porous scaffolds that allow cell migration, vascularization, and connective
tissue formation within scaffolds. The scaffold should fully integrate into the surrounding bone providing the initial three-dimensional (3D) structure which can
allow the cells to adhere, proliferate, differentiate, and lay down extracellular
matrix. A good scaffold is biocompatible, biodegradable, and porous for it to be
used for construction of a biological tissue. This means that even the breakdown
products of the scaffold should be nontoxic to the body. It should also be resorbable
to allow the growing bone to take its place gradually and it should have porous 3D
structures to accommodate implanted cells.
646
Advanced Dental Biomaterials
The scaffold for bone regeneration should accelerate osteoinductivity and
increase cell migration, proliferation, and release growth factors. Immune-potent
activity by such scaffolds is acceptable. Scaffold should have strong water uptake
and water-binding capacity as well as water delivery characteristics in order to
absorb the inflammatory mediators and cellular elements in its architecture, preserve them, and slowly deliver the beneficial growth factors and proinflammatory
mediators in order to provide an optimum environment during different stages of
bone healing (Moshiri and Oryan, 2012). Scaffold should have the capability to
align the callus and establish the continuity in the defect area. Assembling the
growth factors to tissue-engineered scaffolds results in enhanced healing capability
of the injured area (Oryan et al., 2013).
24.1.2 Functions and features of scaffolds
1. Architecture: Scaffolds should provide void volume for vascularization, new tissue formation, and remodeling so as to facilitate host tissue integration upon implantation.
2. Cyto and tissue compatibility: Scaffolds should provide support for either extraneously
introduced or endogenous cells to attach, grow, and differentiate during both in vitro culture and in vivo implantation.
3. Bioactivity: Scaffolds may interact with the cellular components of the engineered tissues
actively to facilitate and regulate their activities.
4. Mechanical property: Scaffolds provide mechanical and shape stability to the tissue
defect. The intrinsic mechanical properties of the biomaterials used for scaffolding or their
postprocessing properties should match that of the host tissue.
24.1.3 Classification of biomaterials
A scaffold material must adequately reproduce the physical and chemical properties
of natural bone in order to promote the attachment, proliferation, and differentiation
of both seeded osteoprogenitor cells and surrounding recipient tissues. The 3D
structure of a scaffold is of critical importance for the adequate bone development
and for the cellular interactions (Kale et al., 2000). An overwhelming variety of
substances are employed by researchers seeking to generate a scaffolding material
that possesses all the desired traits of an ideal scaffold.
Three individual groups of biomaterials—ceramics, synthetic polymers, and natural polymers—are used in the fabrication of scaffolds for tissue engineering. There
has been widespread use of ceramic scaffolds, such as hydroxyapatite (HA) and tricalcium phosphate (TCP), for bone regeneration applications. Ceramic scaffolds are
typically characterized by high mechanical stiffness, very low elasticity, and a
hard-brittle surface. From a bone perspective, they exhibit excellent biocompatibility due to their chemical and structural similarity to the mineral phase of native
bone. The interactions of osteogenic cells with ceramics are important for bone
regeneration as ceramics are known to enhance osteoblast differentiation and proliferation (Ambrosio et al., 2001).
Biomaterials for craniofacial tissue engineering and regenerative dentistry
647
Biomaterials can be classified broadly as natural biomaterials or synthetic
biomaterials.
Natural biomaterials can further be classified as protein-based biomaterials and
polysaccharide-based biomaterials.
G
G
Protein-based biomaterials include collagen, fibrin, and silk.
Polysaccharide-based biomaterials include chitosan (CS), alginate, and hyaluronan.
Synthetic biomaterials include polymer-based biomaterials, peptide-based biomaterials, and ceramic-based biomaterials.
G
G
G
G
Polymer-based biomaterials include PLGA and polyethyleneglycol (PEG).
Peptide-based biomaterials include short amino acids and self-assembling peptides.
Ceramic-based biomaterials include bioactive glass and hydroxyapatite.
Composite biomaterials.
Biomaterials used in tissue engineering and regeneration can be classified based
on their original sources into different categories:
G
G
G
G
Human-derived biomaterials such as human acellular dermal matrix;
Animal-derived biomaterials including processed bovine bone materials and porcinebased collagen membranes;
Other natural biomaterials such as polysaccharide-based biomaterials (cellulose, chitin/
CS);
Synthetic biomaterials such as polymers, composites, and ceramic-based dental
biomaterials.
24.2
Natural biomaterials
24.2.1 Collagen
Collagen is one of the two major components of the bone, making up 89% of the
organic matrix and 32% of the volumetric composition of bone (Kang et al., 2013).
Because of the biomimetic properties, collagen-based biomaterials are the most
highly investigated for bone regeneration (Stoppel et al., 2015; Glowacki and
Mizuno, 2008). Collagen provides strength and structural stability to tissues in the
body, such as the skin, blood vessels, tendon, cartilage, and bone. Native collagen
and denatured collagen (gelatin), alone or in combination with other natural and
synthetic polymeric fibers as well as ceramics, have been assessed for their inherent
scaffold characteristics (Kruger et al., 2013).
Collagen biomaterial has poor mechanical properties and swells readily when
implanted in vivo due to its high hydrophilicity. Therefore collagen is commonly
modified, cross-linked, or mixed with other components (polymers or ceramics) in
order to tailor the physicochemical and mechanical properties of the scaffold to the
requirements of the final application. Collagen is used mainly used in the forms
such as injectable hydrogels, membranes and films, sponges and scaffolds, and
micro nanospheres (Ferreira et al., 2012). The cross-linked collagen scaffolds can
648
Advanced Dental Biomaterials
exhibit minimal inflammatory as well as encapsulation responses and nonfibrotic
cellular growth (Ahmed et al., 2008). The major advantages of using collagen of
natural origin are its profusion, low index of immunological reaction, and its capacity to form fibers from soluble preparations which are similar to those found in natural tissues (Kadler, 2004). Collagen is resorbable with high swelling ability, low
antigenicity, cytocompatibility, and tissue regeneration potential (Abou Neel et al.,
2012).
Collagen-bioactive ceramic composites can be fabricated in many forms such as
3D scaffolds, hydrogels, or dry powders (Villa et al., 2015; Laydi et al., 2013;
Zhang et al., 2012). Collagen/CS/β-TCP (CCTP) based tissue engineering scaffolds were tested (Bian et al., 2016). In order to improve the regeneration ability of
scaffold, raloxifene-loaded poly lactic-co-glycolic acid (PLGA) microsphere was
embedded in the CCTP scaffold. To overcome the lack of neovascularization in
bone tissue engineering, cobalt ion-incorporated bioactive glass/collagen glycosaminoglycan (GAG) scaffolds were developed which enhanced the expression of vascular endothelial growth factor by stabilizing the hypoxia inducible transcription
factor (Quinlan et al., 2015). Induced pluripotent stem cell derived mesenchymal
stem cells cultured on collagen/hydroxy apatite (HAP)/CS nanofibers showed
enhanced osteogenic differentiation (Xie et al., 2015). A collagen network was
incorporated into porous calcium phosphate ceramic by vacuum infusion, which
was then coated with HAP by biomimetic mineralization. This three-level hierarchical CaP-collagen-HAP scaffold demonstrated better mechanical strength together
with rapid and greater bone formation than normal CaP scaffolds when implanted
ectopically in the dorsal muscles of rabbits (Zhou et al., 2014). Collagen CS gels
reinforced with bioactive glass nanoparticles exhibited thermosensitive behavior.
This gel can be injected in the body and is shown to have a great potential in bone
tissue engineering on account of its relative ease of use and minimal surgical procedure (Moreira et al., 2016). Collagen hydrogels have also been used to test the
ability of mesenchymal stem cells (MSCs) from different sources to undergo osteogenic differentiation (Schneider et al., 2010). Several other materials are incorporated
into collagen in order to enhance mechanical properties and enhanced bone matrix
interface strength. 3D collagen scaffolds were used to culture a wide variety of stem
cells for different tissue engineering applications.
24.2.2 Fibrin
Fibrin has captured the interest of bone tissue engineers due to its excellent biocompatibility, controllable biodegradability, and ability to deliver cells and biomolecules. Fibrin is one of the preferred biomaterials for tissue engineering applications.
Fibrin gels promote cell migration, proliferation, and matrix synthesis through the
incorporation of platelet-derived growth factors and transforming growth factor.
Fibrin is particularly appealing because its precursors, fibrinogen, and thrombin,
which can be derived from the patient’s own blood, enable the fabrication of
completely autologous scaffolds (Noori et al., 2017). Addition of fibrin may also be
used to enhance the behavior of cells on other natural polymers. Conjunction of
Biomaterials for craniofacial tissue engineering and regenerative dentistry
649
fibrin on CS/nano-β-TCP composites markedly improved cellular functions on scaffolds including MSC attachment, density, proliferation, differentiation, and mineralization (Siddiqui and Pramanik, 2015). Studies have shown that fibrin alone is
incapable of healing bone defects, and so, addition of other materials and/or biomolecules could yield better outcomes in tissue engineering (Linsley et al., 2016). The
combination of fibrin with osteoconductive ceramics that allows the incorporation
of growth factors, drugs, and metallic ions may enable the fabrication of multifunctional scaffolds to promote bone tissue remodeling (Kim et al., 2014). Hence fibrin
is an attractive biomaterial for bone tissue engineering because of its excellent
biocompatibility, biodegradability, intrinsic bioactivity, and other unique
characteristics.
24.2.3 Alginate
Alginate is a hydrogel comprising 1,4-linked b-D-mannuronic acid and a-L-guluronic acid, typically derived from brown seaweed and also bacteria. It has been extensively investigated and used for many biomedical applications, due to its
biocompatibility, low toxicity, relatively low cost, and simple gelation by addition
of divalent cations such as Ca21, Mg21, Ba21, and Sr21 (Wee and Gombotz,
1998). Alginate is a copolymer of D-mannuronic acid (M) and L-guluronic acid (G).
The gelation of alginate occurs as blocks of guluronic acid bound to other G blocks
via divalent cations, usually calcium ions (Wong, 2004). The modification of the
chemical structure of alginate by combining it with other biopolymers can further
extend the properties of this versatile material (Caterson et al., 2002). Alginate is
readily processable for 3D scaffolding materials such as hydrogels, microspheres,
microcapsules, sponges, foams and fibers, nanoparticles, and multilayers at physiological conditions ensuring the preservation of cell viability and function (Sun and
Tan, 2013).
Alginate allows efficient cell penetration into matrix and cell encapsulation. The
alginate/hydroxyapatite composite scaffolds were prepared by internal gelation followed by a freeze drying procedure to obtain a porous structure. The nanoparticles
can be prepared in the presence of a lactose-modified CS, which is adsorbed on the
scaffolds and can be used as temporary resorbable bone implants (Marsich et al.,
2013). Two different types of polymer scaffolds, that is, CS alginate and
CS alginate with fucoidan, were developed by a freeze drying method, and each
was characterized as a bone graft substitute (Venkatesan et al., 2014). CS alginate
hybrid scaffolds displayed improved mechanical strength and structural stability
and were shown to stimulate new bone formation and rapid vascularization.
Alginate microparticle and microfiber-aggregated scaffolds were produced through
the aggregation method. Such a porous structure allowed vascularization, oxygenation and cell migration, adhesion, and proliferation, which are biological events
that are fundamental for bone tissue regeneration (Valente et al., 2012).
An injectable and biodegradable scaffold based on oxidized alginate microbeads
encapsulating periodontal ligaments and gingival mesenchymal stem cells was found
to be a promising strategy for bone tissue engineering (Moshaverinia et al., 2012).
650
Advanced Dental Biomaterials
A high porosity composite scaffold comprising alginate, CS, collagen, and hydroxyapatite without chemical cross-linking agent was used as a scaffold for regenerating
bone tissue (Yu et al., 2013). Another composite comprising solid free-form fabricated polycaprolactone, bone morphogenetic protein (BMP-2), or bone formation
peptide, and alginate is used for bone tissue regeneration (Kim et al., 2013b). The
physicochemical and biological properties of hybrid materials fabricated from
photocross-linked gelatin, alginate, and gelatin/alginate-based hydrogels combined
with silica particles were studied by Lewandowska-Lancucka et al. (2017). It was
confirmed that the addition of silica particles to gelatin as well as gelatin/alginatebased matrices increased the elastic modulus values when compared to pristine
hydrogels and are promising candidates for bioactive scaffolds in tissue engineering.
One of the disadvantages of the material are the inability to control its degradation
rate in vivo and its low viscoelasticity, although this can be improved by increased
cross-linking or addition of other substances, such as HA (Yuan et al., 2011).
Alginate and alginate/HA mixtures have been used in bone and cartilage tissue engineering (Coluccino et al., 2016; Sarker et al., 2015; Wang et al., 2016).
24.2.4 Silk
Silk fibroin (SF) is a natural fibrous protein and has been shown to be a potential
biomaterial for a number of biomedical applications because of its excellent
biocompatibility, nontoxicity, diverse physical characteristics, and ability towards
cell attachment and proliferation. Silk, a natural polypeptide having very good biological properties either alone or in combination with other suitable materials, can
be fabricated as scaffolds for tissue engineering applications. SF films and fibers
exhibit good ability to support the adhesion and growth of various cells and hence
they are proposed as scaffolds for skin and bone regeneration (Ribeiro et al., 2018;
Li et al., 2018a). SFs are characterized as natural amphiphilic block copolymers
composed of hydrophobic and hydrophilic blocks which combine together to give
rise to the elasticity and toughness to SF (Zhang et al., 2009). Novel SF and carboxymethyl cellulose composite nanofibrous scaffold was developed to investigate its
ability to nucleate bioactive nano-sized calcium phosphate by biomineralization for
bone tissue engineering application. The developed scaffold has proved to be a
novel and excellent candidate for bone tissue engineering with significant improvement in physicochemical, mechanical, and biological properties in comparison to
the gelatin and pure SF nanofibrous scaffolds (Singh et al., 2016). SF/CS-based
magnetic scaffolds showed optimal characteristics such as superparamagnetic
behavior with decreased phosphate-buffered saline (PBS) uptake and degradation
and, hence, can be used for bone tissue engineering applications (Aliramaji et al.,
2017). Xie et al. (2016) developed novel bioscaffolds for bone regeneration, based
on the combination of SF and calcium polyphosphate (CPP). It was found that
Bombyx mori SF (BMSF) and Antheraea pernyi SF (APSF), prepared and applied
into CPP scaffolds with glutaraldehyde cross-linking forms of the BMSF/CPP and
APSF/CPP bioceramics, could be suitable for bone tissue engineering.
Biomaterials for craniofacial tissue engineering and regenerative dentistry
651
Silk, when mixed with hydroxyapatite, serves as a convenient material for bone
and dental tissue growth of extracellular matrix (Melke et al., 2016). Silk gel material is able to create a lasting 3D soft tissue augmentation; hence, it is useful in periodontal and maxillofacial therapies. Hexafluoroisopropanol (HFIP)-based silk is
slower in degradation and supports soft dental pulp formation better than aqueousbased silk. Tooth bud cells seeded on HFIP silk scaffolds, with or without incorporated arginine glycine aspartate (RGD) peptides, have been shown to form mineralized tissue indicating the usefulness of these scaffolds in osteodentine formation
(Zhang et al., 2011). Micron-sized silk fibers have been incorporated as a reinforcement in compact fiber composite to produce high strength biomaterial that would
serve as load bearing bone grafts. These have favored human bone derived stem
cells (hBMSC) differentiation and formation of bone-like tissue suggesting their
use for bone engineering applications (Mandal et al., 2012).
24.2.5 Hyaluronate
Hyaluronic acid (HA), a nonsulfated GAG, present in the extracellular matrix of
connective tissues offers excellent potential as a scaffold for tissue regeneration.
The poor mechanical strength and rapid in vivo degradation rate can be controlled
by cross-linking and chemical modification of the polymers (Ouasti et al., 2011).
Hyaluronic acid is capable of specific cell interaction via the CD4 receptor which
promotes wound healing and induces chondrogenesis. HA has been chemically and
physically incorporated into various tissue engineering scaffold matrices (Kim
et al., 2013a). Hyaluronic acid (HA) hydrogels have been widely applied in the biomedical field because of their good biocompatibility and structural diversity. They
possess some advantages, including facilitating proliferation of seeded cells and
wound healing, good antiinflammatory ability, and promoting intracellular signaling
(Collins and Birkinshaw, 2013). Porous hyaluronic acid scaffolds used for BMP-2
delivery for bone growth showed that the BMP-2 were continuously released for
controlled times in an active form from the scaffolds (Kim and Valentini, 2002).
Solid free-form fabrication of polylactic-co-glycolic acid grafted HA/PEG scaffolds
has successfully delivered BMP-2 in vivo with controllable release from the scaffold for up to a month. Histological analyses and staining after implantation in rats
revealed active bone regeneration, and the BMP-2 released from the scaffold was
thought to contribute in enhanced bone regeneration (Park et al., 2011). A composite of alginate and hyaluronic acid gel showed improved physical, mechanical, and
biological properties (Ganesh et al., 2013). The RGD peptides in hyaluronic acid
hydrogel enhance cellular attachment, cellular spreading, and proliferation.
Hyaluronic acid gels are injectable and hence serve as suitable scaffolds for pulp
regeneration (Inuyama et al., 2010).
24.2.6 Chitosan
CS a linear polysaccharide, derived from partial deacetylation of chitin, is a
highly versatile biomaterial from crustacean exoskeletons. CS evokes minimal
652
Advanced Dental Biomaterials
foreign-body response and fibrous encapsulation. CS is especially attractive as a
bone scaffold material as it supports the attachment and proliferation of boneforming osteoblast cells as well as the formation of mineralized bone matrix (Seol
et al., 2004). Pure CS is a suitable substrate for adhesion and proliferation of
osteoblasts as well as matrix formation and mineralization, but the strength and
structural stability of pure CS scaffolds is inadequate for bone tissue engineering
applications. Studies have shown that modified CS scaffolds exhibit osteoconductivity in vivo in surgically created bone defects (Muzzarelli et al., 1994). CS can
be processed in multiple ways to produce a variety of 3D scaffolds with different
pore structures for use in bone tissue engineering. It can also be combined with
different materials including ceramics and polymers to yield composite scaffolds
with superior mechanical and biological properties (Levengood and Zhang, 2014).
A major limitation in using CS as a standalone polymer for tissue engineering
applications is its faster degradation. To overcome this problem, usually CS is
either modified by adding other biocompatible polymers or by cross-linking with
suitable cross linkers. Blending other polymers/bioactive materials in CS matrices
resulted in functionally improved materials with respect to physicochemical and
biological properties, and hence, CS-based nanofibers have wide relevance for their
use in the field of bone tissue engineering (Balagangadharan et al., 2017). Modified
CS, such as imidazole-modified CS and methylpyrrolidinone CS, are osteoconductive in vivo thereby promoting bone regeneration in surgically created bone defects
(Kim et al., 2002). Importantly, CS is hydrophilic; that it should support adhesion
and proliferation of cells. In vitro studies have demonstrated that CS promotes the
adhesion and proliferation of osteogenic cells and mesenchymal stem cells.
Osteogenic cells cultured on CS deposit extracellular matrix which becomes mineralized to yield bone tissue. In addition, CS has also been implicated in promoting
osteogenic differentiation of mesenchymal stem cells (Yang et al., 2009; Mathews
et al., 2011).
CS combined with bioactive ceramics have a predominant role in bone tissue
engineering as these composites exhibit tailored physical, biological, and mechanical properties favorable for bone regeneration as well as predictable degradation
behavior. The presence of micro- or nanoscale calcium phosphate particles in CS
scaffolds provides important functionalities, but the incorporation or immobilization
of a second or even third functional component can further improve bone tissue
engineering scaffolds’ structural stability and osteogenic response and thereby its
clinical use. The incorporation of nanohydroxyapatite (nHAp) in the CS matrix by
in situ nucleation in the presence of its precursor would provide distinct nanophase
distribution of HAp particles and also improve the mechanical strength of the composite compared to simple mixing of nHAp in CS. In the case of fibrous scaffolds,
addition of binders or synthetic polymers helps in the easy incorporation of nHAp
into the organic solution (Shalumon et al., 2013; Wang et al., 2014). CS/nHAp prepared by cross-linking with glutaraldehyde when implanted to the calvarial bone
defect showed new bone formation which was histologically confirmed as bioactive
and neovascularized (Ma et al., 2011).
Biomaterials for craniofacial tissue engineering and regenerative dentistry
653
Composite CS scaffolds, which incorporate other biocompatible polymers and/or
micro- or nanoscale calcium phosphates, usually possess mechanical and biological
properties superior to pure CS scaffolds. Mesenchymal stem cells introduced into a
defect site may either actively participate in bone formation by synthesizing mineralized matrix or secrete trophic factors that activate endogenous cells. Heparin can
be immobilized on CS scaffolds as a way to exploit naturally occurring noncovalent
interactions between growth factors and extracellular matrix components.
24.2.7 Agarose
Agarose is a natural polysaccharide polymer having unique characteristics that give
reason to consider it for tissue engineering applications. It is one of the two principal components of agar and is purified from agar by removing agaropectin. Due to
their soft tissue like mechanical properties and biocompatibility, agarose gels have
been investigated as potential scaffolds for neural and cartilage tissue engineering
(Zarrintaj et al., 2018). Hydroxyapatite agarose composites accelerate the new bone
formation more than pure HA (Iwai et al., 2015). Biomimetic scaffold containing
agarose and nHAp was used with dental pulp stem cells and periosteal stem cells to
regenerate the bone (Annibali et al., 2013). Biodegradable, biocompatible, and
injectable gel based on HA/agarose was developed for orthopedic, oral, and maxillofacial surgery (Watanabe et al., 2007).
24.2.8 Elastin
Elastin is a key structural protein in extracellular matrix of all mammals which is
responsible for the elastic action of various tissues in the body. Tropoelastin is the
secreted soluble precursor of elastin. Although less abundant than collagen, elastin
is present in large amounts within highly elastic tissues (Muiznieks and Keeley,
2013). Incorporation of elastin in biomaterials is especially significant when its
elasticity or biological effects can be exploited. Major structural contributors to vertebrate ECM are the fibrous proteins collagen and elastin. Collagen provides tissues
with essential tensile strength, enabling resistance to plastic deformation and rupture, while elastin imparts the properties of extensibility and reversible recoil,
enabling tissues to withstand repetitive mechanical stress (Gosline et al., 2002;
Rauscher and Pomes, 2012). Elastin can also be conveniently used in association
with collagen for tissue engineering applications. Rapid growth of preosteoblast
cells was demonstrated in a novel elastin-like polypeptide (ELP) -collagen composite material prepared in the hydrogel form for bone tissue engineering (Amruthwar
and Janorkar, 2013). Porous polycaprolactone scaffolds impregnated with bovine
elastin demonstrated improved mechanical and biological responses (Annabi et al.,
2011). Chondrocytes cultured on coacervated or enzymatically cross-linked ELP
hydrogels were shown to promote chondrogenesis in vitro (Betre et al., 2006).
654
24.3
Advanced Dental Biomaterials
Synthetic biomaterials
24.3.1 Polyethyleneglycol
PEG, also known as polyethylene oxide or polyoxyethylene, is the most commercially important polyether. Polyethers are oligomers or polymers of ethylene oxide.
PEG is a synthetic polymer and offers the advantages of nontoxicity, biocompatibility, low immunogenicity, and ability to undergo in vivo degradation. It is resistant
to cellular and protein adsorption and thereby reduces recognition by immune system and its rejection. In its hydrogel form, it has been widely tested as a scaffold
material for tissue regeneration. PEG hydrogel modified with cell adhesion RGD
peptides improves cell adhesion, cell survival, and matrix synthesis within the 3D
scaffold network (Burdick and Anseth, 2002).
This polymer can also help to seal cell membranes after injury, making it useful
for avoiding cell death. Hydrophilic PEG hydrogels can be made through a variety
of cross-linking schemes to develop scaffolds with different degradation as well as
release rates. The mechanical strength of PEG hydrogel is determined by the molecular weight, cross-linking, and concentration of polymers. By adding cell binding
motifs like RGD peptides into the PEG hydrogel network, cell adhesion can be considered as a crucial feature of PEG-based hydrogel (Lee et al., 2015). PEG has been
used in regeneration of several tissues, including spinal cord/nerve, cardiac tissue,
bone, and skin (Engebretson and Sikavitsas, 2012). Properties such as good biocompatibility, nonimmunogenicity, resistance to protein adsorption, and cell adhesion of
PEG have made them more suitable hydrophilic polymers in biomedical applications including bioconjugation, surface modification, drug delivery, and tissue
engineering (Zhu, 2010). Bioactive molecules such as cell adhesion ligands,
enzyme-sensitive peptides, and growth factors have been incorporated into PEG
hydrogels, to simulate one or more ECM biofunctions such as cell adhesion, proteolytic degradation, and growth factor-binding.
24.3.2 Poly-e-caprolactone
Poly-e-caprolactone (PCL) is a semicrystalline material with good mechanical properties. PCL belongs to a family of poly(α-hydroxyl esters) and is one of the most
widely used biodegradable polyesters for medical applications because of its
biocompatibility, biodegradability, and flexibility (Lin et al., 1999). PCL scaffolds
were used in bone tissue engineering, either alone or combined with hydroxyapatite
(HA) (Weisgerber et al., 2018). PCL scaffolds are excellent in longer term use as
they degrade over 2 years (Pitt et al., 1981). Compared with other polyesters, PCL
has slower degradation kinematics and the degradation products are harmlessly
metabolized via the tricarboxylic acid cycle (Woodward et al., 1985). Scaffolds fabricated using PCL are more resistant to hydrolysis, and consequently are capable of
supporting the viability, proliferation, and differentiation status of encapsulated
cells. The mechanical and degradation characteristics of PCL facilitate long-term
in vitro cell culture before implantation into sites of injury. PCL scaffolds thus
maintain structural integrity during the in vitro culture period, while MSCs
Biomaterials for craniofacial tissue engineering and regenerative dentistry
655
differentiate and synthesize cartilaginous matrix. The electrospinned PCL nanofibrous scaffold supported multilineage differentiation of the human MSCs when cultured under a specific, differentiation-promoting culture condition (Yoshimoto
et al., 2003). Electrospun composite scaffolds, made from PCL/gelatin/nHAp and
PCL/gelatin, enhanced cell proliferation and odontogenic differentiation. It was
shown that the PCL/HAp scaffold supported growth and osteogenic differentiation
of all cells, suggesting the potential of 3D porous PCL/HAp scaffold as a good candidate material for bone tissue engineering (Chuenjitkuntaworn et al., 2016).
24.3.3 Polyglycolic acid
Polyglycolic acid (PGA) is a rigid, thermoplastic, highly crystalline, aliphatic polyester, made by a ring-opening polymerization reaction of a cyclic glycolide. PGA is
preferred in medical applications because its degradation products, lactic and glycolic acids, are biological metabolites. PGA has outstanding properties; however, its
low solubility in organic solvents, faster degradation, and the high acidity of its
degradation products have limited its biomedical applications (Nair and Laurencin,
2007). Though PGA has several applications in tissue engineering, its softness and
inability to hold space make it less preferred in craniofacial defect repair.
24.4
Bioceramics
Bioceramics have attracted great attention in the field of bone tissue engineering.
Bioceramics are fully, partially, or noncrystalline ceramics that are designed for the
regeneration and reconstruction of diseased parts of the body. Bioceramics can create strong bonds to tissues, thereby stimulating osteogenesis and improving bone
graft incorporation and osseointegration (Baino et al., 2015). The dissolution rate
and tissue interaction are influenced by the characteristics such as the composition,
crystallinity, particle size, and porosity which can be controlled during the processing of the bioceramics (Valerio et al., 2004). Current forms of application in clinical use include solid blocks, powders, and granules for bone filling, coatings on
metal joint prostheses, injectable formulations, and porous scaffolds.
24.4.1 Tricalcium phosphate
The major representatives of this class are calcium phosphates that are among the
most widely used crystalline ceramics for bone tissue regeneration. This is due to
their exceptional properties that include (1) similarity, in terms of structure and
chemical composition, to the mineral phase of bone, and (2) osteoconductivity, that
is, the ability of providing a biocompatible interface along with bone migrates, and
thus allows bonding to the host tissue without the formation of scar tissue
(LeGeros, 2002). They are used in the form of porous ceramic pieces and granules
to reconstruct all kinds of bone defects, from augmentation of alveolar ridge defects
after a tooth extraction and before implant positioning to sinus reconstruction
656
Advanced Dental Biomaterials
correction of various deformities and bone reconstruction following injury or disease (Liu and Lun, 2012).
24.4.2 Hydroxyapatite
Hydroxyapatite has been used for a variety of biomedical applications, including
matrices for drug release control and bone tissue engineering materials (Ginebra
et al., 2006). Although the synthetic and natural HA differ in terms of physical
microstructure, crystal size, and porosity, chemical similarities to bone, in both
forms, account for the osteoconductive potential of HA (Fig. 24.1) (Ramesh et al.,
2018). When compared to β-TCP, HA resorbs slowly and undergoes a little conversion to a bone-like material after implantation. There have been efforts toward
developing HA-based bioceramic materials that have been doped with ions.
Strontium-HA, magnesium-HA, and silicon-HA have been tested to improve
mechanical and biological properties for bone tissue engineering applications (Li
et al., 2018b; Panzavolta et al., 2018; Andres et al., 2018). HA is commonly used
for bone repair, bone augmentation, as well as coating of implants. The low
mechanical strength of normal HA ceramics restricts its use mainly to low loadbearing applications. To overcome these limitations nanocrystalline HA was
Figure 24.1 3D-printed scaffold designs using synthetic biomaterials. 3D, Threedimensional.
Biomaterials for craniofacial tissue engineering and regenerative dentistry
657
developed which showed improved sinterability and enhanced densification due to
greater surface area (Zhou and Lee, 2011).
24.4.3 Tricalcium phosphate/hydroxyapatite biphasic ceramics
(biphasic calcium phosphate)
The biphasic calcium phosphate (BCP) concept is based on an optimum balance
between the more stable phase (HA) and the more soluble phase (β-TCP). β-TCP is
more rapidly replaced by bone than the hardly degradable HA, owing to its higher
solubility (Petrov et al., 2001). Upon degradation of β-TCP through a process of
dissolution and absorption, a normal bone structure in the regenerated bone can be
achieved (Von Arx et al., 2001). The development of BCP ceramics (i.e., containing
both HA and β-TCP) has provided materials in which bioactivity and degradation
are controlled based on the ratios of the components (LeGeros et al., 2003). Several
studies have shown that BCP granules have excellent biocompatibility and bioactivity and lead to new bone formation and degradation of the biomaterial (Valimaki
et al., 2005). The rate of degradation or resorption of HA/TCP ceramics can be
accelerated by increasing the amount of the more soluble phase, TCP. Studies have
shown that BCPs with higher β-TCP ratio are expected to yield more replacement
of biomaterial by new bone (Daculsi et al., 1990; Gauthier et al., 1998). BCP compounds containing approximately 60% of HA and 40% of β-TCP seemed to provide
the optimal bone conductive properties (Rouvillain et al., 2009). Nery et al. (1992)
reported optimal bone regeneration in surgically created bone defects with BCP
containing HA/β-TCP ratio of 85/15. However, recently BCP products containing
higher β-TCP ratios (BCP 60/40 and BCP 20/80) have been studied in prospect of
its enhanced osteoconductive effect (Yang et al., 2014; Lee et al., 2013).
24.4.4 Bioactive glasses
Bioactive glasses and glass ceramics, which are used in bone repair, are another
type of bioceramics containing Ca, P, and Si ions with good mechanical strength.
The original bioglass composition is 45% silica (SiO2), 24.5% calcium oxide
(CaO), 24.5% sodium oxide (Na2O), and 6% phosphorous pentoxide (P2O5) in
weight percentage (Hench and Wilson, 1984). Bioglasses are biocompatible, osteoconductive, and depending on their processing condition offer a porous structure
which promotes their resorption and bone ingrowth (De Aza et al., 2003). Bioglass
does not induce an inflammatory response, and the silica-based bioglass completely
degrades in 6 months. Silicon has been found to promote differentiation of mesenchymal cells and bone formation. The SiO2 in combination with apatite is responsible for the inhibition of fibroblast proliferation at the bioimplant surface (Nandi
et al., 2009). The borate-based bioglasses showed a faster degradation than silicabased bioglasses, but this degradation rate can be controlled by adjusting its composition. The phosphate-based bioglasses are a promising group of bioglasses for hard
and soft tissue engineering, since their solubility can be controlled by manipulating
658
Advanced Dental Biomaterials
the composition (Knowles, 2003). Bioglasses are quite brittle and present low
mechanical strength and decreased fracture resistance. Thus their utilization should
be selective or in association with other bone substitutes. Future research can be
directed toward incorporating various other trace elements such as Zn, Cu, F, Mn,
Sr, and B. These individual elements have been known for their osteogenic property
and their incorporation in the compositional flexible glasses make them promising
bioactive materials (Rahaman et al., 2011).
24.5
Metals
Several metals are used in craniofacial repair and regeneration. Metals currently in
use clinically include gold, stainless steel, cobalt chromium, and titanium. Most of
the metals are inert alloplasts which won’t integrate with adjacent tissues or induce
new bone formation. Pure titanium and some of its alloys are widely used as
implant materials under load-bearing conditions in dentistry and orthopedics.
Metals have been long used especially in load-bearing areas in the oral cavity. They
are used as implants to replace lost teeth, reconstruction posttrauma/cancer as
plates, mesh, or screws.
24.5.1 Biodegradable metal scaffolds
Biodegradable metal scaffolds have shown an interesting mechanical property that
was close to that of human bone with tailored degradation behavior. Metals that can
degrade in the physiological environment, namely, biodegradable metals, are proposed as potential materials for hard tissue scaffolding. These biodegradable metals
may have superior mechanical properties in comparison to biodegradable polymers
(Yusop et al., 2012; Yazdimamaghani et al., 2017). Metals that degrade in the physiologic environment, such as magnesium alloys possessing mechanical properties
that are very similar to those of bone, yet retain the ability to naturally degrade
when placed within an aqueous type of environment, are considered promising
scaffolds (Staiger et al., 2006). The porous architecture of Mg scaffold has been
proven to play a significant role in cell growth and proliferation. Efforts to design
polymer magnesium composites are ongoing. Theoretically, the polymer matrix
benefits from magnesium incorporation, as magnesium may confer higher mechanical
strength and fracture toughness while the polymer may prevent premature degradation
(Mantripragada et al., 2013).
Porous Fe and Fe-phosphorous alloys have been investigated as biodegradable
bone replacements, and the results showed that addition of phosphorus increased
compressive strength higher than that of pure Fe which is comparable to that of typical bone (Hermawan et al., 2010). These alloys showed also faster in vitro degradation than pure Fe, hence alloying Fe with phosphorous seems to be a promising
way to optimize both mechanical and degradation properties of Fe, especially for
bone scaffold (He et al., 2016).
Biomaterials for craniofacial tissue engineering and regenerative dentistry
659
Metallic nanoparticles have been incorporated into scaffolds with evidence of
increased mechanical strength, increased cellular adhesion of osteoblasts and chondrocytes, and increased long-term osteoblast function, with notable improvements
in collagen synthesis, alkaline phosphatase activity, and calcium deposition (Kim
and Fisher, 2007; Tran and Webster, 2011). Biodegradable metals as tissue scaffolding materials have been viewed as alternative to polymers for hard tissue regeneration exploiting mostly their superior mechanical properties over biodegradable
polymers.
24.5.2 Titanium
Titanium is the most biocompatible and corrosion-resistant metal, its elasticity modulus corresponds to the elasticity modulus of the bone, and hence it is widely used
in dentistry and orthopedics. Titanium and some titanium alloys are better received
by human tissue when compared to the receptivity of other metal materials.
According to the American Society for Testing and Materials, six types of titanium
are listed as implant biomaterials. Depending on the various concentration of oxygen, nitrogen, hydrogen, iron, and carbon influencing the physical and mechanical
properties, there are four grades of commercially pure titanium (cpTi) (Grades
I IV) and two titanium (Ti) alloys (Grades V and VI)—Ti 6Al 4V and
Ti 6Al 4V extra low interstitial alloys (Özcan and Hämmerle, 2012). Grades I
and II are the most commonly used cpTi types for the production of metal ceramic
fixed dental prosthesis. In cases where good mechanical characteristics are required,
such as in bone screws and plates, Ti 6Al 4V alloy is being used (Özcan and
Hämmerle, 2012; De Viteri and Fuentes, 2013). A superficial layer of titanium
oxide that develops on the surface is responsible for corrosion-resistance as well as
for the adhesion of glycoproteins in vivo, which is important for the biocompatibility. This oxide layer is maintained at physiological pH resisting ion formation tendency and has low reactivity with macromolecules making it highly resistant to
corrosion (Sidambe, 2014).
Osseointegration, a direct structural and functional connection, anchors the titanium dental implant with bone (Le Guehennec et al., 2007). Surface chemistry,
topography, wettability, charge, surface energy, crystal structure, crystallinity,
roughness, chemical potential, strain hardening, the presence of impurities, thickness of titanium oxide layer, and the presence of metal and nonmetal composites
play a role in implant tissue interaction and osseointegration (Anil et al., 2011).
Various approaches are employed to make implants more biomimetic from both
biomechanical and biological perspectives. Alteration in titanium surface morphology is used to influence osteoblast attachment, differentiation, proliferation, and
migration. Altering the macro-, micro-, and nanoscale surface topographies through
plasma spraying, particle blasting, micromachining, grinding, polishing, and chemical methods such as acid etching, alkali etching, and anodization have resulted in
higher bone implant contact (BIC) ratio and improved osseointegration (Subramani
et al., 2018).
660
Advanced Dental Biomaterials
Biochemical binding to bone can be achieved by coating with chemicals or biomaterials such as ceramics and polymers that are known to improve osteogenic
properties. An in vivo study using micro arc oxidation method in phosphoric acid
on titanium implants facilitated more chemical bonding sites for calcium ions during mineralization (Sul et al., 2002). Hydroxyapatite coating through various methods has shown precipitation of biological apatite nanocrystals with the
incorporation of various proteins, which, in turn, promote cell adhesion, differentiation into osteoblast, and the synthesis of mineralized collagen, the extracellular
matrix of bone tissue (Lavenus et al., 2010). Attempts have been made to improve
and accelerate osseointegration by introducing bioactive factors such as known
osteogenic drugs, antiinflammatory mediators, and growth factors to titanium surfaces. The effects of recombinant bone morphogenetic protein-2 (rhBMP-2) on the
osseointegration of titanium implants have shown positive influences in experimental animal studies (Wikesjö et al., 2002). Tetracycline-HCl, an antimicrobial agent,
kills microorganisms that may be present on the contaminated implant surface.
Further, it inhibits collagenase activity and increases cell proliferation as well as
attachment and bone healing (Herr et al., 2008). Oral administration of drugs such
as simvastatin have proved to have a positive impact on osteogenesis; hence, Yang
et al. (2011), when studying the effect of simvastatin-loaded porous implant surfaces, demonstrated accelerated osteogenic differentiation of preosteoblasts.
However, there are esthetic issues due to the gray color of titanium so that in areas
where soft tissue is not optimal, the dark color shines through the thin mucosa,
which has led to the pursuit of esthetic replacements to titanium (Saini et al., 2015).
Titanium foams fabricated by a new powder metallurgical process have bimodal
pore distribution architecture, mimicking natural bone. The mechanical properties
of the titanium foam with low relative densities of approximately 0.20 0.30 are
close to those of human cancellous bone (Wen et al., 2011). The titanium foam
after a simple thermochemical pretreatment process followed by immersion in a
simulated body fluid showed good ability to form a bone-like apatite layer throughout the foam. The thermochemical pretreatments for inducing bone-like apatite formation are attractive due to their simplicity, cost savings, and effectiveness (Kapat
et al., 2017). The titanium foams are anticipated to be promising implant materials
for bone tissue engineering applications due to their excellent biomechanical properties and bioactivity.
24.5.3 Zirconia
Zirconia, a tooth-colored material, was first introduced as endosseous implants for
bone regeneration to replace mainly the impaired esthetic outcomes of dark grayish
color of titanium, visible through the periimplant mucosa. These include unfavorable soft tissue conditions such as thin mucosal biotype, gingival recession, and/or
in the anterior maxillary or mandibular incisor replacements. It was also claimed
that ceramic implants could manage soft tissue better due to less plaque accumulation than titanium (Ozkurt and Kazazoglu, 2011; Hoffmann et al., 2008). Zirconium
implants show lower inflammatory response and increased angiogenic factors
Biomaterials for craniofacial tissue engineering and regenerative dentistry
661
compared to titanium (Degidi et al., 2006). Zirconium dioxide in its pure phase is
unstable and brittle with low shear strength. Hence, to improve the modulus of elasticity and stabilize the material, small amounts of aluminum oxide or yttrium oxide
are added through the hot isostatic pressing method. Such additions also improve
the toughness and crack propagation property. Of the two oxides, yttrium (yttriumstabilized tetragonal polycrystals) appears to offer improved advantages owing to
its higher fracture resilience and higher flexure strength (Saini et al., 2015;
Sennerby et al., 2005).
Zirconium is used as an implant material by itself and zirconia particles as a
coating material on titanium dental implants are also explored (Ozkurt and
Kazazoglu, 2011). Huang et al. (2018) concluded that plasma-sprayed nanostructured-zirconium coating showed hierarchical surface morphology with better surface roughness and wettability than titanium implants. Histological analysis
exhibited earlier and more condensed bone formation improving the BIC and
thereby the osseointegration. Currently the majority of zirconium implants are produced as one-system implants. While microgaps between an implant and abutment
is absent in such systems, the use of angular abutments to correct misalignment or
secondary corrections to alter shape or vertical height is not possible as it may
affect the fracture strength of zirconia (Cionca et al., 2017). Two-piece implant systems with screw-retained abutments are desirable for several reasons, although they
are technically challenging because of the limitations of zirconia (Preis et al.,
2016).
The early failure rates of the zirconia implant systems developed and tested so
far were generally higher compared with titanium implants. Technical failure as a
result of fracture of the material is a sensitive issue and a critical factor for usability
and acceptance in daily practice (Elnayef et al., 2017; Cionca et al., 2017).
24.6
Bioactive restorative materials
The bioactivity of the dental restoratives is an important feature in the preservation
of the hard dental tissues; therefore it is of utmost significance to find a material
which can be used to decrease the amount of excavated dentine during preparation
of the tooth. Several materials have been used as possible dentine substitutes in
repairing teeth damaged by caries. Materials with clear bioactive properties seems
to be the ideal solution for this application. Bioglasses have been accepted as mineralizing agents in caries prevention, as well as desensitizing agents in the treatment
of hypersensitive teeth caused by opened dentinal tubules (Gjorgievska et al.,
2012).
24.6.1 Mineral trioxide aggregate
Mineral trioxide aggregate (MTA) is a biomaterial that has been investigated for
applications in restorative dentistry. Its multiple applications include direct and
662
Advanced Dental Biomaterials
indirect pulp capping, formation of apical plug, root-end filling, perforation
repair, furcation repair, repair of resorptive defects, and management of immature
apices (Rajasekharan et al., 2014). The main components of MTA are tricalcium
oxide, tricalcium silicate, bismuth oxide, tricalcium aluminate, tricalcium oxide,
tetracalcium aluminoferrite, and silicate oxide. In addition, there are a few other
mineral oxides, which are responsible for the chemical and physical properties
of MTA. Studies revealed that MTA materials are biocompatible with an
acceptable in vivo biologic performance when used for root-end fillings, perforation repairs, pulp capping and pulpotomy, and apexification treatment (Roberts
et al., 2008).
24.6.2 Biodentine
Biodentine (BD), a new calcium silicate-based material, has been introduced as a
dentine substitute to repair the damaged dentine. BD has a wide range of applications including endodontic repair (root perforations, apexification, resorptive
lesions, and retrograde filling material in endodontic surgery) and pulp capping and
can be used as a dentine replacement material in restorative dentistry. BD was originally developed for use in direct and indirect pulp capping as a single application
dentine substitute without any cavity conditioning treatment. Biological studies of
this material indicated that it may be safely applied directly to the pulp, since it
induces the formation of a dentine-like matrix (Laurent et al., 2008). It was also
confirmed that BD can be used as a dentine substitute under a composite for posterior restoration (Koubi et al., 2013).
BD can be used as a direct posterior restorative material. The modified composition of the powder, the addition of setting accelerators and softeners, and a new
predosed capsule formulation for use in a mixing device have largely improved
the physical and handling properties of this material (Wang et al., 2011). The
cement has a faster setting time than other related materials and also higher compressive strength. The components of BD are provided in the form of a capsule
containing a powder and an ampule containing a liquid, which are combined by
adding the liquid to the capsule and mixing with an amalgamator. According to
the manufacturer, the setting time of BD is short, between 9 and 12 minutes,
owing to the addition of an accelerator (CaCl2) to the liquid. The push-out bond
strength of BD is similar to that of MTA (Alsubait et al., 2014). It also has excellent color stability (Valles et al., 2013) and is, therefore, more preferred than
MTA for use in anterior teeth. Furthermore, similar to MTA, BD shows complete
dentine bridge formation when used for pulp capping (Nowicka et al., 2013).
Bioactive and biocompatible characteristics of the material were confirmed. BD
when placed directly in contact with the pulp showed enhanced proliferation,
migration, and adhesion of human dental pulp stem cells (Luo et al., 2014).
Considering the superior physical and biologic properties, BD could be used in
the field of endodontics, dental traumatology, restorative dentistry, and pediatric
dentistry.
Biomaterials for craniofacial tissue engineering and regenerative dentistry
24.7
663
Three-dimensional printed scaffolds
3D printing provides a platform that helps to fulfill the hallmarks of tissue engineering, namely, rehabilitation, reconstruction, and regeneration. The technique allows
construction of individualized, patient-specific bone substitutes (Bauermeister et al.,
2016). The complexity and the multicellular interactions of the craniofacial structures can be managed by the application of 3D-printed scaffolds. 3D printing is fundamentally based on the additive manufacturing technology where a 3D construct is
fabricated by adding materials layer by layer. Computed tomography, magnetic resonance imaging, or X-rays are used to create a patient’s specific scaffolds. 3D bioprinting promises precise printing of various biomaterials (bio-ink) with complex
3D architectures, while being able to use multiple cell sources simultaneously and
being customizable to patient-specific needs (Fig. 24.2). Various classes of bio-inks
(polymer hydrogels, inert metals, ceramics, composites, and cell aggregates) may
be used for 3D biomanufacturing of scaffolds to replace damaged tissue, guide in
reconstruction through fixation devices, screws, custom cutting guides, as well as to
create craniofacial tissue analogs for tissue regeneration. Based on the underlying
printing principles, bioprinting can be classified into inkjet-based, extrusionassisted, and laser-assisted (Obregon et al., 2015; Nyberg et al., 2017; Derby,
2012). Depending on the biomaterial properties, the appropriate bioprinting system
is selected. Inkjet 3D printers are capable of applying low-viscosity bio-inks using
a thermal or piezoelectrical controlling system; laser-assisted printers can print cell
Figure 24.2 Examples of various shapes of bioceramics for bone engineering applications:
cylinder, block, root form, and granules as bone fillers.
664
Advanced Dental Biomaterials
and biomaterial sources with various viscosities using laser source; and extrusion
printers extrude high-viscosity and stiff polymeric sources at high temperatures
(Amrollahi et al., 2016).
Bone and cartilage regeneration can be achieved through scaffolds from
extrusion-based printing systems as these areas demand high load bearing properties. In a clinical trial, bioprinted PCL tooth-shaped plugs have shown significant
improvement in alveolar preservation (Goh et al., 2015). The possibility of combining two classes of materials, such as calcium sulfate hydrate and bioactive glass,
was proven by Qi et al. Both in vitro and in vivo studies showed improved osteogenesis and thereby enhanced bone formation in calvarial defects (Qi et al., 2017).
In the craniofacial region, the periodontal complex represents multiple tissues
both soft and hard. Hence multiphase 3D printing using a composite (PCL-HA)
with spatiotemporal arrangement and precise delivery of growth factor and BMP-2
led to the differentiation of distinctive progenitor cells of putative dentin/cementum,
periodontal ligament (PDL), and alveolar bone complex (Lee et al., 2014). Similar
attempts with biphasic scaffolds, cells, and gene delivery with tunable mechanical
properties within the scaffold have been attempted in efforts toward bioengineering
a whole tooth (Kim et al., 2010; Ikeda et al., 2009; Zhang et al., 2010). 3D-printed
Grade V titanium dental implant with a novel dual-stemmed design, when tested in
rabbits against conventional manufactured steel implants, showed better osteogenesis and comparable biocompatibility (Tedesco et al., 2017). Such advances promise
more avenues for 3D printing in craniofacial regeneration.
24.8
Conclusion
Craniofacial reconstruction has undergone tremendous expansion since the inception of the concept of tissue engineering. Various materials such as metals, ceramics, natural and synthetic polymers, and even their composites have been explored
as scaffolds to promote maxillofacial tissue regeneration. The progress in this field
is taking several routes, including cell biology, the development of novel scaffolds,
fabrication methods, and characterization techniques. Regenerating maxillofacial
structures is challenging and requires the recapitulation of the biological development of several tissues and interfaces. Stem cell therapy and engineering of irreversibly damaged tissues is progressing toward a reality. Further research should be
focused on the development of materials which promote rapid tissue regeneration;
the development of processing methods to give scaffolds with designed architecture;
and the delivery of therapeutic molecules, such as antibiotics and growth factors.
References
Abou Neel, E.A., Salih, V., Revell, P.A., Young, A.M., 2012. Viscoelastic and biological
performance of low-modulus, reactive calcium phosphate-filled, degradable, polymeric
bone adhesives. Acta Biomater. 8, 313 320.
Biomaterials for craniofacial tissue engineering and regenerative dentistry
665
Ahmed, T.A., Dare, E.V., Hincke, M., 2008. Fibrin: a versatile scaffold for tissue engineering
applications. Tissue Eng. Part B Rev. 14, 199 215.
Aliramaji, S., Zamanian, A., Mozafari, M., 2017. Super-paramagnetic responsive silk fibroin/
chitosan/magnetite scaffolds with tunable pore structures for bone tissue engineering
applications. Mater. Sci. Eng. C Mater. Biol. Appl. 70, 736 744.
Alsubait, S.A., Hashem, Q., Alhargan, N., Almohimeed, K., Alkahtani, A., 2014.
Comparative evaluation of push-out bond strength of ProRoot MTA, bioaggregate and
biodentine. J. Contemp. Dent. Pract. 15, 336 340.
Ambrosio, A.M., Sahota, J.S., Khan, Y., Laurencin, C.T., 2001. A novel amorphous calcium
phosphate polymer ceramic for bone repair: I. Synthesis and characterization. J.
Biomed. Mater. Res. 58, 295 301.
Amrollahi, P., Shah, B., Seifi, A., Tayebi, L., 2016. Recent advancements in regenerative
dentistry: a review. Mater. Sci. Eng. C Mater. Biol. Appl. 69, 1383 1390.
Amruthwar, S.S., Janorkar, A.V., 2013. In vitro evaluation of elastin-like polypeptide-collagen composite scaffold for bone tissue engineering. Dent. Mater. 29, 211 220.
Andres, N.C., Sieben, J.M., Baldini, M., Rodriguez, C.H., Famiglietti, A., Messina, P.V.,
2018. Electroactive Mg(2 1 )-hydroxyapatite nanostructured networks against drugresistant bone infection strains. ACS Appl. Mater. Interfaces 10, 19534 19544.
Anil, S., Anand, P., Alghamdi, H., Jansen, J., 2011. Dental implant surface enhancement and
osseointegration. Implant Dentistry—A Rapidly Evolving Practice. InTech.
Annabi, N., Fathi, A., Mithieux, S.M., Martens, P., Weiss, A.S., Dehghani, F., 2011. The
effect of elastin on chondrocyte adhesion and proliferation on poly(varepsilon-caprolactone)/elastin composites. Biomaterials 32, 1517 1525.
Annibali, S., Cicconetti, A., Cristalli, M.P., Giordano, G., Trisi, P., Pilloni, A., et al., 2013. A
comparative morphometric analysis of biodegradable scaffolds as carriers for dental pulp
and periosteal stem cells in a model of bone regeneration. J. Craniofac. Surg. 24, 866 871.
Arvidson, K., Abdallah, B.M., Applegate, L.A., Baldini, N., Cenni, E., Gomez-Barrena, E.,
et al., 2011. Bone regeneration and stem cells. J. Cell Mol. Med. 15, 718 746.
Baino, F., Novajra, G., Vitale-Brovarone, C., 2015. Bioceramics and scaffolds: a winning
combination for tissue engineering. Front. Bioeng. Biotechnol. 3, 202.
Balagangadharan, K., Dhivya, S., Selvamurugan, N., 2017. Chitosan based nanofibers in
bone tissue engineering. Int. J. Biol. Macromol. 104, 1372 1382.
Bauermeister, A.J., Zuriarrain, A., Newman, M.I., 2016. Three-dimensional printing in plastic
and reconstructive surgery: a systematic review. Ann. Plast. Surg. 77, 569 576.
Betre, H., Ong, S.R., Guilak, F., Chilkoti, A., Fermor, B., Setton, L.A., 2006. Chondrocytic
differentiation of human adipose-derived adult stem cells in elastin-like polypeptide.
Biomaterials 27, 91 99.
Bian, S., He, M., Sui, J., Cai, H., Sun, Y., Liang, J., et al., 2016. The self-crosslinking smart
hyaluronic acid hydrogels as injectable three-dimensional scaffolds for cells culture.
Colloids Surf., B: Biointerfaces 140, 392 402.
Burdick, J.A., Anseth, K.S., 2002. Photoencapsulation of osteoblasts in injectable RGDmodified PEG hydrogels for bone tissue engineering. Biomaterials 23, 4315 4323.
Caterson, E.J., Li, W.J., Nesti, L.J., Albert, T., Danielson, K., Tuan, R.S., 2002. Polymer/alginate amalgam for cartilage-tissue engineering. Ann. N.Y. Acad. Sci. 961, 134 138.
Chan, B.P., Leong, K.W., 2008. Scaffolding in tissue engineering: general approaches and
tissue-specific considerations. Eur. Spine J. 17 (Suppl. 4), 467 479.
Chuenjitkuntaworn, B., Osathanon, T., Nowwarote, N., Supaphol, P., Pavasant, P., 2016. The
efficacy of polycaprolactone/hydroxyapatite scaffold in combination with mesenchymal
stem cells for bone tissue engineering. J. Biomed. Mater. Res. A 104, 264 271.
666
Advanced Dental Biomaterials
Cionca, N., Hashim, D., Mombelli, A., 2017. Zirconia dental implants: where are we now,
and where are we heading? Periodontol. 2000 73, 241 258.
Collins, M.N., Birkinshaw, C., 2013. Hyaluronic acid based scaffolds for tissue engineering
—a review. Carbohydr. Polym. 92, 1262 1279.
Coluccino, L., Stagnaro, P., Vassalli, M., Scaglione, S., 2016. Bioactive TGF-beta1/HA
alginate-based scaffolds for osteochondral tissue repair: design, realization and multilevel characterization. J. Appl. Biomater. Funct. Mater. 14, e42 e52.
Daculsi, G., Passuti, N., Martin, S., Deudon, C., Legeros, R.Z., Raher, S., 1990. Macroporous
calcium phosphate ceramic for long bone surgery in humans and dogs. Clinical and histological study. J. Biomed. Mater. Res. 24, 379 396.
De Aza, P.N., Luklinska, Z.B., Santos, C., Guitian, F., De Aza, S., 2003. Mechanism of
bone-like formation on a bioactive implant in vivo. Biomaterials 24, 1437 1445.
Degidi, M., Artese, L., Scarano, A., Perrotti, V., Gehrke, P., Piattelli, A., 2006. Inflammatory
infiltrate, microvessel density, nitric oxide synthase expression, vascular endothelial
growth factor expression, and proliferative activity in peri-implant soft tissues around
titanium and zirconium oxide healing caps. J. Periodontol. 77, 73 80.
Derby, B., 2012. Printing and prototyping of tissues and scaffolds. Science 338, 921 926.
De Viteri, V.S., Fuentes, E., 2013. Titanium and titanium alloys as biomaterials. Tribology—
Fundamentals and Advancements. InTech.
Elisseeff, J., Puleo, C., Yang, F., Sharma, B., 2005. Advances in skeletal tissue engineering
with hydrogels. Orthod. Craniofac. Res. 8, 150 161.
Elnayef, B., Lazaro, A., Suarez-Lopez Del Amo, F., Galindo-Moreno, P., Wang, H.L.,
Gargallo-Albiol, J., et al., 2017. Zirconia implants as an alternative to titanium: a systematic review and meta-analysis. Int. J. Oral. Maxillofac. Implants 32, e125 e134.
Engebretson, B., Sikavitsas, V.I., 2012. Long-term in vivo effect of PEG bone tissue engineering scaffolds. J. Long Term Eff. Med. Implants 22, 211 218.
Ferreira, A.M., Gentile, P., Chiono, V., Ciardelli, G., 2012. Collagen for bone tissue regeneration. Acta Biomater. 8, 3191 3200.
Ganesh, N., Hanna, C., Nair, S.V., Nair, L.S., 2013. Enzymatically cross-linked alginic-hyaluronic acid composite hydrogels as cell delivery vehicles. Int. J. Biol. Macromol. 55,
289 294.
Gauthier, O., Bouler, J.M., Aguado, E., Pilet, P., Daculsi, G., 1998. Macroporous biphasic
calcium phosphate ceramics: influence of macropore diameter and macroporosity percentage on bone ingrowth. Biomaterials 19, 133 139.
Giannitelli, S.M., Accoto, D., Trombetta, M., Rainer, A., 2014. Current trends in the design
of scaffolds for computer-aided tissue engineering. Acta Biomater. 10, 580 594.
Ginebra, M.P., Traykova, T., Planell, J.A., 2006. Calcium phosphate cements as bone drug
delivery systems: a review. J. Controlled Release 113, 102 110.
Gjorgievska, E., Nicholson, J.W., Grcev, A.T., 2012. Ion migration from fluoride-releasing dental restorative materials into dental hard tissues. J. Mater. Sci. Mater. Med. 23, 1811 1821.
Glowacki, J., Mizuno, S., 2008. Collagen scaffolds for tissue engineering. Biopolymers 89,
338 344.
Goh, B.T., Teh, L.Y., Tan, D.B., Zhang, Z., Teoh, S.H., 2015. Novel 3D polycaprolactone
scaffold for ridge preservation—a pilot randomised controlled clinical trial. Clin. Oral.
Implants Res. 26, 271 277.
Gosline, J., Lillie, M., Carrington, E., Guerette, P., Ortlepp, C., Savage, K., 2002. Elastic proteins: biological roles and mechanical properties. Philos. Trans. R. Soc. Lond. B Biol.
Sci. 357, 121 132.
Biomaterials for craniofacial tissue engineering and regenerative dentistry
667
He, J., He, F.L., Li, D.W., Liu, Y.L., Yin, D.C., 2016. A novel porous Fe/Fe-W alloy scaffold
with a double-layer structured skeleton: preparation, in vitro degradability and biocompatibility. Colloids Surf., B: Biointerfaces 142, 325 333.
Hench, L.L., Wilson, J., 1984. Surface-active biomaterials. Science 226, 630 636.
Hermawan, H., Dube, D., Mantovani, D., 2010. Degradable metallic biomaterials: design and
development of Fe-Mn alloys for stents. J. Biomed. Mater. Res. A 93, 1 11.
Herr, Y., Woo, J., Kwon, Y., Park, J., Heo, S., Chung, J., 2008. Implant surface conditioning
with tetracycline-HCl: a SEM study. Key Engineering Materials. Trans Tech Publ,
pp. 849 852.
Hoffmann, O., Angelov, N., Gallez, F., Jung, R.E., Weber, F.E., 2008. The zirconia implantbone interface: a preliminary histologic evaluation in rabbits. Int. J. Oral. Maxillofac.
Implants 23, 691 695.
Hsu, E.L., Ghodasra, J.H., Ashtekar, A., Nickoli, M.S., Lee, S.S., Stupp, S.I., et al., 2013. A
comparative evaluation of factors influencing osteoinductivity among scaffolds designed
for bone regeneration. Tissue Eng. Part A 19, 1764 1772.
Huang, Z., Wang, Z., Li, C., Yin, K., Hao, D., Lan, J., 2018. Application of plasma sprayed
zirconia coating in dental implant: study in implant. J. Oral. Implantol.
Ikeda, E., Morita, R., Nakao, K., Ishida, K., Nakamura, T., Takano-Yamamoto, T., et al.,
2009. Fully functional bioengineered tooth replacement as an organ replacement therapy. Proc. Natl. Acad. Sci. U.S.A. 106, 13475 13480.
Inuyama, Y., Kitamura, C., Nishihara, T., Morotomi, T., Nagayoshi, M., Tabata, Y., et al.,
2010. Effects of hyaluronic acid sponge as a scaffold on odontoblastic cell line and
amputated dental pulp. J. Biomed. Mater. Res. B Appl. Biomater. 92, 120 128.
Iwai, S., Shimizu, H., Suzawa, Y., Akashi, M., Yura, Y., 2015. Hydroxyapatite agarose composite gels as a biochemical material for the repair of alveolar bone defects due to cleft
lip and palate. J. Oral Maxillofac. Surg. Med. Pathol. 27, 637 644.
Jafari, M., Paknejad, Z., Rad, M.R., Motamedian, S.R., Eghbal, M.J., Nadjmi, N., et al.,
2017. Polymeric scaffolds in tissue engineering: a literature review. J. Biomed. Mater.
Res. B Appl. Biomater. 105, 431 459.
Kadler, K., 2004. Matrix loading: assembly of extracellular matrix collagen fibrils during
embryogenesis. Birth Defects Res. C Embryo Today 72, 1 11.
Kale, S., Biermann, S., Edwards, C., Tarnowski, C., Morris, M., Long, M.W., 2000. Threedimensional cellular development is essential for ex vivo formation of human bone. Nat.
Biotechnol. 18, 954 958.
Kang, B.J., Kim, Y., Lee, S.H., Kim, W.H., Woo, H.M., Kweon, O.K., 2013. Collagen I gel
promotes homogenous osteogenic differentiation of adipose tissue-derived mesenchymal
stem cells in serum-derived albumin scaffold. J. Biomater. Sci. Polym. Ed. 24,
1233 1243.
Kapat, K., Srivas, P.K., Rameshbabu, A.P., Maity, P.P., Jana, S., Dutta, J., et al., 2017.
Influence of porosity and pore-size distribution in Ti6Al4V foam on physicomechanical
properties, osteogenesis, and quantitative validation of bone ingrowth by microcomputed tomography. ACS Appl. Mater. Interfaces 9, 39235 39248.
Keane, T.J., Badylak, S.F., 2014. Biomaterials for tissue engineering applications. Semin.
Pediatr. Surg. 23, 112 118.
Kim, K., Fisher, J.P., 2007. Nanoparticle technology in bone tissue engineering. J. Drug
Target. 15, 241 252.
Kim, H.D., Valentini, R.F., 2002. Retention and activity of BMP-2 in hyaluronic acid-based
scaffolds in vitro. J. Biomed. Mater. Res. 59, 573 584.
668
Advanced Dental Biomaterials
Kim, I.S., Park, J.W., Kwon, I.C., Baik, B.S., Cho, B.C., 2002. Role of BMP, betaig-h3, and
chitosan in early bony consolidation in distraction osteogenesis in a dog model. Plast.
Reconstr. Surg. 109, 1966 1977.
Kim, K., Lee, C.H., Kim, B.K., Mao, J.J., 2010. Anatomically shaped tooth and periodontal
regeneration by cell homing. J. Dent. Res. 89, 842 847.
Kim, I.L., Khetan, S., Baker, B.M., Chen, C.S., Burdick, J.A., 2013a. Fibrous hyaluronic acid
hydrogels that direct MSC chondrogenesis through mechanical and adhesive cues.
Biomaterials 34, 5571 5580.
Kim, M., Jung, W.K., Kim, G., 2013b. Bio-composites composed of a solid free-form fabricated polycaprolactone and alginate-releasing bone morphogenic protein and bone formation peptide for bone tissue regeneration. Bioprocess Biosyst. Eng. 36, 1725 1734.
Kim, B.S., Sung, H.M., You, H.K., Lee, J., 2014. Effects of fibrinogen concentration on
fibrin glue and bone powder scaffolds in bone regeneration. J. Biosci. Bioeng. 118,
469 475.
Knowles, J.C., 2003. Phosphate based glasses for biomedical applications. J. Mater. Chem.
13, 2395 2401.
Koubi, G., Colon, P., Franquin, J.C., Hartmann, A., Richard, G., Faure, M.O., et al., 2013.
Clinical evaluation of the performance and safety of a new dentine substitute,
Biodentine, in the restoration of posterior teeth—a prospective study. Clin. Oral
Investig. 17, 243 249.
Kruger, T.E., Miller, A.H., Wang, J., 2013. Collagen scaffolds in bone sialoprotein-mediated
bone regeneration. Sci. World J. 2013, 812718.
Laurent, P., Camps, J., De Meo, M., Dejou, J., About, I., 2008. Induction of specific cell
responses to a Ca(3)SiO(5)-based posterior restorative material. Dent. Mater. 24,
1486 1494.
Lavenus, S., Louarn, G., Layrolle, P., 2010. Nanotechnology and dental implants. Int. J.
Biomater. 2010, 915327.
Laydi, F., Rahouadj, R., Cauchois, G., Stoltz, J.-F., De Isla, N., 2013. Hydroxyapatite incorporated into collagen gels for mesenchymal stem cell culture. Biomed. Mater. Eng. 23,
311 315.
Lee, J.H., Ryu, M.Y., Baek, H.R., Lee, K.M., Seo, J.H., Lee, H.K., 2013. Fabrication and
evaluation of porous beta-tricalcium phosphate/hydroxyapatite (60/40) composite as a
bone graft extender using rat calvarial bone defect model. Sci. World J. 2013, 481789.
Lee, C.H., Hajibandeh, J., Suzuki, T., Fan, A., Shang, P., Mao, J.J., 2014. Three-dimensional
printed multiphase scaffolds for regeneration of periodontium complex. Tissue Eng. Part
A 20, 1342 1351.
Lee, T.T., Garcia, J.R., Paez, J.I., Singh, A., Phelps, E.A., Weis, S., et al., 2015. Lighttriggered in vivo activation of adhesive peptides regulates cell adhesion, inflammation
and vascularization of biomaterials. Nat. Mater. 14, 352 360.
LeGeros, R.Z., 2002. Properties of osteoconductive biomaterials: calcium phosphates. Clin.
Orthop. Relat. Res. 81 98.
Legeros, R.Z., Lin, S., Rohanizadeh, R., Mijares, D., Legeros, J.P., 2003. Biphasic calcium
phosphate bioceramics: preparation, properties and applications. J. Mater. Sci. Mater.
Med. 14, 201 209.
Le Guehennec, L., Soueidan, A., Layrolle, P., Amouriq, Y., 2007. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 23, 844 854.
Levengood, S.L., Zhang, M., 2014. Chitosan-based scaffolds for bone tissue engineering. J.
Mater. Chem. B 2, 3161 3184.
Biomaterials for craniofacial tissue engineering and regenerative dentistry
669
Lewandowska-Lancucka, J., Mystek, K., Mignon, A., Van Vlierberghe, S., Latkiewicz, A.,
Nowakowska, M., 2017. Alginate- and gelatin-based bioactive photocross-linkable
hybrid materials for bone tissue engineering. Carbohydr. Polym. 157, 1714 1722.
Li, D.W., He, J., He, F.L., Liu, Y.L., Liu, Y.Y., Ye, Y.J., et al., 2018a. Silk fibroin/chitosan
thin film promotes osteogenic and adipogenic differentiation of rat bone marrow-derived
mesenchymal stem cells. J. Biomater. Appl. 32, 1164 1173.
Li, N., Wang, Z., Zhang, Y., Zhang, K., Xie, J., Liu, Y., et al., 2018b. Curcumin-loaded
redox-responsive mesoporous silica nanoparticles for targeted breast cancer therapy.
Artif. Cells Nanomed. Biotechnol. 46, 921 935.
Lin, W.-J., Flanagan, D.R., Linhardt, R.J., 1999. A novel fabrication of poly(ε-caprolactone)
microspheres from blends of poly(ε-caprolactone) and poly(ethylene glycol)s. Polymer
40, 1731 1735.
Linsley, C.S., Wu, B.M., Tawil, B., 2016. Mesenchymal stem cell growth on and mechanical
properties of fibrin-based biomimetic bone scaffolds. J. Biomed. Mater. Res. A 104,
2945 2953.
Liu, B., Lun, D.X., 2012. Current application of beta-tricalcium phosphate composites in
orthopaedics. Orthop. Surg. 4, 139 144.
Luo, Z., Li, D., Kohli, M.R., Yu, Q., Kim, S., He, W.X., 2014. Effect of Biodentine on the
proliferation, migration and adhesion of human dental pulp stem cells. J. Dent. 42,
490 497.
Ma, X., Wang, Y., Guo, H., Wang, J., 2011. Nano-hydroxyapatite/chitosan sponge-like biocomposite for repairing of rat calvarial critical-sized bone defect. J. Bioact. Compat.
Polym. 26, 335 346.
Mandal, B.B., Grinberg, A., Gil, E.S., Panilaitis, B., Kaplan, D.L., 2012. High-strength silk
protein scaffolds for bone repair. Proc. Natl. Acad. Sci. U.S.A. 109, 7699 7704.
Mantripragada, V.P., Lecka-Czernik, B., Ebraheim, N.A., Jayasuriya, A.C., 2013. An overview of recent advances in designing orthopedic and craniofacial implants. J. Biomed.
Mater. Res. A 101, 3349 3364.
Marsich, E., Bellomo, F., Turco, G., Travan, A., Donati, I., Paoletti, S., 2013. Nanocomposite scaffolds for bone tissue engineering containing silver nanoparticles: preparation, characterization and biological properties. J. Mater. Sci. Mater. Med. 24,
1799 1807.
Mathews, S., Gupta, P.K., Bhonde, R., Totey, S., 2011. Chitosan enhances mineralization
during osteoblast differentiation of human bone marrow-derived mesenchymal stem
cells, by upregulating the associated genes. Cell Prolif. 44, 537 549.
Melke, J., Midha, S., Ghosh, S., Ito, K., Hofmann, S., 2016. Silk fibroin as biomaterial for
bone tissue engineering. Acta Biomater. 31, 1 16.
Moreira, C.D., Carvalho, S.M., Mansur, H.S., Pereira, M.M., 2016. Thermogelling chitosan collagen bioactive glass nanoparticle hybrids as potential injectable systems for
tissue engineering. Mater. Sci. Eng., C 58, 1207 1216.
Moshaverinia, A., Chen, C., Akiyama, K., Ansari, S., Xu, X., Chee, W.W., et al., 2012.
Alginate hydrogel as a promising scaffold for dental-derived stem cells: an in vitro
study. J. Mater. Sci. Mater. Med. 23, 3041 3051.
Moshiri, A., Oryan, A., 2012. Role of tissue engineering in tendon reconstructive surgery and
regenerative medicine: current concepts, approaches and concerns. Hard Tissue 1, 11.
Muiznieks, L.D., Keeley, F.W., 2013. Molecular assembly and mechanical properties of the
extracellular matrix: a fibrous protein perspective. Biochim. Biophys. Acta 1832,
866 875.
670
Advanced Dental Biomaterials
Muzzarelli, R.A., Mattioli-Belmonte, M., Tietz, C., Biagini, R., Ferioli, G., Brunelli, M.A.,
et al., 1994. Stimulatory effect on bone formation exerted by a modified chitosan.
Biomaterials 15, 1075 1081.
Nair, L.S., Laurencin, C.T., 2007. Biodegradable polymers as biomaterials. Prog. Polym. Sci.
32, 762 798.
Nandi, S.K., Kundu, B., Datta, S., De, D.K., Basu, D., 2009. The repair of segmental bone
defects with porous bioglass: an experimental study in goat. Res. Vet. Sci. 86, 162 173.
Nery, E.B., Legeros, R.Z., Lynch, K.L., Lee, K., 1992. Tissue response to biphasic calcium
phosphate ceramic with different ratios of HA/beta TCP in periodontal osseous defects.
J. Periodontol. 63, 729 735.
Noori, A., Ashrafi, S.J., Vaez-Ghaemi, R., Hatamian-Zaremi, A., Webster, T.J., 2017. A
review of fibrin and fibrin composites for bone tissue engineering. Int. J. Nanomed. 12,
4937 4961.
Nowicka, A., Lipski, M., Parafiniuk, M., Sporniak-Tutak, K., Lichota, D., Kosierkiewicz, A.,
et al., 2013. Response of human dental pulp capped with biodentine and mineral trioxide
aggregate. J. Endod. 39, 743 747.
Nyberg, E.L., Farris, A.L., Hung, B.P., Dias, M., Garcia, J.R., Dorafshar, A.H., et al., 2017.
3D-printing technologies for craniofacial rehabilitation, reconstruction, and regeneration.
Ann. Biomed. Eng. 45, 45 57.
Obregon, F., Vaquette, C., Ivanovski, S., Hutmacher, D.W., Bertassoni, L.E., 2015. Threedimensional bioprinting for regenerative dentistry and craniofacial tissue engineering. J.
Dent. Res. 94, 143S 152SS.
Oryan, A., Moshiri, A., Parizi Meimandi, A., Silver, I.A., 2013. A long-term in vivo investigation on the effects of xenogenous based, electrospun, collagen implants on the healing
of experimentally-induced large tendon defects. J. Musculoskelet. Neuronal. Interact.
13, 353 367.
Ouasti, S., Donno, R., Cellesi, F., Sherratt, M.J., Terenghi, G., Tirelli, N., 2011. Network
connectivity, mechanical properties and cell adhesion for hyaluronic acid/PEG hydrogels. Biomaterials 32, 6456 6470.
Özcan, M., Hämmerle, C., 2012. Titanium as a reconstruction and implant material in dentistry: advantages and pitfalls. Materials 5, 1528 1545.
Ozkurt, Z., Kazazoglu, E., 2011. Zirconia dental implants: a literature review. J. Oral.
Implantol. 37, 367 376.
Panzavolta, S., Torricelli, P., Casolari, S., Parrilli, A., Fini, M., Bigi, A., 2018. Strontiumsubstituted hydroxyapatite-gelatin biomimetic scaffolds modulate bone cell response.
Macromol. Biosci. 18, e1800096.
Park, J.K., Shim, J.H., Kang, K.S., Yeom, J., Jung, H.S., Kim, J.Y., et al., 2011. Solid freeform fabrication of tissue-engineering scaffolds with a poly(lactic-co-glycolic acid)
grafted hyaluronic acid conjugate encapsulating an intact bone morphogenetic
protein 2/poly(ethylene glycol) complex. Adv. Funct. Mater. 21, 2906 2912.
Petrov, O., Dyulgerova, E., Petrov, L., Popova, R., 2001. Characterization of calcium phosphate phases obtained during the preparation of sintered biphase Ca-P ceramics. Mater.
Lett. 48, 162 167.
Pitt, C.G., Gratzl, M.M., Kimmel, G.L., Surles, J., Schindler, A., 1981. Aliphatic polyesters
II. The degradation of poly(DL-lactide), poly(epsilon-caprolactone), and their copolymers
in vivo. Biomaterials 2, 215 220.
Preis, V., Kammermeier, A., Handel, G., Rosentritt, M., 2016. In vitro performance of twopiece zirconia implant systems for anterior application. Dent. Mater. 32, 765 774.
Biomaterials for craniofacial tissue engineering and regenerative dentistry
671
Qi, X., Pei, P., Zhu, M., Du, X., Xin, C., Zhao, S., et al., 2017. Three dimensional printing of
calcium sulfate and mesoporous bioactive glass scaffolds for improving bone regeneration in vitro and in vivo. Sci. Rep. 7, 42556.
Quinlan, E., Thompson, E.M., Matsiko, A., O’brien, F.J., Lopez-Noriega, A., 2015.
Functionalization of a collagen-hydroxyapatite scaffold with osteostatin to facilitate
enhanced bone regeneration. Adv. Healthcare Mater. 4, 2649 2656.
Rahaman, M.N., Day, D.E., Bal, B.S., Fu, Q., Jung, S.B., Bonewald, L.F., et al., 2011.
Bioactive glass in tissue engineering. Acta Biomater. 7, 2355 2373.
Rajasekharan, S., Martens, L.C., Cauwels, R.G., Verbeeck, R.M., 2014. Biodentine material
characteristics and clinical applications: a review of the literature. Eur. Arch. Paediatr.
Dent. 15, 147 158.
Ramesh, N., Moratti, S.C., Dias, G.J., 2018. Hydroxyapatite-polymer biocomposites for bone
regeneration: a review of current trends. J. Biomed. Mater. Res. B Appl. Biomater. 106,
2046 2057.
Rauscher, S., Pomes, R., 2012. Structural disorder and protein elasticity. Adv. Exp. Med.
Biol. 725, 159 183.
Ribeiro, V.P., Pina, S., Oliveira, J.M., Reis, R.L., 2018. Silk fibroin-based hydrogels and
scaffolds for osteochondral repair and regeneration. Adv. Exp. Med. Biol. 1058,
305 325.
Roberts, H.W., Toth, J.M., Berzins, D.W., Charlton, D.G., 2008. Mineral trioxide aggregate
material use in endodontic treatment: a review of the literature. Dent. Mater. 24, 149 164.
Rouvillain, J.L., Lavalle, F., Pascal-Mousselard, H., Catonne, Y., Daculsi, G., 2009. Clinical,
radiological and histological evaluation of biphasic calcium phosphate bioceramic
wedges filling medial high tibial valgisation osteotomies. Knee 16, 392 397.
Saini, M., Singh, Y., Arora, P., Arora, V., Jain, K., 2015. Implant biomaterials: a comprehensive review. World J. Clin. Cases 3, 52 57.
Sarker, A., Amirian, J., Min, Y.K., Lee, B.T., 2015. HAp granules encapsulated oxidized
alginate-gelatin-biphasic calcium phosphate hydrogel for bone regeneration. Int. J. Biol.
Macromol. 81, 898 911.
Schneider, R.K., Puellen, A., Kramann, R., Raupach, K., Bornemann, J., Knuechel, R.,
Perez-Bouza, A., Neuss, S., 2010. The osteogenic differentiation of adult bone marrow
and perinatal umbilical mesenchymal stem cells and matrix remodelling in three-dimensional collagen scaffolds. Biomaterials 31, 467 480.
Schulte, M., Schultheiss, M., Hartwig, E., Wilke, H.J., Wolf, S., Sokiranski, R., et al.,
2000. Vertebral body replacement with a bioglass-polyurethane composite in spine
metastases—clinical, radiological and biomechanical results. Eur. Spine J. 9, 437 444.
Sennerby, L., Dasmah, A., Larsson, B., Iverhed, M., 2005. Bone tissue responses to surfacemodified zirconia implants: a histomorphometric and removal torque study in the rabbit.
Clin. Implant Dent. Relat. Res. 7 (Suppl. 1), S13 S20.
Seol, Y.J., Lee, J.Y., Park, Y.J., Lee, Y.M., Young, K., Rhyu, I.C., et al., 2004. Chitosan
sponges as tissue engineering scaffolds for bone formation. Biotechnol. Lett. 26,
1037 1041.
Shalumon, K.T., Sowmya, S., Sathish, D., Chennazhi, K.P., Nair, S.V., Jayakumar, R., 2013.
Effect of incorporation of nanoscale bioactive glass and hydroxyapatite in PCL/chitosan
nanofibers for bone and periodontal tissue engineering. J. Biomed. Nanotechnol. 9,
430 440.
Sidambe, A.T., 2014. Biocompatibility of advanced manufactured titanium implants—a
review. Materials 7, 8168 8188.
672
Advanced Dental Biomaterials
Siddiqui, N., Pramanik, K., 2015. Development of fibrin conjugated chitosan/nano β-TCP
composite scaffolds with improved cell supportive property for bone tissue regeneration.
J. Appl. Polym. Sci. 132.
Singh, B.N., Panda, N.N., Mund, R., Pramanik, K., 2016. Carboxymethyl cellulose enables
silk fibroin nanofibrous scaffold with enhanced biomimetic potential for bone tissue
engineering application. Carbohydr. Polym. 151, 335 347.
Staiger, M.P., Pietak, A.M., Huadmai, J., Dias, G., 2006. Magnesium and its alloys as orthopedic biomaterials: a review. Biomaterials 27, 1728 1734.
Stoppel, W.L., Ghezzi, C.E., Mcnamara, S.L., Black III, L.D., Kaplan, D.L., 2015. Clinical
applications of naturally derived biopolymer-based scaffolds for regenerative medicine.
Ann. Biomed. Eng. 43, 657 680.
Subramani, K., Mathew, R.T., Pachauri, P., 2018. Titanium surface modification techniques
for dental implants—from microscale to nanoscale, Emerging Nanotechnologies in
Dentistry, second ed. Elsevier.
Sul, Y.T., Johansson, C.B., Kang, Y., Jeon, D.G., Albrektsson, T., 2002. Bone reactions to
oxidized titanium implants with electrochemical anion sulphuric acid and phosphoric
acid incorporation. Clin. Implant Dent. Relat. Res. 4, 78 87.
Sun, J., Tan, H., 2013. Alginate-based biomaterials for regenerative medicine applications.
Materials (Basel) 6, 1285 1309.
Tedesco, J., Lee, B.E.J., Lin, A.Y.W., Binkley, D.M., Delaney, K.H., Kwiecien, J.M., et al.,
2017. Osseointegration of a 3D printed stemmed titanium dental implant: a pilot study.
Int. J. Dent. 2017, 5920714.
Tevlin, R., Mcardle, A., Atashroo, D., Walmsley, G.G., Senarath-Yapa, K., Zielins, E.R.,
et al., 2014. Biomaterials for craniofacial bone engineering. J. Dent. Res. 93,
1187 1195.
Tran, P.A., Webster, T.J., 2011. Selenium nanoparticles inhibit Staphylococcus aureus
growth. Int. J. Nanomed. 6, 1553 1558.
Valente, J.F.A., Valente, T.A.M., Alves, P., Ferreira, P., Silva, A., Correia, I.J., 2012.
Alginate based scaffolds for bone tissue engineering. Mater. Sci. Eng., C 32,
2596 2603.
Valerio, P., Pereira, M.M., Goes, A.M., Leite, M.F., 2004. The effect of ionic products from
bioactive glass dissolution on osteoblast proliferation and collagen production.
Biomaterials 25, 2941 2948.
Valimaki, V.V., Yrjans, J.J., Vuorio, E., Aro, H.T., 2005. Combined effect of BMP-2 gene
transfer and bioactive glass microspheres on enhancement of new bone formation. J.
Biomed. Mater. Res. A 75, 501 509.
Valles, M., Mercade, M., Duran-Sindreu, F., Bourdelande, J.L., Roig, M., 2013. Influence of
light and oxygen on the color stability of five calcium silicate-based materials. J. Endod.
39, 525 528.
Venkatesan, J., Bhatnagar, I., Kim, S.K., 2014. Chitosan-alginate biocomposite containing
fucoidan for bone tissue engineering. Mar. Drugs 12, 300 316.
Villa, M.M., Wang, L., Huang, J., Rowe, D.W., Wei, M., 2015. Bone tissue engineering with
a collagen-hydroxyapatite scaffold and culture expanded bone marrow stromal cells. J.
Biomed. Mater. Res. B Appl. Biomater. 103, 243 253.
Von Arx, T., Cochran, D.L., Hermann, J.S., Schenk, R.K., Buser, D., 2001. Lateral ridge augmentation using different bone fillers and barrier membrane application. A histologic
and histomorphometric pilot study in the canine mandible. Clin. Oral. Implants Res. 12,
260 269.
Biomaterials for craniofacial tissue engineering and regenerative dentistry
673
Wang, Z., Jiang, T., Sauro, S., Pashley, D.H., Toledano, M., Osorio, R., et al., 2011. The dentine remineralization activity of a desensitizing bioactive glass-containing toothpaste: an
in vitro study. Aust. Dent. J. 56, 372 381.
Wang, F., Zhang, Y.C., Zhou, H., Guo, Y.C., Su, X.X., 2014. Evaluation of in vitro and
in vivo osteogenic differentiation of nano-hydroxyapatite/chitosan/poly(lactide-co-glycolide) scaffolds with human umbilical cord mesenchymal stem cells. J. Biomed. Mater.
Res. A 102, 760 768.
Wang, M.O., Bracaglia, L., Thompson, J.A., Fisher, J.P., 2016. Hydroxyapatite-doped alginate beads as scaffolds for the osteoblastic differentiation of mesenchymal stem cells. J.
Biomed. Mater. Res. A 104, 2325 2333.
Watanabe, J., Kashii, M., Hirao, M., Oka, K., Sugamoto, K., Yoshikawa, H., et al., 2007.
Quick-forming hydroxyapatite/agarose gel composites induce bone regeneration. J.
Biomed. Mater. Res. A 83, 845 852.
Wee, S., Gombotz, W.R., 1998. Protein release from alginate matrices. Adv. Drug Deliv.
Rev. 31, 267 285.
Weisgerber, D.W., Milner, D.J., Lopez-Lake, H., Rubessa, M., Lotti, S., Polkoff, K., et al.,
2018. A mineralized collagen-polycaprolactone composite promotes healing of a porcine
mandibular defect. Tissue Eng. Part A 24, 943 954.
Wen, C.E., Yamada, Y., Shimojima, K., Chino, Y., Hosokawa, H., Mabuchi, M., 2011.
Novel titanium foam for bone tissue engineering. J. Mater. Res. 17, 2633 2639.
Wikesjö, U.M., Sorensen, R.G., Kinoshita, A., Wozney, J.M., 2002. rhBMP-2/αBSMs
induces significant vertical alveolar ridge augmentation and dental implant osseointegration. Clin. Implant Dent. Relat. Res. 4, 174 182.
Wong, M., 2004. Alginates in tissue engineering. Methods Mol. Biol. 238, 77 86.
Woodward, S.C., Brewer, P.S., Moatamed, F., Schindler, A., Pitt, C.G., 1985. The intracellular degradation of poly(epsilon-caprolactone). J. Biomed. Mater. Res. 19, 437 444.
Xie, J., Lou, X., Wang, X., Yang, L., Zhang, Y., 2015. Electrospun nanofibers of hydroxyapatite/collagen/chitosan promote osteogenic differentiation of the induced pluripotent
stem cell-derived mesenchymal stem cells. J. Controlled Release 213, e53.
Xie, H., Gu, Z., Li, C., Franco, C., Wang, J., Li, L., et al., 2016. A novel bioceramic scaffold
integrating silk fibroin in calcium polyphosphate for bone tissue-engineering. Ceram.
Int. 42, 2386 2392.
Yang, X., Chen, X., Wang, H., 2009. Acceleration of osteogenic differentiation of preosteoblastic cells by chitosan containing nanofibrous scaffolds. Biomacromolecules 10,
2772 2778.
Yang, F., Zhao, S.F., Zhang, F., He, F.M., Yang, G.L., 2011. Simvastatin-loaded porous
implant surfaces stimulate preosteoblasts differentiation: an in vitro study. Oral Surg.
Oral Med. Oral Pathol. Oral Radiol. Endod. 111, 551 556.
Yang, C., Unursaikhan, O., Lee, J.S., Jung, U.W., Kim, C.S., Choi, S.H., 2014.
Osteoconductivity and biodegradation of synthetic bone substitutes with different tricalcium phosphate contents in rabbits. J. Biomed. Mater. Res. B Appl. Biomater. 102,
80 88.
Yazdimamaghani, M., Razavi, M., Vashaee, D., Moharamzadeh, K., Boccaccini, A.R.,
Tayebi, L., 2017. Porous magnesium-based scaffolds for tissue engineering. Mater. Sci.
Eng. C Mater. Biol. Appl. 71, 1253 1266.
Yoshimoto, H., Shin, Y.M., Terai, H., Vacanti, J.P., 2003. A biodegradable nanofiber scaffold by electrospinning and its potential for bone tissue engineering. Biomaterials 24,
2077 2082.
674
Advanced Dental Biomaterials
Yu, C.-C., Chang, J.-J., Lee, Y.-H., Lin, Y.-C., Wu, M.-H., Yang, M.-C., et al., 2013.
Electrospun scaffolds composing of alginate, chitosan, collagen and hydroxyapatite for
applying in bone tissue engineering. Mater. Lett. 93, 133 136.
Yuan, Z., Nie, H., Wang, S., Lee, C.H., Li, A., Fu, S.Y., et al., 2011. Biomaterial selection
for tooth regeneration. Tissue Eng. Part B Rev. 17, 373 388.
Yusop, A.H., Bakir, A.A., Shaharom, N.A., Abdul Kadir, M.R., Hermawan, H., 2012. Porous
biodegradable metals for hard tissue scaffolds: a review. Int. J. Biomater. 2012, 641430.
Zarrintaj, P., Manouchehri, S., Ahmadi, Z., Saeb, M.R., Urbanska, A.M., Kaplan, D.L., et al.,
2018. Agarose-based biomaterials for tissue engineering. Carbohydr. Polym. 187,
66 84.
Zhang, Q., Yan, S., Li, M., 2009. Silk fibroin based porous materials. Materials 2,
2276 2295.
Zhang, W., Ahluwalia, I.P., Yelick, P.C., 2010. Three dimensional dental epithelialmesenchymal constructs of predetermined size and shape for tooth regeneration.
Biomaterials 31, 7995 8003.
Zhang, W., Ahluwalia, I.P., Literman, R., Kaplan, D.L., Yelick, P.C., 2011. Human dental
pulp progenitor cell behavior on aqueous and hexafluoroisopropanol based silk scaffolds. J. Biomed. Mater. Res. A 97, 414 422.
Zhang, Y., Kong, D., Yokogawa, Y., Feng, X., Tao, Y., Qiu, T., 2012. Fabrication of porous
hydroxyapatite ceramic scaffolds with high flexural strength through the double slipcasting method using fine powders. J. Am. Ceram. Soc. 95, 147 152.
Zhou, H., Lee, J., 2011. Nanoscale hydroxyapatite particles for bone tissue engineering. Acta
Biomater. 7, 2769 2781.
Zhou, C., Ye, X., Fan, Y., Ma, L., Tan, Y., Qing, F., et al., 2014. Biomimetic fabrication of a
three-level hierarchical calcium phosphate/collagen/hydroxyapatite scaffold for bone tissue engineering. Biofabrication 6, 035013.
Zhu, J., 2010. Bioactive modification of poly(ethylene glycol) hydrogels for tissue engineering. Biomaterials 31, 4639 4656.
Applications of silver diamine
fluoride in management of
dental caries
25
Wei-Te Huang, Saroash Shahid and Paul Anderson
Centre for Oral Bioengineering, Institute of Dentistry, Queen Mary University of London,
London, United Kingdom
Chapter Outline
25.1 Introduction 675
25.2 Brief history 676
25.3 Clinical effects of silver diamine fluoride applications on caries
management 676
25.3.1 Management of coronal caries in children 677
25.3.2 Management of coronal caries in adults 683
25.3.3 Management of root caries in the elderly 684
25.4 Cariostatic mechanism of silver diamine fluoride 685
25.4.1 Cariostatic effects of silver diamine fluoride on dental mineral 685
25.4.2 Cariostatic effects of silver diamine fluoride on cariogenic bacteria 690
25.4.3 Cariostatic effects of silver diamine fluoride on organic content of dentine 692
25.5 Safety of silver diamine fluoride treatment
25.6 Conclusion 694
References 694
25.1
692
Introduction
Silver diamine fluoride (SDF; Ag[NH3]2F) is an alkaline (pHB10), colorless topical agent containing silver and fluoride, which has been used as a cariostatic agent
for almost 50 years (Shah et al., 2014; Mei et al., 2017; Yamaga et al., 1972). SDF
combines the remineralizing effect of fluoride and the antibacterial effect of silver,
which together make SDF treatment more effective in controlling caries lesions
than many other fluoride treatments, such as sodium fluoride varnish (Chibinski
et al., 2017; Rosenblatt et al., 2009; Shah et al., 2014). Further, as Ag1 in SDF can
be stabilized by forming a silver diamine complex, [Ag(NH3)2]1, the storage period
of SDF is longer than that of AgF (Liu et al., 2012b).
SDF has been regarded as an efficient, affordable, effective, and safe cariostatic
agent, whose application in dental caries management complies with the concept of
minimally invasive dentistry (MID) (Frencken et al., 2012; Murdoch-Kinch and
McLean, 2003; Wilson, 2007). SDF treatment has shown substantial anticaries
Advanced Dental Biomaterials. DOI: https://doi.org/10.1016/B978-0-08-102476-8.00023-2
Copyright © 2019 Elsevier Ltd. All rights reserved.
676
Advanced Dental Biomaterials
efficacy comparable to restorative dentistry in both deciduous and permanent teeth
(Horst et al., 2016; Zhao et al., 2017a). However, the black staining of the treated
lesion is a major disadvantage of topical SDF treatment (Horst et al., 2016; Mei
et al., 2016a). Thus potassium iodide (KI) has been used as a reducing agent to
remove the discoloration from SDF (Ngo et al., 2002). Nonetheless, further studies
are required to verify the cariostatic efficacy of this combination treatment (Knight
et al., 2005).
25.2
Brief history
Since the 1970s SDF has been accepted as a therapeutic agent with an anticaries
function by the Central Pharmaceutical Council of the Ministry of Health and
Welfare in Japan (Yamaga et al., 1972). However, the utilization of SDF is less
common in Western countries (Gao et al., 2016). Recently SDF has drawn attention
from dental researchers due to its effectiveness in preventing and arresting dental
caries, and its noninvasive method of application (Frencken et al., 2012; Mei et al.,
2017). Shortly after being approved for clinical use by the US Food and Drug
Administration (FDA) in 2014, SDF entered the US market in 2015 (Horst et al.,
2016). In 2016 a current dental terminology code was approved for SDF to be used
for arresting dental caries (Horst et al., 2016).
25.3
Clinical effects of silver diamine fluoride
applications on caries management
MID has been advocated since the early 1990s, in order to keep the teeth functional
for a whole lifetime. In contrast to conventional clinical treatment, the aim of MID
is to reduce the need for tissue cutting and save as much healthy tissue as possible
by the enhancement of cariostatic effects, and by minimally invasive restoration
(Frencken et al., 2012; Murdoch-Kinch and McLean, 2003; Wilson, 2007). Even
though fluoride has a pronounced remineralization ability, and is still the cornerstone of MID for dental caries management (Hellwig and Lennon, 2004), the fluoride concentration in the oral cavity is not sufficient to inhibit cariogenic bacterial
activities (Tenuta and Cury, 2010).
Recently there has been a growing trend in the use of SDF in dentistry due to its
antibacterial properties and noninvasive way of application (Horst et al., 2016;
Wilson, 2007; Frencken et al., 2012; Mei et al., 2016a). The application of SDF for
caries control conforms to the World Health Organization’s Millennium Goals and
the US Institute of Medicine’s criteria for 21st century medical care (Mei et al.,
2013a). However, the black staining of the SDF-treated lesion is an esthetic problem (Fig. 25.1) compared with other fluoride treatments (Horst et al., 2016; Mei
et al., 2016a). One solution to this problem is the use of additional KI in the application (Ngo et al., 2002). However, further studies are required to examine the
Applications of silver diamine fluoride in management of dental caries
677
Figure 25.1 Black staining of SDF-treated teeth (Chu et al., 2014). SDF, Silver diamine
fluoride.
effectiveness of this combination treatment. To date many clinical studies have
been carried out to investigate the anticaries effects of SDF treatment on coronal
caries in children and adults, and root caries in the elderly (Contreras et al., 2017),
and these are summarized in Tables 25.1 and 25.2.
25.3.1 Management of coronal caries in children
As SDF application is simple and not costly and is suitable to be used for children
with special health care needs (Wright and White, 2017), and for children from
underprivileged and remote areas, in order to treat early childhood caries (ECC)
(Chu and Lo, 2008b; Contreras et al., 2017; Fung et al., 2013; Yee et al., 2009;
Cheng, 2017; Gold, 2017). One review concluded that due to a large number of
caries-affected preschool children and limited resources, 38 wt.% SDF is the best
choice to be used for ECC in China (Chen et al., 2018).
SDF treatment can be used as an alternative for restorative treatments. The use
of 38 wt.% SDF for arresting cavities in preschool children has been reported to be
safe (Milgrom et al., 2018). Further, clinical studies found that deciduous caries
could be arrested with a single spot application with 38 wt.% SDF without restorative intervention (Chu et al., 2002; Yee et al., 2009). Compared to other noninvasive, cariostatic treatments, SDF treatment has higher caries-arresting efficacy. It
was found that a single annual application of 38 wt.% SDF arrested and prevented
more caries in deciduous teeth than three times weekly application of 5 wt.%
sodium fluoride varnish (Lo et al., 2001). Further, another study found that topical
application of 30 wt.% SDF led to a higher caries arrest rate in cavitated deciduous
teeth than using atraumatic restorative technique (ART) with glass ionomer cement
(GIC) (Dos Santos et al., 2012).
Table 25.1 Clinical effects of silver diamine fluoride (SDF) applications on coronal caries in deciduous and permanent teeth.
References
Cariostatic
effects
studied
Subjects/dentitions
Durations
Groups compared
Main findings
McDonald
and
Sheiham
(1994)
Arrest
52 Children (29 years old)/
deciduous
18
Gotjamanos
(1997)
Arrest
356
Months
Caries in progress (%):
Gp 1: 46.5%
Gp 2: 26.6%
Gp 3: 5.2%
Gp 4: 11.1%
Gp 5: 53.0%
Caries can be treated in a nontraumatic way
SDF treatment for deep caries does not affect pulp
vitality
Lo et al.
(2001)
Arrest and
prevention
55 Carious deciduous teeth
(from 6 to 13 years old)/
deciduous
375 Children (35 years
old)/deciduous
Gp 1: SnF2
Gp 2: SDF/SnF2
Gp 3: Minimal preparation 1 SDF/
SnF2 1 composite resin
Gp 4: Minimal preparation 1 composite
resin
Gp 5: no treatment
55 Carious dentine treated with 50.9%
SDF and GIC
Gp 1: annual 38% SDF 1 carious tissue
removal
Gp 2: annual 38% SDF
Gp 3: 3-monthly NaF (5%) 1 carious
tissue removal
Gp 4: 3-monthly NaF (5%)
Gp 5: no treatment
Chu et al.
(2002)
Arrest
375 Children (35 years
old)/deciduous
30
Mean no. of new carious surfaces/arrest carious
surfaces:
Gp 1: 0.4/2.8
Gp 2: 0.4/3.0
Gp 3: 0.8/1.7
Gp 4: 0.6/1.5
Gp 5: 1.2/1.0
1. 38% SDF is more effective than 5% NaF in
preventing and arresting caries
2. Carious tissue removal is unnecessary for
SDF treatment
Mean no. of arrest carious surfaces:
Gp 1: 2.5
Gp 2: 2.8
Gp 3: 1.5
Gp 4: 1.5
Gp 5: 1.3
SDF is effective in caries arrest in deciduous teeth
Months
18
Months
Months
Gp 1: annual 38% SDF 1 carious tissue
removal
Gp 2: annual 38% SDF
Gp 3: 3-monthly 5% NaF 1 carious tissue
removal
Gp 4: 3-monthly NaF (5%)
Gp 5: no treatment
Llodra et al.
(2005)
Arrest and
prevention
425 Children ( $ 6 years
old)/deciduous and
permanent first molars
36
Braga et al.
(2009)
Arrest
22 Children/permanent first
molars
30
Yee et al.
(2009)
Arrest
976 Children (39 years
old)/deciduous
24
Zhi et al.
(2012)
Arrest
212 Children (34 years
old)/deciduous
24
Dos Santos
et al.
(2012)
Liu et al.
(2012a)
Arrest
91 Children/deciduous
12
Months
Gp 1: CTT
Months
Months
Months
Months
Prevention
501 Children (mean age 9.1
years)/permanent first
molars
Gp 1: biannual 38% SDF
Gp 2: no treatment ( 3 min)
24
Months
Gp 2: 3-time weekly 10% SDF
Gp 3: GIC sealant ( 3 min)
Gp 1: 38% SDF/tannic acid
Gp 2: 38% SDF
Gp 3: 12% SDF
Gp 4: no treatment ( 2 min)
Gp 1: annual 38% SDF
Gp 2: biannual 38% SDF
Gp 3: annual GIC
Gp 1: 30% SDF
Gp 2: GIC ( 3 min)
Gp 1: resin sealant
Gp 2: biannual 5% NaF
Gp 3: annual 38% SDF
Gp 4: placebo control
Mean no. of new carious surfaces (deciduous/
permanent first molars):
Gp 1: 0.29/0.37
Gp 2: 1.43/1.06
SDF is effective for caries reduction in deciduous
teeth and first permanent molars
All treatments are effective in control occlusal
incipient caries
Mean no. of arrest carious surfaces:
Gp 1: 2.2
Gp 2: 2.1
Gp 3: 1.5
Gp 4: 1.0
38% SDF is more effective than 12% SDF in caries
arrest
Caries arrest rates:
Gp 1: 79%
Gp 2: 91%
Gp 3: 82%
Increasing application frequency to biannual can
enhance the caries arrest rate
SDF was more effective than GIC (Relative risk
(RR) 5 38.6%) for caries arrest
Proportions of pit/fissure sites with dentine caries:
Gp 1: 1.6%
Gp 2: 2.4%
Gp 3: 2.2%
Gp 4: 4.6%
All treatments are effective in preventing pit and
fissure caries in permanent molars
(Continued)
Table 25.1 (Continued)
References
Cariostatic
effects
studied
Subjects/dentitions
Durations
Groups compared
Main findings
Monse et al.
(2012)
Prevention
704 Children (68 years
old)/permanent first
molars
18
One-time 38% SDF application cannot prevent caries
development on permanent first molar, while GIC
sealant can
Chu et al.
(2014)
Arrest
Duangthip
et al.
(2016)
Arrest
Gp 1: SDF (38%)
Gp 2: GIC sealant
Gp: no treatment
With or without tooth-brushing program
( 1 min)
Patient with rampant caries was treated
with 38% SDF, followed by
provisional crown restoration
Gp 1: annual 38% SDF
Gp 2: 3-weekly 38% SDF
Gp 3: 3-weekly 5% NaF ( 10 s)
Fung et al.
(2016)
Arrest
Duangthip
et al.
(2017)
Arrest
A 14-year-old Chinese boy/
permanent (rampant
caries)
304 Children (34 years
old)/deciduous
Months
18
Months
888 Children (34 years
old)/deciduous
18
371 Children (34 years
old)/deciduous
30
Months
Months
Gp 1: annual 12% SDF
Gp 2: biannual 12% SDF
Gp 3: annual 38% SDF
Gp 4: biannual 38% SDF
Gp 1: annual 38% SDF
Gp 2: 3-weekly 38% SDF
Gp 3: 3-weekly 5% NaF ( 10 s)
Good prognosis with pain relief
Caries arrest rates:
Gp 1: 40%
Gp 2: 35%
Gp 3: 27%
Annual or 3-weekly applications of 38% SDF is
more effective in caries arrest than 3-weekly
application of 5% NaF varnish
Caries arrest rates:
Gp 1: 50%
Gp 2: 55%
Gp 3: 64%
Gp 4: 74%
SDF is more effective in cares arrest at 38% than
12% and when applied biannually rather than
annually
Caries arrest rates:
Gp 1: 48%
Gp 2: 33%
Gp 3: 34%
Fung et al.
(2018)
Arrest
Milgrom
et al.
(2018)
Arrest
888 Children (34 years
old)/deciduous
30
66 Children (26 years old)/
deciduous
1421
Days
CTT, Cross-tooth-brushing technique; GIC, glass ionomer cement.
Months
Gp 1: annual 12% SDF
Gp 2: biannual 12% SDF
Gp 3: annual 38% SDF
Gp 4: biannual 38% SDF
Gp 1: 38% SDF
Gp 2: placebo
Annual application of 38% SDF is more effective
than 3-weekly applications of SDF or NaF varnish
Caries arrest rates:
Gp 1: 55.2%
Gp 2: 58.6%
Gp 3: 66.9%
Gp 4: 75.7%
SDF is more effective in cares arrest at 38% than
12% and when applied biannually rather than
annually
Averaged proportion of arrested caries lesions:
Gp 1: 72%
Gp 2: 5%
No harms were observed
Topical 38% SDF is effective and safe in arresting
cavities in preschool children
Table 25.2 Clinical effects of silver diamine fluoride (SDF) applications on caries in roots of the elderly.
References
Cariostatic
effects
studied
Subjects/dentitions
Durations
Groups compared
Main findings
Tan et al.
(2010)
Prevention
306 Elders (mean age
78.8 6 6.2 years old)/
permanent roots
3 Years
Zhang
et al.
(2013)
Arrest and
prevention
277 Elders (6089 years old)/
permanent roots
24
Gp 1: OHI
Gp 2: OHI 1 3-monthly
CHX
Gp 3: OHI 1 3-monthly
NaF (5%)
Gp 4: OHI 1 annual 38%
SDF
Gp 1: OHI
Gp 2: OHI 1 annual 38%
SDF
Gp 3: OHI 1 annual 38%
SDF 1 biannual OHE
Li et al.
(2016)
Arrest
83 Elders (mean age 72.2 6 5.8
years old)/permanent roots
30
New root caries surfaces:
Gp 1: 2.5
Gp 2: 1.1
Gp 3: 0.9
Gp 4: 0.7
CHX, 5% NaF and 38% SDF were all more
effective than OHI alone
New/arrested root caries surfaces:
Gp 1: 1.33/0.04
Gp 2: 1.00/0.28
Gp 3: 0.70/0.33
Annual 38% SDF together with biannual OHE
is effective in preventing and arrest caries
Root caries arrest rates:
Gp 1: 45%
Gp 2: 90%
Gp 3: 93%
1. 38% SDF application with or without KI
application is effective in root caries
arrest
2. KI application does not reduce black
staining of SDF in the long term
Months
Months
CHX, Chlorhexidine; KI, potassium iodide; OHE, oral health education; OHI, oral hygiene instruction.
Gp 1: no treatment
Gp 2: 38% SDF
Gp 3: 38% SDF/KI
Applications of silver diamine fluoride in management of dental caries
683
SDF can be used in conjunction with other dental materials for the management
of caries in deciduous teeth. McDonald and Sheiham (1994) used SDF together
with SnF2 as a reducing agent after minimal cavity preparation of caries in deciduous teeth, followed by the restoration with composite resin (CR). It was found that
this combination treatment led to less carious lesions in progression compared to
SnF2 treatment or CR restoration alone. Further, a systematic review proposed that
SDF can be added to the set of other noninvasive methods to treat caries lesions in
deciduous teeth, such as the Hall crown technique and sealing lesions with accessible margins to optimize the cariostatic efficacy (Horst, 2018).
Different application frequencies, concentrations (1238 wt.% SDF), and procedures of SDF treatments have been used in clinical practice (Elevate Oral Care,
2016; Horst et al., 2016; Crystal and Niederman, 2016; Fung et al., 2013; SDI,
2016). Several randomized clinical trials found that biannual application of SDF led
to a higher caries arrest rate in deciduous teeth than annual or three times weekly
SDF applications. Further, the use of 38 wt.% SDF showed higher caries arrest rates
in deciduous teeth than the use of 12 wt.% SDF (Yee et al., 2009; Zhi et al., 2012;
Fung et al., 2016, 2018; Duangthip et al., 2016, 2017). Therefore based on the current evidence, the biannual application of 38 wt.% SDF is the most effective
protocol.
Regarding the procedures of SDF treatment the consensus is that the removal of
carious tissue before the SDF topical application is unnecessary (Lo et al., 2001;
Dos Santos et al., 2012). In 2017 the American Academy of Pediatric Dentistry
announced a guideline of using 1 minute 38 wt.% SDF application followed by gentle air-drying in arresting carious deciduous teeth. They proposed that this procedure can lead to the best cariostatic efficacy of SDF treatment. Further, they
expected similar cariostatic efficacy of SDF treatment in the carious permanent
teeth by using the same procedures (Crystal et al., 2017).
25.3.2 Management of coronal caries in adults
SDF treatment can arrest incipient enamel caries in permanent teeth. It has been
reported that the application of 10 wt.% SDF exerted a comparable caries-arrest
efficacy to that of GIC sealant treatment or tooth-brushing in first permanent molars
(Braga et al., 2009). Further, SDF can be used for adults who cannot tolerate conventional treatments, or for those with extreme risks of caries such as salivary dysfunction (Horst et al., 2016; Chu and Lo, 2008b; Burgess and Vaghela, 2018). A
typical example demonstrating the benefits of the application of SDF to arrest rampant dental caries in permanent teeth was reported in 2014 (Chu et al., 2014). The
patient suffered from chronic oral graft versus host disease following bone marrow
transplantation. One side effect of the disease made it painful for him when moving
his mouth, and therefore he neglected oral hygiene, finally leading to multiple dental decay. In this case SDF was used not only for arresting the caries but also for
relieving the pain resulting from hypersensitivity. Also stainless steel crowns were
needed to restore the chewing function. The prognosis for the patient was good, and
the application of SDF for similar situations was recommended. A treatment involving the application of SDF on cavitated lesions followed by restoration with GIC,
684
Advanced Dental Biomaterials
called silver modified ARTs (SMART), was introduced. In 2016 a case reported
that when SMART was applied on cavitated caries of a 71-year-old female, this
resulted in a positive outcome (Fa et al., 2016).
SDF treatment can prevent the development of dental caries in permanent teeth.
A clinical trial reported that the biannual application of SDF could not only arrest
active caries in deciduous teeth and first permanent molars, but also prevent the
development of new caries (preventive fraction in deciduous dentition: 79.7%; preventive fraction on permanent first molar: 65.0%) (Llodra et al., 2005). Another
study reported that the annual application of 38 wt.% SDF is effective in preventing
caries development in the fissures of permanent molars (Liu et al., 2012a). SDF
may also be able to prevent secondary caries. An in vitro study proposed that SDF
application prior to the application of GIC or CR increased the resistance of the
restorations to secondary caries (Mei et al., 2016b). Another in vitro study used
SDF in conjunction with casein phosphopeptideamorphous calcium phosphatemodified GIC, and the development of secondary caries was also successfully
inhibited (Zhao et al., 2017b).
25.3.3 Management of root caries in the elderly
Due to the advancements in medicine and dentistry, people not only live longer, but
also maintain more of their teeth into their older ages. This inevitably results in
more caries, especially root caries, in this elderly population (Gluzman et al.,
2013). The prevalence of root caries in the elderly has been reported to range from
29% to 89%, which increases with age (Gluzman et al., 2013; Li et al., 2016).
Therefore root caries is a worldwide pandemic in need of an effective preventive
treatment.
SDF treatment can effectively arrest and prevent root caries. It has been shown
that the annual application of 38 wt.% SDF is more effective in preventing new
root caries than merely giving oral hygiene instruction (OHI) alone (Tan et al.,
2010). Another study found that the annual application of SDF in conjunction with
biannual OHI was effective in preventing and arresting root caries (Zhang et al.,
2013). In 2013 a review concluded that the annual application of 38 wt.% SDF is
the best choice for preventing primary root caries, prevailing over other preventive
agents like chlorhexidine (CHX) and sodium fluoride (Gluzman et al., 2013). In
addition, in 2017 a review concluded that SDF is the most cost-effective preventive
treatment for root caries (Schwendicke and Gostemeyer, 2017).
An annual application of SDF followed by the addition of KI can also effectively
arrest root caries (Li et al., 2016). It has been proposed that the application of KI
following SDF treatment will remove excessive Ag1 by forming white AgI, thereby
eliminating the black staining of the treated lesion (Ngo et al., 2002). Further, topical application of SDF with the addition of KI has been proposed to have a desensitizing effect which may be another benefit of SDF treatment on root caries (Craig
et al., 2012; Castillo et al., 2011). However, the long-term camouflaging effect and
anticaries efficacy of this combination treatment are still questionable, and further
studies are required.
Applications of silver diamine fluoride in management of dental caries
25.4
685
Cariostatic mechanism of silver diamine fluoride
Even though topical SDF application has been used for preventing and arresting
dental caries across the age spectrum for almost 50 years, the cariostatic mechanism
of SDF remains obscure (Mei et al., 2017). The effects of SDF on dental mineral,
cariogenic bacteria, and dentinal organic content, as shown in Table 25.3, have
been extensively investigated in order to understand the cariostatic mechanism of
SDF. Further, as SDF treatment involves the effects of fluoride and silver, cariostatic effects of fluoride and silver in SDF have been proposed (Rosenblatt et al.,
2009; Zhao et al., 2017a; Yamaga et al., 1972).
25.4.1 Cariostatic effects of silver diamine fluoride on dental
mineral
The interaction between SDF and dental mineral has been proposed to be
(Rosenblatt et al., 2009; Yamaga et al., 1972):
Ca10 ðPO4 Þ6 ðOHÞ2 1 AgðNH3 Þ2 F ! CaF2 1 Ag3 PO4 1 NH4 OH
(25.1)
As CaF2 and Ag3PO4 are formed following topical SDF treatment, both Ca21
and PO32
4 released from demineralizing dental mineral can be preserved (Yamaga
et al., 1972). Studies have reported that higher percentages of calcium and phosphate with less mineral loss were detected in demineralized dentine treated with
SDF than those without treatment (Mei et al., 2013d; Chu et al., 2012). An ex vivo
study has also reported that a highly remineralized zone abundant in calcium and
phosphate was found on the SDF-treated dentinal carious lesion (Mei et al., 2014b).
Further, the preservation of calcium and phosphate can increase the mineral content
of the treated lesion, leading to higher microhardness. It was found that the application of SDF increased the mineral density of treated incipient enamel caries in permanent premolars (Punyanirun et al., 2018), and the microhardness of the SDFtreated caries was higher than that of the active carious lesions (Chu and Lo, 2008a;
Mei et al., 2013d).
It has been reported that SDF-treated teeth could adsorb Ca21 from a remineralization solution, and inhibit the Ca21 release from enamel treated with SDF when in
demineralization solution (Zhao et al., 2017a). Further, another study reported that
a higher fluoride uptake was found in SDF-treated dentine (Knight et al., 2009).
These findings are consistent with the formation of CaF2 following SDF treatment
(Yamaga et al., 1972). CaF2 was found in hydroxyapatite (HAP) powder, enamel
powder, and dentine powder mixed with SDF (Lou et al., 2011; Zhao et al., 2017a).
However, another study found that the amount of CaF2 formed following SDF treatment dropped drastically after immersion in artificial saliva (Suzuki et al., 1974).
This indicates that CaF2 may not be directly involved in the demineralization inhibition effect of SDF treatment.
Table 25.3 Cariostatic effects of silver diamine fluoride (SDF) on dental mineral, cariogenic bacteria, and dentinal organic content.
Cariostatic effects of SDF on dental mineral
Reference
Methodologies
Main findings
Chu et al.
(2008a)
Carious deciduous teeth treated with either 38% SDF or 5% NaF were
extracted to undergo KHN measurement
Lou et al.
(2011)
HAP powders mixed with 38% SDF, NaF, or AgNO3 were inspected
with SEM, EDX, and ED
Liu et al.
(2012b)
Mei et al.
(2013d)
Sound premolars treated with AgF, KF, AgNO3 or water, were subjected
to demineralization for 7 days before being inspected with micro-CT
Dentine caries generated by multispecies biofilms (Streptococcus
mutans, Streptococcus sobrinus, Lactobacillus acidophilus,
Lactobacillus rhamnosus, and Actinomyces naeslundii) were treated
with either 38% SDF or water and were incubated in the artificial
mouth for 21 days
Carious deciduous teeth treated with 38% SDF were inspected with
micro-CT, EDX, SEM, and TEM
Calcium phosphate with different SDF concentrations (0.38, 1.52, 2.66,
3.80 mg/mL) were incubated at 37 C for 24 h. The shape and
organization of the crystals were examined by bright-field TEM and
electron diffraction. Unit cell parameters of the obtained crystals were
determined with powder XRD. The vibrational and rotational modes
of phosphate groups were analyzed with Raman microscopy
Incipient caries on proximal surfaces of premolars were treated with
38% SDF before undergoing bacterial pH-cycling for 5 days. microCT then was used for mineral density evaluation
The median KHN of arrested lesions (range, 2046 or 196451 MPa)
were greater than those of soft lesions (range, 520 or
49196 MPa) in the outer 25200 µm
Compounds formed on treated surfaces:
SDF: CaF2 and Ag(s)
NaF: NaF globules
AgNO3: Ag3PO4 (turns black immediately)
Topical applications of AgF and KF inhibited enamel demineralization,
while AgNO3 application did not
1. 38% SDF inhibits multispecies cariogenic biofilm formation on
dentine carious lesions
2. The hardness and percentages of calcium and phosphorus of SDFtreated samples from the outermost 50 µm were higher
Mei et al.
(2014b)
Mei et al.
(2017)
Punyanirun
et al. (2018)
A highly remineralized zone rich in calcium and phosphate was found
on the 38% SDF-treated cavitated dentinal lesion
The results suggested that SDF reacted with calcium and phosphate
ions and produced fluorohydroxyapatite (FHH)
Compared to the use of 1000 ppm fluoride toothpaste alone, the
adjunctive use of 38% SDF enhances the remineralization of initial
carious lesions based on mineral density, depth, and remineralization
percentage
(Continued)
Table 25.3 (Continued)
Cariostatic effects of SDF on dental mineral
Reference
Methodologies
Main findings
Cariostatic effects of SDF on cariogenic bacteria
Knight et al.
(2005)
Knight et al.
(2007)
Knight et al.
(2009)
de Almeida Lde
et al. (2011)
Chu et al.
(2012)
Mei et al.
(2013b)
Shah et al.
(2013)
Targino et al.
(2014)
Demineralized dentine discs treated with 50.9% SDF, 50.9% SDF/KI
and KI were incubated in medium of S. mutans for 14 days.
Afterwards, optical density of the medium chambers was measured to
determine bacterial penetration and growth
Dentine discs with or without demineralization, were treated with 50.9%
SDF/KI. Next, they were incubated with S. mutans for 14 days.
EPMA and SEM were then used to inspect the samples. Bacterial
growth was monitored by taking optical density readings
Demineralized dentine discs treated with either 50.9% SDF or 50.9%
SDF/KI were incubated in S. mutans before being inspected by
scanning microscopy (SEM) and EPMA
Antibacterial effects of different concentrations of SDF were studied
using an agar diffusion method
Demineralized dentine blocks were incubated with either S. mutans or A.
naeslundii to be treated with 38% SDF. Lesions were then assessed
by MHT, EDX, and FTIR
Carious lesions were created in dentine blocks by inoculating with dualspecies biofilm (S. mutans and L. acidophilus). They were then
treated with either 38% SDF or water before being incubated at 37 C
for 7 days. The biofilms were evaluated by CFU, SEM, and confocal
laser scanning microscopy (CLSM), while the carious lesion was
inspected with XRD, FTIR, and immune-labeling
S. mutans counts in the mouths of children treated with 38% SDF,
fluoride varnish or APF gel. All subjects were evaluated at 72 h, and
6, 12, and 18 months of follow-up
Evaluate the antimicrobial and cytotoxic activity of 38% SDF. The MIC
was evaluated by the spectrophotometric microdilution method and
turbidity. The MBC was evaluated in brain heart infusion plates
S. mutans migrated through all dentine discs. However, the samples
treated with 50.9% SDF and SDF/KI had significantly lower optical
densities
SDF/KI can inhibit biofilm formation composed of S. mutans
The inhibition of S. mutans might be due to the presence of silver and
fluoride in the outer layer (up to 450 µm) of SDF and SDF/KItreated samples, which make it more resistant to demineralization
Both 12% and 30% can inhibit S. mutans
1. 38% SDF possesses antimicrobial activity against cariogenic biofilm
of S. mutans or A. naeslundii, which inhibit the demineralization
2. The hardness and percentages of calcium and phosphorus of SDFtreated samples
SDF had antimicrobial activity against the cariogenic biofilms
composed of S. mutans and L. acidophilus
38% SDF is more effective in inhibiting S. mutans than fluoride
varnish and APF gel in vivo
The MIC and MBC for SDF were 33.33 6 14.43 and 50.0 µg/mL,
respectively
(Continued)
Table 25.3 (Continued)
Cariostatic effects of SDF on dental mineral
Reference
Methodologies
Main findings
Hamama et al.
(2015)
Dentine discs infected with S. mutans were treated with 50.9% SDF/KI.
The discs were then fractured into two halves, stained with
fluorescent LIVE/DEAD stain and observed using confocal laserscanning microscopy
S. mutans biofilm demineralized enamels were treated with water, 38%
SDF, APF, AHF, AHF 1 CPC, or 0.2% CHX before being incubated
for 2 days. Numbers of viable microorganisms in the biofilms were
counted
The use of the SDF/KI is effective in reducing the numbers of S.
mutans in dentinal tubules
Savas et al.
(2015)
38% SDF showed the highest antibacterial activity over other
treatments
Cariostatic effects of SDF on dentinal organic content
Mei et al.
(2012)
Mei et al.
(2013c)
The inhibitory effects of 12%, 30%, 38% SDF, NaF, and AgNO3 on
MMPs were studied using MMP assay kits
Demineralized dentine blocks were treated with 38% SDF, 10% NaF,
42% AgNO3, and water. They were then subjected to pH cycling for
8 days before being inspected with SEM, XRD, micro-CT, and
spectrophotometry with a hydroxyproline assay
Mei et al.
(2014a)
The inhibitory effects of 12%, 30%, 38% SDF, NaF, and AgNO3 on
cathepsins were studied using cathepsin assay kits
Thanatvarakorn
et al. (2016)
Bovine dentine discs were treated with 38% SDF, KF, APF, ZnF2/HCl
and ZF2 before being demineralized. TMR and optical microscope
were used to examine the antidemineralization and anticollagen
degradation abilities, respectively
Dentine discs treated with 25% AgNO3 followed by 5% NaF, 38% SDF
or water were subjected to pH-cycling for 8 days before being
inspected with SEM, XRD, X-ray microtomography, and
spectrophotometry with a hydroxyproline assay
Zhao et al.
(2017c)
Inhibitory effect of SDF on MMPs increased with concentration. SDF
had more inhibition on MMPs than solutions of NaF and AgNO3
1. Groups treated with 38% SDF and 42% AgNO3 had significantly
less hydroxyproline liberated from the dentine matrix than groups F
and W (P , .01)
2. 38% SDF can inhibit demineralization and preserved collagen from
degradation
1. The solutions containing Ag1 have significantly higher inhibitory
effect than the solutions containing F2 only (P , .01)
2. SDF solution at all 3 tested concentrations significantly inhibited the
activity of cathepsin
38% SDF and ZnF2/HCl exerted best preservative effects against
demineralization
25% AgNO3 followed by 5% NaF or 38% SDF application can
preserve dentinal collagen and result in lower lesion depths
AHF, Ammonium hexafluorosilicate; APF, acidulated phosphate fluoride; CFU, colony forming units; CHX, chlorhexidine; CPC, cetylpyridinium chloride; ED, electron diffraction; EDX, energy-dispersive X-ray analysis;
EPMA, electron probe microanalysis; FTIR, Fourier transform infrared spectroscopy; HAP, hydroxyapatite; KHN, Knoop hardness number; KI, potassium iodide; MBC, minimum bactericide concentration; MHT, microhardness
testing; MIC, minimum inhibition concentration; micro-CT, microcomputed tomography; MMP, matrix metalloproteinase; TEM, transmission electron microscopy; TMR, transverse microradiography; XRD, X-ray diffraction.
Applications of silver diamine fluoride in management of dental caries
689
As the CaF2 formed on a dental surface is unstable (Yamaga et al., 1972), CaF2
will gradually dissociate. It has been proposed that CaF2 can act as reservoir of F2
for further formation of fluorapatite (FAP) through the following interactions (ten
Cate, 2013; Vogel, 2011; Yamaga et al., 1972):
CaF2 ! Ca21 1 2F2
(25.2)
Ca10 ðPO4 Þ6 ðOHÞ2 1 2F2 ! Ca10 ðPO4 Þ6 F2 1 2OH2
(25.3)
10Ca21 1 2F2 1 6PO32
4 ! Ca10 ðPO4 Þ6 F2
(25.4)
After the dissociation of CaF2 [Eq. (25.2)], the free F2 adsorbs onto enamel and
further interacts with dental mineral or attracts Ca21 and PO32
4 in saliva to form
FAP [Eqs. (25.3) and (25.4)]. Subsequently, an acid-resistant FAP surface can protect the dental surface against acid attack (Featherstone, 2008). Mei et al. (2017)
found that fluorohydroxyapatite (FHA), which is partial FAP-substituted HAP, was
formed in the calcium phosphate [Ca3(PO4)2] medium incubated with SDF
(0.383.8 mg/mL) (Mei et al., 2017). As FHA is more stable than CaF2 in solution,
they proposed that FHA formation is the major demineralization inhibitory mechanism of SDF treatment.
Ag3PO4 is a yellow, insoluble compound (solubility 5 6.5 3 1024 g/100 mL)
(Lewis, 1920), which can be gradually reduced to black metallic silver after being
exposed to light and heat (Lou et al., 2011). Metallic silver, reduced from photosensitive Ag3PO4, was found in HAP powder mixed with SDF (Lou et al., 2011).
However, even though Ag3PO4 was found in enamel powder mixed with SDF, it
was replaced by AgCl and silver thiocyanate after being immersed in artificial
saliva (Suzuki et al., 1974). Another study also found AgCl rather than Ag3PO4 in
demineralized dentine treated with SDF (Mei et al., 2013c). These findings might
be due to the solubility of AgCl (solubility 5 8.9 3 1025 g/100 mL) being lower
than that of Ag3PO4 (solubility 5 6.5 3 1024 g/100 mL), and therefore Ag3PO4
reacts with alkali chlorides in solution to form AgCl (Zhao et al., 2017c). Further
studies are required to confirm that silver compounds are formed following SDF
topical treatment on dental mineral in clinical practice.
The demineralization inhibition effect of SDF treatment is mainly associated
with the F2 in SDF (Horst et al., 2016). A study using microcomputed tomography
found that, after artificial caries-like acidic challenge, the difference between the
depth of an enamel lesion treated with AgNO3 and the depth of an enamel lesion
treated with deionized water was negligible, whereas KF and AgF treatments
showed significant inhibitory effects on enamel demineralization (Fig. 25.2) (Liu
et al., 2012b).
690
Advanced Dental Biomaterials
Figure 25.2 Typical micro-CT images of tooth blocks treated with (a) AgF; (b) KF; (c)
AgNO3; (d) De-ionized water (Liu et al. 2012b). No demineralization lesions were shown in
AgF and KF treated tooth blocks, whereas, demineralized lesions were observed in AgNO3
and de-ionized water treated tooth bocks.
25.4.2 Cariostatic effects of silver diamine fluoride on cariogenic
bacteria
SDF has strong antibacterial properties (Zhao et al., 2017a). The minimum inhibition concentration and the minimum bactericide concentration of SDF are
33.33 6 14.43 and 50.0 µg/mL, respectively (Targino et al., 2014). It was found that
both 12 and 38 wt.% SDF have pronounced antibacterial capacities (de Almeida
Lde et al., 2011). Further, 38 wt.% SDF has been proposed to be the most potent
antibacterial agent against Streptococcus mutans compared to other antibacterial
agents like sodium fluoride (NaF), acidulated phosphate fluoride (APF), ammonium
hexafluorosilicate, and CHX (Shah et al., 2013; Savas et al., 2015). The application
Applications of silver diamine fluoride in management of dental caries
691
Figure 25.3 Confocal laser-scanning micrographs of the growth of multispecies cariogenic
biofilm on dentine treated with (A) SDF and (B) deionized water after 14 days. The red-togreen ratio represents ratio of dead-to-live bacteria. Higher ratio was shown on the SDFtreated dentine than on the deionized water-treated dentine (Mei et al., 2013d). SDF, Silver
diamine fluoride.
of 38 wt.% SDF can reduce the amounts of bacteria in biofilms composed of cariogenic bacteria like S. mutans, Lactobacillus acidophilus, and Actinomyces naeslundii (Fig. 25.3) (Mei et al., 2013b,d; Chu et al., 2012). In addition, SDF treatment
followed by KI application has also been reported to have pronounced antibacterial
capacity, which can reduce the number of S. mutans in biofilm and in dentinal
tubules (Knight et al., 2005, 2007, 2009; Hamama et al., 2015).
It has been proposed that with high fluoride concentrations in SDF products
(141660,000 ppm F2) (Fung et al., 2013; SDI, 2016), F2 can bind to bacterial
cellular components and influence the enzymes in charge of glycolysis, such as
enolase and proton-extruding adenosine triphosphatase (Targino et al., 2014;
Rosenblatt et al., 2009), leading to the inhibition of biofilm formation (Zhao et al.,
2017a). On the other hand, it has been proposed that 1040 ppm of Ag1 is sufficient to destroy most of the cariogenic bacteria (Lansdown, 2006). It was found that
20 ppm Ag1 was lethal to S. mutans after contact of 34 hours, while 200 ppm
Ag1 is instantaneously lethal to S. mutans (Thibodeau et al., 1978). It should be
emphasized that it is the Ag1 that exerts the antimicrobial effects, whereas the
metallic silver is relatively inert (Peng et al., 2012).
The antibacterial actions of Ag1 include cell wall destruction, disturbance of
bacterial enzymes, and hindrance in microbial DNA replication (Rosenblatt et al.,
2009; Targino et al., 2014). Further, it has been proposed that the silver-killed bacteria (termed “zombies”) can act as a reservoir of Ag1 to kill living bacteria
(Wakshlak et al., 2015). The pivotal antibacterial reaction is associated with the
interaction of Ag1 with a thiol group in bacteria, which can be simplified as:
A=N 2 SH 1 AgX ! A=N 2 S 2 AgX 1 HX
(25.5)
692
Advanced Dental Biomaterials
In Eq. (25.5) A/N represents amino (A) or nucleic (N) acids, while SH represents
a thiol group and X represents an anion such as diamine fluoride (Rosenblatt et al.,
2009). By binding Ag1 to SH groups, the activities of bacterial enzymes will be
inhibited. Further, by binding Ag1 to the S222 in cell membrane, the permeability
of the membrane will be increased, leading to cell perturbation. Moreover, the
attachment of Ag1 to guanine will cause the inhibition of the DNA replication process (Peng et al., 2012). It has been proposed that the oligodynamic action against
bacteria enables Ag1 to consistently elicit antimicroorganism effects even after
binding (Yamaga et al., 1972).
25.4.3 Cariostatic effects of silver diamine fluoride on organic
content of dentine
SDF can inhibit the degradation of dentine collagen (Mei et al., 2018). It has been
reported that deciduous dentine treated with SDF led to smoother surfaces with
fewer collagen fibers exposed than active dentine lesions (Fig. 25.4) (Mei et al.,
2014b). Further, it has been reported that more dentine collagen under an acidic
challenge is preserved by SDF treatment than by NaF, KF, or APF treatment
(Thanatvarakorn et al., 2016; Mei et al., 2013c). Another study reported that 25 wt.
% AgNO3 treatment followed by 5 wt.% NaF varnish on dentine collagen degradation is comparable to that of 38 wt.% SDF treatment (Zhao et al., 2017c).
SDF can inhibit the proteolytic activities of matrix metalloproteinases (MMPs)
and cysteine cathepins, the proteolytic enzymes in charge of dentine collagen degradation (Mei et al., 2012, 2014a). The inhibitory effect of 38% SDF on MMPs has
been reported to be significantly greater than 10% NaF and 42% AgNO3 that have
equivalent concentrations of F2 and Ag1 (Mei et al., 2012), whereas the inhibitory
effect on cathepsins is mainly due to the effect of Ag1 (Mei et al., 2014a).
Furthermore, Ag1 has been suggested to preserve dentine collagen by inactivating
the catalytic functions of bacteria after interacting with a reactive side chain of their
collagenase (Mei et al., 2013c). F2 and Ag1 in SDF have been proposed to have a
synergistic effect on preserving dentine collagen (Mei et al., 2018).
25.5
Safety of silver diamine fluoride treatment
There is a broad concentration range of commercial SDF products available on the
market (Fung et al., 2013; SDI, 2016). The SDF product with the lowest concentration (Caristop 12%, Biodinamica Quı́mica E Farmacéutica Ltda, 1416 ppm F2)
contains a fluoride concentration similar to that of a fluoride dentifrice
(1001500 ppm F2) (Mohammed et al., 2014). The SDF product with the highest
concentration (Riva Star, SDI Ltd, 60,000 ppm F2) contains fluoride at a concentration much higher than that of fluoride varnish (B22,000 ppm F2) (Hazelrigg et al.,
2003). Therefore safety concerns about the extremely high F2 concentrations in
Applications of silver diamine fluoride in management of dental caries
693
Figure 25.4 Scanning electron microscopy images of (A) SDF-treated dentine surface and
(B) active dentine caries (Mei et al., 2014b). SDF, Silver diamine fluoride.
SDF products have been expressed (Gotjamanos, 1997; Gotjamanos and Afonso,
1997; Gotjamanos and Orton, 1998).
The possibility of causing fluorosis in children following application with highconcentration SDF has been raised by several studies (Gotjamanos and Orton,
1998; Gotjamanos, 1997; Gotjamanos and Afonso, 1997). However, the Dental
Services of the Health Department of Western Australia has asserted that there is
no report indicating that any fluorosis has developed in patients (Shah et al., 2014).
According to FDA guidelines, the average lethal dose (LD50) of SDF by oral and
subcutaneous administrations in animal studies are 520 and 380 mg/kg, respectively
(Horst et al., 2016). It has been proposed that the concentrations of SDF products
used in clinical practice are hundreds of times less than the lethal dose of SDF by
oral administration (520 mg/kg) (Horst et al., 2016). Further, a clinical study suggested that the use of SDF poses no toxic risk with reference to the US
694
Advanced Dental Biomaterials
Environmental Protection Agency oral reference dose (Vasquez et al., 2012).
However, allergy to silver might be a contraindication of treatment, which may
cause gingivitis or mucositis (Horst et al., 2016). Some patients have been reported
to have tooth pain, gum pain, gum swelling, and gum bleaching after being treated
with SDF (Duangthip et al., 2018). Therefore a high-concentration SDF should still
be used with caution.
25.6
Conclusion
In conclusion, SDF is an efficient, affordable, effective, and safe cariostatic agent,
which can be used in the management of dental caries in both deciduous and permanent teeth. The cariostatic mechanism of SDF treatment is associated with the
formation of fluoride and silver compounds, antibacterial properties, and anticollagen degradation efficacy.
References
Braga, M.M., Mendes, F.M., De benedetto, M.S., Imparato, J.C., 2009. Effect of silver diammine fluoride on incipient caries lesions in erupting permanent first molars: a pilot
study. J. Dent. Child. (Chic.) 76, 2833.
Burgess, J.O., Vaghela, P.M., 2018. Silver diamine fluoride: a successful anticarious solution
with limits. Adv. Dent. Res. 29, 131134.
Castillo, J.L., Rivera, S., Aparicio, T., Lazo, R., Aw, T.C., Mancl, L.L., et al., 2011. The
short-term effects of diammine silver fluoride on tooth sensitivity: a randomized controlled trial. J. Dent. Res. 90, 203208.
Chen, K.J., Gao, S.S., Duangthip, D., Lo, E.C.M., Chu, C.H., 2018. Managing early childhood caries for young children in china. Healthcare (Basel) 6 (1), 11.
Cheng, L.L., 2017. Limited evidence suggesting silver diamine fluoride may arrest dental
caries in children. J. Am. Dent. Assoc. 148, 120122.
Chibinski, A.C., Wambier, L.M., Feltrin, J., Loguercio, A.D., Wambier, D.S., Reis, A., 2017.
Silver diamine fluoride has efficacy in controlling caries progression in primary teeth: a
systematic review and meta-analysis. Caries Res. 51, 527541.
Chu, C.H., Lo, E.C., 2008a. Microhardness of dentine in primary teeth after topical fluoride
applications. J. Dent. 36, 387391.
Chu, C.H., Lo, E.C., 2008b. Promoting caries arrest in children with silver diamine fluoride:
a review. Oral Health Prev. Dent. 6, 315321.
Chu, C.H., Lo, E.C., Lin, H.C., 2002. Effectiveness of silver diamine fluoride and sodium
fluoride varnish in arresting dentin caries in Chinese pre-school children. J. Dent. Res.
81, 767770.
Chu, C.H., Mei, L., Seneviratne, C.J., Lo, E.C., 2012. Effects of silver diamine fluoride on
dentine carious lesions induced by Streptococcus mutans and Actinomyces naeslundii
biofilms. Int. J. Paediatr. Dent. 22, 210.
Applications of silver diamine fluoride in management of dental caries
695
Chu, C.H., Lee, A.H., Zheng, L., Mei, M.L., Chan, G.C., 2014. Arresting rampant dental caries
with silver diamine fluoride in a young teenager suffering from chronic oral graft versus
host disease post-bone marrow transplantation: a case report. BMC Res. Notes 7, 3.
Chu, C.H., Lo, E.C., 2008a. Microhardness of dentine in primary teeth after topical fluoride
applications. J Dent 36, 387391.
Contreras, V., Toro, M.J., Elias-Boneta, A.R., Encarnacion-Burgos, A., 2017. Effectiveness
of silver diamine fluoride in caries prevention and arrest: a systematic literature review.
Gen. Dent. 65, 2229.
Craig, G.G., Knight, G.M., Mcintyre, J.M., 2012. Clinical evaluation of diamine silver fluoride/potassium iodide as a dentine desensitizing agent. A pilot study. Aust. Dent. J. 57,
308311.
Crystal, Y.O., Niederman, R., 2016. Silver diamine fluoride treatment considerations in children’s caries management. Pediatr. Dent. 38, 466471.
Crystal, Y.O., Marghalani, A.A., Ureles, S.D., Wright, J.T., Sulyanto, R., Divaris, K., et al.,
2017. Use of silver diamine fluoride for dental caries management in children and adolescents, including those with special health care needs. Pediatr. Dent. 39, 135145.
de Almeida Lde, F., Cavalcanti, Y.W., Valenca, A.M., 2011. In vitro antibacterial activity of
silver diamine fluoride in different concentrations. Acta Odontol. Latinoam. 24,
127131.
Dos Santos JR., V.E., de Vasconcelos, F.M., Ribeiro, A.G., Rosenblatt, A., 2012. Paradigm
shift in the effective treatment of caries in schoolchildren at risk. Int. Dent. J. 62,
4751.
Duangthip, D., Chu, C.H., Lo, E.C., 2016. A randomized clinical trial on arresting dentine
caries in preschool children by topical fluorides—18 month results. J. Dent. 44, 5763.
Duangthip, D., Wong, M.C.M., Chu, C.H., Lo, E.C.M., 2017. Caries arrest by topical fluorides in preschool children: 30-month results. J. Dent. 70, 7479.
Duangthip, D., Fung, M.H.T., Wong, M.C.M., Chu, C.H., Lo, E.C.M., 2018. Adverse effects
of silver diamine fluoride treatment among preschool children. J. Dent. Res. 97,
395401.
Elevate Oral Care, 2016. Safety Data Sheet Advantage Arrest Silver Diamine Fluoride 38%
[Online]. Elevate Oral Care (accessed 06.04.17.).
Fa, B.A., Jew, J.A., Wong, A., Young, D., 2016. Silver modified atraumatic restorative technique (SMART): an alternative caries prevention tool. EDU J. 3, 1824.
Featherstone, J.D., 2008. Dental caries: a dynamic disease process. Aust. Dent. J. 53,
286291.
Frencken, J.E., Peters, M.C., Manton, D.J., Leal, S.C., Gordan, V.V., Eden, E., 2012.
Minimal intervention dentistry for managing dental caries—a review: report of a FDI
task group. Int. Dent. J. 62, 223243.
Fung, M.H., Wong, M.C., Lo, E.C., Chu, C., 2013. Arresting early childhood caries with silver diamine fluoride—a literature review. J. Oral Hyg. Health 1, 117.
Fung, M.H.T., Duangthip, D., Wong, M.C.M., Lo, E.C.M., Chu, C.H., 2016. Arresting dentine caries with different concentration and periodicity of silver diamine fluoride. JDR
Clin. Transl. Res. 1, 143152.
Fung, M.H.T., Duangthip, D., Wong, M.C.M., Lo, E.C.M., Chu, C.H., 2018. Randomized
clinical trial of 12% and 38% silver diamine fluoride treatment. J. Dent. Res. 97,
171178.
Gao, S.S., Zhao, I.S., Hiraishi, N., Duangthip, D., Mei, M.L., Lo, E.C.M., et al., 2016.
Clinical trials of silver diamine fluoride in arresting caries among children: a systematic
review. JDR Clin. Transl. Res. 1, 201210.
696
Advanced Dental Biomaterials
Gluzman, R., Katz, R.V., Frey, B.J., Mcgowan, R., 2013. Prevention of root caries: a literature review of primary and secondary preventive agents. Spec. Care Dentist. 33,
133140.
Gold, J., 2017. Limited evidence links silver diamine fluoride and caries arrest in children. J.
Evid. Based Dent. Pract. 17, 265267.
Gotjamanos, T., 1997. Safety issues related to the use of silver fluoride in paediatric dentistry. Aust. Dent. J. 42, 166168.
Gotjamanos, T., Afonso, F., 1997. Unacceptably high levels of fluoride in commercial preparations of silver fluoride. Aust. Dent. J. 42, 5253.
Gotjamanos, T., Orton, V., 1998. Abnormally high fluoride levels in commercial preparations
of 40 per cent silver fluoride solution: contraindications for use in children. Aust. Dent.
J. 43, 422427.
Hamama, H.H., Yiu, C.K., Burrow, M.F., 2015. Effect of silver diamine fluoride and potassium iodide on residual bacteria in dentinal tubules. Aust. Dent. J. 60, 8087.
Hazelrigg, C.O., Dean, J.A., Fontana, M., 2003. Fluoride varnish concentration gradient and
its effect on enamel demineralization. Pediatr. Dent. 25, 119126.
Hellwig, E., Lennon, A.M., 2004. Systemic versus topical fluoride. Caries Res. 38, 258262.
Horst, J.A., 2018. Silver fluoride as a treatment for dental caries. Adv. Dent. Res. 29,
135140.
Horst, J.A., Ellenikiotis, H., Milgrom, P.L., 2016. UCSF protocol for caries arrest using silver
diamine fluoride: rationale, indications and consent. J. Calif. Dent. Assoc. 44, 1628.
Knight, G.M., Mcintyre, J.M., Craig, G.G., Mulyani, Zilm, P.S., Gully, N.J., 2005. An
in vitro model to measure the effect of a silver fluoride and potassium iodide treatment
on the permeability of demineralized dentine to Streptococcus mutans. Aust. Dent. J. 50,
242245.
Knight, G.M., Mcintyre, J.M., Craig, G.G., Mulyani, Zilm, P.S., Gully, N.J., 2007.
Differences between normal and demineralized dentine pretreated with silver fluoride
and potassium iodide after an in vitro challenge by Streptococcus mutans. Aust. Dent. J.
52, 1621.
Knight, G.M., Mcintyre, J.M., Craig, G.G., Mulyani, Zilm, P.S., Gully, N.J., 2009. Inability
to form a biofilm of Streptococcus mutans on silver fluoride- and potassium iodidetreated demineralized dentin. Quintessence Int. 40, 155161.
Lansdown, A.B., 2006. Silver in health care: antimicrobial effects and safety in use. Curr.
Probl. Dermatol. 33, 1734.
Lewis, E.I., 1920. Inorganic Chemistry. Cambridge University Press.
Li, R., Lo, E.C., Liu, B.Y., Wong, M.C., Chu, C.H., 2016. Randomized clinical trial on
arresting dental root caries through silver diammine fluoride applications in communitydwelling elders. J. Dent. 51, 1520.
Liu, B.Y., Lo, E.C., Chu, C.H., Lin, H.C., 2012a. Randomized trial on fluorides and sealants
for fissure caries prevention. J. Dent. Res. 91, 753758.
Liu, B.Y., Lo, E.C., Li, C.M., 2012b. Effect of silver and fluoride ions on enamel demineralization: a quantitative study using micro-computed tomography. Aust. Dent. J. 57,
6570.
Llodra, J.C., Rodriguez, A., Ferrer, B., Menardia, V., Ramos, T., Morato, M., 2005. Efficacy
of silver diamine fluoride for caries reduction in primary teeth and first permanent
molars of schoolchildren: 36-month clinical trial. J. Dent. Res. 84, 721724.
Lo, E.C., Chu, C.H., Lin, H.C., 2001. A community-based caries control program for preschool children using topical fluorides: 18-month results. J. Dent. Res. 80, 20712074.
Applications of silver diamine fluoride in management of dental caries
697
Lou, Y.L., Botelho, M.G., Darvell, B.W., 2011. Reaction of silver diamine [corrected] fluoride with hydroxyapatite and protein. J. Dent. 39, 612618.
McDonald, S.P., Sheiham, A., 1994. A clinical comparison of non-traumatic methods of
treating dental caries. Int. Dent. J. 44, 465470.
Mei, M.L., Li, Q.L., Chu, C.H., Yiu, C.K., Lo, E.C., 2012. The inhibitory effects of silver
diamine fluoride at different concentrations on matrix metalloproteinases. Dent. Mater.
28, 903908.
Mei, M.L., Chu, C.H., Lo, E.C., Samaranayake, L.P., 2013a. Fluoride and silver concentrations of silver diammine fluoride solutions for dental use. Int. J. Paediatr. Dent. 23,
279285.
Mei, M.L., Chu, C.H., Low, K.H., Che, C.M., Lo, E.C., 2013b. Caries arresting effect of silver diamine fluoride on dentine carious lesion with S. mutans and L. acidophilus dualspecies cariogenic biofilm. Med. Oral Patol. Oral Cir. Bucal. 18, e824e831.
Mei, M.L., Ito, L., Cao, Y., Li, Q.L., Lo, E.C., Chu, C.H., 2013c. Inhibitory effect of silver
diamine fluoride on dentine demineralisation and collagen degradation. J. Dent. 41,
809817.
Mei, M.L., Li, Q.L., Chu, C.H., Lo, E.C., Samaranayake, L.P., 2013d. Antibacterial effects
of silver diamine fluoride on multi-species cariogenic biofilm on caries. Ann. Clin.
Microbiol. Antimicrob. 12, 4.
Mei, M.L., Ito, L., Cao, Y., Li, Q.L., Chu, C.H., Lo, E.C., 2014a. The inhibitory effects of
silver diamine fluorides on cysteine cathepsins. J. Dent. 42, 329335.
Mei, M.L., Ito, L., Cao, Y., Lo, E.C., Li, Q.L., Chu, C.H., 2014b. An ex vivo study of
arrested primary teeth caries with silver diamine fluoride therapy. J. Dent. 42, 395402.
Mei, M.L., Lo, E.C., Chu, C.H., 2016a. Clinical use of silver diamine fluoride in dental treatment. Compend. Contin. Educ. Dent. 37, 9398. quiz100.
Mei, M.L., Zhao, I.S., Ito, L., Lo, E.C., Chu, C.H., 2016b. Prevention of secondary caries by
silver diamine fluoride. Int. Dent. J. 66, 7177.
Mei, M.L., Nudelman, F., Marzec, B., Walker, J.M., Lo, E.C.M., Walls, A.W., et al., 2017.
Formation of fluorohydroxyapatite with silver diamine fluoride. J. Dent. Res. 96,
11221128.
Mei, M.L., Lo, E.C.M., Chu, C.H., 2018. Arresting dentine caries with silver diamine fluoride: what’s behind it? J. Dent. Res. 97, 751758.
Milgrom, P., Horst, J.A., Ludwig, S., Rothen, M., Chaffee, B.W., Lyalina, S., et al., 2018.
Topical silver diamine fluoride for dental caries arrest in preschool children: a randomized controlled trial and microbiological analysis of caries associated microbes and
resistance gene expression. J. Dent. 68, 7278.
Mohammed, N.R., Lynch, R.J., Anderson, P., 2014. Effects of fluoride concentration on
enamel demineralization kinetics in vitro. J. Dent. 42, 613618.
Monse, B., Heinrich-Weltzien, R., Mulder, J., Holmgren, C., van Palenstein Helderman, W.
H., 2012. Caries preventive efficacy of silver diammine fluoride (SDF) and ART sealants in a school-based daily fluoride toothbrushing program in the Philippines. BMC
Oral Health. 12, 52. Available from: https://doi.org/10.1186/1472-6831-12-52.
Murdoch-Kinch, C.A., McLean, M.E., 2003. Minimally invasive dentistry. J. Am. Dent.
Assoc. 134, 8795.
Ngo, H., Knight, M., George, G., Sekiguchi, T., 2002. United States Patent. US 6,461,161
B1.
Peng, J.J., Botelho, M.G., Matinlinna, J.P., 2012. Silver compounds used in dentistry for caries management: a review. J. Dent. 40, 531541.
698
Advanced Dental Biomaterials
Punyanirun, K., Yospiboonwong, T., Kunapinun, T., Thanyasrisung, P., Trairatvorakul, C.,
2018. Silver diamine fluoride remineralized artificial incipient caries in permanent teeth
after bacterial pH-cycling in-vitro. J. Dent. 69, 5559.
Rosenblatt, A., Stamford, T.C., Niederman, R., 2009. Silver diamine fluoride: a caries “silver-fluoride bullet”. J. Dent. Res. 88, 116125.
Savas, S., Kucukyilmaz, E., Celik, E.U., Ates, M., 2015. Effects of different antibacterial
agents on enamel in a biofilm caries model. J. Oral Sci. 57, 367372.
Schwendicke, F., Gostemeyer, G., 2017. Cost-effectiveness of root caries preventive treatments. J. Dent. 56, 5864.
SDI, 2016. Riva Star SDS. Version No: 4.1.1.1 ed. SDI Limited.
Shah, S., Bhaskar, V., Venkataraghavan, K., Choudhary, P., Ganesh, M., Trivedi, K., 2013.
Efficacy of silver diamine fluoride as an antibacterial as well as antiplaque agent compared to fluoride varnish and acidulated phosphate fluoride gel: an in vivo study. Indian
J. Dent. Res. 24, 575581.
Shah, S., Bhaskar, V., Venkatraghavan, K., Choudhary, P., Ganesh, M., Trivedi, K., 2014.
Silver diamine fluoride: a review and current applications. J. Adv. Oral Res. 5, 2535.
Suzuki, T., Nishida, M., Sobue, S., Moriwaki, Y., 1974. Effects of diammine silver fluoride
on tooth enamel. J. Osaka. Univ. Dent. Sch. 14, 6172.
Tan, H.P., Lo, E.C., Dyson, J.E., Luo, Y., Corbet, E.F., 2010. A randomized trial on root caries prevention in elders. J. Dent. Res. 89, 10861090.
Targino, A.G., Flores, M.A., dos Santos Junior, V.E., de Godoy Bene Bezerra, F., de Luna
freire, H., Galembeck, A., et al., 2014. An innovative approach to treating dental decay
in children. A new anti-caries agent. J. Mater. Sci. Mater. Med. 25, 20412047.
ten Cate, J.M., 2013. Contemporary perspective on the use of fluoride products in caries prevention. Br. Dent. J. 214, 161167.
Tenuta, L.M., Cury, J.A., 2010. Fluoride: its role in dentistry. Braz. Oral Res. 24 (Suppl 1),
917.
Thanatvarakorn, O., Islam, M.S., Nakashima, S., Sadr, A., Nikaido, T., Tagami, J., 2016.
Effects of zinc fluoride on inhibiting dentin demineralization and collagen degradation
in vitro: a comparison of various topical fluoride agents. Dent. Mater. J. 35, 769775.
Thibodeau, E.A., Handelman, S.L., Marquis, R.E., 1978. Inhibition and killing of oral bacteria by silver ions generated with low intensity direct current. J. Dent. Res. 57, 922926.
Vasquez, E., Zegarra, G., Chirinos, E., Castillo, J.L., Taves, D.R., Watson, G.E., et al., 2012.
Short term serum pharmacokinetics of diammine silver fluoride after oral application.
BMC Oral Health 12, 60.
Vogel, G.L., 2011. Oral fluoride reservoirs and the prevention of dental caries. Monogr. Oral
Sci. 22, 146157.
Wakshlak, R.B., Pedahzur, R., Avnir, D., 2015. Antibacterial activity of silver-killed bacteria:
the “zombies” effect. Sci. Rep. 5, 9555.
Wilson, N.H.F., 2007. Minimally Invasive Dentistry: The Management of Caries.
Quintessence Pub., Chicago, IL; London.
Wright, J.T., White, A., 2017. Silver diamine fluoride: changing the caries management paradigm and potential societal impact. N. C. Med. J. 78, 394397.
Yamaga, R., Nishino, M., Yoshida, S., Yokomizo, I., 1972. Diammine silver fluoride and its
clinical application. J. Osaka. Univ. Dent. Sch. 12, 120.
Yee, R., Holmgren, C., Mulder, J., Lama, D., Walker, D., van Palenstein Helderman, W.,
2009. Efficacy of silver diamine fluoride for arresting caries treatment. J. Dent. Res. 88,
644647.
Applications of silver diamine fluoride in management of dental caries
699
Zhang, W., Mcgrath, C., Lo, E.C., Li, J.Y., 2013. Silver diamine fluoride and education to
prevent and arrest root caries among community-dwelling elders. Caries Res. 47,
284290.
Zhao, I.S., Gao, S.S., Hiraishi, N., Burrow, M.F., Duangthip, D., Mei, M.L., et al., 2017a.
Mechanisms of silver diamine fluoride on arresting caries: a literature review. Int. Dent.
J. 68, 6776.
Zhao, I.S., Mei, M.L., Burrow, M.F., Lo, E.C., Chu, C.H., 2017b. Effect of silver diamine
fluoride and potassium iodide treatment on secondary caries prevention and tooth discolouration in cervical glass ionomer cement restoration. Int. J. Mol. Sci. 18 (2), 340.
Zhao, I.S., Mei, M.L., Li, Q.L., Lo, E.C.M., Chu, C.H., 2017c. Arresting simulated dentine
caries with adjunctive application of silver nitrate solution and sodium fluoride varnish:
an in vitro study. Int. Dent. J. 67, 206214.
Zhi, Q.H., Lo, E.C., Lin, H.C., 2012. Randomized clinical trial on effectiveness of silver
diamine fluoride and glass ionomer in arresting dentine caries in preschool children. J.
Dent. 40, 962967.
Index
Note: Page numbers followed by “f,” “t,” and “b” refer to figures, tables, and boxes,
respectively.
A
Ablation, 532
Abrasion resistance, 50 51
Abrasives, 589
Academy of Dental Materials, 166
Accelerator, 45 46
Acetone, 330
Acetoxy silastic adhesives, 636 638, 638f
Acetoxy silicone adhesives, 632, 638t
Achromatic color, 8 9
Acid Blue 9. See Erioglaucine disodium
Acid decomposable glasses, 178
Acid etching
of dentin, 238
technique, 232 235
citric acid, 233 234
EDTA, 235
ferric chloride solution, 234
NaOCl, 235
phosphoric acid, 233
of titanium surfaces, 590
Acid orthophosphate, 378
Acid-functionalized monomers, 130
Acid-resistant ceramic, 67
Acidic functional monomers, 156 157
Acidulated phosphate fluoride (APF),
690 691
ACPS. See 3Acryloxypropyltrimethoxysilane
(ACPS)
ACPs. See Amorphous calcium phosphates
(ACPs)
Acrylic artificial teeth, 99 100
Acrylic denture base materials, 80 86
acrylic artificial teeth, 99 100
chemical structure and mechanism of
polymerization, 82 85
commercial forms and composition
gel form, 86
powder liquid form, 85 86
denture base material, 80
development, 80 86
and manufacturing technologies, 86 94
requirements, 81t
denture lining materials, 94 99
Acrylic polymers, 79 80
Acrylic resins, 2, 82, 128, 617 618
3-Acryloxypropyltrimethoxysilane (ACPS),
76
Actinomyces naeslundii, 690 691
Activ GP, 219
Active surface, 569 570
ADA. See American Dental Association
(ADA)
Addition reaction, cross-linking by, 625
Additive manufacturing (AM), 519 520
Adhesion, 230
of fibers to polymer matrix, 310
tozirconia, 329 333
Adhesives
adhesively bonded amalgam restoration,
114
advancement
antibacterial properties, 242 245
bioactive properties, 245 247
classifications, 237 241
based on clinical steps, 240 241
based on interaction with smear layer,
241
first-generation adhesives, 237
composition, 231 232
bonding, 231 232
etchant, 231
primer, 231
702
Adhesives (Continued)
dentin bonding, 241 242
dentistry, 319 320
development, 229
eighth-generation, 240
fifth-generation, 239
fourth-generation, 238 239
indications, 230 231
in restorations, 230
second-generation, 237 238
seventh-generation, 240
sixth-generation, 239 240
third-generation, 238
Admixed composition alloy, 112 113
Ag3PO4, 689
Agar, 202
Agarose, 653
AH-26 resin sealers, 280
Air abrasion, 330
AISI 316L steel, 545
Al2O3/SiO2 ratio, 179 180
Alcohol, 330
Alginate, 201 202, 649 650
Alkali glass. See Glass A
Alkaline earth ions. See Alkaline ions
Alkaline glass fillers, 130 131
Alkaline ions, 178 179
Alkyl silicate, 203
“All-in-one” adhesive system. See Seventhgeneration adhesives
Allergic reaction, 25 26
Allografts, 353 354, 353t
DFDBA, 354
fresh or frozen, 353
mineralized freeze-dried bone, 354
Alloplasts, 355 362
bioactive glasses, 360 361
calcium phosphates, 357 360, 358t
calcium polyphosphate, 361
calcium sulfate, 362
glass ionomers, 361 362
magnesium-based biodegradable
materials, 362
polymers, 357
Alloyed gold, 107
Alloys, 217 218
silver, 217 218
α β titanium (α β Ti), 549
α form, 39
Index
α-hemihydrate, 39
α-titanium (αTi), 549
α-tricalcium phosphate (α-TCP), 358t, 359,
398 399
Alternative restorative treatment (ART),
189, 219
Alumina (Al2O3), 89 90, 117 118, 320,
322, 527 528, 589
airborne-particle abrasion, 330
ceramic brackets, 552 553
ceramics, 55 56
materials, 485
Alumina-based ceramics, 323
Alumina-toughened zirconia (ATZ), 320
Aluminosilicate polyacrylate (ASPA).
See Glass ionomers
Aluminum, 218 219
Aluminum oxide. See Alumina (Al2O3)
Alveolar bone properties, 587
AM. See Additive manufacturing (AM)
Amalgam. See Dental amalgam
Amalgamation process, 109
Amalgambond, 234
Amalgomer, 186
American Dental Association (ADA), 238
Ammonium hexafluorosilicate, 690 691
Ammonium persulfate, 180
Amorphous, 55
Amorphous calcium phosphates (ACPs),
358t, 387, 388t, 396 398, 483
Anatomical dental duplicate capture, 518
Animal-derived biomaterials, 647
Anterior composite restoration, 148
Antheraea pernyi SF (APSF), 650
Antibacterial
activity, 465
composites, 152 153, 152t
nanoparticle modified endodontic sealer,
489
properties of adhesives, 242 245
Antimicrobial peptides, 3
APAFILL-G, 412
Apatites, 399 403
apatite-containing formulations, 401 402
formation, 456
APSF. See Antheraea pernyi SF (APSF)
Arabic Gum, 39 40
Aramid fibers, 88, 133
Arestin, 483
Index
Arginine, 245
Aromatic hydrocarbons, 82
Aromatic polyamide fibers, 88
ART. See Alternative restorative treatment
(ART)
Atlantis abutment, 529
Atraumatic restorative treatment.
See Alternative restorative treatment
(ART)
Atraumatic restorative technique (ART), 677
Attachments in clear aligners, 569 571,
570f, 570t
ATZ. See Alumina-toughened zirconia
(ATZ)
Austenitic NiTi wires (A-NiTi wires).
See Superelastic NiTi
Austenitic SS, 545 547
Australian stainless steel wires, 557
Autoclave, 77
Autografts, 352 353, 352t
Autopolymerizing resin, 86
B
BAG. See Bioactive glass (BG)
Bakelite, 79 81
Barium, 144
Barium oxide (BaO), 130 131
Barium titanate (BaTiO3), 90
bcc lattice. See Body-centered cubic lattice
(bcc lattice)
BCP. See Biphasic calcium phosphate (BCP)
BD. See Biodentine (BD)
Beautifil from Shofu, 152
Begg light archwire technique, 557
Benzalconium chloride, 153, 242 243
Benzoylperoxide (BPO), 135
β-hemihydrate, 39
β-titanium (β-Ti), 549
alloys, 561
β-tricalcium phosphate (β-TCP), 358t, 359,
360f, 398 399, 415, 657
BFS. See Biaxial FS (BFS)
BG. See Bioactive glass (BG)
BHT. See Butylated hydroxytoluene (BHT)
Biaxial FS (BFS), 187 188
BIC. See Bone implant contact (BIC)
Bidirectional fibers, 308 309
Bio-glass. See Bioactive glass (BG)
Bio-inks, 663 664
703
Bio-Oss, 354 355
Bioactive cement, 600
Bioactive glass (BG), 131, 246 247, 274,
360 361, 454, 657 658
clinical applications, 460 469
antibacterial activity, 465
bioactive glass scaffolds, 465 468
bone graft substitute, 461
bone regeneration, 461 462
coating of implants, 463
drug delivery system, 462
particle size of bioactive glasses,
468 469
role in minimal invasive dentistry, 465
use in toothpastes, 463 464
composition, 456 460
factors affecting apatite formation, 456
fibers, 29
future, 469
methods of synthesis, 460
scaffolds, 465 468
Bioactive/bioactivity, 28 29
of glasses, 454 456
mechanism of action, 455
solubility, 455 456
molecules, 654
nanoscale glass for root canal disinfection,
490
properties of adhesives, 245 247
remineralizing composites, 150 151
restorative materials, 661 662
BD, 662
MTA, 661 662
Bioaggregate, 262
Bioceramic(s), 380 381, 603, 655 658
BCP, 657
bioactive glasses, 657 658
bioceramic-based sealers, 284, 284t
HA, 656 657
materials, 256, 262 263
onlays or crowns, 380 381
restorations, 380 381
tricalcium phosphate, 655 656
Biochemical binding to bone, 660
Biocompatibility, 2, 22 23, 23t, 25f,
118 119
of resin composites, 145 147
toxicology of mercury, 118 119
Biodegradability, 2
704
Biodegradable/biodegradation, 28
of implanted graft materials and bone
formation, 363 365
macrophages respond to small fragments
and particles, 365f
materials, 644
metal scaffolds, 658 659
polymers, 469
Biodentine (BD), 262, 600, 662
Biofilm, 74
BioForce wires, 560
Bioglasses, 657 658, 661
Biological apatite, 378
Biological nanoceramics, 488 489
Biomaterials, 1, 106, 217 218, 644.
See also Nanomaterials
classification, 646 647
properties and implant surface
characteristics of dental implants,
584
in tissue engineering and regeneration, 647
used in dentistry, 305 306
ceramics, 306
composites, 306
metals, 305
Biomedical engineering, 2
Biomedical science, 2
BiominF. See Fluoride-containing BG
(BiominF)
BioRoot RCS, 600
Biphasic calcium phosphate (BCP), 406, 657
Biphasic CaPO4 formulations, 404
Bis-GMA. See Bisphenol-A
glycidyldimethacrylate (Bis-GMA)
Bis-GMA/TEGDMA resin matrix, 130 131
Bis(acryloyloxymethyl)tricyclo[5. 2. 1. 02,
6]decane. See TCD-DI-HEA
Bismethacryloyloxy ethyl phosphate
(BMEP), 156 157
Bismuth oxide, 257 261
Bisphenol-A glycidyldimethacrylate (BisGMA), 128 130, 147, 277
Bitewing imaging technique, 510t
Black staining of SDF-treated teeth, 677f
Blackboard, 533 534
Blended learning, 533 534
Blue Elgiloy, 557
BMEP. See Bismethacryloyloxy ethyl
phosphate (BMEP)
Index
BMPs. See Bone morphogenetic proteins
(BMPs)
BMSF. See Bombyx mori SF (BMSF)
Body-centered cubic lattice (bcc lattice),
543 544
Bombyx mori SF (BMSF), 650
Bond strength evaluation, 71 73
Bonded amalgam restorations, 114
Bonding, 231 232
Bone
augmentation procedures, 353
formation, 347 348
regeneration, 405, 461 462
replacement, 347 348
biodegradation of implanted graft
materials and bone formation,
363 365
future of bone tissue graft materials,
365 366
graft materials biocompatibility and
degradation products, 363
natural tissues and synthetic
biomaterials, 350 362
rationale behind use of bone
replacement graft materials,
348 349, 351t
scaffolds, 458
supported guides, 526
Bone grafts, 347 348, 645
natural tissues and synthetic biomaterials,
350 362
allografts, 353 354, 353t
alloplasts, 355 362
autografts, 352 353, 352t, 353t
xenografts, 354 355
substitute, 461
Bone implant contact (BIC), 659
Bone morphogenetic proteins (BMPs), 349
BMP-2, 649 651
Bone tissue engineering, scaffolds for,
645 646
Bone tissue graft materials, future of,
365 366
Borate glass, 454
Borate-based BGs, 462
Borate-based bioactive glasses, 458 460
Borate-based bioglasses, 657 658
Borax, 205 206
Boron, 144
Index
BOs. See Bridging oxygens (BOs)
“Bottom-up” nanomanufacturing, 219 220
BPO. See Benzoylperoxide (BPO)
Braided NiTi wires, 560
Braided wires, 557
Branched polymers, 620
Bridging oxygens (BOs), 178 180
Brilliant Blue FCF. See Erioglaucine
disodium
Brittleness, 19
Brushite. See Dicalcium phosphate dihydrate
(DCPD)
Bulk-fill composites, 157 165, 160t
Bulk-fill RBCs, 138
Butylated hydroxytoluene (BHT), 290 292
C
C-factor. See Cavity configuration factor (Cfactor)
CAD CAM system. See Computer-aided
design computer-aided
manufacturing system (CAD CAM
system)
Calcination method, 39, 39t
Calcium, 378, 390 391
Calcium fluoride (CaF2), 222 223
Calcium fluoroaluminosilicate glass powder,
190
Calcium hydroxide (Ca(OH)2), 271 272,
275f
sealers, 278 279, 280t, 286t
Calcium hydroxyapatite (CHAp), 590
Calcium orthophosphate (CaPO4), 378 379,
381, 382t, 383 385
CaPO4-containing endodontic and/or root
canal sealers, 406, 406t
ceramic brackets, 408f
chewing gums, 386 389
classification according to dental
specialties
endodontics, 404 406
oral and maxillofacial surgery, 407
oral applications, 413
orthodontics, 407 409
periodontics, 411 413, 411f
prosthodontics, 409 411
tissue integration of dental implant,
410f
classification according to existing CaPO4
705
ACPs, 396 398
α-TCP and β-TCP, 398 399
apatites, 399 403
biphasic and multiphasic CaPO4
formulations, 404
DCPD and DCPA, 395 396
MCPM and MCPA, 395
OCP, 396
TTCP, 403 404
clinical applications in dentistry,
394 413, 394t
for dental caries prevention and in
dentifrices, 385 394
dentin hypersensitivity treatments,
392 394
information on current biomedical
applications, 385
teeth remineralization, 390 392
tissue engineering approaches, 414 415
toothpastes, 386 389, 388t
Calcium oxide (CaO), 63, 657 658
Calcium phosphate (CaP), 150, 357 360
CaP based bioceramics, 363
CaP coated titanium surfaces, 590
dicalcium phosphates, 359 360
hydroxyapatite, 357 359, 358t
TCP, 359
Calcium phosphorous nanoparticles (Ca P
nanoparticles), 485
Calcium polyphosphate (CPP), 361,
396 397, 650
Calcium silicate, 262 263
Calcium sulfate, 362
Calcium sulfate dehydrate, 44
Calcium sulfate hemihydrate, 38 40, 44, 44f
Calcium-deficient hydroxyapatite (CDHA),
358t, 393 394, 399 403
Calcium-enriched mixture cement, 600
Calset, 155, 156f
Calthane, 619
Camphorquinone (CQ), 136
free radical formation by light activation,
135f
Candida albicans, 27
CaP. See Calcium phosphate (CaP)
Ca P nanoparticles. See Calcium
phosphorous nanoparticles (Ca P
nanoparticles)
Caphosol, 413
706
Capseal, 284t, 406, 406t
Carbides, 133 134
Carbon, 543 544, 544t
Carbon dioxide (CO2), 331
laser, 531
Carbon fiber, 307 308
carbon fiber reinforced carbon, 586 587
Carbon nanotubes (CNTs), 133 134, 602
Carbon-carbon double bonds (C 5 C), 139
Carbon-carbon single bonds (C C), 139
Carbonate hydroxyl apatite nanoparticles,
483
Carbonization, 532
Carbothermic smelting, 621
Carcinogenicity, 27 28
CARES. See Computer-Aided Restoration
Service (CARES)
Caries management, clinical effects of silver
diamine fluoride applications on
in adults, 683 684
in children, 677 683
in the elderly, 684
Cariogenic bacteria
cariostatic effects of silver diamine
fluoride on, 690 692
Carnauba, 9 11
Casearia sylvestris, 601 602
Casein phosphopeptide (CPP), 483
Casein phosphopeptide ACP (CPP ACP),
390
CAT. See Clear aligner therapy (CAT)
Cavalite, 402 403
Cavity. See Dental caries
Cavity configuration factor (C-factor), 142,
154
CBCT. See Cone beam computed
tomography (CBCT)
CCD. See Charged-coupled device (CCD)
CCTP. See Collagen/CS/β-TCP (CCTP)
CDHA. See Calcium-deficient
hydroxyapatite (CDHA)
Celluloid, 80
Cellulose nitrates, 79 80
Cellulose phthalate, 483
Cementitious materials, graphene to
improve, 600 609
Cements, 2
Cementum, 304
Cephalometric projections, 511t
Index
Ceramic bonding, 65 74
bond strength evaluation, 71 73
fatigue, 73 74
mechanism, 65 71
chemical surface conditioning, 65 70
mechanical surface conditioning,
70 71
Ceramic brackets, 551 553, 551b. See also
Metal brackets
alumina, 552 553
polycrystalline zirconia, 552
Ceramic(s), 133 134, 306, 318, 586 587,
646
biological interaction, 74 77
physical parameters, 76 77
sterilization methods, 77
surface chemistry, 74 76
ceramic-based biomaterials, 647
ceramic resin ceramic system, 71 73
materials in dentistry
glass ceramics, 56 61
oxide ceramics, 61 64
polymer-infiltrated ceramics, 64 65
scaffolds, 646
CEREC 3D, 529
Cerec system, 518 519
Cerium trioxide (Ce2O3), 63
Cetylpyridinium chloride, 153
CGIS. See Computer-guided implant surgery
(CGIS)
Chairside milling, 518
CHAp. See Calcium hydroxyapatite (CHAp)
Charged-coupled device (CCD), 514 515
Chemical adhesion with tooth, 188 189
Chemical composition, 55 56
Chemical degradation reaction process, 458
Chemical structure and mechanism of
polymerization, 82 85
Chemical surface conditioning
hydrofluoric acid etching, 65 67
primer, 67 70
Chemical vapor deposition (CVD), 599 600
CVD-grown graphene, 607f
Chemical-resistant glass. See Glass C
Chemically activated resins, 97 98
Chewing gums, 386 389
Chitosan (CS), 278, 483 484, 647,
651 653
CS alginate hybrid scaffolds, 649
Index
Chlor-XTRA, 270t
Chlorhexidine (CHX), 153, 201 202,
242 243, 266 267, 272 273, 684,
690 691
Chlorinated polyethylene, 619
Chloropercha, 286t
Chroma. See Saturation of color
Chromium, 543 544, 544t
CHX. See Chlorhexidine (CHX)
CHX-Plus, 270t
Citric acid, 233 234
CLD. See Cross-link density (CLD)
Cleaning agents, 330
Clear aligner therapy (CAT), 562
Clear aligners, 562 572
attachments, 569 571, 570f, 570t
cytotoxicity, 571 572
forces of thermoplastic aligners, 565 567
material composition, 562 565
mechanical properties, 567 569
thermoforming process, 565
Clearfil Bond System F, 237 238
Clearfil Protect Bond, 244
Clinical durability of resin composites, 147 148
Clinpro white varnish, 399
Closed systems, 518 519
CMO SAPS. See Complementary metal
oxide semiconductor active pixel
sensor (CMO SAPS)
CNIS. See Computer-navigated implant
surgery (CNIS)
CNTs. See Carbon nanotubes (CNTs)
Coating of implants, 463
Cobalt-based wear-resistant alloy, 548, 548t
Cobalt chromium brackets (CoCr brackets),
548
Cobalt chromium-based archwires,
557 558, 558t
coDiagnostiX software, 523
Coe-Comfort materials, 633 635, 634f
Coe-Soft materials, 633 635, 634f
Coefficients of thermal expansion (CTE),
14, 57
Cold-cured resins, 85 86, 95, 96t
acrylic resins, 84
Collagen, 490, 606, 647 648
collagen-bioactive ceramic composites,
648
sponge-form scaffolds, 606 607
707
Collagen/CS/β-TCP (CCTP), 648
Colloidal dispersion of rGO-coated
hydroxyapatite, 607 608
Color, 8 9
Coloring agents, 635 638
acetoxy silastic adhesives, 636 638
colored flocking, 635 636
extrinsic colors, 636
intrinsic stains, 636
Commercially pure titanium (cpTi), 585, 659
grade 2 CP-Ti, 549
grade 4 CP-Ti, 549, 585 587
Complementary metal oxide semiconductor
active pixel sensor (CMO SAPS),
514
Compomers, 130, 153 154
Composite resin (CR), 683
Composites, 306
CS scaffolds, 653
material, 55, 137 138, 220
preheating, 155
resins, 290 292, 306
Compressive load, 19
Compressive strength (CS), 16, 49,
114 115, 180 181, 185 186
Computed tomography (CT), 510, 511t, 515,
520, 663 664
Computer-aided design computer-aided
manufacturing system (CAD CAM
system), 93 94, 517 521
abutments in implant dentistry, 528
block, 64 65
CAD/CAM blocks, 319
Chairside milling, 518
composites, 159, 165
custom implant abutments, 529 530
in implant restorative dentistry, 527 528
laboratory and industrial milling,
518 519
machining of restorations, 519
three-dimensional printing, 519 521
versions, 58 60, 60f
Computer-Aided Restoration Service
(CARES), 529
Computer-assisted technologies, 51
Computer-guided implant surgery (CGIS),
522, 524
Computer-navigated implant surgery
(CNIS), 522, 524 527
708
Computer-supported implant dentistry,
521 530
CAD CAM
abutments in implant dentistry, 528
custom implant abutments, 529 530
system in implant restorative dentistry,
527 528
CGIS, 524
CNIS, 524 527
materials, 529
prosthetic abutments, 528
recent advances in implant technologies,
522 523
three-dimensional printing in implant
dentistry, 521 522
Condensation
polymerization, 201
reaction, cross-linking by, 624 625
silicone, 203
Cone beam computed tomography (CBCT),
509 510, 511t, 512, 515, 520
Conventional cements, 329
Conventional endodontic treatment, 490
Conventional glass ionomers, 218 219
Conventional plaster casting materials,
205 206
Conventional silicate-based glasses,
460 461
Conventional waxes, 204 205
Cooling process, 57
Copper, 543 544, 544t
NiTi, 560
Core obturation materials
Gutta-percha, 275 277
resilon, 277
root canal sealers, 277 289
silver points, 274 275, 275t
Coronal caries management
in adults, 683 684
in children, 677 683
Corrosion, 116 117
marginal sealing, 116 117
resistance, 545
Coupling agents, 332 333
CPP. See Calcium polyphosphate (CPP);
Casein phosphopeptide (CPP)
CPP ACP. See Casein
phosphopeptide ACP (CPP ACP)
cpTi. See Commercially pure titanium (cpTi)
Index
CQ. See Camphorquinone (CQ)
CQ/TA, 136
Creep, 115 116, 568
diffusion, 61 62
resistance, 568
Cross-link density (CLD), 201 202
Cross-linking
by addition reaction, 625
collagen scaffolds, 647 648
by condensation reaction, 624 625
materials, 86
polymers, 620
of polymers, 624
Crystalline
HA, 488
phase, 57
structure, 63
theory, 44
CS. See Chitosan (CS); Compressive
strength (CS)
CT. See Computed tomography (CT)
CTE. See Coefficients of thermal expansion
(CTE)
Cumulative fluoride [F]c release, 184
Curing, 175 176
mechanisms of acrylic denture base
materials
cold-cured acrylic resins, 84
heat-cured acrylic resins, 83
microwave-cured acrylic resins, 84 85
pour-type denture resins, 85
visible light cured resins, 84
resin composites classification according
to, 138
Cushioning effect, 94, 96
Custom-made trays, 198 199
CVD. See Chemical vapor deposition (CVD)
Cysteine cathepins, 692
Cytotoxicity, 24 25
tests, 26
D
Daro water-based skin adhesive, 638, 639f
DC. See Degree of conversion (DC)
DCPA. See Dicalcium phosphate anhydrous
(DCPA)
DCPD. See Dicalcium phosphate dehydrate
(DCPD); Dicyclopentadiene (DCPD)
Deformation resistance, 167t
Index
Degree of conversion (DC), 136, 139 140
cavity location effect, 140
light-curing
duration effect, 140
system effect, 139 140
tip distance effect from RBC surface,
140
resin increment thickness effect, 139
resin shade effect, 139
Demineralization process, 378, 378f
Demineralized freeze-dried bone allograft
(DFDBA), 354
Denatured collagen, 647
Densely sintered aluminum-oxide ceramic,
61 62
Dental
applications of nanobiomaterials,
481 492
attrition process, 380
CaPO4 classification according to dental
specialties, 404 413
cements, 176
zinc oxide eugenol, 15
ceramics, 321 322
composites, 108 109
enamel, 378
erosion, 379 380
filling biomaterials
amalgam, 109 111
gold fillings, 107 108
fluorosis, 27
FRCs, 311
gypsum and investments
dies and models produced from digital
data, 51 52
production of calcium sulfate
hemihydrate, 38 40
properties of gypsum products, 38
setting and manipulation characteristics
of gypsum products, 42 47
setting expansion hygroscopic setting
expansion, 47 51
types of gypsum products, 40 41
implantology, 410 411
impression materials, 3
IMs for dental prosthesis
characteristics, 207 211
elastic, 200 204
inelastic, 204 206
709
materials, 12, 217 218
prosthetics. See Prosthodontics
public health, 383 385
pulp, 304
resin composite. See Resin composites
restorations, 8
silane products, 134
stone. See α form
stone Type V, 41, 42f
Dental abrasion process, 380
Dental adhesives, 27 28, 237, 240
Dental amalgam, 2, 106, 109 111,
217 218, 290, 305, 492 493
amalgam bonding, 113 114
biocompatibility, 118 119
bonding
bonded amalgam restorations, 114
nonbonded amalgam restorations,
113 114
nonbonded vs. adhesively bonded
amalgam restorations, 114
composition, 112 113
high-copper dental amalgam, 112 113
low-copper dental amalgam, 112
dental filling biomaterials, 107 111
dimensional change, 117
failure mode, 118
hardness, 117 118
history, 111 112
material properties
compressive and tensile strength, 114 115
creep, 115 116
tarnish and corrosion, 116 117
Young’s modulus, 118
Dental biomaterials, 1, 8
bioactivity, 28 29
biodegradation, 28
biological properties
biocompatibility, 22 23
usage tests, 24
in vitro testing, 23
in vivo testing, 24
carcinogenicity, 27 28
cytotoxicity tests, 26
electrical conductivity and resistivity, 15
fluoride and caries, 26 27
foreign body reaction, 29 30
limitation of mechanical testing methods,
22
710
Dental biomaterials (Continued)
mechanical properties and characterization
methods, 16 22, 17f
optical properties, 8 9
osseointegration, 29
osteoinduction, 29
thermal properties, 9 14
coefficient of thermal expansion, 14
heat of fusion, 11
specific heat, 13
temperature, 9
thermal conductivity, 12
thermal diffusivity, 13 14
transition temperatures, 9 11
toxicity and cytotoxicity, 24 25
viscosity, 14
Dental caries, 26 27, 107, 377 378, 379f,
400 401
CaPO4 in, 385 394
detection, 516
location effect, 140
preparation, 229
Dental implants, 581 582
biomaterial properties and implant surface
characteristics, 584
biomechanical properties, 584 585
comparison of different hard tissue with,
584t
functionally graded/hierarchical dental
implant surfaces, 590
materials, 586 588
alveolar bone properties, 587
influence of oral health and systemic
disease on implant survival,
587 588
modification, 588 590
of PEEK dental implants, 590 592
of zirconia implants, 592
nanomaterials for, 484 486
osseointegration, 583 584
surface properties, 585 586
titanium screw in dog mandible, 582f
Dental mineral, cariostatic effects of silver
diamine fluoride on, 685 689
DentalSlice software, 523
Dentifrices, CaPO4 in, 385 394
Dentin, 230, 303 304
bonding, 241 242
hypersensitivity treatments, 392 394
Index
Dentine collagen, cariostatic effects of silver
diamine fluoride on, 692
Dentistry, 2, 106, 217 219, 383, 455 456.
See also Computer-supported implant
dentistry; Digital dentistry
biomaterials used in, 305 306
clinical applications of CaPO4 in, 394 413
GICs in, 219
zirconia in, 222, 324 325, 325t
Denture base material, 79 80
development, 80 86
and manufacturing technologies, 86 94
fiber-reinforced resins, 87 89
hybrid reinforcement, 91
hypoallergenic resins, 91
novel technologies in manufacturing
removable denture base, 93 94
particulate-reinforced resins, 89 91
rubber-reinforced resins, 87
thermoplastic resins, 92 93
requirements, 81t
Denture lining materials, 94 99
clinical indication, 94 95
hard relining, 95
soft relining, 96 98
tissue conditioners, 98 99
DFDBA. See Demineralized freeze-dried
bone allograft (DFDBA)
Di-organo-polysiloxane, 625
Diaket, 292
Diametral tensile strength, 20
DiaRoot. See Bioaggregate
Dibutyl phthalate, 86
Dicalcium phosphate anhydrous (DCPA),
358t, 387, 388t, 395 396
Dicalcium phosphate dehydrate (DCPD),
150 151, 358t, 359 360, 360f, 387,
388t, 395 396
Dicalcium phosphates, 359 360
Dicyclopentadiene (DCPD), 154
Die stone. See Modified α-hemihydrate
Dies, 37 38
and models produced from digital data,
51 52
Differential thermal analysis, 9 11
Diffusion creep, 61 62
Digital camera and imaging systems, 517
Digital data, dies and models produced from,
51 52
Index
Digital dentistry, 508. See also Dentistry
CAD CAM system, 517 521
caries detection, 516
computer-supported implant dentistry,
521 530
digital radiography and magnetic
resonance imaging, 508 515
lasers and dental applications, 530 533
photography and shade selection,
516 517
technology and dental education,
533 534
Digital imaging, 511t, 513t
Digital radiography, 508 515
clinical applications, 509 512
intraoral, extraoral, including cone beam
CT, 508 509
limitations, 512 515
Digital simulators, 534
Digital X-ray systems, 514
Dihydrate calcium sulfate, 38 39
Dilatant fluid, 14
Diluents monomers, 141
Dimer acid, 150
dimer acid based dimethacrylate
monomer, 150
Dimethacrylates, 128
Dimethylaminododecyl methacrylate
(DMADDM), 243 244
Dimethyldichlorosiloxane, 622
Diode laser, 532
Dipentaerythritol Penta acrylate phosphate
(PENTA), 130
Diphenyl (2,4,6-trimethylbenzoyl) phosphine
oxide (TPO), 136
Direct composite
resins, 138
restoration, 154
Direct contact tests, 23
Direct dental
materials, 217 218
restorations, 110
Direct metal layer sintering (DMLS),
520 522
Direct restoration, 138, 166 171
Direct restorative dental materials, 3
Dismetral compression test, 20
DMADDM. See Dimethylaminododecyl
methacrylate (DMADDM)
711
DMAE-CB. See Methacryloxylethylcetyldimethyl ammonium chloride
(DMAE-CB)
DMAHDM. See 2-Methacryloyloxyethyl
phosphorylcholine,
dimethylaminohexadecyl
methacrylate (DMAHDM)
DMFT (number of decayed, missing, and
filled teeth due to caries), 387
DMLS. See Direct metal layer sintering
(DMLS)
DMP-1, 606
Dominant wavelengths, 8 9
Double-walled halloysite nanotubes,
133 134
Drug delivery system, 462
Dry skulls, 512
Drynaria fortunei, 355
DSPP, 606
Dual-cured composite, 136
Ductility, 19
Duplex stainless steel, 547
DX-511, 143, 149
E
E-beam deposition. See Electron-beam
deposition (E-beam deposition)
E-glass fibers, 133, 586 587
E-learning tools, 533 534
Early childhood caries (ECC), 677
Easy Guide software, 523
Edge adhesives, 639
EDTA. See Ethylenediamine tetra-acetic
acid (EDTA)
Education materials, 533 534
Eicosapentaenoic acid, 586
Eighth-generation adhesives, 240
Elastic cavity wall concept, 143, 155
Elastic impression materials. See Inelastic
impression materials
agar, 202
alginate, 201 202
polyethers, 200
polysulfide, 201
silicones, 202 204
Elastic limit, 18
Elastic modulus, 18 19, 567
Elastic region, 17 19
Elasticity, 305
712
Elastin, 653
Elastomeric materials, 14, 198
Electric glass. See Glass E
Electrical conductivity and resistivity, 15
Electrical fibers, 133
Electrically assisted enhanced
remineralization, 392
Electroforming, 107
Electron-beam deposition (E-beam
deposition), 590 592
Electrospinning process, 1 2, 491 492
Electrospun nanomaterials, 491 492, 493t
Elemental magnesium, 362
Elgiloy. See Cobalt chromium-based
archwires
Enamel, 230, 303, 393
demineralization, 379
etching technique, 231 236
acid etching, 232 235
laser etching, 235 236
self-etching, 236
Endo-CPM, 600
Sealer, 284t
EndoBinder, 600
Endocem, 600
Endodontic(s), 256, 312, 383 385,
404 406
imaging, 512
materials
intracanal medicaments, 271 274
perforation repair materials, 292 293,
293b
as root canal irrigants, 263 270
root canal obturation materials,
274 289
root-end filling materials, 290 292
in vital pulp therapy, 256 263
nanobiomaterials, 488 490
regeneration, 490
EndoSeal MTA, 600
EndoSequence, 262 263, 600 601
EndoSequence BC Sealer, 395, 488 489
Endosequence root repair material (ERRM),
262
Endosequence root repair putty (ERRP), 262
Energy dispersive spectroscopy, 28 29
Enolase, 691
Epigallocatechin-3-gallate. See Green tea
extract
Index
Epithane-3, 619
Epoxy resin, 50, 128
sealers, 280
Equia system, 487 488
Erbium, chromium:
yttrium scandium gallium garnet
radiation (Er, Cr:YSGG radiation),
235 236
Erbium laser, 531 532
Erosive mechanism, 184
ERRM. See Endosequence root repair
material (ERRM)
ERRP. See Endosequence root repair putty
(ERRP)
Essix C 1 , 569
Esters, 82
Esthet-X (Dentsply Caulk, United States),
130 131
Esthetic(s), 188
orthodontic brackets, 325
restoration, 144
Etch-and-rinse technique, 233
Etchant, 231
Etching, 231 232
Ethyl alcohol, 203
Ethylene glycol dimethacrylate, 83
Ethylenediamine tetra-acetic acid (EDTA),
235, 265 266
Etkon, 529
“Evaporable” water. See “Loosely bound”
water
Everest, 529
Exceed-30 aligner material, 564 565
Exceed-40 aligner material, 564 565
Excitation purity, 8 9
Extraoral
digital imaging, 509 510, 511t
MRI, 509
prostheses, 616
radiography, 508 509
Extrinsic colors, 636
F
F-BAG. See Fluoride-based BAG (F-BAG)
Fabrication of dental implants, 521 522
Face-centered cubic lattice (fcc lattice),
543 544
Failure analysis of zirconia restorations,
333 335
Index
Failure mode, 118
Fatigue, 73 74
fcc lattice. See Face-centered cubic lattice
(fcc lattice)
FDA. See US Food and Drug Administration
(FDA)
FDBA. See Freeze-dried bone allograft
(FDBA)
Fe-phosphorous alloys, 658
Feldspathic ceramic, 318, 322 323
Feldspathic porcelain, 56 58
Ferric chloride solution, 234
Ferrite, 545
steel, 547
FGMs. See Functionally graded materials
(FGMs)
FHA. See Fluorohydroxylapatite (FHA)
Fiber
distribution, 308
length, 309
orientation, 136, 308 309, 309f
position and placement, 89
quantity, 308
types, 306
Fiber-reinforced composites (FRCs), 3,
133 134, 136, 302, 302f, 306 311
carbon, 307 308
clinical applications, 311 312
endodontics, 312
implants, 311
orthodontic, 312
periodontal, 312
prosthodontics, 312
tooth restoration, 311
glass, 307
influencing factors on mechanical
properties
adhesion of fibers to polymer matrix,
310
impregnation of fibers with polymer
matrix, 310
polymerization shrinkage, 311
water sorption, 310
polyethlene, 308
Fiber-reinforced resins, 87 89
position and placement of fibers, 89
Fibrin, 648 649
Fifth-generation adhesives, 239
Fillers, 130 134, 306
713
fiber-reinforced composites, 133 134
nanofilled resin composite, 132 133
prepolymerized filler particles, 132
size and loading, 131 132
Filtek Supreme (3M ESPE), 132
Fineness, 46
Finite element stress analysis, 155
First Class, 533 534
First generation
adhesives, 237
M-NiTi. See Stabilized martensitic NiTi
of Y-TZP, 63 64
Fixed dental prosthesis (FPD), 318
Flat-panel detectors, 515
Flexural strength (FS), 16, 186 188
Flowable bulk-fill materials, 158
Flowable composites, 137 139
Fluorapatite, 220 222, 385 386, 399 403,
454, 478 480, 689
Fluorescent agents, 136
Fluoride, 26 27
anticariogenic potential, 152
concentrations, in SDF products, 691
fluxes, 179 180
toxicity, 27
Fluoride release
from fillers, 152
from GICs, 183 185
affecting factors, 184 185
chemical adhesion with tooth, 188 189
compressive strength, 185 186
esthetics, 188
flexural strength, 186 188
GICs in ART, 189
mechanism, 184
moisture sensitivity of GICs, 189
nanoapatite-filled glass ionomers,
189 190
RMGICs, 190 191
source of fluoride, 183 184
thermo-cured glass ionomers, 190
and recharge of compomer, 153 154
restorative materials, 218
Fluoride-based BAG (F-BAG), 247
Fluoride-containing BG (BiominF), 464,
465t
Fluoride-modified dental implants, 590
Fluorine ions, 242 243
Fluorine-containing glass ceramics, 58
714
Fluormica, 58
Fluoroaluminosilicates, 178, 179f
components, 179t
glass, 218
Fluorocore composite, 114 115
Fluorohydroxyapatite (FHA), 400, 689
Fluorophlogopite, 58, 59t
Food grade silicones, 623
Force, 16 17
Foreign body reaction, 29 30
Formability, 549, 554 555
Formaldehyde, 27 28
Four-point flexural bond strength, 73
Fourth-generation adhesives, 238 239
FPD. See Fixed dental prosthesis (FPD)
Fractographic analysis of zirconia
restorations, 333 335
Fracture
resistance, 167t
stress, 19
toughness, 467 468
FRCs. See Fiber-reinforced composites
(FRCs)
Free-radical addition polymerization, 82 83
Freeze-dried bone allograft (FDBA), 354
Fresh allografts, 353
FRIACOM (computer-assisted analysis
device), 514
Frozen allografts, 353
FS. See Flexural strength (FS)
FTIR analysis, 180 182
Functional tissue engineered products, 1
Functionally graded materials (FGMs), 590
Functionally graded/hierarchical dental
implant surfaces, 590
G
GAG. See Glycosaminoglycan (GAG)
Gamma waves, 77
Gel form, 86
Gel point, 142
Gelation phase in GICs, 182
Generex B ProRoot Endo Sealer, 284t
Gentamicin sulfate, 462
Geometric Studio, 518
GFRCs, 308
Gibbs free energy, 75
GICs. See Glass-ionomer cements (GICs)
Gilmore test for final setting time, 47
Index
Glass, 318
fibers, 133, 307
particles, 218 219
polyalkenoate cements, 175 176
powder decomposition, 182
transition temperature, 11, 455
Glass A, 307
Glass C, 307
Glass Carbomer by GCP Dental,
Netherlands, 189 190
Glass ceramics, 55 56
feldspathic porcelain, 56 58
fluorine-containing glass ceramics, 58
leucite-reinforced porcelain, 58
lithium disilicate, 58 61
Glass E, 307
Glass ionomers, 177, 177f, 189 190,
361 362
conventional, 218 219
nanoapatite-filled, 189 190
as “nondental” cement, 191
sealers, 280, 286t
thermo-cured, 190
Glass ionomer cement (GIC), 677
Glass R, 307
Glass S, 307
Glass-ceramics, 306, 319 321
blocks, 527 528
Glass-infiltrated aluminum-oxide ceramic,
61
Glass-infiltrated ceramics, 321 322
Glass-infiltrated zirconia development,
337 338
Glass-ionomer cements (GICs), 2, 175 176,
217 219, 290 292, 306, 487
applications, 219
in ART, 189
ASPA, 177, 177f
chemistry of setting reaction, 181 183
components, 178 181
composition and nature
of acid component, 180 181
of glass component, 178 180
decomposition of glass powder, 182
development, 176 178
fluoride release from, 183 185
gelation phase, 182
maturation phase, 183
moisture sensitivity of, 189
Index
nanomodifications of GIC powders,
219 224
setting reaction in, 181 183
water, 181
Glossary of Prosthodontics Treatment
(GPT), 616
GLUMA, 290 292
Glycerol phosphate-dimethacrylate (GPDM),
130, 156 157, 158f
Glycosaminoglycan (GAG), 648
GNS. See Graphene nanosheets (GNS)
GO. See Graphene oxide (GO)
GO chitosan hydroxyapatite
(GO CS HA), 603
Gold, 107, 305
advantages and disadvantages of gold
wires, 556t
alloys, 555 556
fillings, 107 108, 108f
gold copper alloy system, 15
plated brackets, 550
GP. See Gutta-percha (GP)
GPDM. See Glycerol phosphatedimethacrylate (GPDM)
GPT. See Glossary of Prosthodontics
Treatment (GPT)
Grain boundaries sliding, 61 62
Grandio (Voco, Germany), 130 131
Graphene
and derivatives, 599 600
films, 599
to improve cementitious materials,
600 609
nanofillers, 609
Graphene nanosheets (GNS), 603, 604f
Graphene oxide (GO), 599 600, 605f
GO-modified scaffolds, 606 607
GO-modified β-tricalcium phosphate
scaffold, 607 608
Grassmann’s law, 8 9
Gray unit (Gy unit), 513
Green Elgiloy, 558
Green machining, 519
Green tea extract, 153
Grit-blasting, 70 71, 337, 589
GTR membranes. See Guided tissue
regeneration membranes (GTR
membranes)
Guided surgery, 526
715
Guided tissue regeneration membranes (GTR
membranes), 483 484
Gusuibu, 355
Gutta-percha (GP), 219, 275 277, 276t
GuttaFlow Bioseal, 600
GuttaFlow sealer, 489
Gy unit. See Gray unit (Gy unit)
Gypsum products, 2, 37 38
H
HA. See Hyaluronic acid (HA);
Hydroxyapatite (HA)
Hafnia (HfO2), 75 76
Hap. See Hydroxyapatite (HA)
Hard relining, 95
Hardness, 117 118, 305
HCA. See Hydroxy-carbonate apatite (HCA)
HCl. See Hydrochloric acid (HCl)
Heat
of fusion, 11, 12t
heat-activated resins, 97 98
heat-cured acrylic resins, 83
heat-cured acrylics, 95
HEBP. See 1-Hydroxyethylidene-1,1bisphosphonate (HEBP)
HEMA. See Hydroxyethyl methacrylate
(HEMA)
Hemihydrate crystalline species, 39
Herculite XRV (Kerr, United States),
130 131
Hexafluoroisopropanol-based silk (HFIPbased silk), 651
HF. See Hydrofluoric acid (HF)
HFIP-based silk. See Hexafluoroisopropanolbased silk (HFIP-based silk)
High molecular-weight resin, 149
High-copper
amalgam, 116 117
dental amalgam, 112 113
High-strength core ceramics, 55 56
High-temperature vulcanization silicone
(HTV silicone), 624 625
Highest occupied molecular orbitals
(HOMO), 75, 76f
HL. See Hybrid layer (HL)
HOMO. See Highest occupied molecular
orbitals (HOMO)
Homogeneous conductor’s resistance, 15
Hot isostatic pressing, 61 62
716
Hot pressing, 61 62
HTR Synthetic Bone, 357
HTV silicone. See High-temperature
vulcanization silicone (HTV silicone)
“Hue”, 8 9
Human tissue replacements, 1
Human-derived biomaterials, 647
Hyaline, 407 408
Hyaluronate. See Hyaluronic acid (HA)
Hyaluronic acid (HA), 651
Hybrid
acrylic, 83
ceramic, 159 165
reinforcement, 91
Hybrid layer (HL), 231 232
Hydration, 47
Hydrochloric acid (HCl), 590, 621 622
Hydrocolloids, 198
Hydrofluoric acid (HF), 65 66, 332, 590
etching, 65 67, 66f, 67t
Hydrogen peroxide (H2O2), 269
Hydrolyzable alkyl group, 134
Hydrophilic
elastomeric IMs, 202 203
IMs, 208
PEG hydrogels, 654
Hydrophilicity, 585 586
Hydroxy-carbonate apatite (HCA), 454
Hydroxyapatite (HA), 28, 220 222, 230,
347 348, 357 359, 358t, 360f,
386 387, 388t, 399 403, 454 455,
478 480, 646, 654 657
fillers, 91
HA-containing toothpaste, 393 394
HA/GNS composites, 607 608
nanocrystals, 485
structure, 394
Hydroxyethyl methacrylate (HEMA),
156 157, 190
1-Hydroxyethylidene-1,1-bisphosphonate
(HEBP), 269, 270t
Hydroxyl-free radicals (HO2), 269
Hygroscopic setting expansion, 47 51, 47t,
48f
compressive strength, 49
dimensional stability, 51
mixing technique, 42 43
pouring the impression, 43
properties, 38
Index
reproduction, 49
setting processes, 44 46
fineness, 46
modifying agents, 45 46
effect of pH, 46
rate of setting reaction, 44
spatulation, 45
stages, 44
temperature, 45
W/P ratio, 45
setting time
final setting time, 46 47
gilmore test for final setting time, 47
initial setting time, 46
surface hardness and abrasion resistance,
50 51
tensile strength, 50
types, 40 41, 41f
Hypoallergenic resins, 91
Hypochlorous acid (HOCl), 231 232
Hypoclean A, 270t
Hypoclean B, 270t
I
IA. See Itaconic acid (IA)
ICADS. See International Caries Assessment
and Detection System (ICADS)
ICP, 183
ICs. See Impression compounds (ICs)
IGI. See Image-guided implantology (IGI)
IIT. See Image intensifier tubes (IIT)
IKI. See Iodine potassium iodide (IKI)
Image intensifier tubes (IIT), 515
Image-guided implantology (IGI), 525
Imidazole-modified CS, 652
Immobilization, 485 486
Immunomodulatory strategies, 365 366
Implant3D Media Lab Software, 523
ImplantMaster TM software, 523
Implants
coating, 463
failure, 583
FRCs in, 311
grade silicones, 622
technologies, recent advances in,
522 523
Impregnation of fibers with polymer matrix,
310
Impression compounds (ICs), 205
Index
Impression materials (IMs), 198
comparison of various types of dental
impression properties, 210t
dimensional accuracy/dimensional
stability, 207 208
elastic, 200 204
recovery/flexibility, 208 209
inelastic, 204 206
mechanical properties, 209
miscellaneous, 209 211
wettability, 208
Impression plasters (IPs), 205 206
Impression wax, 204 205
IMs. See Impression materials (IMs)
In vitro cytotoxicity, 26
In vitro testing, 23
In vivo study, 660
In vivo testing, 24
Incremental layering technique, 143
Indirect composites, 138, 159 165, 163t
Indirect contact tests, 23
Indirect dental materials, 217 218
Indirect tensile test, 20
Industrial grade silicones, 623
Industrial milling, 518 519
Inelastic impression materials. See Elastic
impression materials
ICs, 205
impression wax, 204 205
IPs, 205 206
metallic oxide pastes, 206
Infiltrated ceramics, 306
Inflammatory cells, 29 30
Infrared (IR)
analysis, 183
spectroscopy, 457 458
Initiator accelerator system, 134 136
dual-cured composite, 136
light-cured composites, 135 136
self-cured composites, 135
Inkjet 3D printers, 663 664
Inorganic fillers, 130
particles, 486
Inorganic oxides, 136
Inorganic polyP, 361
Inox steel. See Stainless steel brackets (SS
brackets)
Intermediate restorative material (IRM),
290 292, 291t
717
International Association for Dental
Research, 189, 386
International Caries Assessment and
Detection System (ICADS), 516
International Standards Organization (ISO),
276
Intracanal medicaments, 271 274, 272t
bioactive glass, 274
calcium hydroxide, 271 272, 275f
chlorhexidine, 272 273
Ledermix, 273
rationale of usage, 271b
triple antibiotics pastes, 273
Intraoral capture, 518
Intraoral digital imaging, 509 510, 510t
Intraoral digital radiography, 514 515
Intraoral prostheses, 616
Intraoral radiography, 508 509
Intrinsic stains, 636, 637f
Invisalign
appliance by Align Technology, 562,
564 565
trays, 569
Iodine potassium iodide (IKI), 265, 269
Ion-delivering agents, 385 386
Ionomers, 220 222
salt hydrogel, 190 191
IPs. See Impression plasters (IPs)
IRM. See Intermediate restorative material
(IRM)
Iron, 543 544
Iron oxide, 136
iRoot, 600 601
iRoot SP, 284t
ISO. See International Standards
Organization (ISO)
Isocyanates, 571
chemical reaction for synthesis of
polyurethanes from, 571f
Itaconic acid (IA), 218
K
Ketac, 487
Ketones, 82
Kevlar fibers, 88
L
Laboratory milling, 518 519
Lactobacillus, 378
718
Lactobacillus acidophilus, 690 691
Lactose-modified CS, 649
LASER. See Light amplification by the
stimulated emission of radiation
(LASER)
Laser etching technique, 235 236. See also
Acid etching technique
Lasers, 71, 331
irradiations, 235 236, 331
Lava, 529
LCUs. See Light control units (LCUs)
LED. See Light-emitting diode (LED)
Ledermix, 273
Leucite (K2O Al2O3 4SiO2), 322
leucite-based ceramics, 323
leucite-reinforced ceramics, 319
leucite-reinforced porcelain, 58
Light
amplification, 71
fluorescence technology, 516
Light amplification by the stimulated
emission of radiation (LASER),
531 532
and dental applications, 530 533
in dentistry, 531
light, 532
mechanism of laser action, 532 533
Light control units (LCUs), 136
Light-curing
composites, 135 136
photoinitiators, 135 136
duration effect, 140
modes, 142 143
resins, 146
system effect, 139 140
tip distance effect from RBC surface, 140
Light-emitting diode (LED), 140
Linear polymers, 620
Lining material use, 155 156
Lipopolysaccharides (LPS), 266 267
Liquid, 86
Liquid silicone rubber (LSR), 627, 627t
Lithium disilicate (Li2O 2SiO2), 58 61,
319, 322
lithium disilicate based ceramics, 323
lithium disilicate ceramic blocks,
527 528
reinforced ceramics, 319
Lithography, 219 220
Index
LMSRT (computer-assisted analysis device),
514
Load deflection rate, 554
Local toxicity, 24
Long-term fluoride release, 184
“Loosely bound” water, 181
Low elastic modulus liners, 143
Low molecular-weight compounds,
128 130
Low-and medium-fusing dental porcelain
frits, 58
Low-copper dental amalgam, 112
Low-shrinkage composites, 148 150
Dimer acid based dimethacrylate
monomer, 150
high molecular-weight resin, 149
low-shrinkage TCD urethane based
monomer, 150
ring-opening epoxy siloxane, 148 149
Low-shrinkage TCD urethane based
monomer, 150
Low-temperature degradation (LTD), 63,
332
“Lower contraction stress” monomers, 143
Lower shrinkage stress monomer chemistry,
143
Lowest unoccupied molecular orbitals
(LUMO), 75, 76f
LPS. See Lipopolysaccharides (LPS)
LSR. See Liquid silicone rubber (LSR)
LTD. See Low-temperature degradation
(LTD)
Lucirin, 136
Luminous reflectance, 8 9
LUMO. See Lowest unoccupied molecular
orbitals (LUMO)
Luting/lining cement, 176
Luvit, 533 534
M
M-510 gel catalyst, 628
M-511 platinum silicone rubber, 628 631
properties, 629
silicone fluids, 629 631
M-513 softening agent, 628
M-514 antislump agent, 628
Machining, 219 220
of restorations, 519
Macrolevel surface roughness, 585
Index
Magnesia (MgO), 63
Magnesium (Mg), 362
biodegradable materials, 362
Magnetic resonance imaging (MRI),
508 515, 511t, 663 664
clinical applications, 509 512
intraoral, extraoral, including cone beam
CT, 508 509
limitations, 512 515
Maleic acid, 218
Malleability, 19
Mandibular autografts, 352 353
Manganese (Mn), 543 544, 544t
Marginal sealing, 116 117
Martensitic active NiTi, 560
Martensitic steels, 547
Matrix metalloproteinases (MMPs), 692
Maturation, 218 219
phase in GICs, 183
Maxillofacial pathology, 383 385
Maxillofacial prosthetic rehabilitation, 3
coloring agents, 635 638
historical background, 616, 617t
ideal properties of maxillofacial material,
617, 618t
M-511 platinum silicone rubber, 628 631
mechanical and physical properties, 618t
primers, 632
search for ideal materials for, 617 620
silicones, 620 622
skin adhesives, 638 639
soft liners and tissue conditioners,
633 635
Maxillofacial prosthodontics, 616
Maxillofacial silicones, 622 628. See also
Silicones
A-304, 632
A-306, 632
A-330G, 632
A-2186, 626, 626f
common room temperature vulcanizing
silicones, 625 626
comparative properties, 627t
food grade, 623
G-611, 632
HTV silicone elastomer, 625
implant grade, 622
industrial grade, 623
MDX4 4210, 626
719
medical grade, 623
liquid silicone elastomers, 627
VerSiTal silicone elastomers, 628
recommendations, 627
research studies about, 630t
RTV silicone elastomer, 624 625
Maxillofacial surgery, 407
Maximum elastic deflection, 554
Maximum flexibility, 554
MCPA. See Monocalcium phosphate
anhydrous (MCPA)
MCPM. See Monocalcium phosphate
monohydrate (MCPM)
MDP. See Methacryloyloxydecyl dihydrogen
phosphate (MDP)
MDPB. See Methacryloyloxydodecyl
pyridinium bromide (MDPB)
Mechanical surface conditioning
grit-blasting, 70 71
laser, 71
polishing/grinding, 71
Medical grade
liquid silicone elastomers, 627
silicones, 623, 623f
VerSiTal silicone elastomers, 628
Melt-blending process, 590 592, 591f
Mercury toxicology, 118 119, 119t
Mesenchymal stem cells (MSCs), 469,
583 584, 606 607
4-MET. See Trimelitic acid methacrylate (4MET)
Metal brackets, 542 550. See also Ceramic
brackets
CoCr brackets, 548
precious, 550
SS brackets, 543 547
titanium brackets, 548 549
Metal(lic), 217 218, 305, 658 661
biodegradable metal scaffolds, 658 659
ceramics, 306
core of PFMs, 318 319
metal-free restorations, 380
metal-reinforced cements, 178
nanoparticles, 659
oxide pastes, 206
oxides, 320
titanium, 659 660
zirconia, 660 661
Methacrylate resin
720
Methacrylate resin (Continued)
liners, 97
sealers, 280, 281t
Methacrylate-based SEP, 236
Methacrylic acid, 128
Methacryloxylethyl-cetyldimethyl ammonium
chloride (DMAE-CB), 153
Methacryloyl fluoride methyl acrylate, 152
Methacryloyloxy propyltrimethoxysilane
(MPS), 68
Methacryloyloxydecyl dihydrogen phosphate
(MDP), 68 70, 130, 330
Methacryloyloxydodecyl pyridinium
bromide (MDPB), 153, 242 243
2-Methacryloyloxyethyl phosphorylcholine,
dimethylaminohexadecyl
methacrylate (DMAHDM), 243 244
Methyl groups (CH3 groups), 621
Methyl methacrylate monomers, 82 83
Methyl methacrylate structure, 83
Methylchloride, 621 622
Methylpyrrolidinone CS, 652
MFP. See Monofluorophosphate (MFP)
MFP 1 DCPD, 387
MI varnish, 396 397
μ-ONE HA implant, 400
MicroMega MTA, 600
Microspheres of Mg-doped TCP, 398 399
Microwave-cured acrylic resins, 84 85
Milling, 219 220
burs, 519
Mineral trioxide aggregate (MTA),
257 261, 261t, 284, 600, 661 662
MTA Angelus, 262
MTA Bio, 600
MTA Fillapex, 284t, 600 601
MTA HP Repair, 600
MTA Plus, 284t, 600 601
Mineralization, 600 601
Mineralized freeze-dried bone allografts, 354
Mineralized tooth structure, 230
Minimally invasive dentistry, 319 320, 465,
675 676
Mixing technique
adding powder and water, 43
measuring powder, 42
measuring water, 42
Modified glass bead sterilizer, 155
Modified stone. See Modified α-hemihydrate
Index
Modified α-hemihydrate, 39 40
Modulus of elasticity, 553
Modulus of resilience, 554
“Moist bonding” technique, 242
Moisture sensitivity of GICs, 189
Molybdenum, 543 544, 544t
“Monoblock”, 277
Monocalcium phosphate anhydrous
(MCPA), 358t, 395
Monocalcium phosphate monohydrate
(MCPM), 358t, 389 390, 395
Monochromatic light, 8 9
Monocrystalline alumina brackets, 552
Monofluorophosphate (MFP), 387
Monolithic restoration, 517
Monolithic zirconia, 63 64
Monomer chemistry, 141
Monomer phosphate, 333
Moodle platforms, 533 534
MPS. See Methacryloyloxy
propyltrimethoxysilane (MPS)
MRI. See Magnetic resonance imaging
(MRI)
MSCs. See Mesenchymal stem cells (MSCs)
MTA. See Mineral trioxide aggregate
(MTA)
MTAD, 267 269, 268t
MTAS, 284t
Mucocompressive techniques, 198 199
Mucosa supported guides, 526
Mucositis, 413
Mucostatic techniques, 198 199
Multiphasic CaPO4 formulations, 404
Multistranded NiTi wires, 560
Multistranded stainless steel wires, 557
N
N,N-dimethyl-p-toluidine, 135
N-vinylpyrrolidone (NVP), 222
N’Durance composite, 150
NACP. See Nanoparticles of amorphous
calcium phosphate (NACP)
NaF. See Sodium fluoride (NaF)
NAg. See Nanoparticles of silver (NAg)
Nano-FAp (nFAp), 220 222
Nano-Hap. See Nanohydroxyapatite (nHAp)
Nano-RMGICs. See Nanomodified resinmodified glass ionomer cements
(Nano-RMGICs)
Index
Nano-TiO2 (nTiO2), 222 223
Nanoapatite-filled glass ionomers, 189 190
Nanobiomaterials, 478, 481. See also
Restorative nanobiomaterials
dental applications, 481 492
endodontic, 488 490
for preventive dentistry, 482 483
Nanocapsules, 245
Nanoclusters, 133, 133f
Nanocomplexes in CPP ACP, 483
Nanocomposites, 486 487
Nanodentistry, 477 478
Nanodiamond coatings, 485 486
Nanodiamond-loaded poly(lactide-coglycolide), 483 484
Nanofibrous scaffolds, 490
Nanofilled composites, 138 139
Nanofilled resin composite, 132 133
Nanofillers, 133, 133f
Nanoglass ionomer cement
applications of GICs, 219
nanomodifications of GIC powders,
219 224
Nanoglass ionomers, 487 488
Nanohydroxyapatite (nHAp), 220 222, 652
gutta percha, 489
Nanohydroxyl apatite toothpaste, 483
Nanoionomers, 487 488
Nanomaterials, 477 478, 481t, 490, 602.
See also Biomaterials
applications in disciplines of dentistry, 482f
characterization, 478, 480f
for dental implants, 484 486
general properties, 480 481
for periodontics, 483 484
potential, 492 493
and tissue engineering, 490 491
Nanomodifications
of GIC powders, 219 224
GIC modified with nanoparticles,
222 223
mechanical properties of, 221t
nanohydroxyapatite and ionomers,
220 222
nanomodified RMGICs, 223 224
powder-based, 220
of GIC powders, 219 224
glass ionomer cements modified with
other nanoparticles, 222 223
721
mechanical properties, 221t
nano-RMGICs, 223 224
nanohydroxyapatite and ionomers,
220 222
powder-based nanomodification of
GICs, 220
Nanomodified resin-modified glass ionomer
cements (Nano-RMGICs), 223 224
Nanoparticles (NPs), 82
GIC modified with, 222 223
nanoparticles-based endodontic sealer,
488 489
Nanoparticles of amorphous calcium
phosphate (NACP), 242 243
Nanoparticles of silver (NAg), 242 243
Nanoscience, 478 480
Nanosized HAp, 222
Nanosized zirconia (nZrO2), 222
Nanostructured titanium implant surfaces,
589
Nanotechnology, 219, 477 478
Nanozirconia, 485
Native collagen, 647
Natural biomaterials, 217 218, 478 480,
647 653. See also Synthetic
biomaterials
agarose, 653
alginate, 649 650
collagen, 647 648
CS, 651 653
elastin, 653
fibrin, 648 649
hyaluronate, 651
silk, 650 651
Natural materials at metric scales, 478, 479f
Natural polymers, 646
Natural tissues for bone grafting, 350 362
Naturally derived scaffold materials,
644 645
Naval Ordinance Laboratory (nol), 558 559
NBOs. See Nonbridging oxygens (NBOs)
NC. See Network connectivity (NC)
Neodymium (Nd), 531
Neodymium:yttrium aluminium garnet
laser (Nd:YAG laser), 531
NeoMTA Plus, 600
Network connectivity (NC), 455
Newtonian fluids, 14
nFAp. See Nano-FAp (nFAp)
722
Index
nHAp. See Nanohydroxyapatite (nHAp)
Nickel, 543 544, 544t
Nickel-containing alloys, 27 28
Nickel titanium wires (NiTi wires),
558 560
advantages and disadvantages, 559t
generations, 559 560
Niobium (Nb2O5), 543 544, 544t, 602
Nisin, 244 245
NiTi wires. See Nickel titanium wires (NiTi
wires)
Nitinol, 558 559
Nitric acid (HNO3), 590
Nitrogen, 543 544, 544t
NMR analysis, 183
Nonbiodegradable materials, 644
Nonbonded amalgam restorations, 113 114
Nonbonded bonded amalgam restorations,
114
Nonbridging oxygens (NBOs), 178 180,
457
Noneugenol sealers, 286t
“Nonevaporable” water. See “Tightly
bound” water
Noninvasive radiography, 508
Nonreleased antibacterial agents, 152t
Nonthermal processes, 590 592
Normal setting expansion, 47
Novabone product, 461
Novamin, 464, 465t
NPs. See Nanoparticles (NPs)
NVP. See N-vinylpyrrolidone (NVP)
Nylon fibers, 88 89
Organofunctional (methoxy) group, 134
Organofunctional silanes, 134
Ormocers, 109
Orthodontic(s), 312, 383 385, 407 409,
541
archwires, 553 562
classification, 555 562, 555f
properties and ideal features, 553 555,
554f
brackets, 542 553, 543t
classification of orthodontic materials,
542b
clear aligners, 562 572
tooth movement, 565 566
OrthoMTA, 600
Orthophosphate ions, 390 391
Osseoconductive materials, 586
Osseointegration, 29, 581 582, 659
cellular and biomaterial aspects, 583 584
Osteoblasts, 347 348
Osteocalcin, 606
Osteoconduction, 349
Osteoconductive grafts, 645
Osteogenesis, 349, 606 607
Osteoinduction, 29, 348 349
Osteopontin, 606
Oxide ceramics, 55 56
densely sintered aluminum-oxide ceramic,
61 62
glass-infiltrated aluminum-oxide ceramic, 61
zirconia, 62 64
Oxiranes, 148 149
Oxyapatite, 358t
O
Occlusal imaging technique, 510t
Octacalcium phosphate (OCP), 358t, 396
Odontoblasts, 303 304
“One-bottle” systems, 239
“One-step self-etch” adhesive system.
See Seventh-generation adhesives
Open systems, 518 519
Oral
cavity, 71
pathology, 383 385
surgery, 407
tissues, 37 38
Oral hygiene instruction (OHI), 684
Organic acids, 378
P
PAA. See Polyacrylic acid (PAA)
Packable composites, 138 139
Packing techniques, 158f
Panoramic imaging technique, 511t
para-chloroaniline (PCA), 267
Paraffin, 9 11, 10f
Partial fiber reinforcement, 87
Particle size of bioactive glasses, 468 469,
468t
Particulate filler composites, 136
Particulate-reinforced resins
alumina, 89 90
titanium, 90 91
zirconia, 90
Index
Pattern wax, 204 205
PCA. See para-chloroaniline (PCA)
PCL. See Poly-e-caprolactone (PCL)
PDGF. See Platelet-derived growth factor
(PDGF)
Pediatric dentistry, 383 385
PEEK. See Polyetheretherketone (PEEK)
PEG. See Polyethyleneglycol (PEG)
PENTA. See Dipentaerythritol Penta acrylate
phosphate (PENTA)
Peptide-based biomaterials, 647
Perforation repair materials, 292 293, 293b
Periapical imaging technique, 510t
Periodontal disease, FRCs in, 312
Periodontics, 383 385, 411 413, 411f.
See also Orthodontic(s)
nanomaterials for, 483 484
Periodontology. See Periodontics
PerioSim, 534
Periradicular surgery, 290
PET-G. See Polyethylene terephthalate-G
(PET-G)
PET-G polymer, 569
PFM. See Porcelain-fused metal (PFM)
PFZ. See Porcelain fused to zirconia (PFZ)
PGA. See Polyglycolic acid (PGA)
pH effect, 46
17 4 PH SS alloys, 547
Phagocytic mechanisms, 364
Pharmacology, 2
Pharmacy, 2
Phenol-formaldehyde, 79 80
Phenyl-propanedione (PPD), 135 136
photoinitiator systems, 136
Phosphate
glass, 454
phosphate-based bioglasses, 657 658
Phosphoric acid, 233
gel, 330
Phosphorous, 543 544, 544t
Phosphorous pentoxide (P2O5), 657 658
Photography, 516 517
Photoinitiators, 135 136
Photopolymerization, 108 109
Photostimulable phosphor plates (PSP), 514
PICN. See Polymer-infiltrated ceramic
network (PICN)
Pigments, 136
Planmeca Planmill system, 518 519
723
Plasma
gas etching treatment, 590 592
proteins, 583
technology, 331
Plaster of Paris, 217 218
Plastic
brackets, 550 551, 551t
plastic-coated NiTi, 560
region, 17 19
Plasticizers, 86, 619
Platelet-derived growth factor (PDGF), 349,
364 365
Platelets, 583
Platinum primers, 632, 633t
PMMA. See Polymethyl methacrylate
(PMMA)
Polishability, 138 139
Polishing/grinding, 71
Poly-e-caprolactone (PCL), 654 655
Poly-Works, 518
Poly(1,4-b-D-glucopyranosamine).
See Chitosan
Poly(acrylic acid) (PAA), 176 177,
180 181, 190, 218 219
Poly(alkenoate) cement, 188
Poly(alkenoics), 180
Poly(D,L-lactide-co-glycolide), 483
Poly(D,L-lactide), 483
Poly(L-lactide)-co-(e-caprolactone) scaffolds,
483 484
Poly(methylmethacrylate)-based denture
materials, 590 592
Polyacid(s), 180 181, 218
modified composite, 153 154
Polyaminocarboxylic acid, 266f
Polybiquanide family, 273f
Polycarbonate, 93
Polycrystalline
alumina brackets, 552
ceramics, 306, 320, 328
zirconia, 552
Polydimethylsiloxane. See Silicones
Polyelectrolyte cement, 176 177
Polyelectrolytes, 180
Polyethene, 89
Polyetheretherketone (PEEK), 586 587
dental implant modification, 590 592
Polyethers, 200, 200f
polyether ether ketones, 3
724
Polyethylene, 308
fibers, 133
Polyethylene oxide. See Polyethyleneglycol
(PEG)
Polyethylene terephthalate-G (PET-G), 562
Polyethyleneglycol (PEG), 647, 654
Polyglycolic acid (PGA), 415, 655
PolyHEMA matrix, 190 191
Polymer-infiltrated ceramic network (PICN),
73, 74t
blocks, 159 165
materials, 165
Polymeric/polymer(s), 357
fibers, 133
matrix
fibers adhesion to, 310
impregnation of fibers with, 310
polymer-based biomaterials, 647
polymer-infiltrated ceramics, 58, 64 65
polymer monomer ratio, 82
reinforced composites, 586 587
Polymerization
chemical structure and mechanism of,
82 85
curing mechanisms of acrylic denture base
materials, 83 85
initiators, 190
kinetics, 142
shrinkage, 138, 140 143, 311
Polymerization shrinkage stress, 141, 155
affecting factors in dental composites
C-factor, 142
polymerization kinetics, 142
substrate compliance, 142
viscoelastic behaviour, 142
volumetric shrinkage, 141 142
water sorption, 142
consequences, 141f
management
incremental layering technique, 143
light-curing modes, 142 143
low elastic modulus liners, 143
lower shrinkage stress monomer
chemistry, 143
preheating, 143
Polymethyl methacrylate (PMMA), 79 80,
82, 99, 357
Polyoxyethylene. See Polyethyleneglycol
(PEG)
Index
Polyphosphates (polyP), 361
Polypropylene fibers, 89
Polysaccharide-based biomaterials, 647
Polysiloxane (PVS), 202 203, 203f,
207 208
Polysorbate-80 detergent (Tween 80),
267 269
Polysulfide, 201
Polyurethane (PC), 564
brackets, 550 551
elastomers, 619
Polyvinyl chloride (PVC), 81
and copolymer, 619
Porcelain, 56, 71
Porcelain fused to zirconia (PFZ), 320
Porcelain-fused metal (PFM), 58, 318
Porcine bone graft tissue, 355
Pore-free high-fusing product, 57
Porous Fe alloys, 658
Portland cement, 257 261
Positive air pressure method, 565
Postextraction bone resorption, 412
Potassium iodide (KI), 675 676, 684
Potassium sulfate (K2SO4), 205 206
Pour-type denture resins, 85
Powder-based nanomodification of GIC, 220
Powder liquid ratio, 49, 85 86
liquid, 86
powder, 85 86
PPD. See Phenyl-propanedione (PPD)
Pre-gel stage, 142
Precipitated hydroxyapatite, 358t
Precipitation-hardenable steels, 547
Preheating, 143
Prepolymerized filler(s)
fabrication, 132, 132f
particles, 132
Pressure, 16 17
Presurgical 2D radiograph imaging, 522
Preventive dentistry, nanobiomaterials for,
482 483
Preventive nanocomposites surface coatings,
482 483
Primers, 67 70, 231, 632
Pristine graphene films, 599 600
Procera-software, 523, 529
Processing wax, 204 205
Proportional limit, 18
ProRoot MTA Gray, 257 261
Index
Prosthetic abutments, 528
Prosthetic dentistry. See Prosthodontics
Prosthodontics, 312, 383 385, 409 411
Protein-based biomaterials, 647
Proton-extruding adenosine triphosphatase,
691
PSP. See Photostimulable phosphor plates
(PSP)
“Pulse-delay”, 143
Punch-test method, 21
Pure titanium wires, 561 562
PVC. See Polyvinyl chloride (PVC)
PVS. See Polysiloxane (PVS)
Pyrolysis, 458 459
Pyroplastic flow, 57
Q
QADM. See Quaternary ammonium
dimethacrylate (QADM)
QDs. See Quantum dots (QDs)
QMiX, 270, 270t
QPEI. See Quaternary ammonium
polyethyleneimine (QPEI)
QTH, 139
QTH LCU, 139 140
Quantum dots (QDs), 245
Quaternary ammonium compounds, 153
Quaternary ammonium dimethacrylate
(QADM), 153, 242 243
Quaternary ammonium polyethyleneimine
(QPEI), 153, 489
Quick-Set, 600
R
Radiograph operators, 514
Raman analysis, 180 181
Range of activation, 554
Range of deflection, 554
RANKL. See Receptor activator of nuclear
factor jB ligand (RANKL)
Rapid heat-polymerized resin, 83
Rapid Injection System, 92
Rapid prototyping (RP), 93 94, 519 520
RapidForm, 518
Rayon flocking for silicone elastomers,
635 636, 636f
Recaldent, 396 397
Receptor activator of nuclear factor jB
ligand (RANKL), 364 365
725
Recombinant human bone morphogenetic
protein-2 (rhBMP-2), 413
Recombinant human growth and
differentiation factor-5 (rhGDF-5),
413
Recombinant human platelet-derived growth
factor BB (rhPDGF-BB), 413
Red Elgiloy, 558
Reduced GO (rGO), 600
Regenerative tissue engineering, 644
Reinforcement glass. See Glass R
Released antibacterial agents, 152t
Relief ACP, 393 394
Remineralization, 378f, 391 392, 465
Resilience, 19, 19f
Resilon, 277
Resin composites, 128
attempts for improvement
regarding both material formulation and
manipulation, 156 165
regarding manipulation, 154 156
regarding material formulation,
148 154
chemical structure of resin systems, 131f
classification
according to composite consistency,
137 138
according to curing techniques, 138
according to fillers size and
distribution, 136, 137f, 137t
according to packing (placement)
technique, 138
clinical indications, 138 139
composition
fillers, 130 134
initiator accelerator system, 134 136
pigments, 136
resin matrix, 128 130
silane coupling agent, 134
degradation, 147
evolution, 129f
guidelines for laboratory evaluation, 166
methods for mechanical evaluation, 167t
properties and limitations
biocompatibility, 145 147
clinical durability, 147 148
degradation, 147
degree of conversion, 139 140
esthetic properties, 144 145
726
Resin composites (Continued)
mechanical properties, 145, 146t
polymerization shrinkage, 140 143
polymerization shrinkage stress, 141
solubility, 144
thermal properties, 144
recommendations for future clinical
studies, 166 171
strain, 141
Resin-modified glass-ionomer cements
(RMGICs), 190 191, 223 224, 487
nanomodified, 223 224
Resin(s), 620
cements, 130
increment thickness effect, 139
matrix, 128 130
resin-based composites, 136
restorations, 138
resin-based dental composites, 486
resin-based materials, 319
resin-modified cements, 178
resin ceramic bond strength, 71
resin ionomer suspension and compomer,
292
sealers, 280 283, 286t
shade effect, 139
Resistivity values of dental hard tissues, 15, 15t
Resorbable-GTR membranes, 483 484
Restoration, 317
Restorative dental biomaterials, 380
Restorative dental materials, 15, 318
Restorative dentistry, 107, 317
Restorative materials, 218, 469
Restorative nanobiomaterials, 486 488.
See also Nanobiomaterials
nanocomposites, 486 487
nanoglass ionomers, 487 488
RetroMTA, 600
Retroplast, 290 292
Retroplast-GLUMA system, 290 292
RGD peptides, 651
rGO. See Reduced GO (rGO)
rhBMP-2. See Recombinant human bone
morphogenetic protein-2 (rhBMP-2)
rhGDF-5. See Recombinant human growth
and differentiation factor-5 (rhGDF-5)
rhPDGF-BB. See Recombinant human
platelet-derived growth factor BB
(rhPDGF-BB)
Index
Rigid IMs, 198 199
Ring polymers, 620
Ring-opening epoxy siloxane, 148 149
RMGICs. See Resin-modified glass-ionomer
cements (RMGICs)
Room-temperature vulcanization silicone
(RTV silicone), 98, 624 625
cross-linking
by addition reaction, 625
by condensation reaction, 624 625
Root canal
chlorhexidine, 266 267
citric acid, 267
EDTA, 265 266
filling materials, 404 405
HEBP, 269
hydrogen peroxide, 269
IKI, 269
irrigants
interactions between different, 268t
properties and effects of, 264t
materials used as root canal irrigants,
263 270
MTAD, 267 269, 268t
obturation, 404 405
materials, 274 289
properties, 263b
QMiX, 270, 270t
sealers, 277 289, 278b, 286t
sodium hypochlorite, 263 265
tetraclean, 269
Root caries management in the elderly, 684
Root-end filling materials, 290 292
Amalgam, 290
composite resins, 290 292
Diaket, 292
GIC, 292
other types of cement, 292
requirements of, 290b
resin ionomer suspension and compomer,
292
zinc oxide eugenol cements, 290, 291t
RP. See Rapid prototyping (RP)
RTV silicone. See Room-temperature
vulcanization silicone (RTV silicone)
Rubber-reinforced resins, 87
Rubbery consistency silicones, 622
RUNX2, 606
Rutile, 549
Index
S
S174000 PH alloys, 547
S2G. See Scan2Guide (S2G)
Saliva, 106
Salivary functions, 379
Sand-blasting. See Grit-blasting
Sandwich technique, 155
Sankin apatite root canal sealer, 284t, 406,
406t
Saturation of color, 9
Scaffolds, 465 466, 644
for bone tissue engineering, 645 646
functions and features, 646
Scan2Guide (S2G), 523
Scanning electron microscopy (SEM), 460,
464f, 466f
“Sclerotic dentin”, 235
Scopus database, 383 385, 384t
Scotchbond 2, 238
Sculpturing clays and waxes, 635, 635f
Second-generation
adhesives, 237 238
of dental zirconia, 63 64
Secondary caries, 242 243
Selective infiltration etching, 332
Selective laser sintering, 520 521
Selective pressure techniques, 198 199
Selenium, 543 544, 544t
Self-adhesive composites, 156 157, 157t
resin cements, 130
Self-cured composites, 135
Self-etching primer (SEP), 236
Self-etching technique, 236
Self-healing composites, 154
Self-priming etchant. See Two-step self-etch
systems
Self-setting apatite-forming, 401 402
SEM. See Scanning electron microscopy
(SEM)
Sensitization, 543 544
SEP. See Self-etching primer (SEP)
Seventh-generation adhesives, 240
Seventh-generation adhesives, 241
SF. See Silk fibroin (SF)
Shade
selection, 516 517
shade-matching technique, 516 517
Shear strength, 21
Shore A hardness of VST silicones, 628, 629t
727
Short-term
fluoride burst release, 184
resilient liners, 98 99
Sialogram, 511t
SICAT software, 523
Sieverts unit (Sv unit), 513
Silane(s), 319, 332 333
coupling agent, 134
film thickness, 134
silane-treated aluminum particles, 89 90
Silanization, 485 486
Silastic MDX4 4210 biomedical grade
elastomer, 626
Silica (SiO2), 130 131, 455 456, 657 658
nanocomposites, 485
silica-based filler, 91
vapor nanofilm, 331
Silicate
cement, 176
silicate-based bioactive glasses,
457 458
Silicon, 657 658
Silicon carbide, 133 134
Silicon dioxide (SiO2), 91, 130
Silicon nitride, 133 134
Silicones, 620 622
A-221-05, 627
A-223-30, 627
A-223-40, 627
basic silicone unit, 621f
basic steps in silicone polymer synthesis,
621f
composition of silicone elastomer, 622t
condensation, 203
fluids, 629 631
polymer structures, 620 622, 620f
PVS, 202 203
silicone-based liners, 97 98
silicone-based sealers, 286t
VPES, 204
Silk, 650 651
Silk fibroin (SF), 650
Silorane, 130, 143, 148 149
Silver (Ag), 90 91, 153
points, 274 275, 275t
Silver diamine fluoride (SDF), 675 700
cariostatic effects
on caries in roots of the elderly, 682t
on cariogenic bacteria, 690 692
728
Silver diamine fluoride (SDF) (Continued)
on coronal caries in deciduous and
permanent teeth, 678t
on dental mineral, 685 689, 686t
on organic content of dentine, 692
clinical effects on caries management,
676 684
in adults, 683 684
in children, 677 683
in the elderly, 684
history, 676
safety of SDF treatment, 692 694
Silver fillings. See Dental amalgam
Silver modified ARTs (SMART), 683 684
Silver NPs (Ag NPs), 90 91
SIMODONT dental trainer, 534
Simplant, SurgiCase software, 523
Simvastatin-loaded porous implant surfaces,
660
Single-composition alloy, 112 113
Single-crystal alumina, 552
Single-edge-notched test method, 21
Sintering process, 56 57, 318, 552
Sixth-generation adhesives, 239 240
Sizing process, 310
Skin adhesives, 638 639
Slim, 518
Slip casting process, 306, 320
Smart composites, 150 154, 151f
antibacterial composites, 152 153, 152t
bioactive remineralizing composites,
150 151
polyacid modified composite, 153 154
self-healing composites, 154
SmartTrack, 564 565
Smear Clear, 270t
Smear layer, 231 232
adhesives classification based on
interaction with, 241
dissolving systems, 241
removing systems, 241
Sodium chloride, 45 46
Sodium fluoride (NaF), 152
Sodium hypochlorite (NaOCl), 231 232,
235, 263 265, 330
Sodium oxide (Na2O), 455 456, 657 658
Sodium phosphate, 201 202
Sodium-containing glass G338, 184 185
Sodium fluoride (NaF), 684, 690 691
Index
Sodium-free glass LG26, 184 185
Soft liners, 633 635, 634f
Soft relining, 96 98
methacrylate resin liners, 97
silicone-based liners, 97 98
“Soft-start” protocol, 143
Solid liquid transition endotherms, 9 11
Solid solid endotherms, 9 11
Solubility, 455 456
of resin composites, 144
Spatulation, 45
Specialty dentistry, 383 385
Specific heat, 13
Spin-coating, 590 592
Springback, 554
SrF2. See Strontium fluoride (SrF2)
SrO. See Strontium oxide (SrO)
SS. See Stainless steel (SS)
Stabilized martensitic NiTi, 559
Stainless steel (SS), 463, 542 543
alloys, 542 543, 546t
archwires, 556 557
advantages and disadvantages, 556t
austenitic SS, 545 547
brackets, 543 547
classifications, 544 545
effect of different elements on properties,
544t
materials, 545b
Stannous octoate, 203
Steel, 305
18 8 steel. See 304L steel
304L steel, 545
Stereolithography, 527
Sterilization methods, 77
Stiffness, 554
Strain, 17, 18f
Strength, 554
Streptococcus mutans, 243 244, 378,
690 691
Stress, 17
relaxation, 568
stress-shielding, 584 585
stress strain
cure region, 18
relationship, 16
Strontium, 144
Strontium fluoride (SrF2), 152
Strontium oxide (SrO), 130 131
Index
Substrate compliance, 142
Subtractive manufacturing, 517
Sugar-free gums, 390
Sulfuric acid (H2SO4), 590
Super austenitic SS, 547
Super ethoxybenzoic acid (Super EBA),
290 292, 291t
Supercable NiTi, 560
Superelastic NiTi, 560
Surface
chemistry, 74 76
grinding methods, 330 331
hardness, 50 51
roughness, 585
smoothness, 145
topography of zirconia surface, 329 333
Synthetic biomaterials, 217 218, 647,
654 655. See also Natural
biomaterials
for bone grafting, 350 362
PCL, 654 655
PEG, 654
PGA, 655
Synthetic calcium phosphate materials, 246
Synthetic HA, 357 359
Synthetic materials at metric scales, 478,
479f
Synthetic polymers, 646
Synthetic scaffold materials, 644 645
Syringe, 14
Systemic toxicity, 24
T
TA. See Tertiary amine (TA)
Tantalum, 543 544, 544t
Tarnish, 116 117
Tartaric acid ( 1 ), 180 181
TCD-DI-HEA, 143
TCP. See Tricalcium phosphate (TCP)
Tech Biosealer, 600
Teeth
anatomy and physiology, 302 304
cementum, 304
dental pulp, 304
dentin, 303 304
enamel, 303
cross section, 303f
development, 304
mechanical properties, 305
729
remineralization, 385 386, 390 392
TEETHMATE DESENSITIZER, 393 394
TEGDMA. See Triethylene glycol
dimethacrylate (TEGDMA)
Temperature, 9, 10f, 45
Temperature transition range (TTR), 559
Temporomandibular joint disorders, 512
Tensile
bond strength test, 71 73
loading, 19
strength, 20, 50, 114 115
Tertiary amine (TA), 135
Tetracalcium phosphate (TTCP), 389 390,
403 404
Tetraclean, 269
Tetracycline-HCl, 660
TetricEvoCeram (IvoclarVivadent,
Liechtenstein), 130 131
TFS. See Three-point FS (TFS)
Thallium amalgam, 109
TheraCal LC, 600
Thermaflo, 155
Thermal conductivity, 12, 13t
of fine composites, 144
Thermal diffusivity, 13 14
Thermal shock, 58
Thermal stress, 57 58, 144
Thermo-cured glass ionomers, 190
Thermocouples, 9
Thermoelasticity of NiTi alloys, 559 560
Thermoforming process, 565
Thermogram, 9 11, 10f
Thermoplastic aligners
forces, 565 567
differences in force generation,
565 566
material factors affecting force
delivery, 566 567
materials used for, 562, 564t
Thermoplastic resins, 92 93
thermoplastic acetal, 92
thermoplastic acrylic, 93
thermoplastic nylon, 92
thermoplastic polycarbonate, 93
Thermoset urethane elastomers, 619
Thiol-ene siloxane, 202 203
Third generation
adhesives, 238
of zirconia, 64
730
Thixotropic silicone extrinsic stains, 636,
637f
Thixotropy, 14
Three-dimension (3D)
CT imaging, 522 523
images, 509 510
printed scaffolds, 663 664
printers, 522
printing, 519 521, 530, 663 664
in implant dentistry, 521 522
systems, 37 38
structure, 645
Three-point flexural bend test, 186, 187f
Three-point FS (TFS), 187 188
“Three-step etch-and-rinse” technique.
See “Total-etch” technique
Ti 6Al 4V alloy, 549, 585 587, 659
“Tightly bound” water, 181
Timolium wires, 562
Tissue
conditioners, 98 99, 633 635
engineering, 1, 465 466, 490 491
approaches in calcium orthophosphate,
414 415
scaffolds, 1 2
triad, 644
regeneration, 490 491
Titania (TiO2), 75 76, 222 223, 589
Titanium, 90 91, 305, 543 544, 544t,
585 587, 659 660
brackets, 548 549
foams, 660
implants, 325
surface modifications and respective
properties, 586t
modification of titanium implants,
588 590
nanocomposites, 485
titanium-based wires, 561 562
titanium niobium wires, 561
titanium vanadium wires, 562
Titanium dioxide. See Titania (TiO2)
Titanium plasma spraying (TPS), 588 589,
588f
Titanium molybdenum alloys (TMA), 561
properties, 561b
Tomography, 511t
Tooth
decay. See Dental caries
Index
restoration, 311
tooth-supported guides, 526
Toothpastes, 386 389, 388t, 463 464
Top-down manufacturing, 219 220
Top-down nanomanufacturing, 219 220
“Total-etch” technique, 238 240
Toughness, 19
Toxic reaction, 25 26
Toxicity, 24 25
Toxicology of mercury, 118 119
TPO. See Diphenyl (2,4,6-trimethylbenzoyl)
phosphine oxide (TPO)
TPS. See Titanium plasma spraying (TPS)
Transbond XT, 407 408
Transition temperatures, 9 11
Transmission electron microscopy, 112
Tribochemical silica, 331
Tricalcium phosphate (TCP), 355 356, 359,
388t, 394, 646, 655 656
Triclosan, 153
Triethylene glycol dimethacrylate
(TEGDMA), 128 130
TEGDMA/Bis-GMA ratios, 141
Trimelitic acid methacrylate (4-MET),
156 157
Triple antibiotics pastes, 273
Tris-buffer solution, 454 455
Tropoelastin, 653
TTCP. See Tetracalcium phosphate (TTCP)
TTR. See Temperature transition range
(TTR)
Twisted wires, 557
Two-dimensional image (2D image),
514 515
Two-step
etch-and-rinse system, 240
self-etch systems, 241
systems, 240 241
Tx Studio software, 523
U
UDMA. See Urethane dimethacrylate
(UDMA)
UF. See Urea formaldehyde (UF)
Ultimate tensile strength, 20
Ultraviolet (UV), 77
Unalloyed zirconia, 326
Uncontrolled periodontal lesions, 483
Undisclosed CaPO4, 388t
Index
Unidirectional fibers, 308 309
United Nations Environment Programme
(UNEP), 106
Urea formaldehyde (UF), 154
Urethane dimethacrylate (UDMA), 84,
128 130, 153 154
Urethane methacrylate resin sealers, 280
US Food and Drug Administration (FDA),
454
UV. See Ultraviolet (UV)
V
Vacuum-form method, 565
Vascular endothelial growth factor (VEGF),
364 365
VDO. See Vertical dimension of occlusion
(VDO)
Venus Diamond Nanohybrid Composite
(Heraeus Kulzer), 143
Venus Diamond resin composite, 150
Vertical dimension of occlusion (VDO), 94
Vibrant human oral atmosphere, 16
Vinyl polyether siloxane (VPES), 204
Vinyl resins, 81
Vinylpolysiloxane (VPS), 204
Virtual Implant Planning software, 523
Viscoelastic behaviour, 142
Viscoelasticity, 305
Viscosity, 14, 207 208
Visible light cured resins, 84
Vita Enamic, 159 165
Vital pulp therapy
bioaggregate, 262
biodentine, 262
endosequence, 262 263
materials used in, 256 263, 258t
MTA, 257 261
MTA Angelus, 262
properties, 257b
Vitapan Chart system, 516 517
Vitrification, 56
Volumetric shrinkage, 141 142
Voxel-Man, 534
VPES. See Vinyl polyether siloxane (VPES)
VPS. See Vinylpolysiloxane (VPS)
VST silicones, 628
elastomers for maxillofacial prosthetics,
628f
properties, 629t
731
Vulcanite, 79 80
Vulcanization reaction of polymers, 624
W
W/P ratio. See Water/powder ratio (W/P
ratio)
Water
absorption, 568 569
wear, abrasion, and intraoral aging, 569
in GICs, 181
sorption, 142, 310
storage of resin composites,
144
water-based adhesives, 639
Water/powder ratio (W/P ratio), 44 45, 50f
Watt’s method, 149
Wax(es), 204 205
warmer, 155
Wear resistance, 167t
Weibull moduli, 73
Wettability of IMs, 208
Whiskers, 133 134
White spot lesions (WSL), 246 247
Wollastonite (CaSiO3), 602
Working range, 554
World Health Organization, 189
WSL. See White spot lesions (WSL)
X
X-ray diffraction (XRD), 28 29, 458 459
X-ray(s), 663 664
photoelectron spectroscopy, 457 458
Xenoestrogenic effect, 147
Xenografts, 354 355. See also Allografts
XRD. See X-ray diffraction (XRD)
Y
Y-TZP. See Yttria-stabilized tetragonal
zirconia crystal (Y-TZP)
YAG. See Yttrium aluminium garnet
(YAG)
YbF3. See Ytterbium trifluoride (YbF3)
Yellow Elgiloy, 558
Yield strength, 18
Young’s modulus, 108 109, 118, 484 485,
553
Ytterbium, 130 131
Ytterbium trifluoride (YbF3), 152
Yttria (Y2O3), 63, 326
732
Yttria-stabilized tetragonal zirconia crystal
(Y-TZP), 63
Yttrium, 660 661
Yttrium fluoride, 130 131
Yttrium oxide. See Yttria (Y2O3)
Yttrium-stabilized tetragonal zirconia,
326 328
physicochemical, electrical, and thermal
properties of, 327t
tetragonal monoclinic transformation
phase during crack propagation, 327f
Yttrium-stabilized zirconium oxide (ZrO2,
Y-TZP), 527 528
Yttrium aluminium garnet (YAG), 531
Z
Zinc oxide (ZnO), 117 118, 133 134,
242 243, 245
nanoparticles, 153
Zinc oxide eugenol (ZOE), 271, 278, 279t
cements, 176, 290, 291t
sealers, 278, 279t, 286t
Zinc oxide eugenol impression paste.
See Metallic oxide pastes
Zinc phosphate cement, 176
Zirconia (ZrO2), 61 64, 62f, 68f, 72t, 75f,
90, 222, 320, 322, 328, 485,
586 587, 660 661
adhesion to, 329 333
Index
classification, 321 324, 321t, 322f
in dentistry, 222, 324 325, 325t
failure and fractographic analysis of
zirconia restorations, 333 335
fully crystallized glass-ceramic milling
block, 321f
limitations and challenges, 337 338
mechanical testing of zirconia ceramics,
335 337
modification of zirconia implants, 592
surface topography, clinical treatments of
zirconia surface, 329 333
yttrium-stabilized tetragonal zirconia,
326 328
zirconia-based ceramics, 324
zirconia-lithium silicate, 60 61
zirconia/silica, 133 134
ZTA, 328 329
Zirconia-toughened alumina (ZTA), 320,
328 329
Zirconium (Zr), 324, 661
Zirconium dioxide, 324, 660 661
Zirconium-oxide/zirconia ceramics, 55 56
ZnO QDs (ZnOQDs), 245
ZOE. See Zinc oxide eugenol (ZOE)
Zombies, 691 692
ZTA. See Zirconia-toughened alumina
(ZTA)